Sonography and the Acute Abdomen
8
AJR:168, January 1997 179 Perspective Sonography and the Acute Abdomen: Practical Considerations Julien B. C. M. Puylaert1, Friso M. van der Zant1, Arie M. Rijke2 O ver the past 10 years, sonography . . has gained acceptance for examin- ing patients with acute abdominal pain. Sonography is dynamic, noninvasive, rapid, inexpensive, and readily accessible; however, it has some serious drawbacks. Use is limited in obese patients; the ultrasound beam cannot penetrate bone or gas; and sonography, more than other radiologic techniques, is oper- ator-dependent and requires skill, dedication, and experience. In this perspective, several practical aspects of using sonography on patients with acute abdominal pain are highlighted. These aspects include the choice between sonography and CT as an initial examining technique, the timing of the sonographic examination, sonographically guided puncture, the value of indirect sono- graphic findings, the significance of normal findings on a sonogram, and, finally, commu- nication with the clinician. Indications Traditionally, surgeons have accepted a high negative laparotomy rate to avoid the risks of ill-advised surgical delay. Nonetheless, serious surgical delay inside the hospital is common. A prospective study of patients with a suspected appendicitis showed a negative laparotomy rate of 27%; and concomitant serious therapeutic delay in 14% of patients who needed surgery [1]. Another prospective study dividing patients into three categories (high, equivocal, and low clinical suspicion) showed that even in the high- suspicion group, 35% of the patients did not have an appendicitis, whereas 5% of the patients in the low-suspicion group had an inflamed appendix [2]. In 30 patients with a ruptured aortic aneurysm, treatment was delayed more than 6 hr because of misdiagnosis [3]. These figures show that the clinical diagno- sis of an acute abdomen is unreliable and that the threshold for radiologic imaging studies should be low. The concept of sonography as a helpful diagnostic tool used only in cases of clinical doubt is and should be rejected. The impact of sonography on clinical man- agement of patients with an acute abdomen is impressive. In a study of patients with sus- pected appendicitis, sonographic findings sig- nificantly changed the therapeutic management in 26% of patients [4]. In three independent studies using sonography, negative laparotomy rates were 13%, 13%, and 7%, respectively, [4-61 with a concomitant reduction in unneces- sary surgical delay. In our institution, virtually all patients with acute or subacute abdominal pain are referred for a sonogram, including patients for whom surgery seems definitely required as well as patients with a remote possi- bility ofrequiring surgery (Figs. 1 and 2). Not surprisingly, sonography of the acute abdomen has markedly affected routine prac- tice in many institutions. Sonography per- formed on indication of acute abdominal pain makes up 25% of all abdominal sonographic examinations at our institution, and nation- wide, acute abdominal pain has become the most frequent reason for radiologists to go in to the hospital when they are on call. Sonography or CT as Initial Technique? Several acute abdominal conditions are more easily detected on a CT scan than on a sono- gram. They include a ruptured aortic aneurysm, an aortic dissection, an esophageal rupture, a mycotic aneurysm, an acute pancreatitis, an incarcerated internal hernia, and perirenal and hepatic abscesses. In addition, CT scans usually provide better results in obese patients who have retrocecal appendicitis, appendiceal abscess, deeply located sigmoid diverticulitis, closed-loop bowel obstruction, gastrointestinal perforation to the retropetitoneum, and emphy- sematous cholecystitis. However, in experi- enced hands, the sonograrn can still be used to reliably diagnose most acute abdominal condi- tions in most patients [4]. Therefore, a reason- Received June 1, 1995; accepted after revision July 23, 1996. 1 Department of Radiology, Westeinde Hospital. Ujnbaan 32, 2512 VA The Hague, the Netherlands. Address correspondence to J. B. C. M. Puylaert 2Department of Radiology. Health Sciences Center, University of Virginia. Lee St, Charlottesville, VA 22908. AJR 1997;168:179-186 0361-803X/97/1681-179 © American Roentgen Ray Society
-
Upload
alexander-natroshvili -
Category
Documents
-
view
45 -
download
4
Transcript of Sonography and the Acute Abdomen
AJR:168, January 1997 179
Perspective
Sonography and the Acute Abdomen: PracticalConsiderationsJulien B. C. M. Puylaert1, Friso M. van der Zant1, Arie M. Rijke2
O ver the past 10 years, sonography. . has gained acceptance for examin-
ing patients with acute abdominal
pain. Sonography is dynamic, noninvasive,
rapid, inexpensive, and readily accessible;
however, it has some serious drawbacks. Use is
limited in obese patients; the ultrasound beam
cannot penetrate bone or gas; and sonography,
more than other radiologic techniques, is oper-
ator-dependent and requires skill, dedication,
and experience.
In this perspective, several practical aspects
of using sonography on patients with acute
abdominal pain are highlighted. These aspects
include the choice between sonography and CT
as an initial examining technique, the timing of
the sonographic examination, sonographically
guided puncture, the value of indirect sono-
graphic findings, the significance of normal
findings on a sonogram, and, finally, commu-
nication with the clinician.
Indications
Traditionally, surgeons have accepted a high
negative laparotomy rate to avoid the risks of
ill-advised surgical delay. Nonetheless, serious
surgical delay inside the hospital is common. A
prospective study of patients with a suspected
appendicitis showed a negative laparotomy rate
of 27%; and concomitant serious therapeutic
delay in 14% of patients who needed surgery
[1]. Another prospective study dividing patients
into three categories (high, equivocal, and low
clinical suspicion) showed that even in the high-
suspicion group, 35% of the patients did not
have an appendicitis, whereas 5% of the
patients in the low-suspicion group had an
inflamed appendix [2]. In 30 patients with a
ruptured aortic aneurysm, treatment was
delayed more than 6 hr because of misdiagnosis
[3]. These figures show that the clinical diagno-
sis of an acute abdomen is unreliable and that
the threshold for radiologic imaging studies
should be low. The concept of sonography as
a helpful diagnostic tool used only in cases of
clinical doubt is and should be rejected.
