
Space occupying lesions of the Brain
68
SPACE OCCUPYING SPACE OCCUPYING LESIONS LESIONS OF THE BRAIN OF THE BRAIN 16 DECEMBER 2013 16 DECEMBER 2013
-
Upload
liew-boon-seng -
Category
Education
-
view
1.363 -
download
19
description
Intracranial Space occupying lesions
Transcript of Space occupying lesions of the Brain
SPACE SPACE OCCUPYING OCCUPYING
LESIONSLESIONSOF THE BRAINOF THE BRAIN
16 DECEMBER 201316 DECEMBER 2013
CONTENTCONTENT
DEFINITION OF SOLDEFINITION OF SOL TYPES OF SOL IN THE BRAINTYPES OF SOL IN THE BRAIN SIGNS AND SYMPTOMSSIGNS AND SYMPTOMS NEUROIMAGING AND OTHER NEUROIMAGING AND OTHER
INVESTIGATIONSINVESTIGATIONS TREATMENTTREATMENT PROGNOSISPROGNOSIS
DEFINITION OF SOLDEFINITION OF SOL
Substantial physical lesions, e.g. Substantial physical lesions, e.g. neoplasm, hemorrhage, granuloma, neoplasm, hemorrhage, granuloma, which occupy space; the effect is which occupy space; the effect is more significant if the lesion is more significant if the lesion is within a space confined by bone, e.g. within a space confined by bone, e.g. thorax, cranium, thorax, cranium, bone bone marrowmarrow cavity. cavity.
SOL OF THE BRAIN : SOL OF THE BRAIN : Within the Within the cranium or skull. cranium or skull.
TYPES OF SOL IN THE TYPES OF SOL IN THE BRAINBRAIN
NeoplasmNeoplasm Meningioma, glioma, pituitary tumourMeningioma, glioma, pituitary tumour
InfectionInfection E.g. abscess, tuberculomaE.g. abscess, tuberculoma
Vascular lesionsVascular lesions AVM, cavernoma, giant aneurysmAVM, cavernoma, giant aneurysm HemorrhageHemorrhage
NeoplasmNeoplasm
InfectionInfection
Vascular lesionsVascular lesions
SIGNS AND SYMPTOMSSIGNS AND SYMPTOMS Neurological phenomena is caused by irritation or Neurological phenomena is caused by irritation or
destruction of brain tissue, e.g.destruction of brain tissue, e.g. Focal seizures (Jacksonian epilepsy)Focal seizures (Jacksonian epilepsy) Paralysis. Paralysis.
Headache Headache Do not respond to simple medicines refers to the possibility Do not respond to simple medicines refers to the possibility
of ICSOL. of ICSOL. The headache is felt in the midline over the head of at times The headache is felt in the midline over the head of at times
it is referred over the site of lesion, e.g meningioma. it is referred over the site of lesion, e.g meningioma. It will be continuous and progressive, paroxysmal (as in It will be continuous and progressive, paroxysmal (as in
migraine), or aggravated by coughing, stooping forward migraine), or aggravated by coughing, stooping forward and changing postures.and changing postures.
Patients with headaches that wake them at night or are Patients with headaches that wake them at night or are worse in the morning, or who have focal neurologic deficits, worse in the morning, or who have focal neurologic deficits, require urgent neuroimaging. require urgent neuroimaging.
However, many patients with brain tumours present with However, many patients with brain tumours present with headaches that are indistinguishable from tension headaches that are indistinguishable from tension headaches.headaches.
SIGNS AND SYMPTOMSSIGNS AND SYMPTOMS Vomiting and visual loss: Vomiting and visual loss:
In many cases, protracted vomiting is a common In many cases, protracted vomiting is a common symptom. symptom.
Projectile vomiting is mistaken for gastrointestinal or Projectile vomiting is mistaken for gastrointestinal or psychiatric disturbances. psychiatric disturbances.
Failure of vision because of late papilloedema Failure of vision because of late papilloedema phenomenon.phenomenon.
Impairment of conscious level due to raised intracranial Impairment of conscious level due to raised intracranial pressure.pressure. Headaches, nausea, vomiting, and changes in mental Headaches, nausea, vomiting, and changes in mental
status, cognition, and progressive altered levels of status, cognition, and progressive altered levels of consciousness alongside other indicative signs such as consciousness alongside other indicative signs such as papilloedema usually reflect raised intracranial papilloedema usually reflect raised intracranial pressure from mass effect or hydrocephalus.pressure from mass effect or hydrocephalus.
Late onset of seizures: Late onset of seizures: Any type of seizure if occurs for the first time after the Any type of seizure if occurs for the first time after the
age of 15 years will suggest the possibility of ICSOL. age of 15 years will suggest the possibility of ICSOL.
SIGNS AND SYMPTOMSSIGNS AND SYMPTOMS Both nonspecific and focal neurologic complaints Both nonspecific and focal neurologic complaints
and symptoms can alert the primary care and symptoms can alert the primary care physician or neurologist to the possibility of an physician or neurologist to the possibility of an underlying mass lesion and indicate the need for underlying mass lesion and indicate the need for further work - up. further work - up.
Key aspects of the history that help differentiate Key aspects of the history that help differentiate neoplastic lesions from other diagnoses includeneoplastic lesions from other diagnoses include Timing of symptom onset, Timing of symptom onset, Tempo of progression, Tempo of progression, Severity of symptoms. Severity of symptoms.
Systemic symptoms and the presence of other Systemic symptoms and the presence of other diseases or hereditary syndromes are additional diseases or hereditary syndromes are additional valuable pieces of information that can help valuable pieces of information that can help narrow the diagnosis by their association with narrow the diagnosis by their association with specific CNS tumours.specific CNS tumours.
SIGNS AND SYMPTOMSSIGNS AND SYMPTOMS Other symptoms and signs, such as global mental Other symptoms and signs, such as global mental
status changes, are quite common and include status changes, are quite common and include apathy, change in personality, irritability, apathy, change in personality, irritability, psychomotor retardation, lethargy, and psychomotor retardation, lethargy, and forgetfulness.forgetfulness.
Such nonspecific impairments in mental function Such nonspecific impairments in mental function have been linked to lesions in the frontal and have been linked to lesions in the frontal and temporal lobes, corpus callosum, thalamocortical temporal lobes, corpus callosum, thalamocortical fibers, and reticular formation, among others.fibers, and reticular formation, among others.
Still other non-localizable presentations are the Still other non-localizable presentations are the result of multifocal tumours, often seen in result of multifocal tumours, often seen in metastatic disease, presenting with a mixture of metastatic disease, presenting with a mixture of focal signs and symptoms that can be confused focal signs and symptoms that can be confused for generalized clinical manifestations.for generalized clinical manifestations.
