
Sonic and ultrasonic scaling
40
-
Upload
jignesh-patel -
Category
Health & Medicine
-
view
99 -
download
12
Transcript of Sonic and ultrasonic scaling
* Introduction
* Mode of action
* Sonic scaling devices
* Ultrasonic scaling devices
* Instrument tip design
* Indications
* Contraindications
* Efficacy and efficiency of the instruments
* Precaution/ special consideration
Manual instrumentation was the only method available for the
safe removal of supra and subgingival calculus until the
ultrasonic devices were introduced into 1950.
Ultrasonic/sonic scalers are famous by names of Power driven
scalers or machine driven scalers.
These scalers convert high frequency electrical energy
(ultrasonic) or air pressure (sonic) into high frequency sound
waves.
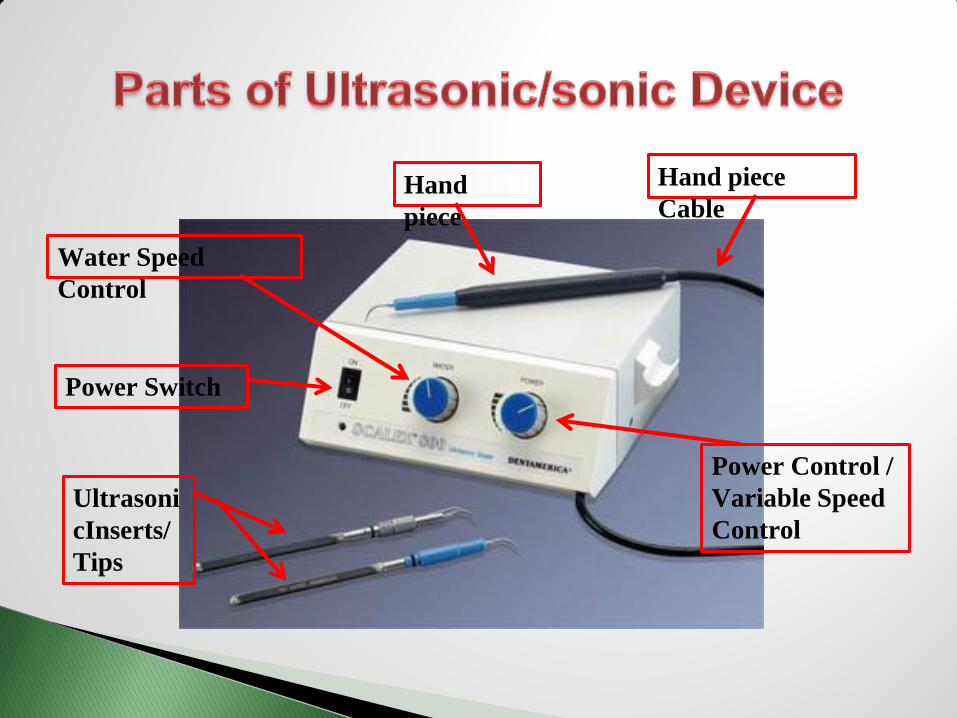
Hand piece
Cable Hand
piece
Power Control /
Variable Speed
Control
Water Speed
Control
Power Switch
Ultrasoni
cInserts/
Tips
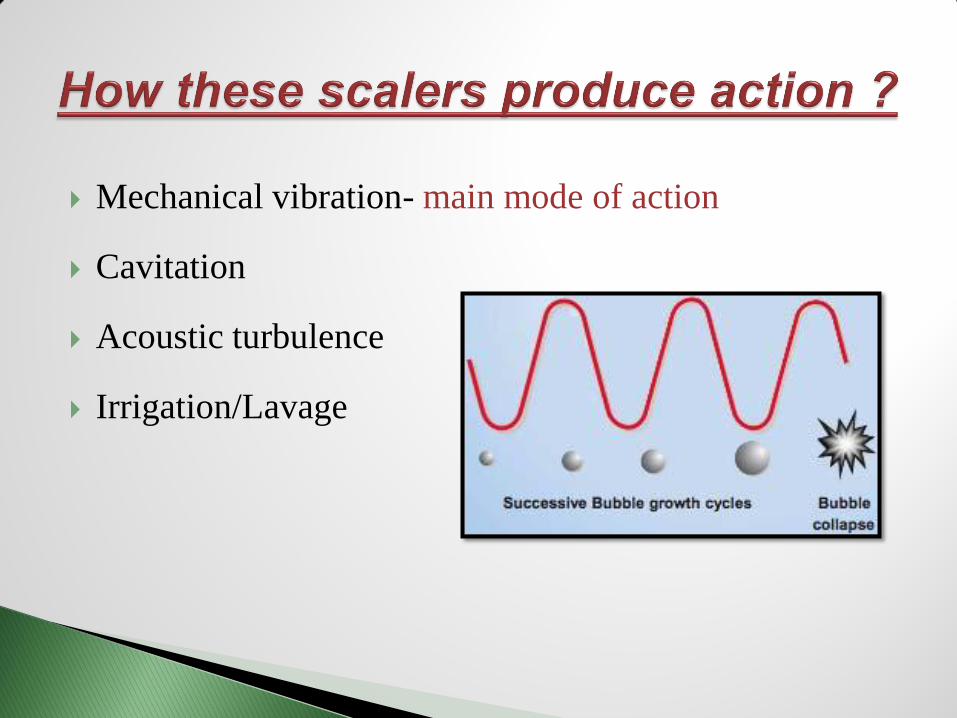
Mechanical vibration- main mode of action
