
A Novel, Time-effective Approach for Capturing Bac- teria ...

Social Medicine (www.socialmedicine.info) - 106 - Volume 6, Number 2, June 2011
IntroductionThis article introduces Comprehensive Partici-
patory Planning and Evaluation (CPPE), an ap-proach to community participation and empower-ment developed from the work of Rifkin,1,2 La-verack,3 Pérez,4 and others. More than just a meth-odology, CPPE is an approach which encouragescomprehensive analysis and participation by vari-ous actors at local, regional, and national level inthe planning and evaluation of health actions.
CPPE has its roots in the 1980s, when an inter-national team of researchers from the Institutes ofTropical Medicine in Antwerp (ITM-Belgium) andAmsterdam (KIT-Netherlands) developed a frame-work of comprehensive participatory evaluation fornutritional improvement programs. Following itsinitial application in the Philippines, further workextended the evaluation approach to planning.CPPE was gradually refined with the support ofresearch teams in Indonesia, the Philippines, andBrazil5 as they applied it in different contexts andprojects.6 Since 2008 projects have been carried outin Cuba to analyze the possibilities offered byCPPE for increasing community participation inhealth.
This article illustrates the rationale and toolsemployed in CPPE through our experience in Cubain the urban municipalities of Centro Habana andLas Tunas and in a rural community in the moun-tains of Cumanayagua. We discuss key methodo-
logical components, the conditions needed for thesuccess of CPPE, and potential differences betweenthe Cuban experience and the possible applicationof CPPE in other contexts.
CPPE methodologyWe consider genuine participation as a process
of developing a community’s capacities to identifyits needs and then to generate proposals and initia-tives which defend its interests. This is a gradualprocess. Consequently, CPPE takes place in a cy-cle: planning, implementation, and evaluation, fol-lowed by a new stage of planning. Periodic evalua-tion—perhaps annually—is carried out to assessprogress on planned initiatives and the level of localorganization. In each cycle community situation isreassessed and plans updated for the following peri-od.
Stage I. Planning workshopThe central activity of CPPE is a workshop
which lasts about four days. This duration is flexi-ble but sufficient time should be allowed for devel-opment of the various stages, supported by the sug-gested tools. (Figure 1)
A proper diagnosis is essential to planning; gen-eral community issues—including health prob-lems— have multiple causes and typically involvevarious sectors. A diagnosis is elaborated using acausal model which allows potential interventionsto be identified. A selection table with defined cri-teria (importance of the problem, feasibility, cost-effectiveness, sustainability, etc.) can help partici-pants select the most appropriate interventions byconsensus. Three tools can then be used consecu-tively to develop operational plans for each selectedintervention:
1. The HIPPOPOC table identifies Inputs, Pro-cesses, Outputs, and Impacts;
2. The dynamic model makes explicit the rationalefor the set of activities proposed and how theycome together in the proposed outcome, and:
SOCIAL MEDICINE IN PRACTICE
Comprehensive Participatory Planning andEvaluation (CPPE)
Pol De Vos , Mayda Guerra , Irma Sosa, Lilian del R Ferrer, Armando Rodríguez ,Mariano Bonet, Pierre Lefèvre and Patrick Van der Stuyft
Corresponding Author: Pol De Vos , Department ofPublic Health, Institute of Tropical Medicine, Antwerp,Belgium. Email: [email protected].
Mayda Guerra, Irma Sosa, Lilian de R. Ferrer, ArmandoRodríguez, and Mariano Bonet are with the Instituto Na-cional de Higiene y Epidemiología, Havana, CubaPierre Lefèvre and Patrick Van der Stuyft are with theDepartment of Public Health, Institute of Tropical Medi-cine, Antwerp, Belgium
Submitted: 9/5/2011Accepted: 10/5/2011Peer Reviewed: YesConflicts of Interest: None declared

Social Medicine (www.socialmedicine.info) - 107 - Volume 6, Number 2, June 2011
3. The operational plan (what, when, who, whatwith, and with whom).
The planning stage should produce three results:1) improved understanding of the multiple causesof the problem to be tackled, 2) a consensuallyagreed upon intervention plan, and 3) a trained andcommitted work team.
Stage II. Implementation of the interventionsImplementation follows the plan that was for-
mulated at the workshop and is led by the workteam. Continuous feedback on the plan’s progressand problems is provided to all team members andto the community as a whole. This is essential forfostering the dynamic of community involvement.
Stage III. EvaluationAfter the implementation phase, the team re-
views the results in an evaluation workshop; thiswill involve both evaluation and further planning.Strengths and weaknesses are identified and solu-tions developed for the problems encountered dur-ing the preceding period.
Each follow-up workshop begins with an assess-ment of what has been accomplished using the dy-namic model developed the previous year. Thisallows participants to ask pertinent questions inthree domains:
1. What were the immediate results of the in-tervention?
2. Are the objectives relevant? (e.g. were theobjectives appropriate? Do the interventionsremain relevant?)
3. How well was the project implemented?(Did we manage to include more people?
Were we able to strengthen grass-roots or-ganization in the neighborhood?)
Following this discussion, the team prepares aconsensus evaluation looking at what worked well.They also examine where and why problems arose.This information serves to inform a review of theprevious year’s causal model. The model is revisedto take into account how the community haschanged and the lessons it has learned during theprevious year. Interventions proposed for the newcycle can be either amendments or extensions ofthe previous year’s work plan or completely novel.(Figure 1)
Fifteen to twenty people are involved in theplanning workshop. To the extent possible theyshould reflect all community stakeholders. Thisincludes leaders of civil society and grass-rootsmovements as well as local representatives of thevarious public sectors (health, education, municipalservices, farming, etc.). We also include informalcommunity leaders such as young activists, the lo-cal hairdresser who knows everyone, housewiveswho care about the neighborhood, etc. The idea isto involve all groups who can contribute to local(health) planning; this ensures their commitment toproject implementation.
