
Smoking Cessation Pregnancy
19
Smoking Cessation During Pregnancy A Clinician’s Guide to Helping Pregnant Women Quit Smoking 2011 Self-instructional Guide and Tool Kit An Educational Program from the American College of Obstetricians and Gynecologists
-
Upload
aimee-gutierrez -
Category
Documents
-
view
31 -
download
0
description
smoking cessation
Transcript of Smoking Cessation Pregnancy

Smoking Cessation During PregnancyA Clinician’s Guide to Helping Pregnant Women Quit Smoking
2011 Self-instructional Guide and Tool KitAn Educational Program from the American College of Obstetricians and Gynecologists
FACULTY Sharon T. Phelan, MD, FACOG Vice ChairProfessor, OB GYN Maternal Fetal Medicine University of New Mexico Health Science Center School of Medicine Albuquerque, New MexicoThis faculty member has no disclosures to declare.
Susan Albrecht, PhD, MPM, FAANAssociate Professor & Associate Dean for Student/Alumni Services, Development and Continuing Education Department of Health and Community Systems University of Pittsburgh School of Nursing Pittsburgh, Pennsylvania
This faculty member has no disclosures to declare.
Cathy L. Melvin, PhD, MPHDirector, Dissemination Core UNC Lineberger Comprehensive Cancer CenterAssociate Professor, Department of Maternal and Child Health Gillings School of Global Public Health The University of North Carolina Chapel Hill, North Carolina
This faculty member has no disclosures to declare.
CONSULTANTSCatherine Rohweder, DrPHResearch Associate UNC Lineberger Comprehensive Cancer Center The University of North Carolina Chapel Hill, North Carolina
This faculty member has no disclosures to declare.
Jane Laping, MS, MPHResearch Associate UNC Lineberger Comprehensive Cancer Center The University of North Carolina Chapel Hill, North Carolina
This faculty member has no disclosures to declare.
ACOG DIVISION OF WOMEN’S HEALTH ISSUESJanet Chapin, RN, MPHDirectorJeanne Mahoney, RN, BSNProgram Director
Theinformationisdesignedtoaidpractitionersinmakingdecisionsaboutappropriateobstetricandgynecologiccare.Theseguidelinesshouldnotbeconstruedasdictatinganexclusivecourseoftreatmentorprocedure.Variationsinpracticemaybewarrantedbasedontheneedsoftheindividualpatient,resources,andlimitationsuniquetotheinstitutionortypeofpractice.
Disclosure of Faculty and Industry RelationshipsIn accordance with College policy, all faculty members and consultants have signed a conflict of interest statement in which they have disclosed any financial interests or other relationships with industry relative to topics they discuss in this program.
THE AMERICAN COLLEGE OF OBSTETRICIANS AND GYNECOLOGISTS
CONTINUING MEDICAL EDUCATION INFORMATION . . . . . . . . . . . . . . . . . . . . . . . . . . . 2
INTRODUCTION . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 4Brief clinical interventions can substantially improve smoking cessation rates during pregnancy
EVIDENCE-BASED GUIDELINES: THE 5 A’S . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 6A five-step intervention, the 5 A’s, is readily adapted to the clinician’s style and the patient’s needs
5 A’S QUICK REFERENCE . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 16Quick reference guide to the 5 A’s and their role in smoking cessation
SIX STEPS TO IMPLEMENTATION . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 18Creating a successful smoking cessation program involves six steps and full staff participation
POSTPARTUM RELAPSE . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 21Careful documentation and positive language are key to reducing the risk of relapse
REFERENCES . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 22
APPENDIX . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 24Resource materials, checklists, and forms that may be photocopied and used in practice
SELF-ASSESSMENT QUIZ . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 29
ANSWER SHEET AND EVALUATION FORM . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 33
TABLE OF CONTENTS
1
ACCME ACCREDITATIONTheAmericanCollegeofObstetriciansandGynecologistsisaccreditedbytheAccreditationCouncilforContinuingMedicalEducation(ACCME)toprovidecontinuingmedicaleducationforphysicians.
