SOME GUIDING PRINCIPLES IN THE EVACUATION OF … · SOME GUIDING PRINCIPLES IN THE EVACUATION OF...
16
SOME GUIDING PRINCIPLES IN THE EVACUATION OF CASUALTIES.' By MAJOR T. J. MITCHELL, D:S.O., D.A.D.G., WAR OFFICE. Royal Army Medical Corps. I PROPOSE to confine my attention to the questions suggested to me by Colonel N eedham, and I have purposely excluded all detail in connexion with organization, as I recall a lecture given by an eminent zoologist, in the course of which he remarked that if he wanted to know the exact number of scales on any fish he could always find it in a text- book. I prefer rather to discuss with you the practical Staff problems that crop up daily, the majority of which are not mentioned in the textbooks. May I remind you that medical officers during times of peace are perhaps more interested in their purely professional work; they do not pass through any Staff College or course in Staff duties; and if by chance they' occupy a Staff app()intment the sympathy and help they receive from the Staff College graduate are both encouraging and instructive. This is especially so on active service, when it would always be a help if the Staff . officer were to explain briefly and simply to the administrative medical officer the details of any operations in which the force is likely to be ,engaged. It was from the Staff College, too, that medical strategical and tactical problems first saw the light of day. Twenty years ago ideas on the . subject were rather chaotic, but fortumitely at that time there was in the Medical Service an enthusiastic officer who had studied the systems of evacuation in continental armies and who had been a British represen- tative in the Russo-Japanese 'Var. I refer to Major-General Sir W. G. Macpherson, who ultimately held the office of Deputy Director-General in France during the Great War, and subsequently was Editor-in-Chief of the official" Medical History of the War." In 1907 he was invited by the Staff College to lecture on the evacuation of casualties, and he was there- fore forced to crystallize his ideas on the subject. These ideas, clothed in official language, became the regulations which guided us during the Great War. As a result of the experience gained in the different campaigns, the Medical Service. has endeavoured to put its house in order; its organiza- tions have been revised; its official Medical History of the War has been published; a revised edition of its Training Manual has been issued; and its regulations have been reviewed and will appear shortly in the new edition of the soldier's Bible, Field Service Regulations. . 1 A lecture delivered to the Staff College, Camberley, on March 27, 1926. Protected by copyright. on August 2, 2021 by guest. http://militaryhealth.bmj.com/ J R Army Med Corps: first published as 10.1136/jramc-47-01-03 on 1 July 1926. Downloaded from
Transcript of SOME GUIDING PRINCIPLES IN THE EVACUATION OF … · SOME GUIDING PRINCIPLES IN THE EVACUATION OF...

SOME GUIDING PRINCIPLES IN THE EVACUATION OF CASUALTIES.'
By MAJOR T. J. MITCHELL, D:S.O., D.A.D.G., WAR OFFICE.
Royal Army Medical Corps.
I PROPOSE to confine my attention to the questions suggested to me by Colonel N eedham, and I have purposely excluded all detail in connexion with organization, as I recall a lecture given by an eminent zoologist, in the course of which he remarked that if he wanted to know the exact number of scales on any fish he could always find it in a textbook. I prefer rather to discuss with you the practical Staff problems that crop up daily, the majority of which are not mentioned in the textbooks.
May I remind you that medical officers during times of peace are perhaps more interested in their purely professional work; they do not pass through any Staff College or course in Staff duties; and if by chance they' occupy a Staff app()intment the sympathy and help they receive from the Staff College graduate are both encouraging and instructive. This is especially so on active service, when it would always be a help if the Staff
. officer were to explain briefly and simply to the administrative medical officer the details of any operations in which the force is likely to be ,engaged.
It was from the Staff College, too, that medical strategical and tactical problems first saw the light of day. Twenty years ago ideas on the
. subject were rather chaotic, but fortumitely at that time there was in the Medical Service an enthusiastic officer who had studied the systems of evacuation in continental armies and who had been a British representative in the Russo-Japanese 'Var. I refer to Major-General Sir W. G. Macpherson, who ultimately held the office of Deputy Director-General in France during the Great War, and subsequently was Editor-in-Chief of the official" Medical History of the War." In 1907 he was invited by the Staff College to lecture on the evacuation of casualties, and he was therefore forced to crystallize his ideas on the subject. These ideas, clothed in official language, became the regulations which guided us during the Great War.
As a result of the experience gained in the different campaigns, the Medical Service. has endeavoured to put its house in order; its organizations have been revised; its official Medical History of the War has been published; a revised edition of its Training Manual has been issued; and its regulations have been reviewed and will appear shortly in the new edition of the soldier's Bible, Field Service Regulations. .
1 A lecture delivered to the Staff College, Camberley, on March 27, 1926.
Protected by copyright.
on August 2, 2021 by guest.
http://militaryhealth.bm
j.com/
J R A
rmy M
ed Corps: first published as 10.1136/jram
c-47-01-03 on 1 July 1926. Dow
nloaded from