Three years’ experience in CubaCPPE was first applied in Cuba in 2008. The
methodology had been developed initially for plan-ning projects carried out by international NGOs andother organizations and had to be adapted to com-munity work within the context of a local healthsystem.7
Figure 1: CPPE rationalePlanning—Implementation—Evaluation—Plan Revision
Planning workshop STAGES TOOL
Analysis Identification of problems Causal model
Prioritization of interventions Selection table
Planning Intervention objectives HIPPOPOC table
Rationale of the intervention Dynamic model
Intervention plan Operational plan
Implementation
New workshop: Evaluation + Planning Next Cycle

Social Medicine (www.socialmedicine.info) - 108 - Volume 6, Number 2, June 2011
The Cuban government has constructed a policyframework which has enabled substantial progressin population health over the last 50 years.8,9 Localhealth services have developed many linkages withcommunity organizations.10,11,12 Many projectshave managed to avoid the risks of paternalism andbureaucracy by developing truly participatorystyles of leadership.13,14,15 However, in general theresults of community participation in health havebeen somewhat mitigated. Opportunities to allowfor participation in health decisions are not fullyexploited. Local health planning does not consist-ently involve other social sectors nor does it alwaysinclude participation by formal and informal com-munity leaders.16
In collaboration with the Institute of Hygieneand Epidemiology (INHEM) and the Cuban Minis-try of Health, we set out to find ways of addressingthese problems. We hypothesized that greater com-munity participation in planning and evaluationwould lead not only to more realistic and feasibleplans but also to more active, sustained communityparticipation in the implementation of the proposedinterventions. The result, finally, would be im-proved health outcomes. Increased participationreinforces a sense of community ownership ofhealth activities which, indirectly, ensures that the-se initiatives are more sustainable.
Three municipalities were involved in this firststage. Dragones is located in the Centro Habanamunicipality of Centro Habana, a commercial areawithin the capital city. With 30,000 inhabitants in0.5 km², it is one of the country’s most denselypopulated areas. La Sierrita is located in the centerof Cuba in the municipality of Cumanayagua, prov-ince of Cienfuegos. This is a rural area with nineworking-class settlements at the foot of the Guamu-haya mountains. The main economic activities arecattle-raising and coffee-growing. People’s CouncilNo. 5 is in the municipality of Las Tunas, capital ofLas Tunas province. With a population of 25,000, itforms an urban area in the eastern region of Cuba.The main economic activity is small industry.
By the end of 2010 seven workshops had takenplace (one in 2008, three in 2009, three in 2010)covering four full planning—implementation—evaluation cycles; three cycles were in progress.
Examples of the methodology in CubaThe various steps of the CPPE methodology can
be illustrated using the models and plans developedin Cuba.
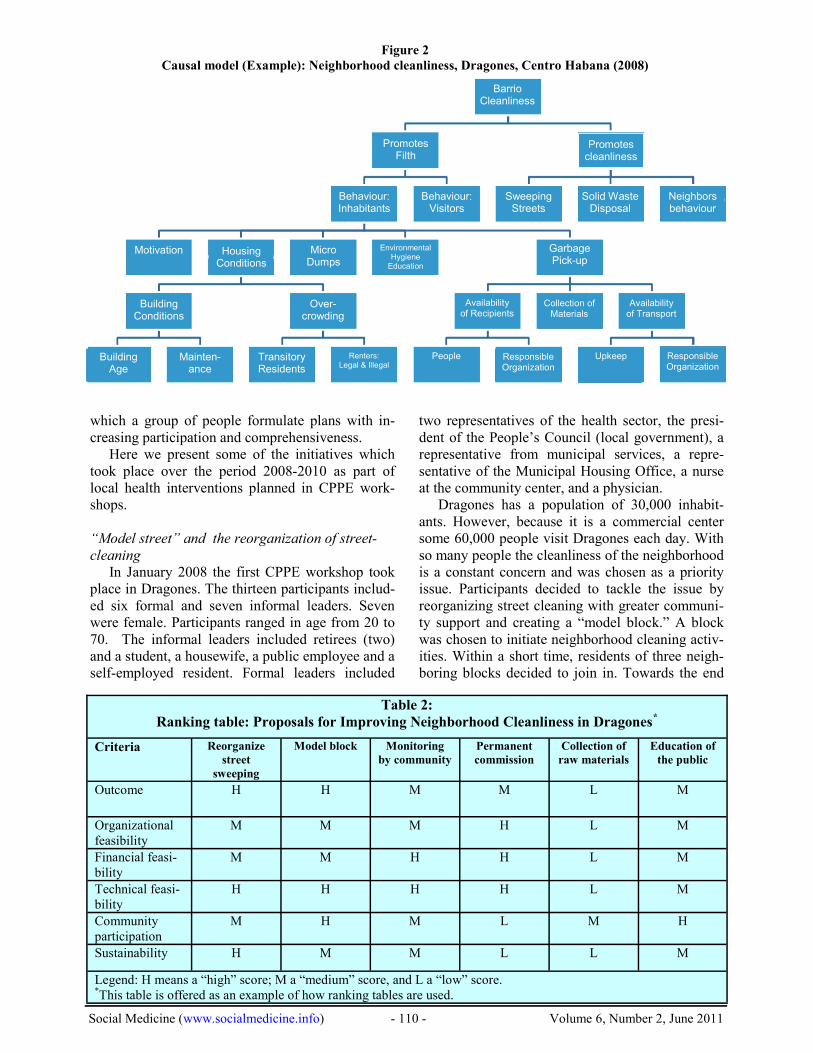
In order to select interventions a causal model isbuilt based on an analysis of community problems.(Figure 2) During a brainstorming session, partici-pants identify the main causes which ensure or af-fect health in their neighborhood or community.First the direct causes of potential problems aredetermined, followed by an exploration of the fac-tors which favor these causes. Depending on theirparticular needs, participants can subdivide certainparts of the model for further in-depth analysis. Afull causal model can be quite extensive. Figure 2shows one part of the analysis of neighborhoodcleanliness undertaken in Dragones, viz. how thebehavior of the inhabitants affects cleanliness.
A lack of comprehensiveness is a recurringproblem in program planning and evaluation; thiscan have major consequences. Proposals risk notbeing applicable because they do not take into ac-count a series of existing conditions and sensitivi-ties. CPPE can help reduce these risks because thecausal model helps explore the complexity of theproblems and identify possible solutions. Discus-sion makes for better understanding of how differ-ent people have different perceptions of the prob-lem. This enables group identification of core tar-gets for intervention.
In principle the team works with available infor-mation. Most elements of the problem can be iden-tified using the participants’ pre-existing know-ledge. Some causes can be put forth as hypothesesand, if necessary, verified with additional infor-mation (quantitative and qualitative) before pro-ceeding with the planning stage.
