
SOUTHAMPTON UNIVERSITY HOSPITALS NHS TRUST 3-Monthly ...
25
SOUTHAMPTON UNIVERSITY HOSPITALS NHS TRUST 3-Monthly Patient Safety Report: Report to: Trust Board 29 th September 2009 Report from: Julia Barton, Associate Director of Nursing Sponsoring Executive: Judy Gillow, Director of Nursing and Patient Services Aim of Report: 1) To brief members on performance against patient safety targets (PIF and Integrated Patient Safety Strategy) 2) To Highlight areas of progress and challenge, and identify the work streams in place to address these. Review History to Date: Previous patient safety reports included in quarterly governance reports. All Integrated Safety Strategy work streams are reported quarterly to Trust Safety Steering Group. This is the first detailed report on patient safety, which will be presented 3-monthly to the Trust Board as part of the PIF review. Assurance Framework: 1. To be the hospital of first choice for patients 2. In the UK top quartile for quality indicators. Principle Objectives: Recommendations: Trust Board Members are asked to • Review and agree the new format of the report • Critically review all the work streams • Identify any areas where further assurance is required 1.0 Summary of Performance over Reporting Period Areas of Outstanding Performance: • MRSA and C.DIfficile over achievement of performance trajectory • Return of Spontaneous Circulation after Cardiac Arrest (cf benchmarking Trusts) • Medication Safety Improvement Programme impact Areas Demonstrating Steady Improvement: • Actual Harm from Medication Safety levels decreasing • Falls – over 92& compliance with SIRFIT maintained and reducing actual harm from falls incidents. (See Appendix C for action plan.) • Thromboprohylaxsis compliance improved. • MEWS compliance improving (See Appendix D for action plan.) • Pressure Injury reporting increased and base lining of new data-sets underway (Action plan in Appendix B) • Correct Site Surgery Areas of Slower Progress: • MUST assessment compliance slowly improving (see Appendix E for action plan)
Transcript of SOUTHAMPTON UNIVERSITY HOSPITALS NHS TRUST 3-Monthly ...

SOUTHAMPTON UNIVERSITY HOSPITALS NHS TRUST
3-Monthly Patient Safety Report:
Report to: Trust Board 29th September 2009 Report from: Julia Barton, Associate Director of Nursing Sponsoring Executive: Judy Gillow, Director of Nursing and Patient Services Aim of Report: 1) To brief members on performance against patient safety targets (PIF
and Integrated Patient Safety Strategy) 2) To Highlight areas of progress and challenge, and identify the work
streams in place to address these. Review History to Date: Previous patient safety reports included in quarterly governance reports.
All Integrated Safety Strategy work streams are reported quarterly to Trust Safety Steering Group. This is the first detailed report on patient safety, which will be presented 3-monthly to the Trust Board as part of the PIF review.
Assurance Framework: 1. To be the hospital of first choice for patients 2. In the UK top quartile for quality indicators. Principle Objectives: Recommendations: Trust Board Members are asked to
• Review and agree the new format of the report
• Critically review all the work streams
• Identify any areas where further assurance is required
1.0 Summary of Performance over Reporting Period
Areas of Outstanding Performance:
• MRSA and C.DIfficile over achievement of performance trajectory
• Return of Spontaneous Circulation after Cardiac Arrest (cf benchmarking Trusts)
• Medication Safety Improvement Programme impact Areas Demonstrating Steady Improvement:
• Actual Harm from Medication Safety levels decreasing
• Falls – over 92& compliance with SIRFIT maintained and reducing actual harm from falls incidents. (See Appendix C for action plan.)
• Thromboprohylaxsis compliance improved.
• MEWS compliance improving (See Appendix D for action plan.)
• Pressure Injury reporting increased and base lining of new data-sets underway (Action plan in Appendix B)
• Correct Site Surgery Areas of Slower Progress:
• MUST assessment compliance slowly improving (see Appendix E for action plan)
2
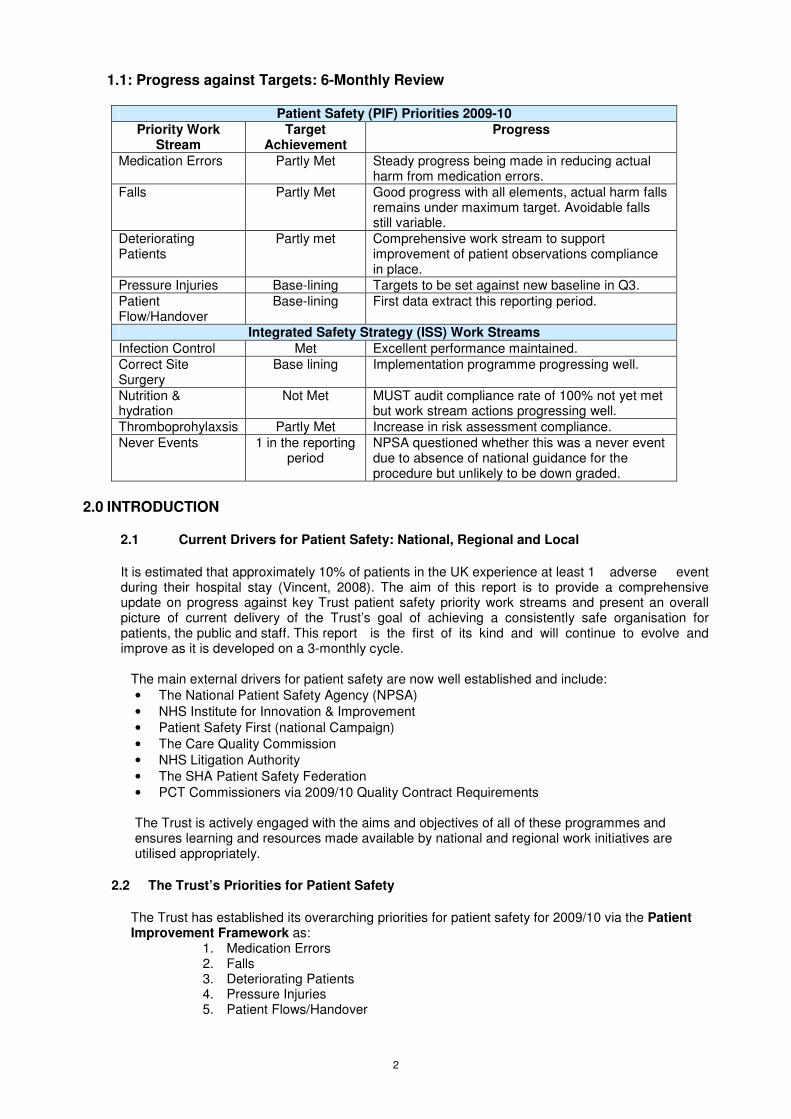
1.1: Progress against Targets: 6-Monthly Review
Patient Safety (PIF) Priorities 2009-10
Priority Work Stream
Target Achievement
Progress
Medication Errors Partly Met Steady progress being made in reducing actual harm from medication errors.
Falls Partly Met Good progress with all elements, actual harm falls remains under maximum target. Avoidable falls still variable.
Deteriorating Patients
Partly met Comprehensive work stream to support improvement of patient observations compliance in place.
Pressure Injuries Base-lining Targets to be set against new baseline in Q3.
Patient Flow/Handover
Base-lining First data extract this reporting period.
Integrated Safety Strategy (ISS) Work Streams
Infection Control Met Excellent performance maintained.
Correct Site Surgery
Base lining Implementation programme progressing well.
Nutrition & hydration
Not Met MUST audit compliance rate of 100% not yet met but work stream actions progressing well.
Thromboprohylaxsis Partly Met Increase in risk assessment compliance.
Never Events 1 in the reporting period
NPSA questioned whether this was a never event due to absence of national guidance for the procedure but unlikely to be down graded.
2.0 INTRODUCTION
2.1 Current Drivers for Patient Safety: National, Regional and Local
It is estimated that approximately 10% of patients in the UK experience at least 1 adverse event during their hospital stay (Vincent, 2008). The aim of this report is to provide a comprehensive update on progress against key Trust patient safety priority work streams and present an overall picture of current delivery of the Trust’s goal of achieving a consistently safe organisation for patients, the public and staff. This report is the first of its kind and will continue to evolve and improve as it is developed on a 3-monthly cycle.
The main external drivers for patient safety are now well established and include:
• The National Patient Safety Agency (NPSA)
• NHS Institute for Innovation & Improvement
• Patient Safety First (national Campaign)
• The Care Quality Commission
• NHS Litigation Authority
• The SHA Patient Safety Federation
• PCT Commissioners via 2009/10 Quality Contract Requirements The Trust is actively engaged with the aims and objectives of all of these programmes and ensures learning and resources made available by national and regional work initiatives are utilised appropriately.
2.2 The Trust’s Priorities for Patient Safety
The Trust has established its overarching priorities for patient safety for 2009/10 via the Patient Improvement Framework as:
1. Medication Errors 2. Falls 3. Deteriorating Patients 4. Pressure Injuries 5. Patient Flows/Handover

3
In addition a further 4 patient safety priorities are included in the Trust’s Integrated Safety Strategy:
• Infection Control
• Correct Site Surgery
• Nutrition and Hydration
• Thromboprophylaxsis
The SHA and Trust’s PCT commissioners also monitor never events and serious untoward incidents (SUIs).
2.3 The Integrated Patient Safety Strategy Themes
The Integrated Safety Strategy was approved in April 2009 and launched in June 2009. Delivery of this strategy and local awareness and ownership is a key theme of national patient safety week.
3.0 Patient Safety Delivery and Monitoring Mechanisms Patient Safety is delivered and monitored via a range of methods & groups, summarised as follows:
• Trust Safety Steering Group
• Risk and Safety Operational Group
• In-Patient Falls Group
• Tissue Viability Group
• Nutrition Steering Group (due for relaunch in autumn 2009).
• Acuity Group
• Infection Prevention and Control Committee
• Medication Safety Group
Quarterly Performance Overview
3.1 Patient Safety Initiatives Patient Safety First National Campaign
The Trust signed up to the Patient Safety First Campaign and its goal to ensure ‘no avoidable death or harm’ in January 2008. The specific focus of the campaign at SUHT is the reduction of harm from high-risk medicines but focus groups have also been established for the other 4 campaign interventions. SUHT’s Director of Nursing is the regional representative on the campaign’s steering committee. The campaign has gained momentum over the last 2 quarters and is actively promoting the following initiatives, which are all being utilised/implemented at SUHT:
• WebEx’s (Safety topic teleconferences)
• Plot the Dot (Opportunity to upload data on the measurement extranet)
• Networking, fora and online clinics
• Series of “How to..” Guides
• National Patient Safety Week (W/C 21/9/09) Never Events
The concept of a list of Never Events was introduced by the National Patient Safety Agency (NPSA) in April 2009. SUHT has adopted their definitions and criteria locally as have the PCTs in their Quality Contracts for 2009/2010. The Never Event list relevant to acute Trusts covers the following:
� Wrong site surgery � Retained instrument post-op � Wrong route administration of chemotherapy � Misplaced or not detected naso-gastric tube � In hospital maternal death from post partum haemorrhage after an elective
caesarean � IV administration of mis-selected Potassium Chloride
In June, 2009, The Trust declared a never event in which a patient’s spinal surgery was carried out at the wrong vertebrae level. The event has been subject to intensive investigation internally and with external partners (PCT & SHA). Whilst this incident is unlikely to have it’s classification changed, the case has been taken up by the NPSA who have questioned us calling this a “never event” and recognised the absence of national guidelines for this surgical procedure.

