So PAP Doesn’t Work
31
Rochelle Goldberg, MD, FAASM, FCCP Diplomat, American Board of Sleep Medicine Director Sleep Medicine Services Main Line Health Systems Lankenau Medical Center and Paoli Hospital So PAP Doesn’t Work
Transcript of So PAP Doesn’t Work
Rochelle Goldberg, MD, FAASM, FCCP
Diplomat, American Board of Sleep Medicine
Director Sleep Medicine Services
Main Line Health Systems
Lankenau Medical Center and Paoli Hospital
So PAP Doesn’t Work

Disclosures
• Speaker: Teva, UCB, Purdue
• Advisory Board: Welltrinsic Sleep Network
• Consultant: Vapotherm, Inc.
• National Interpretor: Novasom

The Translation
• What they say... “It doesn’t work!”
• What they may mean… – I hate it and don’t want to use it.
– I have problems with it (mask, air, etc)
– I’m still snoring, choking, etc.
– I still can’t fall asleep.
– I still don’t sleep well.
– I am still sleepy.

Translation 101a
“I hate it and don’t want to use it!”
• Is it an education issue?
– Do they understand sleep apnea?
• Relate their specific symptoms to the diagnosis.
• Are they aware of the risks of untreated apnea?
– Are test results clear?
• Severity, oxygen and sleep effects; PAP findings
– Are they aware of other treatment options?
Translation 101b
“I have problems using it.”
• Is it a technical or compliance issue?
– Do they understand PAP treatment?
– Are they using equipment properly?
– Are side effects of PAP interfering with sleep?
– Are there environmental or family issues?

