


Social Determinants of Health 101 - Advisory€¦ · operations, service offerings •Unsustainable...
47
Population Health Advisor Social Determinants of Health 101 Addressing patients’ non-clinical risk factors in ongoing management Darby Sullivan Senior research analyst [email protected]
Transcript of Social Determinants of Health 101 - Advisory€¦ · operations, service offerings •Unsustainable...

Population Health Advisor
Social Determinants
of Health 101Addressing patients’ non-clinical risk
factors in ongoing management
Darby Sullivan
Senior research analyst

© 2019 Advisory Board • All rights reserved • advisory.com
6
Get up to speed on two population health priorities
Two-part webconference series lays out path to success
Source: Population Health Advisor and Health Disparities Initiative interviews and analysis.
Targeted efforts drives societal shifts towards health equity
Building an
equitable, healthy society
Access the recording here.
Focusing efforts on historically
marginalized communities
Addressing structural inequalities
that impact health outcomes
Health Equity 101
Learn best practices to design a data-
driven framework to identify and prioritize
equity efforts across the system and
incorporate them into patient care.
Social Determinants of Health 101
Learn how to partner with community-
based organizations to provide quality
non-clinical support and impact
community economic strength.
Thursday, June 13th, 2019 • 1:00pmReview the webconference recording here.

© 2019 Advisory Board • All rights reserved • advisory.com
ROAD MAP7
The impact of the social determinants
of health1
2The role of community partnerships in addressing patients’ non-
clinical risk factors
3 Key considerations for promoting long-term sustainability

© 2019 Advisory Board • All rights reserved • advisory.com
8
Key drivers of risk are often non-clinical in nature
Must meet certain needs before care can inflect positive change
Source: McLeod, “Maslow’s Hierarchy of Needs,” Simply Psychology,
https://www.simplypsychology.org/maslow.html; Population Health Advisor interviews and analysis.
Applying Maslow's hierarchy of needs to population health management
Self-actualization
Esteem
Within a provider
organization’s
sphere of influence
Physiological
Belongingness
• Community
• Social relationships
• Trust
Safety
• Security
• Stability
• Law and order
• Food
• Shelter
• Warmth
© 2019 Advisory Board • All rights reserved • advisory.com
9
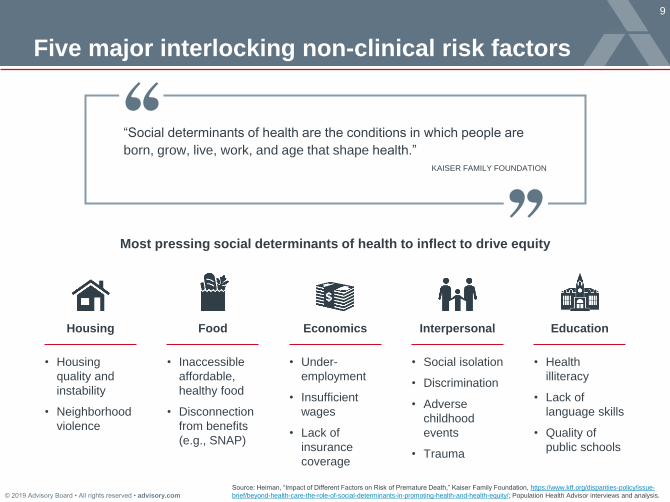
Five major interlocking non-clinical risk factors
Economics EducationInterpersonalFood Housing
• Under-
employment
• Insufficient
wages
• Lack of
insurance
coverage
• Health
illiteracy
• Lack of
language skills
• Quality of
public schools
• Social isolation
• Discrimination
• Adverse
childhood
events
• Trauma
• Inaccessible
affordable,
healthy food
• Disconnection
from benefits
(e.g., SNAP)
• Housing
quality and
instability
• Neighborhood
violence
Most pressing social determinants of health to inflect to drive equity
Source: Heiman, “Impact of Different Factors on Risk of Premature Death,” Kaiser Family Foundation, https://www.kff.org/disparities-policy/issue-
brief/beyond-health-care-the-role-of-social-determinants-in-promoting-health-and-health-equity/; Population Health Advisor interviews and analysis.
“Social determinants of health are the conditions in which people are
born, grow, live, work, and age that shape health.”
KAISER FAMILY FOUNDATION

© 2019 Advisory Board • All rights reserved • advisory.com
10
Undeniably critical impact on patients’ lives
Food Housing Interpersonal EducationEconomics
Patient
impact 66%
Food insecure
households had to
choose between
paying for food and
medical care
26-36Years reduced life
expectancy for
those experiencing
homelessness
26%Increased risk of
mortality resulting
from loneliness
9 yearsGap in life
expectancy for
those without a
high school
diploma vs. college
graduates
Greater mortality
risk for Medicaid
beneficiaries vs.
private insurance
2.13x
Scale of non-clinical challenges impact health systems’ financial strength
Pro
vid
er
impact
$155BAnnual health-
related costs
directly attributed to
food insecurity
1.8xMedian LOS for
patients
experiencing
homelessness
compared to those
with secure
housing
60%Higher risk of ED
utilization for
patients requiring
language services
$32KAverage per patient
cost for those with
inadequate health
literacy over three
years
Higher likelihood of
readmission for
patients dually-
enrolled in
Medicare and
Medicaid
24-67%
Source: See appendix for full sources; Population Health Advisor interviews and analysis.