4
Never Events M1-5 2009/10
0
1
2
Apr-09 May-09 Jun-09 Jul-09 Aug-09
Never Events
Target of 0 per month
Significant Events and SUIs Serious Events/SUIs(cont’d)
Serious incidents (SUIs, Significant Events Clinical and Serious Events Non-Clinical).
SUI's and SEC M1-5 2009/10
0
1
2
3
4
5
6
7
8
Apr-09 May-09 Jun-09 Jul-09 Aug-09
SUIs reported by SUHT
Target of 6 per month
There were 17 serious incidents reported between April and August 2009. The Trust’s Significant Event Review Group (SERG) seeks to ensure that all significant events are actively investigated and improvement plans are delivered to ensure lesson’s learnt and subsequent risk reduced. The SERG group ensures investigations are carried out in a timely and comprehensive way and receives 80-100 case presentations per annum. So far in 2009, SERG has reviewed its terms of reference, devised a new case presentation proforma and report template. The group has increased clarity concerning suitable cases to be presented, and has seen growing engagements from senior clinicians and nurses. Robust monitoring of investigation and action planning deadlines is in operation with the use of divisional traffic light reporting.
SUI's reported by SUHT between April - August 2009
0
1
2
3
4
5
6
7
8
April May June July August
Month
Nu
mb
er
of
SU
I's b
y c
au
se
(blank)
Ventialtion issue
Unexpected Death of Comm.Pt
Other
Grade 4 pressure ulcer
Communication Issue
Communicable Disease & Infection Issue
C Diff & HCAI
Sum of Number of SUI's reported
Month
SUI Incident cause

5
Significant Event Management Dashboard information for
July 2009
0
1
2
3
4
5
6
7
8
9
SUI SEC INQ Reds T otal Open
SE 's
Due SE Act
P l ans
PCT
Inci dents
Division 1
Division 2
Division 3
Division 4
Division 5
Nature of Case to SERG Jan-June 2009
INQ
34%Unexp death
6%
Never Event
2%
SEN
17%
SEC
27%
Nil
4%SUI
10%
IN addition to divisional and care group learning, key themes from SERG are also shared across the organisation via the Trust’s Safety newsletter (Safety Matters) or via the Associate Medical Director for Clinical Outcomes & Safety’s briefing for senior clinical staff. Service improvement initiatives stemming from learning from significant event cases includes:
• An updated incident and Management Policy Nov-08.
• Updated bedrails policy to include reference to Mental Capacity Act and DOLS out to consultation Jul-09.
• Consent policy currently under review.
• Patient ID Policy currently under review.
The Medical Director and ADNS for Patient Experience and Safety have completed a comprehensive review of Trust wide Significant Event management and the SUI process and this is due to report in October 2009.
Global Trigger Tool
The Trust implemented the Global Trigger Tool methodology in January 2009. The tool is a retrospective method of reviewing case notes for safety triggers that may indicate an adverse event has occurred. If found the adverse event is scored for the degree of harm. 20 case notes for each clinical division are reviewed monthly (80 Trust wide per month). Data has now been entered onto the NHS Institute’s web portal database, which is still in pilot phase. This database will be able to provide reports and statistical data analysis shortly. The Trust backlog of completed GTT proformas has now been entered onto the system. GTT leads are attending divisional meetings and running a master-class during Patient Safety week. The first data report will be presented in November 2009.

6
Incidents and Reporting:
It is estimated that incident reporting via the National Reporting & Learning System (NRLS) only captures 6% of events. In the first NRLS reporting period in March 2009, SUHT reported 5.31 incidents per 100 admissions, compared with 4.98 for similar Trusts. Of the 27 Trusts in the acute hospital group, SUHT lies 12
th. The next set of
NRLS national benchmarking data is due to be published in early October. Initiatives to increase reporting include:
• Development of e-incident forms for web based reporting - progress made but significant amount of data cleansing and management of system has been required.
• Separation of actual harm from reporting metrics for key safety targets.
• Monthly “Safety Matters” newsletter detailing breakdown of key themes and trends form incident reporting.
• “Safety in Clinical Practice” newsletter monthly from AMD for Clincial Outcomes & Safety.
• Weekly safeguard incident reports sent to all divisions
• Divisional delivery of incident actions plans monitored via a traffic light system.
• Re-assessment safety culture being undertaken in each Care Group in Q3 using Manchester tool.
Number of PSI incidents of moderate, severe, catastrophic/death levels at
SUHT
0
20
40
60
80
100
120
140
160
Apr-09 May-09 Jun-09 Jul-09 Aug-09
Reported PSI incidents of
moderate, severe,
catastrophic/death levelsTarget of 120 or less
Number of reported Non PSI of levels moderate, severe, catastrophic/death
levels
0
5
10
15
20
25
30
35
40
45
Apr-09 May-09 Jun-09 Jul-09 Aug-09
Number of Non PSI
reported incidents of
moderate, severe,
catastrophic/death
levelsTarget of 41 or less

7
The longitudinal Trust incident reporting trend demonstrates a gradual increase in reporting activity. In order to standardise investigation processes for incidents, root cause analysis training has been provided to a variety of clinicians via the education rolling half day.
Leadership & Safety Walks
The Trust was awarded an organisational place on the NHS Institute’s Leading Improvement in Patient Safety (LIPS) course which commenced in Q1 of 2009/10. 3 members of staff with safety responsibilities and a junior doctor are implementing the learning from this programme, including rigorous measurement, strategic, organisational and local planning techniques, a wide variety of safety improvement tools and techniques including the use of PDSA cycles and measurement for sustained safety improvement. The Director of Nursing and Medical Director, Trust senior nurses and matrons now undertake regular safety walkabouts and this process will be further extended to include all executives and senior managers. Prompt cards will be developed.
8
4.0 Key Performance Data and Summary reports
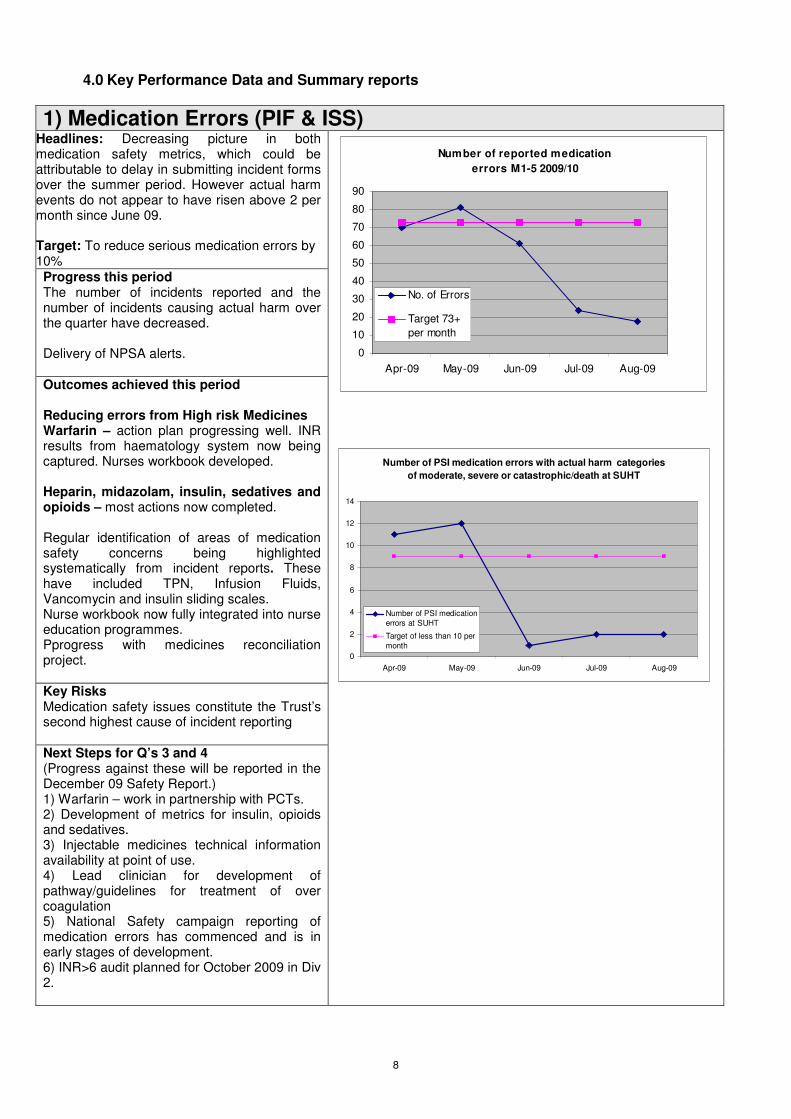
1) Medication Errors (PIF & ISS) Headlines: Decreasing picture in both medication safety metrics, which could be attributable to delay in submitting incident forms over the summer period. However actual harm events do not appear to have risen above 2 per month since June 09. Target: To reduce serious medication errors by 10% Progress this period The number of incidents reported and the number of incidents causing actual harm over the quarter have decreased. Delivery of NPSA alerts. Outcomes achieved this period Reducing errors from High risk Medicines Warfarin – action plan progressing well. INR results from haematology system now being captured. Nurses workbook developed. Heparin, midazolam, insulin, sedatives and opioids – most actions now completed. Regular identification of areas of medication safety concerns being highlighted systematically from incident reports. These have included TPN, Infusion Fluids, Vancomycin and insulin sliding scales. Nurse workbook now fully integrated into nurse education programmes. Pprogress with medicines reconciliation project.
Key Risks Medication safety issues constitute the Trust’s second highest cause of incident reporting Next Steps for Q’s 3 and 4 (Progress against these will be reported in the December 09 Safety Report.) 1) Warfarin – work in partnership with PCTs. 2) Development of metrics for insulin, opioids and sedatives. 3) Injectable medicines technical information availability at point of use. 4) Lead clinician for development of pathway/guidelines for treatment of over coagulation 5) National Safety campaign reporting of medication errors has commenced and is in early stages of development. 6) INR>6 audit planned for October 2009 in Div 2.
0
10
20
30
40
50
60
70
80
90
Apr-09 May-09 Jun-09 Jul-09 Aug-09
No. of Errors
Target 73+
per month
Number of reported medication
errors M1-5 2009/10
Number of PSI medication errors with actual harm categories
of moderate, severe or catastrophic/death at SUHT
0
2
4
6
8
10
12
14
Apr-09 May-09 Jun-09 Jul-09 Aug-09
Number of PSI medication
errors at SUHT
Target of less than 10 per
month