Translation 101c
“I’m still snoring, choking, sleepy, not
sleeping well.”
• What were the original symptoms?
– Is there any symptom resolution?
– Are these consistent with treatment problems
or limited compliance?
– Are symptoms unrelated to sleep apnea and
PAP?
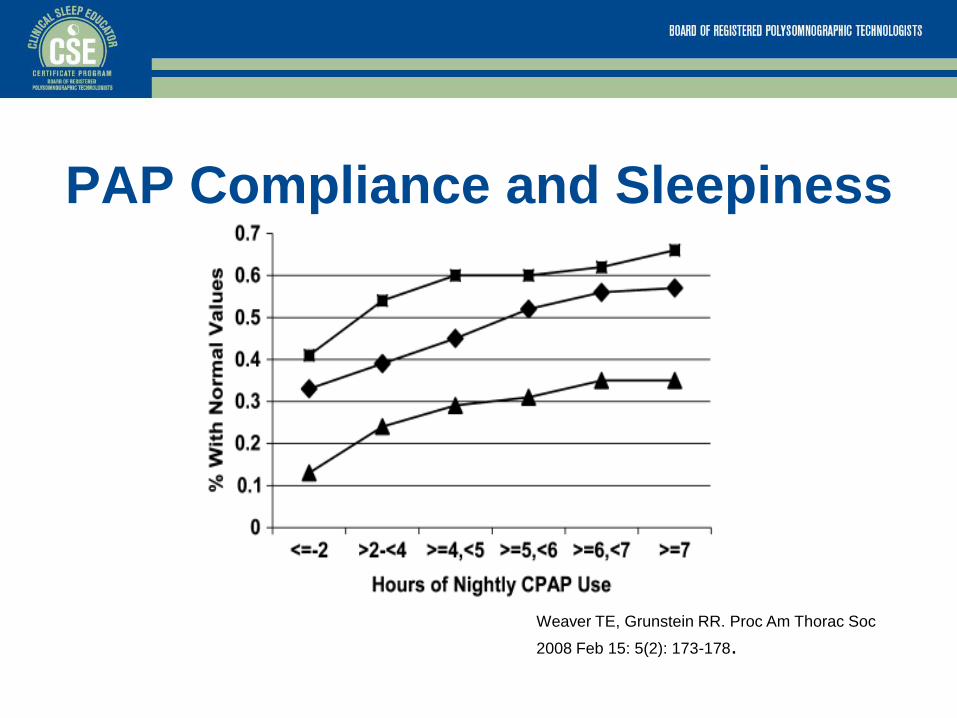
PAP Compliance and Sleepiness
Weaver TE, Grunstein RR. Proc Am Thorac Soc
2008 Feb 15: 5(2): 173-178.
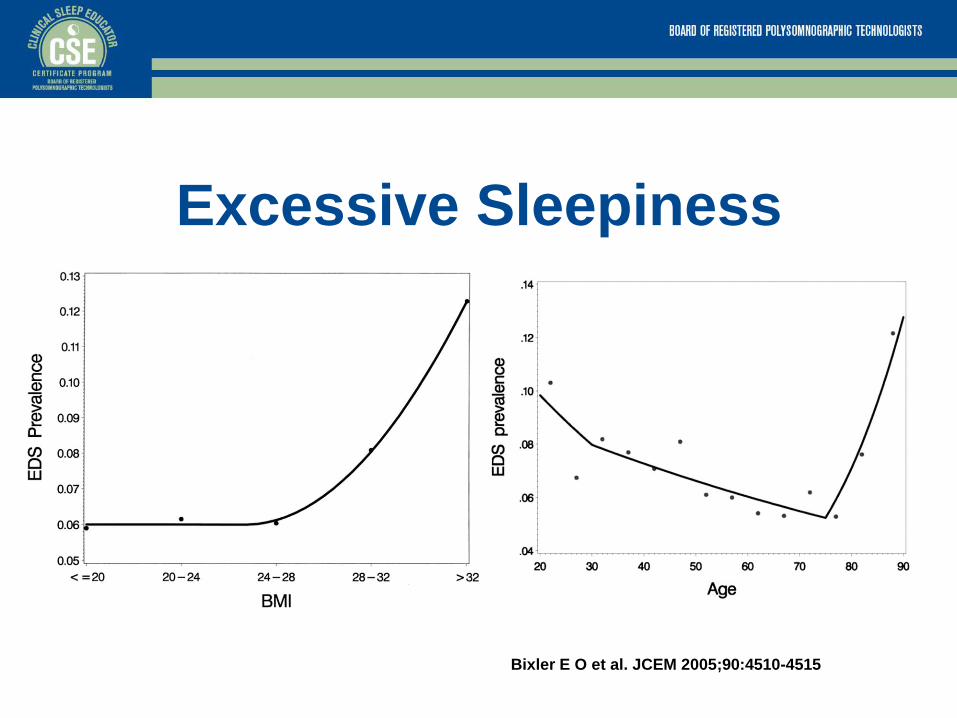
Excessive Sleepiness
Bixler E O et al. JCEM 2005;90:4510-4515
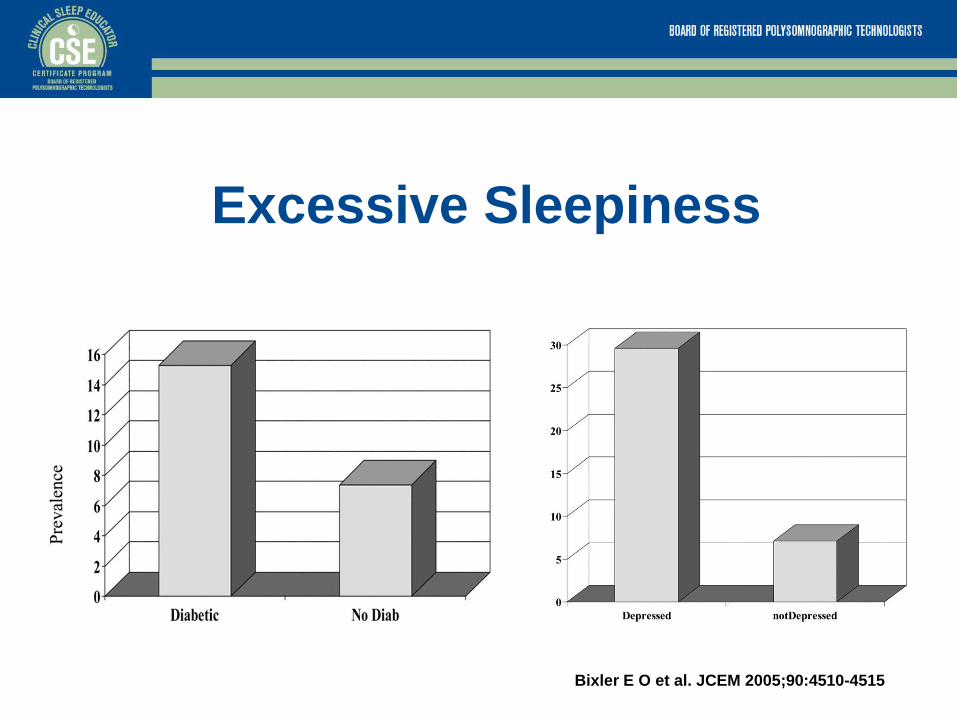
Excessive Sleepiness
Bixler E O et al. JCEM 2005;90:4510-4515
Sleep in Translation
• Are there other sleep problems?
–“It ain’t all apnea, and even when it
is-it ain’t all PAP!” R Goldberg-famous sleep philosopher
Question 1 Joe Stevens has been using CPAP for 3 months. He is not
snoring, but continues to have dry mouth (using a nasal
mask). He returns with complaints of continued daytime
sleepiness? Which of the following would be most helpful
to evaluate his ongoing concerns?
A. compliance report
B. urine drug screen
C. medication review
D. Epworth sleepiness scale
“It’s not working” (…but it
should)
• Consider timing of the problem:
– Early: learning curve, settings (pressure,
ramp, humidity), training, mask fit, side effects
– Later: equipment wear, patient changes
(weight, allergies, other medical), new side
effects
Early Equipment Issues
• Mask vs. machine
• Fit, leaks, the “180”have patient put mask on; training, refitting;
• Pressure, ramping, humidity review test, adjust ramp or heater
• Patient specifics • Sleep position review sleep test details, consider pressure
• Allergies / nasal complaints heater, filter, cleaning, RX
• Family dynamics, cultural implications
• Environmental changes • Altitude, humidity adjust settings, patient education
• Swimming with PAP or the dog ate my…