The impact of sonography on clinical man-
agement of patients with an acute abdomen is
impressive. In a study of patients with sus-
pected appendicitis, sonographic findings sig-
nificantly changed the therapeutic management
in 26% of patients [4]. In three independent
studies using sonography, negative laparotomy
rates were 13%, 13%, and 7%, respectively,
[4-61 with a concomitant reduction in unneces-
sary surgical delay. In our institution, virtually
all patients with acute or subacute abdominal
pain are referred for a sonogram, including
patients for whom surgery seems definitely
required as well as patients with a remote possi-
bility ofrequiring surgery (Figs. 1 and 2).
Not surprisingly, sonography of the acute
abdomen has markedly affected routine prac-
tice in many institutions. Sonography per-
formed on indication of acute abdominal pain
makes up 25% of all abdominal sonographic
examinations at our institution, and nation-
wide, acute abdominal pain has become the
most frequent reason for radiologists to go in
to the hospital when they are on call.
Sonography or CT as Initial Technique?
Several acute abdominal conditions are more
easily detected on a CT scan than on a sono-
gram. They include a ruptured aortic aneurysm,
an aortic dissection, an esophageal rupture, a
mycotic aneurysm, an acute pancreatitis, an
incarcerated internal hernia, and perirenal and
hepatic abscesses. In addition, CT scans usually
provide better results in obese patients who
have retrocecal appendicitis, appendiceal
abscess, deeply located sigmoid diverticulitis,
closed-loop bowel obstruction, gastrointestinal
perforation to the retropetitoneum, and emphy-
sematous cholecystitis. However, in experi-
enced hands, the sonograrn can still be used to
reliably diagnose most acute abdominal condi-
tions in most patients [4]. Therefore, a reason-
Received June 1, 1995; accepted after revision July 23, 1996.
1 Department of Radiology, Westeinde Hospital. Ujnbaan 32, 2512 VA The Hague, the Netherlands. Address correspondence to J. B. C. M. Puylaert
2Department of Radiology. Health Sciences Center, University of Virginia. Lee St, Charlottesville, VA 22908.
AJR 1997;168:179-186 0361-803X/97/1681-179 © American Roentgen Ray Society
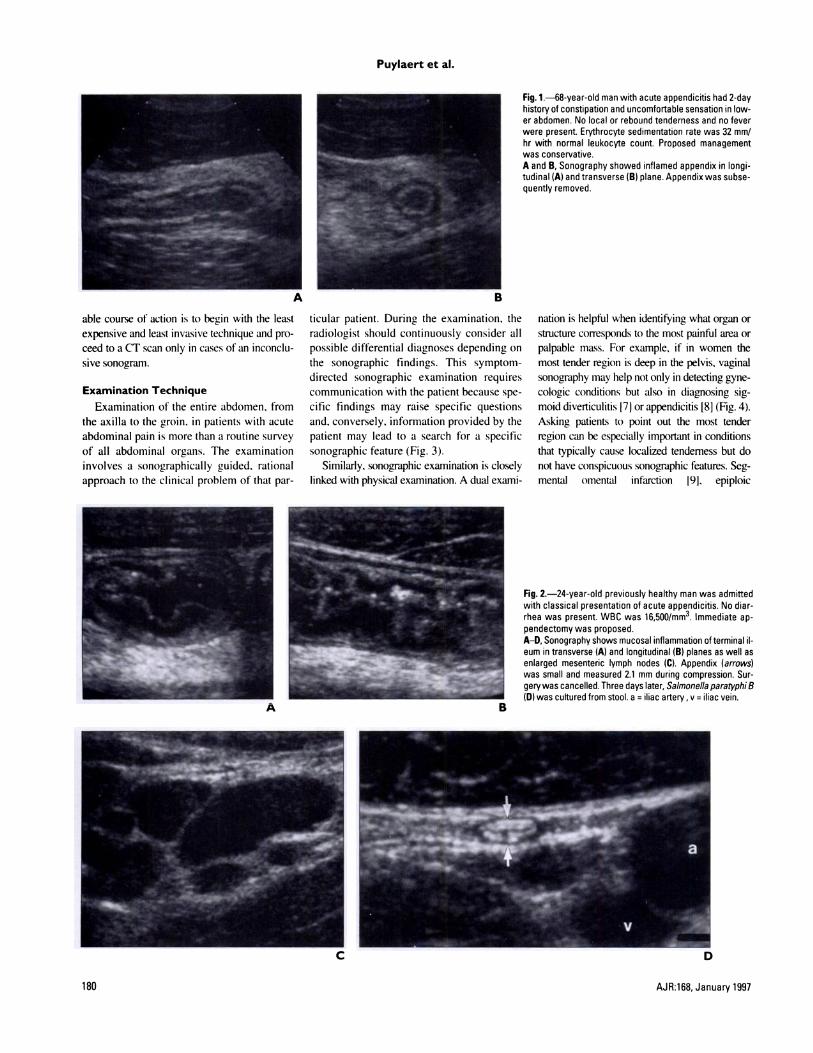
Fig. 2-24-year-old previously healthy man was admittedwith classical presentation of acute appendicitis. No diar-rhea was present WBC was 16,500!mm3. Immediate ap-pendectomy was proposed.AD, Sonography shows mucosal inflammation ofterminal 1-eum in transverse (A) and longitudinal (B) planes as well asenlarged mesenteric lymph nodes (C). Appendix (arrows)was small and measured 2.1 mm during compression. Sur-gery was cancelled. Three days later, Salmonella paratyphi B(D) was cultured from stool. a = iliac artery , v = iliac vein.
Puylaert et al.
180 AJR:168, January 1997
able course of action is to begin with the least
expensive and least invasive technique and pro-
ceed to a CT scan only in cases of an inconclu-
sive sonogram.
Examination Technique
Examination of the entire abdomen, from
the axilla to the groin. in patients with acute
abdominal pain is more than a routine survey
of all abdominal organs. The examination
involves a sonographically guided. rational
approach to the clinical problem of that par-
ticular patient. During the examination, the
radiologist should continuously consider all
possible differential diagnoses depending on
the sonographic findings. This symptom-
directed sonographic examination requires
communication with the patient because spe-
cific findings may raise specific questions
and. conversely, information provided by the
patient may lead to a search for a specific
sonographic feature (Fig. 3).