'22 Some Guiding Principles in the Evac~[ation of Oasualties
I am asked to commence with a general outline of the Medical Service as it is organized for war at the present time.
GENERAL OUTLINE OF MEDICAL SERVICE.
The responsibilities laid upon the Medical Service of an army in the field comprise :-(1) advice to commanders regarding the maintenance of the health of the troops and the prevention of disease; (2) the collection, treatment and evacuation of the sick and wounded; (3) the administration of medical units;. and (4) the supply and replenishment of medical stores and equipment.
Underlying this service are the principles that to fight well the troops must be fit, and that having fought and become casualties they must have their sufferings alleviated as soon as possible, and be evacuated as quickly and as comfortably as the conditions of warfare permit. Not only can forethought and prevention stay the spread of disease, w,hich in epidemic form can decimate an army more effectively than any human enemy, but a rapid evacuation of· casualties from the battlefield inspires confidence in the men, keeps up their moral and gives the fighting 'force greater mobility. Such a system of evacuation must be complete in every detail and so constituted as to stand the test of war.
Take then a battlefield and watch the progress of the wounded from front to base, and in imagination add to the picture all the difficulties attendant upon modern warfare. During the chaos of battle the regimental stretcher-bearers administer first aid to the wounded and carry them to shelter or to the medical aid post nearest to the firing line. This first' stage in the chain of evacuation is called the Regimental Aid Post. It is generally situated in some position, dug-out or other shelter near unit headquarters, so that the medical officer in charge of the establishment may be kept in constant touch with the trend of events. Here the wounded are sorted out, and those who are able to walk are despatched with or without a guide to the advanced dressing-station (A.D.S.), or to the walking wounded collecting post, if there is one, where they receive medical attention.
The more seriously wounded are conveyed by the bearer personnel of the field ambulance, either by hand stretcher or by wheeled stretcher carrier, from the regimental aid post to the A.D.S., which is formed as far forward as operations allow and with due regard to facilities for road transport. Here these cases have their first field dressings adjusted, and 0
are revived by hot drinks and bodily warmth before being conveyed by the field ambulance road transport to the next stage in their evacuation, the main dressing station (M.D.S.).
Main dressing statIOns are formed by the h~ad'quarters of .the field ambulances, and as they are situated further back, they enjoy a somewhat greater protectIOn and can offer the wounded better accommodation. Only very urgent operations are performed here. Dressings are adjusted,
Protected by copyright.
on August 2, 2021 by guest.
http://militaryhealth.bm
j.com/
J R A
rmy M
ed Corps: first published as 10.1136/jram
c-47-01-03 on 1 July 1926. Dow
nloaded from

T. J. Mitchell 23
and the necessary clerical entries in connexion with the records of admissions are made.
Motor ambulance convoys ply between the M.D.S. and the casualty clearing stations, which form the first hospital link betw~en the front and the base. Casualty clearing stations must have good road communication with the M.D.S. and be within easy access of the ambulance trains at railhead. During the early part of the Great vVar they acted more as distributing centres for the hospitals on the lines of communication and at the base, but subsequently they acted as hospitals, where important operations were performed and skille,d treatment was given to the wounded.
Casualties who require no further active medical treatment and are , likely to recover within a short time are transferred from the C.C.S. to an'
advanced convalescent depot in the particular area, whence after a short period spent in the recuperation of their health and strength they are sent back to duty. Cases requiring further medical treatment are conveyed from the casualty clearing stations to the general hospitals on the lines of communication and at the base.
Many methods of distribution are employed from casualty clearing stations; e.g. :-
,(1) Motor Ambulance Convoy. ,(2) Ambulance Train. (3) River Steamer and Ambulance Barge on inland' waterways and
canals, if the nature of the country permits. From the general hospitals at the base to hospitals out of the area of
operations or overseas, evacuation is effected by ambulance train, hospital carrier, hospital ship or ambulance transport.
Such in outline is the systern of the evacuation of casualties frorn the battlefield. In theory it seerns quite simple. 7'0 be a, success in practice, it requiTes close co-operation and sympathetic understanding between the ~[edical Service and those other services of the Arrny upon which to a veTY large extent it is dependent.
FIELD AMBULANCE.
As it is the disposal of divisional wounded in mobile warfare that specially interests you at present, let us consider the main medical unit in the division, the Field A mbulance. There are three fi€ld ambulances to a
I Division, and one toa Corps, and their role is twofold :(1) To clear the R.A.P. of casualties. (2) To form dressing stations. The field ambulance is organized into: (1) headquarters; (2) two
companies. The headq uarters holds the mo,re elaborate medical and surgical equipment and the bulk of the ordnance equipment as it forms the M.D.S. The companies, which are self· contained in personnel, equipment and transport; form the A.D.Ss. The transport available for the carriage of wounded is as follows :-
Protected by copyright.
on August 2, 2021 by guest.
http://militaryhealth.bm
j.com/
J R A
rmy M
ed Corps: first published as 10.1136/jram
c-47-01-03 on 1 July 1926. Dow
nloaded from