Table 1: Synopsis of Work in Cuba (2008-2010)Location 2008 2009 2010
Dragones Planning &Implementation
Evaluation (of the previ-ous year), Planning &Implementation
Evaluation (of the previ-ous year), Planning &Implementation
Sierritas Planning &Implementation
Evaluation (of the previ-ous year), Planning &Implementation
Las Tunas Planning &Implementation
Evaluation (of the previ-ous year), Planning &Implementation

Social Medicine (www.socialmedicine.info) - 109 - Volume 6, Number 2, June 2011
The ranking table is used to select interventions.Participants define selection criteria: the im-portance of the outcome, its weak points, the poten-tial to reduce inequities in the community, the de-gree to which participation is fostered, etc. The par-ticipants then choose the most appropriate interven-tions to solve the selected problem. With the rank-ing table, each criteria is analyzed to see if it ap-plies to the proposed intervention, using gradesHigh (H), Medium (M) and Low (L). Bearing inmind the prioritization criteria, those interventionswith the greatest number of High and least numberof Low grades are highlighted. The selection tableensures consistent focus when selecting possibleinterventions and helps reach agreement amongparticipants on manageable proposals. Table 2demonstrates how proposals to make a healthierneighborhood were ranked. Once the ranking iscomplete, the group decides which interventionsshould be carried out.
The first step of the planning stage is to identifywhat is needed to implement each individual inter-vention. To do this HIPPOPOC* table is made up.Inputs (IP) are the elements necessary for imple-mentation of the intervention (e.g. budget, materialresources, human resources, etc.). Processes (P)refer to the actions which must be undertaken toachieve the desired result. Outputs (OP) are theimmediate results of these actions while Outcomes(OC) are changes induced by the project. Figure 3shows the HIPPOPOC table which was completedfor a project reorganizing street sweeping inDragones, Centro Habana.
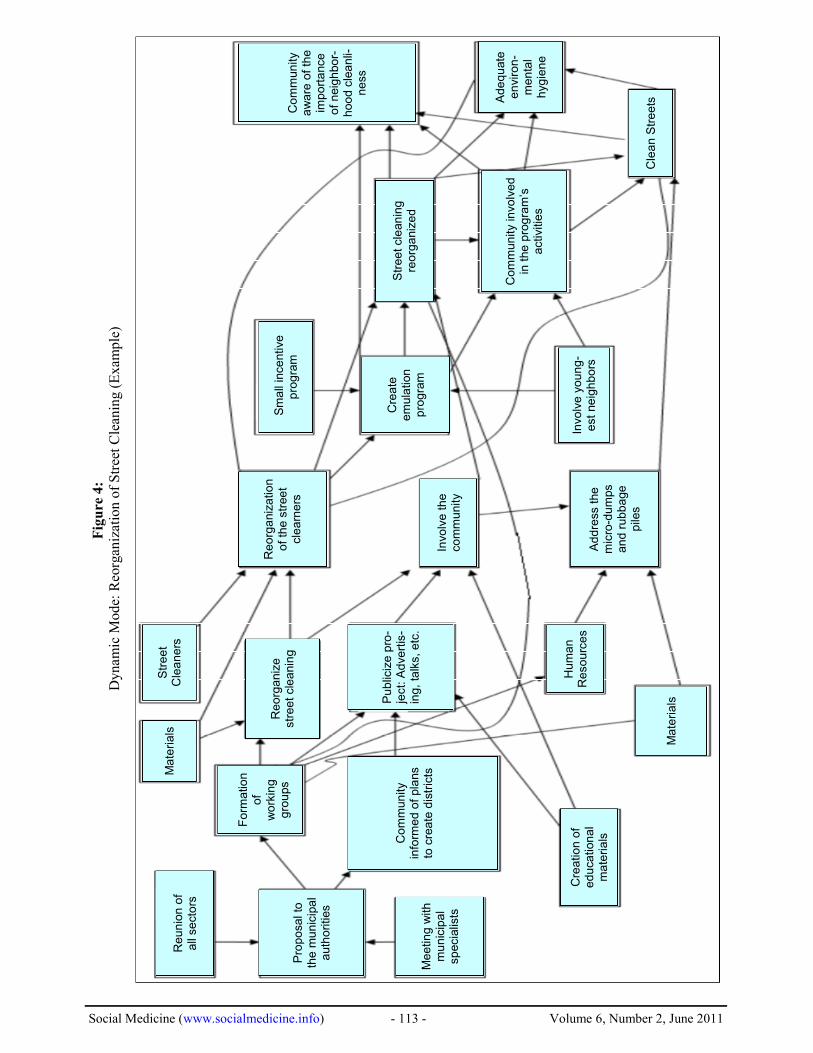
The following step, the dynamic model, repre-sents the core of the planning stage. The dynamicmodel provides a graphic representation of the logi-cal progression of the project. (Figure 4) It repre-sents how participants visualize the project devel-oping from the inputs, through a succession of pro-cesses, to achieve operational objectives (the inter-vention’s outputs) and finally the desired outcomes,directly related to the intervention) and finally thedesired impacts. The dynamic model is constructedfrom right to left, beginning with the impacts, thenthe outputs, the processes and—on the left—theinputs. Sometimes, during the elaboration of thedynamic model, it is necessary to go back and re-visit the HIPPOPOC table. This is perfectly ac-ceptable.
This approach makes it possible to identify thecrucial steps in project implementation. It clarifiesthe sequence of activities and allows for structuredmonitoring and evaluation during project imple-mentation.
In the final step, estimates of the time needed tocomplete each activity are noted in the model eitherwithin the activities box or along side the arrows.(Figure 4) Having completed these steps, it is nowtime to prepare for the operational stage.