Similarly. sonographic examination is closely
linked with physical examination. A dual exami-
Fig. 1-68-year-old man with acute appendicitis had 2-dayhistory of constipation and uncomfortable sensation in low-er abdomen. No local or rebound tenderness and no feverwere present Erythrocyte sedimentation rate was 32 mm!hr with normal leukocyte count Proposed managementwas conservative.A and B, Sonography showed inflamed appendix in longi-tudinal (A) and transverse (B) plane. Appendix was subse-quently removed.
nation is helpful when identifying what organ or
structure corresponds to the most painful area or
palpable mass. For example. if in women the
most tender region is deep in the pelvis, vaginal
sonography may help not only in detecting gyne-
cologic conditions but also in diagnosing sig-
moid diverticulitis 171or appendicitis [8] (Fig. 4).
Asking patients to point out the most tender
region can be especially important in conditions
that typically cause localized tenderness but do
not have conspicuous sonographic features. Seg-
mental omental infarction 19]. epiploic
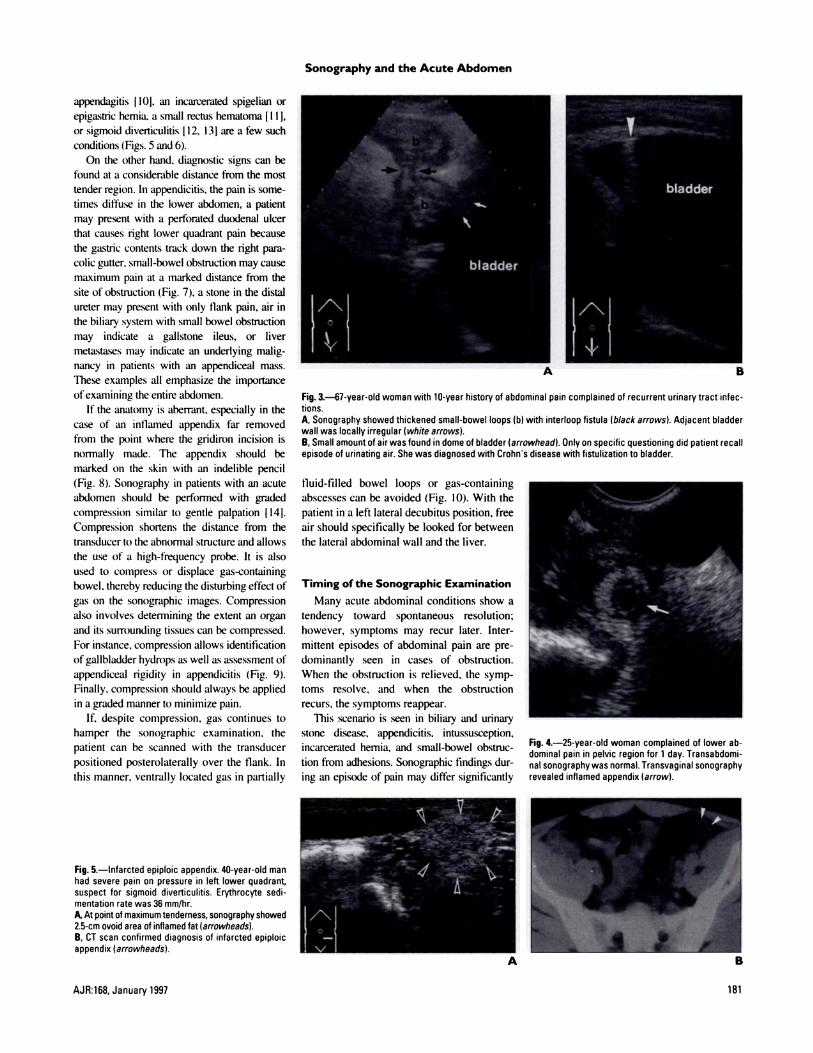
Fig. 3-67-year-old woman with 10-year history of abdominal pain complained of recurrent urinary tract infec-tions.A, Sonography showed thickened small-bowel loops (b) with interloop fistula (black arrows). Adjacent bladderwall was locally irregular (white arrows).B, Small amount of air was found in dome of bladder (arrowhead). Only on specific questioning did patient recallepisode of urinating air. She was diagnosed with Crohns disease with fistulization to bladder.
Fig. 4.-25-year-old woman complained of lower ab-dominal pain in pelvic region for 1 day. Transabdomi-nal sonography was normal. Transvaginal sonographyrevealed inflamed appendix (arrow).
Fig. 5.-Infarcted epiploic appendix. 40-year-old manhad severe pain on pressure in left lower quadrant,suspect for sigmoid diverticulitis. Erythrocyte sedi-mentation rate was 36 mm!hr.A, At point of maximum tenderness, sonography showed2.5-cm ovoid area of inflamed fat (arrowheads).B, CT scan confirmed diagnosis of infarcted epiploicappendix (arrowheads).
Sonography and the Acute Abdomen
AJR:168, January 1997 181
appendagitis f 10), an incarcerated spigelian or
epiga.stric hernia, a small rectus hematoma [I I],
or sigmoid diverticulitis [ I 2, 13j are a few such
conditions (Figs. 5 and 6).
On the other hand. diagnostic signs can be
found at a considerable distance from the most
tender region. In appendicitis. the pain is some-
times diffuse in the lower abdomen, a patient
may present with a perforated duodenal ulcer
that causes right lower quadrant pain because
the gastric contents track down the right pare-
colic gutter. small-bowel obstruction may cause
maximum pain at a marked distance from the
site of obstruction (Fig. 7), a stone in the distal
ureter may present with only flank pain, air in
the biliary system with small bowel obstniction
may indicate a gallstone ileus, or liver
metastases may indicate an underlying malig-
nancy in patients with an appendiceal mass.
These examples all emphasize the importance
of examining the entire abdomen.
If the anatomy is aberrant. especially in the
case of an inflamed appendix far removed
from the point where the gridiron incision is
normally made. The appendix should be
marked on the skin with an indelible pencil
(Fig. 8). Sonography in patients with an acute
abdomen should be performed with graded
compression similar to gentle palpation [ 14).