SIGNS AND SYMPTOMSSIGNS AND SYMPTOMS Brain tumourBrain tumour
Symptoms produced by brain tumors may be Symptoms produced by brain tumors may be either nonspecific or focal, and in general tend either nonspecific or focal, and in general tend to be subacute in onset. to be subacute in onset.
The presentation varies widely and neither a The presentation varies widely and neither a normal neurologic exam nor presentation with normal neurologic exam nor presentation with acute onset of symptoms rules out a brain acute onset of symptoms rules out a brain tumour. tumour.
At the outset many brain tumours produce At the outset many brain tumours produce minimal or no symptoms.minimal or no symptoms.
Brain tumors can also present with acute onset Brain tumors can also present with acute onset stroke - like symptoms. stroke - like symptoms.
SIGNS AND SYMPTOMSSIGNS AND SYMPTOMS Brain tumourBrain tumour
This type of acute presentation is usually the This type of acute presentation is usually the result of a focal seizure or hemorrhage into result of a focal seizure or hemorrhage into the tumour bed.the tumour bed.
The rate of progression of symptoms is also The rate of progression of symptoms is also quite variable but tends to be gradual over quite variable but tends to be gradual over weeks to months, helping to differentiate weeks to months, helping to differentiate neoplasms from other more static disorders neoplasms from other more static disorders such as degenerative disease or more rapidly such as degenerative disease or more rapidly progressing infectious conditions. progressing infectious conditions.
By paralleling the growth and spread of CNS By paralleling the growth and spread of CNS neoplasms, the rate of symptomatic neoplasms, the rate of symptomatic progression can serve as a rough clinical progression can serve as a rough clinical estimate to tumour grade.estimate to tumour grade.
SIGNS AND SYMPTOMSSIGNS AND SYMPTOMS Brain tumourBrain tumour
Typically, benign tumours such as meningiomas, or Typically, benign tumours such as meningiomas, or low - grade neoplasms such as oligodendrogliomas, low - grade neoplasms such as oligodendrogliomas, will have a slower progression of symptoms than will have a slower progression of symptoms than more malignant tumours such as glioblastomas.more malignant tumours such as glioblastomas.
A careful review of systems, for instance, should A careful review of systems, for instance, should identify symptoms such as weight loss, lethargy, identify symptoms such as weight loss, lethargy, and night sweats that are nonspecific but can be and night sweats that are nonspecific but can be associated with many types of cancers.associated with many types of cancers.
When combined with neurologic symptoms, these When combined with neurologic symptoms, these symptoms should raise suspicion of primary or symptoms should raise suspicion of primary or metastatic CNS neoplasms, though should not rule metastatic CNS neoplasms, though should not rule out subacute infectious, inflammatory, or out subacute infectious, inflammatory, or autoimmune CNS processes.autoimmune CNS processes.
SIGNS AND SYMPTOMSSIGNS AND SYMPTOMS Brain tumourBrain tumour
Likewise, a detailed review of past medical Likewise, a detailed review of past medical history may identify genetic syndromes or history may identify genetic syndromes or other conditions with a higher than normal other conditions with a higher than normal incidence of CNS neoplasms.incidence of CNS neoplasms.
Neurofibromatosis type 1 is associated with Neurofibromatosis type 1 is associated with gliomas and cutaneous manifestations, gliomas and cutaneous manifestations,
Neurofibromatosis type 2 is associated with Neurofibromatosis type 2 is associated with vestibular schwannomas and meningiomas, vestibular schwannomas and meningiomas,
Von Hippel – Lindau syndrome is associated Von Hippel – Lindau syndrome is associated with hemangioblastomas.with hemangioblastomas.
SIGNS AND SYMPTOMSSIGNS AND SYMPTOMS Intracranial InfectionIntracranial Infection
The onset of acute bacterial meningitis is The onset of acute bacterial meningitis is rapid: hours to a day or so. rapid: hours to a day or so.
Classic clinical findings include signs of an Classic clinical findings include signs of an acute cerebral disorder, with lethargy, acute cerebral disorder, with lethargy, seizures, and agitation as well as specific signs seizures, and agitation as well as specific signs of meningeal involvement manifested by of meningeal involvement manifested by severe neck stiffness, called severe neck stiffness, called meningismusmeningismus
Fever that may not be immediately present. Fever that may not be immediately present. The patient rapidly becomes confused, sleepy, The patient rapidly becomes confused, sleepy,
obtunded, and often comatoseobtunded, and often comatose
SIGNS AND SYMPTOMSSIGNS AND SYMPTOMS Intracranial InfectionIntracranial Infection
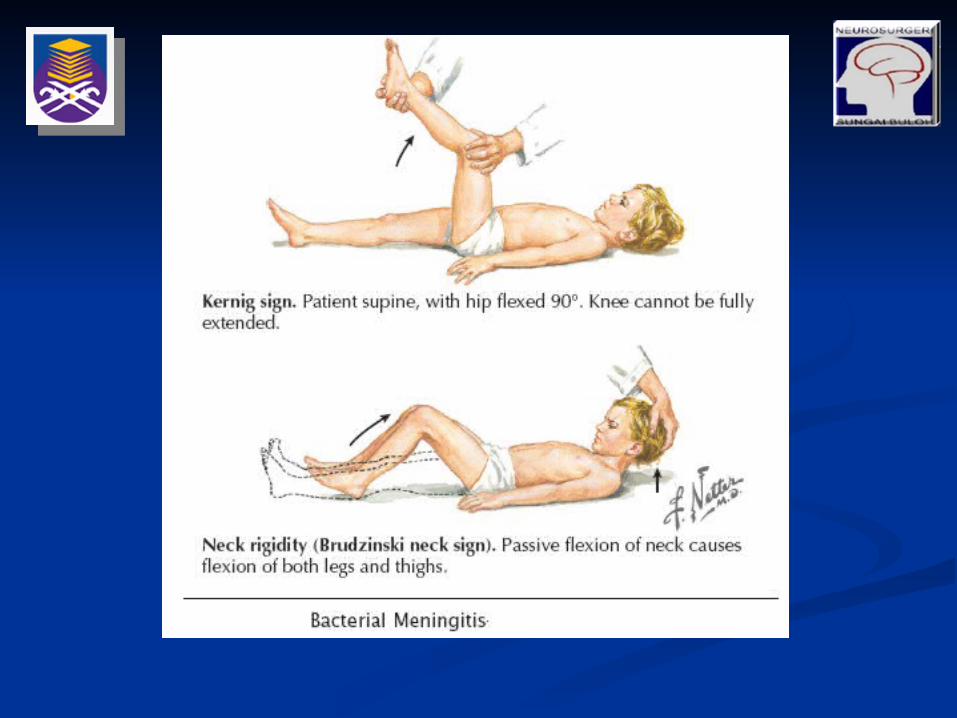
For identifying the presence of inflamed For identifying the presence of inflamed meningeal coverings involving the lumbosacral meningeal coverings involving the lumbosacral nerve roots: nerve roots: The The Kernig sign Kernig sign
is elicited by flexing the patient’s hip to a is elicited by flexing the patient’s hip to a 90-degree angle and then attempting to 90-degree angle and then attempting to passively straighten the leg at the knee; passively straighten the leg at the knee; pain and tightness in the hamstring muscles pain and tightness in the hamstring muscles prevent completion of this maneuver. This prevent completion of this maneuver. This sign should be present bilaterally to support sign should be present bilaterally to support a diagnosis of meningitis. a diagnosis of meningitis.
