Socket Treatment - Divas in Dentistry - Our Goal, Our...
8
Socket Treatment Procedure Guide www.implantdirect.com | 888.649.6425
Transcript of Socket Treatment - Divas in Dentistry - Our Goal, Our...

Socket Treatment
Procedure Guide
www.implantdirect.com | 888.649.6425
Extraction Healing and Ridge Resorption | The Why
Working with patients to educate them on the benefits of bone maintenance post extraction is a rewarding endeavor. Socket treatment allows for bone maintenance and prevents the typical reduction of height and width that can occur after tooth loss. With no treatment, a socket can lose up to 50% bone reduction in width in the first year (Johnson 1963)1 which in time can impact adjacent teeth, the jaw line, chewing, occlusion, and bite. However, 2/3 of the socket reduction occurs in the first 3 months (Schropp 2003)2.
Practice of wound socket treatment utilizing bone grafts and membranes will provide a reliable way of saving alveolar bone to support future pontics and/or implants. Predictable healing of extraction sites with minimal intervention is the goal. Complicated tooth extraction can lead to additional bone loss due to surgical trauma.
The success of bone grafting is ultimately dependent on vascularization and remodeling of the bone graft into vital bone. Buccal plate is the key factor in the pink and white interface to create a favorable architecture of the alveolar ridge. The main sources of vascularization, who contributes of the viability of buccal plate are periosteum, periodontal ligament and bone marrow. Healing of the socket depends on the number of the walls present, vascularization which starts from the walls to the center and blood clot stabilization which plays an important role in any regenerative procedures. Space maintenance is a must when we want to maintain the volume of soft and hard tissue, especially at the gum level considering that socket healing starts from the bottom of the socket to the top of the ridge.
Treatment Decision Tree | The How
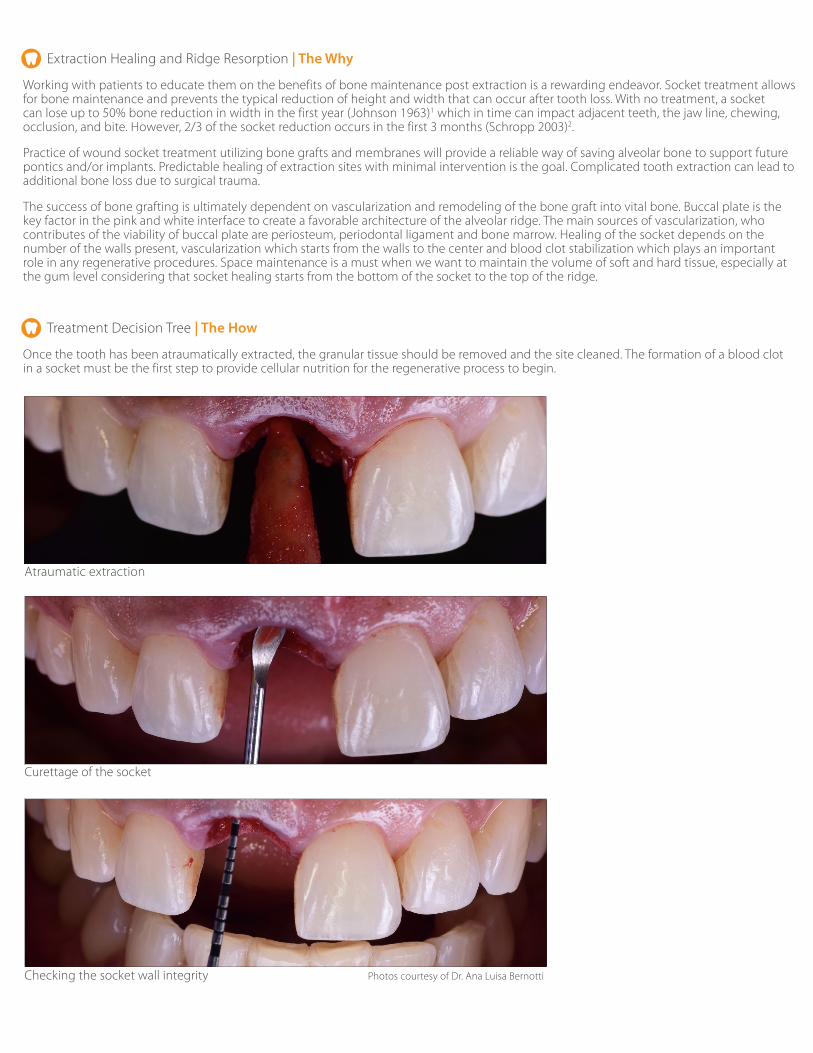
Once the tooth has been atraumatically extracted, the granular tissue should be removed and the site cleaned. The formation of a blood clot in a socket must be the first step to provide cellular nutrition for the regenerative process to begin.
Atraumatic extraction
Checking the socket wall integrity
Curettage of the socket
Photos courtesy of Dr. Ana Luisa Bernotti