Compression shortens the distance from the
transducer to the abnormal structure and allows
the use of a high-frequency probe. It is also
used to compress or displace gas-containing
bowel. thereby reducing the disturbing effect of
gas on the sonographic images. Compression
also involves determining the extent an organ
and its surrounding tissues can be compressed.
For instance, compression allows identification
of gallbladder hydrops as well as assessment of
appendiceal rigidity in appendicitis (Fig. 9).
Finally, compression should always be applied
in a graded manner to minimize pain.
If. despite compression. gas continues to
hamper the sonographic examination, the
patient can be scanned with the transducer
positioned posterolaterally over the flank. In
this manner. ventrally located gas in partially
fluid-filled bowel loops or gas-containing
abscesses can be avoided (Fig. 10). With the
patient in a left lateral decubitus position, free
air should specifically be looked for between
the lateral abdominal wall and the liver.
Timing of the Sonographic Examination
Many acute abdominal conditions show a
tendency toward spontaneous resolution;
however, symptoms may recur later. Inter-
mittent episodes of abdominal pain are pre-
dominantly seen in cases of obstruction.
When the obstruction is relieved, the symp-
toms resolve. and when the obstruction
recurs, the symptoms reappear.
This scenario is seen in biliary and urinary
stone disease. appendicitis. intussusception,
incarcerated hernia, and small-bowel obstruc-
tion from adhesions. Sonographic findings dur-
ing an episode of pain may differ significantly
Puylaert et al.
182 AJR:168, January 1997
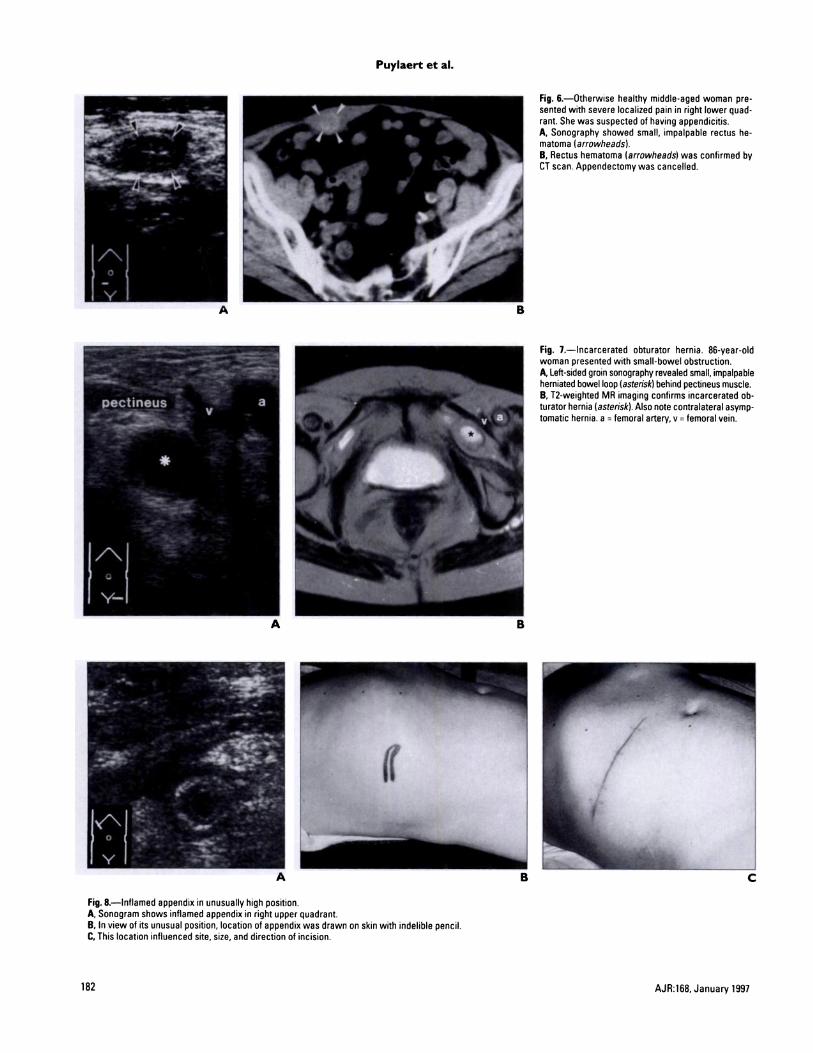
Fig. 8.-Inflamed appendix in unusually high position.A, Sonogram shows inflamed appendix in right upper quadrant.B. In view of its unusual position, location of appendix was drawn on skin with indelible pencil.C. This location influenced site, size, and direction of incision.
Fig. 6.-Otherwise healthy middle-aged woman pre-sented with severe localized pain in right lower quad-rant. She was suspected of having appendicitis.A, Sonography showed small, impalpable rectus he-matoma (arrowheads).B, Rectus hematoma (arrowheads) was confirmed byCT scan. Appendectomy was cancelled.
Fig. 1.-Incarcerated obturator hernia. 86-year-oldwoman presented with small-bowel obstruction.A, Left-sided groin sonography revealed small, impalpableherniated bowel loop (asterisk) behind pectineus muscle.B, T2-weighted MR imaging confirms incarcerated ob-turator hernia (asterisk). Also note contralateral asymp-tomatic hernia. a = femoral artery, v = femoral vein.