Cavitation
Acoustic turbulence
Irrigation/Lavage
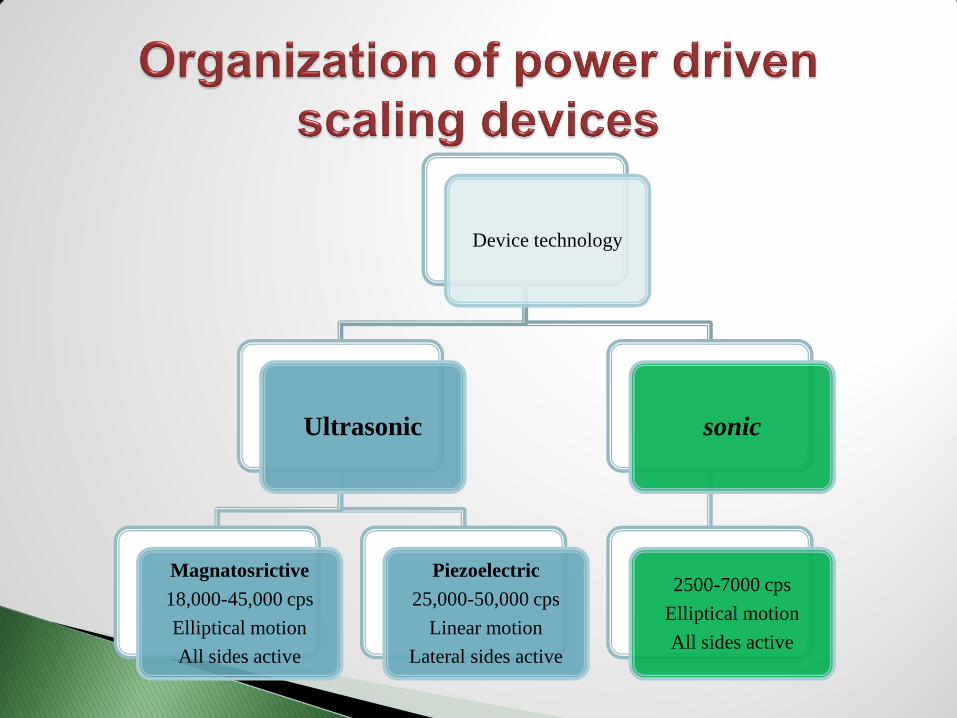
Device technology
Ultrasonic
Magnatosrictive
18,000-45,000 cps
Elliptical motion
All sides active
Piezoelectric
25,000-50,000 cps
Linear motion
Lateral sides active
sonic
2500-7000 cps
Elliptical motion
All sides active
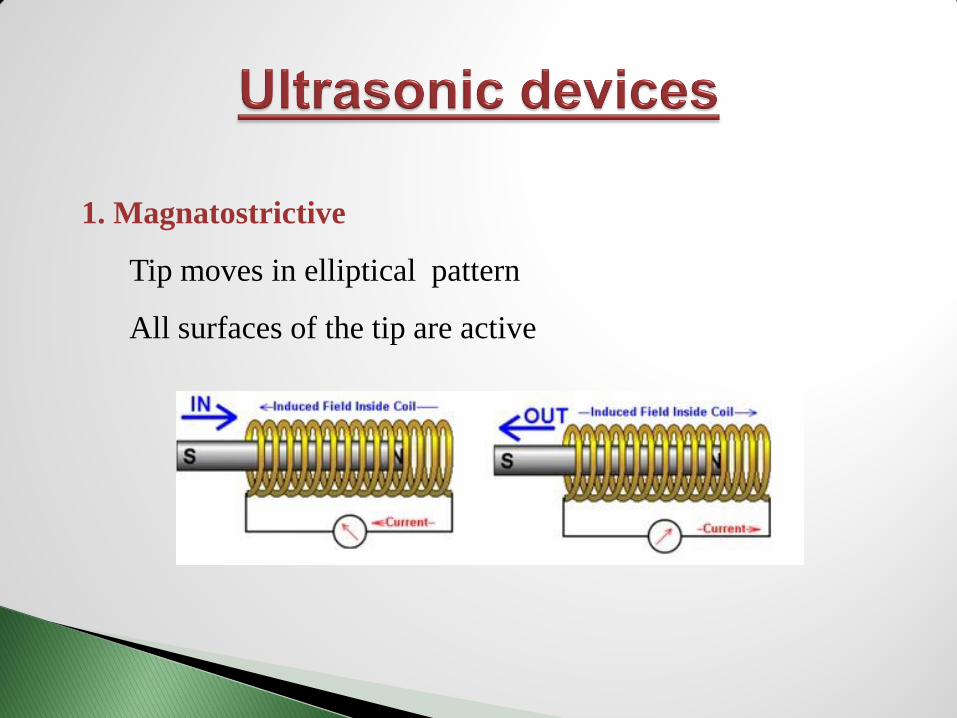
1. Magnatostrictive
Tip moves in elliptical pattern
All surfaces of the tip are active

Magnatostrictive generator with insert tips