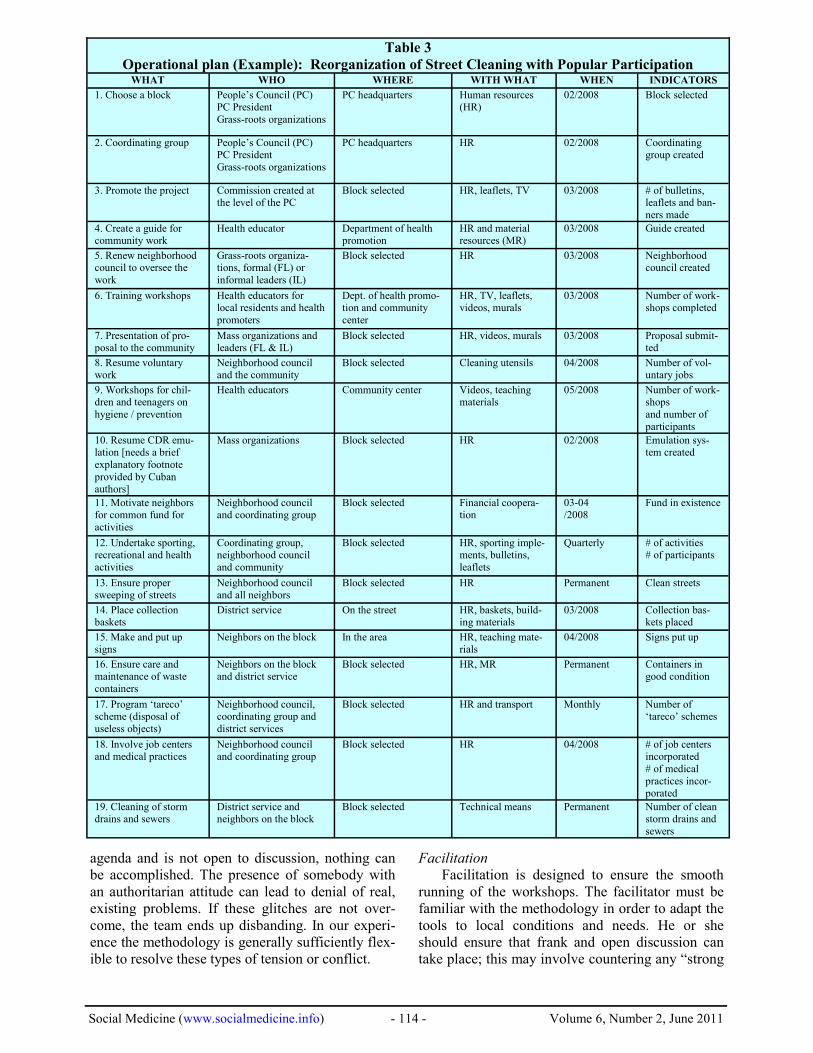
Once a consensus has been reached on the over-all process, participants translate the model into anoperational plan which delineates activities, re-sources, implementation dates, and responsible per-sons. This plan must provide detailed answers tothe basic elements such as: What? Who? Where?When? With what (resources)? Why (evaluationmeasures)? (Table 3) Lastly, participants nominatea coordinating team which is responsible to ensurethe plan is followed.
Initiatives in the period 2008-2010In Dragones, Centro Habana, three CPPE cycles
have already taken place, and the process now hasconsiderable momentum. In part, this is becauseparticipatory projects had already been undertakenin Dragones; the pre-existing community centermaintained and strengthened its leadership. Thanksto CPPE, a greater and more diverse popular in-volvement was achieved. The consensus among theextended coordinating group is that the method al-lowed them to be better organized. They managedto work more systematically and with greater in-volvement by individuals. Coordination with localgovernment also improved.
In Cumanayagua and Las Tunas too, communityparticipation and local initiative were both en-hanced. However, these communities had less pre-vious experience in community participation. Onlytwo years into the project, results in these two lo-calities are not as far-reaching.
As detailed below, some activities were under-taken by either the health services or some otherbranch of the municipal government with only lim-ited community involvement. Other initiatives man-aged to develop genuine forms of social care orchanged hygienic / social health determinants withthe community playing a prominent role. The vastmajority of those involved directly or indirectly inthese processes confirmed their satisfaction andenthusiasm with the level of engagement theythemselves felt had been developed.
Even with a favorable context and committedindividuals, participatory processes are not linear.They require time to evolve and there are momentsof both progress and retreats. These processes can-not be forced; the dynamics of community engage-ment foster growing consciousness of the most ap-propriate organizational forms. CPPE merely offersa structured way for this constructive process by* (H)-IP-P-OP-OC: Inputs-Processes-Outputs-Outcomes
Social Medicine (www.socialmedicine.info) - 110 - Volume 6, Number 2, June 2011
which a group of people formulate plans with in-creasing participation and comprehensiveness.
Here we present some of the initiatives whichtook place over the period 2008-2010 as part oflocal health interventions planned in CPPE work-shops.
“Model street” and the reorganization of street-cleaning
In January 2008 the first CPPE workshop tookplace in Dragones. The thirteen participants includ-ed six formal and seven informal leaders. Sevenwere female. Participants ranged in age from 20 to70. The informal leaders included retirees (two)and a student, a housewife, a public employee and aself-employed resident. Formal leaders included
two representatives of the health sector, the presi-dent of the People’s Council (local government), arepresentative from municipal services, a repre-sentative of the Municipal Housing Office, a nurseat the community center, and a physician.
Dragones has a population of 30,000 inhabit-ants. However, because it is a commercial centersome 60,000 people visit Dragones each day. Withso many people the cleanliness of the neighborhoodis a constant concern and was chosen as a priorityissue. Participants decided to tackle the issue byreorganizing street cleaning with greater communi-ty support and creating a “model block.” A blockwas chosen to initiate neighborhood cleaning activ-ities. Within a short time, residents of three neigh-boring blocks decided to join in. Towards the end
Table 2:Ranking table: Proposals for Improving Neighborhood Cleanliness in Dragones*
Criteria Reorganizestreet
sweeping
Model block Monitoringby community
Permanentcommission
Collection ofraw materials
Education ofthe public
Outcome H H M M L M
Organizationalfeasibility
M M M H L M
Financial feasi-bility
M M H H L M
Technical feasi-bility
H H H H L M
Communityparticipation
M H M L M H
Sustainability H M M L L M
Legend: H means a “high” score; M a “medium” score, and L a “low” score.*This table is offered as an example of how ranking tables are used.
BarrioCleanliness
PromotesFilth
Solid WasteDisposal
Promotescleanliness
SweepingStreets
UpkeepResponsibleOrganization
Collection ofMaterials
GarbagePick-up
Availabilityof Recipients
People
Behaviour:Inhabitants
Renters:Legal & Illegal
Over-crowding
EnvironmentalHygiene
Education
MicroDumps
HousingConditions
Motivation
BuildingConditions
TransitoryResidents
Mainten-ance
BuildingAge
Neighborsbehaviour
Availabilityof Transport
ResponsibleOrganization
Behaviour:Visitors
Figure 2Causal model (Example): Neighborhood cleanliness, Dragones, Centro Habana (2008)

Social Medicine (www.socialmedicine.info) - 111 - Volume 6, Number 2, June 2011
of 2008 an additional two blocks had been incorpo-rated.