© 2019 Advisory Board • All rights reserved • advisory.com
11
Social needs complicate clinical care and outcomes
Care teams unable to provide full range of services alone
Source: Heiman, “Impact of Different Factors on Risk of Premature Death,” Kaiser Family Foundation, https://www.kff.org/disparities-
policy/issue-brief/beyond-health-care-the-role-of-social-determinants-in-promoting-health-and-health-equity/; “Health Care’s Blind
Side,” Robert Wood Johnson Foundation, http://www.rwjf.org/en/library/articles-and-news/2011/12/health-cares-blind-side-unmet-
social-needs-leading-to-worse-heal.html; Population Health Advisor interviews and analysis.
Physicians reporting that unmet
social needs lead directly to
poorer health outcomes
85%
Physicians who are confident
in their ability to address
unmet social needs
20%
Interlocking social determinants of health inform clinical outcomes
20%
10%
30%
40%
Social and
environmental
factors
Health
care
Genetics
Individual
behavior
Impact of different factors on risk of
premature death

© 2019 Advisory Board • All rights reserved • advisory.com
12
Partner for sustainability and efficacy
Don’t reinvent the wheel to address non-clinical needs
Source: Population Health Advisor interviews and analysis.
1 2 3
• Play minimal role in
operations, service
offerings
• Unsustainable funding
model if addressing all
social determinants
of health
• Demands large scale
time and resources
• Outside scope of staff
skills, experience
• Delayed ROI
• Deepens community
connections, network
• Low-cost investment into
existing successful
services
Build
• Dedicate hospital
resources and staff
• Construct programs
from ground-up
Buy
• Contract out to social
services organizations
• Devote hospital funding
to addressing nonclinical
risk factors
Partner
• Distribute resource
investment across
multiple partners
• Tap into existing
services and
relationships
Imp
lica
tio
ns
De
scrip
tion

© 2019 Advisory Board • All rights reserved • advisory.com
13
Tremendous innovation driven by partnerships
Focus on determinants of health driving short- and long-term impact
Source: Population Health Advisor interviews and analysis.
1) The BUILD Health Challenge is an
initiative designed to foster and
expand meaningful partnerships
among health systems, community-
based organizations, local health
departments, and other organizations
that impact health in the community.
Overview of the BUILD Health Challenge1 communities
Healthy Hill Initiative
Spurring economic
development and
improving public safety
Healing Together
Empowering youth
leaders to stand
against violenceThe Healthy
Ontario Initiative
Developing “health
hubs” to foster
strong bodies and
communities
The Harris County BUILD
Health Partnerships
Mitigating food insecurity
by redesigning the local
food system
Increasing Access to
Behavioral Health
Screening and Support
Eliminating health
disparities by age five
BUILDing Health
and Equity in East
Portland
Expanding access to
affordable housing,
green space, and
health food
Building a Healthy
and Resilient Liberty
City
Breaking the cycle of
violence at all ages
© 2019 Advisory Board • All rights reserved • advisory.com
14
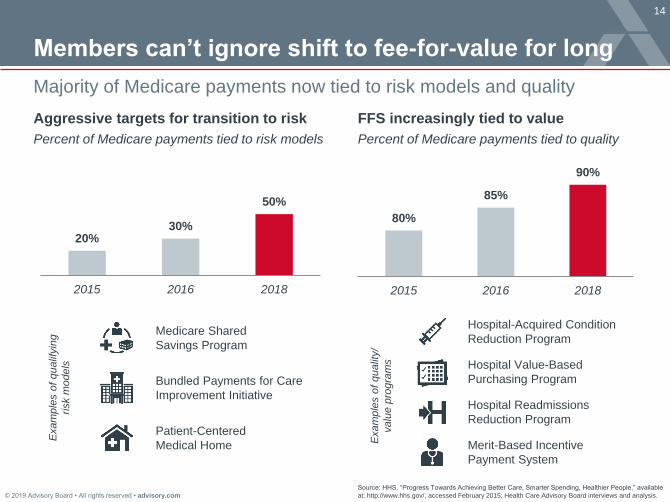
Members can’t ignore shift to fee-for-value for long
Source: HHS, “Progress Towards Achieving Better Care, Smarter Spending, Healthier People,” available
at: http://www.hhs.gov/, accessed February 2015; Health Care Advisory Board interviews and analysis.
20%30%
50%
2015 2016 2018
Aggressive targets for transition to risk
Percent of Medicare payments tied to risk models
80%
85%
90%
2015 2016 2018
FFS increasingly tied to value
Percent of Medicare payments tied to quality
Medicare Shared
Savings Program
Patient-Centered
Medical Home
Bundled Payments for Care
Improvement Initiative
Exam
ple
s o
f qualif
yin
g
risk m
odels
Hospital-Acquired Condition
Reduction Program
Hospital Readmissions
Reduction Program
Hospital Value-Based
Purchasing Program
Merit-Based Incentive
Payment System
Exam
ple
s o
f qualit
y/
valu
e p
rogra
ms
Majority of Medicare payments now tied to risk models and quality
© 2019 Advisory Board • All rights reserved • advisory.com
ROAD MAP15
The impact of the social determinants of health1
2The role of community partnerships in
addressing patients’ non-clinical risk factors
3 Key considerations for promoting long-term sustainability

© 2019 Advisory Board • All rights reserved • advisory.com
16
Addressing non-clinical needs to improve outcomes
Identify structural barriers that contribute to health disparities
Source: Population Health Advisor interviews and analysis.
Map major community health needs to partner organizations with tools for success
Decreasing resource requirements and severity of need
Engage disconnected
patients at-risk of
clinical escalation
Meet fundamental
needs critical to clinical
success
Remove barriers to
access based on
severity of need
• Community health workers
• Health literacy support
• Congregational liaisons
Resources
to achieve
health equity
aims
• Safe, stable housing
• Healthy foods
• Economic support
• Language services
• Transportation services
• Mobile health clinics
Address baseline needs
(e.g., hunger, housing)
that must be met before
patients can begin to
prioritize health care
Enhance engagement and
reduce the trust gap by
aligning with community-
based organizations
serving at-risk, disengaged
patient populations
Increase access to health
services, from preventive
to specialist care, for
patients facing logistical
barriers (e.g., work hours,
lack of transportation)
Opportunities
to partner