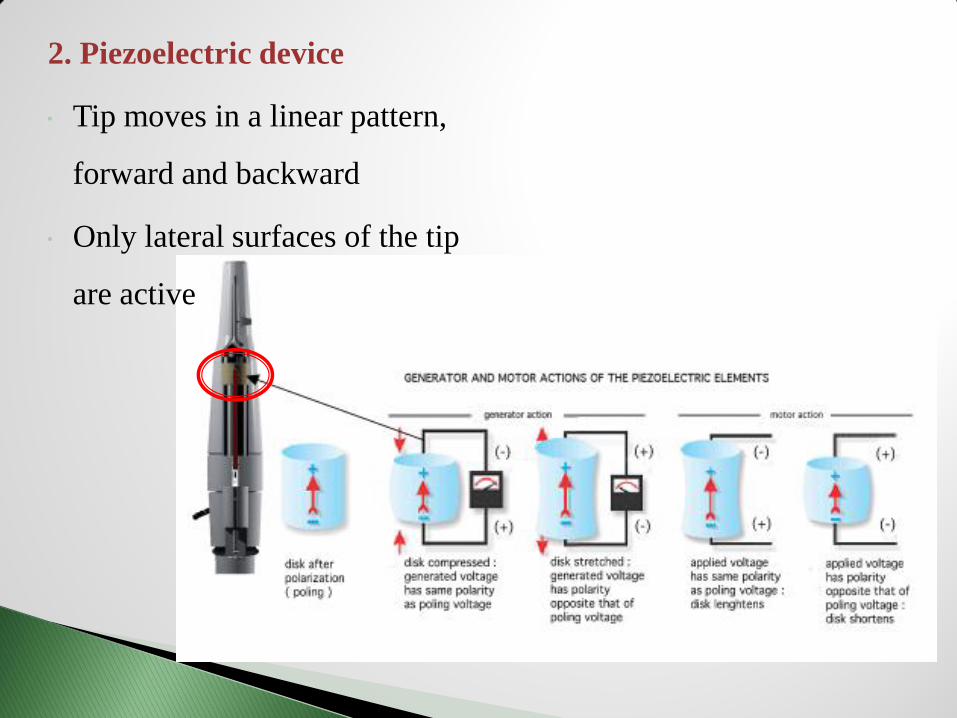
2. Piezoelectric device
Tip moves in a linear pattern,
forward and backward
Only lateral surfaces of the tip
are active
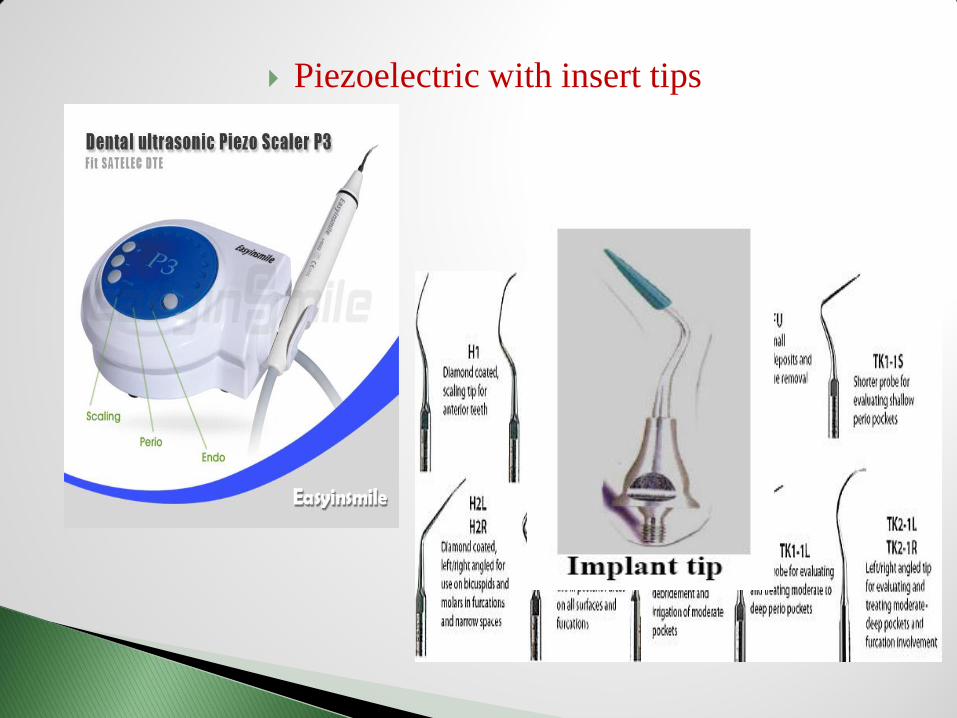
Piezoelectric with insert tips
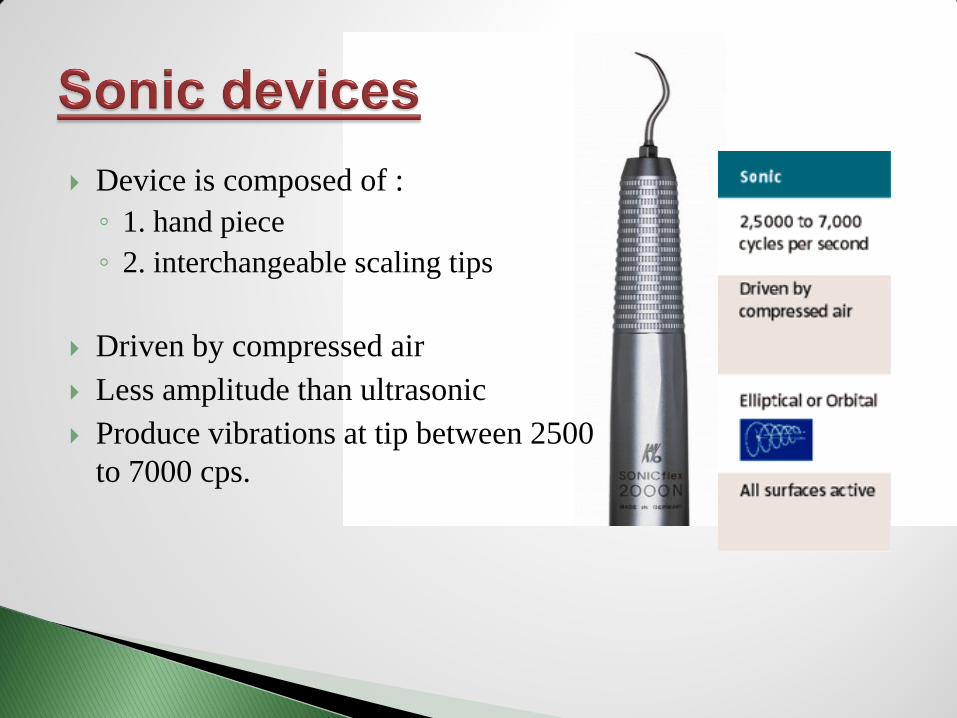
Device is composed of :
◦ 1. hand piece
◦ 2. interchangeable scaling tips
Driven by compressed air
Less amplitude than ultrasonic
Produce vibrations at tip between 2500
to 7000 cps.
Removal of supragingival calculus and tenacious stains.
