
SOCIO-ECONOMIC INEQUITIES IN ACCESS TO MATERNAL … · Under 5 Mortality Rat e SC-Other ST-Other...
21
1 SOCIO-ECONOMIC INEQUALITIES IN ACCESS TO MATERNAL HEALTH CARE IN INDIA: CHALLENGES FOR POLICY Prof. Rama V. Baru Centre of Social Medicine and Community Health Jawaharlal Nehru University New Delhi
Transcript of SOCIO-ECONOMIC INEQUITIES IN ACCESS TO MATERNAL … · Under 5 Mortality Rat e SC-Other ST-Other...

1
SOCIO-ECONOMIC INEQUALITIES IN ACCESS TO MATERNAL HEALTH CARE IN INDIA: CHALLENGES FOR POLICY
Prof. Rama V. BaruCentre of Social Medicine and Community HealthJawaharlal Nehru UniversityNew Delhi

2
Overview
This paper provides a brief overview of socio- economic inequalities in access to maternal
health services in India
It explains why these inequalities persist
It argues that commercialisation
of health services is a determinant of accentuating inequities and contributing to poverty

3
The acceleration of economic growth since 1981 has not translated adequately into a sustained improvement in India’s human development outcomes[GDP growth: 1950-80 = 3.5; 1980-2000= 5.5; 2000-2011= 8.0 approx]
MMR and Under five mortality are unacceptably high and the decline has been slow. This is a cause for concern for both national and global policy (Subramanian et al :2006).
India offers a complex picture of multiple inequalities. There
are regional, sub regional, social and economic dimensions of inequality along multiple axes of class, caste, gender and religion
Broadly, these inequalities get reflected in health outcomes and
access to health services
The available macro data sets enable us to examine these relationships and the patterns
However these data sets do not lend themselves to an analysis of
intersectionality
between these various inequalities (Iyer
et al : 2007)
A few micro studies have analysed the relationship between inequalities, commercialisation and access (Jeffery et al :2007; 2008; 2010)

4
Inequalities in Under-Five Mortality in India, 2006
14
3034
59
7074
79
95 96101
117
0
20
40
60
80
100
120
140
UrbanKerala
Motherswith more
than 12years of
education
Highestquintile
Non ST,SC and
OBC
Male All India Female Motherswith no
education
ST Lowestquintile
Rural UP
Und
er 5
Mor
talit
y
Source: Baru et al (2010) Inequities in Access to Health Services in India: Caste, Class and Region, Economic & Political Weekly,September 18, 2010 vol xlv no 38. Pp 49-58
5
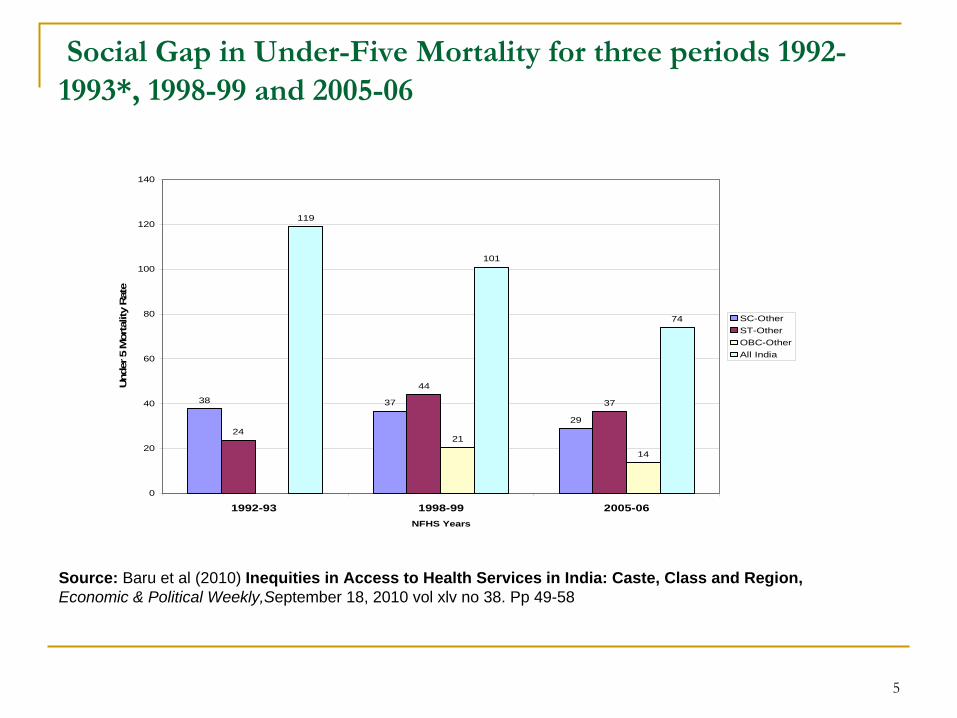
Social Gap in Under-Five Mortality
for three periods 1992-
1993*, 1998-99 and 2005-06
38 37
2924
44
37
21
14
119
101
74
0
20
40
60
80
100
120
140
1992-93 1998-99 2005-06NFHS Years
Und
er 5
Mor
talit
y R
ate
SC-OtherST-OtherOBC-OtherAll India
Source: Baru et al (2010) Inequities in Access to Health Services in India: Caste, Class and Region, Economic & Political Weekly,September 18, 2010 vol xlv no 38. Pp 49-58