© 2019 Advisory Board • All rights reserved • advisory.com
17
Prioritize needs that preclude health improvement
Review evidence to surface community’s most pressing barriers
Opportunity #1: Meet fundamental needs critical to clinical success
Source: See appendix for complete sources; Population Health Advisor interviews and analysis.
LowAcuity:
26% increased risk of
mortality resulting from
loneliness
• Leads to increased
rates of behavioral
health problems,
dementia, hospital
readmissions, and
mortality
• Reduces ability for the
elderly to live
independently
Social isolation
10% increased
annual visits to the
doctor
26-36 years reduced
life expectancy
• Leads to increased
rates of physical
trauma, chronic
diseases, dental
issues, behavioral
health problems, and
exposure
• Reduces access to
primary care and
ability to self-manage
$44K average annual
cost per highest-
volume ED patient
experiencing
homelessness
Housing instability
HighAcuity:
Food insecurity• Leads to increased
rates of chronic
diseases, dental
issues, behavioral
health problems,
stress, and
hospitalizations
• Influences purchasing
decisions between
food and: medicine
(74%), transportation
(67%), utilities (59%),
and housing (57%)
$179B annual direct
and indirect health-
related costs attributed
to food insecurity
HighAcuity:
HighAcuity:
2.13x increased risk
of mortality for
Medicaid vs. private
beneficiaries
• Leads to increased
rates of distress and
behavioral health
problems
• Reduces access to
clinical care and
increases likelihood of
living in a resource-
poor area
Economic insecurity
24-67% increased
risk of readmission for
dual-eligible patients

© 2019 Advisory Board • All rights reserved • advisory.com
18
Collaborate to make big community investments
Vermont’s housing offerings meets range of needs with tangible ROI
Source: Population Health Advisor interviews and analysis.
1) University of Vermont Medical Center.
UVMMC¹ develops housing portfolio through partnership
Services
Case management: UVMMC funds 1 onsite FTE Case Manager from CHC¹ who
connects patients to CHC provider and fulfills additional needs (e.g., insurance)
Mental health services: Howard Mental Services dedicates one case manager to each
site (1 FTE), who is reimbursed separately
Additional clinical services : Various providers (e.g., Visiting Nurse Association,
physician house call) visit each site as needed
Short-term Permanent
Results
Decreased inpatient admissions:
Reduced from 95 to 30 stays
Decreased ED utilization:
Reduced from 161 to 94 visits
Decreased annual cost of care:
Dropped health care from $750K to
$250K for permanently housed patients
Infrastructure
Harbor Place Rooms: 22 family units, 34
single units with an average stay of 8 days
Beacon Apartments: 18 single units
across an indefinite stay
Funding
Pay per diem rate for patients
Guarantees minimum number of nights
Helped fund purchase and
renovation of motel and pays
operations amount per patient

© 2019 Advisory Board • All rights reserved • advisory.com
CASEEXAMPLE
University of Vermont
Medical Center
562-bed medical center located in Burlington, Vermont
and sole tertiary hospital in the state
• Developed a partnership with Champlain Housing Trust, a
non-profit that creates and preserves affordable housing in
Vermont; UVMMC pays to house their patients in
Champlain Housing Trust’s buildings and funds additional
case management services by the Community Health
Centers of Burlington
• Additional services are provided onsite (e.g., Howard
Mental Services, Visiting Nurse Association) and
reimbursed independently
• Started with short-term housing, expanded to include
permanent, and developing intermediate housing that will
include additional onsite services in mid-2017
Source: Population Health Advisor interviews and analysis.

© 2019 Advisory Board • All rights reserved • advisory.com
20
Universalize screening to unearth food insecurity
Source: Population Health Advisor research and analysis.
ProMedica’s cross-setting screening process
Households
served in 2017
3.3KReduced
readmission rates
53%Reduced health
care costs
15%Patients
screened in 2017
781K
Short-term response
to inpatient admission
Patient discharged from hospital with
one day’s worth of calories,
information on follow-up support (e.g.,
federal programs, food banks), and
PCP appointment
RN performs initial food insecurity
screen using two-question Hunger
Vital Sign™
LCSW or discharge planner follows
up with identified patients to validate
need and connect to any additional
psychosocial services
Primary care staff across all
practices screen for food insecurity
and PCPs refer appropriate
patients to the system’s food clinic
Patients visit food clinic for healthy,
condition-specific food once a
month for six months before
needing new referral, encouraging
regular preventive care
Long-term support
embedded in primary care
ProMedica offers emergency support and longer term food prescriptions

© 2019 Advisory Board • All rights reserved • advisory.com
CASEEXAMPLE
ProMedica
Not-for-profit, 13-hospital healthcare organization based in
Toledo, Ohio serving communities in 30 states
► System-wide food insecurity screenings prompted by food
insecurity prevalence and link to obesity; patients are screened
for food insecurity in both the inpatient and outpatient setting,
with differing interventions
► In 2017, ProMedica conducted more than 781,000 food security
screenings and the food clinic served 3,260 unique households
► Preliminary data from a small group of Medicaid patients
showed those who screened positive and visited the food clinic
had 3% reduction in ED usage, 53% reduction in readmission
rates, 4% increase in primary care usage, and 15% reduction in
healthcare costs compared to those not using the program
Source: Population Health Advisor research and analysis.