Subgingival debridement:
◦ Removal of calculus, attached biofilm and endotoxins from
the root surface
◦ Removal of unattached biofilm from the sulcular space
Initial debridement:
◦ For patients of ANUG and other conditions that can be
relieved by removal of deposits
Debridement prior to oral surgery
Removal of orthodontic cement; debonding
Removal of overhanging margins of restorations
Step by step:
1. Pre procedural Antimicrobial rinse (Chlorhexidine gluconate 0.12% oral rinse)
or Listerine
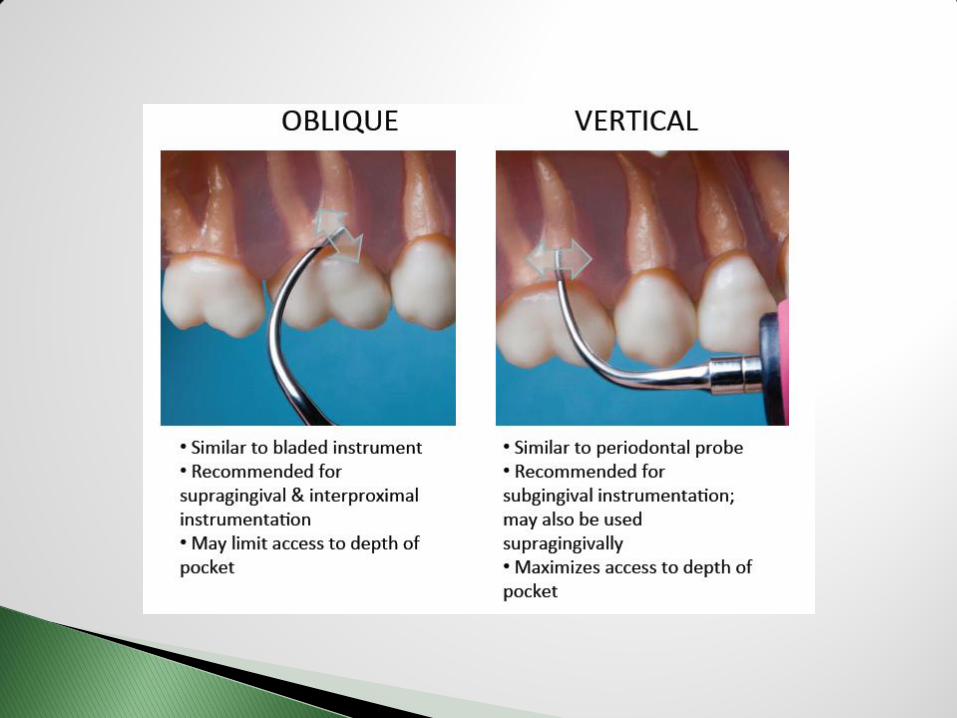
2. Proper positioning of working tip
◦ Use probing depths and radiographs as guides for ultrasonic activation
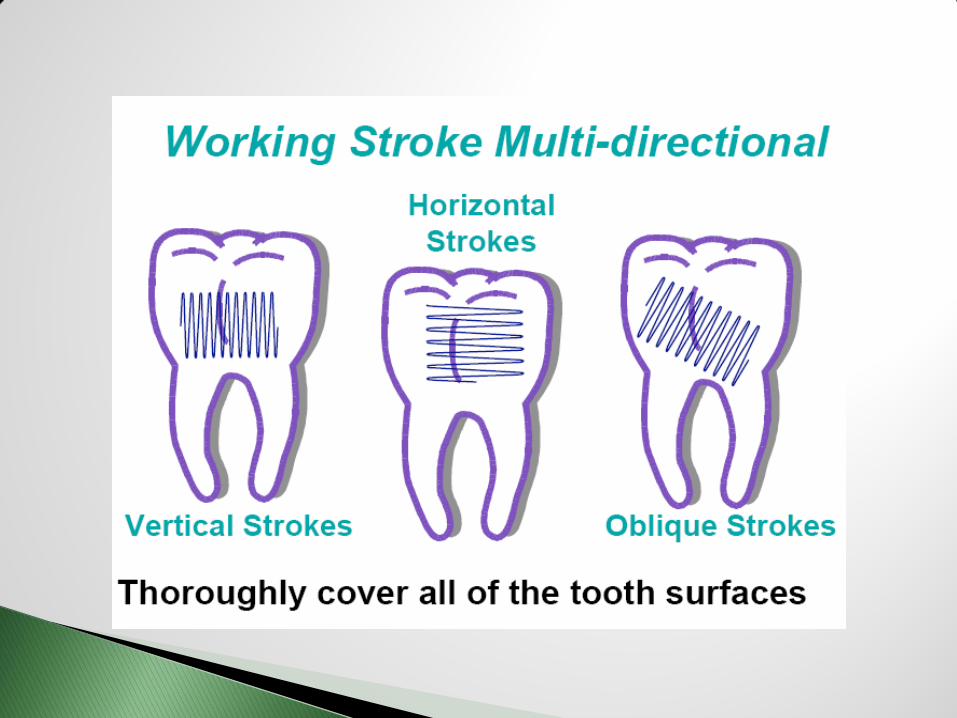
◦ Use “Painting” strokes/Tapping Strokes for large deposits