6
Full Immunisation Rate*, Inequalities in utilisation of preventive care
24.4
31.3
23
35.538.6 39.7
43.5
57.6
71
75.3 75.2
0
10
20
30
40
50
60
70
80
Low
est Q
uint
ile
Sche
dule
d tr
ibe
Utta
r Pra
desh
All
Indi
a (1
992-
93)
Rur
al
Sche
dule
d ca
ste
All
Indi
a (2
005-
06)
Urb
an
Hig
hest
Qui
ntile
Ker
ala
Mot
hers
with
mor
eth
an 1
2 ye
ars
ofed
ucat
ion
Full
Imm
unis
atio
n (%
)
Source: Baru et al (2010) Inequities in Access to Health Services in India: Caste, Class and Region, Economic & Political Weekly,September 18, 2010 vol xlv no 38. Pp 49-58

7
Socio-economic inequalities and access to delivery services
16 18
3338 39
51
100
0
20
40
60
80
100
120
R ural U P ST SC OB C A ll Ind ia N o n ST , SC andOB C
U rb an Kerala
Source: IIPS and Macro International (2007): National Health and Family Survey – 2005-06 (NFHS 3), Mumbai.

8
Delivery in health facility across wealth index
8
14
23
2724
13
24
39
58
84
0
10
20
30
40
50
60
70
80
90
Lo west Seco nd M id d le F o urt h Hig hest
W ealt h Ind ex
Percentage delivered in Government Health facilityTotal Percentage delivered in Health facility
Source: IIPS and Macro International (2007): National Health and Family Survey – 2005-06 (NFHS 3), Mumbai.
9
Commonly cited reasons for inequities
supply side factors like weak public provisioning; poor quality of services
Demand side factors-
lack of knowledge; cultural beliefs; poverty; lack of purchasing power

10
Determinants of inequities in access
Health service determinants and socio- economic determinants. Both these intersect
and are responsible for the persistence of inequities
Commercialisation
of health services has been a key factor perpetuating inequities in access
11
Defining commercialisation
Commercialisation includes processes like marketisation, commoditisation, privatisation and liberalisation.
“
the provision of health care services through market relationships to those able to pay; investment in, and production of those services, and of inputs to them, for cash income or profit, including private contracting and supply to publicly financed health care; and health care finance derived from individual payments and private insurance”
(Mackintosh &Koivusalo: 2005,p.3)

12
Attitude to public and private sectors is sharply divided between the academic view of privatisation
and the approach of policymakers
Need to ‘unbundle’
the complexity of commercialisation
of health service systems-
private and public