24 Some Guiding Principles m the Evacuation of Casualties
4 heavy horsed-ambulance wagons .. 6 light motor ambulance cars 2 heavy motor ambulance cars!
Total
Carrying cupacity _--- _..-A . __ _
Lying.down Sitting cases cases Mixed cases
16 or 48 or 8 lying and 16 sitting 12 18 8 12
36 78 ! A special type for service use is under consideration at the War Office.
The field ambulances are divisional units and are opened or closed by the A.D.M.S. of the Division. Any change in their situation is notified to the division, brigades and medical units. The A.D.S. is usually situate.d near Brigade Headquarters and the i\'LD.S. in the vicinity of Divisional Headquarters. This is only a rough guide, but I ask you to remember It. Its importance will be discussed later.
If the A.D.M.S. decides to open one A.D.S. only, the second company of the field ,ambulance remains with headquarters at the M.D.S. ready to go forward, either to reinforce the A.D.S., if required, or to relieve it.
Nominally the field ambulance is equipped for 150 patients, the total accommodation therefore for the division being 450, but as you all probably know the field ambulance is. often called upon to deal with gr'eater numbers, and its powers in this direction depend upon the system of el'acuation established.
Casualties retained in a field unit are impedimenta to mobility during an advance and must be evacuated to medical units in the rear of your force. It is only possible to retain casualties in field units :-
(1) During intervals between battles. , (2) During prolonged halts. (3) During quiescent periods of defensive warfare. (4) When the Division is enjoying a co~plete rest from fighting. The neglect or ignorance of this simple elementary principle is well
illustrated in the history of the Mesopotamian campaign. In practically the first battle of the campaign no system of evacuation had been worked out, and at the battle of Sahil the G.O.C.'s orders were: "Sick and wounded will be carried with the force by these medical units." This order was responsible for many subsequent hardships and failures as it initiated a pernicious system which recurred again and :again, e.g., at the first battle of Kut-el-Amara, at Ctesiphon and at Dujaila Redoubt.
In my opening reniarks I gave you an outline of the course of a wounded man from the R.A.P. backwards. Let us examine the methods of evacuation more in detail. Within the divisional area we have two stages: (1) from the R.A.P. to the A.D.S., and (2) from A.D.S. to M.D.S.
In the first stage the 'cases are evacuated by one of four methods:(1) By walking. (2) By stretcher, carried by the bearers from the A.D. S. (3) By wheeled stretcher carrier (six per field ambulance) or by trolly
if a tramline has been laid.
Protected by copyright.
on August 2, 2021 by guest.
http://militaryhealth.bm
j.com/
J R A
rmy M
ed Corps: first published as 10.1136/jram
c-47-01-03 on 1 July 1926. Dow
nloaded from

T. J. Mitchell 25
(4) Occasionally by wheeled transport coming right up to, the R.A.P. Before we can use the last method we must have the decision of the
brigade or division because the use of wheeled transport may draw the attention of the enemy to your positions. .
In the second stage five methods are open to us :-
(1) Horse or motor transport Divisional transport. (2) 'Buses, lorries or empty supply wagons1
(3) Light railway ') Extra divisional (4) Motor ambulance convoys, occasionally transport. (5) Launches and other forms of transport
The broad fact to remember is that divisional transport is ordinarily used for the evacuation of cases back to the M.D.S., but in an emergency,
. or when casualties are heavy and it is essential to free the area, extra divisional and medical transport are sometimes used.
I have already given ,you the transport, horse and motor, that is laid 'down at present in our war equipment tables, but may I quote you a few lines regarding transport from the new F .S.R. that will shortly be published?
"In country where motor tlmbulances cannot be used the, transport provided under orders made by Q.M.G. will whet'ever possible be specially fitted out for the conveyance of sick and wounded."
This is a very necessary regulation, and is the outcome of our lessons in the past war. Front line medical units, mobilized on the official scale, found that when they were sent to a theatre of operations other than the
. western front they had to dump their transport at the base as it was practically useless for the country in which they had to operate. Special transport had to be organized, e.g., travois and litters for the hills of Macedonia; sand-carts, sand-sledges and camel convoys for the deserts of Palestine; carrier companies and light stretchers for the bush of East Africa; local craft, motor launches and river steamers for, the rivers of Mesopotamia; and sledges drawn by men, ponies, reindeer or dbgs for the icebound. wastes of North Russia. These illustrations may impress upon. you the necessity of considering the question of the evacuation of wounded in any foreign country you may be visiting either officially or for sport or pleasure~ ,
CAVALRY FIELD AMBU.LANCE,
Cavalry field ambulances are organized into headquarters and,~ ~ company. The cavalry unit is an organization simIlar to the field ambul-ance of an infantry division, but it is smaller, more compact and built for mobility. You know far better than I do that cavalry move over extensive areas of country, and consequently, if casualties are to be cared 'for, medical 'personnel must be provided with equally fast-moving
1 The adaptation of these for sitting cases is being considered .
• :=;'
Protected by copyright.
on August 2, 2021 by guest.
http://militaryhealth.bm
j.com/
J R A
rmy M
ed Corps: first published as 10.1136/jram
c-47-01-03 on 1 July 1926. Dow
nloaded from