The model block program was particularly suc-cessful in terms of community action. Volunteerscleaned up their blocks and made them more attrac-tive. This was a joint effort between the communi-ty, the health sector, and the municipal government.The initial leadership came from the health sector;this changed as the project continued. A culture ofcollaboration developed in which the communityplayed the major role; between 50 and 80 peopletook part in each of the activities.
In order to repairs the façades and houses in themodel blocks, the municipal government providedresidents with cement, paint, doors, windows, etc.An agreement was negotiated so that 80% of theresources were government-supplied and 20% wereprovided by the community. Project activities werecharacterized by spontaneity and a spirit of collabo-ration among residents and activists from local or-ganizations.
In addition to cleaning and beautification,health promotion and prevention activities tookplace. Recreational and sporting activities drew bigcrowds.
The second CPPE workshop (2009) decided toextend the “model block” project by creating“model streets.” At the initiative of the communitymaterials were provided to undertake home repairs.All materials were stored at designated sites andguarded by the neighbors themselves. Someonewas chosen to distribute the materials according toan agreed-upon list of needs. The individuals cho-
sen for this position were replaced twice because ofcommunity dissatisfaction.
Local artists from different disciplines were in-corporated into the project. They helped decoratethe streets, designed community logos, held work-shops, and organized exhibitions.
In December 2009 local government—whichhad actively participated in these activities—decided to give the project a workspace. At a meet-ing involving all community leaders a CommunityCenter for Neighborhood Development was creat-ed. Its purpose was to promote community partici-pation in the solution of local problems.
In February 2010 the third workshop took place.The evaluation noted that community participationin project activities was gradually increasing. Adecision was made to focus on issues affecting“Neighborhood Health.” The result was a reorgani-zation of family medical practices in order tostrengthen the relationship of the health teams withthe community. The plan includes using volunteersto renovate the clinics, a discussion concerning theroles and functions of health teams, health promotertraining, the identification of learning needs, and aproposal to proclaim these practices “model medi-cal practices.”
From January 2008 to date (end of 2010), fulfill-ment of the operational plan has been analyzed inmonthly meetings; these have been attended bycommunity members and representatives of thevarious municipal institutions. Attendance has beenhigh. The current coordinating group includes all itsoriginal members as well as additional, more recentrecruits
Inputs Processes Outputs Outcomes
Work equipment:brooms, shovels,gloves
Street cleaners Minimum budget
for material incen-tives
Materials for edu-cational work
Community humanresources
Time
Information to the community aboutstreet sweeping reorganization by district
Meeting with municipal specialists Proposal to the Municipal Directorate of
Community Services Proposal to the Provincial Directorate of
Community Services:1. Meeting of all sectors involved in the
project2. Create an emulation system3. Involve the youngest through educa-
tional talks4. Involve the whole community5. Incorporate work centers6. Promote the project through education-
al talks, transmission of messages inthe districts
7. Seek solution to micro-dumps
Reorganized streetsweeping
Clean streets Community
awareness of theimportance ofneighborhoodcleanliness
Adequate environ-mental hygiene
A healthier life Improved health
Figure 3HIPPOPOC table: Reorganization of Street Cleaning with Greater Community Participation

Social Medicine (www.socialmedicine.info) - 112 - Volume 6, Number 2, June 2011
The Experienced Youngsters Social Club*
In 2009 the Las Tunas community decided tocreate a comprehensive program for the elderly.There had been a similar program in the past but ithad fallen into serious decline. It was decided torenovate a space for social activities and talks.Work centers were recruited to provide lunches forelderly people who lived alone. Both formal andinformal social care networks were set up to helpneedy nuclear families. Elderly people from otherdistricts got involved in the workouts (gym, club)and social activities of the Club. It evolved into amovement of friends which has spread throughoutthe municipality. The active collaboration betweenthe population and different sectors of the munici-pal government has been most beneficial for theelderly.
In April 2010 Las Tunas created an environmen-tal program: “A Community of Gardens means aHealth Community.”† The aim is to involve fami-lies and work centers in the cleaning and plantingof yards and plots of land.
Health convoysThe rural area of Cumanayagua had more lim-
ited results with CPPE. The group decided to or-ganize health convoys to isolated mountainous set-tlements. The goal was to provide these remote are-as with better access to prevention and health pro-motion campaigns, general medical and dental care,and clinical laboratory services. Three training ses-sions were held for health promoters, who then rep-licated the trainings in schools, work centers, com-munity centers, and settlements. In 2010 the initia-tive was expanded to include more sustained follow-up of chronic patients.
These programs primarily involved the healthsector; there was relatively little input from thecommunity itself.
Discussion on methodological approachThe application of the same tools in different
contexts provided important insights. In general,the best results were obtained where the CPPE ra-tionale and conditions were most closely respected.But even errors helped clarify certain methodologi-cal questions. Below we present some of the les-sons learned.
Rationale and sequence of the methodIt is important to complete all steps without
omitting any of the stages. There may well be other,possibly better ways of performing the analysis of
the situation, selecting interventions and planningthem in a structured manner, but each of these stag-es is required. The tools reinforce a systematic ap-proach and ensure everybody’s participation.
The time required for each stage can vary. In ourexperience a workshop never lasts less than fourdays. Two days are needed for analyzing the prob-lems and selecting interventions, and an additionaltwo days are required for developing the rationaleof the intervention and formulating the plan. Thisinitial work results in some time savings for laterworkshops. However, additional time is neededlater on for evaluation. If workshops are too short,the various objectives will not be met in terms ofthe analysis and the plan, nor will it be possible tobuild a stronger team to ensure follow-up and mo-bilization throughout the year.
The collective planning process must be basedon the specific realities of the location; it needs totake into account existing possibilities and limita-tions in terms of people, resources, and time. Ascommunity leaders become more capable of takinginitiative, community empowerment is strengthenedand the organized community establishes more ef-fective links—at times collaborative, sometimesconflictive—with government sectors.
Iterative work involving regular evaluation and(re-)planning workshops—annual ones work best inour experience—helps to maintain mobilizationover time. Every workshop serves to renew interestin participation and mobilization.
ParticipantsFamiliarity with the local area is essential to
ensure that formal and informal leaders truly repre-sent the various informal groups within the commu-nity. Participation by representatives of the variouscommunity stakeholders ensures the pluralist natureof planning and evaluation.17
Pluralist approaches have been studied in theevaluation of state-run activities in the UnitedStates and Europe at the end of the 80s,(e.g. in eval-uating improvements in underprivileged neighbor-hoods).18,19 In the Cuban context the presence andcommitment of formal sectors of local governmentis relatively easy to obtain. There are no fundamen-tal contradictions of interest between working-classsectors and the State. Institutions understand theirresponsibility towards community health and itsdeterminants.