9
2) Falls (PIF & ISS) Headlines: In-patient falls continues to be the highest Trust wide patient safety incident. SIRFIT compliance has run at over 92% for the last 4 months. Avoidable falls are running at between 10 and 25% per month and therefore under the target of 5%. Target: To reduce avoidable falls by 20% • To maintain SIRFIT Compliance above
95%
• 175 falls incident reports per month.
• <17 Falls causing actual harm
• SIRFIT of >95%
• Avoidable Falls <5%
Progress this period: The number of falls reported has stayed on or just below the target of 175 per month. Actual harm from falls has remained under target of 17 at between 5 and 15. SIRFIT compliance remains on or just below the revised SIRFIT compliance target of 95%. Avoidable falls remains off target at between 10 & 25%. Outcomes achieved this period The Trust multidisciplinary falls group is delivering an extensive falls improvement plan. Work achieved to date includes:
• New falls metrics established.
• Falls policy updated and revised.
• Development of SIRFIT tool and algorithm for managing in-patient falls in place.
• New guidance on action after a fall and on reporting and critical incidents analysis available.
• Consistent screening of older people attending the Emergency Department by the OPOST team.
• Falls e-learning education programme in place.
• Good engagement from Care Group Falls Champions
Key Risks Direct impact on patient morbidity and mortality. Cost of extended length of stay for patients who fall. Need for a designated falls nurse specialist and fracture liaison post has been identified in the national falls audit of December 2008. Next Steps for Q’s 3 and 4 Please see detailed In Patient Falls Improvement Plan found in Appendix C
Number of Falls reported at SUHT
0
20
40
60
80
100
120
140
160
180
200
Apr-08 May-08 Jun-08 Jul-08 Aug-08
Number of Falls reported at SUHT
Target of 175 or more
Number of Falls by actual harm of moderate, severe,
catastrophic/death levels
0
2
4
6
8
10
12
14
16
18
Apr-09 May-09 Jun-09 Jul-09 Aug-09
Number of Falls by actual
harm levels of moderate,
severe and
catastrophic/death levelsTarget of 17 or less
Number of SIRFITS completed at SUHT
82.00%
84.00%
86.00%
88.00%
90.00%
92.00%
94.00%
96.00%
98.00%
100.00%
Apr-09 May-09 Jun-09 Jul-09 Aug-09
Number of SIRFITs completed
at SUHT
Target of 90% or more per
month
Avoidable Falls at SUHT
0.00%
5.00%
10.00%
15.00%
20.00%
25.00%
30.00%
Apr-09 May-09 Jun-09 Jul-09 Aug-09
Avoidable Falls
Target of 5% or less
10
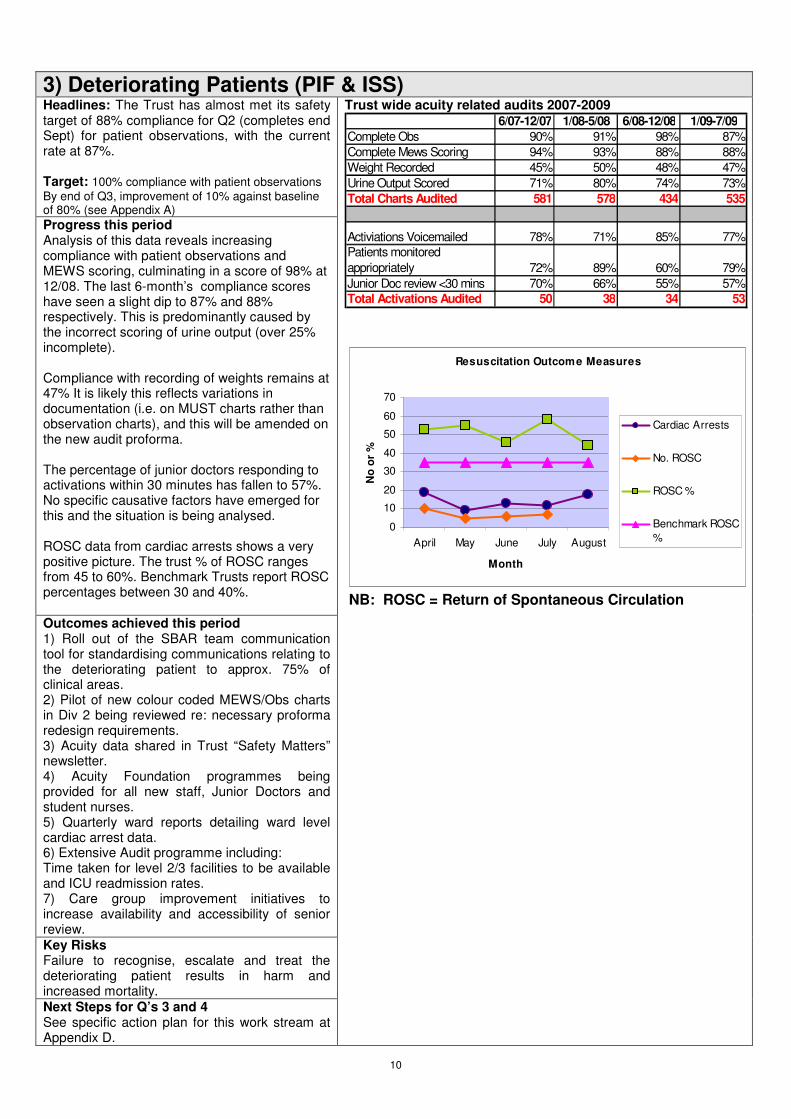
3) Deteriorating Patients (PIF & ISS) Headlines: The Trust has almost met its safety target of 88% compliance for Q2 (completes end Sept) for patient observations, with the current rate at 87%. Target: 100% compliance with patient observations
By end of Q3, improvement of 10% against baseline of 80% (see Appendix A) Progress this period Analysis of this data reveals increasing compliance with patient observations and MEWS scoring, culminating in a score of 98% at 12/08. The last 6-month’s compliance scores have seen a slight dip to 87% and 88% respectively. This is predominantly caused by the incorrect scoring of urine output (over 25% incomplete). Compliance with recording of weights remains at 47% It is likely this reflects variations in documentation (i.e. on MUST charts rather than observation charts), and this will be amended on the new audit proforma. The percentage of junior doctors responding to activations within 30 minutes has fallen to 57%. No specific causative factors have emerged for this and the situation is being analysed. ROSC data from cardiac arrests shows a very positive picture. The trust % of ROSC ranges from 45 to 60%. Benchmark Trusts report ROSC percentages between 30 and 40%. Outcomes achieved this period 1) Roll out of the SBAR team communication tool for standardising communications relating to the deteriorating patient to approx. 75% of clinical areas. 2) Pilot of new colour coded MEWS/Obs charts in Div 2 being reviewed re: necessary proforma redesign requirements. 3) Acuity data shared in Trust “Safety Matters” newsletter. 4) Acuity Foundation programmes being provided for all new staff, Junior Doctors and student nurses. 5) Quarterly ward reports detailing ward level cardiac arrest data. 6) Extensive Audit programme including: Time taken for level 2/3 facilities to be available and ICU readmission rates. 7) Care group improvement initiatives to increase availability and accessibility of senior review. Key Risks Failure to recognise, escalate and treat the deteriorating patient results in harm and increased mortality. Next Steps for Q’s 3 and 4 See specific action plan for this work stream at Appendix D.
Trust wide acuity related audits 2007-2009 6/07-12/07 1/08-5/08 6/08-12/08 1/09-7/09
Complete Obs 90% 91% 98% 87%
Complete Mews Scoring 94% 93% 88% 88%
Weight Recorded 45% 50% 48% 47%
Urine Output Scored 71% 80% 74% 73%
Total Charts Audited 581 578 434 535
Activiations Voicemailed 78% 71% 85% 77%
Patients monitored
appriopriately 72% 89% 60% 79%
Junior Doc review <30 mins 70% 66% 55% 57%
Total Activations Audited 50 38 34 53
Resuscitation Outcome Measures
0
10
20
30
40
50
60
70
April May June July August
Month
No
or
%
Cardiac Arrests
No. ROSC
ROSC %
Benchmark ROSC
%
NB: ROSC = Return of Spontaneous Circulation

11
4) Pressure Injuries (PIF & ISS) Headlines: This quarter has seen a significant focus on the prevention, management and reporting of pressure ulcers. New metrics have been agreed and an extensive action plan (see appendix E) developed to minimise harm from preventable hospital acquired pressure ulcers. There have been 2 grade 4 hospital acquired pressure ulcers in the reporting period but none during August. Both cases have been subject to rigorous internal investigation and root causes were linked to co-morbidities and care pathways external to the Trust. Partners have been involved with this process. The second grade 4 should have arguably been downgraded due to assessment in the presence of eschar. Target: To set the baseline and an
improvement metric for reduction of Grade 3 & 4 Pressure Ulcers in Q3 of 2009/10. Data Completeness:
Green = 100% Amber = 90 – 99% Red = < 90%
Progress this period: There have been significant changes in the reporting metrics for pressure ulcers this period, but the emerging picture would appear to indicate that grade 1-pressure ulcers are increasing whilst grades 2, 3 and 4 are decreasing. Data submission completeness has increased between April and July from 75% to over 90%, with a slight dip in August predominantly attributable to Divisions 2 and 3. Monitoring of divisional and care group performance data continues via monthly divisional performance meetings. Outcomes achieved this period: 1) New process for reporting grade 4 Hospital Acquired pressure Ulcers as SUIS in place. 2) Development of a new assurance framework including CEO and Director of Nursing review of all HA grade 4 SUIs, DHNs to review all grade 3’s and Matrons to review all grade 2’s. 3) New set of metrics agreed internally and with partners and now collating data in accordance with this.
Pressure Ulcer Incidence for August 2009
No. of New Ulcers
No. of New Patients %
Hospital Acquired 41 38 0.87%
Non Hospital Acquired
_
34 0.72%
Zero Grade 4’s
Trust: Hosptial Acquired Incidence Pressure Ulcer Location
August 09
2
6
01
0 0 0 0
8
0
7
0 0 0
2
0 0 0 01
0 00
2
4
6
8
10
12
14
16
18
Ankle
Butto
ck
Elbow H
eel
Hip
Mal
leol
i Lat
eral
Mal
leol
i Med
ial
Occ
iput
Sacru
mSpi
ne
Oth
er
Location
Nu
mb
er
of
Pre
ssu
re U
lcers
Grade
1
Grade
2
Grade
3
Grade
4
Zero Grade 4’s
Trust: Non Hosptial Acquired Incidence Pressure Ulcer Location
August 09
0
2
0
3
10 0 0
16
0 00 0 0 0 0 0 0 0
4
0 00
2
4
6
8
10
12
14
16
18
Ankle
Butto
ck
Elbow H
eel
Hip
Mal
leol
i Lat
eral
Mal
leol
i Med
ial
Occ
iput
Sacru
m
Spine
Oth
er
Location
Nu
mb
er
of
Pre
ssu
re U
lcers Grade
1
Grade
2
Grade
3
Grade
4
One grade
4 in August

12
Key Risks The cost of each Grade 3 or 4 pressure ulcer episode is estimated at: £6,000 to £24,000. However, this does not portray the cost to the individual and their loved ones in terms of human suffering and disablement. *Bennett G et al (2004). The cost of pressure ulcers in the UK. Age and Ageing; 33: 230-235
Next Steps for Q’s 3 and 4 See comprehensive action plan and progress update for Sept 2009 in Appendix B.
Pressure Ulcer Prevalence July - August 09
0
0.5
1
1.5
2
2.5
3
3.5
4
Jul-09 Aug-09
Number of actual ulcers
by 1000 bed days (HA)
Number of actual ulcers
by 1000 bed days
(NHA)
Number of Hospital Acquired Grade 4 Pressure Ulcers
M1-5 2009/10
0
1
2
3
4
5
Apr-09 May-09 Jun-09 Jul-09 Aug-09
Number of Grade 4 pressure
ulcersTarget of 0
Completeness of Pressure Ulcer data received by the Tissue
Viability team between April - August 09
0
0.1
0.2
0.3
0.4
0.5
0.6
0.7
0.8
0.9
1
Trust Division 1 Division 2 Division 3 Division 4
Apr-09
May-09
Jun-09
Jul-09
Aug-09

