Sodium 2,3-dimercaptopropane-1-sulfonate challenge test for mercury in humans: II. Urinary mercury,...
11
voL 272, No. 1 Printed in USA ABBREVIATiONS: DMPS, sodium 2,3-dimercaptopropane-1 -sulfonate; SAT, simple reaction time; IMSS, Insituto Mexicano del Seguro Social; HPLC, high-performance liquid chromatography. 264 O022-3565/95/2721-0264$03.OO/0 THE Jouai. o Paaucowoy um Expaswmi. Tissiui’n.mcs Copyright C 1995 by The American Society for Pharmacology and Experimental Therapeutics ,mET 272:264-274, 1995 Sodium 2,3-Dimercaptopropane-1 -Sulfonate Challenge Test for Mercury in Humans: II. Urinary Mercury, Porphyrins and Neurobehavioral Changes of Dental Workers in Monterrey, Mexico1 DIEGO GONZALEZ-RAMIREZ, RICHARD M. MAIORINO, MIGUEL ZUNIGA-CHARLES, ZHAOFA XU, KATHERINE M. HURLBUT, PABLO JUNCO-MUNOZ, MARY M. APOSHIAN, RICHARD C. DART, JOSE HORACIO DIAZ GAMA, DIANA ECHEVERRIA, JAMES S. WOODS and H. VASKEN APOSHIAN Depattment of Pharmacology, Centro de Investigacion Biomedica Del Noreste, Instituto Mexicano Del Seguro Social, Monterrey, Mexico (D.G.R., M.ZC.); Departments of Molecular and Cellular Biology (R.M.M., ZX., M.M.A, H.V.A.) and Pharmacology, University of Arizona, Tucson, Arizona (H.V.A.); Rocky Mountain Poison Center, Denver, Colorado (K.M.H., R.C.D.); Department of Pharmacology, Division Ciencias de Ia S&ud, ITESM, Suc Correso “J” and (P.J.M.) Cuauhtemoc y Famosa Clinic, Monterrey, Mexico (J.H.D.G.); Battelle SeaWe Research Center (D.E., J.S.W.) and Department of Envimnmentei Health, University of Washington, Seattle, Washington (D.E., J.S.W.) Accepted for publication September 6, 1994 ABSTRACT The sodium salt of 2,3-dimercaptopropane-1 -sulfonic acid (DMPS) challenge test (300 mg p.o. after an 1 1 -hr fast) was given in Monterrey, Mexico to dental and nondental personnel. Unne samples were collected and analyzed for total mercury. The mean mercury urinary excretion (± S.E.) for 6 hr before and 6 hr after DMPS administration for 10 dental technicians, who formulate amalgam, was 4.84 p.g ± 0.742 and 424.0 g ± 84.9; for 5 dentists, who use amalgam in their practice, 3.28 pg ± 1 .1 1 and 1 62.0 p,g ± 51 .2; and for 13 nondental personnel, 0.783 L9 ± 0.189 and 27.3 tg ± 3.19. The urinary copropor- phyrin levels before DMPS administration, which are indicative of renal mercury content, were quantitatively associated with the urinary mercury levels among the three study groups after DMPS administration. This was not so if the urinary mercury level before DMPS administration was compared with the un- nary coproporphynin concentration. The urinary mercury level after DMPS administration is a better indicator of exposure and renal mercury burden than is the mercury level measured in the unne before DMPS is given. Regression analysis showed that the coefficient of urinary mercury was statistically and ad- versely associated with complex attention (switching task), the perceptual motor task (symbol-digit substitution), symptoms and mood. The easily performed DMPS-mercury challenge test is useful for monitoring dental personnel for mercury vapor exposure. DMPS has been distributed and used in Europe since 1976. In fact, as stated by Schiele et al. in 1989, DMPS “has been the approved treatment of choice for more than ten years in West Germany and is valued for its negligible side effects.” Its therapeutic uses have been reviewed (Aposhian, 1983; Kemper et al. , 1990; Aposhian et al. , in press, 1995). Phar- macokinetic studies of DMPS, p.o. and i.v., in humans have been performed (Maiorino et al., 1991; Hurlbut et al., 1994) and DMPS has been used to treat humans intoxicated with mercury (Campbell et al. , 1986), arsenic (Gerhard et al., 1992), lead (Chisoim and Thomas, 1985) or other heavy met- Received for publication June 9, 1994. 1 Tk work was supported in part by the Superfund Basic Research Pro- gram, National Institute of Environmental Health Sciences, grant ES-04940 and in part by grant number ES-04696 from the National Institute of Envi- ronmental Health Sciences, National Institutes of Health. ala or metalloids (Aposhian, 1983; Kemper et al. , 1990). The first suggestion for the use of DMPS as a provocative or challenge test for mercury was made by Osinska and Pro- janowska (1981) and in the western world by Cherian et al. (1988). Before this time, DMPS was first made available by the Soviets to American toxicologists working with Iraqi phy- sicians who were treating people who had eaten bread pro- pared from grain seeds that had been treated with a mercu- ry-containing fungicide (Clarkson et al., 1981). Since then, it has been used in humans by physicians in attempts to ap- proximate the body burden of mercury before beginning che- lation “therapy” (Gerhard et al. , 1992; Schiele et al. , 1989). The use ofDMPS to treat bona fide mercury toxicity is well established and accepted (Campbell et al. , 1986; Schiele et al. , 1989). The use of a provocative or challenge test to esti- mate the body content or exposure to a heavy metal is well
-
Upload
mercuryfree -
Category
Documents
-
view
58 -
download
4
description
Gonzalez-Ramirez D, Maiorino RM, Zuniga-Charles M, Xu Z, Hurlbut KM, Junco-Munoz P, Aposhian MM, Dart RC, Diaz Gama JH, Echeverria D. The Journal Of Pharmacology And Experimental Therapeutics 1995; 272 (1): 264-74.
Transcript of Sodium 2,3-dimercaptopropane-1-sulfonate challenge test for mercury in humans: II. Urinary mercury,...

voL 272, No. 1Printed in USA
ABBREVIATiONS: DMPS, sodium 2,3-dimercaptopropane-1 -sulfonate; SAT, simple reaction time; IMSS, Insituto Mexicano del Seguro Social;
HPLC, high-performance liquid chromatography.
264
O022-3565/95/2721-0264$03.OO/0THE Joua�i. o� P�aaucowoy �um Expasw�mi. Tissiui’n.mcsCopyright C 1995 by The American Society for Pharmacology and Experimental Therapeutics,mET 272:264-274, 1995
Sodium 2,3-Dimercaptopropane-1 -Sulfonate Challenge Test forMercury in Humans: II. Urinary Mercury, Porphyrins andNeurobehavioral Changes of Dental Workers in Monterrey,Mexico1
DIEGO GONZALEZ-RAMIREZ, RICHARD M. MAIORINO, MIGUEL ZUNIGA-CHARLES, ZHAOFA XU,KATHERINE M. HURLBUT, PABLO JUNCO-MUNOZ, MARY M. APOSHIAN, RICHARD C. DART,JOSE HORACIO DIAZ GAMA, DIANA ECHEVERRIA, JAMES S. WOODS and H. VASKEN APOSHIAN
Depat�tment of Pharmacology, Centro de Investigacion Biomedica Del Noreste, Instituto Mexicano Del Seguro Social, Monterrey, Mexico(D.G.R., M.ZC.); Departments of Molecular and Cellular Biology (R.M.M., ZX., M.M.A, H.V.A.) and Pharmacology, University of Arizona,Tucson, Arizona (H.V.A.); Rocky Mountain Poison Center, Denver, Colorado (K.M.H., R.C.D.); Department of Pharmacology, Division Cienciasde Ia S&ud, ITESM, Suc Correso “J” and (P.J.M.) Cuauhtemoc y Famosa Clinic, Monterrey, Mexico (J.H.D.G.); Battelle SeaWe ResearchCenter (D.E., J.S.W.) and Department of Envimnmentei Health, University of Washington, Seattle, Washington (D.E., J.S.W.)
Accepted for publication September 6, 1994
ABSTRACT
The sodium salt of 2,3-dimercaptopropane-1 -sulfonic acid(DMPS) challenge test (300 mg p.o. after an 1 1 -hr fast) wasgiven in Monterrey, Mexico to dental and nondental personnel.Unne samples were collected and analyzed for total mercury.The mean mercury urinary excretion (± S.E.) for 6 hr before and6 hr after DMPS administration for 10 dental technicians, whoformulate amalgam, was 4.84 p.g ± 0.742 and 424.0 �g ± 84.9;for 5 dentists, who use amalgam in their practice, 3.28 p�g ±1 .1 1 and 1 62.0 p,g ± 51 .2; and for 13 nondental personnel,0.783 �L9 ± 0.189 and 27.3 �tg ± 3.19. The urinary copropor-phyrin levels before DMPS administration, which are indicativeof renal mercury content, were quantitatively associated withthe urinary mercury levels among the three study groups after
DMPS administration. This was not so if the urinary mercurylevel before DMPS administration was compared with the un-nary coproporphynin concentration. The urinary mercury levelafter DMPS administration is a better indicator of exposure andrenal mercury burden than is the mercury level measured in theunne before DMPS is given. Regression analysis showed thatthe coefficient of urinary mercury was statistically and ad-versely associated with complex attention (switching task), theperceptual motor task (symbol-digit substitution), symptomsand mood. The easily performed DMPS-mercury challenge testis useful for monitoring dental personnel for mercury vaporexposure.