But nothing is ever quite so simple. Over theyears we have seen what happens when the meth-odology is not followed. If a local government rep-resentative cannot discuss matters with residents asan equal, this hinders development of any proposal.Similarly, if a leader comes along with a pre-set
*Club Social Juventud Acumulada†Comunidad sembrada, salud garantizada
Social Medicine (www.socialmedicine.info) - 113 - Volume 6, Number 2, June 2011
Re
un
ion
of
all
se
cto
rs
Ad
dre
ssth
em
icro
-du
mps
an
dru
bb
age
pile
s
Invo
lve
the
co
mm
unity
Invo
lve
you
ng
-e
st
ne
igh
bo
rs
Cre
ate
em
ula
tion
pro
gra
m
Re
org
aniz
atio
no
fth
estr
ee
tcle
arn
ers
Sm
all
ince
ntive
pro
gra
m
Str
ee
tcle
an
ing
reo
rga
niz
ed
Co
mm
un
ity
invo
lve
din
the
pro
gra
m’s
activi
ties
Cle
an
Str
ee
tsAd
eq
uate
en
viro
n-
me
nta
lh
ygie
ne
Co
mm
un
ity
aw
are
of
the
imp
ort
ance
of
neig
hbo
r-h
oo
dcle
an
li-n
ess
Me
etin
gw
ith
mu
nic
ipa
lsp
ecia
lists
Cre
atio
no
fe
du
cation
al
ma
teria
ls
Hu
ma
nR
eso
urc
es
Ma
teri
als
Fo
rma
tion
of
wo
rkin
gg
rou
ps
Ma
teri
als
Str
ee
tC
lea
ne
rs
Re
org
aniz
estr
ee
tcle
anin
g
Pu
blic
ize
pro
-je
ct:
Ad
vert
is-
ing
,ta
lks,e
tc.
Co
mm
un
ity
info
rme
do
fpla
ns
tocre
ate
dis
tric
ts
Pro
po
salto
the
mu
nic
ipa
la
uth
orities
Fig
ure
4:
Dyn
amic
Mo
de:
Reo
rgan
izat
ion
of
Str
eet
Cle
anin
g(E
xam
ple
)
Social Medicine (www.socialmedicine.info) - 114 - Volume 6, Number 2, June 2011
agenda and is not open to discussion, nothing canbe accomplished. The presence of somebody withan authoritarian attitude can lead to denial of real,existing problems. If these glitches are not over-come, the team ends up disbanding. In our experi-ence the methodology is generally sufficiently flex-ible to resolve these types of tension or conflict.
FacilitationFacilitation is designed to ensure the smooth
running of the workshops. The facilitator must befamiliar with the methodology in order to adapt thetools to local conditions and needs. He or sheshould ensure that frank and open discussion cantake place; this may involve countering any “strong
WHAT WHO WHERE WITH WHAT WHEN INDICATORS
1. Choose a block People’s Council (PC)PC PresidentGrass-roots organizations
PC headquarters Human resources(HR)
02/2008 Block selected
2. Coordinating group People’s Council (PC)PC PresidentGrass-roots organizations
PC headquarters HR 02/2008 Coordinatinggroup created
3. Promote the project Commission created atthe level of the PC
Block selected HR, leaflets, TV 03/2008 # of bulletins,leaflets and ban-ners made
4. Create a guide forcommunity work
Health educator Department of healthpromotion
HR and materialresources (MR)
03/2008 Guide created
5. Renew neighborhoodcouncil to oversee thework
Grass-roots organiza-tions, formal (FL) orinformal leaders (IL)
Block selected HR 03/2008 Neighborhoodcouncil created
6. Training workshops Health educators forlocal residents and healthpromoters
Dept. of health promo-tion and communitycenter
HR, TV, leaflets,videos, murals
03/2008 Number of work-shops completed
7. Presentation of pro-posal to the community
Mass organizations andleaders (FL & IL)
Block selected HR, videos, murals 03/2008 Proposal submit-ted
8. Resume voluntarywork
Neighborhood counciland the community
Block selected Cleaning utensils 04/2008 Number of vol-untary jobs
9. Workshops for chil-dren and teenagers onhygiene / prevention
Health educators Community center Videos, teachingmaterials
05/2008 Number of work-shopsand number ofparticipants
10. Resume CDR emu-lation [needs a briefexplanatory footnoteprovided by Cubanauthors]
Mass organizations Block selected HR 02/2008 Emulation sys-tem created
11. Motivate neighborsfor common fund foractivities
Neighborhood counciland coordinating group
Block selected Financial coopera-tion
03-04/2008
Fund in existence
12. Undertake sporting,recreational and healthactivities
Coordinating group,neighborhood counciland community
Block selected HR, sporting imple-ments, bulletins,leaflets
Quarterly # of activities# of participants
13. Ensure propersweeping of streets
Neighborhood counciland all neighbors
Block selected HR Permanent Clean streets
14. Place collectionbaskets
District service On the street HR, baskets, build-ing materials
03/2008 Collection bas-kets placed
15. Make and put upsigns
Neighbors on the block In the area HR, teaching mate-rials
04/2008 Signs put up
16. Ensure care andmaintenance of wastecontainers
Neighbors on the blockand district service
Block selected HR, MR Permanent Containers ingood condition
17. Program ‘tareco’scheme (disposal ofuseless objects)
Neighborhood council,coordinating group anddistrict services
Block selected HR and transport Monthly Number of‘tareco’ schemes
18. Involve job centersand medical practices
Neighborhood counciland coordinating group
Block selected HR 04/2008 # of job centersincorporated# of medicalpractices incor-porated
19. Cleaning of stormdrains and sewers
District service andneighbors on the block
Block selected Technical means Permanent Number of cleanstorm drains andsewers
Table 3Operational plan (Example): Reorganization of Street Cleaning with Popular Participation

Social Medicine (www.socialmedicine.info) - 115 - Volume 6, Number 2, June 2011
personalities.” Conflicts are inevitable in this typeof workshop; in fact, they are healthy. If well man-aged, conflicts offer the opportunity to deepen un-derstanding of a problem and find better solutions.The consensus reached following debate will al-ways be better than the original proposal.
