Some Biochemistry I. Metabolism of the Red Blood Cell A. Glycolysis B. Hexose Monophoshate Shunt II....
42
Some Biochemistry I. Metabolism of the Red Blood Cell A. Glycolysis B. Hexose Monophoshate Shunt II. Heme Synthesis and Degradation III. Anemia A. Hemolytic B. Megaloblastic C. Iron Deficiency
-
Upload
roland-thompson -
Category
Documents
-
view
214 -
download
1
Transcript of Some Biochemistry I. Metabolism of the Red Blood Cell A. Glycolysis B. Hexose Monophoshate Shunt II....

Some Biochemistry
I. Metabolism of the Red Blood Cell
A. Glycolysis
B. Hexose Monophoshate Shunt
II. Heme Synthesis and Degradation
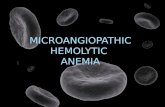
III. Anemia
A. Hemolytic
B. MegaloblasticC. Iron Deficiency

Case 1:Peter T.
History– Back Pain
– Biliary Colic
– Gallstones (bilirubin pigment)
Presenting symptomsMalaise
Palpable spleen
Anemia
Jaundice

Peter T. Laboratory Results
Red Blood Cells, x 1012/L 2.9 (5)
Reticulocytes, % 15 (0.5-1.5)
Hemoglobin, g/dl 8.0 (14-18)
Serum Bilirubin, µmol/L 78 (2-44)
• Serum bilirubin is unconjugated
• Urobilinogen in urine

Bilirubin
UnconjugatedMade in tissues
Insoluble in plasma
Bound to albumin
Elevated in hepatic disease
Elevated with hemolysis
ConjugatedMade in the liver
Soluble
Direct
Elevated in biliary disease

Peter T: Red Blood Cells
• Spherocytes• Osmotic fragility

Osmotic FragilityHarrison’s Figure 108-1

Red Blood Cell Shape
Maintenance of electrolyte gradients– Fine architecture of the membrane– Supply of ATP
ATP
K+
Na+Na+
K+

Peter T: Post splenectomy
• Laboratory Values return to normal
• Patient feels better
Red Blood Cells, x 1012/L 5.4 (5)
Reticulocytes, % 1 (0.5-1.5)
Hemoglobin, g/dl 15.7 (14-18)
Serum Bilirubin, µmol/L 8.5 (2-44)

Case 2: R.P.
History• Malaria• Primaquine prescribed• Black urine• Weakness• Abdominal and back
pain
Presenting Symptoms• Yellow sclerae• Weak• Anorexic• Vomiting

R.P. Laboratory Results
• Serum bilirubin is unconjugated
• Urobilinogen in urine
Red Blood Cells, x 1012/L 3.5 (5)
Reticulocytes, % 12 (0.5-1.5)
Hemoglobin, g/dl 9.2 (14-18)
Serum Bilirubin, µmol/L 340 (2-44)

R.P.: Red Blood Cells
• Contain small dark inclusion bodies
• Polymerized hemoglobin
2Hb-SH +oxidizing agent Hb Hb
S S

Glutathione
• Tripeptide consisting of glutamic acid, cysteine (-SH group) and glycine.
• Protects cells from oxidative damage
• Requires NADPH for conversion from oxidized to reduced form.

Glutathione and NADPH
G S S G 2 G SH
NADPH NADP
2G SH + Hb Hb 2Hb SH + G S S G S S
2G SH +primaquine reduced primaquine + G S S G

R.P.: Ten Days Later
• Urine is normal color• R.P. feels better• Discharged from
hospital
Red Blood Cells, x 1012/L 5 (5)
Reticulocytes, % 4 (0.5-1.5)
Hemoglobin, g/dl 14.5 (14-18)
Serum Bilirubin, µmol/L 23 (2-44)

Case 3: George III
History• Attacks of severe pain,
excited overactivity, paralysis and delirium.
• Began in 1765 (age 27)
• Became frequent by 1788
Presenting symptoms • 1811, violently insane• blind

pedigree

Harrison’s
Fig. 346-1
Heme synthesis

MarksFig. 41.5
Heme synthesis. Marks

Harrison’s Fig. 346-2
Gene

Porphyria Cutanea Tarda

George III

Precipitating Factors
• Drugs
• Increase in Heme Synthesis
• Fasting or low carbohydrate intake

Treatment
• Heme
• Glucose

Case 4: Herbert B.
History• Progressive anorexia• Liquid foods to avoid
abdominal pain
Presenting Symptoms• Loss of weight• Weakness• Shortness of breath• Sore tongue• Difficulty with swallowing• Epigastric pain• Numb, tingling hands• Palpitations

Herbert B.: Laboratory ResultsPatient Normal
Red blood cells, x 1012/l 1.9 5
Gastric secretion
volume, liters per 24 h 0.3 2.5
pH 7.0 1.5
Urine methylmalonate, mgper 24 h
45 <4

Herbert B: Red Blood Cells

B12 and folate
MethionineSynthase
“ folate trap”
Harrison’sFig.107-2

Methylmalonyl CoA mutase
L- Methylmalonyl CoA Succinyl CoAB12
Methylmalonate in urine
From ß-oxidation
To TCA cycleand/or Heme biosynthesis

B12 absorption
Harrison’sFig. 107-1

Herbert B.: Treatment
IM injections of B12 monthly

Herbert B.: Summary
• Loss of weight• Weakness• Shortness of breath• Sore tongue• Difficulty with swallowing• Epigastric pain• Numb, tingling hands• Palpitations

Case 5: Vincent M.
History• Abnormal blood
values• Low dietary intake of
iron
Presenting Symptoms• Short of breath• Difficulty climbing
stairs• Can not work

Vincent M.: Laboratory Results
Hematocrit % 13.5 (47)
Hemoglobin g/dl 5.4 (16)

Vincent M.: Physical Exam
No abdominal mass
Stool and urine are negative for blood

Iron Metabolism
Harrison’s Fig. 105-1

Factors Affecting Iron Absorption
• Positive
– Heme vs. non heme
– MFP factor or meat factor
– pH- reduction of ferric to ferrous iron
– Organic acids-ascorbic, malic and lactic
• Negative
– Phytates
– Polyphenols
– Fiber
– Calcium

Treatment
• Iron supplements
• Nutrition education

Some Biochemistry
I. Metabolism of the Red Blood Cell
A. Glycolysis
B. Hexose Monophoshate Shunt
II. Heme Synthesis and Degradation
III. Anemia
A. Hemolytic
B. MegaloblasticC. Iron Deficiency

MarksFig. 41.7
Bilirubin Metabolism

Normal Blood Smear

Glycolysis
Harrison’sFigure 108-3

Red Blood Cell MembraneHarrison’s Figure 108-2