26 Some Guiding Principles in the Evacuation of Casualties
transport to convey them expeditiously to the A.D.S. and to transport the wounded back over great distances. We find, therefore, that in the cavalry unit there are fewer bearers and more transport. The transport laid down is as follows :-
Carrying eapacity
Lying~Ciown cases 4 heavy motor ambulance cars! 6 light motor ambulance cars 6 light horsed-ambulance wagons ..
Total " 1 See footnote p. 24.
16 or 12 12
40 "
Sitting 'cases 32 18 48
98
During the war cavalry field ambulances were almost useless during active cavalry operations. They had not been built for speed; they could not move with their formations, and usually the greater part of the unit was left behind at the divisional dump. I will deal with the question of employing these units when we consider the method of dealing with the wounded in a purely cavalry engagement.
Prior to the war,field ambulances were composed of a headquarters and three sections, A, Band C, and cavalry field ambulances of a headquarters and two sections, A and B. Each section was divided into a bearersubdivision and a tent-subdivisio'n. This was a cumbersome organization and always led to confusion. It was difficult to know what to detail, and that is one reason why we have adopted the nomenclature and organization now in use.
The great point, however, is the inclusion of motor transport and wheeled stretcher carriers. The carrying of wounded is a strenuous duty, ,and men took time and became easily fatigued. It was found more economical in certain areas to use wheeled stretcher-carriers. In the same way horse-drawn ambulances were too slow for the rapid evacuation of wounded. At one time in France in the early days of the war every unit was crying out for motor ambulance cars, and wished to abolish horsed ambulance wagons entirely. It is, I think, a wise decision to retain a certain proportion of horsed transport, because time and again they proved their value in crossing muddy fields or finding their way along shell-pitted roads; and in 1918 when the questions of repairs to M.T. vehicles and the supply of petrol became acute, it was fortunate that there was a reserve of horsed ambulance wagons to save the situation.2
I have now brought you back to the limit of your responsibilities as a divisional staff officer regarding the evacuation of wounded.
, MOTOR AMBULANCE CONVOYS.
The next unit employed in the evacuation of wounded that we wish to consider is the motor ambulance convoy. I ask you to remember
• At one time there were 352 different types of mechanical transport vehicles in France, with 281,000 different kinds of spare parts, none of which were interchangeable.
Protected by copyright.
on August 2, 2021 by guest.
http://militaryhealth.bm
j.com/
J R A
rmy M
ed Corps: first published as 10.1136/jram
c-47-01-03 on 1 July 1926. Dow
nloaded from

T. J. Mitchell 27
that these are not divisiona,l units. They are controlled by the D.M.t:l. but may be loaned to a D.D.M.S. or A.D.M.S.
Prior to the war M.A.C.'s were suggested, but being something· Dew they were merely the subject of criticism aud talk, and ultimately failed to cross the great barrier known as "financial stringency." A compromise was effected, and we started the war with an exc.ellent paper scheme of evacuating the wounded by returning empty supply convoys. During my research among the thousands of papers connected with the preparation of the Official Medical History of the War, I came across a report by Lord Haig on manoouvres in 1913, in which he stated that the evacuation of casualties by this method would lead to failure. He was right, and some of you may remember the cries that came from France in the early days of the war. Still, this Inethod has its uses, as was prove'd in several different theatres of operations.
Motor ambulance convoys are allotted, at the present time, in the pro-! portion of one per corps, with a reserve company at General Headquarters
under the D.G. They are organized into a headquarters and three sections, each section consisting of 25 heavy cars with a carrying capacity of 100 lying-down cases. The sections are usually divided into five groups of five cars each. This organization facilitates the clearing of casualtIes in (1) quiet times; (2) during raids or minor operations; or (3) when a battle is raging. The convoys usually work a definite number of hours when road circuits
,are clear of other transport. At times a commanding officer, imbued with a strict military sense of formation, retains his cars until all are loaded. This is not sound,arid it is advisable to send off each car immediately it is loaded.
The type of car used varies with the nature of the country in which operations are bei~g conducted. In Italy, during the Great War, the Fiat car was most satisfactory for mountain roads, while for the rough tracks of Mesopotarnia and East Africa the Ford car proved most useful.
Motor ambulance convoys are used as follows :-(1) For evacuating casualties from M.D.S. to casualty clearing station. (2) For clearing casualty clearing stations to ambulance train railhead. (3) Occasionally, for clearing casualty clearing stations to hospitals on
the lines of communication when the railways are blocked. (4) Occasionally, in times of stress, for evacuating casualties from
A.D.S. Ambulance car companies (R.A.S.C.) are llormally employed on the
I lines of communication for clearing ambulance trains arriving from the' front and distributing the sick and wounded to the various hospitals, and for conveying patients invalided from hospital to quayside for embarkation.
CASUALTY CLEARING STATIONS.
The casualty clearing station was another unit which in 1914 had never actually stood the test of war. It was the pivot of evacuation. It still .
Protected by copyright.
on August 2, 2021 by guest.
http://militaryhealth.bm
j.com/
J R A
rmy M
ed Corps: first published as 10.1136/jram
c-47-01-03 on 1 July 1926. Dow
nloaded from