© 2019 Advisory Board • All rights reserved • advisory.com
22
Form coalitions to elevate economic opportunity
Phipps neighborhoods’ workforce development tackles economic barriers
Source: Population Health Advisor interviews and analysis.
Career Network: Healthcare program relies on expertise of three major players
Phipps Neighborhoods
• Career development
community-based
organization that connects
participants to education
and training for health care-
related jobs
• Community members
eligible to apply are 18-26
years old with a GED or
high school diploma
• Phipps hosts intensive
induction boot camp week
to identify final roster based
on professional qualities
(e.g., punctuality, attire)Hostos Community College
Local community college hosts
the nine week educational
component, including:
• Health care labor market
• How to navigate a higher
education environment
Montefiore Health
• Local health system hosts the
four week externship component,
preparing students for roles like:
– Patient care technician
– Dietary worker
– Community health worker
– Medical assistant
– Research coordinator
• Montefiore guarantees
participants an interview at the
end of the program
Participants secure
employment
80%

© 2019 Advisory Board • All rights reserved • advisory.com
CASEEXAMPLE
Phipps Neighborhoods
Workforce development nonprofit in the Bronx, NY
► Partnered with Montefiore Health System and a local
community college (Hostos Community College) to create a
workforce development program called Career Network:
Healthcare
► Program offers a pathway to health care jobs by providing
participants with a 13-week training program. Upon
completion, Montefiore guarantees candidate interviews for
all participants across one or more of the health system’s
1,500 existing vacancies
► To ensure stability in employment, Career Network also
helps to solve participants’ pressing employment barriers
(e.g., housing insecurity, childcare needs)
Source: Population Health Advisory and Health Disparities Initiative interviews and analysis.

© 2019 Advisory Board • All rights reserved • advisory.com
24
Design program to address root cause of care gap
Stabilize at-risk with consistent touchpoints to health system
Opportunity #2: Remove barriers to access based on severity of need
Source: Population Health Advisor interviews and analysis.
Lack understanding of
health status and care
plan next steps due to
limited English
proficiency
Disconnected patients face three common access barriers that threaten outcomes
1 2 3
Map program to community’s most pressing access barriers and level of care required
Miss appointments
due to a lack of
adequate transport or
logistical barriers (e.g.,
clinic location)
Lack key resources to
manage health and
access care (e.g.,
housing, economic
stability, insurance)
Offer language-
concordant care
• Hire providers who
speak common
community languages
• Contract for telephonic
or virtual interpretation
Arrange transit and
convenient care
hotspots
• Coordinate with
rideshares, taxis
• Launch targeted
health fairs
Bring full scale
services to targeted
locations
• Invest in mobile
health clinic for
community hotspots
• Set up worksite clinics
Low HighProvider integration into the community

© 2019 Advisory Board • All rights reserved • advisory.com
25
Connect patients with care they can understand
Cambridge Health Alliance offers multiple language support options
Source: Hacker, K, et al., “Exploring the Impact of Language Services on Utilization and Clinical
Outcomes for Diabetics,” PLoS ONE 7(6); Population Health Advisor interviews and analysis.
39%
Lower likelihood of
hospitalization or ED
utilization related to diabetes
compared to those receiving
no language services
• What is your primary language?
• In what language do you prefer to communicate
with your provider?
• Would you like to use interpreter services for
your visit?
Importance of understanding language
preferences
How to connect patients to interpretation services
Annual testing on CHA language policies and how
to implement them
Language-concordant providers
for diabetes management led to:In-person
interpretation
Language-
concordant
provider
Telephonic
interpretation
Language line
interpretation
service
In-visit interpretation offerings
Training and standardized screening critical to program success
Staff training components Standardized questions assessed at check in

© 2019 Advisory Board • All rights reserved • advisory.com
CASEEXAMPLE
Cambridge Health Alliance
Massachusetts-based community health system serving a
diverse patient population
► To meet the needs of patients with limited English
proficiency (LEP), CHA developed robust language
services across health care settings. Over half of CHA
patients report speaking a language other than English at
home and 42% of CHA’s primary care patients have limited
English proficiency
► On the system’s website, patients can search for a doctor
that speaks their preferred language. When patients check
in for an office visit, CHA registration staff screen patients
for language preferences. Patients identified as having LEP
are supported by language-concordant providers, in-person
or telephonic interpretation, or language line interpretation
services, based on availability
Source: Hacker, K, et al., “Exploring the Impact of Language Services on Utilization and Clinical
Outcomes for Diabetics,” PLoS ONE 7(6); Population Health Advisor interviews and analysis.

© 2019 Advisory Board • All rights reserved • advisory.com
27
Getting patients to, rather than through, the door
MedStar teams up with Uber to bring qualifying patients to appointments
Source: Syed, Samina T., Ben S. Gerber, and Lisa K. Sharp.
“Traveling Towards Disease: Transportation Barriers to Health
Care Access.” Journal of community health 38.5 (2013): 976–
993. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC4265215/.
Population Health Advisor interviews and analysis.
Case manager
calls patient up
to 90 minutes
before
appointment
Patient makes
appointment
Case manager
schedules ride
through
UberCENTRAL
U
Patient
indicates no-
show due to
lack of
transportation
Case manager
identifies
qualifying
patient at-risk
for no-show
3.6M
People miss
medical
appointments
due to lack of
transportation,
annually
25%
Of low-income
patients report
missing
appointments
due to lack of
transportation
11-30%Average clinic
no-show rate
Average daily revenue capture <100%
Case managers use Uber to help patients overcome transportation barrier

© 2019 Advisory Board • All rights reserved • advisory.com
CASEEXAMPLE
MedStar Health and Uber
Health system based in Columbia, MD and serving
Maryland, Washington, DC, and Northern Virginia
► Uber is a national ride-hailing company based in San
Francisco, California
► In January 2016, MedStar and Uber formed a partnership to
improve access to transportation for MedStar patients
Source: Population Health Advisor interviews and analysis.