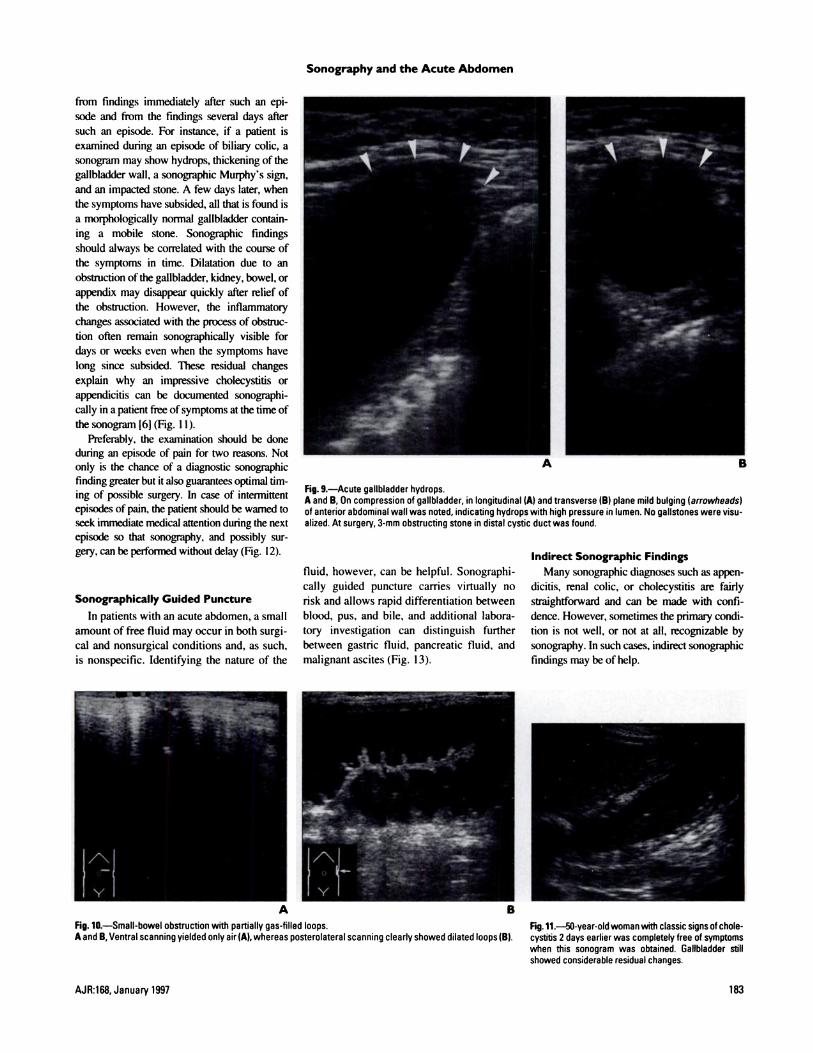
Fig. 9.-Acute gallbladder hydrops.A and B, On compression of gallbladder, in longitudinal (A) and transverse (B) plane mild bulging (arrowheads)of anterior abdominal wall was noted, indicating hydrops with high pressure in lumen. No gallstones were visu-alized. At surgery, 3-mm obstructing stone in distal cystic duct was found.
Fig. 10.-Small-bowel obstruction with partially gas-filled loops. Fig. 11.-50-year-oldwomanwith classic signs of chole-A and B, Ventral scanning yielded only air(A), whereas posterolateral scanning clearly showed dilated loops (B). cystitis 2 days earlier was completely free of symptoms
when this sonogram was obtained. Gallbladder stillshowed considerable residual changes.
Sonography and the Acute Abdomen
AJR:168, January 1997 183
from findings immediately after such an epi-
sode and from the findings several days after
such an episode. For instance, if a patient is
examined during an episode of biliary colic, a
sonogram may show hydrops, thickening of the
gallbladder wall, a sonographic Murphy’s sign,
and an impacted stone. A few days later, when
the symptoms have subsided, all that is found is
a morphologically normal gallbladder contain-
ing a mobile stone. Sonographic findings
should always be correlated with the course of
the symptoms in time. Dilatation due to an
obstruction ofthe gallbladder, kidney, bowel, or
appendix may disappear quickly after relief of
the obstruction. However, the inflammatory
changes associated with the process of obstruc-
tion often remain sonographically visible for
days or weeks even when the symptoms have
long since subsided. These residual changes
explain why an impressive cholecystitis or
appendicitis can be documented sonographi-
cally in a patient free ofsymptoms at the time of
the sonogram 16](Fig. I1).
Preferably, the examination should be done
during an episode of pain for two reasons. Not
only is the chance of a diagnostic sonographic
finding greater but it also guarantees optimal tim-
ing of possible surgery. In case of intennirtent
episodes ofpain, the patient should be warned to
seek immediate medical attention during the next
episode so that sonography, and possibly sur-
gery, can be performed without delay (Fig. 12).
Sonographically Guided Puncture
In patients with an acute abdomen, a small
amount of free fluid may occur in both surgi-
cal and nonsurgical conditions and, as such,
is nonspecific. Identifying the nature of the
fluid, however, can be helpful. Sonographi-
cally guided puncture carries virtually no
risk and allows rapid differentiation between
blood, pus, and bile, and additional labora-
tory investigation can distinguish further
between gastric fluid, pancreatic fluid, and
malignant ascites (Fig. 13).
Indirect Sonographic Findings
Many sonographic diagnoses such as appen-
dicitis, renal colic, or cholecystitis are fairly
straightfoaward and can be made with confi-
dence. However, sometimes the primary condi-tion is not well, or not at all, recognizable by
sonography. In such cases, indirect sonographic
findings may be of help.