28 Some Guiding Principles ~n the Evac~tation of Casualties
remains the pivot' of evacuation, but it serves other equally important functions. Casualty clearing stations are provided on mobilization on the scale of one per division, and they come under the control of the D.M.S. ,of the Army. As already stated; they receive casualties from the M.D.S., and in addition admit the sick from units in the neighbourhood. They are generally situated at railhead, but if the distance between railhead and the fighting troops is too great, then we must' stage the distance by advancing one or more casualty clearing stations. Casualty clearing stations should not be nearer to a railway junction or dump of war stores than 1,000 yards, nor should they be nearer than 500 yards to a railway or waterway used for supplies. They should, however, have their own railway sidings, if possible, especially if there is a group of casualty clearing stations in the vicinity, or they should be connected to the railway either by a special branch line or a light railway.
The functions of a casualty clearing station are fourfold :(1) To evacuate all cases fit to be moved. (2) To retain cases unfit to be moved. (3) To return light cases to duty or send them to a convalescent depot
1Il the neighbourhood. (4) To select operation and gas cases which require rest and quiet for
,as long as possible. These units are provided with first line transport of two three-ton
lorries so that during an advance they can send forward a iight section to , take over, wounded from a M.D.S. and establish an "Advanced Operating Centre."
The complete unit is usually equipped for 20(} serious and 400 light cases; the light or mobile section for 50 serious and 150 light cases. The heavy section is moved by lorry or rail. At the casualty clearing stations are a physician, dental surgeon, radiologist and a surgical team. Surgical teams were specially organized to ~ndertake the more serious operations, and it was found that a maximum of eight could work at one time. These teams were often sent at a moment's notice to different casualty clearing stations receiving the heavy casualties of any special battle.
ORGANIZATION ON LINES OF COMMUNICATION AND A'l' BASE.
I am not going to delay long in describing the organization further back, partly because I am expected to deal more with certain problems of the disposal of wounded in the advance of a division, and partly because the subject is a very big one.
Having got your casualties to the casualty clearing station, they are either treated and sent back to duty, retained as being unfit to be moved, or evacuated to the base. Evacuation to a general hospital is carried out 1Il many ways :-
(1) Ambulance train. (2) Improvised ambulance train.
Protected by copyright.
on August 2, 2021 by guest.
http://militaryhealth.bm
j.com/
J R A
rmy M
ed Corps: first published as 10.1136/jram
c-47-01-03 on 1 July 1926. Dow
nloaded from

T. J. Mitchell
(3) 'I'emporary ambulance train. (4) Barges (in ]'rance and Mesopotamia). (5) River steamers (in Mesopotamia). (6) Motor ambulance convoys.
'29
The ambulance; trains proper are' perfectly equipped in every way for the comfort of casualties alldare designed to accommodate 360 lying-down cases. The questions of equipment and accommodation are at present under review. They are organized on the scale of one per division for a small force and two per three divisions for a large force.
In times of stress improvised and temporary ambulance trains and M .A.C.s are used for the evacuation of sitting cases. On the routes to the base served by these trains rest stations are formed for the purpose of providing the wounded with necessary food and drink.
General hospitals are provided on a ~e.ILper cent basis of the total force in the field, but this is subject to .varHltion and depends on evacuation ,overseas. They are modern hospitals equipped with the latest and best , appliances.
If the line is long they are formed into three groups, as follows ;- . (1) Advanced base area, for cases not likely to be invalided. (2) Main base. (3) Other arreas.
CONVALESOENT DEPOTS.
In close association with the casualty clearing station and the general hospital are the convalescent depots for officers and men who require no
. further active medical treatment and although unfit are likely t'o become fit in a reasonable time.. There are two forms of convalescent depot: (1) advanced convalescent depot; ('2) base convalescent depot. The former relieves the pressure in casualty clearing stations, and the latter in base hospitals.
Convalescent depots present problems which are worth considering, and' If I seem to emphasize their importance it is because they are more or less
. improvised units which canbe made or marred by sympathetic treatment or the lack of it. Personally I am a great believer in them. By the end of the war there were in France sixteen convalescent depots with a total accommodation, including crisis expansion, for over 60,000.
No matter how mechanical the army becomes, men will always be required. The r61e of the medical service is to supply units with fit men, to keep them fit, or to make them fit in the shortest space of time. YOll have heard of financial millionaires before the war. During the war, for the first time in the history of our army, commanders became millionaires in men and medical officers millionaires in casualties. Just as the financier reviews his investments, let us do the same and see whither we are led.
Certain factors influence us when organizing a convalescent depot;
Protected by copyright.
on August 2, 2021 by guest.
http://militaryhealth.bm
j.com/
J R A
rmy M
ed Corps: first published as 10.1136/jram
c-47-01-03 on 1 July 1926. Dow
nloaded from