The The Brudzinski sign Brudzinski sign is positive if the patient’s hips and knees flex is positive if the patient’s hips and knees flex
automatically when the examiner flexes the automatically when the examiner flexes the patient’s neck while the patient is supinepatient’s neck while the patient is supine. .
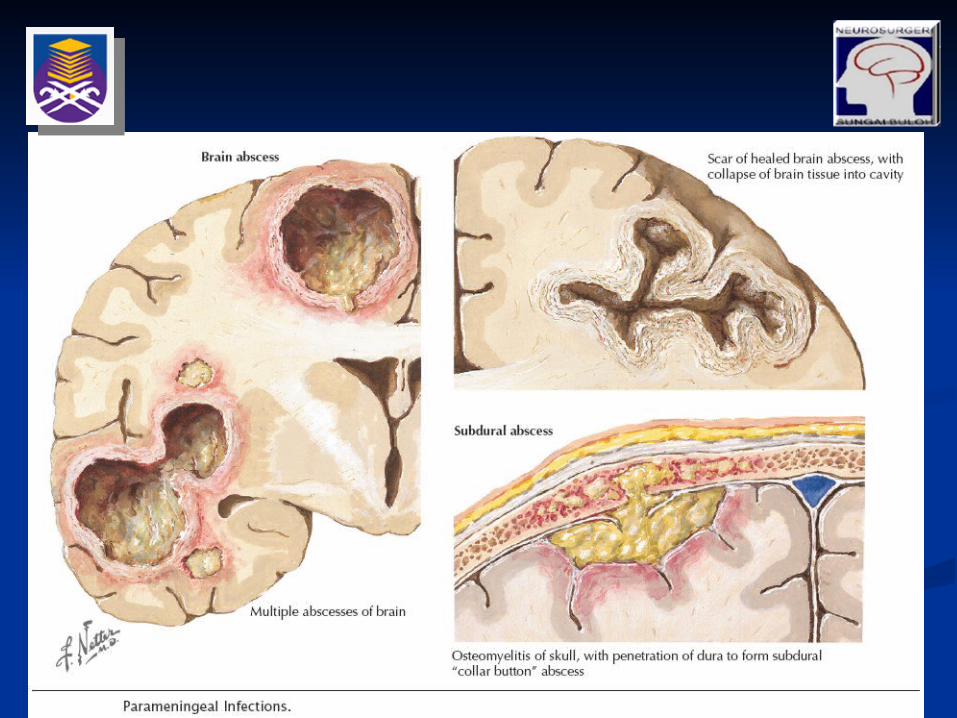
SIGNS AND SYMPTOMSSIGNS AND SYMPTOMS Brain abscessBrain abscess
The cardinal symptom of brain abscess is The cardinal symptom of brain abscess is persistent and progressive headache, usually persistent and progressive headache, usually followed by focal neurologic manifestations. followed by focal neurologic manifestations.
Only two thirds of patients have fever. Only two thirds of patients have fever. Papilloedema and other signs of increased Papilloedema and other signs of increased
intracranial pressure may occasionally develop; intracranial pressure may occasionally develop; however, the availability of imaging studies however, the availability of imaging studies makes it more likely that the abscess will be makes it more likely that the abscess will be identified prior to its obtaining significant identified prior to its obtaining significant enough mass to create increased intracranial enough mass to create increased intracranial pressure.pressure.
SIGNS AND SYMPTOMSSIGNS AND SYMPTOMS Subdural abscessSubdural abscess
It is typically characterized by a purulent It is typically characterized by a purulent collection within the potential space between the collection within the potential space between the dura mater and arachnoid membrane dura mater and arachnoid membrane
Localized swelling, erythema, headache, or Localized swelling, erythema, headache, or tenderness of the site overlying the primary tenderness of the site overlying the primary infection may occur. infection may occur.
As the illness progresses, the headache becomes As the illness progresses, the headache becomes generalized and severe, with a high fever, generalized and severe, with a high fever, vomiting, and nuchal rigidity developing. vomiting, and nuchal rigidity developing.
Seizures, hemiparesis, visual field defects, and Seizures, hemiparesis, visual field defects, and papilledema sometimes occur.papilledema sometimes occur.
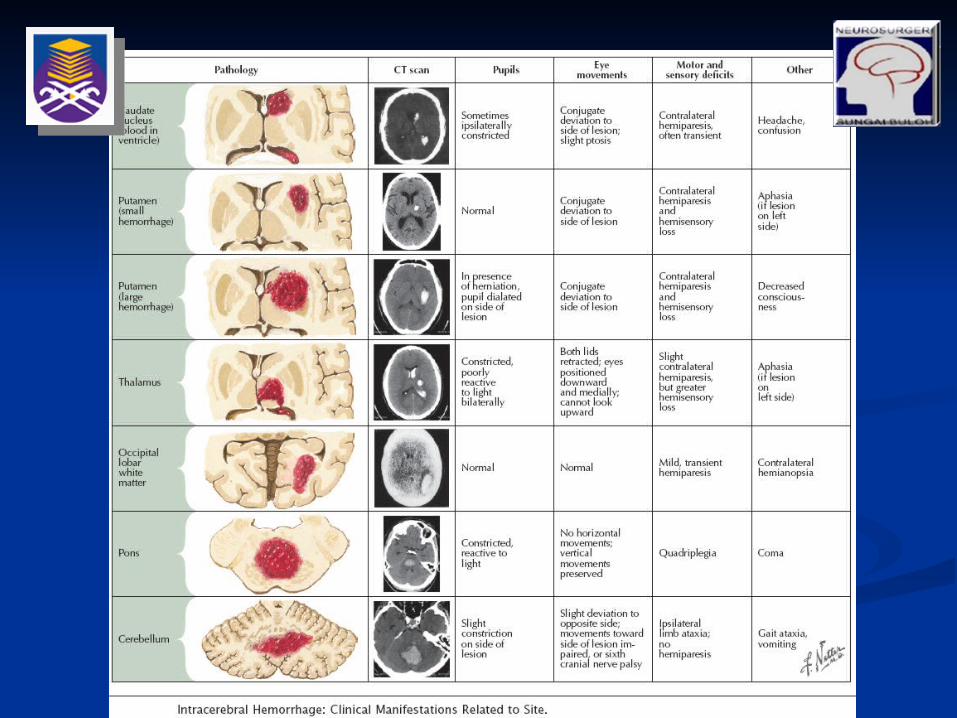
SIGNS AND SYMPTOMSSIGNS AND SYMPTOMS Intracranial HemorrhageIntracranial Hemorrhage
Intraparenchymal hemorrhages vary in Intraparenchymal hemorrhages vary in presentation depending on the site of the presentation depending on the site of the bleeding. bleeding.