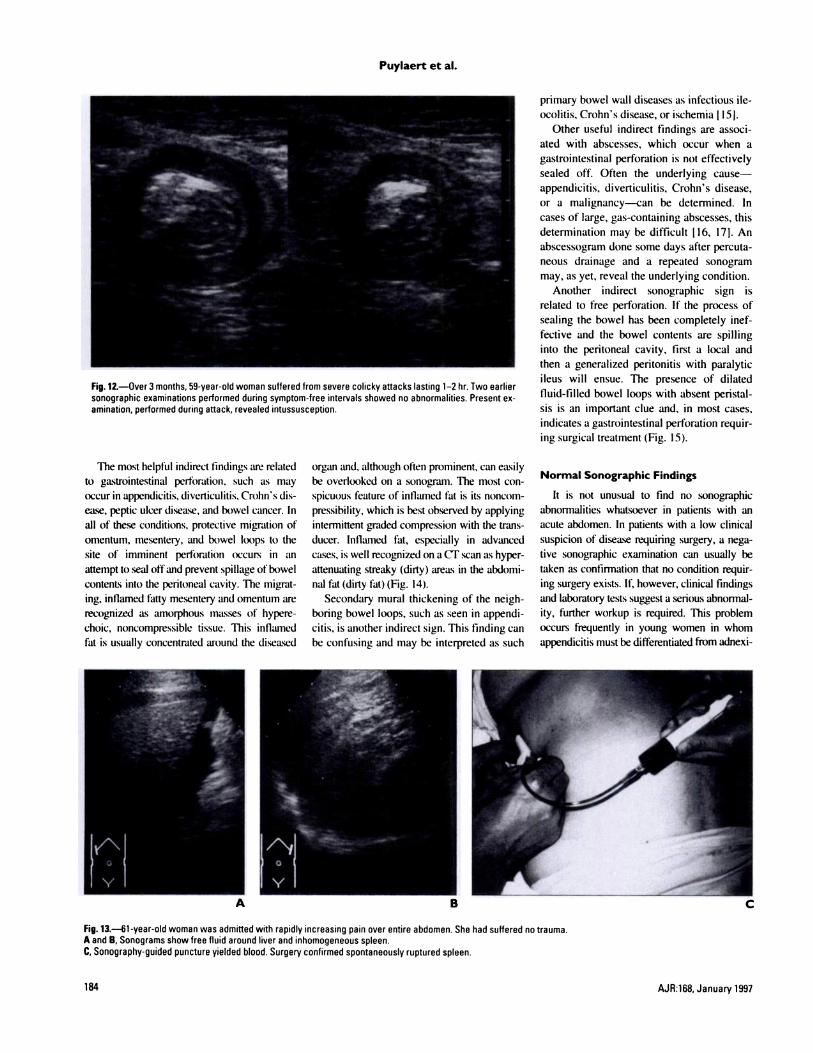
Fig. 12.-Over 3 months, 59-year-old woman suffered from severe colicky attacks lasting 1-2 hr. Two earliersonographic examinations performed during symptom-free intervals showed no abnormalities. Present ex-amination, performed during attack, revealed intussusception.
Puylaert et al.
184 AJR:168, January 1997
primary bowel wall diseases as infectious ile-
ocolitis. Crohn’s disease, or ischemia I 15).
Other useful indirect findings are associ-
ated with abscesses, which occur when a
gastrointestinal perforation is not effectively
sealed off. Often the underlying cause-
appendicitis, diverticulitis, Crohn’s disease,
or a malignancy-can be determined. In
cases of large, gas-containing abscesses, this
determination may be difficult I 16, 17). An
abscessogram done some days after percuta-
neous drainage and a repeated sonogram
may, as yet, reveal the underlying condition.
Another indirect sonographic sign is
related to free perforation. If the process of
sealing the bowel has been completely inef-
fective and the bowel contents are spilling
into the peritoneal cavity. first a local and
then a generalized peritonitis with paralytic
ileus will ensue. The presence of dilated
fluid-filled bowel loops with absent peristal-
sis is an important clue and. in most cases,
indicates a gastrointestinal perforation requir-
ing surgical treatment (Fig. 15).
The most helpful indirect findings are related
to gastrointestinal pert�ration. such as may
occur in appendicitis, diverticulitis. Crohn’s dis-
ease, peptic ulcer disease, and bowel cancer. In
all of these conditions, protective migration of
omentum, inesenteiy, and bowel loops to the
site of imminent perThration occurs in an
attempt to seal offand prevent spillage of howel
contents into the peritoneal cavity. The migrat-
ing, inflamed fatty mesentery and omentum are
recognized as amorphous masses of hypere-
choic, noncompressible tissue. This inflamed
fat is usually concentrated around the diseased
organ and, although often prominent, can easily
be overlooked on a sonogram. The most con-
spicuous feature of inflamed fat is its noncom-
pressibility, which is best observed by applying
intermittent graded compression with the trans-
ducer. Inflamed fat, especially in advanced
cases, is well recognized on a CT scan as hyper-
attenuating streaky (dirty) areas in the abdomi-
nal fat(dirtyfat)(Fig. 14).
Secondary mural thickening of the neigh-
boring bowel loops, such as seen in appendi-
citis, is another indirect sign. This finding can
be confusing and may be interpreted as such
Normal Sonographic Findings
It is not unusual to find no sonographic
abnormalities whatsoever in patients with an
acute abdomen. In patients with a low clinical
suspicion of disease requiring surgery, a nega-
tive sonographic examination can usually be
taken as confirmation that no condition requir-
ing surgery exists. lf� however, clinical findings
and laboratory tests suggest a serious abnormal-
ity, further workup is required. This problem
occurs frequently in young women in whom
appendicitis must be differentiated from adnexi-
Fig. 13.-61-year-old woman was admitted with rapidly increasing pain over entire abdomen. She had suffered no trauma.A and B, Sonograms show free fluid around liver and inhomogeneous spleen.C, Sonography-guided puncture yielded blood. Surgery confirmed spontaneously ruptured spleen.