13
5) Patient Flows/Handovers (PIF) Headlines: This safety priority was identified via a “bottom-up” approach by divisional teams. This is the first extract and analysis of incidents relating to patient flows. Targets: Targets to be established for this work stream
Progress this period A total of 129 incidents were reported between April and August 2009 relating to patient flows and transfers. The top 3 reasons for incidents were delay or failure in treatment, failure in referral process and delay of failure in transfer. Outcomes achieved this period
• Establishment of an interagency discharge bureau
• Revised bed management policy approved
• Review of transport arrangements
• Service improvement programme to achieve 11am discharge.
• HMR completion drive now owned by Care Group leads and integrated into junior doctor’s induction.
• TTO turnaround times project.
• Hospital at Night handover plans in place.
Key Risks Patient safety incidents from multiple handoffs, failure to deliver capacity plan and Same Sex Accommodation goals. Next Steps for Q’s 3 and 4 Further analysis of the reporting codes is required to prevent inaccurate coding. TTO Turnaround times project target of 1 hour by the end of December.
Cause 1 2009 4 2009 52009 6 2009 7 2009 8 Grand Total
A1500 Failure In Referral Process 4 3 7 15 3 32
A1700 Transfer - Delay / Failure 7 4 2 4 1 18
A1800 Transport - Delay / Failure 2 2 1 5
G0700 Extended Stay / Episode Of Care 3 3
H0400 Lack Of / Delayed Availability Of Beds 4 6 1 2 13
H0500 Lack Of / Delayed Availability Of Beds 3 3 2 8
N0600 Extended Stay / Episode Of Care 1 1
N1600 Transfer - Delay / Failure 3 1 4
N1700 Treatment/procedure - Delay/failure 7 16 12 9 1 45
Grand Total 27 35 28 33 6 129
0
5
10
15
20
25
30
35
40
45
50
A1500 F
ailure
In
Re
ferr
al P
rocess
A1700 T
ransfe
r -
Dela
y / F
ailure
A180
0 T
ransport
-
Dela
y / F
ailure
G0
700 E
xte
nded
Sta
y / E
pis
ode O
f
Care
H0400
Lack O
f /
Dela
yed A
vailability
Of B
eds
H0500
Lack O
f /
Dela
yed A
vailability
Of B
eds
N0600 E
xte
nded
Sta
y / E
pis
ode O
f
Care
N1600 T
ransfe
r -
Dela
y / F
ailu
re
N1
700
Tre
atm
ent/p
rocedure
- D
ela
y/failure
2009 8
2009 7
2009 6
2009 5
2009 4
Include? y
Count of Incident Number
Cause 1
Month
6) Correct Site Surgery (ISS) Headlines: Target: 100% compliance with WHO Safer Surgery Checklist by Feb. 2010.
Progress this period No Metrics to report until auditing commences. Outcomes this period In the last quarter, the pilot phase of SUHT's Safer Surgery Checklist has continued in identified areas with testing and modification to meet our needs. A survey of the pilot has elicited positive responses from all members of the theatre teams using the checklist. A final version of the checklist has been produced in preparation for roll out in November 2009. Teaching and awareness sessions at Education half-days have taken place as well as three half-hour Q&A sessions during Patient Safety First week. Key Risks A number of challenges remain in implementing the Safer Surgery Checklist in terms of addressing a reluctance amongst a number of staff to take part in the team brief as well as allaying concerns that the checklist will slow down theatre lists. Next Steps Roll out phase from 1st November 2009.
Example comments from staff now using the new checklist:
'positive benefit for new and unfamiliar members of the team and for regular use to check warming, antibiotics and foot pumps' - Surgeon
'positive - better all round awareness' – ODP
'useful when someone else is covering for me' - Anaesthetist

14
7) Thromboprohylaxsis (ISS) Headlines:
Target: Suggested targets for 2009-10
Q1 Q2 Q3 Q4 Risk Assessment
50% 75% 85% 95%
Appropriate Treatment
80% 85% 90% 95% Progress this period Outcomes achieved this period Continued work to ensure guidelines are updates, clear and understood by health care staff. A cross divisional audit has been undertaken. The CMO team visit on 1
st July. Initial feedback
is that trust has excellent systems in place and a clear commitment at all levels to achieving excellence in VTE prevention. Key Risks Warfarin management improvements await inputs of the strengthened team. Next Steps for Q’s 3 and 4
Care Group Sample Appropriate Treatment %
Record of risk assessment in
notes %
Surgery 50 72 54
Orthopaedics 30 97 33
O&G 18 67 50
Oncology 10 50 10
Medicine & Elderly Care
41 88 46
Cardiac Surgery 13 100 8
Critical Care 16 88 63
Average/Summary 178 81% (80% in 2008)
43% (24% in 2008)
8) Nutrition & Hydration (ISS) Headlines: Target: To achieve a 20% improve with MUST
compliance
Progress this period Compliance with MUST assessment has been audited in September 2009. Overall Trust compliance with MUST is 36%. 22% had evidence of a MUST care plan. MUST compliance via the BAPN audit undertaken in 2008 was 15%, so this recent audit reflects an improving picture, whilst recognising the significant work still needed on this agenda. Outcomes this period
• Liaison with Medirest to ensure new catering contract fit for purpose and KPIs, which have been developed, can now be tested.
• “Prompt card” developed for guidance on peri operative fluid management. Now being audited – initial results suggest beneficial shift in fluid management.
Key Risks All staff engagement and compliance with MUST and implementing nutritional plans on the basis of MUST assessments. Next Steps for Q’s 3 and 4 See detailed action plan in Appendix E)
Date of Audit: September 2009 n=222 patient records in sample
Number
patients
MUST fully
complete
No MUST or partially
completed
MUST care plan
n % n % n %
Division 1
Total
38
10
26%
28
74%
5
13%
E5 17 2 15 0 0
E7 21 8 13 5
Division 2
Total
135
61
45%
74
55%
29
22%
Medicine &
MOP total
80
27
53
28
AMU 32 6 26 0
G5 24 6 18 10
D8 24 15 9 18
Cancer
Care (C4,
D3)
40
22
18
1
C6L Haem 15 12 3 0
Division 3
Total
49
14
29%
35
71%
14
29%
F8 28 3 25 8
E2 21 11 10 6
TRUST
TOTAL
222 85 38% 137 62% 48 22%

15
9) Infection Prevention & Control (ISS) Headlines: Trust remains within both trajectories for performance. All divisions are rated green. Excellent and sustained delivery of all infection control targets in first 2 quarters of 2009/10. Target: MRSA target to end of July 9 cases C.Diff. target to end July 107 Cases. Progress this period: MRSA: 2 bacteraemia cases between April and August 09. C. DIfficile: Actual = 63 to July 2009 MRSA Screening at 97% Outcomes achieved this period: High compliance with care bundle audits. Immediate isolation for C.Difficile 100% with high compliance with other aspects of the care bundle. Key Risks Capacity and the ability to achieve early isolation – mitigation by close working between site and IPC teams to manage patient flows effectively. Next Steps for Q’s 3 and 4 Delivery of IFPC Plans Appointment of new Deputy Director of IPC
SUHT MRSA BSI
2007 - 2010
3
0
2
3
5
4
3
5 5
2
1
3 3 3
4
2 2
4
2
1 1 1 1
0
1
3
1
0
0123456789
101112131415
Apr-
07
May-0
7
Jun-0
7
Jul-07
Aug-0
7
Sep-0
7
Oct-07
Nov-0
7
Dec-0
7
Jan-0
8
Feb-0
8
Mar-
08
Apr-
08
May-0
8
Jun-0
8
Jul-08
Aug-0
8
Sep-0
8
Oct-08
Nov-0
8
Dec-0
8
Jan-0
9
Feb-0
9
Mar-
09
Apr-
09
May-0
9
Jun-0
9
Jul-09
No o
f C
ases
Actual Cases Trajectory Linear Trend (Actual Cases) SUHT Number of C. difficile Cases (>2 Yrs)
Including SHA Trajectory
1111
18
23
38
2522
1922
15
282525
27
2320
29
9
3437
31
38
56
46
57
6461
63
0
10
20
30
40
50
60
70
Apr-
07
May-0
7
Jun-0
7
Jul-07
Aug-0
7
Sep-0
7
Oct-07
Nov-0
7
Dec-0
7
Jan-0
8
Feb-0
8
Mar-
08
Apr-
08
May-0
8
Jun-0
8
Jul-08
Aug-0
8
Sep-0
8
Oct-08
Nov-0
8
Dec-0
8
Jan-0
9
Feb-0
9
Mar-
09
Apr-
09
May-0
9
Jun-0
9
Jul-09
No. of C
ases
SUHT SHA Trajectory
8.0 Summary & Conclusion This paper demonstrates:
• Significant activity is taking place in the Trust against the safety priorities
• Areas where improvement is required have detailed action plans and are being monitored closely
• The Trust, through the divisions and care groups is actively engaged in the safety agenda as part of the overall continuous improvement agenda.
Julia Barton ADNS, 21st September 2009

16
S
afe
ty T
arg
et
Metr
ic
Ba
se
lin
e
Q1
Q2
Q3
Q4
Med
icati
on
E
rro
rs
To
re
du
ce
se
rio
us m
ed
ica
tio
n
err
ors
by 1
0%
B
ase
lin
e t
o b
e
esta
blis
hed
. A
ctu
al h
arm
fr
om
me
dic
atio
n e
rro
rs f
or
be
twe
en
4 a
nd
16
in
cid
en
ts p
er
mo
nth
in
Q1
-3
of
20
08
/9.
Se
t b
ase
line
S
et
realis
tic
imp
rovem
en
t tr
aje
cto
ry
De
live
r ta
ng
ible
im
pro
vem
en
t a
gain
st
ba
selin
e
De
live
r ta
ng
ible
im
pro
vem
en
t a
gain
st
ba
selin
e
Th
rom
bo
pro
ph
yla
xs
is
10
0%
Com
plia
nce
with
NIC
E
gu
idan
ce
in
acu
te a
dm
issio
ns
un
its
To
be
esta
blis
he
d
Se
t b
ase
line
S
et
realis
tic
imp
rovem
en
t tr
aje
cto
ry
De
live
r ta
ng
ible
im
pro
vem
en
t a
gain
st
ba
selin
e
De
live
r ta
ng
ible
im
pro
vem
en
t a
gain
st
ba
selin
e
Acu
ity
10
0%
com
plia
nce
with
patien
t o
bse
rva
tio
ns
80
%
(ME
WS
Au
dit)
1
0%
Im
pro
ve
me
nt
ag
ain
st b
ase
line
a
ch
ieve
d
1
0%
Im
pro
ve
me
nt
ag
ain
st b
ase
line
a
ch
ieve
d
Infe
cti
on
M
on
thly
co
mp
liance
with
MR
SA
a
nd
C.
Difficile
Im
pro
ve
men
t T
raje
cto
rie
s
As p
er
ag
ree
d t
raje
cto
ry
On
Ta
rge
t O
n T
arg
et
On
Ta
rge
t O
n T
arg
et
Falls
•
To
re
du
ce
avo
idab
le
falls
by 2
0%
•
To
ma
inta
in S
IRF
IT
Co
mp
liance
ab
ove
95%
* A
vo
ida
ble
fa
lls a
ve
rag
e
20
% p
er
mo
nth
Q1
-3 o
f 2
00
8/9
*
SIR
FIT
80
to
95
%
co
mp
lian
ce
pe
r m
on
th in
2
00
8/9
* 5
% I
mp
rove
me
nt
ag
ain
st b
ase
line
a
ch
ieve
d
*
SIR
FIT
95
%
10
% I
mp
rove
me
nt
ag
ain
st b
ase
line
a
ch
ieve
d
*
SIR
FIT
95
%
15
% I
mp
rove
me
nt
ag
ain
st b
ase
line
a
ch
ieve
d
*
SIR
FIT
95
%
20
% I
mp
rove
me
nt
ag
ain
st b
ase
line
a
ch
ieve
d
*
SIR
FIT
95
%
Pre
ssu
re
Inju
ries
To
se
t th
e b
ase
line
an
d a
n
imp
rovem
en
t m
etr
ic f
or
red
uctio
n
of
Gra
de
3 &
4 P
ressu
re U
lce
rs
in 2
01
0/1
1
To
be
esta
blis
he
d
(TV
Da
ta R
etu
rns)
Se
t B
ase
line
S
et
imp
rove
me
nt
targ
et
Aim
to d
eliv
er
imp
rovem
en
t fo
r Q
4
or
Q1
of
20
10
/11
Hyd
rati
on
&
Nu
trit
ion
To
ach
ieve
a 2
0%
im
pro
ve
with
M
US
T c
om
plia
nce
T
o b
e e
sta
blis
he
d
(MU
ST
Au
dit)
1
0%
Im
pro
ve
me
nt
ag
ain
st b
ase
line
A
ch
ieve
d
2
0%
Im
pro
ve
me
nt
ag
ain
st b
ase
line
A
ch
ieve
d
Co
rre
ct
Sit
e
Su
rge
ry
10
0%
Com
plia
nce
with
WH
O
Sa
fer
Su
rge
ry C
he
cklis
t T
o b
e e
sta
blis
he
d
(Bre
ach R
ep
ort
s)
85
% C
om
pli
an
ce
9
0%
Co
mp
lia
nc
e
95
% C
om
pli
an
ce
1
00
% C
om
pli
an
ce
Fir
e
To
ach
ieve
a 2
0%
im
pro
ve
men
t in
sta
ff a
tte
nd
ance
in
Fire
Sa
fety
T
rain
ing
& c
om
ple
te fir
e a
ud
its
To
be
esta
blis
he
d
(80
%+
in
20
07
) 5
% I
mp
rove
me
nt
ag
ain
st b
ase
line
a
ch
ieve
d
10
% i
mp
rove
me
nt
ag
ain
st b
ase
line
a
ch
ieve
d
15
% i
mp
rove
me
nt
ag
ain
st b
ase
line
ach
ieve
d
20
% i
mp
rove
me
nt
ag
ain
st b
ase
line
a
ch
ieve
d
Healt
h &
S
afe
ty
•
10
% r
ed
uctio
n in
no
n-
pa
tien
t in
cid
en
ts a
nd
a
ccid
ents
(d
irect
ha
rm)
To
be
esta
blis
he
d.
Ave
rag
e o
f 6
0+
pe
r m
on
th
in Q
1-3
of
200
8/9
5
% I
mp
rove
me
nt
ag
ain
st b
ase
line
a
ch
ieve
d
1
0%
Im
pro
ve
me
nt
ag
ain
st b
ase
line
a
ch
ieve
d
Occu
pati
on
al
Healt
h &
S
ecu
rity
To
re
du
ce
Ne
ed
lestick in
jurie
s b
y
10
%
To
be
esta
blis
he
d
(30
0+
in
20
07
-8)
Se
t b
ase
line
S
et
realis
tic
imp
rovem
en
t tr
aje
cto
ry
De
live
r ta
ng
ible
im
pro
vem
en
t a
gain
st
ba
selin
e
De
live
r ta
ng
ible
im
pro
vem
en
t a
gain
st
ba
selin
e
Appen
dix
A:
2009/1
0 Inte
gra
ted S
afe
ty S
trate
gy T
arg
ets