DMPS has been distributed and used in Europe since 1976.In fact, as stated by Schiele et al. in 1989, DMPS “has beenthe approved treatment of choice for more than ten years in
West Germany and is valued for its negligible side effects.”
Its therapeutic uses have been reviewed (Aposhian, 1983;Kemper et al. , 1990; Aposhian et al. , in press, 1995). Phar-macokinetic studies of DMPS, p.o. and i.v., in humans havebeen performed (Maiorino et al., 1991; Hurlbut et al., 1994)and DMPS has been used to treat humans intoxicated withmercury (Campbell et al. , 1986), arsenic (Gerhard et al.,
1992), lead (Chisoim and Thomas, 1985) or other heavy met-
Received for publication June 9, 1994.
1 Tk� work was supported in part by the Superfund Basic Research Pro-
gram, National Institute of Environmental Health Sciences, grant ES-04940and in part by grant number ES-04696 from the National Institute of Envi-ronmental Health Sciences, National Institutes of Health.
ala or metalloids (Aposhian, 1983; Kemper et al. , 1990). Thefirst suggestion for the use of DMPS as a provocative orchallenge test for mercury was made by Osinska and Pro-janowska (1981) and in the western world by Cherian et al.
(1988). Before this time, DMPS was first made available bythe Soviets to American toxicologists working with Iraqi phy-sicians who were treating people who had eaten bread pro-pared from grain seeds that had been treated with a mercu-ry-containing fungicide (Clarkson et al., 1981). Since then, ithas been used in humans by physicians in attempts to ap-
proximate the body burden of mercury before beginning che-lation “therapy” (Gerhard et al. , 1992; Schiele et al. , 1989).
The use ofDMPS to treat bona fide mercury toxicity is wellestablished and accepted (Campbell et al. , 1986; Schiele et
al. , 1989). The use of a provocative or challenge test to esti-mate the body content or exposure to a heavy metal is well

1995 DMPS-Mercury Challenge Test 265
established in medicine. For example, calcium disodiumEDTA has been used as a provocative test for lead for many
years but recently has been CriticiZed (Chisoim, 1987). Therationale and basis for the test is essentially that, over acertain range, the urine and blood concentration oflead with-out calcium disodium EDTA treatment may not be suffi-ciently indicative ofthe body’s lead burden. Although calciumdisodium EDTA mobilizes lead, it is not an effective mobilizerof mercury and is thus useless as a mercury challenge test.
Aposhian et al. (1992) concluded that after p.o. adminis-
tration of 300 mg of DMPS as a challenge test, urinarymercury excretion was increased substantially and that col-lege students with dental amalgams in their mouth excretedapproximately three times more mercury in their urine than
those without amalgams.Urinary porphyrin measurements have been proposed as a
biomarker of mercury exposure (Woods et al. , 1991). Porphy-
rims are formed as intermediates in the biosynthesis of hemein essentially all tissues. In humans and other mammals, fivestructurally distinct porphyrins, characterized by side chainswith four to eight carboxyl groups, are excreted in the urine
in a well established pattern. Prolonged exposure of animalsto mercury as methyl mercury hydroxide produced a changein the urinary porphyrin excretion pattern. There was asmuch as a 30-fold increase ofthose porphyrins with four andfive carboxyl groups (Woods et al. , 1991; Bowers et al. , 1992)plus the excretion ofan atypical porphyrin (“precoproporphy-rin”). The latter is eluted on HPLC between the 4- and5-carboxyl porphyrins. Similar findings have been reported
for human subjects occupationally exposed to mercury vapor(Woods et al., 1991; Bowers et al., 1992). The change in theporphyrin excretion pattern is attributed to Hg� �, which is
produced by the oxidation of Hg#{176}in the body. Hg� � inhibitsporphyrin metabolism at the site of coproporphyrinogen uti-lization and promotes oxidation of reduced porphyrins (por-
phyrinogens) in kidney cortical cells (Woods et al., 1991;Bowers et al., 1992). Changes in porphyrin excretion proffles
are highly correlated with both the dose and time course ofmercury exposure (Woods et al. , 1991). Therefore, urinary
porphyrin levels, specifically those of 4- and 5-carboxyl por-
phyrins and of precoproporphyrin, may be viewed as abioindicator both of mercury exposure and of renal mercurycontent.
The occupational effects of elemental mercury (Hg#{176})expo-
sure on human behavior and mood have long been recognized
(Neal et al., 1941). Recent information concerning dentalamalgams has made mercury exposure thresholds for ad-verse behavior, mood and symptoms of increasing impor-tance in regard to risk assessment and public health. In a1991 national sample of dentists in the United States, theaverage urinary mercury excretion was 5 pg/liter (Naleway etal., 1991). This does not necessarily mean that the mercuryburden of such professionals is within the “normal” range.Small but statistically significant changes as to behavior,mood and symptoms among dentists at mean urinary mer-cury concentrations of36 pg/liter have been reported (Echev-erria et al. , in press, 1995). Four previous dental studies havereported health effects associated with urinary mercury 1ev-els below 50 p.g/liter (Shapiro et al. , 1982; Uzzell and Oler,1986; Ngim et al. , 1992; Echeverria et al. , in press, 1995).Unfortunately, these four studies used diverse epidemiologicmethods with major weaknesses in recruitment of subjects,
definition of acute versus chronic effects, criteria of exposureor reliable dose-effect information. Thus, a threshold effectlevel has yet to be established, although efforts on the part ofseveral researchers have led to proposed biological thresholdlimit values of 25 or 50 p,g/liter of urine (Miller et al. , 1975;World Health Organization Study Group 1991; Roels et al.,1985).
Dental technicians are an excellent population for the
study of threshold effects because they are more homoge-neous than other exposed populations with respect to manual
dexterity, education, training and test-taking ability. Theiruse as the study population of choice in the present studyamplifies the possibilities of detecting subtle subclinical ef-fects of neurobehavior. The present study was expanded toevaluate neurobehavioral performance in 10 mercury-ex-posed dental technicians and 13 unexposed medical techni-cians.
The purpose of the present research was to determinewhether urinary mercury levels of dental workers in a devel-
oping country were within the normal range. Urine samplesof dental workers employed in a modern, new hospital/clinicin Monterrey, Mexico and those of a nondental control groupwere collected under standardized conditions before and upto 6 hr after DMPS administration and analyzed for totalmercury and porphyrins. Finally, to examine the relation-ships between urinary mercury levels and health status,neural behavioral performance was evaluated.
Methods
Clinical. Each subject underwent a history and physical exami-nation; female subjects had a urine pregnancy test performed; and
informed consent was obtained before enrollment in the study. Par-
ticipants were required to refrain from eating seafood for 15 daysbefore DMPS administration. The physical examination was re-peated, vital signs were monitored and blood was obtained for chem-iced analysis (SMAC 20 and complete blood count) immediately be-
fore and 6 hr after DMPS administration. CliniCal laboratory studieswere performed at the Cuauhtemoc y Famosa Clinic, Monterrey,
N.L. Mexico. Subjects were encouraged to void immediately beforeand up to 6 hr after DMPS administration and to drink sufficientwater to maintain a urine output of approximately 500 ml per col-lection period. Informed written consent was obtained. The experi-
mental protocol was approved by the Human Subjects and EthicsCommittees ofthe IMSS and the Human Subjects Committee of theUniversity of Arizona. Because DMPS is an investigational drug in
the United States, the study was performed under the Food andDrug Administration investigational new drug application number
34,682.PrOtOCOL Before DMPS administration, each participant filled
out a consent form, a computerized symptom checklist, a Profile onMood Scale, a brief medical and occupational questionnaire and thebehavioral test battery. Test administrators were blind with respect
to exposure status. Subjects were not informed oftheir mercury leveland test scores until the end of their participation.
For the DMPS mercury challenge test, the subjects were fasted
overnight beginning 11 hr before DMPS administration to 4 hr after
DMPS administration, at which time a turkey sandwich was eaten
(table 1).Urinewascollectedfrom-llto0hrandfrom0to6hr
after administration ofthe chelating agent. (The mercury content ofthe 11-hr urine was determined and then divided by 11 and multi-
plied by 6 to obtain the -6 hr or pre-DMPS urinary mercury value).