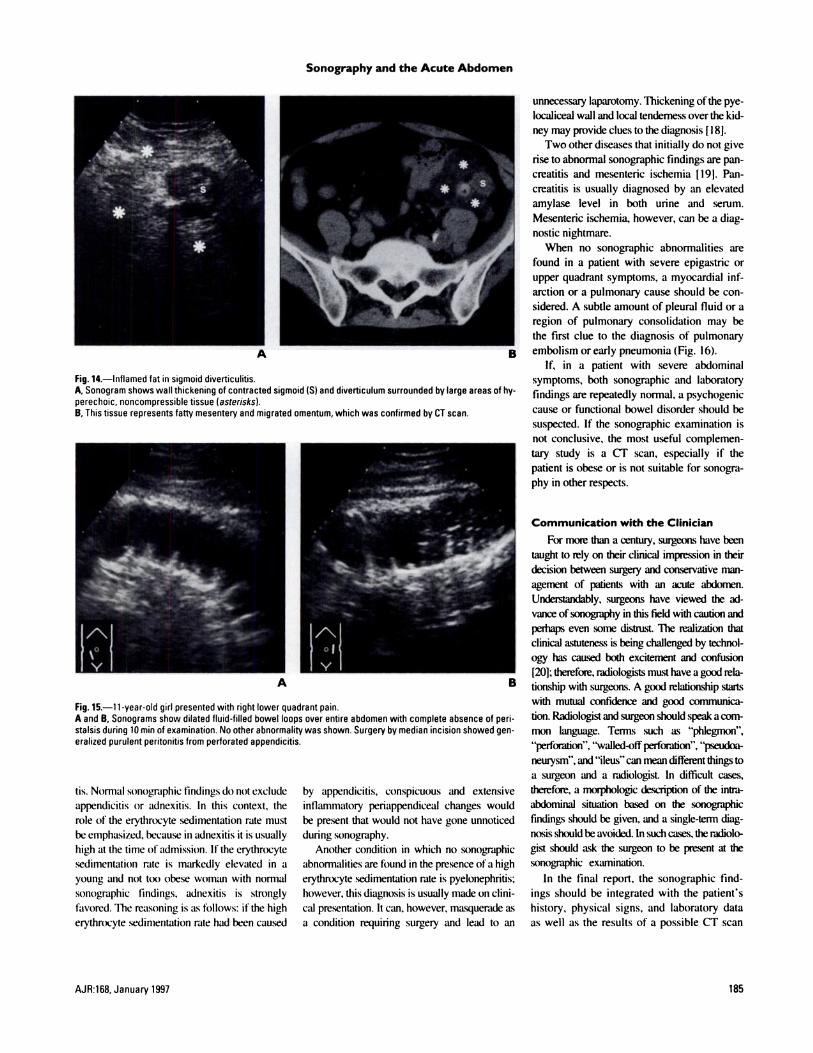
Fig. 14.-Inflamed fat in sigmoid diverticulitis.A, Sonogram shows wall thickening of contracted sigmoid (5) and diverticulum surrounded by large areas of hy-perechoic, noncompressible tissue (asterisks).B, This tissue represents fatty mesentery and migrated omentum, which was confirmed by CT scan.
A B
Fig. 15.-i 1-year-old girl presented with right lower quadrant pain.A and B, Sonograms show dilated fluid-filled bowel loops over entire abdomen with complete absence of pen-stalsis during 10 mm of examination. No other abnormality was shown. Surgery by median incision showed gen-eralized purulent peritonitis from perforated appendicitis.
Sonography and the Acute Abdomen
AJR:168, January 1997 185
tis. Normal sonographic findings do not exclude
appendicitis or adnexitis. In this context, the
role of the erythrocyte sedimentation rate must
be emphasized, because in adnexitis it is usually
high at the time of admission. If the etythrocyte
sedimentation rate is markedly elevated in a
young and not too obese woman with normal
sonographic findings. adnexitis is strongly
favored. The reasoning is as follows: if the high
erythrocyte sedimentation rate had been caused
by appendicitis, conspicuous and extensive
inflammatory periappendiceal changes would
be present that would not have gone unnoticed
during sonography.
Another condition in which no sonographic
abnormalities are found in the presence ofa high
erythrocyte sedimentation rate is pyelonephritis;
however, this diagnosis is usually made on clini-
cal presentation. It can, however, masquerade as
a condition requiting surgery and lead to an
unnecessary laparotomy. Thickening ofthe pye-
localiceal wall and local tenderness over the kid-
ney may provide clues to the diagnosis [ I 8J.
Two other diseases that initially do not give
rise to abnormal sonographic findings are pan-
creatitis and mesenteric ischemia [19). Pan-
creatitis is usually diagnosed by an elevated
amylase level in both urine and serum.
Mesenteric ischemia, however, can be a diag-
nostic nightmare.
When no sonographic abnormalities are
found in a patient with severe epigastric or
upper quadrant symptoms, a myocardial inf-
arction or a pulmonary cause should be con-
sidered. A subtle amount of pleural fluid or a
region of pulmonary consolidation may be
the first clue to the diagnosis of pulmonary
embolism or early pneumonia (Fig. 16).
If, in a patient with severe abdominal
symptoms, both sonographic and laboratory
findings are repeatedly normal. a psychogenic
cause or functional bowel disorder should be
suspected. If the sonographic examination is
not conclusive, the most useful complemen-
tary study is a CT scan, especially if the
patient is obese or is not suitable for sonogra-
phy in other respects.
Communication with the Clinician
For mote than a century, surgeons have been
taught to rely on their clinical impression in their
decision between surgery and conservative man-
agement of patients with an acute abdomen.
Understandably, surgeons have viewed the ad-
vance ofsonography in this field with caution and
perhaps even some distrust. The realization that
clinical astuteness is being challenged by technol-
ogy has c&tsed both excitement and confusion
[20}; therefore, radiologists must have a good rela-
tionship with surgeons. A good relationship starts
with mutual confidence and good communica-
tion. Radiologist and surgeon should speak acorn-
mon language. Tenns such as “phlegmon”,
“perforation”, “walled-offperforation”, “pseudoa-
neulysm”, and “ileus”can mean differentthings to
a surgeon and a radiologist In difficult cases,
therefore, a morphologic description of the intni-
abdominal situation based on the sonographic
findings should be given, and a single-term diag-
nosis should be avoided. ln such cases, the radiolo-
gisi should ask the surgeon to be present at the
sonographic examination.
In the final report, the sonographic find-
ings should be integrated with the patient’s
history, physical signs, and laboratory data
as well as the results of a possible CT scan
Puylaert et al.