17
Imp
rovem
en
t P
lan
fo
r th
e R
ed
ucti
on
of
Pre
ssu
re U
lcers
No
A
ims
/Go
als
A
cti
on
s
Le
ad
D
ate
Du
e
Se
pt
200
9 P
rog
ress
U
pd
ate
Wh
ole
Syste
ms L
evel
1
To e
nsure
corr
ect
org
anis
ational
assig
nation a
nd
investig
ations o
f gra
de 3
and 4
ulc
ers
are
undert
aken.
Work
with p
art
ners
to c
larify
responsib
ilities
and p
rocess for
report
ing a
nd investig
ation o
f gra
de 3
and 4
pre
ssure
ulc
ers
D
evelo
p a
join
t appro
ach w
ith local pro
vid
ers
Judy G
illo
w
Lynn T
aylo
r
Septe
mber
2009
•
Now
ag
reed to d
o
RC
A o
n a
ll gra
de 3
&4
pre
ssure
ulc
ers
.
•
SU
I fo
r gra
de 4
ulc
ers
•
Colla
bora
tive a
udit
tool still
to b
e a
gre
ed
2
To c
larify
the d
escription
of
the p
ressure
ulc
er
prior
to a
dm
issio
n
To a
gre
e p
rocess w
ith c
om
munity n
urs
ing
team
Lynn T
aylo
r S
epte
mber
2009
Conta
cting
Elle
n
McN
icola
s t
o d
iscuss
imple
menting
a p
rocess
3
To s
afe
guard
the p
atient
or
oth
er
patients
within
an institu
tion a
s
appro
priate
Lin
k g
rades 3
/4 p
ressure
ulc
ers
into
safe
guard
ing
ale
rt
Use G
uid
ance fro
m B
radfo
rd P
roto
col fo
r D
ete
rmin
ing
pote
ntial poor
care
Matr
ons
Ward
Sis
ters
In
Pla
ce
Safe
guard
ing
ale
rts a
re
bein
g r
ais
ed for
patients
w
ith g
rade 3
&4 P
Us if
neg
lect is
suspecte
d
4
To e
nsure
that
patients
are
pro
vid
ed w
ith
appro
priate
eq
uip
ment
Ag
ree m
anag
em
ent
and u
se o
f eq
uip
ment fo
r safe
care
and tra
nsitio
n b
etw
een c
are
pro
vid
ers
for
bariatr
ic p
atients
and e
nsure
com
munic
ation p
rior
to
dis
charg
e
Ward
D
ischarg
e
Team
Revie
w
end
Septe
mber
2009
Bariatr
ic e
quip
ment
agre
ed (
10/0
9/0
9)
prior
to
transfe
r of
a p
atient to
a
com
munity h
ospital
SU
HT
Acti
on
s
5
To a
gre
e s
tandard
isation
of
data
report
ing
A
gre
e m
inim
um
data
set, m
etr
ics a
nd a
udit tools
lin
ked to o
utc
om
e o
f re
gio
nal and n
ational g
uid
ance
Judy G
illo
w
Com
mis
sio
ners
Julia
Bart
on
Lynn T
aylo
r
Revie
w
Octo
ber
2009
•
Inte
rnal m
etr
ics
agre
ed
•
No n
ational data
set
agre
ed a
s y
et.
•
Port
sm
outh
has
agre
ed to s
hare
and
com
pare
data
.
6
To im
pro
ve a
ccura
cy o
f data
and e
nable
the
pro
duction o
f tim
ely
re
port
s
Develo
p r
eport
ing p
rocess a
nd r
eq
uirem
ents
of
data
base a
nd a
gre
e fre
quency o
f re
port
ing –
Inte
rnal
and e
xte
rnal
Lynn T
aylo
r
Revie
w
Octo
ber
2009
•
Month
ly K
PI
report
s t
o
Board
on G
rade 4
ulc
ers
in p
lace.
•
Tru
st pro
vid
ing
report
fo
r Q
ualit
y C
ontr
act.
•
Month
ly d
ata
pro
vid
ed
Ap
pen
dix
B:
Pre
ssu
re U
lcer
Ac
tio
n P
lan

18
for
Div
isio
n
Perf
orm
ance
Revie
ws.
•
Quart
erly S
afe
ty
Report
in p
lace.
•
Data
base for
month
ly
data
colle
ction
redesig
ned.
7
To identify
those p
atients
at risk a
nd m
onitor
qualit
y s
tandard
s o
f care
to
patients
Com
ple
te R
isk a
ssessm
ent
and c
are
pla
nnin
g a
gain
st
Nic
e G
uid
elin
e #
29
Care
Gro
up
Matr
ons
Lynn T
aylo
r
Revie
w
Octo
ber
2009
Pro
gre
ss b
ein
g m
ade
with D
ivis
ions
undert
akin
g s
elf
assessm
ent. O
n tra
ck for
com
ple
tion b
y e
nd o
f O
cto
ber.
8
To e
nsure
all
sta
ff a
re
aw
are
of
the T
rust’s R
CA
pro
cess f
or
gra
de 3
/4
pre
ssure
ulc
ers
Matr
ons t
o w
ork
with A
NT
s a
nd W
ard
Manag
ers
to
ensure
a c
onsis
tent and d
eta
iled “
deep d
ive”
revie
w
Matr
ons
Ris
k a
nd
Safe
ty T
eam
F
ran S
pra
tt
Revie
w
Septe
mber
2009
•
Achie
ved -
new
RC
A
pro
cess r
olle
d o
ut
acro
ss t
he T
rust.
•
Has b
een
successfu
lly u
sed b
y
Div
2 M
edic
ine a
nd
Eld
erly C
are
.
•
No R
CA
s r
eq
uired in
oth
er
Div
isio
ns
9
To im
pro
ve s
tandard
s in
the p
revention o
f pre
ssure
ulc
ers
and
incre
ase k
now
ledg
e
base
Share
learn
ing
fro
m g
rade 4
RC
As &
case s
tudie
s
acro
ss t
he tru
st to
assis
t in
drivin
g u
p im
pro
vem
ent
Julia
Bart
on
Lynn T
aylo
r R
evie
w
Septe
mber
2009
Good r
esponse fro
m D
iv
2. T
eachin
g s
essio
ns
arr
ang
ed
10
To s
hare
info
rmation a
nd
agre
e a
ctions p
lans t
o
reduce the n
um
ber
of
pre
ssure
ulc
ers
Month
ly R
CA
revie
w m
eeting
s w
ith D
irecto
r of
Nurs
ing
and T
V S
pecia
lists
with r
ele
vant
clin
ical te
am
to
revie
w a
ll G
rade 4
incid
ents
to e
nsure
urg
ent
and
appro
priate
action h
as b
een t
aken,
agre
e
impro
vem
ent action p
lan
Judy G
illo
w
Com
mence
in A
ug
ust
2009
No H
osp A
cq
uired g
rade
4 p
ressure
ulc
ers
in
Aug
ust.
11
To e
nsure
record
ing
of
appro
priate
info
rmation
to s
implif
y e
xtr
apola
tion
of
data
Revie
w N
urs
ing
/Medic
al docum
enta
tion
Lynn T
aylo
r M
ary
Clu
nie
O
cto
ber
2009
Redesig
n o
f w
ard
assessm
ent to
ol is
pro
gre
ssin
g a
nd w
ill b
e
used fro
m O
cto
ber.