© 2019 Advisory Board • All rights reserved • advisory.com
29
Clinic brings care to CBOs¹ serving the homeless
Parkland’s mobile clinics eliminate barriers to care and medications
Source: Population Health Advisor interviews and analysis.
1) Community Based Organizations.
2) Homeless Outreach Medical Services.
Patients served in 2015
9,377Patients uninsured
78%Annual program budget
$5M
HOMES² program addresses needs of patients experiencing homelessness during and
after visit
Specialty, emergent care
22-person shuttle loops around
central business district to Parkland
main campus for additional care (e.g.,
x-rays, ED care, Class A pharmacy)
Needs addressed
after clinic visit
Needs
addressed on
the clinicPsychosocial services
Supplemental services vary by
site and population need
(e.g., staff health educator,
interpreter, psychologist when
visit domestic violence shelter)
Clinical care
Mobile clinic staff provide
acute and chronic disease
care, education, check-ups,
immunizations, mental health
counseling, and dental care
for children and adults
Medication access
Pharmacy supplies 35
medications for patients free
of charge to enable patients to
start regimen immediately
Referrals to other programs
Staff connect patients to other
programs (e.g., specialty
clinics, housing support)

© 2019 Advisory Board • All rights reserved • advisory.com
CASEEXAMPLE
Parkland Health & Hospital
System’s HOMES Program
862-bed safety-net and teaching hospital system,
including 20 community-based clinics and 12 school-
based clinics in Dallas County, Texas
• Established mobile HOMES program to increase access to
medical, dental, and behavioral health care for homeless
children and adults
• Five medical and one dental mobile clinic visit 31 different
community partners to serve existing concentrations of
individuals with unstable housing; partners are chosen
based on logistical factors
• Nurse, physician or advanced practice provider, and driver
deliver immediate care supplemented by an on-site Class D
pharmacy; additionally, a 22-person shuttle transports
homeless patients to Parkland’s main campus for specialty,
emergent care, and prescriptions
• In 2015, the HOMES program served 9,377 patients, 78% of
whom were uninsured, with an annual budget of $5 million
Source: Population Health Advisor interviews and analysis.

© 2019 Advisory Board • All rights reserved • advisory.com
31
Select trusted partners with deep community ties
Supplement programs with partner expertise to jump start engagement
Opportunity #3: Engage disconnected patients at-risk of clinical escalation
Source: Population Health Advisor interviews and analysis.
• Build a longstanding
relationship by catering
to the specific needs of a
particular population
• Promote top-of-site
utilization by connecting
patients with appropriate
services
• Embed a health system
staff member in the
community to build
patient loyalty
• Choose partners based
on existing positive
relationships with target
population
• Augment partner
expertise with health
system resources
• Build rigorous
partnership agreements
based on joint principles
of collaboration
Time, resource commitment
High LowHealth system control
Collaborate with trusted
community partners
Devote staff to strengthening
community relationships

© 2019 Advisory Board • All rights reserved • advisory.com
32
Use CHWs to capture disconnected patients
UNM Health System achieved long term funding with targeted pilot
Source: Source: Johnson, D. et al, “Community Health Workers and Medicaid Managed Care in New Mexico,” Journal of
Community Health, June 2012; UNM Health System, Albuquerque, NM; Population Health Advisor interviews and analysis.
1) Managed Care Organization.
2) Control group not managed by CHWs had 53% fewer inpatient admissions.
3) Data measured 12 months after the start of the six month intervention.
CHWs show promising ROI with highest-risk Medicaid patients
Results
• High-risk MCO members
• People returning from the
criminal justice system
• Undocumented immigrants
• Children at-risk for abuse
Target
patients
6 months of didactic training (e.g.,
health coaching, service
coordination) paired with 6 months
of field workTraining
Local MCOs¹ needed help
identifying their high-risk members,
provided funding to UNM to hire,
train, and deploy CHWsImpetus
Address social needs: offer
interpretation services, connect with
social services, communicate with
cultural humility
Support disease self-
management: reinforce basic
disease education, address health
literacy, navigate to clinical care
Services
Program costs vs. savings
Costs Savings
$521K
$2M
83%Fewer inpatient
admissions²³
4:1ROI

© 2019 Advisory Board • All rights reserved • advisory.com
CASEEXAMPLE
University of New Mexico Health System
Three-hospital academic health center in
Albuquerque, NM
► University of New Mexico Health System (UNM) deploys
CHWs to establish trusting relationships with disengaged,
high-risk patients attributed to a local managed care
organization (MCO)
► After a successful pilot, UNM obtained stable, long term
funding from internal stakeholders and from additional
MCOs to expand programming. While UNM continues to
serve the highest-risk, they’ve expanded support to
vulnerable subpopulations (e.g., undocumented immigrants,
children)
► UNM Health’s efforts resulted in a 4:1 ROI with 83% fewer
inpatient admissions¹²
Source: Source: Johnson, D. et al, “Community Health Workers and Medicaid Managed Care in New Mexico,” Journal of
Community Health, June 2012; UNM Health System, Albuquerque, NM; Population Health Advisor interviews and analysis.
1) Control group not managed by CHWs had 53% fewer
inpatient admissions.
2) Data measured 12 months after the start of the six month
intervention.