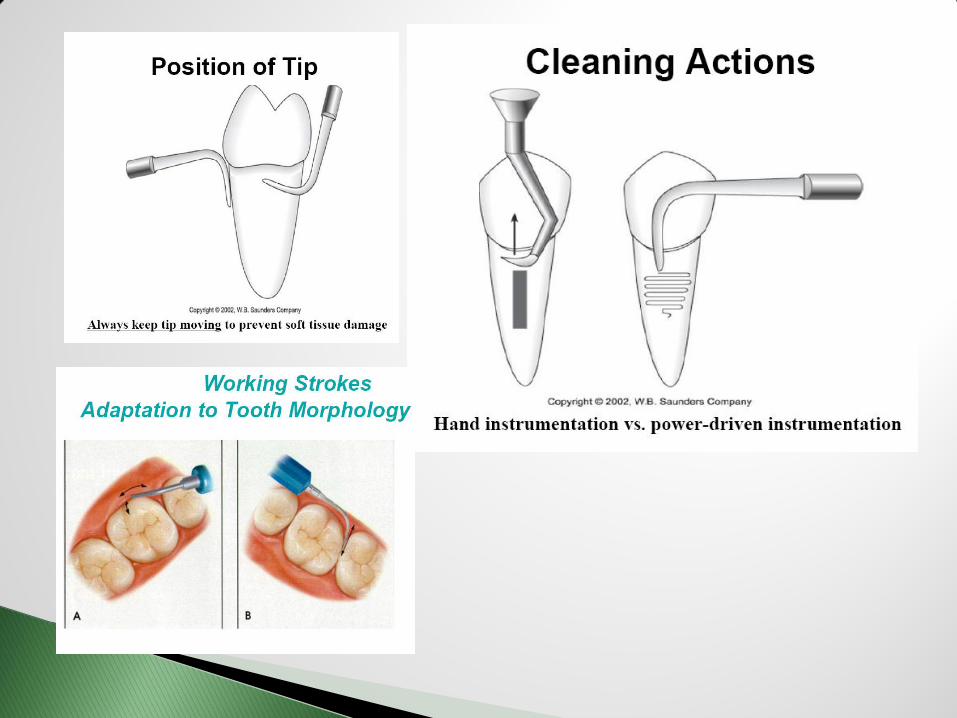
◦ Keep insert moving at all times
◦ Use light lateral pressure
◦ Work from coronal areas apically to root surfaces
◦ Control water - Use saliva ejector to control aerosols
3. Application of desensitizing paste or varnish
4. Selective polishing
5. Flossing
6. Oral Hygiene Instructions
7. Antimicrobial rinse
Efficacy and clinical performance have been evaluated under
following parameters:
Plaque and calculus removal
Bacterial reduction and endotoxin/cementum removal
Leaving smoothest root surface
Reduction in bleeding on probing, probing depth and a gain in a
clinical attachment
Ability to access furcation
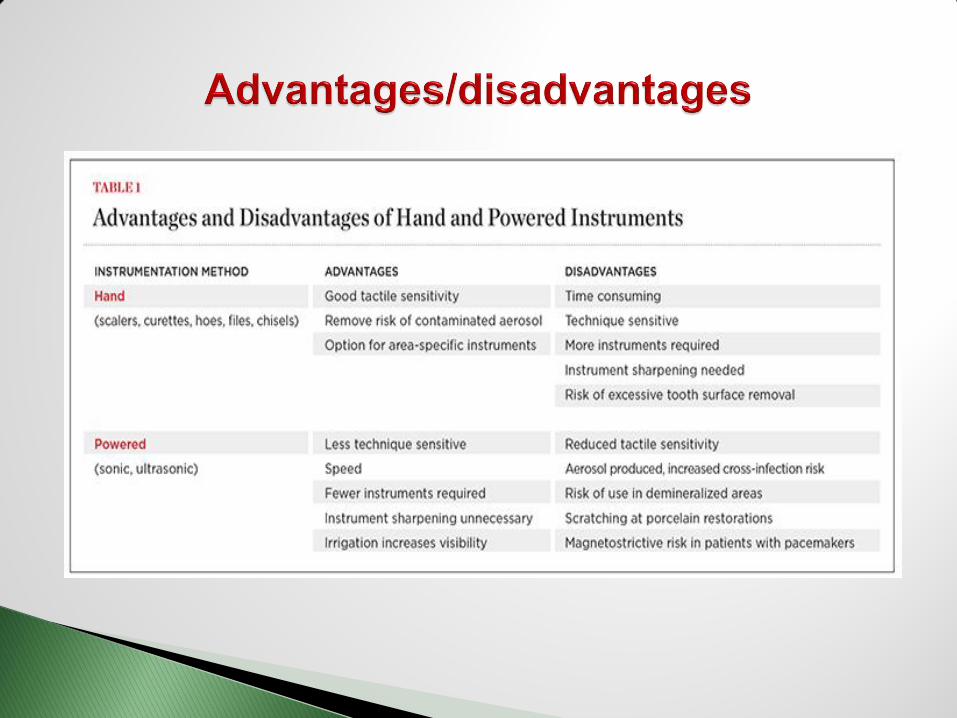
Traditionally, power driven instruments were used to remove
heavy supragingival calculus only.