19
12
To r
ais
e a
ware
ness a
nd
reduce n
um
ber
of
ulc
ers
pro
gre
ssin
g t
o g
rades
3/4
Revie
w r
eport
ing a
s c
linic
al in
cid
ents
gra
de 2
and
above
Julia
Bart
on
Lynn T
aylo
r A
ug
ust
2009
Action a
chie
ved a
nd w
ill
be o
ng
oin
g t
o e
nsure
consis
tency.
Ac
tio
ns a
t W
ard
& C
are
Gro
up
Level
13
To e
nsure
the
imple
menta
tion o
f best
pra
ctice
Devis
e,
imple
ment and m
onitor
achie
vem
ent of C
are
G
roup A
ction p
lans.
Develo
p a
pro
cess for
the p
revention o
f gra
de 2
pre
ssure
ulc
ers
Matr
ons
Aug
ust
2009
Pla
ns b
ein
g d
evelo
ped to
monitor
thro
ug
h T
issue
Via
bili
ty G
roup
14
To g
ain
assura
nce that
all
clin
ical are
as a
re
follo
win
g tru
st
polic
y in
the m
anag
em
ent of
pre
ssure
ulc
ers
Ward
AN
T t
o a
udit b
i-m
onth
ly a
min
imum
of
4 s
ets
of
case n
ote
s a
nd d
iscuss o
utc
om
es w
ith c
are
gro
up
matr
on
DH
N&
P
Lynn T
aylo
r July
2009
R
evis
ed
com
ple
tion
date
N
ov 0
9
•
Audit p
rocess r
olle
d
out
in T
rust and n
ow
needs e
mbeddin
g.
•
Audit t
ool ju
st
agre
ed
with c
om
mis
sio
ners
.
Ac
tio
ns f
or
Tis
su
e V
iab
ilit
y T
eam
15
To p
rovid
e s
pecia
list
advic
e o
n a
ppro
priate
m
anag
em
ent
of pre
ssure
ulc
ers
Devis
e c
are
path
ways
DH
ON
Lynn T
aylo
r S
epte
mber
2009
•
Triag
e s
yste
m in
pla
ce t
o p
rioritise
refe
rrals
accord
ing
to
need.
•
All
team
mem
bers
have a
job p
lan w
hic
h
ensure
s e
xpert
advic
e
is a
lwa
ys a
va
ilable
16
To e
nsure
access to
rele
vant
info
rmation
when p
lannin
g p
atient
care
Tis
sue V
iabili
ty F
old
ers
on a
ll w
ard
s t
o c
onta
in
pre
ssure
ulc
er
polic
y a
nd g
uid
elin
es.
Info
rmation o
n
the a
vaila
bili
ty a
nd c
orr
ect
use o
f eq
uip
ment
Lynn T
aylo
r O
cto
ber
2009
Work
in p
rogre
ss in
develo
pin
g t
he r
esourc
e
fold
ers
. polic
y a
nd
guid
elin
es a
lready
availa
ble
.
17
To h
ave a
pic
torial
record
of
a w
ound a
nd to
com
ply
with d
ata
pro
tection
Ag
ree p
roto
col fo
r photo
gra
phy; g
rade 3
&4s a
re
curr
ently p
hoto
gra
phed.
Lynn T
aylo
r A
ug
ust
2009
Dis
cussed a
t R
SO
G
meeting
2/0
9/0
9. P
rocess
still
under
delib
era
tion
18
To e
nsure
Tru
st re
ferr
al
polic
y is f
ollo
wed
Tis
sue V
iabili
ty r
efe
rral pro
cedure
to b
e a
vaila
ble
on
all
ward
s.
Education s
essio
ns w
ith m
atr
ons to b
e s
et
up t
o e
nsure
they u
nders
tand the p
rocess
Fra
n S
pra
tt
Lynn T
aylo
r A
ug
ust
2009
The r
efe
rral polic
y is
availa
ble
and e
ducation
sessio
ns h
ave

20
com
menced.
19
To im
pro
ve r
elia
bili
ty o
f risk a
ssessm
ent
Imple
ment B
raden R
isk A
ssessm
ent T
ool
Em
ma C
oole
y
Fra
n S
pra
tt
Revie
w
Novem
ber
2009
•
Pilo
t bein
g
undert
aken in G
ICU
.
•
Pla
n f
or
rollo
ut
in
pla
ce o
nce learn
ing
fo
rm the p
ilot is
taken
forw
ard
.
20
To r
educe t
ime to r
evie
w
patients
with s
uspecte
d
gra
de 3
/4 p
ressure
ulc
ers
Set
up h
otlin
e f
or
the r
efe
rral of gra
de 3
/4 p
ressure
ulc
ers
S
et
a s
tandard
for
specia
list
conta
ct
in 2
4hours
Lynn T
aylo
r A
ug
ust
2009
Achie
ved
Triag
e p
rocess in p
lace.
Tim
ing
s n
eed to b
e
agre
ed.
21
To incre
ase n
urs
ing
level
of
know
ledg
e to im
pro
ve
sta
ndard
s o
f care
Continue e
ducation s
essio
ns w
hic
h w
ill b
e o
pen to
att
endance fro
m a
cute
and a
ny p
rim
ary
care
team
m
em
bers
.
Lynn T
aylo
r R
evie
w
pro
gre
ss
Decem
ber
2009
Date
s o
f pla
nned
education s
essio
ns
availa
ble
in S
UH
T a
nd
com
munity
22
To a
gre
e m
etr
ics t
o
identify
im
pro
vem
ent in
th
e n
um
ber
of
hospital
acq
uired p
ressure
ulc
ers
To e
sta
blis
h %
im
pro
vem
ent ta
rget ag
ain
st baselin
e in
Q3.
DH
ON
M
atr
ons
Lynn T
aylo
r
Revie
w
pro
gre
ss
Decem
ber
2009
•
Metr
ics a
nd d
ata
re
port
ing p
rocess
agre
ed.
•
Ag
reem
ent
with
Com
mis
sio
ners
to
undert
ake a
baselin
e
assessm
ent
of
perf
orm
ance in Q
3
(see T
rust S
afe
ty
Str
ate
gy)

21
Acti
on
sL
ea
d
Revie
w a
nd U
pda
te t
he S
IRF
IT T
ool
Jun
e 2
009
.
Com
ple
te.
Deve
lop
en
ha
nced
guid
eline
s f
or
sta
ff t
o a
ssis
t th
em
in
com
ple
tin
g t
he
SIR
FIT
To
ol
Jun
e 2
009
.
Com
ple
te.
Deve
lop
exa
mple
SIR
FIT
to
ol to
aid
in w
ard
ba
sed
tra
inin
g a
nd
com
plian
ce
Aug
-09
Inclu
de
on
N&
M S
trate
gic
Fra
me
work
Ob
jective
s t
o p
erm
ea
te a
t
indiv
idu
al n
urs
e a
nd
ward
/dep
art
men
t le
ve
l.
JB
/NL
Oct-
09
Ne
ed
to in
cre
ase
co
mp
lia
nce w
ith
rea
sse
ssm
en
t
rate
s a
nd r
ecord
ing
pa
st
his
tory
with f
alls.
Spo
t S
IRF
IT A
ud
its t
o c
he
ck f
or
repe
at
assessm
ents
. P
NO
ct-
09
Tru
st
has c
on
fid
en
ce
th
at
inte
rve
ntio
ns t
o d
ecre
ase
avo
ida
ble
falls a
nd incre
ase S
IRF
IT c
om
plian
ce
are
eff
ectiv
e.
Care
gro
up
s t
o m
on
itor
SIR
FIT
com
pliance
and
take a
pp
ropri
ate
actio
ns.
Fa
lls
Cha
mp
ion
s
Qua
rte
rly
Com
mencin
g Q
2
2
Fall
s
Co
ord
ina
tor a
nd
Fra
ctu
re L
iais
on
Po
sts
Falls r
em
ain
s h
ighe
st
incid
ent
in t
erm
s o
f pa
tient
harm
. S
pe
cia
list
nurs
e/lea
ders
hip
re
sou
rce
for
red
ucin
g h
arm
fro
m f
alls :
SU
Ht
to b
enchm
ark
an
d
se
ek f
und
ing
to
incre
ase r
esou
rce.
Pro
gre
ss a
nd s
ecure
fu
nd
ing
fo
r a
falls C
oord
inato
r P
ost
and
A
fra
ctu
re L
iais
on P
ost
MM
/SZ
/DH
/JB
Jan
-10
3
Fin
alise
an
d d
istr
ibute
pa
tien
t in
form
ation
lea
fle
ts/g
uid
ance d
uri
ng
adm
issio
n a
nd
aft
er
a f
all f
or
dis
cha
rge.
HP
Com
ple
ted
May
200
9
Deve
lop
SU
HT
Fa
lls L
eafl
et
TB
C
Mar-
10
4L
ea
rnin
g f
rom
Incid
en
ts
Lea
rnin
g f
rom
incid
en
t re
po
rt f
orm
s a
nd a
udits o
f
com
plian
ce
Ana
lysis
of
incid
ent
Falls d
ata
repo
rted t
o S
UH
t P
atien
t F
alls G
roup
MM
Each m
ee
ting
De
liv
ery
of
PC
T Q
uality
Con
tract
data
an
d t
arg
ets
. A
gre
e B
ase L
ine
, P
resent
Data
. U
nd
ert
ake 1
0 in
dep
th a
ud
its p
er
qua
rte
rD
HQ
ua
rte
rly
Falls K
PIs
on
Inte
gra
ted
Sa
fety
Str
ate
gy a
re
deliv
ere
d.
Set
an
d a
gre
e a
void
ab
le f
alls b
ase
lin
e a
nd s
et
qu
art
erl
y
imp
rove
me
nt
targ
ets
. JB
Qua
rte
rly R
evie
w
Agre
e c
ale
nda
r a
nd
re
sp
on
sib
ilitie
s f
or
na
tion
al a
nd lo
cal au
dits
Com
ple
ted
Ju
ne
200
9
Falls A
udits d
eliv
ere
d o
n t
ime ,
resu
lts a
re d
isse
min
ate
d t
o C
are
Gro
up
Le
ad
s a
nd a
ctio
ns in
co
rpo
rate
d into
SU
HT
Falls
Pre
ve
ntio
n P
lan
. O
ct-
09
Actio
ns f
rom
pre
vio
us f
alls a
udits a
re d
eliv
ere
d a
nd r
ep
ort
ed
to
SU
HT
Falls G
rou
pO
ct-
09
6E
ng
ag
em
en
t an
d
Acc
ou
nta
bil
ity
Div
isio
na
l/C
are
Gro
up e
ng
ag
em
en
t in
fa
lls
pre
ve
ntio
n p
rogra
mm
e is h
igh
Goo
d a
tte
nd
an
ce
fro
m D
ivis
iona
l R
ep
s a
nd F
alls C
ham
pio
ns a
t
SU
HT
Patien
t F
alls G
roup
Div
Reps &
Fa
lls
Cha
mp
ion
s
Revie
w a
t Jun
e
200
9
dem
on
str
ate
s
much
im
pro
ve
d
positio
n.
Cle
are
r sig
npo
sting
to f
alls e
-le
arn
ing
tra
inin
g p
rogra
mm
e v
ia
IDE
AL
web
site.
M
M
Aug
-09
Tra
inin
g n
eeds a
na
lysis
com
ple
ted
by f
alls c
ham
pio
ns f
or
each
clin
ica
l are
a.
Fa
lls
Cha
mp
ion
sF
irst
rep
ort
Ju
ly
200
9
Falls t
rain
ing d
eliv
ery
as p
art
of
Rollin
g M
an
da
tory
Edu
ca
tion
train
ing
Da
ys
MM
Oct-
09
8F
all
s P
ath
way
s
Inte
r-o
rga
nis
ation
al p
ath
wa
ys a
re d
ev
elo
ped
In
ter-
org
anis
ation
al p
ath
wa
ys a
re d
ev
elo
pe
d v
ia n
ew
Dis
tric
t fa
lls
gro
up
SZ
/DH
Com
ple
ted
but
furt
he
r w
ork
nee
ded
on
imp
lem
en
tatio
n.
Upda
te r
eg
iste
r o
f F
alls C
ha
mpio
ns
DP
Sep
-09
Falls C
ham
pio
n R
ole
Descri
pto
r a
nd
Ind
uction
Sessio
n t
o b
e
dev
elo
ped
.
KO
Sep
-09
10
Usin
g C
orr
ec
t
Bed
He
igh
t
Secure
add
itio
nal L
ow
Be
d S
tock
Com
ple
te a
naly
sis
of
safe
ty issue
s a
roun
d low
bed
s a
nd p
rogre
ss
with
me
dic
al e
qu
ipm
ent
com
mitte
e.
Com
ple
te lo
w b
ed r
isk
asse
ssm
en
t fo
rm.
KO
/CG
Ls
Sep
-09
MM
SIR
FIT
to
ol com
pliance
ma
inta
ine
d a
t >
95
% in a
ll
div
isio
ns.
Au
dit
Falls A
udit p
rogra
mm
e is e
sta
blished
an
d
imp
lem
en
ted
. P
N
No
.
Sta
ff a
re f
ully info
rmed
and
un
de
rsta
nd
the
assessm
en
t, inte
rvention a
nd
do
cu
me
nta
tion
pro
ce
sse
s in r
ela
tio
n t
o f
alls a
sse
ssm
ent
an
d
pre
ve
ntio
n.
7
Falls C
ha
mpio
ns in
all a
reas
9
Tra
inin
g
Fall
s C
ha
mp
ion
s
Pati
en
t
Info
rm
ati
on
Patie
nt
wri
tten info
rma
tion
pre
and
post
falls is u
p
to d
ate
, re
lev
an
t and
av
aila
ble
to a
ll p
atien
ts in a
ll
sp
ecia
ltie
s.
Pe
rfo
rman
ce
5
SU
HT
Falls P
rev
en
tio
n P
lan
2009/1
0 (
V1)
Item
SIR
FIT
(F
all
s
As
ses
sm
en
t a
nd
Inte
rve
nti
on
s)
1
Tim
e F
ram
eK
ey D
eli
ve
rab
les
Falls a
udits c
om
ple
ted o
n s
chedule
with s
uff
icie
nt
evid
ence f
or
NH
SLA
/NP
SA
/PC
TS
/S4B
H e
tc.
Dedic
ate
d s
taff
in p
ost
Falls leaflets
are
dis
trib
ute
d b
y s
taff
in a
ll s
pecia
ltie
s.
SU
HT
Falls leaflet available
and u
ses c
orp
ora
te identity
in d
esig
n.
Inte
llig
ence a
bout fa
lls is a
cte
d u
pon a
ppro
pri
ate
ly.
Requir
ed P
TC
Contr
act
report
ing is c
om
ple
ted o
n t
ime a
nd w
ith
corr
ect
deta
il.
Avoid
able
falls r
educed b
y 2
0%
again
st
baseline f
or
2009/1
0.
All d
ivis
ions r
epre
sente
d a
t each m
onth
ly S
UH
T P
atient
Falls
Gro
up.
Incre
ase in n
um
bers
of
sta
ff c
om
ple
ting f
alls e
-learn
ing t
rain
ing
pro
gra
mm
e
% o
f sta
ff t
rain
ed t
o u
se S
IRF
IT is k
now
n a
nd d
eficit n
arr
ow
ed b
y
end o
f 2009/1
0.
Num
bers
of
sta
ff a
ttendin
g f
alls t
rain
ing incre
ases.
Str
onger
PC
T lin
ks f
or
patient
path
ways a
re e
vid
ent.
Additio
nal lo
w b
eds a
re a
vailable
to n
urs
e p
atient
who n
eed t
hese.
Update
d S
IRF
IT t
ool, g
uid
elines a
nd e
xam
ple
will be a
ppro
ved a
t
CS
CS
G a
nd a
vailable
on t
he S
UH
TR
AN
ET
.
Falls A
udits r
eflect
perf
orm
ance d
ata
and a
re r
eport
ed o
n tim
e.
Falls c
ham
pio
ns a
re e
mpow
ere
d t
o f
ulfil t
heir
role
and f
ully
support
ed b
y C
are
Gro
up leads.
Su
cc
es
s C
rite
ria
Ap
pen
dix
C:
Falls A
cti
on
Pla
n