In approximately 60% of patients, neurologic In approximately 60% of patients, neurologic symptoms develop gradually or stepwise over a symptoms develop gradually or stepwise over a period of hours. period of hours.
To some extent, the location and size of the To some extent, the location and size of the hematoma predict clinical outcome.hematoma predict clinical outcome.
Headache occurs at presentation in Headache occurs at presentation in approximately 40% of patients with ICH. approximately 40% of patients with ICH.
Less commonly, headache develops within a few Less commonly, headache develops within a few days after the ictus. days after the ictus.
Intracerebral hemorrhages presenting with Intracerebral hemorrhages presenting with headache are often located at the brain surface or headache are often located at the brain surface or within the cerebellum.within the cerebellum.
SIGNS AND SYMPTOMSSIGNS AND SYMPTOMS Intracranial HemorrhageIntracranial Hemorrhage
Depression in the level of consciousness and Depression in the level of consciousness and vomiting occur in 50% of patients, particularly vomiting occur in 50% of patients, particularly those with large cerebellar bleeds. those with large cerebellar bleeds.
Seizures occur at onset in up to 10% and are Seizures occur at onset in up to 10% and are seen most commonly with lobar bleeds in the seen most commonly with lobar bleeds in the anterior circulation. anterior circulation.
There are rare incidences of patients with There are rare incidences of patients with deep hemorrhages having seizures.deep hemorrhages having seizures.
SIGNS AND SYMPTOMSSIGNS AND SYMPTOMS Intracranial HemorrhageIntracranial Hemorrhage
The subsequent risk for seizures in ICH The subsequent risk for seizures in ICH patients is up to 29% for those with lobar patients is up to 29% for those with lobar hemorrhages but only 4% for those with deep hemorrhages but only 4% for those with deep hemorrhages. hemorrhages.
Other symptoms seen in association with ICH Other symptoms seen in association with ICH include low-grade fever without obvious include low-grade fever without obvious infection, cardiac arrhythmias, and infection, cardiac arrhythmias, and dysautonomia, especially with pontine bleeds. dysautonomia, especially with pontine bleeds.
NEUROIMAGING AND NEUROIMAGING AND OTHER INVESTIGATIONSOTHER INVESTIGATIONS
Routine blood tests will include FBC, U&E and LFTs. Routine blood tests will include FBC, U&E and LFTs. Na+ will be low due to inappropriate ADH secretion.Na+ will be low due to inappropriate ADH secretion. Skull x-ray is usually done , but if pineal gland is Skull x-ray is usually done , but if pineal gland is
calcified, then a shift is seen.calcified, then a shift is seen. Imaging studies include CT scan and MRI-scan are Imaging studies include CT scan and MRI-scan are
required. required. Both works very good but MRI is better in Both works very good but MRI is better in
delineating soft tissue.delineating soft tissue. A known primary tumour will exist or it can be A known primary tumour will exist or it can be
sought out by chest x-ray or by mammography.sought out by chest x-ray or by mammography. Imaging tests will indicate the site of a lesion but Imaging tests will indicate the site of a lesion but
usually it will not indicate the nature or whether it is usually it will not indicate the nature or whether it is a tumour or an abscess. a tumour or an abscess.
NEUROIMAGINGNEUROIMAGING Skull radiographSkull radiograph
Pituitary fossa abnormalities.Pituitary fossa abnormalities. Bone density changes (e.g. tumour, Bone density changes (e.g. tumour,
meningioma, Paget’s).meningioma, Paget’s). Position of calcified pinealPosition of calcified pineal
NEUROIMAGINGNEUROIMAGING Cranial CTCranial CT
Disturbances in the normal anatomy of the Disturbances in the normal anatomy of the ventricular system.ventricular system.
Skull base and vault.Skull base and vault. Width of cortical fissures/sulci.Width of cortical fissures/sulci. Midline shift.Midline shift. Areas of abnormal tissue density.Areas of abnormal tissue density. Opacity or lucency of sinuses.Opacity or lucency of sinuses. Normal flow voids.Normal flow voids.
NEUROIMAGINGNEUROIMAGING Cranial CTCranial CT
High density (‘white’) signalHigh density (‘white’) signal Fresh blood.Fresh blood. Calcification:Calcification:
Slow growing tumour.Slow growing tumour. AVM/aneurysm.AVM/aneurysm. Hamartoma.Hamartoma. In pineal/choroid plexus/basal ganglia, In pineal/choroid plexus/basal ganglia,
may be normalmay be normal..
NEUROIMAGINGNEUROIMAGING Cranial CTCranial CT
Low density (‘black’) signalLow density (‘black’) signal Infarction.Infarction. Tumour.Tumour. Abscess.Abscess. Oedema.Oedema. Encephalitis.Encephalitis. Resolving haematoma.Resolving haematoma.
NEUROIMAGINGNEUROIMAGING Cranial CTCranial CT
Mixed densityMixed density Tumour.Tumour. Abscess.Abscess. AVM.AVM. Contusion.Contusion. Haemorrhagic infarct.Haemorrhagic infarct.

NEUROIMAGINGNEUROIMAGING Cranial CT (Cranial CT (After administration of IV contrast After administration of IV contrast
medium)medium) Common patterns of enhancement includeCommon patterns of enhancement include
Ring enhancement of tumours and Ring enhancement of tumours and abscesses.abscesses.
Solid enhancement of meningiomas.Solid enhancement of meningiomas. Meningeal enhancement with meningeal Meningeal enhancement with meningeal
disease involvement.disease involvement.