AMA PRA CATEGORY 1 CREDIT(S)™TheAmericanCollegeofObstetriciansandGynecologistsdesignatesthisenduringmaterialforamaximumof3AMA PRA Category 1 Credits™.
Physiciansshouldonlyclaimcreditcommensuratewiththeextentoftheirparticipationintheactivity.
COLLEGE COGNATE CREDIT(S)TheAmericanCollegeofObstetriciansandGynecologistsdesignatesthisenduringmaterialforamaximumof3Category1CollegeCognateCredits.TheCollegehasareciprocityagreementwiththeAMAthatallowsAMA PRA Category 1 Credits™tobeequivalenttoCollegeCognateCredits.
CONTINUING MEDICAL EDUCATION INFORMATION
ACKNOWLEDGMENTACOGgratefullyacknowledgesTheRobertWoodJohnsonFoundationforthegrantthatmadetheoriginalactivitypossible,andTheUniversityofNorthCarolina(TheUniversityCancerResearchFund-UNCLinebergerComprehensiveCancerCenter,NCTraCS-HomeoftheCTSAatUNC,andtheUNCCenterforMaternal&InfantHealth)forthiscurrentupdate.
INSTRUCTIONS FOR EARNING CME CREDITParticipationinthisself-studyprogramshouldbecompletedinapproximately3hours.Tosuccessfullycompletethisprogramandreceivecredit,participantsmustfollowthesesteps:
1. Readthelearningobjectives.
2. Readthearticle,text,andtables.
3. Completetheregistrationinformation
4. Read,complete,andsubmitanswerstotheself-assessmentexaminationandprogramevaluationquestions.Participantsmustreceiveatestscoreofatleast70%andrespondtoallprogramevaluationquestions.
5. ACOGFellowswillreceivecognatesdirectlywhichcanbetracedintheironlineprofile.Otherclinicianswillreceiveacertificatebymail.
6. FollowmailinginstructionorFAXinginstructionsontheregistrationformattheendofthisdocument.
Ifyouhavequestionsregardingthesecontinuingmedicaleducationcredits,pleasetelephoneACOGdirectlyat(202)863-2496.
TARGET AUDIENCETheintendedaudienceforthisCMEactivityisaclinicianwhopracticesobstetrics/gynecologyandotherswhosepracticeorinterestincludesprovidinghealthcaretopregnantandpostpartumwomen.
LEARNING OBJECTIVES Uponcompletionofthiscontinuingmedicaleducationactivity,participantswillbeableto:
• employevidence-basedguidelinesforsmokingcessationduringpregnancy
• effectivelyfollowuponpatientswhoarereluctanttoquitsmoking
• understandthepotentialharmsandbenefitsofusingpharmacotherapiesasanaidtoquittingsmokingforpregnantandpostpartumwomen
• establishasmokingcessationprograminthepracticesetting
• counselpatientsaboutpostpartumrelapse
• addresspatientconcernsaboutquitting
• helppatientsovercomebarrierstosuccess
• providebothclinician-andpatient-orientedinformationsourcesonsmokingcessation
RELEASE AND EXPIRATIONReleasedate:August31,2010Expirationdate:September1,2013
2 3
INTRODUCTION
Smokingduringpregnancyisthemostmodifiableriskfactorforpoorbirthoutcomes.TheAmericanCollegeofObstetricsandGynecologistsrecommendsthatobstetrichealthcareprovidersscreenallpatientstodeterminewhethertheysmokeandoffertreatmentforsmokingcessation.Smokingduringandafterpregnancyisassociatedwithfetalandinfantrisks,includinglowbirthweight,pretermdelivery,abruptioplacentae,suddeninfantdeathsyndrome,andanincreaseinchildhoodrespiratoryillnessesaswellaspossiblecognitiveeffectsassociatedwithlearningdisabilitiesandconductdisorders(DiFranza1996,Drews1996,Fiore2008,Makin1991,Wakschlag1997).Maternalsmokingduringpregnancyincreasestheriskofectopicpregnancy,pretermprematureruptureofmembranes,placentalcomplicationsofpregnancy,pretermdelivery,andspontaneousabortion.Long-termhealthriskstowomenwhosmokeincludeheartdisease,cancer,earlydeath,andlinkstomanyotherdiseasesandhealthproblems(USDHHS2001).