13
Commercialisation
and embodying inequality: Evidence from India
Historical roots of commercialisation
of Indian public
sector in provisioning and drugs
Formal and informal payments in public services during post independence period
Growth and diversification of ‘for profit’
health services
since 1970s
India has a large, differentiated ‘for profit’
sector
(Muraleedharan: 1999; Nandraj
and Duggal
:1997; Baru:1998)
Formal and informal providers (Narayana:2006; Singh: 2010)

14
Institutional arrangements replicate the social hierarchy (Baru:1998)
Differences in qualification of providers, scale of operation and quality of care
Lack of regulation
Complex inter relationships between public sector doctors and paramedical personnel with private institutions (Baru:1998)

15
Health sector reforms accelerated commercialisation-
public and private (Qadeer
et al: 2002)
High out of pocket private spending (Bonu
et al:2007)
Adverse consequences for access; cost and quality of care in public and private sectors (Nandraj
& Duggal
:1997; Bonu
et al :2007)
Cause for households going into poverty and also a defining aspect of being poor –
i.e. those who are poorest
cannot afford access to care (Hart:2000; Garg &Karan:2005; Bonu
et al 2007)
16
Rise in cost of care, high out of pocket expenditure, rising burden on households leading to differential levels of impoverishment of households across income quintiles for maternal health services (Skordis-Worrall :2011; Pathak
et al:2010)
Significant poor-non poor gap in access to maternal health services (Pathak
et al:2010)
Reasons for these trends are attributed to growth of ‘for profit’
services and a deficient public sector

17
Consequences of commercialisation
for maternal health services
Informal payments for antenatal, delivery and post natal services to the public sector form a significant percentage of expenditure on maternal health services
(Sharma et al: 2005;Pathak et al: 2010; Skordis-
Worrall:2011)
Informal charging in the public sector is linked to abuse, exclusion and impoverishment. Indifferent and rude behaviour of health personnel
(Pathak
et al: 2010; Jeffery&Jeffery: 2010; Unisa: 1999)
Shortage of supply of drugs through public institutions force women into purchasing from the free market

18
The contracting out of ultrasound facilities by public sector and referral from public to private sectors adds to out of pocket expenditure (NFHS 3: 2007; Jeffery & Jeffery: 2010)
Back and forth linkages between public and private sector; between formal and informal sector for maternal health services. (Unisa: 1999; Narayana:2006; Singh:2009; Jeffery & Jeffery: 2010)
Paying for care has therefore become entrenched in public and private sectors. This has resulted in the blurring of the roles
of public and private sectors (Baru
& Nundy:2008)
Rising commercialisation has altered the behaviour of public institutions and personnel. Normative values of public institutions have been gradually eroded (Baru:2005)

19
Complex interaction between socio-economic inequalities and health services
Commercialisation
as a driver of inequities in access
Health services planning and regulation must be in tandem to address inequities caused by commercialisation
Recognising
the limits of health services in addressing inequalities in access
Addressing structural inequalities beyond health services
Need for inter sectoral coordination and greater convergence between health services and strategy for poverty reduction
Summing Up