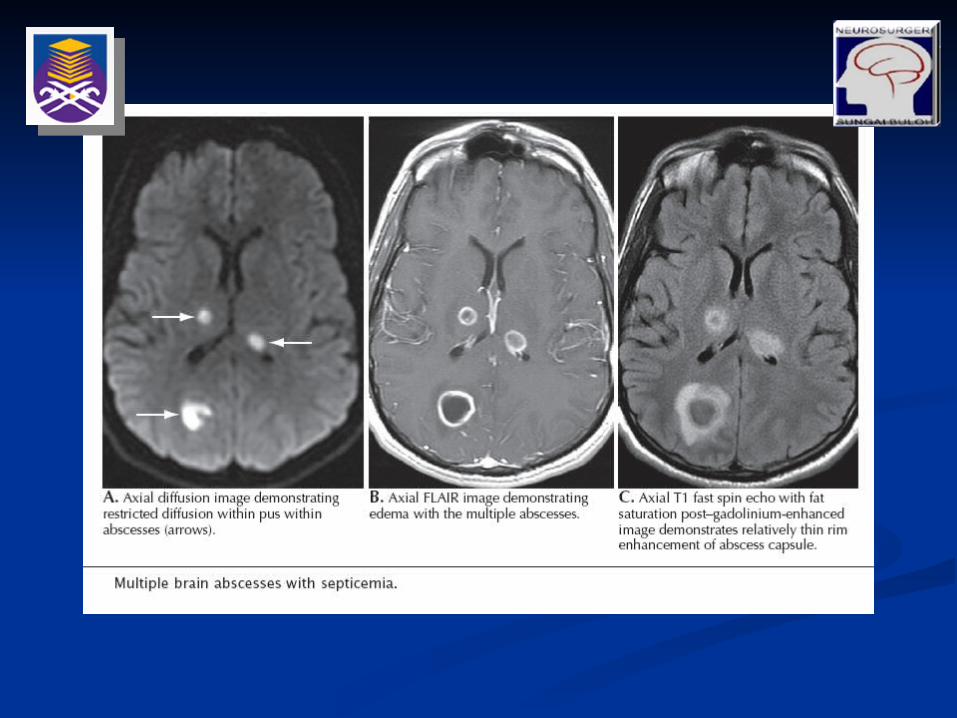
NEUROIMAGINGNEUROIMAGING Magnetic resonance imaging (MRI)Magnetic resonance imaging (MRI)
In generalIn general T1 CSF is hypointense (‘black’); fat and mature T1 CSF is hypointense (‘black’); fat and mature
blood clot white.blood clot white. T2 CSF is hyperintense (‘white’).T2 CSF is hyperintense (‘white’).
MRI with enhancement (MRI with enhancement (Intravenously Intravenously administered gadolinium leaks through areas of administered gadolinium leaks through areas of damaged blood--brain barrier to give a marked damaged blood--brain barrier to give a marked enhancement)enhancement)
Ischaemia.Ischaemia. Infection.Infection. Tumour (may help differentiate from Tumour (may help differentiate from
surrounding oedema).surrounding oedema). Active demyelination.Active demyelination.
NEUROIMAGINGNEUROIMAGING Positron Emission TomographyPositron Emission Tomography
Form of molecular imaging that requires an Form of molecular imaging that requires an injection of a radioactive tracer into the blood injection of a radioactive tracer into the blood stream.stream.
Radionuclide tracers are prepared using a Radionuclide tracers are prepared using a cyclotron device and a wide variety of cyclotron device and a wide variety of molecules can be labelled by this means, molecules can be labelled by this means, including metabolically active substances.including metabolically active substances.
18 F-fluorodeoxyglucose (FDG).18 F-fluorodeoxyglucose (FDG).
NEUROIMAGINGNEUROIMAGING Positron Emission TomographyPositron Emission Tomography
Metabolic imaging technique that is capable of Metabolic imaging technique that is capable of differentiating benign and malignant tumours differentiating benign and malignant tumours more accurately.more accurately.
Used extensively in staging of brain tumours Used extensively in staging of brain tumours as it can produce a visual mapping of as it can produce a visual mapping of biochemical changes caused by the metabolic biochemical changes caused by the metabolic activity of the brain tumour.activity of the brain tumour.
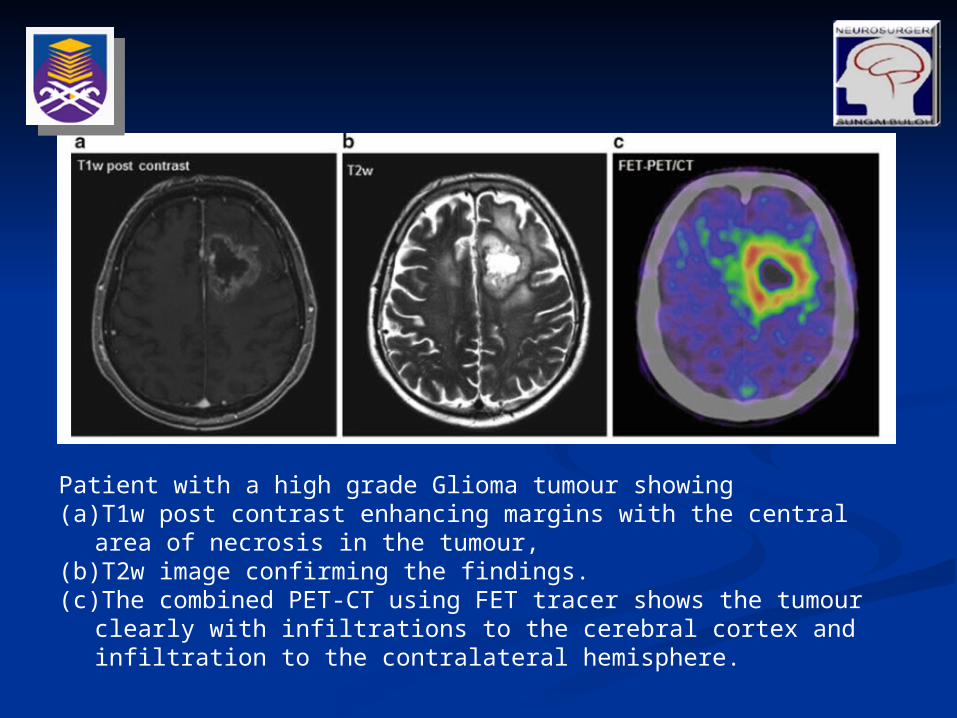
Patient with a high grade Glioma tumour showing (a) T1w post contrast enhancing margins with the central area of necrosis in
the tumour, (b) T2w image confirming the findings. (c) The combined PET-CT using FET tracer shows the tumour clearly with
infiltrations to the cerebral cortex and infiltration to the contralateral hemisphere.