Molin et al. (1991) reported a close correlation (r = 0.99) betweenurinary mercury excretion during the first 6 hr after DMPS, and thatduring the 24-hr period after DMPS. DMPS, 300 mg p.o. was given

266 Gonzalez-Ramirez et al
TABLE 1
DMPS challenge test protocol
-1 1 hr Begin fastingBegin overnight urine collection
0 hr End overnight urine collectionCollect blood sampleAdminister 300 mg of DMPS p.o.Begin 0-6-hr urine collection
+4 hr End fast+6 hr End 0-6-hr urine collection
Collect blood sample
and subjects were encouraged to drink sufficient mercury-free waterto maintain a urine output of approximately 500 ml per collection
period. The DMPS dose was chosen on the basis of previous studiesat the University of Arizona (Aposhian et al., 1992; Maiorino et al.,1991) and other clinical reports (Kemper et al., 1990). This dose wasgiven to each subject independent of the body weight because theregimen is a diagnostic test.
Urine was collected in acid-washed 3-liter polyethylene collectors(Baxter, McGaw Park, IL) and the volume was measured in plasticgraduated cylinders. Concentrated HC1 was immediately added togive a final concentration of 1.8%. The acidified urine was trans-ferred to polyethylene bottles, frozen by placement in a dry-ice con-tamer and stored frozen until analyzed. All glassware or plastic warewas soaked in 2% nitric acid at least overnight or was washed with
20% nitric acid. All urine samples were digested, at least, in dupli-cate and three cold vapor atomic absorption determinations were
made on each digest. The amalgam score was determined for eachsubject. It is a measure of the diameters of all the amalgam surfaces
on all the teeth in a subject’s mouth. It has been defined morespecifically and a more detailed determination of it has been de-scribed previously (Aposhian et al. , 1992).
Study design for neurobehavioral testing. Before the DMPSchallenge test, a cross-sectional behavioral evaluation was conductedto assist in the interpretation of the health significance of urinarymercury levels. The primary hypothesis was that mercury-exposedsubjects would demonstrate mild subclinical effects associated with
recent and cumulative body burden of mercury with the urinarymercury values after DMPS administration as the criteria of burden.It is difficult to measure adverse subclinical nervous system effectsbecause of large individual variation in most functions and thenumber of individual factors that may affect these functions. Theprocess of standardization across behavioral studies is still a re-search question but considerable progress has been made in thedesign of such studies, in the use of control measures and in the testmeasures. The present study was designed to be consistent withseveral guiding principles that would maximize the detection ofsmall changes in performance among a small population. First, thestudy population itself provided a high degree of uniformity, whichreduced background noise and amplified the possibility of detectingsubclinical effects. Second, comparisons were made with a carefully
chosen control group that had comparable, but not identical, techni-
cal training. Third, the study relied on previously validated, reliableand well characterized measures of the central nervous system,which were based on previous clinical epidemiologic study results. Toimprove standardization and quality control and reduce potentialinterviewer bias, we chose to use previously validated computerized
tests drawn from the World Health Organization recommended listof tests, which have been translated into Spanish.
Subjects. Thirteen unexposed laboratory technicians and 10 mer-cury-exposed dental technicians were recruited from the IMSS lab-oratory and the participating dental clinic. The five dentists wereomitted from the neurobehavioral analysis because the number whovolunteered was small and the dentists were not comparable insocioeconomic status, education and training with the dental tech-mcians or the nondental controls.
Vol. 272
Symptom, medical and work history questionnaires. The
symptom questionnaire included measures of physiologic, psycho-logic and somatic symptoms that have been reported after acute andchronic exposures. It was based in part on the Swedish “Question-naire 16” (Hogstedt et al., 1985) and questionnaires used in previouscentral nervous system studies of mercury (Albers et al., 1988; Kal-lenbach 1988), organic solvents (Echeverria et al., in press, 1995) and
lead (Baker et al., 1984).
One component of the questionnaire evaluated conditions thatmight influence test performance. The variables ofinterest includedage; race; gender; education; eyeglass wear; income; and medical
history of neurologic disorders, hypertension, diabetes and use ofmedications. Questions regarding personal habits included a de-
tailed history ofthe use ofalcohol, caffeine and nicotine and chemicalexposures received from hobbies.
This information supplemented an occupational history and workpractice questionnaire that covered sources of mercury exposure
such as the number of operatories in one clinic; the number ofamalgam placements, removals and spills per week; the number of
amalgams each subject had in his or her mouth; and consumption ofseafood.
Mood and vocabulary. An evaluation of mood (Proffle of MoodStates; McNair et al., 1971) was included because such effects have
been consistently reported in workers with mercury concentrationsbetween 30 and 100 �gIliter ofurine (Roels et at., 1985; Fawer et al.,1983; Zedda et al., 1980; Piikivi et al., 1984; Soleo et al, 1990).
Behavioral test battery. These tests of digit-span (Smith et al.,1983), symbol-digit substitution (Baker et al., 1985), simple reactiontime (Baker et al., 1985), the ability to switch between tasks (Tou-tonghi et al., 1991) and verbal ability (Baker et al., 1985) were based
on previous results found among mercury-, lead- and solvent-ex-posed cohorts. To assess potential deficits in manual dexterity, theone-hole test (Salvendy 1975), a validated manual dexterity task, animprovement on the traditional Purdue peg board test, was selected.This test independently assesses component tasks such as the time ittakes to grasp, move, position and reach while transferring small
pins from a large target to a small target hole. The test has been
found to be sensitive to other neurotoxicants such as toluene and
ethanol (Echeverria et al., 1991) and in previously exposed mercury
workers (Echeverria et al. , in press, 1995). Tremor was not includedbecause of the short test development time.
Data analysis. Multivariate regression (SAS-PC, SAS Institute,
Cary, NC) techniques were used to test the hypotheses that recentand chronic measures of mercury exposure were associated with
adverse changes in symptoms, mood and behavioral function. Allcontinuous variables used in the analysis were graphically reviewed(AXUM technical graphics and data analysis, Timetrik, Seattle, WA)to evaluate their approximation to a normal distribution. Variableswith poor approximations of a normal distribution or with extremevalues that might dominate the analysis were log transformed. Re-cent exposure was evaluated in a continuous dose-effect manner withthe use of the concentration of mercury in the urine. The chronicindex was also evaluated as a continuous variable. A P value of < .1was considered marginally associated and a P value of < .05 wasconsidered statistically significant. Age in years, race, gender, in-come, use of eyeglasses, alcohol consumption (a five-level scale basedon frequency of drinking per week), vocabulary scores, medications,a medical history of neurologic importance and use of nitrous oxidewere each evaluated as potential confounders. Only the most impor-
tant confounders were retained in the final analysis because of thesmall number of subjects.
For analysis of mercury excretion and porphyrin excretion, single
factor analysis of variance or Student’s t test was used to determinesignificant differences. A confidence interval of 95% was consideredto be statistically significant (P � .05). Linear regression analyseswere performed with a general purpose statistics package acquiredfrom Microsoft, Inc.

1995 DMPS-M.rcury Challenge Test 267
Analytical procedures. The urinary mercury levels were deter-mined by cold vapor generation-atomic absorption procedures, aspreviously described (Aposhian et al., 1992). The procedure wasagain validated immediately before doing the present assays byanalyzing freshly voided urine from a normal individual to whichmercury nitrate had been added to final concentrations ofO.50, 5.0 or30.0 ng/ml, in duplicate, according to the procedure described byAposhian et ci. (1992). After a correction for the mercury content ofthe urine before the spike was added, six determinations ofthe 30.0ag/nil of Hg gave a mean of 29.9 ng/ml of Hg (range, 29.8-30.0), sixdeterminations ofthe 5.00 ng/ml of Hg gave a mean of 4.52 ag/mi ofHg (range, 4.51-4.53) and six determinations of the 0.500 ng/ml ofHg gave a mean of 0.418 ag/mi of Hg (range, 0.382-0.454). Themercury content of urine samples was analyzed both at the Univer-sity of Arizona in Tucson and the IMSS Biomedical Research labo-
ratories in Monterrey, Mexico.
Urinary porphyrin analysis, Urine was collected and acidifiedas described previously and then a 35-nil aliquot was dispensed into
50-tul polypropylene bottles, frozen and sent to Seattle by overnightexpress delivery service. Porphyrin analysis was performed on a10-mi aliquot, as previously described (Woods et al., 1991; Bowers etal., 1992). Briefly, the acidified urine was applied to a C-18 solid-phase extraction column (Waters Associates, Milford, MA) and
washed with a 35% methanol and 65% sodium phosphate buffer, pH3.5, to remove interfering substances (Bowers et a!., 1992). Porphy-
Tins were eluted with 100% methanol; the methanol was then evap-orated and the samples were reconstituted in 0.5 ml of 1 N HC1.Porphyrins were separated and quantified by HPLC with a WatersHPLC system that was equipped with an Econosphere (Alltech/Applied Science, Deerfield, IL) C-18 column. Sodium phosphate (50mM, pH 3.5) was used as the starting mobile phase and individual
porphyrin congeners were eluted with a linear gradient of increasingmethanol concentration. Porphyrins were measured by their fluores-
cence intensity (excitation wavelength, 395 am; emission wave-length, 620 am) with a Shimadzu (Columbia, MD) RF-535 detector.