22
AP
PE
ND
IX D
: D
ete
rio
rati
ng
Pati
en
t W
ork
Str
eam
Pla
n
No
G
oal
Acti
on
L
ead
C
om
ple
tio
n
Date
P
rog
ress a
t S
ep
tem
ber
2009
1)
Pilo
t of
ne
w c
olo
ur
co
de
d M
EW
S/O
bs c
hart
in
Div
isio
n 2
.
2)
Deliv
er
a p
hase
d launch
and r
oll
out
of
the
revis
ed o
bserv
atio
n c
hart
.
KH
In
Pro
gre
ss
F
ebru
ary
2010
Pilo
t com
menced. C
urr
ently r
evie
win
g
pro
form
a to m
ake n
ecessary
cha
nges
on th
is b
efo
re r
e-t
estin
g.
Inte
gra
te P
ain
Scorin
g o
nto
ME
WS
chart
K
H
Febru
ary
2010
Pla
nn
ing
du
e to c
om
mence s
hort
ly.
1
Incre
ase q
ualit
y a
nd c
onsis
tency o
f re
cord
ing
an
d d
ocum
enta
tion o
f patie
nt
observ
ations
Pilo
t use o
f R
ele
asin
g T
ime to C
are
Patient
Observ
ations m
odule
D
evelo
pm
ent of
contin
uous a
ud
it p
rogra
mm
e
KH
/MC
HN
To
com
mence
by N
ovem
ber
2009
Due t
o c
om
mence.
2
Ensure
eff
ective lin
kin
g o
f all
initia
tives
to e
nsure
patie
nts
with d
ete
riora
ting o
r hig
h a
cu
ity a
re s
afe
.
Develo
pm
ent of
an A
cu
ity C
are
Bund
le f
or
tria
ng
ula
tion o
f m
easure
s.
Revie
w o
f patients
th
at
are
re-a
dm
itte
d t
o G
ICU
and e
xplo
ration o
f an
y r
eve
rsib
le p
recip
ita
nts
HN
KH
Decem
ber
2009
Earl
y p
lannin
g c
om
menced.
Ongoin
g
3
Ensure
patients
are
assessed a
nd
treate
d b
y th
e m
ost appro
priate
m
em
ber
of
clin
ica
l sta
ff a
t th
e r
ight
level.
All
div
isio
ns to p
lan p
rogra
mm
es to incre
ase
ava
ilab
ility
of
senio
r re
vie
w w
here
appro
priate
.
Revie
w o
f appro
priate
esca
lation a
nd
revie
w
pro
cedure
s lin
ked t
o H
osp
ital @
Nig
ht
Serv
ice
and O
utr
each t
eam
.
Acute
ly ill
refe
rral path
wa
y a
lgorith
m d
eve
lop
ed t
o
assis
t sta
ff
in
escala
tion
pro
cess
and
tim
ely
in
terv
en
tion f
or
senio
r re
vie
w
Dis
cussio
n
an
d
rais
ing
aw
are
ness
sessio
n
with
D
CD
s a
nd
DH
Ns a
t T
EC
DW
HN
ST
HN
/DW
Jan 20
10
D
ecem
ber
2009
C
om
ple
ted
C
om
ple
ted
Phase
d r
oll
out of
ne
w s
yste
ms f
or
senio
r re
vie
w t
akin
g p
lace in a
ll div
isio
ns.
Revie
w a
nd
de
ve
lopm
ent of
new
pro
tocols
has c
om
menced.
Com
ple
ted
Com
ple
ted
4
Ensure
sta
ff a
re e
ffectively
tra
ine
d a
nd
meet acuity c
om
pete
ncy s
tandard
s
Acuity F
ound
ation P
rogra
mm
e for
new
sta
ff,
inclu
din
g r
egis
tere
d n
urs
es, ju
nio
r d
octo
rs a
nd
stu
dent
nurs
es.
KH
Com
ple
ted
Pro
gra
mm
e d
eve
lop
ed a
nd
bein
g
deliv
ere
d.