NEUROIMAGINGNEUROIMAGING AngiographyAngiography
Strongly suspected or confirmed SAH.Strongly suspected or confirmed SAH. Suspected cerebral vasculitisSuspected cerebral vasculitis Delineation of other vascular abnormalitiesDelineation of other vascular abnormalities
arteriovenous malformations, AVMarteriovenous malformations, AVM Delineation of tumour blood supplyDelineation of tumour blood supply
NEUROIMAGINGNEUROIMAGING
NEUROIMAGINGNEUROIMAGING
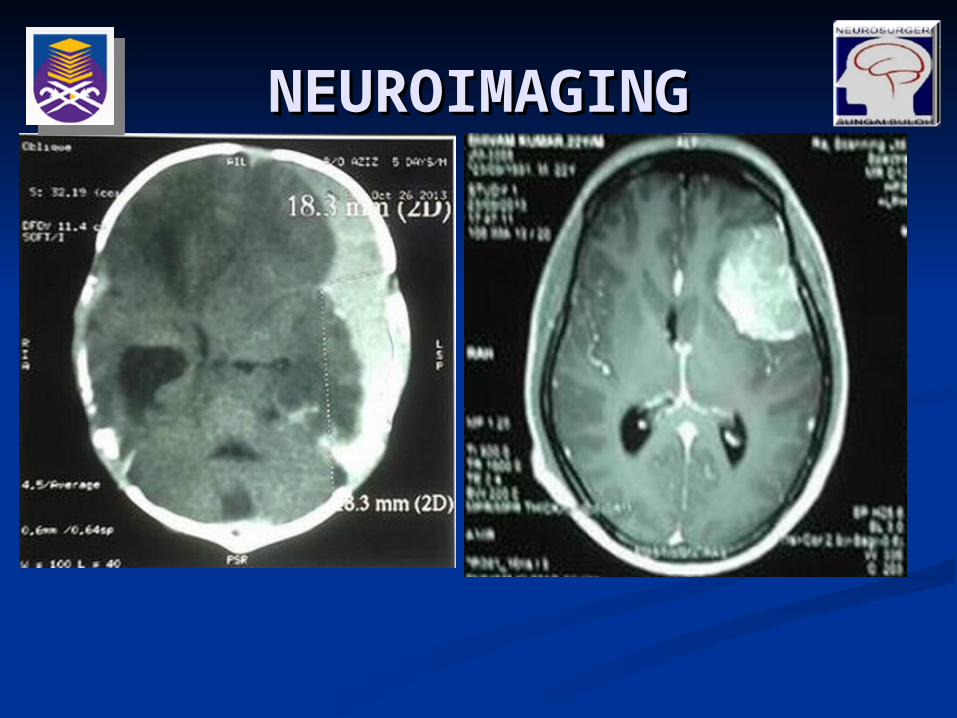
NEUROIMAGINGNEUROIMAGING
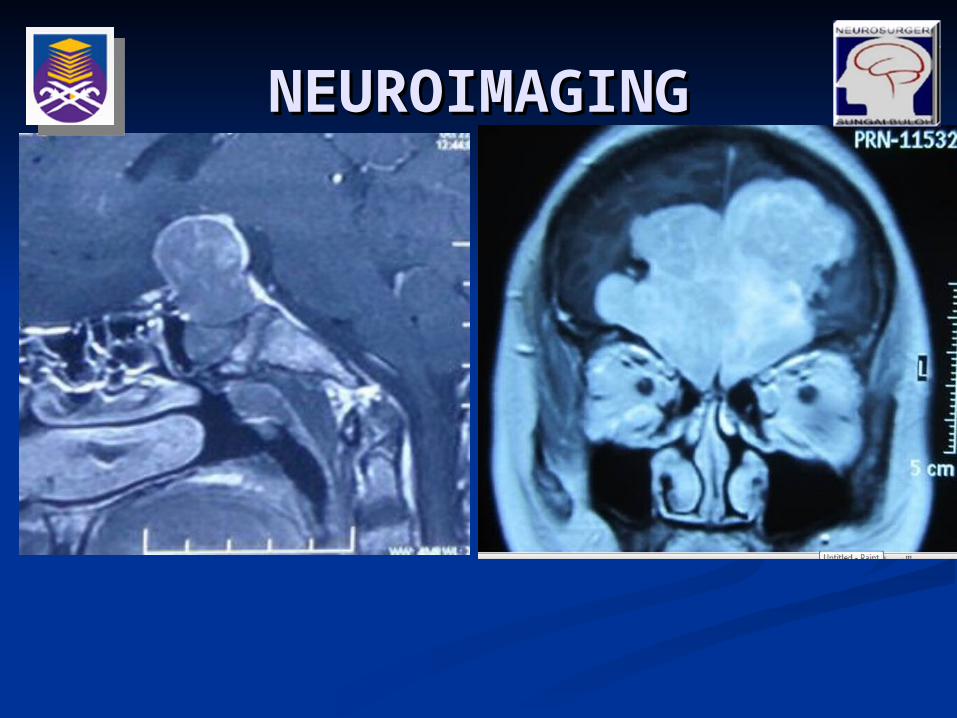
NEUROIMAGINGNEUROIMAGING
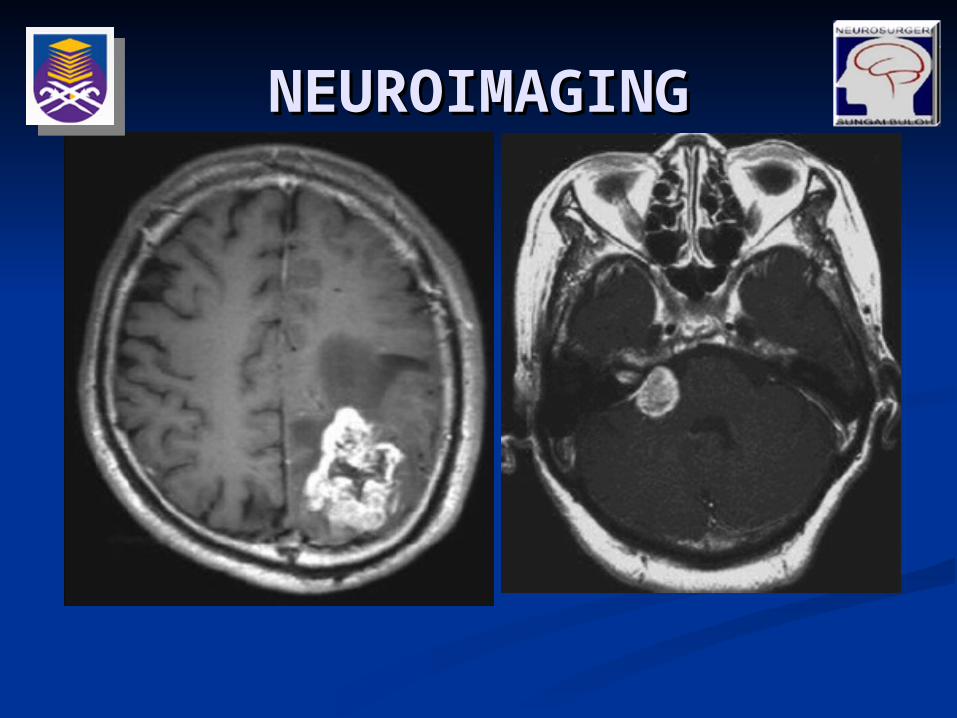
NEUROIMAGINGNEUROIMAGING

INVESTIGATIONSINVESTIGATIONS Lumbar puncture (LP)Lumbar puncture (LP)
CNS Infection:CNS Infection: Meningitis.Meningitis. Encephalitis/ Cerebral abscessEncephalitis/ Cerebral abscess
Suspected subarachnoid haemorrhage (SAH). Suspected subarachnoid haemorrhage (SAH). In general, a –ve CT does not exclude a SAH.In general, a –ve CT does not exclude a SAH.