Later Equipment Issues
• Mask vs machine – Worn supplies, equipment cleaning patient education
• Patient specifics – Weight change consider pressure adjust and / or mask re-fit
– Other medical, allergies
• Environmental changes – Travel implications and adjustments humidifier, altitude
It is working…
but symptoms persist
• “I still can’t fall asleep.”
• “I still don’t sleep well.”
• “I am still sleepy.”

“I still can’t fall asleep”
– Insomnia
– Inadequate sleep hygiene
– Circadian rhythm disturbance
– Restless legs syndrome
– Medications
– Other medical or psychiatric conditions
“I still don’t sleep well.”
• Insomnia
• Inadequate sleep hygiene
• Parasomnias
• Medications
• Other medical or psychiatric conditions

Question 2 Susan Waakup is a 53 yo woman with OSA. She has been using
CPAP regularly for the past 6 months. She reports good PAP
compliance and is pleased that she is not snoring. She is still having
problems sleeping. These include trouble falling asleep, frequent
waking and “discomfort”. Her medical history includes hypertension,
hyperlipidemia, depression. She is perimenopausal. She is married
with twins who recently started college in another state. Of the
following choices, which is the best next step?
A. obtain actigraphy and order a ferritin level.
B. download PAP compliance report and start sleep logs.
C. repeat PAP titration and review medication list.
D. start auto PAP unit and refer back to her psychiatrist.
“I am still sleepy.”
• Insufficient sleep (sleep deprivation)
• Circadian rhythm disorders
• Narcolepsy and other hypersomnias
• Medications
• Other medical or psychiatric conditions
Medications and Poor Sleep • Cold and allergy remedies
• Antihypertensives (beta antagonists)
• Cardiac treatments (digoxin)
• Lipid-lowering drugs
• Thyroid supplements
• Birth control medications
• Asthma therapy
• Pain medications
• Antidepressants (especially SSRIs)
Medications and Sleepiness • Codeine (pain medications and cough suppressants)
• Morphine (and other pain medications)
• Antihypertensives (alpha 2 agonists)
• Antiarrhythmic agents (fatigue)
• Dopamine agonists (pramipexole, ropinirole)
• Antiepileptics
• Sleep aids (including benzos, non-benzos, OTC remedies)
• Anxiolytics
• Antihistamines (prescription and OTC)
• Antidepressants (older TX-TCAs, MAOIs)