One discussion on medical care in a neighbor-hood began with the (superficial) conclusion that“all is well.” Eventually one resident brought up aseries of criticisms, contradicting one of the formalleaders. Following the timely intervention of thefacilitator, the leader was able to (re)learn that truesocial commitment does not consist in minimizingproblems, but rather in investigating them thor-oughly and mobilizing the community to resolvethem. From that point on, the discussion opened upmuch more, furthering understanding of the prob-lems. The facilitator had performed her role proper-ly.
The facilitator is perhaps the most importantperson in the workshop. He or she must ensure thateverybody has an equal opportunity to participate.By actively listening and asking questions, facilita-tors show the group that each person’s contributionis important, helping everyone develop communi-cation skills and promoting discussion. In this re-gard the facilitator also plays a key role in buildinga team which can lead community work. Appropri-ate facilitation reinforces this person’s leadership.They must have the capacity to listen, summarize,mobilize, and bring more people into the action andto the local organization.
Selection of the facilitator is crucial. They canbe a community member or someone from outside.Even if the facilitator is from the community, he orshe must be neutral regarding participants’ opin-ions.
It is necessary to spend enough time for prepara-tion of the workshop and to get to know the com-munity’s background. If the facilitator is from out-side the community, a preliminary introduction tothe situation consists of reviewing relevant docu-ments and holding interviews to obtain informationfrom those involved in the community and its insti-tutions. In this way the facilitator gains differingperceptions about the nature and magnitude of theproblems and their causes. He or she learns of pos-sible interventions already present in the area andidentifies potential participants in the workshopwho could assist with in-depth analysis.
For facilitation to work, it is important to clearlyexplain the objectives and methodology of eachstep. Time needs to be set aside for questions. Itmay be necessary to repeat these steps until every-one is in agreement. It is important to check fre-
quently that everyone is following the progress ofthe workshop. All participants should be treated asequals, be they Mayor or housewife. It is essentialthat the facilitator not take sides or actively takepart in discussions among participants, although heor she can always suggest alternatives. For theworkshops to run smoothly, the schedule should notbe too flexible. Lastly, it is important for a commu-nity not to keep changing facilitators from year toyear. If a change is necessary, it must be well pre-pared for.
If the objective is to reinforce and extend thisparticipatory method, then facilitator training is acore task. In Cuba we are preparing a facilitatortraining program and have produced a facilitationguide. But workshop training has its limitations;facilitation cannot be learned by theory alone. Theskill is gained only by taking part in workshop fa-cilitation in the community.
Conclusions and outlookThree years’ experience has demonstrated the
potential of this methodology to promote participa-tion and empowerment in the Cuban context.20
In putting the right to health into practice, thereis a synergy between the Cuban State and grass-roots organizations. A variety of organizations(women’s, workers’, youth, neighborhood, etc.)have made and continue to make significant contri-butions to the transformation of the country.21-25
The political nature of the State and the actions oflocal government lead to closer popular identifica-tion with social policies despite existing materialconstraints and deficiencies. We hope to continuethis work in Cuba over the next few years, and tocontinue learning. Additionally, in coordinationwith the Ministry of Health and with support fromPAHO and the Belgian NGO INTAL, facilitatorinstruction is being extended with the hope of en-suring adequate levels of training in this essentialresource.
CPPE is a comprehensive method of participa-tion which requires and enables the free discourseof participants and in-depth group discussions. Thisleads to increased self-esteem and self-fulfillment,as well as greater commitment to the community.CPPE is very flexible in that it can be applied to awide range of situations (services, programs andprojects) and at various levels (national, regional,municipal and local). During 2010, in a study ofsocial determinants of neglected diseases and otherpoverty-related illnesses in Yucatán, Mexico, weintroduced CPPE as a method of participatory re-search. We demonstrated that for any communityintervention it was imperative to directly and ac-

Social Medicine (www.socialmedicine.info) - 116 - Volume 6, Number 2, June 2011
tively involve communities in analyzing their reali-ty and in proposing measures and interventions af-fecting their own lives. We also showed that CPPEcan be an appropriate tool to do this26. In mid-2010an exchange was begun with the People’s HealthMovement-Latin America (PHM-LA) about experi-ences in participation and empowerment in order tocontinue learning and participated in strengtheningthis movement.27
The right to health in other contextsThe Cuban State’s policy on health, despite any
constraints it may face, is based on defending theright to health of all Cubans. To achieve this objec-tive there exists a synergy between the State andgrass-roots organizations.13 In countries where thereis a major gap between the interests of the eliteswhich dominate public institutions and the needs ofcommunities, any negotiation or search for consen-sus on how best to move forward in exercising theright to health inevitably confronts important limi-tations. In these cases, claim-holders seek otherways of pressuring the political authorities (duty-bearers) to listen to them and respect their rights.11
Through demands and protests they seek a moreadvantageous negotiating position. In these “other”contexts—where there may be a greater conflict ofinterest between state and society—this same plan-ning exercise can help communities identify realcontradictions, better understand to whom theyshould address their demands, and how to progresstowards the realization of their right to health.
A rights-based approach does not simply meanthe right to something. It implies the possibility andobligation to claim this right from those who havethe power and duty of ensuring it. This involves astrategy of community empowerment. The planningexercise can be set up to see how best to defendpopular interests or conquer (a share of) power.
The concepts of obligations, duties, and respon-sibilities of the State are crucial to community em-powerment. They allow it to make demands andnegotiate the necessary changes with those who arein power. If those responsible do not act, group ac-tion might be necessary before success is achieved.
On the other hand, nobody can be held responsi-ble if conditions make it impossible for them tocomply. The person must first accept responsibility,have the necessary authority to act, and have accessto and control over resources. A “capacity analysis”can clarify which individuals or institutions shouldand can act in each of the actions required. The re-sult can be an appendix to the proposed interven-tion plan, listing key individuals or institutions tocarry out the proposed objectives.28 This capacity
analysis can be an important complement to CPPEsince it focuses social mobilization on the relevantgovernmental authorities. To the extent that morecommunities and organizations are successful indemanding their rights, the movement for the rightto health becomes stronger and more successful.
Practice will continue to enrich this approach asit is applied in diverse situations in different coun-tries, regions, and locales. When circumstances al-low, this collective planning exercise not only leadsto greater commitment and better organization atgrass-root level, but also to greater political aware-ness.
AcknowledgementsWe would like to thank all participants and sup-
port teams in the communities involved in the pro-jects mentioned in this article for their selfless par-ticipation with the sole aim of boosting health de-velopment in their communities.
References
1. Rifkin S. Equity, empowerment and choice: fromtheory to practice in public health. London Schoolof Economics, United Kingdom. Presentation madeat Forum 9, Mumbai, India,12-16 September 2005.