© 2019 Advisory Board • All rights reserved • advisory.com
34
Embed targeted health literacy approach with rigor
Initiating effort with Rx adherence goals to achieve trackable success
Source: Meyer D, “The Health Education and Adult Literacy (HEAL) Program,” Healthy Tomorrows Partnership for
Children Program, http://mchlibrary.jhmi.edu/downloads/file-7146-1; “Heal - Health Education and Adult Literacy
Program,” NewYork-Presbyterian, http://www.nyp.org/clinical-services/ambulatory-care-network-programs/heal---
health-education-and-adult-literacy-program; Population Health Advisor interviews and analysis.
1) Community Based Organizations.
Improving health literacy necessitates standardized, community-inclusive process
Repeat research process as
necessary to adapt curriculum
with changing community needs
Train health and community
leaders to use effective health
literacy techniques
• Medical center staff (e.g.,
pediatricians, residents, and
family support/ community
health workers)
• Staff from seven participating
CBOs¹ (medical students,
volunteers)
Perform individual patient
interventions across all partner
organizations
• Perform teach-back
• Provide visual and written
educational materials
Develop culturally-relevant and
evidence-based health literacy
curriculum
• Incorporate community input
on unit topics
• Use data from needs
assessments or studies

© 2019 Advisory Board • All rights reserved • advisory.com
35
Leverage community as program design lab
Columbia university’s three step HEAL¹ curriculum based on research
Source: Meyer D, “The Health Education and Adult Literacy (HEAL) Program,” Healthy Tomorrows Partnership
for Children Program, http://mchlibrary.jhmi.edu/downloads/file-7146-1; “Heal - Health Education and Adult
Literacy Program,” NewYork-Presbyterian, http://www.nyp.org/clinical-services/ambulatory-care-network-
programs/heal---health-education-and-adult-literacy-program; Population Health Advisor interviews and analysis.
1) Health Education and Adult Literacy.
• Community pediatrics unit initiated health
literacy program targeted towards parents
• Staff researcher performed an
observational study on communication
quality between patients and providers
• Included patient exit interviews
Provider role
• Key nonprofit partner gathered 22
community members to form three focus
groups in Spanish and English
• Groups offered input on patient
communication with providers, medication
use, and home remedies
Community role
• Seven-unit course developed on a 5th grade
reading level and a train-the-trainer manual
• Spanish versions created by speakers
native to countries represented by patients
• Unit topics include:
• Doctor’s appointment preparation
• Over-the-counter medications
• Prescription medications
• Home remedies
• Medication management
• Upper respiratory infections
• Antibiotic use
Health literacy curriculum
Shape curriculum according to community-sourced needs and provider-led analysis

© 2019 Advisory Board • All rights reserved • advisory.com
36
Results indicate improved health literacy is viable
Incorporate applicable lessons into nascent efforts
Source: Meyer D, “The Health Education and Adult Literacy (HEAL) Program,” Healthy Tomorrows Partnership for
Children Program, http://mchlibrary.jhmi.edu/downloads/file-7146-1; “Heal - Health Education and Adult Literacy
Program,” NewYork-Presbyterian, http://www.nyp.org/clinical-services/ambulatory-care-network-programs/heal---
health-education-and-adult-literacy-program; Population Health Advisor interviews and analysis.
1) Columbia University Medical Center.
2) Community Based Organizations.
Patients approached in
waiting rooms indicating
interest in program
83%
Increased knowledge/attitude
score for parents receiving
upper respiratory infection
education
61%
Pediatric faculty, residents,
and family support workers
trained at CUMC¹ clinics
145
Key lessons to guide health literacy programs
Use partners to expand program reach
Extend health literacy programming outside the
health system into community health clinics and
social service organizations
Leverage networks of CBOs² to build course
Local social services and nonprofits can connect
providers with community representatives who help
guide topic development
Base program on explicit, quantifiable goals
Strong vision for health literacy intervention (e.g.,
improved medication adherence) spurs metric
tracking to prove efficacy and sustain funding
Inform clinical staff of proven best practices
All patient-facing staff should be aware of and
trained on health literacy best practices to improve
communication protocols

© 2019 Advisory Board • All rights reserved • advisory.com
CASEEXAMPLE
Columbia University Medical Center
738-bed academic medical center in New York, New York,
part of NewYork-Presbyterian
►In 2007, Columbia University Medical Center’s Community
Pediatrics department and NewYork-Presbyterian Hospital
launched the Health Education and Adult Literacy (HEAL)
program in collaboration with seven local community
partners
►The program’s goal is to reduce medication errors and
increase compliance by improving the health literacy of
children and parents in the Washington Heights and Inwood
communities
►The program to date has trained 184 providers, residents,
medical students, family support workers, and volunteers
with their health literacy curriculum, serving 180 patients’
caregivers at Columbia University Medical Center
ambulatory care clinics
Source: Population Health Advisor interviews and analysis.

© 2019 Advisory Board • All rights reserved • advisory.com
38
Pillars of community can help breach the trust gap
MedStar brings care to barbershops to reach the disconnected
Source: Population Health Advisor interviews and analysis.
Surfacing undiagnosed issues
54%
9%Previously undiagnosed participants
with elevated blood sugar
19%Participants with uncontrolled BP
referred to and tracked for follow-
up care
Previously undiagnosed participants
with hypertensive
or pre-hypertensive BP readings
Barbers trained to promote diabetes and
hypertension screening, provide health
education
• Receive 8-hour training on informed
consent, measuring height and weight,
and collecting data
RN, Dietician, Diabetes Educator perform
follow up appointments on-site
• Do not travel for regular screenings
Health navigators conduct blood pressure
and blood glucose screenings on-site
• Present in rotating, high-traffic
barbershops from 2-7pm five days/week
Staff perform screenings through the “Hair, Heart and Health” program to identify
Black men at-risk for hypertension and diabetes

© 2019 Advisory Board • All rights reserved • advisory.com
CASEEXAMPLE
MedStar Health
10-hospital health system based in Columbia, Maryland
• In 2008, MedStar established “Hair, Heart and Health”
program to screen for diabetes and hypertension in local
barbershops
• The program was designed to reach African American men
who previously had infrequent contact with the system to
screen them for cardiovascular disease and diabetes
Source: Population Health Advisor interviews and analysis.