Socket classification (Salama et al, 1993)3
Type 1 Socket - Intact walls and soft tissue - we will proceed with socket preservation
Type 2 Socket - Buccal plate defect- we will proceed with socket augmentation
Type 3 Socket - Buccal plate and interproximal defect

This surgical technique is the recommendation of Dr. Delia Tuttle, DDS. Implant Direct is a medical device manufacturer and does not dispense medical advice. Clinicians should use their own judgment in treating their patients.
The ideal treatment in Type 3 socket will be orthodontic extrusion first followed by socket augmentation with CTG and epithelial graft. This treatment increases morbidity, it takes longer for healing and requires soft tissue surgical skills. When the ideal treatment cannot be performed using patient’s own biologicals use biomaterials. A bone graft is placed into the socket to provide a scaffold interface for osteoconduction. A secondary benefit of the graft is that it maintains space to support a membrane as bone healing is competing with soft tissue healing. This provides an advantage for the slower growing bone to regenerate in the site. When placing a membrane in the site make sure that the membrane completely covers the defect and overlaps the intact walls to a minimum of 2mm. If trimming of the membrane is required, round the edges to minimize injury of the tissue by sharp edges. The membrane can be pre-shaped to have a rounded effect by placing it on a periosteal elevator handle to take on the ridge shape. For more traumatic extractions in which two or more bony walls are not intact, steps must be made to support the architecture. Implant Direct offers a complete line of regenerative choices to give the clinician choice in his armamentarium. (Please see table on the next page for protocol suggestions).
Type 2 socket illustration - Anterior buccal bone deficiency grafted with bone graft and covered by membrane:
Courtesy of Dr .Snjezana Pohl, MD, DMD
Courtesy of Dr. Delia Tuttle, DDS
Type 2 Socket
Photos courtesy of Dr. Delia Tuttle, DDS
Photos courtesy of Dr. Delia Tuttle, DDS

Options for Socket Treatment
Conventional Prosthesis Implant Site Development Implant Site Development Implant Site Development
Long - term ridge preservation Intact socket 1-2 walls missing More than 2 walls missing
βioResorb® DirectGen™DirectOss™
DirectGen™DirectOss™
DirectGen™ FLEXDirectGen™DirectOss™
Kontour Adapt™ if primary closure is achieved
Kontour Adapt™ if primary closure is achieved
Kontour Sustain™ if primary clo-sure is achieved
CytoPlast® RTM if primary closure is achieved
(PTFE or TiPTFE) Non Resorbable Membrane if primary closure is not achieved
(PTFE or TiPTFE) Non Resorbable Membrane if primary closure is not achieved
(PTFE or TiPTFE) Non Resorbable Membrane if primary closure is not achieved
(PTFE or TiPTFE) Non Resorbable Membrane if primary closure is not achieved
Photos courtesy of Dr. Delia Tuttle, DDS - DirectGen™ Flex
In an effort to minimize postoperative complications hygiene compliance becomes critical. Very light gentle brushing is recommended at the site for 2 weeks. If the membrane is exposed the use of a sponge applicator dipped in chlorhexidine is recommended. The sutures may be removed at 10 days and, if a non-resorbable was used it may be taken out at 4-6 weeks. Prescribing postoperative antibiotics may be the choice of the doctor. Management of healing may require a temporary prosthesis. This may be especially desirable in anterior situations where esthetics are a concern. It is important in these cases that the temporary is relieved and does not create pressure on the new soft tissue. The indentation will form the soft tissue profile, which will play a role in the esthetics of the final prosthesis.
Initial clinical situation Socket type 3 Photos courtesy of
Dr. Snjezana Pohl MD, DMD
Maryland temporary bridge Final outcome