30 S01ne Guiding Principles in the Evacuation of Oasualties
(1) We of the regular army are accustomed to discipline, but if you mobilize, enlist, and make use of raw recruits in battle, what bappens? The ratio of admissions to hospital for neurasthenia, etc., rises. (2) We know, too, that at intervals we hear the call of pleasure and require some relaxation from boredom and temporary depression, especially when tired, rUll down, or recovering from a slight illness. So it is with the soldier. (3) In peace certain diseases cause the greatest number of admissions to hospital, e.g., venereal disease, combated largely by increasing the esprit de corps of a unit by actively interesting the offiCf~rs in their men through games and, social functions; diseases of the areolar tissue, i.e., slight inflammation of the skin, and skin diseases, reduced by cleanliness. Let us apply this knowledge in constructing our convalescent depots, and let us see discipline and recreation go hand in hand. Let us organize concert halls and parties, bands, athletic sports, and everything that assists us to build up again a healthy manhood and make officers and men fit, bright and keen to return to duty.
Cultivate this convalescent depot spirit in your divisions when they are not actively engaged in operations. It was carried out most successfully by one of our ablest generals in the Far East. His maxim was: "Kill or capture"; his badge a star; and his motto "Sweat and swear, but smile and get on with it." He paid great attention to every detail likely to keep his men fit and healthily occupied with work and recreation, and was not above organizing chicken and dairy farms, vegetable gardens, sports, fishing and baths. Evidently he had had his own ideas on vitamines !
HOSPITAL SHIPS.
I do not propose to say much about Hospital Carriers, Ships, and Ambulance Transports. The first are passenger boats temporarily used for the evacuation of sick and wounded until the second are properly equipped for the purpose. The third convey troops and material overseas and invalids on the return journey. The first two are protected by the Geneva Convention, but the last are not, though serving a most useful purpose and economizing transport.
METHODS OF DEALING WITH WOUNDED IN ADVANCED GUARD ACTION.
You have raised several points in connexion with the employment of the medical units in a division. I ask your indulgence if I start off by raising a point I have never seen noted in a textbook. It is one of those subjects which administrative staff officers do not like to discuss, but it is only by an interchange of ideas during peace that we can have a settled scheme for war. We hear much about co-operation. In practically every lecture I have listened to this subject has been enlarged upon. Well, our medical arrangements depend upon the information we get from the staff. The closer the co-operation the better the results. In most medical
Protected by copyright.
on August 2, 2021 by guest.
http://militaryhealth.bm
j.com/
J R A
rmy M
ed Corps: first published as 10.1136/jram
c-47-01-03 on 1 July 1926. Dow
nloaded from

T. J. Mitchell 31
appreciations of the situation calculations are made as to the number of casualties expected. Now the medical service is only a part of your machinery .. 'rrue, we have built up 'an efficient and special part of. that machinery; but you .are the fighting machine; y~u have the information ;. you know your plans. It is for you to tell us what cas1talties to prepare for and where you expect~them. It is useless for us to have our dressing-stations on the right if you intend attacking on the left. I know you will hesitate. There is the question of secrecy. There is furthermore the effect on the moral of the troops if it becomes known that you expect heavy casualties. You must give us some information or prepare for a breakdown. Surely the history of Gallipoli, Mesopotamia, and East Africa will guide us in settling this question.
Man-power and wastage are important factors in battle. We are out to keep up the moral of the troops by increasing their confidence in the knowledge that wherever they fight, wherever they faIl, they will be collected, treated and evacuated smoothly and quickly. We are out to save your men and return them to you fit and sound, in as short a time as possible.
In front-line work my maxim has always been that if it is possible for your troops to occupy any position, it is usually possible for the medical service to eater for casualties occurring in that position:
Whatever phase of operations you intend pursuing, remember before you start to have the sick and unfit weeded out and evacuated" Wherever you stop or haIt, have your sick attended to and a medical unit open to receive them. Sickness, causes you more wastage than any other factor. At present the daily percentage of sick may be 0'6 per cent of your force. We are working on this subject, and perhaps the following figures, comparing the battle casualties with the admissions for one disease only-viz., malaria-in Macedonia, may stamp this important fact on your memory.
1916 1917 1918
CasualtiesKilled and wounded
4,824 11,072
6,022
21,918
Admissions for malaria 32,~24
71,412 57,775
161,411
The sick rate among the troops is the income and super-tax an army commander pays for conducting operations in certain countries. You can make the rate high or low according to the attention paid to the prevention of disease. '
With an advanced guard you will have a medical unit or unit medical officers with a regimental establishment to form a R.A.P. and to see your sick every morning. This is a regimental post, and its position will be detailed by the regimental commander in consultation with the M.O. concerned. One or two companies of a F.A. will accompany the advanced guard, but please remember that field ambulances are not brigade units, but
Protected by copyright.
on August 2, 2021 by guest.
http://militaryhealth.bm
j.com/
J R A
rmy M
ed Corps: first published as 10.1136/jram
c-47-01-03 on 1 July 1926. Dow
nloaded from

32 Some Guiding Principles in the Evacuation of Oasualties
divisional units, and are detailed not by the brigade-commander, but by the A.D.M. S. The company. or. companies detailed will depend upon your objective, the size of your advanced guard and the information you give. Your object may be surprise. You may not want motor transport. This need not worry you, because motor transport can foliow when the objective is attained. Suppose you come into contact with the enemy, and the troops go into action, a RA.P. is formed. It is the duty of the regimental stretcher-bearers to clear casualties to the RA.P. '1'he F.A. company remains with the advanced guard commander, opens an A.D.S. after consultation with him, informs the RA.P. of its position, and finally clears the casualties from the RA.P. Remember two facts: The regimental stretcher-bearers evacuate casualties to R.A.P.,and the F.A. personnel from R.A.P. to A.D.S.
The clearing of the A.D.S. is a divisional matter. Information as to its position and the number of casualties is sent back to the division or formation.
In an attack on two brigade fronts, with each regiment .there is a M.O. who has certain staff and equipment. As already stated, th.e O.O.'s.of the unit battalions arrange in conjunction with the M.O.'sthe selection of the site for the RA.P., and will give full consideration to the requirements of the RA.P.'s in the allotment of available cover. The site of a RA.P. is notified to all the companies. It should be near regimental headquarters, so that ' the M.O. can get the latest information as to the progress of the fight. It is not advisable to change the location of the RA.P. untIl it can no longer function efficiently.
The A.D.M.S. after consultation with the General Staff would likely open one M.D.S. and two A.D.S.'s, one for each brigade. The position would be notified in operation orders. '1'he A.D.S. would probably be situated near brigade headquarters, and the M.D.S. near the divisional headquarters. This would leave one field ambulance, i.e., one M.D.S. and two A.D.S.'s in nlserve, ready to advance and open in any new positions. Distances between medical posts vary according to the nature of. the country and the trend of battle, but roughly speaking the distance from
i R.A.P. to A.D.S. is two miles, from A.D.S. to M.D.S. three miles, and .~. from M.D.S. to O.O.S. five miles.
The brigade, on receipt of operation orders, would notify their units of the .positions of the A.D.S. and the M.D.S. The regimental M.O.usually, on receipt of this information, gets in touch with the A.D.S. through (1) signals or telephone, (2) runners, or (3) a personal visit. He gives the A.D.S. definit~ information about the position of his RA.P.
The officer commanding the A.D.S. usually makes a tour of the front line, sizing up the possible and best routes for_evacuating the wounded. He may also detail four or more bearers to each RA.P. These. bearers will bring back the first serious cases, and also information as 'to the number of cases in the respective R.A.P.'s. A.D.S. bearers will evacuate the R.A.P. as
Protected by copyright.
on August 2, 2021 by guest.
http://militaryhealth.bm
j.com/
J R A
rmy M
ed Corps: first published as 10.1136/jram
c-47-01-03 on 1 July 1926. Dow
nloaded from