© 2019 Advisory Board • All rights reserved • advisory.com
ROAD MAP40
The impact of the social determinants of health1
2The role of community partnerships in addressing patients’ non-
clinical risk factors
3Key considerations for promoting long-term
sustainability

© 2019 Advisory Board • All rights reserved • advisory.com
41
Select potential partners based on internal gaps
Avoid duplicating services for program sustainability
Source: Population Health Advisor interviews and analysis.
Common resource gaps mapped to potential partners
Po
tential P
art
ners • Local government
• Social services (e.g., food
banks, schools)
• Behavioral health facilities
• IT vendors
• Medical schools
• Local pharmacy
• Mental health or substance
abuse providers
• Academic institution
• Community organizations
• Social service providers
• Housing, transit services
• Social service providers
• Local clergy/chaplains
• Legal services
• Local businesses (e.g.,
supermarkets, barbershops)
Infrastructure Staffing Reach
Ga
ps
• Funding
• Facility space and utilities
• Data sharing and analytics
• Clinical and non-clinical
expertise (e.g., social
workers)
• Grant-writing assistance
• Volunteers (e.g., peer
coaches, medical students)
• Expanded clinical services
(e.g., expanded hours)
• Expanded social services
(e.g., housing, food)
• Connection with at-risk
populations

© 2019 Advisory Board • All rights reserved • advisory.com
42
Value to patients, system must be critically assessed
Partner relationships a two-way street, success not guaranteed
Source: Health Care Advisory Board interviews and analysis.
Conveniently located near crowded,
high-Medicaid system EDs
Articulates clear value to system,
with demonstrable ROI
Provides high quality services
valuable to Medicaid population
Maintains open, transparent
communication channels
Willing to meet clinical
standardization expectations
Willing to progress toward
risk-based arrangements
Hallmarks of effective relationships
Sustainable infrastructure for
stakeholder engagement, feedback
Enthusiastic buy-in from leadership
and frontline staff
Clear metrics for measuring ROI,
transparency, accountability
Shared mission and culture
Aligned back office capabilities for
data transparency, continuity
Community partner checklist:

© 2019 Advisory Board • All rights reserved • advisory.com
43
Set expectations with detailed goals, responsibilities
Non-binding contract outlines responsibilities of providers, clinic staff
Source: Population Health Advisor interviews and analysis.
Hospital-employed navigator and community liaison collaboration starts at admission
Memorandum of understanding designates party responsibilities for care support
Navigator visits
patient once
identified upon
admission,
obtains
permission to
contact liaison
Navigator
answers liaison’s
ongoing
questions related
to patient’s health
or care plan
Liaison continues
care support as
needed, informs
navigator if there
are health-related
concerns
Liaison recruits
volunteers to
provide inpatient
and post-
discharge support
Liaison visits
patient to assess
need for
volunteer
services and
social support
• Relationship between MCHI, the health system, and each
congregation is grounded in a signed MOU
• All parties required to sign document before official
admittance into network

© 2019 Advisory Board • All rights reserved • advisory.com
CASEEXAMPLE
Maryland Faith Health Network at LifeBridge Health
Three hospitals in Maryland’s LifeBridge Health system (Sinai
Hospital of Baltimore, Northwest Hospital and Carroll Hospital) that
operate in urban, suburban and rural settings joined 68 faith-based
congregations under the leadership of Maryland Citizens’ Health
Initiative Fund to form the Maryland Faith Health Network
► Hospital navigators initiate community post-discharge
support upon patient admission and offer health education
to faith-based liaisons; liaisons identify potential program
participants and provide them with spiritual and social
support post-discharge
► Network requires formal entry into the network by signing a
memorandum of understanding among MCHI, the
hospitals, and each congregation, outlining specific
responsibilities
► To date, 121 liaisons serve more than 1,600 community
members
Source: Population Health Advisor interviews
and analysis.
© 2019 Advisory Board • All rights reserved • advisory.com
45
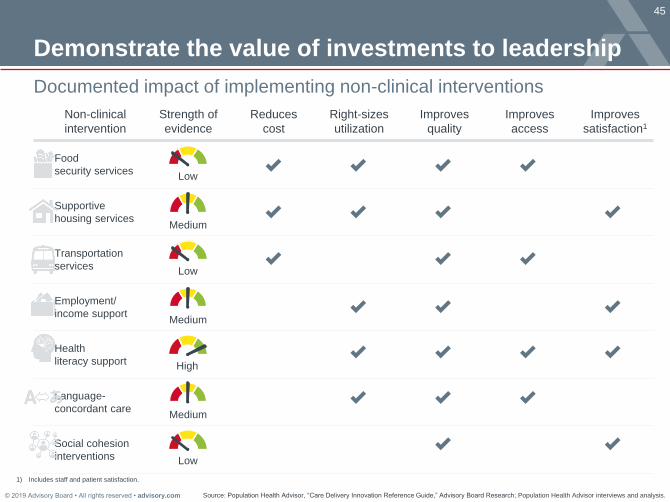
Non-clinical
intervention
Strength of
evidence
Reduces
cost
Right-sizes
utilization
Improves
quality
Improves
access
Improves
satisfaction1
Food
security services
Supportive
housing services
Transportation
services
Employment/
income support
Health
literacy support
Language-
concordant care
Social cohesion
interventions
Demonstrate the value of investments to leadership
Source: Population Health Advisor, “Care Delivery Innovation Reference Guide,” Advisory Board Research; Population Health Advisor interviews and analysis.
Documented impact of implementing non-clinical interventions
1) Includes staff and patient satisfaction.
Low
High
Medium
Low
Medium
Medium
Low