Porphyrin identification and concentrations were determined bycomparison with a standard curve of authentic porphyrin isomers
(Porphyrin Products, Logan, UT).
Results
Study population. The subjects were 5 dentists (1 female
and 4 males; age range, 26-34 years; mean, 30.2 years); 10female dental technicians (age range, 17-27 years; mean,20.2 years) whose duties included the formulation of amal-gam; and 13 nondental personnel (5 females and 8 males; agerange, 23-51 years; mean, 36.4 years). All dental personnelwere employed in a dental clinic in Monterrey, Mexico androutinely worked with amalgam. The dental clinic is part ofa hospital built by a progressive company to provide im-proved medical and dental care for its employees. The build-ing was less than 5 years old at the time this study began and
has excellent modern medical and dental facilities. The den-tal clinic has four exsimining rooms and one very small win-dowless preparation room. It is in the latter that a dentaltechnician prepares dental amalgam as needed. To do this,the technician removes metallic mercury from a bottle andplaces it on a small piece of white filter paper and then addsto it a portion of alloy powder. The technician then carriesthis to the dentist in the examining room who squeezes theexcess mercury with his or her hands through the ifiter paperand uses the amalgam to complete the restoration. This
method of amalgam preparation was used in the United
States about 20 years ago. It has been replaced in the UnitedStates by capsules that contain amalgam.
The control, nondental subjects were employed at the Cen-tro de Investigacion Biomedica Del Noreste, IMSS, inMonterrey. Dentistry is not practiced at this IMSS facility
and research using mercury is nil. The alcohol consumptionof this population was small. More than 65% of the subjectsdrank alcohol less than once per month (table 2).
Clinical. Three subjects had mild headaches, one feltweak and one felt somewhat lightheaded, all of which effectswere thought to be related to the prolonged fast. Two subjectsfelt nauseous and two others reported symptoms of reflux
and belching. These symptoms may have been attributable to
DMPS or to the carbonated water the subjects consumed.One subject reported nausea and two episodes of diarrhea;
his symptoms were thought to be drug related. No otheradverse signs developed. Slight differences in several bloodlevels were observed before and after DMPS administration,
without accompanying clinical effects (table 3).Urinary excretion of mercury. The administration of
the DMPS challenge to dental technicians, dentists and non-dental personnel resulted in an 88-fold (range, 11-335), 49-fold (range, 45-76) and 35-fold (range, 14-132) increase, re-spectively, in the mean 6-hr urinary excretion of mercury
compared with that during the 6-hr period before the admin-istration of this chelating agent (table 4). These increases
were statistically highly significant (table 4). The mean urn-nary mercury excretion before DMPS administration for thedental technician group and dentists was 6 times and 4 timesgreater, respectively, than that of the nondental controls.After DMPS administration, however, the mean urinary
mercury for the dental technician group and dentists was 15times and 6 times greater, respectively, than that of thenondental controls.
Because toxicologists are usually more concerned with con-
centrations, the level in micrograms of mercury per liter ofurine was also calculated (table 4). The urinary mercuryconcentration also showed a substantial (at least 12-fold)increase after DMPS administration. In addition, such dataindicate that the difference in urinary concentrations of mer-cury is not as marked as the difference in absolute amountsthat were excreted during the 6-hr period after DMPS.
Was there a strong positive correlation between the meanurinary mercury level before and after DMPS administra-
TABLE 2A comparison of demographic factors associated with mdlcaltechnicians occupationally unexposed and dental technIciansoccupatIonally exposed to mercuryValues are mean ± S.D.
Unexposed Exposed
Numberofsubjects 13 10Age(yr) 35±8 22±8Male 8 0Income (new pesos)
<10,000 11 7<20,000 2 2<30,000 1
Without glasses 5 7Alcoholic dnnks/wk 3 0Frequency
1-2days 4<1/wk 1<1/mon 8 10
Medication user 3 1Vocabulary scores 18 ± 3 16 ± 3

�t300
Ca 200
%iso
�100
012345678�tg URINARY Hg; -6 TO 0 HR BEFOREDUPS
0 2 4 6 8 10I.Lg URINARY Hg; -6TO 0 HR BEFORE DMPS
268 Gonzalez-Ramlrez et al Vol. 272
TABLE 3Changes in blood chemistries after DMPS adminIstrationThe paired t test was used.
Before DMPS (mean ± SE.) After DMPS (Mean ± SE.) Percent Change P Value
Leukocyte count (x106/mm�) 7.6 ± 0.4 8.5 ± 0.4 +12 .0005Potassium (mEq/liter) 4.3 ± 0.1 3.9 ± 0.1 -1 1 <.005Direct bilirubin (mg/dl) 0.03 ± 0.01 0.05 ± 0.01 +67 <.005Phosphorus (mg/dl) 3.2 ± 0.1 3.5 ± 0.1 +9 <.005Triglycerides (mg/do 101.0 ± 16.0 112.0 ± 16.0 +11 <.05
TABLE 4UrInary mercury level before and after DMPS challenge testP values determined by single-factor analysis of variance. For u�nary Hg before and after treatment, P < .001 for the dental technicians, P < .015 for the dentists andP < .001 for the nondental personnel. For -6 to 0 hr, dental technicians vs. nondental, P < .001 ; dentists vs. nondental, P < .005; dental technicians vs. dentists, P= .252; ForO to +6hr, dental technicians vs. nondental, P < .001; dentists vs. nondental, P < .001; dental technicians vs. dentists, P = .0597.
Group nMercu ry level ± SE. Mercury Concentratlon ± S.E.
-6 to 0 hr (before) 0 to +6 hr (after) -6 to 0 hr (before) 0 to +6 hr (after)
�Lg �g/1iter
Dental techniciansDentistsNondental
105
13
4.84 ± 0.7423.28 ± 1 .1 1
0.783 ± 0.189
424.0 ± 84.9162.0 ± 51 .2
27.3 ± 3.19
29.7 ± 6.7319.8 ± 7.193.00 ± 0.620
481 .0 ± 121.0275.0 ± 107.0
37.2 ± 15.1
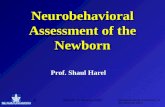
tion? Although there was a strong positive correlation for theurinary mercury levels ofthe dentists before and after DMPS
administration (r = 0.996, fig. 1), this was not the case for the
dental technicians (r = 0.051) or for the nondental controls (r= 0.473). Although there was a high correlation in the case of
the dentists and a poor correlation for the dental technicians,
�12oo. (B)DENTALTE�HS
�Iooo U
�8oo
(0
g600 UU Ur = 0.0512
a��400-� U
�200 U U U
U
a 0 -
�. 0 2 4 6 8 10�tg URINARY Hg; -6T00 HR BEFORE DMPS
wI:
=Ca
ga
=
z:� � 0.5 1.0 1.5 2.0 2.5 3.0
P1 URINARY Hg; -6 TO 0 HR BEFORE DMPS
Fig. I . There was a strong positive cor-relation between urinary mercury levelbefore and after DMPS administrationfor the dentists but not for the dentaltechnicians and controls.

1995 DMPS-Mercury Challenge Test 269
we cannot explain this. It is possible that the results with thedentists might be different ifthere had been a larger number
of them.Urinary porphyrin excretion. In the present studies,
urinary porphyrin concentrations were measured for two rea-sons. First, we wanted to see whether they correlated posi-tively with the burden ofmercury, as indicated with or with-out the DMPS challenge test, for subjects occupationallyexposed to mercury vapor. Second, we wanted to determinewhether the concentrations ofurinary porphyrins were also ameasure of the efficacy of DMPS in promoting mercury ex-cretion from the kidney.
Correlations were examined between urinary coproporphy-
rin and urinary total mercury among the three groups ofstudy subjects before or after DMPS challenge (table 5).Linear-regression correlation analyses were performed to
compare different parameters of urinary mercury and uri-nary porphyrins such as concentration (in micrograms per
liter), amount (micrograms), nanograms per milligram ofcreatinine and pre- (before DMPS) and postadministration(after DMPS). The best correlations were obtained when theurinary coproporphyrin concentration (in micrograms per II-tar) before DMPS was compared with the urinary total mer-cury amount (in micrograms) after DMPS (dental technician,r = 0.921; dentists, r = 0.667; nondental personnel, r =
-0.642). There was insufficient data on pentacarboxylpor-
phyrin and coproporphyrin levels to do linear-regression cor-relation analyses. Changes in the urinary porphyrin levelswere examined among the three groups before and after theDMPS challenge (table 6). After DMPS administration (table6), there was a decline in the urinary concentrations of eachporphyrin compared with the pre-DMPS levels except for theprecoproporphyrms ofthe nondental controls. Although mostof these declines were not statistically significant (P > .05),perhaps because of the wide variability in porphyrin excre-
tion rates and the relatively small number ofsubjects in eachgroup, the trend was consistent. Coproporphyrin had themost substantial decline in this respect, decreasing to 66%,68% and 48% of the before-DMPS values among the dentaltechnicians, dentists and nondental controls, respectively.This suggests substantial depletion of renal mercury afterDMPS treatment.