. T. J. Mitchell 33
opportunity offers. Wheeled stretcher carriers or other wheeled transport may be used, but naturally the latter will n'ot be employed without permission, as the dispositions of the units may be indicated to the enemy by the movement of the wheeled' transport. A motor ambulance .is usually kept parked at the A.D.S., ready to take any urgent case, e.g., abdominal wound,direct toM.D.S., or advanced operating centre. The divisional motor ambulance cars clear' the A.D.S. to the M.D.S.
We may consider the situation from three standpoints ;- . (1) If opposition is slight and cases are few, the move forward may be
continuous. Medical posts will then conform to the niovement of" the troops .
• (2) Should there be, however, a moderate number of casualties befotea move forward takes place, the A.D.M.S. might consider that the divisional arrangements, i.e., the F.A. and their transport, were sufficient for evacuating all the cases. In the eventof a move forward he would order the F.A., which are open and receiving casualties, to be closed and
_ evacuat~d, at the same time ordering the F.A. in reserve to proceed with -the advancing troops. In a country where the local population is hostile arrangements have to be made to protect the A.D.S. and M.D.S. until they have been cleared of wounded. This was necessary in several theatres
\
of operations during the Great War. . , (3) Should, however, the casualties be very severe the advance ,might
be held up for a certain time. Extra medical arrangements, possibly already considered,would come into the pictur,e.. These are;-
(a) Divisional arrangements. . (b) Provision of additional stretchers. (c) Use bfM:A.C. as already explained. (d) Use of 'buses, improvised transport, as already explained. With regard to (a) the Field Service Regulations state that it is the
. duty of the A.G.'s branch of the staff to issue orders or instructions for the collection, identification and burial of the dead, and to search for and collect the wounded after a battle. The arrangements made. are as follows ;.-
(1) Provision of extra bearers to the regiment,. supplied by the regiment. .
(2) Organization of an improvised bearer company from a regiment not in action, usually 200 per division. Crocks are of no use; the mell must be healthy and fit.
. (3) Use of prisoners of war, who should not be allowed to pass backwards without carrying some stretcher cases:
_ (4) Organization of a Walking Wounded Collecting Post. This post is -usually formed by a Corps F .A. and its position is notified to all formations. , The wounded are marched back in squads, 'or directed singly, or conveyed in 'buses ,Or . lorries. The. A.P.M. is advised to picquet the· A.D.S. and W.W.C.P; and to collect and return sympathetic helpers to the firing line.
rhe post is organized on the lines of a rest house, i.e., food and 3 . . .
Protected by copyright.
on August 2, 2021 by guest.
http://militaryhealth.bm
j.com/
J R A
rmy M
ed Corps: first published as 10.1136/jram
c-47-01-03 on 1 July 1926. Dow
nloaded from