Suspected malignancy with meningeal Suspected malignancy with meningeal involvement.involvement.
To seek specific antibodies/markers in CSF, To seek specific antibodies/markers in CSF, Syphilis.Syphilis. Tumour markers.Tumour markers.
INVESTIGATIONSINVESTIGATIONS Diagnostic & prognostic antibodies and Diagnostic & prognostic antibodies and
other markers in blood other markers in blood Systemic infectionsSystemic infections
Serology for many diseases Serology for many diseases e.g. e.g. Borrelia Borrelia in Lyme disease; HIV.in Lyme disease; HIV.
PCR for TB.PCR for TB. Disorders of coagulation: thrombophilia Disorders of coagulation: thrombophilia
screen currently commonlyscreen currently commonly Protein S and C levels.Protein S and C levels. Antithrombin III levels.Antithrombin III levels. Screening for the Leiden mutation in factor Screening for the Leiden mutation in factor
V.V. Lupus anticoagulant.Lupus anticoagulant.
INVESTIGATIONSINVESTIGATIONS Diagnostic & prognostic antibodies and Diagnostic & prognostic antibodies and
other markers in blood other markers in blood Tumour markersTumour markers
CEA for gut neoplasia (brain metastasis)CEA for gut neoplasia (brain metastasis) Beta HCG, Alphafetoprotein in pineal Beta HCG, Alphafetoprotein in pineal
tumourtumour EndocrinopathiesEndocrinopathies
TSH, T4, GH, Prolactin, Cortisol in pituitary TSH, T4, GH, Prolactin, Cortisol in pituitary lesion lesion
INVESTIGATIONSINVESTIGATIONS Neuro-otologyNeuro-otology
Pure tone audiometryPure tone audiometry For lesion with the involvement of auditory For lesion with the involvement of auditory
meatusmeatus Acoustic neuromaAcoustic neuroma CPA meningiomaCPA meningioma
Neuro-ophtalmologyNeuro-ophtalmology Visual field and Visual acuityVisual field and Visual acuity
Lesion with the involvement of optic nerves, Lesion with the involvement of optic nerves, optic tract, optic radiation and visual cortexoptic tract, optic radiation and visual cortex
TREATMENTTREATMENT Management will depends mainly on the cause of Management will depends mainly on the cause of
lesion.lesion. If possible, especially with primary tumours If possible, especially with primary tumours
complete excision is done but this is so difficult complete excision is done but this is so difficult due to infiltration and by surrounding structures.due to infiltration and by surrounding structures.
These will vary with radiosensitivity and will These will vary with radiosensitivity and will show response to chemotherapy.show response to chemotherapy.
If malignancy is metastatic then treatment should If malignancy is metastatic then treatment should include radiotherapy. include radiotherapy.
However, surgery is contemplated with up to 3 However, surgery is contemplated with up to 3 metastases.metastases.
Haematoma will need evacuation.Haematoma will need evacuation. Infectious lesions will need both evacuation and Infectious lesions will need both evacuation and
antibiotics.antibiotics.
TREATMENTTREATMENT Other treatments are required either as a part of Other treatments are required either as a part of
radical treatment or as palliative care.radical treatment or as palliative care. Dexamethasone will reduce cerebral oedema.Dexamethasone will reduce cerebral oedema. Mannitol will reduce raised intracranial Mannitol will reduce raised intracranial
pressure.pressure. Anticonvulsants are required but are not to be Anticonvulsants are required but are not to be
given prophylactically .given prophylactically . Treat headache with codeine phosphate because Treat headache with codeine phosphate because
it will avoids the pupillary effect of opiates.it will avoids the pupillary effect of opiates.
TREATMENTTREATMENT BiopsiesBiopsies
A biopsy should be undertaken to answer specific A biopsy should be undertaken to answer specific questions, in the light of a differential diagnosis questions, in the light of a differential diagnosis formulated following history, examination and formulated following history, examination and other investigations.other investigations.
Diagnosis and management of suspected primary Diagnosis and management of suspected primary and some metastatic brain tumours. (Tissue and some metastatic brain tumours. (Tissue diagnosis)diagnosis)
Differential diagnosis of other mass lesions Differential diagnosis of other mass lesions (inflammatory and infective).(inflammatory and infective).
Differentiation of radiation necrosis and tumour Differentiation of radiation necrosis and tumour regrowth.regrowth.
Differentiation of neoplastic and non-neoplastic Differentiation of neoplastic and non-neoplastic cysts (and their drainage).cysts (and their drainage).
Diagnostic biopsy of a suspected infectious Diagnostic biopsy of a suspected infectious lesion that has not responded to a trial of lesion that has not responded to a trial of therapy.therapy.
Diagnosis of cerebral vasculitis or vasculopathy.Diagnosis of cerebral vasculitis or vasculopathy.

TREATMENTTREATMENT SurgerySurgery
CytoreductionCytoreduction Cytoreductive surgery for low - grade and Cytoreductive surgery for low - grade and
malignant gliomas improves survival. malignant gliomas improves survival. Survival benefits for the resection of single Survival benefits for the resection of single
and multiple brain metastases.and multiple brain metastases. Extent of resection (EOR) may be significant Extent of resection (EOR) may be significant
in determining survival for both low – grade in determining survival for both low – grade and high - grade gliomas.and high - grade gliomas.
TREATMENTTREATMENT SurgerySurgery
Surgical CureSurgical Cure Many extra - axial tumors and some intra - Many extra - axial tumors and some intra -
axial tumors afford the neurosurgeon the axial tumors afford the neurosurgeon the opportunity for gross total resection and opportunity for gross total resection and surgical cure. surgical cure.
Benign tumors such as meningiomas, Benign tumors such as meningiomas, pituitary adenomas, cranial nerve pituitary adenomas, cranial nerve schwannomas, chordomas, dermoids and schwannomas, chordomas, dermoids and epidermoids, choroid plexus papillomas, epidermoids, choroid plexus papillomas, pilocytic astrocytomas, and pilocytic astrocytomas, and hemangioblastomas may, in many cases, be hemangioblastomas may, in many cases, be cured with complete surgical resection.cured with complete surgical resection.
TREATMENTTREATMENT CNS InfectionCNS Infection
Antibiotic treatment must be initiated as soon as Antibiotic treatment must be initiated as soon as possible, and later guided by CSF examination possible, and later guided by CSF examination results. results.
Patients must receive at least 10 days of high-Patients must receive at least 10 days of high-dose IV antibiotics that easily cross the blood–dose IV antibiotics that easily cross the blood–brain barrier. brain barrier.
Empiric IV therapy with a third-generation Empiric IV therapy with a third-generation cephalosporin, such as ceftriaxone or cefotaxime, cephalosporin, such as ceftriaxone or cefotaxime, plus vancomycin must commence pending results plus vancomycin must commence pending results of the bacterial cultures. of the bacterial cultures.