TABLE 5
Associations between behavior, mood, symptoms
and post-DMPS mercury levels. The associations between
urinary mercury levels and health outcomes are described intables 7 and 8. The urinary excretion of mercury both before
and after DMPS administration was associated with adverseeffects but the calculated index of cumulative mercury expo-sure based on work histories alone was collinear with age and
was not useful as an indicator of potential adverse effects.Based on the urinary excretion of mercury after the DMPS
challenge, multiple-regression analyses found that the time
to match symbols with digits (digit-symbol substitution) andthe time to switch between tasks (the switching task) wereincreased and thus adversely affected by exposure to mer-cury (table 7). The simpler attention task, which calculated a
subject’s digit span, decreased in the expected direction byone-third ofa digit but did not achieve statistical significance
(table 7). Thus, between the two attention tests, the morecomplex task was affected by exposure. The two tests with astrong manual motor component, SRT and the one-hole test,were not significantly affected by mercury exposure eventhough the SRT response time increased by 46 msec in theexpected direction.
All the mood scales (table 8) deteriorated with exposure
but only the differences in scales for tension, anger andconfusion were statistical significant. Reported symptoms
related to increased headaches, increased emotionality, poor
comprehension and poor coordination were also associatedwith increased urinary mercury excretion.
Discussion
There are a number of results of the present investigationthat warrant discussion, namely DMPS-Hg challenge test,urinary porphyrins and neurobehavioral testing.
First, the DMPS-Hg challenge test indicated that the body
stores of mercury are larger in dental personnel in a moderndental clinic in Monterrey, Mexico than in nondental person-nel who have not been occupationally exposed to mercury(table 4). At the occupational level, elemental mercury vaporis the main form of mercury exposure. Skerfving (1991)stated that the largest group of such workers are dentalprofessionals but that, in Sweden, their exposure is low, with
Unear-rgression correlation (r) analysis of urinary mercury and coproporphyrin
Coproporphyrin Total HgDental Technicians
r
Dentists
r
Nondental
r
p9/liter (pre) �L9 (post) 0.921 0.667 -0.642
Mg/liter (pre) p.9 (post - pre) 0.921 0.666 -0.642�g/lfter (pre) �Lg/liter (post) 0.977 0.0281 -0.716Mg/liter (pre) �L9/l�Iter (post - pre) 0.981 0.00728 -0.710,A9 (pre) ,.i.9 (post) 0.464 0.427 -0.333�L9 (pre) g.�g/liter (post) 0.391 -0.256 -0.378ng/mg of creatinine (pre) ng/mg of creatinine (post) -0.350 0.164 -0.573�.�g/liter (pre) �L9 (pre) 0.152 0.706 -0.250pg/liter (post) ,.L9 (post) 0.366 0.636 -0.220�Lg/liter (pre) p.giliter (pre) -0.0304 0.296 0.191IL9/liter (post) p.g/Ilter (post) 0.338 0.912 0.0904p9 (pre) p9 (pre) 0.376 0.474 0.01 51�L9 (post) IL9 (post) 0.291 0.441 -0.147�L9 (pre) �&g/liter (pre) -0.479 0.0106 -0.2781�g (post) p.g/liter (post) 0.203 0.00222 0.0783ng/mg of creatinine (pre) ng/mg of creatinine (pre) 0.175 -0.1 18 0.212ng/mg of creatinine (post) ng/mg of creatinine (post) 0.61 1 -0.800 -0.228

270 Gonzalez-Ramirez at al. Vol. 272
TABLE 6Changes in urinary porphyrin lsv&s among dental and nondental Personnel before and after DMPS challenge testEach value is the mean ± S.E. The number of subjects used for the porphyrin determInations was Ieee than those used In the Hg studies because insufficient volumesof urine were saved for that purpose.
Pentacarboxylporphyrin Precoproporphyrin CoproporphyrinGroup (n)
Before After Before After Before After
p4IlItSf
Dental Technicians (7) 2.1 ± 1.2 1.4 ± 0.9 1.0 ± 0.5 0.5 ± 0.5 38.5 ± 10.5 25.3 ± 9.7Dentists (4) 2.5 ± 1 .3 2.3 ± 1 .4 1 .5 ± 0.4 0.3 ± 0.3 70.7 ± 25.5 47.8 ± 8.2*NOndental (8) 3.2 ± I .0 1.9 ± 0.9 0.6 ± 0.3 0.6 ± 0.4 29.3 ± 8.0 14.0 ± 3.0
* Signfflcantty different from value before DMPS administratIon, P < .05.
TABLE 7
BehavIoral test results and P values based on the coefficient for urinary mercury level after DMPS with the regression analysiscontrollIng for age, ethanol consumption, .ysgiass wear and vocabulary
Mean Values ± S.D. U�nary Mercuryafter OMPS
Unexposed Exposed P Value
Symbol-digit substitution response time (eec)Unadjusted 19.7 ± 3.2 21 .2 ± 4.2Adjusted 19.7 ± 2.3 21.2 ± 3.6 .00
The switching task (msec)Unadjusted 1 1 755 ± 135 830 ± 266Adjusted 1 1 756 ± 108 830 ± 253 .06Unadjustedl2 678±136 817±258Adjusted 12 678 ± 109 818 ± 252 .01Unadjusted 13 626 ± 136 709 ± 236Adjusted 13 626 ± I 18 709 ± 202 .04Unadjusted 21 619 ± 141 704 ± 279Adjusted 21 619 ± I 15 704 ± 241 .02Unadjusted 22 636 ± 105 768 ± 263Adjusted 22 636 ± 090 768 ± 226 .01Unadjusted 23 531 ± 127 622 ± 222Adjusted 23 531 ± 089 622 ± 205 .03
The one-hole testPin/mm
Unadjusted 38 ± 5 39 ± 5Adjusted 38±3 39±3 a
Reach ± msecUnadjusted 323 ± 55 320 ± 71Adjusted 323 ± 38 328 ± 57 .02
Digit spanUnadjusted 5.9 ± .9 5.6 ± .8Adjusted 5.9 ± .4 5.6 ± .6
sm- ±Right
Unadjusted 41 1 ± 71 467 ± 81Adjusted 41 1 ± 30 467 ± 77
LeftUnadjusted 414 ± 60 452 ± 84Adjusted 414 ± 40 452 ± 21
a The exposed group performed better than the unexposed group.
their urinary mercury level only marginally higher than thatof nonoccupationally exposed controls. This appears to betrue in the United States, also, where a divided capsule, onepart ofwhich contains elemental mercury and the other part
of which contains the alloy powder is commonly used toprepare amalgam. The capsule is shaken vigorously to break
the divider and form the amalgam. Such a device and procedure
for preparing amalgam is designed to minimize exposure of
dental personnel to mercury vapor but is not commonly used in
many developing countries for economic reasons. In Mexico, it isestimated that less than 1% of dentists use the amalgam cap-sules in their practice. In addition, Occupational Safety andHealth Administration standards are not necessarily enforced
in many developing countries.