34 Some Guiding Principles. in the Evacuation oj Oasualties
accommodation are .provideq, and it is also adyisable· to reserve accommodation for men who have walked but ultimately become lying-down cases. Evacuation. from the W.\V.C.P. is carried out by:buses, lorries or trams, except in the case of lying-down casualties for wh<;>m special arrangements must be made.
We have at present a rough method of calculating the different varieties of casualties, and make ouratrangements accordingly :
(i) Slight-returned to duty. (ii) Walking. (iii) Severe-requiring lying-down accommodation. (iv) Killed and missing. - . The proportion of lying~down cases to walking wounded cases for one
division from July 26 to August 11, 1916, during the Somme battles in France, was 1·22 : 1·00; or 54·9 per cent of the total cases admitted were lying-down cases.
The records of one field ambulance for three days during the same period show that 44'2 per cent of admissions were walking cases; 33·9 per cent of admissions were sitting cases; 21·7 per cent of admissions were lying-down cases.
In the first operations for the capture of Gaza in Palflstine, the number of· wounded was 3,022, of whom about 2,000 or 66'6 per cent were slight. 'l'he killed and missing numbered 810, or 21·1 per cent of the total casualties. .,
These figures are approximate, but, as a rough guide, you may take it -that 25 per cent 'of troops are' killed or missing, and of the remaining casualties approximately 40 per cent are walking cases, 35 per cent are sitting cases and 25 per cent are lying-down cases.
With regard to (b) in the earlier stages of all the campaigm, the evacuation of casualties was delayed owing to the want of stretchers~ Stretchers accumulated at the A.D.S., as medical officers would not willingly move a seriously wounded patient from a stretcher. The officer with experience and initiative stored up stretchers, but this did not promote efficiency. The first comprehensive scheme for the supply of stretchers to units in the front line .formed part of the medical arrangements for the Battle of Loos in Septemb'er, 1915. Gradually it was found that 200 per division were sufficient.
A forward dump of stretchers is now organized for all engagements where heavy casualtIes are e~pected.
IN DEFENCE OR RETIREMENT.
The first duty of the regimental medical officer is to get the walking and slightly wounded cases away, as they are likely to become fit to fight again. Lying-down cases are evacuated in any possible way. .
The route of the retirement must be detailed. If the rate of' withdrawal is rapid, it may not be possible for field ambulances to open an A.D.S.
Protected by copyright.
on August 2, 2021 by guest.
http://militaryhealth.bm
j.com/
J R A
rmy M
ed Corps: first published as 10.1136/jram
c-47-01-03 on 1 July 1926. Dow
nloaded from

T. J. },fitchell 35
and M.D.S. and the main problem is to co-ordinate the movement ot all wheeled transport.' A central position near a main road, may be selected as a point fo,r concentrating wounded. All divisional ambulance transport will be used in fr,ont of this fixed point, where M.A.C.'s and all available transport will be stationed to take over cases and convey them direct to a C.C.S. or ambulance train. These points may have to be moved frequently and it is therefore important to keep the officer commanding the post and the M.A.C. informed. If the wounded cannot be evacuated they must be left to the care of the ~ocal inhabitants.
At Dujaila Redoubt the walking wounded were formed into platoons under offi()ers. All transport vehicles were emptied and the stores destroyed, and every vehicle was used for carrying back the wounded~ Casualties occurring in the rearguard were carried either by stretcher-bearers or on limbers.
CASUALTIES IN A PURELY CAVALBY ENGAGEMENT.
We have now come to the last problem, that of the best method of dealing with the wounded in a purely cavalry engagement. A study of the Medical History of the War does not help us to put forward any useful solution of your difficulties. I have already pointed out that the pre-war cavalry field ambulances were of little or no .use except for treating, sick in a stationary camp~ When the cavalry moved out a very small dressing station party accompanied the force. They collected the sick and wounded and passed them by motor ambulance cars to the nearest infantry field ambulance. This frequently happened in Mesopotamia.
In Palestine the C.F.A. retained the serious cases until a C.C. S. came, up and evacuated them; the slight case,s were sent back in ambulance cars and lorries.
We have reorganized our cavalry field ambulance and it is now a compact mobile unit, and our possible mode of attending to casualties in a: cavalry engagement would be to detail a light horsed ambulance wagon to each regiment. The regimental medical officer would then have some method of sending his cases to a collecting point on a main road where an A.D.S. could be established and the cases transferred to a motor vehicle. The O.C. field ambuJance would have to keep in close touch with brigade headquarters and with the regiments.
With our rapidly advancing experience of aeroplanes, one solution of the problem does, however, present itself, and it is a fascinating theme. I mean the use of aeroplane ambulances and aeroplane troop carriers with accommodation for twenty-five sitting cases. Our present Director-General, Sir W. Leishman, is at present specially interested in this method of evacuating cases, and is following all the developments with the closest attention. We know that both types of machines are being used with success in Mesopota:miaand that the French now have a regular service of
, ambulance planes in Morocco.
Protected by copyright.
on August 2, 2021 by guest.
http://militaryhealth.bm
j.com/
J R A
rmy M
ed Corps: first published as 10.1136/jram
c-47-01-03 on 1 July 1926. Dow
nloaded from

36 Some Guiding Principles. m the Evacuation of Oasualties
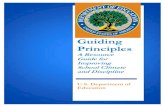
No.I.Sta9~ I. Walkinq 2. StretChers. ~ R. A. P. t ~:;~~~ Stretchers~. T 5. Wheeled Transport. .. ~ ramw~
No.2. Stag!L. . fi) A.D.S. \.' Horse or Motor- Divisional. l.Bus. II 3.Light RailwaY}_E t I/"D' 4.M.A.C. x ra IV.
S.Launches. ~
EA.150 patientstNNo·2\.CCo~" . 0.. >.::J In reserve
3 per Dlv. HdqrS .. ---+\-7-t\--
M.A.C.---( 1-----"\\
Z ,3. 5 of Stage 2.
Barges. } River Steamers.
M.A.C.---,
A. Trains. } I.A.Trains. T.A. Trains.
line
Bus Lorry.
3 Miles.
Division.
5 Miles.
Protected by copyright.
on August 2, 2021 by guest.
http://militaryhealth.bm
j.com/
J R A
rmy M
ed Corps: first published as 10.1136/jram
c-47-01-03 on 1 July 1926. Dow
nloaded from