Garnick and Dent (1989) showed that both hand and ultrasonic
instrumentations removed plaque equally.
Clifford et al. (1996) found no significant difference among traditional and
ultrasonicmini inserts in disrupting apical border of plaque. But
ultrasonicmini inserts disrupts apical plaque border better in pockets
greater than 7 mm.
Busslinger et al. (2001) found that hand and ultrasonic instrumentation
with either a magnatostrictive or a piezoelectric inserts were equally
effective in calculus removal.
According to Ganot et al. (2004) ultrasonic mini inserts were more
effective in apical plaque zone than curettes.
Clinical outcomes for scaling using either a hand or a power scaler are
similar.
Power driven instruments remove plaque, biofilm, bacteria by
mechanical action and activities like cavitation and acoustic
streaming facilitates subgingival bacterial reduction.
O’Leary et al. (1997) found that up to 5 minutes of ultrasonic
activation resulted in significant reduction of
A.actinomycetemcomitans & P.gingivalis
Leon and Vogel (1987) who found that ultrasonic
instrumentation in class II and class III furcations was more
effective than hand scaling
Chlorhexidine as a coolant and lavage – it did not reduce
subgingival pathogens better than water
Most studies found that ultrasonic devices to be effective in
reducing root surface endotoxins.
Smart et al. (1990) & chiew et al. (1991) found that using light
pressure with an ultrasonic instrument effectively removed
endotoxin while conserving the root structure.
Nisimine & O’Leary (1979) found that hand instruments were
more effective than an ultrasonic scaler for this purpose.
Studies have reported mixed results
Ritz et al. (1991) measured tooth substance loss on mandibular
incisors after 12 working strokes over an apicocoronal
distance of 6 mm by an ultrasonic scaler, sonic scaler and hand
instrument.
Results showed ultrasonic scaler removed the least substance,
11.6 μm, versus 93.5 μm for sonic scaler and 108.9 μm for
hand instrument.
both types demonstrates similar outcomes for reduction in
BOP, probing depth and gain in CAL.
Badersten et al. (1998) found both instruments reduce BOP
and pocket depth similarly
Boretti et al. (1995) observed similar gains in CAL with both
the instruments
Researches done by Kocher et al.(2001), and Loos et al.