High-dose corticosteroids, administered before High-dose corticosteroids, administered before antibiotic therapy, are recommended for all antibiotic therapy, are recommended for all children and should be seriously considered for children and should be seriously considered for adults with community-acquired meningitis. adults with community-acquired meningitis.
When culture and sensitivity data are available, a When culture and sensitivity data are available, a specific antimicrobial therapy can be determined.specific antimicrobial therapy can be determined.
TREATMENTTREATMENT Brain abscessesBrain abscesses
Empiric medical therapy is started with a Empiric medical therapy is started with a third- or fourth-generation cephalosporin or third- or fourth-generation cephalosporin or penicillin plus metronidazole, depending on penicillin plus metronidazole, depending on the setting. the setting.
Brain edema associated with acute brain Brain edema associated with acute brain abscess necessitates use of steroids and abscess necessitates use of steroids and mannitol, as well as phenytoin, to prevent mannitol, as well as phenytoin, to prevent convulsions.convulsions.
Patients must receive at least 4 to 6 weeks of Patients must receive at least 4 to 6 weeks of high-dose IV antibiotics that easily cross the high-dose IV antibiotics that easily cross the blood–brain barrier, followed by 2-4 weeks of blood–brain barrier, followed by 2-4 weeks of oral antibiotics. oral antibiotics.
TREATMENTTREATMENT Brain abscessesBrain abscesses
Therapeutically, the abscess may be directly Therapeutically, the abscess may be directly aspirated. aspirated.
Burrhole and drainage of abscess or Burrhole and drainage of abscess or craniotomy and excision of abscess may be craniotomy and excision of abscess may be indicated depending on the size of the indicated depending on the size of the abscesses and the depth from the cortical abscesses and the depth from the cortical surface.surface.
Surgery may not be necessary if follow-up CT Surgery may not be necessary if follow-up CT demonstrates decreased abscess size. demonstrates decreased abscess size.
TREATMENTTREATMENT Cerebral tuberculomaCerebral tuberculoma
PCR and CSF culture or culture of biopsied PCR and CSF culture or culture of biopsied lesional material confirms the diagnosis. lesional material confirms the diagnosis.
Because standard medical therapy is usually Because standard medical therapy is usually successful if multidrug resistance is not successful if multidrug resistance is not identified, antituberculous therapy must be identified, antituberculous therapy must be attempted before surgery is contemplated. attempted before surgery is contemplated.
Of course, if there are signs of impending Of course, if there are signs of impending herniation, immediate surgery is indicated.herniation, immediate surgery is indicated.

TREATMENTTREATMENT Intracranial HemorrhageIntracranial Hemorrhage
The initial management of ICH, after ensuring The initial management of ICH, after ensuring adequate ventilation and hemodynamic stability, adequate ventilation and hemodynamic stability, involves correcting coagulopathies, treating involves correcting coagulopathies, treating hypertension, and addressing the possibility of hypertension, and addressing the possibility of increased intracranial pressure. increased intracranial pressure.
In patients with intraventricular blood and early In patients with intraventricular blood and early hydrocephalus, placement of a temporary external hydrocephalus, placement of a temporary external drain should be considered. drain should be considered.
Beyond these basics principles, the best treatment Beyond these basics principles, the best treatment of ICH remains unclear and quite variable from of ICH remains unclear and quite variable from center to center and in different countries. center to center and in different countries.
Although some advocate invasive techniques for Although some advocate invasive techniques for hematoma evacuation, others rely mostly on hematoma evacuation, others rely mostly on medical treatment and supportive caremedical treatment and supportive care
TREATMENTTREATMENT Intracranial HemorrhageIntracranial Hemorrhage
However, when a nondominant hemispheric or However, when a nondominant hemispheric or cerebellar ICH threatens impending herniation cerebellar ICH threatens impending herniation and before the patient’s level of consciousness and before the patient’s level of consciousness significantly deteriorates, emergent surgery significantly deteriorates, emergent surgery may be lifesaving and may provide a may be lifesaving and may provide a reasonably good recovery, especially in reasonably good recovery, especially in younger patients.younger patients.
PROGNOSISPROGNOSIS Intracranial NeoplasmIntracranial Neoplasm
Gliomas are rarely completely excised, as Gliomas are rarely completely excised, as infiltration spreads beyond the radiologically infiltration spreads beyond the radiologically evident boundaries of the tumour.evident boundaries of the tumour.
Recurrence is therefore common, even if the Recurrence is therefore common, even if the tumour mass is apparently completely tumour mass is apparently completely removed.removed.
Prognosis for benign tumours is good, Prognosis for benign tumours is good, provided complete surgical excision can be provided complete surgical excision can be achieved. achieved.
PROGNOSISPROGNOSIS Intracranial InfectionIntracranial Infection
Of patients with bacterial meningitis, Of patients with bacterial meningitis, approximately 15% experience acute and approximately 15% experience acute and chronic complications, including various cranial chronic complications, including various cranial nerve dysfunction, particularly those affecting nerve dysfunction, particularly those affecting extraocular function (cranial nerves III, IV, and extraocular function (cranial nerves III, IV, and VI), CN-VII, and sometimes CN-VIII, although VI), CN-VII, and sometimes CN-VIII, although this is less common today with the antibiotics this is less common today with the antibiotics lacking specific ototoxicity or vestibular toxicity. lacking specific ototoxicity or vestibular toxicity.
Even with early diagnosis, mortality rates are Even with early diagnosis, mortality rates are still at least 10% for meningococcal and 30% for still at least 10% for meningococcal and 30% for pneumococcal meningitis.pneumococcal meningitis.
PROGNOSISPROGNOSIS Intracerebral hemorrhageIntracerebral hemorrhage
Surgery demonstrated slightly better outcome Surgery demonstrated slightly better outcome (26.1% vs. 23.8%), but survival rates appeared to (26.1% vs. 23.8%), but survival rates appeared to be similar in surgically and medically treated be similar in surgically and medically treated patients. patients.
The outcome from surgery likely depends on The outcome from surgery likely depends on several factors, including the fact that deep-several factors, including the fact that deep-seated basal ganglia or thalamic hemorrhages are seated basal ganglia or thalamic hemorrhages are difficult to evacuate without disrupting difficult to evacuate without disrupting surrounding normal structures and exacerbating surrounding normal structures and exacerbating brain damage, especially with open craniotomy. brain damage, especially with open craniotomy.
Patients who have small hematomas (smaller than Patients who have small hematomas (smaller than 30 cm3) seem to do generally well without 30 cm3) seem to do generally well without surgical evacuation. However, larger hematomas surgical evacuation. However, larger hematomas (larger than 60 cm3) do poorly, even when (larger than 60 cm3) do poorly, even when evacuated surgically. evacuated surgically.

THANK YOUTHANK YOU


