23
Develo
p c
ascade-t
rain
ing
appro
ach.
Pro
vis
ion o
f A
LE
RT
/SM
AR
T m
ulti-pro
fessio
nal
pro
gra
mm
es for
deve
lop
ing
skill
s in th
e
recognitio
n o
f th
e a
cute
ly ill
patient.
D
evelo
pm
ent of
Vita
l L
ife S
upport
co
urs
e (
VL
S)
to
pro
vid
e e
ducation r
ela
ting
to p
recurs
ors
of
card
iac
arr
est.
K
H
K
H
K
H
M
arc
h 2
010
O
ng
oin
g
O
ng
oin
g
Pla
nn
ing
du
e to c
om
mence s
hort
ly.
Ongoin
g p
rovis
ion in p
lace.
D
evelo
ped
an
d in p
rogre
ss.
5
Ensure
hig
hest d
egre
e o
f a
ccura
cy
and
inte
rpre
tation
in
the
record
ing o
f blo
od
pre
ssure
.
Develo
p n
ew
tra
inin
g p
rogra
mm
e in c
om
pete
ncy
for
the r
ecord
ing (
manual) o
f blo
od p
ressure
.
Agre
e s
tand
ard
for
the c
on
sis
tent usa
ge o
f m
anual B
P r
ecord
ing.
CV
/
KH
HN
Jan
uary
2010
Com
ple
ted in D
iv2, ro
llin
g o
ut in
Div
1
and 4
. P
lann
ing
du
e to c
om
mence s
hort
ly f
or
band
2 ind
uctio
n p
rogra
mm
e. .
Develo
p m
ore
com
pre
hensiv
e s
tandard
s a
nd
com
pete
ncie
s f
or
patie
nt o
bserv
atio
ns a
nd
im
ple
ment th
ese a
cro
ss a
ll re
levant
clin
ica
l are
as.
HN
/KH
D
ec
2009
Rolle
d o
ut
in D
ivis
ion 2
and
no
w
underw
ay in
Div
isio
n 1
.
6
Ensure
sta
ff a
re w
ork
ing to c
urr
ent
evid
ence b
ase
d p
ractice g
uid
elin
es f
or
all
aspects
of
acuity m
anag
em
ent.
Develo
pm
ent of
an a
cute
ly ill
pa
thw
ay a
lgorith
m to
assis
t sta
ff in the e
scala
tion
pro
cess a
nd t
imely
in
terv
en
tion f
or
senio
r re
vie
w.
KH
D
ec 0
9
Develo
ped
an
d in p
rocess o
f cascadin
g t
o s
taff
.
7
Ensure
co
nsis
tent
escala
tio
n a
nd
com
munic
ation
for
patient’s w
hose
acuity is d
ete
riora
ting
.
Roll
ou
t of
SB
AR
com
munic
ation
an
d h
ando
ver
tool.
KH
D
ec 0
9
75%
of
clin
ica
l are
as n
ow
utilis
ing
SB
AR
(a
ll of
div
isio
n 1
an
d 2
). P
lans
for
full
imple
menta
tion a
cro
ss
Specia
lty a
reas in D
ivis
ions 3
an
d 4
pro
gre
ssin
g w
ell.
Share
acuity d
ata
in “
Safe
ty M
atters
”, th
e m
onth
ly
safe
ty c
om
munic
ation b
riefing.
KH
/SS
A
ug
ust 09
Com
ple
ted.
8
Dis
sem
ination
of
perf
orm
ance a
nd a
ud
it
data
to r
ele
van
t sta
ff to d
rive a
cuity
impro
vem
ent.
Q
uart
erl
y W
ard
Report
s d
eta
ilin
g w
ard
le
ve
l card
iac a
rrest a
nd a
ud
it d
ata
to b
e issued.
KH
HN
Septe
mber
09
Com
ple
ted.
Com
ple
ted
6 m
onth
ly r
olli
ng a
ud
it p
rog
ram
me (
again
st N
ICE
50 s
tan
dard
s)
KH
C
om
ple
ted
In p
lace
9
Ensure
eff
ective m
easure
ment a
nd
record
ing
of
perf
orm
ance for
acuity
KP
Is.
R
evie
w o
f patients
that
are
readm
itte
d to
GIC
U
and e
xplo
ration o
f an
y r
eve
rsib
le p
recip
ita
nts
.
KH
M
arc
h 2
010
Ongoin
g.
Re
vie
w o
n a
Q b
asis
.
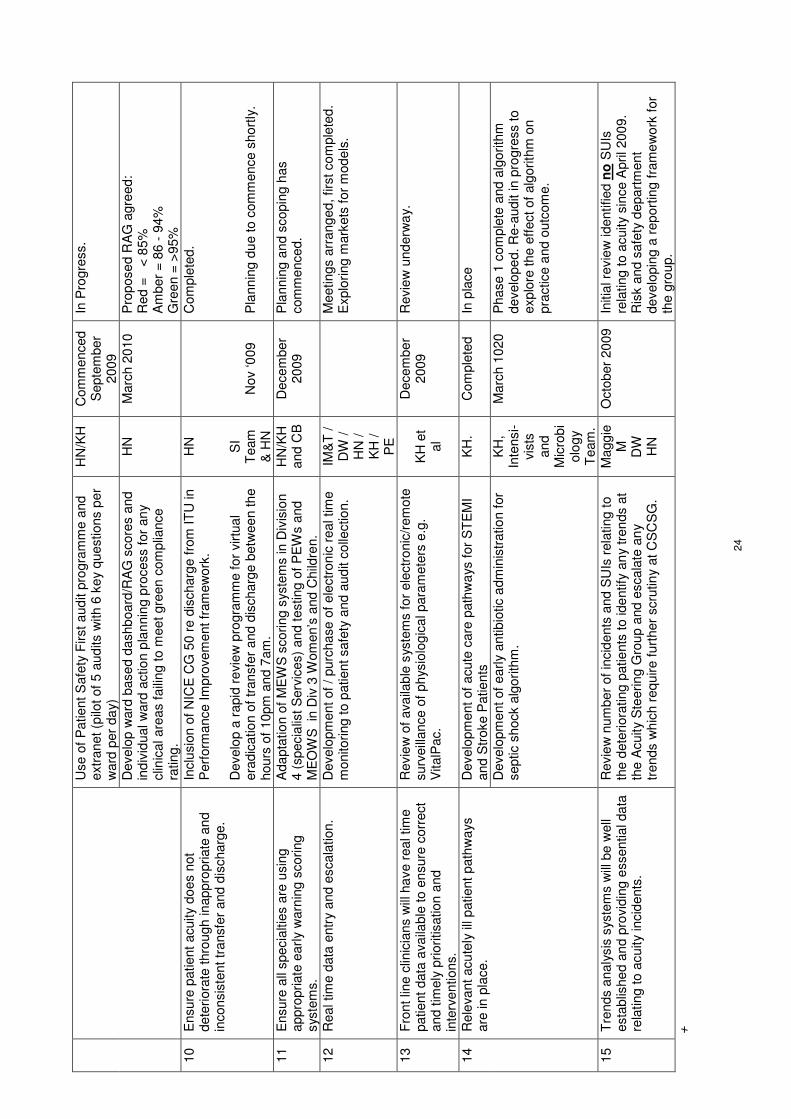
24
Use o
f P
atient
Safe
ty F
irst
aud
it p
rogra
mm
e a
nd
extr
anet (p
ilot of
5 a
ud
its w
ith 6
ke
y q
uestions p
er
ward
per
da
y)
HN
/KH
C
om
menced
Septe
mber
2009
In P
rogre
ss.
Develo
p w
ard
base
d d
ashb
oard
/RA
G s
core
s a
nd
in
div
idual w
ard
actio
n p
lan
nin
g p
rocess f
or
an
y
clin
ical are
as f
aili
ng to m
ee
t gre
en
com
plia
nce
rating
.
HN
M
arc
h 2
010
Pro
pose
d R
AG
agre
ed:
Red =
<
85%
A
mber
= 8
6 -
94%
G
reen =
>95%
10
Ensure
patient
acuity d
oes n
ot
dete
riora
te thro
ugh in
appro
priate
an
d
inconsis
tent tr
ansfe
r and d
ischarg
e.
Inclu
sio
n o
f N
ICE
CG
50 r
e d
ischarg
e f
rom
IT
U in
Perf
orm
ance Im
pro
vem
ent fr
am
ew
ork
. D
evelo
p a
rapid
re
vie
w p
rogra
mm
e for
virtu
al
era
dic
atio
n o
f tr
ansfe
r and d
ischarg
e b
etw
ee
n th
e
hours
of
10pm
and 7
am
.
HN
SI
Team
&
HN
N
ov ‘0
09
Com
ple
ted.
Pla
nn
ing
du
e to c
om
mence s
hort
ly.
11
Ensure
all
specia
ltie
s a
re u
sin
g
appro
priate
earl
y w
arn
ing
scoring
sys
tem
s.
Ada
pta
tio
n o
f M
EW
S s
coring s
yste
ms in D
ivis
ion
4 (
specia
list
Serv
ices)
an
d t
esting
of
PE
Ws a
nd
ME
OW
S in
Div
3 W
om
en’s
and C
hild
ren.
HN
/KH
and C
B
Decem
ber
2009
Pla
nn
ing
an
d s
copin
g h
as
com
menced.
12
Real tim
e d
ata
entr
y a
nd e
scala
tion.
Develo
pm
ent of
/ purc
hase o
f ele
ctr
on
ic r
eal tim
e
monitoring t
o p
atient safe
ty a
nd a
ud
it c
olle
ctio
n.
IM&
T /
DW
/
HN
/
KH
/
PE
M
eetings a
rrang
ed, firs
t co
mple
ted.
Explo
ring
mark
ets
for
models
.
13
Fro
nt lin
e c
linic
ians w
ill h
ave r
eal tim
e
patient
data
ava
ilable
to
en
sure
corr
ect
and t
imely
pri
oritisation a
nd
in
terv
en
tions.
Revie
w o
f ava
ilab
le s
yste
ms f
or
ele
ctr
onic
/rem
ote
surv
eill
ance o
f ph
ysio
log
ica
l para
mete
rs e
.g.
VitalP
ac.
K
H e
t al
Decem
ber
2009
Revie
w u
nd
erw
ay.
Develo
pm
ent of
acute
care
path
wa
ys f
or
ST
EM
I and S
troke P
atie
nts
K
H.
Com
ple
ted
In p
lace
14
Rele
va
nt acu
tely
ill
patient
path
wa
ys
are
in
pla
ce.
Develo
pm
ent of
earl
y a
ntib
iotic a
dm
inis
tratio
n f
or
septic s
hock a
lgori
thm
.
KH
, In
tensi-
vis
ts
and
Mic
rob
iolo
gy
Team
.
Marc
h 1
020
Phase 1
com
ple
te a
nd a
lgo
rith
m
develo
pe
d. R
e-a
ud
it in p
rogre
ss to
explo
re t
he e
ffect of
alg
orith
m o
n
pra
ctice a
nd o
utc
om
e.
15
Tre
nds a
naly
sis
syste
ms w
ill b
e w
ell
esta
blis
he
d a
nd p
rovid
ing e
ssentia
l da
ta
rela
ting t
o a
cuity incid
ents
.
Revie
w n
um
ber
of
incid
ents
and S
UIs
rela
ting t
o
the d
ete
riora
ting p
atie
nts
to
ide
ntify
an
y tre
nds a
t th
e A
cuity S
teerin
g G
roup a
nd e
scala
te a
ny
trends w
hic
h r
eq
uire
furt
her
scru
tin
y a
t C
SC
SG
.
Magg
ie
M
DW
H
N
Octo
ber
20
09
Initia
l re
vie
w identified n
o S
UIs
re
lating t
o a
cuity s
ince A
pril 200
9.
Ris
k a
nd s
afe
ty d
epart
ment
develo
pin
g a
rep
ort
ing f
ram
ew
ork
for
the g
roup.
+

25
Ap
pen
dix
E:
Nu
trit
ion
/MU
ST
Acti
on
Pla
n
N
o
Go
al
Acti
on
L
ead
C
om
ple
tio
n
Date
P
rog
ress a
t S
ep
tem
ber
2009
1
Ensure
that
patien
ts h
ave
suff
icie
nt a
nd c
onsis
tent
help
an
d s
up
port
to e
at
and d
rink
Carr
y o
ut a “
Mea
ltim
e A
ssis
tant”
Pilo
t and
imple
ment use o
f volu
nte
ers
to a
ssis
t w
ith
feedin
g in
a p
hase
d w
ay a
cro
ss p
riority
are
as.
HW
JB
K
S
Marc
h 2
010
Pilo
t com
ple
ted in O
lder
Pe
rsons C
are
gro
up.
Report
wri
tte
n a
nd d
iscussed a
t P
atie
nt
Experi
ence S
teerin
g g
rou
p.
Roll
out p
lans b
ein
g
develo
pe
d.
2
Patients
will
experi
ence
hig
h levels
of
pri
vacy a
nd
dig
nity a
t m
ealtim
es a
nd
not b
e inte
rrup
ted
unnecessari
ly f
or
clin
ical
pro
cedure
s.
Undert
ake a
re
vie
w a
nd r
ela
unch o
f “P
rote
cte
d
Mea
ltim
es“
in th
e c
onte
xt of
ne
w c
ate
rin
g
contr
act m
ealtim
es a
rrange
ments
due to b
e
rolle
d o
ut acro
ss a
ll w
ard
s b
y Y
E.
HW
JB
M
atr
ons
Decem
ber
2009
.
Man
y w
ard
s h
ave im
ple
mente
d p
rote
cte
d
mealtim
es a
nd g
uid
ance
ha
s b
een d
issem
inate
d.
Revie
w o
f th
is a
nd n
um
bers
of
are
as s
till
not
live
with p
rote
cte
d m
ealtim
es d
ue to
be u
nd
ert
aken
short
ly.
3
Ward
based N
utr
itio
n lin
k
role
s w
ill b
e w
ell
train
ed
and e
ffective in p
rom
oting
best nu
tritio
n p
ractice in
their c
linic
al are
as.
Revie
w o
f A
NT
(A
gents
for
Tis
sue V
iab
ility
and
Nutr
itio
n)
Role
an
d c
on
trib
ution
to e
nsuri
ng local
sta
ndard
s a
re m
ain
tain
ed
and a
udited.
Refo
cus
and tra
inin
g to b
e p
rovid
ed w
here
nee
d
ide
ntifie
d.
HW
&
D
iete
tics
team .
Decem
ber
2009
Revie
w o
f A
NT
role
underw
ay.
Sessio
n w
ith A
NT
s
revea
led n
ee d
to m
inim
ise v
ari
ation a
nd incre
ase
support
for
this
vita
l ro
le.
Pla
ns in
pla
ce.
4
The N
utr
itio
n S
teerin
g
gro
up w
ill b
e e
ffective
in
pro
vid
ing t
he r
ight
str
ate
gic
direction f
or
an
nua
l w
ork
priorities.
Mon
itori
ng a
nd
assura
nce o
f nutr
itio
n a
nd
hydra
tio
n w
ork
str
eam
s w
ill
be c
arr
ied o
ut eff
ective
ly.
Revie
w a
nd
rela
unch o
f com
mitte
e s
tructu
re f
or
nutr
itio
n
HW
JB
N
ovem
ber
2009
Revie
w c
om
ple
ted a
nd d
ue
to g
o o
ut fo
r consulta
tio
n s
hort
ly.
5
Sta
ff w
ill b
e c
lear
abou
t re
quirem
ents
for
MU
ST
assessm
ent.
Rela
unch o
f M
US
T p
rogra
mm
e g
uid
elin
es
HW
D
ecem
ber
2009
Revie
w u
nd
erw
ay.
6
Sta
ff w
ill k
no
w w
hen
, w
here
and h
ow
to
docum
ent m
ust
assessm
ents
and o
ngo
ing
care
pla
ns f
or
patients
with
nutr
itio
n a
nd h
ydra
tio
n
needs
Revie
w o
f M
US
T d
ocum
enta
tio
n a
nd c
are
path
wa
ys f
or
patie
nts
at ri
sk o
f m
aln
utr
itio
n.
Lin
ks w
ith a
cu
ity w
ork
str
eam
for
record
ing o
f fluid
bala
nce.
HW
JB
M
arc
h 2
010
MU
ST
Docum
enta
tio
n is in p
lace b
ut re
vie
w h
as
hig
hlig
hte
d n
ee
d f
or
ong
oin
g c
are
pla
ns a
nd
reassessm
ents
in p
atie
nts
record
s. P
lan t
o D
/W
sta
ff m
em
ber
undert
akin
g r
evie
w o
f docum
enta
tio
n.


