20
Selected References
Baru, R (1998): Private Health Care in India: Social Characteristics and Trends (New Delhi: Sage Publications).
Baru, R and Nundy, M ( 2008) Blurring of Boundaries: Public-Private Partnerships in Health Services in India. Economic and Political Weekly, January 26th 2008. pp.62-71
Baru,R and Bisht, R (2010) Health service inequities as challenge to health security, IHD and Oxfam Working Paper Series.
Bonu, S, I Bhushan and D H Peters (2007): “Incidence, Intensity and Correlates of Catastrophic Out-of- Pocket Health Payments in India”, ERD Working Paper No 102, Asian Development Bank, October; Manila, Philippines.
Garg, C and A K Karan (2005): “Health and Millennium Development Goal 1: Reducing Out-of-Pocket Expenditures to Reduce Income Poverty-evidence for India”, EQUITAP Project, Working Paper No 15, Institute of Health Policy, Colombo
Hart, T J (2000): “Commentary-Three Decades of the Inverse Care Law”, British Medical Journal, 320 (7226): pp 18-19.
IIPS and Macro International (2007): National Health and Family Survey – 2005-06 (NFHS 3), Mumbai
Iyer, A, G Sen and A George (2007): “The Dynamics of Gender and Class in Access to Health Care: Evidence from Rural Karnataka, India”, International Journal of Health Services, 37(3): 537-54
Jeffery, P, A Das, J Dasgupta and R Jeffery (2007): “Unmonitored Intrapartum Oxytocin Use in Home Deliveries: Evidence from Uttar Pradesh, India”, Reproductive Health Matters, 15(30), 172-78.
Jeffery,P and Jeffery, R (2008) ‘Money itself discriminates obstetric emergencies in the time of liberalisation’ Contributions to Indian Sociology, vol 42, no 1. pgs 59-91
Jeffery, P and Jeffery, R (2010) “ Only when the boat has started sinking: A maternal death in rural north India” Social Science and Medicine. November. 71(10), pp.1711-1718
Muraleedharan, V R (1999): “Characteristics and Structure of the Private Hospital Sector in Urban India: A Study of Madras City”, Small Applied Research Paper 5, Partnerships for Health Reform Project, ABT Associates Inc, Bethesda.
Nandraj, S and R Duggal (1997): Physical Standards in the Private Health Sector: A Case Study of Rural Maharashtra, Centre for Enquiry into Health and Allied Themes, Mumbai

21
Narayana, K V (2006): “The Unqualified Medical Practitioners: Methods of Practice and Nexus with Qualified Doctors”, Working Paper No 70, Centre for Economic and Social Studies, Hyderabad.
Nayar, K R (2007): “Social Exclusion, Caste and Health – A Review Based on Social Determinants Framework”, Indian Journal of Medical Research, (126), October, pp 355-63
Praveen Kumar Pathak, Abhishek Singh, S. V. Subramanian (2010) Economic Inequalities in Maternal Health Care: Prenatal
Care and Skilled Birth Attendance in India, 1992–2006. PLOS open access journal
Qadeer, I, K Sen and K R Nayar (2001): Public Health and the Poverty of Reforms: The South Asian
Predicament (New Delhi: Sage Publications).
Rani, M, S Bonu and S Harvey (2007): “Differentials in the Quality of Ante Natal Care in India”, International
Journal for Quality in Health, pp 1-10.
Rao, S (2005): “Delivery of Services in the Public Sector: Financing and Delivery of Healthcare Services in India”, National Commission on Macroeconomics and Health Background Papers, Ministry of Health and Family Welfare, Government of India, New Delhi.
Rao, S, M Nundy and A S Dua (2005): “Delivery of Health Services in the Private Sector: Financing and Delivery of Health Care Services in India”, National Commission on Macroeconomics and Health Background Papers, Ministry of Health and Family Welfare, Government of India, New Delhi
Sharma,S, S. Smith, E. Sonnavelett, M.Pine, V. Dayaratna, R. Sanders (2005) Formal and Informal Fees for Maternal Health Care Services in Five Countries:Policies and Perspectives. Policy Working Paper Series No. 16, USAID, June.
Singh, K (2009) Practices of unqualitied practitioners in urban slums of south west delhi: an exploratory study. Unpublished MPhil dissertation, Jawaharlal Nehru University, New Delhi.
Skordis-Worrall et al. Maternal and neonatal health expenditure in mumbai slums (India): A cross sectional study BMC Public Health 2011, http://www.biomedcentral.com/1471-2458/11/150
Subramanian, S V, S Nandy, M Irving, D Gordon, H Lambert and G D Smith (2006): “The Mortality Divide in India: The Differential Contributions of Gender, Caste and Standard of Living across the Life Course”, American Journal of Public Health, 96, pp 818-25
Unisa, S (1999): “Childlessness in Andhra Pradesh: Treatment Seeking and Consequences’, Reproductive Health Matters, 7(13), pp 54-64, May


