186 AJR:168, January 1997
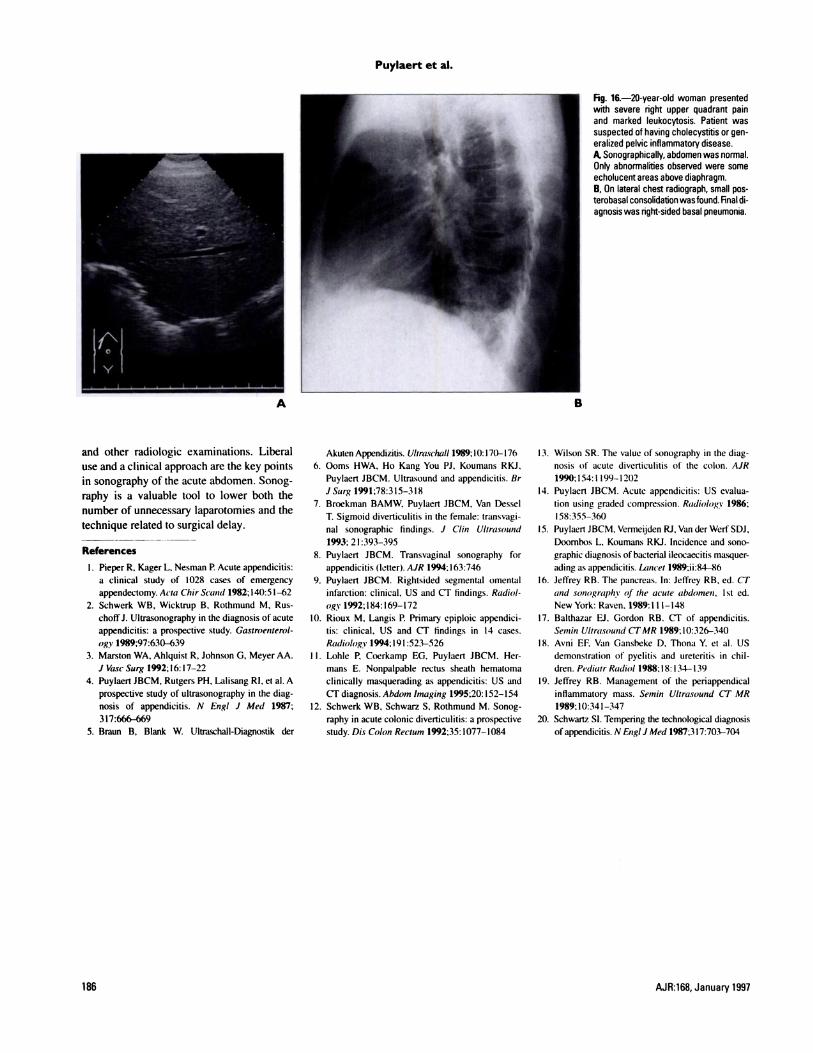
Fig. 16.-2O-year-old woman presentedwith severe right upper quadrant painand marked leukocytosis. Patient wassuspected of having cholecystitis or gen-eralized pelvic inflammatory disease.A, Sonographically. abdomen was normal.Only abnormalities observed were someecholucent areas above diaphragm.B, On lateral chest radiograph, small pos-terobasal consolidation wasfound. Final di-agnosis was right-sided basal pneumonia.
and other radiologic examinations. Liberal
use and a clinical approach are the key points
in sonography of the acute abdomen. Sonog-
raphy is a valuable tool to lower both the
number of unnecessary laparotomies and the
technique related to surgical delay.
References
I. Pieper R. Kager L, Nesman P. Acute appendicitis:a clinical study of 1028 cases of emergencyappendectomy. Acw Chir Scand 1982; 140:51-62
2. Schwerk WB, Wicktrup B, Rothmund M, Rus-
choffi. Ultrasonography in the diagnosis of acute
appendicitis: a prospective study. Gastroenterol-
ogv 1989:97:630-6393. Marston WA, Ahlquist R, Johnson G, Meyer AA.
J VascSurg 1992:16:17-22
4. Puylaert JBCM. Rutgers PH. Lalisang RI, et al. A
prospective study of ultrasonography in the diag-
nosis of appendicitis. N Engi J Med 1987;317:666-669
5. Braun B, Blank W. Ultraschall-Diagnostik der
Akuten Appendizitis. Ultraschall 1989: 10: 17()-l76
6. Ooms HWA. Ho Kang You PJ, Koumans RKJ,
Puylaert JBCM. Ultrasound and appendicitis. Br
JSurg 1991:78:315-3 18
7. Broekman BAMW, Puylaert JBCM, Van Dessel
1. Sigmoid diverticulitis in the female: transvagi-
nal sonographic findings. J C/in Ultrasound
1993; 2 1:393-395
8. Puylaert JBCM. Transvaginal sonography for
appendicitis (letter). AJR 1994:163:746
9. Puylaert JBCM. Rightsided segmental omental
infarction: clinical, US and CT findings. Radiol-
Og)� 1992;l84: 169-172
10. Rioux M, Langis P. Primary epiploic appendici-
tis: clinical, US and CT findings in 14 cases.
Radiolog% 1994:191:523-526
I I . Lohle P. Coerkamp EG. Puylaert JBCM. Her-
mans E. Nonpalpable rectus sheath hematoma
clinically masquerading as appendicitis: US and
CT diagnosis. Abdom Imaging 1995:20:152-154
12. Schwerk WB, Schwarz 5, Rothmund M. Sonog-
raphy in acute colonic diverticulitis: a prospective
study. Dis Colon Rectum 1992:35:1077-1084
I 3. Wilson SR. The value of sonography in the diag-
nosis of acute diverticulitis of the colon. AiR
1990:154:1199-120214. Puylaert JBCM. Acute appendicitis: US evalua-
tion using graded compression. Radiology 1986:
158:355-360
IS. Puylaert JBCM. Vermeijden Ri, Van der WerfSDJ,Doornhos L, Koumans RKJ. Incidence and sono-
graphic diagnosis of bacterial ileocaecitis masquer-
ading as appendicitis. Lrnicet l989:ii:84-86
16. Jeffrey RB. The pancreas. In: Jeffrey RB. ed. CT
and sonographv of the acute abdomen, 1St ed.
New York: Raven. 1989:111-14817. Balthazar El. Gordon RB. CT of appendicitis.
Semin Ultrasound CT MR 1989; 10:326-340
18. Avni EF. Van Gansheke D, Thona Y. et al. US
demonstration of pyelitis and ureteritis in chil-
dren. Pediatr Radio! 1988:18:134-139
19. Jeffrey RB. Management of the periappendical
inflammatory mass. Seinin Ultrasound CT MR
1989;10:341-34720. Schwartz SI. Tempering the technological diagnosis
ofappendicius. N EnglJ Med 1987:317:703-704