It is of interest not only to compare the changes in theurinary mercury concentration after the DMPS challenge butalso to compare the urinary mercury level ofthe three groupsbefore treatment (table 4). The differences between the non-dental group and the dental technicians or dentists beforeDMPS were highly significant. The difference between thedental technicians and dentist groups as far as -6- to 0-hrurinary Hg content (before administration) was not statisti-cally significant (P = .252). After DMPS administration,
however, although the difference between the two dentalgroups appeared marked, it was on the borderline of signif-icance (P = .057) This may be because of the small samplesize of the dentist group. The original expectation was thateight dentists from the clinic would participate in these ex-

Profile of mood scales and symptom P values based onage, ethansi cons�, eye� wesr and vocabulary
urinary mercury level after DMP5 with the regression analysis controlling for
Mean Values ± S.D. Urinary Mercuryafter DMPS
P ValueUnexposed-
Exposed
MoodTension
Unadjusted 8.3 ± 3.6 9.8 ± 5.4Adjusted 8.3 ± 1 .5 9.8 ± 4.4 .06
DepressionUnadjusted 4.1 ± 3.8 7.2 ± 10.2Adjusted 4.1 ± 3.0 7.2 ± 7.2
AngerUnadjusted 7.3 ± 3.1 9.7 ± 7.7Adjusted 7.3 ± 2.6 9.7 ± 4.8 .05
VigorUnadjusted 16.9 ± 3.2 13.2 ± 4.5Adjusted 16.9 ± 2.6 13.2 ± 2.3
FatigueUnadjusted 5.0 ± 4.2 4.6 ± 3.1Adjusted 5.0 ± 2.1 4.6 ± 2.3
ConfusionUnadjusted 3.7 ± 2.0 5.5 ± 4.9Adjusted 3.7 ± 1 .7 5.5 ± 3.7 .04
Symptoms
HeadachesUnadjusted 2.2 ± .4 2.5 ± .5Adjusted 2.1 ± .3 2.5 ± .4 .00
EmotionalUnadjusted 4.2 ± .4 4.4 ± .5Adjusted 4.2 ± .3 4.4 ± .3 .05
CoordinationUnadjusted 8.3 ± .6 8.3 ± .5Adjusted 8.3 ± .5 8.3 ± .3
ComprehensionUnadjusted 3.1 ± .3 3.3 ± .5Adjusted 3.1 ± .1 3.4 ± .3 .05
MemoryUnadjusted 4.4 ± .8 4.6 ± .9Adjusted 4.4±.4 4.6±.7
SensoryUnadjusted 6.7 ± .8 7.1 ± 1.2Adjusted 6.7 ± .6 7.1 ± .8
DizzinessUnadjusted 3.6 ± .9 4.0 ± 1.0Adjusted 3.5 ± .1 4.0 ± .1
Poor sleepUnadjusted 3.4 ± .9 3.8 ± 1.0Adjusted 3.4±.5 3.8±.3
Skin disordersUnadjusted 2.0 ± .0 2.2 ± .4
Adjusted 2.1 ± .0 2.2 ± .1Chest
Unadjusted 4.1 ± .3 4.3 ± .6Adjusted 4.1 ± .2 4.3 ± .4
PainUnadjusted 2.1 ± .3 2.7 ± 1.2Adjusted 2.1 ± .1 2.7 ± .9
OdorsUnadjusted 1 .9 ± .3 2.3 ± 1.7Adjusted 1.9 ± .2 2.3 ± .8
M symptomsUnadjusted 2.8 ± 2.7 3.6 ± 3.0Adjusted 2.8 ± 1.8 3.6 ± 1.4
1995
TABLE 8
DMPS-M.rcUry Challenge Test 271
periments. Because ofcircumstances beyond our control, onlyfive participated.
The magnitude of the increased urinary excretion afterDMPS was greatest in the case ofthe dental technician group
(table 4). The greatest increase in each group after the DMPS
challenge occurred in the individual in that group who had
the lowest urinary mercury excretion before DMPS adminis-
tration. The working conditions and employment tasks ofthese dental technicians have been described in the StudyPopulation section under Results to explain their mercuryexposure. Obviously, corrective measures should be taken inthis clinic and perhaps in others in developing countries in

272 Gonzalez-Ramirez at al. Vol. 272
regard to better training in the handling ofmercury by dentaltechnicians, better ventilation in the preparation room of thedental clinic and the use of amalgam capsules.
It should not be overlooked that the DMPS challenge test1) increased the mean urinary mercury excretion 35-, 49- and88-fold in the respective study groups (table 4), 2) offeredadditional information on the body load of mercury because
there was no correlation between the before and after urinary
mercury excretion ofthe dental technicians or controls (fig. 1)and 3) showed that the latter observation was not true for thedentists, perhaps because of the small number of dentists in
the study. In addition, these results point out the tremendouscapacity of the kidney for retaining mercury and the lack ofobvious clinical signs and symptoms ofmercury toxicity whenurinary mercury levels rise to 481, 275 and 37 �gIliter of Hgin contrast to < 5 pg/liter ofHg, which is considered normal.
Mercury levels in the urine of German dental personnel,before and after DMPS administration, have been reported
by Zander et al. (1992). Dental nurses were reported to bemore exposed than dentists but this seemed to be related to
the larger number of dental fillings that the dental nurseshad. In the present study, there was no linear correlationbetween the urinary mercury level either before or afterDMPS and the number of amalgams or the amalgam score
(data not shown). A possible reason for this is that the amal-gam restorations in the mouths of the subjects in this studyappear to have had much larger diameters than those foundin a previous study ofAmerican college students (Aposhian et
al., 1992).Second, urinary coproporphyrin concentration was found
to be well correlated with urinary total mercury amount or
concentration only in the case ofthe dental technicians whenthe pre-DMPS coproporphyrin was compared with the post-
DMPS mercury (r = 0.921 for amount; r = 0.977 for concen-
tration; table 5). The pre-DMPS urinary coproporphyrin levelbut not the post-DMPS urinary coproporphyrin levels ap-pears to be indicative of mercury exposure. Based on theevidence, the urinary mercury level after DMPS administra-tion is a better indicator of the renal mercury burden than isthe mercury concentration measured in the urine beforeDMPS was given. The implications of this for occupationalmedicine are obvious. The correlation between the pre-DMPS
urinary coproporphyrin concentration and the post-DMPSurinary total mercury amount within these dentists (r =
0.667) was not as high as was found for the dental techni-cians. This may be due to the small size ofthe dentist group.There was a negative correlation among the nondental groupbetween the pre-DMPS urinary coproporphyrin concentra-tion and post-DMPS urinary total mercury amount or con-centration (r = -0.642 amount; r = -0.716 concentration).This may be due to the fact that the nondental personnel did
not have a history ofrecent or extended exposure to mercury,
as reflected by their low post-DMPS urinary mercury levels.
Their coproporphyrin levels were lower than the other two
groups and may be in the normal range.After the DMPS challenge, urinary porphyrin concentra-
tions declined with respect to pre-DMPS levels (table 6). The
decrease in coproporphyrin level was most substantial in thisrespect, decreasing to 68%, 66% and 48% ofthe before-DMPSvalues among dentists, dental technicians and nondentalpersonnel, respectively, which suggests a substantial deple-tion of renal mercury. The only statistically significant dif-
ference, however, was found in the dentists. After the DMPSchallenge, urinary porphyrin levels fell to 58% and 68% of thebefore DMPS values for dental technicians and nondentalpersonnel, respectively, which suggests depletion of renalmercury.
These findings are consistent with results ofprevious stud-ies that demonstrate a highly significant dose and time-related correlation between the urinary concentration ofthese three porphyrins and renal mercury content in rats(Woods et al., 1991) and also with observations that show asignificant association between urinary levels of these por-phyrins and mercury exposure among dentists (Woods et al.,1993). The present results indicate the value of urinary por-phyrin measurements in addition to urinary mercury deter-minations for the assessment of the efficacy of DMPS inreducing renal mercury levels.
Third, based on the results of neurobehavioral assays, thepresent investigation found evidence of the occurrence ofsubclinical effects caused by the exposure of humans to mer-cury, as indicated by urinary mercury concentrations thataveraged between 30 and 481 pg/liter before and after theDMPS challenge. The pattern ofthe results ofthese neurobe-havioral tests provided particularly convincing evidence ofthe health effects at low levels of mercury exposure becausethey occurred in the younger, mercury-exposed group who donot consume much alcohol compared with the referencegroup of older subjects who did drink alcohol. Within theconstraints imposed by a small number of subjects, potentialcultural differences between the United States and Mexicoand relatively low exposure to mercury, the urinary mercury
levels both before and after the DMPS challenge were ad-versely and statistically associated with functions associated
with complex attention (switching task), a psychomotor task(symbol-digit latency), mood and symptoms in a linear dose-effect manner. These results were consistent with previousfindings among dentists with low-level mercury exposure(Echeverria et al. , in press, 1995) and reflected similar sub-clinical deficits found at higher exposures (Fawer et al. , 1983;Zedda et al. , 1980; Piikivi et al. , 1984; Soleo et al. , 1990;Smith et al. , 1983) among other occupational populations.The consistency in direction among most of the associationsis noteworthy even though the differences in the results inthe test for digit span and SRT did not meet statisticalsignificance, perhaps because of the small number of sub-jects. Improved performance among the exposed group forthe one-hole test may also be explained by the strong asso-ciation with age, in which the younger group of subjects wasexpected to do better.