(1989) found similar results
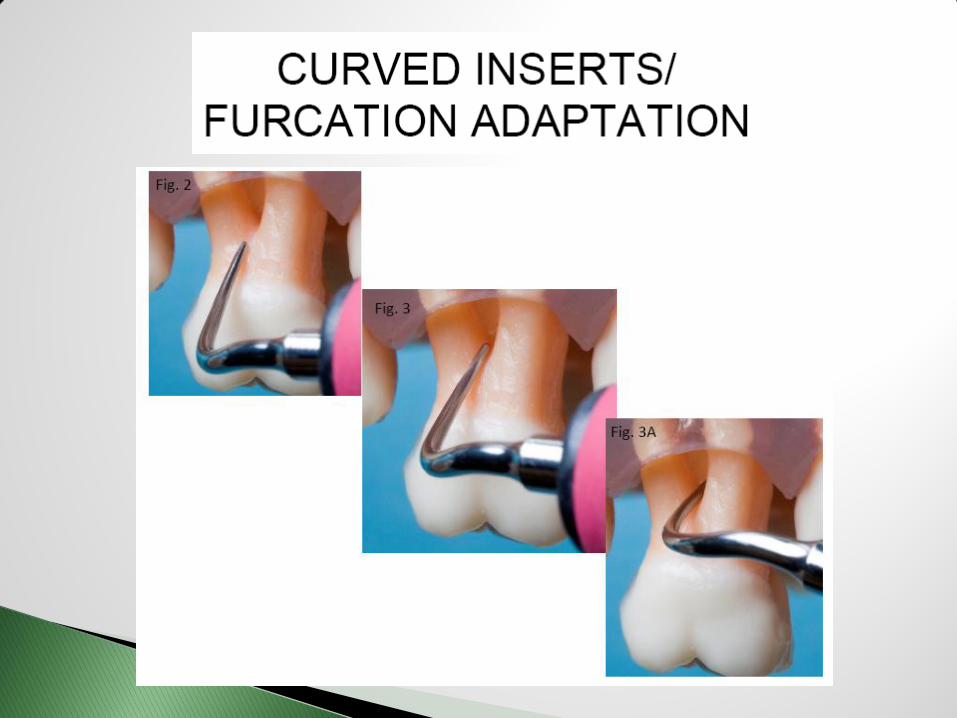
In many cases opening of the furcation is narrower than the
access achievable by the conventional hand instruments
Therefore, power scalers have been recommended as a mean
to improve access when scaling furcation.
Leon et al. (1987) demonstrated that ultrasonic scalers were
equal to hand scalers in reducing the bacteria in class I
furcations but more effective in class II and class III
furcations.
Sugaya et al.(2002) found that ultrasonic tips specifically
designed for furcations were more effective in deriding class II
and III furcations.
Aerosol production contaminated with blood
Neurologic disturbance of the hand caused by vibration
Hearing loss
Interference with cardiac pacemakers
Barnes et al. (1998) Demonstrated aerosol contaminated with
blood produced by the in Vivo use of power scalers.
Universal infection control procedures can help minimize the
amount of aerosol produced.
Harrel and Molinari (2004) recommended three levels of
defence in the reduction of dental aerosols:
1. personal protective barriers such as mask, gloves and
safety glasses
2. routine use of preprocedural antiseptic Rinse
3. use of high speed evacuation device
Miller et al. (1998) found atrial and ventricular pacing was
inhibited by electromagnetic interference produced by a
magnatostrictive ultrasonic scale.
Newer models of cardiac pacemakers have bipolar titanium
insulation that shields the unit from the effects of power
scalers
In general health conditions
1. communicable disease: Patient with a communicable
disease that can be transmitted by aerosols, such as TB.
2. Susceptibility to infection:
◦ Immunosupression from disease or chemotherapy, uncontrolled
diabetes, debilitation, or kidney or other organ transplant
3. Respiratory risk: septic material and microorganisms
from biofilm and pockets can be aspirated into the
lungs
◦ H/O- COPD, asthma or cystic fibrosis
◦ CVD with secondary pulmonary disease or breathing problem
4. swallowing difficulty or patients prone to gagging
5. cardiac pace makers
In oral conditions like,
1. demineralized areas
2. exposed dentinal surface
3. primary and newly erupted permanent teeth have large pulp
chambers, vibrations and heat from the ultrasonic scaler may
damage the pulp tissue
1. damage to integrity of restorations
◦ Porcelain- fracturing, loss of marginal integrity
◦ Amalgam- surface defects
◦ Composite- surface alteration
2. titanium implant abutments
Ultrasonic/sonic and hand instrumentation are both utilized in
initial and supportive periodontal therapy
Clinical studies have shown results (periodontal tissue health)
to be the same following ultrasonic/sonic or hand
instrumentation
The goal of both hand instrumentation and
ultrasonic/sonic instrumentation is debridement to a state
of periodontal health.
So, the key concept is,
◦ A combination of hand Instrumentation and
mechanized instrumentation is probably most effective
clinically and in terms of time management.
1. Esther M. Wilkins, Textbook of clinical practice of the dental hygienist,
10th edition, Wolters-Kluwer health publishers.
2. Newman, Takei, Klokkevold, Carranza’s Textbook of clinical
periodontology, 10th Ed.,Elsevire publication.
3. Current concepts and advances in manual and power-driven
instrumentation, Shigeru Oda, Hiroshi Nitta, Takashi Setoguchi, Yuichi
Izumi & Isao Ishikawa, Periodontology 2000, Vol. 36, 2004, 45–58.
4. www.hu-fridey.com
5. www.dentsplycoinc.com


