Socket Preservation | The Benefit
Allowing bone growth to successfully compete against soft tissue growth is the central issue in the healing of extraction sockets. The use of bone grafts and membranes best facilitates this objective by allowing the preservation and regeneration of the bony architecture of the jaw line.
Additional benefits of membrane therapy include physical protection of the wound, retention of the bone graft, and acting as a barrier to bacteria.
- ADA CDA Code Fees in 2016 (USD) 40th percentile
Fees in 2016 (USD) 95th percentile
Non-surgical Extraction D7140 175 270
Non-resorbable Membrane D4267 850 1,252
Socket Graft D7953 465 1,652
Total Fees - 1,490 3,174
Non-Resorbable Material Costs Product Cost
Bone Grafting Material DirectGen™ Mineralized Cort/Can Blend Allograft: 0.5cc (250-1000µm)
80.99
Non-resorbable Membrane Cytoplast® GBR-200 SINGLES ~32.00 ea
Non-resorbable PTFE Suture Cytoplast® PTFE Non Resorbable 2-0 suture, FS-2 needle, undyed
~8.33 ea
Total Material Cost - ~121.32
Non-Resorbable Fees in 2016 (USD) 40th percentile Fees in 2016 (USD) 95th percentile
Fees 1,490 3,174
Material Costs* ~121.32 ~121.32
- 1,368.68 3,052.68
*Does not include overhead
Extraction and Treatment Codes | The Return for the Patient
Socket Preservation requires only a few minutes. It improves patient care and reduces time for proper blood clotting to occur. It is also a procedure which may improve practice growth.
Photos courtesy of Dr. Delia Tuttle, DDS
1. K. Johnson M.D.Sc, 1963 Study of dimensional changes occurring in the maxilla after tooth extraction. Part 1 Normal healing, Australian Dental Journal , Vol 8. Issue 5, October 1963, pages 428-433
2. Schropp L, Wenzel A, Kostopoulos L, et al. Bone healing and soft tissue contour changes following single-tooth extraction: a clinical an radiographic 12-month prospective study. International Journey of Periodontics Restorative Dent. 2003;23:313-323.
3. Salama et al. The Role of Orthodontic Extrusive Remodeling in the Enhancement of Soft and Hard Tissue Profiles Prior to Implant Placement: A Systematic Approach to the Management of Extraction Site Defects, International Journey of Periodontics & Restorative Dentistry, Vol 13, Issue 4, 1993 pages 313 - 333
Froum S, Orlowski W. Ridge preservation utilizing an alloplast prior to implant placement–clinical and histological case reports. Pract Periodontics Aesthet Dent. 2000; 12:393-402.
Bartee BK. Extraction site reconstruction for alveolar ridge preservation. Part 1: rationale and materials selection. J Oral Implantol. 2001; 27:187-193.
Fowler EB, Breault LG, Rebitski G. Ridge preservation utilizing an acellular dermal allograft and demineralized freeze-dried bone allograft: Part 1. A report of 2 cases. J Periodontol. 2000; 71:1353-1359.
Wang HL, Kiyonobu K, Neiva RF. Socket augmentation: rationale and technique. Implant Dent. 2004; 13:286-296.
Misch CE. Bone augmentation for implant placement: keys to bone grafting. In: Contemporary Implant Dentistry. 2nd ed. St Louis, MO: Mosby; 1999: 451-468.
Misch CE, Dietsh F. Bone-grafting materials in implant dentistry. Implant Dent. 1993; 2:158-167.
Misch CE, Suzuki JB. Tooth extraction, socket grafting, and barrier membrane bone regeneration. In: Contemporary Implant Dentistry. 3rd ed. St Louis, MO: Mosby; 2007:870-904.
McCall RA, Rosenfeld AL. Influence of residual ridge resorption patterns on implant fixture placement and tooth position. Part 1. Int J Periodontics Restorative Dent. 1991; 11:8-23.
Tischler M, Misch CE. Extraction site bone grafting in general dentistry. Review of applications and principles. Dent Today. May 2004; 23:108-113.
Becker W, Becker BE, Caffesse R. A comparison of demineralized freeze-dried bone and autologous bone to induce bone formation in human extraction sockets [published correction appears in J Periodontol. 1995;66(4):309]. J Periodontol. 1994; 65(12):1128-1133.
Artzi Z, Tal H, Dayan D. Porous bovine bone mineral in healing of human extraction sockets. Part 1: histomorphometric evaluations at 9 months. J Periodontol. 2000; 71:1015-1023.
Misch CM. Comparison of intraoral donor sites for onlay grafting prior to implant placement. Int J Oral Maxillofac Implants. 1997; 12:767-776.
Dr. Delia Tuttle DDS Dr. Snjezana Pohl, MD, DMD, Periodontist, Oral Surgeon - Croatia
Dr. Ana Luisa Bernotti, Periodontist - Venezuela

Copyright © 2017 Implant Direct Sybron International. All Rights Reserved.
All trademarks are property of their respective companies. Pricing and product availability subject to change without notice. Not all products shown are available in all countries. Please contact Implant
Direct or your local dealer for more information on product availability.
Sales and Technical Support (USA & Canada) www.implantdirect.com | 888-649-6425
08-17 OL-021 Rev. 01 Printed in the U.S.A.*08-17-0062*
Simply Smarter ImplantologyInnovative Designs with Inclusive Packaging
Prosthetics & SMART PACKS LOCATOR®
Mount-Free
Multi-Unit Internal Hex Conical ....and more
Call to find out which one best fits your practice!