A number of questions remain to be answered. First, doesDMPS given under the conditions of the challenge test mo-bilize mercury only from the kidney or does it also mobilizemercury in other tissues and then allow the kidney to con-centrate and excrete the mercury? Buchet and Lauwerys(1989) reported that, when rats were given mercury vapor byinhalation, mercury accumulated mainly in the kidneys andthat DMPS mobilized the mercury stored in the kidney. AfterDMPS treatment, there was a decrease of the mercury con-tent of the kidney from about 30 �g/100 g of body weight toabout 4 �g/100 g of body weight. Animal experiments, how-ever, often do not or sometimes cannot replicate environmen-tel conditions in humans. After a 4-day course of therapywith the chelating agent DMSA(2,3-dimercaptosuccinic acid)

(which is structurally analogous with DMPS) for workersexposed to large amounts of Hg#{176},Bluhm et al. (1992) con-cluded that prolonged therapy was required to influence ap-preciably the urinary mercury proffle. They also observedthat blood mercury levels did not increase during chelation
therapy, which suggests that DMSA did not mobilize tissuemercury, other than that of the kidney at the dose and the
conditions used. DMSA, however, unlike DMPS, is primarily
extracellular in its distribution. Molin et al. (1991) suggested
that a single dose of DMPS mobilizes mercury mainly from“readily accessible body pools” and the resultant urinary
mercury excretion is mainly an index of recent exposure.We once stated (Aposhian et al., 1992) that “our experi-
mental results can not be used to support either side of the
controversy dealing with whether mercury vapor liberated
from dental amalgam is harmful or involved in the etiology ofdisease(s) (Eley and Cox, 1987; Sikorski et al. , 1987; Hanson
and Pleva, 1991; Enwonwu, 1987).” In the present study,however, in which dental technicians were exposed to mer-
cury vapor as a result of their working with amalgams, themean urinary mercury level after the DMPS challenge wasadversely and statistically associated with functions relatedto complex attention, a psychomotor task, mood and symp-
toms in a linear dose-effect manner. Their mean urinary
mercury concentration before the DMPS challenge test was
29.7 pg/liter but increased to 481 p.g/liter after the DMPS
challenge.In sufficient amounts, there is no question that mercury
can be toxic. Clarkson (1990) in a provocative article hascalled mercury “the element ofmystery.” Certainly, in regard
to the mercury emitted from dental amalgams, with whichthe dental technicians worked, neurobehavioral changes oc-curred. However, the mystery as to whether or not dentalamalgams in the mouth are or are not toxic will continueuntil more sensitive biological markers of human disorders
caused by mercury exposure can be developed. Certainly,neurobehavioral tests appear to be the most promising in thisrespect at the present time.
Studies that deal with the possible mechanism of action ofthe central nervous system toxicity ofmercury (Palkiewicz et
al. , 1994) and the relationship between amalgam mercuryvapor, mercury resistance and antibiotic resistance in hu-mans, as recently reported by Summers et al. (1993), need to
be continued until a cause-and-effect relationship in humansis either established or negated. Otherwise, just as the de-velopmental toxicity of low levels of lead was not recognized20 years ago, which bestowed a toxic legacy on the children oftoday and perhaps those of tomorrow, the mystery of mer-cury, in this case, dental amalgams, must be solved or stillanother toxic legacy will burden the young of tomorrow.Mercury is not only a problem for dental personnel in devel-oping countries but also mercury from amalgam (Lorscheider
and Vimy, 1993) may be a potential public health problem forall people who can afford dental care.
Aclmowledgments
We express our appreciation to Dr. Salvador Said Ferdnandez,Director of The Centro de Investigacion Biomedica Del Noreste,Institute Mexicano Del Seguro Social, Monterrey, Mexico for his
encouragement, helpfulness, cooperation and support.
1995 DMPS-Mercury Challenge Test 273
References
ALBERS, J. W., KALLENBACH, L. R., Fn�x, L J., L�coir, G. D., Wois�, R. A.,DONOFRIO, P. D., Aussi, A. G., SroLp-Si�cim, K A., BROMBERG, M. B. �m ThxMERCURY Woiuc�as Srtmy Ganup: Neurological abnormalities associated withremote occupational elemental mercury exposure. Ann. Neurol. 24: 651-659,1988.
APOSHIAN, H. V.: DMSA and DMPS-Water soluble antidotes for heavy metalpoisoning. Annu. Rev. Pharmacol. Toxicol. 23: 193-215, 1983.
APos}UAN, H. V., BRUCE, D. C., Ai.,�a, W., Dm, R. C., Huiu.su’r, K. M. �APOSHIAN, M. M.: Urinary mercury after administration of 2,3-dimercapto-propane-1-sulfonic acid: Correlation with dental amalgam score. FASEB J.6: 2472-2476, 1992.
APOSIIIAN, H. V., Go�az-Ru,.maz, D., M�ioanio, R. M., ZUNIGA-CHARLES, M.,Xu, Z. F., Hum.su�r, K M., Jtmco-Mu�ioz, P., Aposm,�N, M. M. 4�i�ir D�urr, R. C.:Mobilization of heavy metals by newer, therapeutically useful chelating
agents. Toxicology, in press, 1995.BAKER, E. L, FELDMAN, R. G., Wmra, R. F., H,�paxy, J. P., Nu.as, C. A., DINSE, G.
E. #{163}�mB�m�r, C. S.: Occupational lead neurotoxicity: A behavioural and
electrophysiological evaluation. Study design and year one resulta. Br. J.md. Med. 41: 352-361, 1984.
B�icaa, E. L., Lrrz, R. E., Fwixa, A. T., S�u�tT, S., Pi.#.NmMuR,�, D. L �rLLYNDON, M. L: A computer-based neurobehavioral evaluation system foroccupational and environmental epidemiology: Methodology and validationstudies. Neurobehav. Toxicol. Teratol. 7: 369-377, 1985.
BLUHM, R E., BOBBrrF, R. G., WELCH, L W., WOOD, A. J. J., BONFIGLIO, J. F.,SARzEN, C., HEATH, A. J. �n BRANCH, R. A.: Elemental mercury vapourtoxicity, treatment and prognosis after acute, intensive exposure in chloal-kali plant workers. Part I: History, neuropsychological findings and chelatoreffects. Hum. Exp. Toxicol. 11: 201-210, 1992.
Bowaas, M. A., Aicsaa, L D., DAVIS, H. A. � Woons, J. S.: Quantitativedetermination of porphyrins in rat and human urine and evaluation ofurinary profiles during mercury and lead exposures. J. Lab. Clin. Med. 12O’�272-281, 1992.
BucsE’r, J. P. 4�z’n L�uw�ays, R. R.: Influence of 2,3 dimercaptopropane-1-sulfonate and dimercaptosuccinic acid on the mobilization of mercury fromtissues of rats pretreated with mercuric chloride, phenylmercury acetate ormercury vapors. Toxicolo� 54: 323-333, 1989.
CAMPBELL, J. R., CLARKSON, T. W. �n O�a, M. D.: The therapeutic use of2,3-dimercaptopmpane-1-sulfonate in two cases of inorganic mercury poi-soning. J. Am. Med. Assoc. 256: 3127-3130, 1986.
CHERM.N, M. G., Mmas, E. F., CL.�iucsoN, T. W. �rrn Cox, C.: Estimation ofmercury burdens in rats by chelation with dimercaptopropane sulfonate. J.Pharmacol. Exp. Ther. 245: 479-484, 1988.
CHISHOLM, J. J., JR.: Mobilization of lead by calcium disodium edetate; a
reappraiaal (Editorial). Am. J. Dis. Child. 141: 1256-1257, 1987.Cmsiiou�i, J. J., Ja. �i�ii Tho�s, D. J.: Use of2,3-dimercaptopropane 1-sulfon-
ate in treatment oflead poisoning in children. J. Pharmacol. Exp. Ther. 235:665-669, 1985.
CLARKSON, T. W.: Mercury-An element of mystery. N. Engl. J. Med. 323:1137-1139, 1990.
CLARKSON, T. W., M�oos, L, Cox, C., GREENWOOD, M. R, Awr�i-Z,uc, L., MAszsaD,
M. A. AND Az.-D�w,n, S. F.: Te8ts of efficacy of antidotes for removal ofmethyl mercury in human poisoning during the Iraq outbreak. J. Pharma-col. Exp. Ther. 215: 74-83, 1981.
ECHEVERRIA, D., Fmia, L, L�ooi.r, G., Scsomc, T. �r�i S�pMo, C.: Acutebehavioural comparisons of toluene and ethanol in human subjects. Br. J.lad. Med. 45: 750-761, 1991.
ECHEVERRIA, D., WHITE, R. 4�m S�pMo, C.: A neurobehavioral evaluation ofPCE exposure in patients and dry cleaners: A possible relationship betweenclinical and preclinical effects. J. Occup. Med., in press, 1995.
Eizr, B. M. AND Cox, S. W.: Mercury from dental amalgam fillings in patients.Br. Dent. J. 163: 221-226, 1987.
ENwo�wu, C. 0.: Potential health hazard of use of mercury in dentistry:Critical review of the literature. Environ. Res. 42: 257-274, 1987.
FAWER, R. F., DE RIBAUPIERRE, Y., Guui.sawr, M. P., BERODE, M. 4�i’ii LOB, M.:Hand tremor measurements: Methodology and applications. In Advances inthe Biosciences, Neurobehavioral Methods in Occupational Health, ed. by RGilioli, M. G. Cassitto and V. Foa, vol. 46, pp. 137-144, Pergamon Press,Oxford, England, 1983.
Gaiuww, I., W�uBn�aa, P., THRUO, H. �i Ruan�u�, B.: Diagnosis ofheavy metal loading by the oral DMPS and chewing-gum tests. lOin. Lab.38: 404-411, 1992.