Medical Conditions and Sleep
• Medical conditions commonly associated with sleep
problems: – Pregnancy
– Menopause
– Headaches
– Cardiac disease
– Pulmonary diseases
– GERD
– Rheumatologic conditions
– Chronic pain conditions (including fibromyalgia)
– Degenerative neurologic disease
– Stroke
– Substance abuse (alcohol, drugs active and withdrawal)

Psychiatric Conditions and Sleep • Depression
– Insomnia or sleepiness
– Insomnia as a risk factor for depression
• Bipolar disorder – Sleep complaints vary with cycling
• Generalized anxiety – Sleep initiation problems, or extended wake time
• Panic disorder – May be isolated nocturnal
• Schizophrenia – “In schizophrenia, sleep is habitually disturbed.”-Bleuler 1950

Insomnia(s) • Characterized by difficulty initiating sleep, disturbed sleep during the
night (or non-restorative sleep complaint).
• Considered a hyperarousal phenomenon.
• May be primary; secondary to other sleep, medical or psychiatric
conditions.
• Prevalence 5-48% in general population.
– Varies broadly by definition applied.
• Increased risk: female, older, lower socioeconomic status
• “Growth industry”!
– Role of pharmacology??
• Treatment generally includes behavioral measures.
– Cognitive therapy, stimulus control.
Inadequate Sleep Hygiene
• Behavioral condition (lifestyle).
• Routines that interfere with proper sleep
timing and stability.
• Frequent component to insomnia and
sleepiness complaints.

Good sleep hygiene
1. Keep a regular schedule for bedtime and wake time.
2. Avoid mentally or physically stimulating activities, and emotional stress close to bed. Relax prior to getting into bed.
3. The bedroom should be cool, dark and quiet.
4. No TV in the bedroom. Turn clock away-DO NOT CLOCK WATCH.
5. The bedroom is reserved for sleep (and sex).
6. Avoid naps.
7. Maintain regular daily activites. Avoid exercise close to bedtime.
8. If hungry, have a light snack at bedtime.
9. Avoid alcohol late in the evening.
10. Limit caffeine later in the day.
11. Avoid sleeping medications (prescription and OTC).

Circadian rhythm disorders
• Common theme is misalignment of body
clock and environment.
• Supported by temperature disregulation
and melatonin.
• Delayed sleep phase, advanced sleep
phase, shift work disorder, jet lag.

Question 3 Jay Night is a 22 year old man who complains of significant
daytime sleepiness. This has been a problem for 4 years.
He may nap on weekends but does not find naps
refreshing. The Epworth score is 15. Statistically, the most
likely explanation for his sleepiness is:
A. Sleep apnea
B. Narcolepsy
C. Insufficient sleep
D. Restless legs syndrome
Insufficient Sleep
• Behavioral condition.
• Limited time in bed, does not meet sleep needs.
– Sleep itself is not impaired.
• Daytime sleepiness results.
• Extended sleep hours improve symptoms.
• An epidemic!

Good Sleep Care Recipe
• Take a thorough sleep history
– Order sleep testing (if needed)
• Apply education
• Provide support
• Combine gently
• Repeat as needed
Conclusion • It ain’t all apnea!
• Even when it is apnea, patients may have
other sleep problems!
• It is our job as sleep clinicians and
educators to spread this word…
– to patients, other clinicians (and those who
determine treatment authorizations)