2. Rifkin S, Pridmore P. Partners in Planning. London:Macmillian, TALC. 2001.
3. Laverack G. Using a domains approach to buildcommunity empowerment. Commun Dev J 2005.(www.oup.co.uk/journals/cdj/advance, accessed on11 March 2005).
4. Pérez D, Lefévre P, Romero MI, Sánchez L, De VosP and Van der Stuyft. Augmenting frameworks forappraising the practices of community-based healthintervention. Health Policy and Planning HealthPolicy and Planning 2009; 24(5): 335-341.doi:10.1093/heapol/czp028.
5. Urban Health Study Group,Atma Jaya University ofIndonesia; Department of Agricultural Education,University of The Philippines at Los Baños; Nutri-tion Institute of the Federal University of Rio deJaneiro, Brazil
6. International Fund for Agricultural Development(IFAD) (Ethiopia, Kenya, Mali, Uganda, Seychelles,Tchad), United Nations Children’s Education Fund(UNICEF), Save the Children Fund (SCF), MedicalMission Action (MEMISA), etc.
7. Greenwood, D. J. & Levin, M., Introduction to ac-tion research: social research for social change,Thousand Oaks, Calif.: Sage Publications, 1998.
8. De Vos P, De Ceukelaire W, Malaise G, Pérez D,Lefèvre P, Van der Stuyft P. Health through peo-ple’s empowerment: a rights-based approach to par-ticipation. Health and Human Rights 2009;11(1):23-35.

Social Medicine (www.socialmedicine.info) - 117 - Volume 6, Number 2, June 2011
9. Constitution of the Republic of Cuba (1992).www.cubanet.org/ref/dis/const_92_e.htm.
10. De Vos P. No one left abandoned: Cuba’s nationalhealth system since the 1959 revolution. Internation-al Journal of Health Services 2005;35:189–207.
11. Delgado G. Desarrollo histórico de la salud públicaen Cuba. Revista Cubana de Salud Pública 1998;24(2):110–118.
12. Feinsilver J. M. Healing the masses: Cuban healthpolitics at home and abroad. Berkeley, University ofCalifornia Press, 1993.
13. Reyes-Alvarez I, Sanabria Ramos G, Medina Gon-dres Z, Baez-Dueñas RM. Metodología para la ca-racterización de la participación comunitaria en sa-lud. Revista Cubana de Salud Pública 1996;22(1):75–84.
14. Ferrer-Ferrer L, Alfonso-Sagué K, Bonet-Gorbea M,et al. Intervenciones comunitarias contra enfermeda-des crónicas no transmisibles en el consejo popularDragones. Revista Cubana de Salud Pública 2006;32(3).www.imbiomed.com.mx/1/1/articulos.php?mehod=showDetail&id_articulo=38803&id_seccion-=1250&id_ejemplar=4003&id_revista=79
15. Sanabria Ramos G. Participación social en el campode la salud. Revista Cubana de Salud Pública2004;30(3). http://redalyc.uaemex.mx/redalyc/pdf/214/21430305.pdf.
16. Sosa I. Percepción sobre Análisis de Situación deSalud en un Consejo Popular del municipio CentroHabana en 2008. Revista Cubana de Higiene y Epi-demiología 2011 in press.
17. Lefèvre P. Acteurs et évaluation de projets de déve-loppements. Vers une approche pluraliste de l’éva-luation. Universidad Libre de Bruselas 1999 (p.115-117).
18. Guba EG, Lincoln YS. Fourth Generation Evalua-tion. Beverly Hills, Sage Publication 1989.
19. Monnier E. Evaluations de l’action des pouvoirspublics. Paris, Economica, 1987.
20. Dilla H, Fernandez A, Castro M. Movimientos ba-rriales en Cuba: Un análisis comparativo. In: Váz-quez A, Davalos R (eds). Participación social: Desa-rrollo urbano y comunitario:1er taller de desarrollourbano y participación. Havana, Universidad de LaHabana. Facultad de filosofía e Historia/Departamento de Sociología, 1996.
21. Dilla H, Fernandez A, Castro M. Movimientos ba-rriales en Cuba: Un análisis comparativo. In: Váz-quez A, Davalos R (eds). Participación social: Desa-rrollo urbano y comunitario:1er taller de desarrollourbano y participación. Havana, Universidad de LaHabana. Facultad de filosofía e Historia/Departamento de Sociología, 1996.
22. Valdes J. Notas sobre Poder Local, movimiento co-munitario y democracia en Cuba. In: Davalos R,Basail A. Desarrollo urbano: Proyectos y experien-cias de trabajo. 2do taller de desarrollo urbano yparticipación. Havana, Universidad de La Habana,Facultad de filosofía e Historia/Departamento deSociología, 1997.
23. Rojas-Ochoa F, Lopez-Pardo CM. Economy, poli-tics and health status in Cuba. International Journalof Health Services 1997;27:791–807.
24. Serrano P. Cuban democracy does not stop at formalrepresentation. Interview with Ricardo Alarcón,2004. www.cubanismo.net/teksten_eng/democratie/interview_alarcon_ pr.htm.
25. Vazquez A, Davalos R. Comunidad y descentraliza-ción: Una reflexión desde los 90. In: Vázquez A,Davalos R (eds). Participación social: Desarrollourbano y comunitario: 1er taller de desarrollo ur-bano y participación. Havana, Universidad de LaHabana, Facultad de filosofía e Historia/Departamento de Sociología, 1996.
26. Centro de Investigaciones Regionales "Dr. HideyoNoguchi" Universidad Autónoma de Yucatán(UADY México) y el Institute of Tropical Medicine(ITM Bélgica). Estudio de los determinantes socia-les de las enfermedades desatendidas y otras enfer-medades relacionadas con la pobreza en AméricaLatina y el Caribe. Informe final. OPS/OMS Con-trato CS-10-01392. Septiembre 2010.
27. Steunfonds Derde Wereld - INTAL (2010) Rein-forcing the capacities of PHM - Latin America forbetter action towards the right to Health. In: Steun-fonds Derde Wereld, INTAL. DGCD-program 2011-2013, Empowerment for the Right to Health. (Part2, pp.99-112).
28. Jonsson U. An approach to human rights based pro-gramming in UNICEF (Eastern and Southern Afri-ca). SCN News 20, July 2000. ACC/SCN, Geneva,and UNICEF ESARO.


