HANSON, M. AND PLEVA, J.: The dental amalgam issue. A review. Experientia(Basal) 47: 9-22, 1991.
Hoorr�r, C., ANDERSSON, K �n H�a, M.: A questionnaire approach to themonitoring of early disturbances of the central nervous function. In Biolog-ical Monitoring and Survefflance ofWorkers Exposed to Chemicals, ad. by A.Aitio, V. Riliimaki and H. Vainio, Hemisphere Publishing Corp., Washing-ton, DC, 1984.
Huiu.wr, K M., M�ioamio, R. M., M�yaasomi, M., D�urr, R. C., BRUCE, D. C. �r�in
APO8HIAN, H. V.: Determination and metabolism of dithiol chelating agents:XVI. Pharmacokinetics of 2,3-dimercapto-1-propanesulfonate after intrave-nous administration to human volunteers. J. Pharmacol. Exp. Ther. 265:662-668, 1994.

274 Gonzalez-Ramirez et al.
KALLENBACH, L. R.: Health Evaluation and Reported Symptoms in Workerswith Past Occupational Exposure to Elemental Mercury, Ph.D. thesis, Urn-versity of Michigan, Ann Arbor, Ml, 1988.
KEMPER, F. H., JEKAT, F. W., Bmm�w, H. P. �r�m Ecx�iw, R.: New chelatingagents. In Basic Science in Toxicology, Proceedings ofthe 5th InternationalCongress of Toxicology, England, 1989, ed. by G. N. Volans, J. Sims, F. M.Sullivan and P. Turner, Taylor & Francis Ltd., London, 1990.
LORSCHEIDER, F. L. �o Vmrr, M. J.: Evaluation of the safety issue of mercuryrelease from dental fillings. FASEB J. 7: 1432-1433, 1993.
MAJORINO, R. M., DART, R. C., C�urmn, D. E. �u APOSHIAN, H. V.: Determinationand metabolism ofdithiol chelating agents: XII. Metabolism and pharmaco-kinetics of sodium 2,3-dimercaptoprnpane-1-sulfonate in humans. J. Phar-macol. Exp. Ther. 259’� 808-814, 1991.
MCNAIR, D. M., Lopjt, M. �n Dsoppin�, L. F.: Edits Manual Profile on MoodStates, Educational and Industrial Testing Service, San Diego, 1971.
MILLER, J. M., Cw�rri�, D. B. � S�cm, R. G.: Subclinical psychomotor andneuromuscular changes in workers exposed to inorganic mercury. Am. lad.Hyg. Assoc. J. 36: 725-733, 1975.
Mouri, M., SCHI.rrz, A., Sic�arvrria, S. � S�tusrw, G.: Mobilized mercury insubjects with varying exposure to elemental mercury vapour. Int. Arch.Occup. Environ. Health 63: 187-192, 1991.
NALEWAY, C., CHOU, H. N., Muu.aa, T., D�ay, J., Roxa, D., SIDDIQUI, F.: On sitescreening for urinary mercury concentrations and correlation with glomer-ular and renal tubule function. J. Public Health Dent. 51: 12-17, 1991.
Na�, P. A., FLINN, R. H., EDWARDS, T. I., Rannwrr, W. H., HOUGH, J. W.,� J. M., Goumwi, F. H., ARMSFR0NG, D. W., Gs�y, A. S., Coi.ai�,A. L. �u Pormi�, B. F.: Mercurialism and Its Control in the Felt-HatIndustry, bulletin 263, U. S. Public Health Service, Washington, DC, 1941.
Noiai, C. H., Foo, S. C., Bogy, K W. �r�u JEYARATNAM, J.: Chronic neurobehav-ioural effects ofelemental mercury in dentists. Br. J. md. Med. 49:782-790,1992.
OSIN8KA, J. AND TRoJANowsxA, B.: The clinical state ofpersons with the mercurydeposits detected by the use of the unithiol test. Przegl. Lek. 38: 595-598,1981.
PALK!EwICZ, P., Zwiaas, H. 4�m Loascuamaa, F. L: ADP-ribosylation of brainneuronal proteins is altered by in uitro and in viuo exposure to inorganicmercury. J. Neurochem. 62: 2049-2052, 1994.
P11KW:, L, HANNINEN, H., Mm�i.ni, T. �n M�m’aas, P.: Psychological perfor-mance and long-term exposure to mercury vapors. Scand. J. Work Environ.Health 1O’� 35-41, 1984.
ROELS, H., G�irr, J. P., L&tr�iapxs, R, Bucsa’r, J. P., M�ca�uaa, J. �nBaa�an, A.: Survefflance of workers exposed to mercury vapour: Validationofa previously proposed biological threshold limit value for mercury concen-tration in urine. Am. J. hid. Med. 7: 45-71, 1985.
S�i.va�nv, G.: Selection ofindustrial operators: The one hole test. mt. J. Prod.Res. 132: 303-321, 1975.
SCHIELE, R., SCHALLER, K. H. �n WELmE, D.: Mobilization ofmercury reserves
in the organism by means of DMPS (DIMAVAL). Occup. Med. Soc. Mod.Prey. Med. 24: 249-251, 1989.
Vol. 272
SHAPIRO, I. M., CoRN�BLATH, D. R., Suan�rEa, A. J., Uzzzu., B., Spn’z, L K, Sm,’, I.I. AND BLOCH, P.: Neurophysiological and neuropsychological function inmercury-exposed dentists. Lancet 1: 1147-1150, 1982.
SIKoRsiu, R., JUSZKIEWICZ, T., PA.SZKOWSKI, T. AND SZPRENOIER-JUSZIEWICZ, T.:Women in dental surgeries: Reproductive hazards in occupational expo-sure to metallic mercury. mt. Arch. Occup. Environ. Health 59: 551-557,1987.
SKERFVING, S.: Exposure to mercury in the population. In Advances in Mercury
Toxicology, ed. by T. Suzuki, N. Imura and T. Clarkson, pp. 411-425,Plenum Press, New York, 1991.
S0LE0, L., Ui�au�o, M. L., PE�rsza�, V. �r�n AaesRosi, L: Effects oflow exposureto inorganic mercury on psychological performance. Br. J. md. Med. 47:105-109, 1990.
SMITH, P. J., LANG0LF, G. D. �r Goumxao, J.: Effects ofoccupational exposureto elemental mercury on short-term memory. Br. J. md. Med. 41k 413-419,1983.
SUMMERs, A. 0., Wmz�, J., Vmw, M. J., Loascuamas, F. L, M�mw�, B., Law,S. B., Bs�e�z’rr, S. �n Bru.�uw, L: Mercury released from dental “silver”fillings provokes an increase in mercury- and antibiotic-resistant bacteria inoral and intestinal floras of primates. Antimicrob. Agents Chemother. 37:825-834, 1993.
Tou’roNom, G., ECszvnaiu.�, D., Bn’ri�na, A. �u�m RONHOVDE, N.: The use ofswitching ability to assess central nervous system function. In Advances inIndustrial Ergonomics and Safety III, ed. by W. Karwowski and J. W. Yates,pp. 629-636, Taylor and Francis, Inc., London, 1991.
Urmi., B. P., AND OLER, J.: Chronic low-level mercury exposure and neuropsy-chological functioning. J. Cliii. Exp. NeuropsychoL & 581-593, 1986.
Wooce, J. S., Bowsss, M. A. �u�m DAVIS, H. A.: Urinary porphyrin profiles asbiomarkers oftrace metal exposure and toxicity: Studies on urinary porphy-rin excretion patterns in rats during prolonged exposure to methyl mercury.Toxicol. Appl. Pharmacol. 11th 464-476, 1991.
Wooce, J. S., M�urrm, M. D., NALEWAY, C. A. �m Ecszvzmu�, D.: Urinaryporphyrin profiles as a biomarker of mercury exposure: Studies on dentistswith occupational exposure to mercury vapor. J. Toxicol. Environ. Health 4�235-246, 1993.
Woaw HEALTh ORGANIZATION 5vur�y Gsoup: IPCS Environmental Health Cri-teria 118, Inorganic Mercury, World Health Organization, Geneva, 1991.
ZANDER, D., EWERS, U., Faziza, I. �um Becciutaus, A.: Studies on human expo-sure to mercury: IV. Mercury exposure in male and female dentists andfemale dental assistants. Zentralbl. Hyg. Umweltmed. 193: 318-328, 1992.
ZEDDA, S., Cuu�, A. M., R�u’ri, R., S�, C. �uw Z�au’ou�o, A.: Rischio damercurio nella fabbricazione de lanipade fluorescenti studio clinic e ambi-entale. G. Ital. Med. Lay. 2: 187-192, 1980.
Send reprint requests to: Dr. H. Vasken Aposhian, Department of Molecu-lar and Cellular Biology, Life Sciences South Building, University of Arizona,Tucson, AZ 85721.