© 2019 Advisory Board • All rights reserved • advisory.com
46
A few lessons from experienced peers
Source: Health Care Advisory Board interviews and analysis.
Three key principles to maximize impact and avoid missteps
Drive
community
development
through your
business
Commit to
long-term
involvement in
the community
Sporadic and short-
term efforts are
unlikely to produce
meaningful results
and could do more
harm than good
Maximize your
impact by hiring and
sourcing within the
local community
when possible
Work with members of the
community to ensure that efforts
address issues most important to
them and are embraced rather
than viewed as patronizing
Use a grassroots to
grass tips approach
Not all investments in social determinants are created equal

© 2019 Advisory Board • All rights reserved • advisory.com
47
Missed our last webconference?
Surface disparities in outcomes and care delivery
Source: Population Health Advisor interviews and analysis.
Review
Health Equity 101
Review the webconference recording here.
Learn best practices to design a data-driven
framework to identify and prioritize equity
efforts across the system and incorporate them
into patient care.

© 2019 Advisory Board • All rights reserved • advisory.com
50
Sources cited, page 10
Source: Population Health Advisor interviews and analysis.
Housing
“Health Care and Homelessness,” National Coalition for the Homeless, http://www.nationalhomeless.org/factsheets/health.html;
Feigal L, et al., “Homelessness and Discharge Delays from an Urban Safety Net Hospital,” Public Health, 128, no. 11 (2014):
1033-1035, https://www.sciencedirect.com/science/article/pii/S0033350614001292.
Food
“What are the Connections Between Food Insecurity and Health?,” Hunger + Health,
https://hungerandhealth.feedingamerica.org/understand-food-insecurity/hunger-health-101/; Estimating the Health-Related
Costs of Food Insecurity and Hunger,” Bread for the World,
https://www.bread.org/sites/default/files/downloads/cost_of_hunger_study.pdf.
Economics
Robert Wood Johnson Foundation, “How Does Employment—or Unemployment— Affect Health?” Health Policy Snapshot
Issue Brief, 2013, http://www.rwjf.org/content/dam/farm/reports/issue_briefs/2013/rwjf403360; “Social Risk Factors and
Performance Under Medicare’s Value-Based Purchasing Programs,” United States Department of Health and Human Services,
2016, https://aspe.hhs.gov/system/files/pdf/253971/ASPESESRTCfull.pdf.
Interpersonal
“Threat to Health,” Campaign to End Loneliness, https://www.campaigntoendloneliness.org/threat-to-health/; Njeru J, et al.,
“Inpatient Health Care Utilization Among Patients Who Require Interpreter Services,” BioMed Central, 15, no. 214 (2015),
https://www.ncbi.nlm.nih.gov/pmc/articles/PMC4448538/.
Education
“Population Health: Behavioral and Social Science Insights,” Agency for Healthcare Research and Quality,
https://www.ahrq.gov/professionals/education/curriculum-tools/population-health/zimmerman.html; Haun J, “Association
Between Health Literacy and Medical Care Costs in an Integrated Healthcare System: A Regional Population Based Study,”
BMC Health Services Research, 15, no. 249 (2015), https://www.ncbi.nlm.nih.gov/pmc/articles/PMC4482196/.

© 2019 Advisory Board • All rights reserved • advisory.com
51
Sources cited, page 18
Source: Population Health Advisor interviews and analysis.
Lack of housing
“Health Problems of Homeless People,” NCBI, (1988), https://www.ncbi.nlm.nih.gov/books/NBK218236/; “Health Care and
Homelessness,” National Coalition for the Homeless, http://www.nationalhomeless.org/factsheets/health.html; “The Cost of
Homelessness Facts,” Green Doors, http://www.greendoors.org/facts/cost.php.
Food insecurity
Aungst, “Food Insecurity and Health Impacts,” Michigan State University Extension,
http://msue.anr.msu.edu/news/food_insecurity_and_health_impacts; “What are the Connections Between Food Insecurity and
Health?,” Hunger + Health, https://hungerandhealth.feedingamerica.org/understand-food-insecurity/hunger-health-101/; Cook,
J et al., “Estimating the Health-Related Costs of Food Insecurity and Hunger,” Bread for the World Institute,
http://www.childrenshealthwatch.org/wp-content/uploads/JohnCook_cost_of_hunger_study.pdf.
Economic insecurity
Robert Wood Johnson Foundation, “How Does Employment—or Unemployment— Affect Health?” Health Policy Snapshot
Issue Brief, 2013, http://www.rwjf.org/content/dam/farm/reports/issue_briefs/2013/rwjf403360; “Social Risk Factors and
Performance Under Medicare’s Value-Based Purchasing Programs,” United States Department of Health and Human Services,
2016, https://aspe.hhs.gov/system/files/pdf/253971/ASPESESRTCfull.pdf.
Social isolation
Seegert, “Social Isolation, Loneliness Negatively Affect Health for Seniors,” Association of Health Care Journalists,
https://healthjournalism.org/blog/2017/03/social-isolation-loneliness-negatively-affect-health-for-seniors/; “Threat to Health,”
Campaign to End Loneliness, https://www.campaigntoendloneliness.org/threat-to-health/; Gerst-Emerson, “Loneliness as a
Public Health Issue: The Impact of Loneliness on Health Care Utilization Among Older Adults,” American Journal of Public
Health, 105, no. 5 (2015): 1012-1019, https://www.ncbi.nlm.nih.gov/pmc/articles/PMC4386514/.


