Smokingduringpregnancyremainsamajorpublichealthproblem.Despitethewell-knownhealthrisksassociatedwithsmokingduringpregnancy,manywomencontinuetosmokeevenafterlearningthattheyarepregnant(USDHHS2001,Melvin2000).Thesewomenneedassistanceinquitting,andobstetrichealthcareprovidersareinauniquepositiontohelpthem.Successful smoking cessation strategies supported by clinical evidence are available and should be integrated into routine prenatal care for every pregnant woman.
Thiseducationalprogramprovidesthebackgroundandtoolsnecessaryforclinicianstoimplementaneffectivebehavioralinterventiontohelptheirpatientsquitsmoking.Theinterventiondescribedconsistsoffivesteps,iseasilyintegratedintoanofficepractice,requiresamanageableinvestmentoftimeandresources,andissupportedbyevidenceintheliterature.
RATIONALE FOR INTERVENTIONSuccessfultreatmentoftobaccouseanddependencecanhaveasignificanteffectonpregnancy-relatedoutcomes.Areviewofclinicaloutcomesforpregnantwomenwhoquitsmokingrevealeda20%reductioninthenumberoflow-birth-weightbabies,a17%decreaseinpretermbirths,andanaverageincreaseinbirthweightof28g(Lumley2000,Goldenberg2000).Quittingsmokingevenwellintothepregnancytermhasbeenshowntoprovidebenefits.Birthweightcanbesignificantlyimprovedifcessationeffortsaresuccessfulinhelpingapregnantwomantoquitsmokingbeforeher30thweekofpregnancy(Goldenberg2000,ACOG2010).
Quittingsmokingnotonlyreducesrisksofhealthproblemsforthebabyandcomplicationsduringdeliverybutalsobenefitsawoman’slong-termhealth.Smokingisassociatedwithmanyhealthrisksforwomen,including:
• Cardiovasculardisease–Mostcoronaryheartdiseaseamongwomenyoungerthan50isattributabletosmoking(USDHHS2001).
• Lungcancer–Lungcancersurpassedbreastcancerastheleadingcauseofcancerdeathinwomenin1987.About90%ofalllungcancerdeathsamongUSwomensmokersareattributabletosmoking(USDHHS2001).
• Prematuredeath–Theannualriskfordeathfromallcausesisabout80%to90%greateramongwomenwhosmokecomparedwiththosewhohaveneversmoked.Foreverydeathattributabletosmoking,anaverageof14yearsoflifeislost.
Quittingsmokingsubstantiallyreducestheriskforcoronaryarterydiseasewithineventhefirstyearandreducestheriskofotherhealthproblemsincludingcervicalcancer,kidneydisease,respiratorydisease,hipfractures,menstrualdisorders,early
menopause,fertilityproblems,anddepression(USDHHS2001).
Cost effectiveness of intervention.Tobaccodependenceinterventionsforpregnantwomenareparticularlycost-effectivebecausetheyreducethenumberoflowbirth-weightbabiesandperinataldeaths(Lightwood1999),reduceuseofnewbornintensivecareunits,shortenlengthsofstay,anddecreaseserviceintensity(Adams2004).A2006analysisindicatedthatimplementingasmokingcessationinterventionsuchasthe5A’swouldcostfrom$24to$34andsave$881perU.S.pregnantsmoker,nettingsavingsofupto$8millioninavertedneonatalcostsgivena70%increaseinquitrate(Ayadi2006).
Smokeless and non-cigarette tobacco useisbecomingmoreprevalentamongyoungwomen.Likecigaretteuse,smokelesstobacco,suchaschewingtobacco,snuff,moistsnuff(snus),dissolvabletobaccostripsandelectroniccigarettescontainnicotine,areaddictive,andhaveserioushealthconsequencesforthepregnantwomanandherfetus.Non-cigarettetobaccouseisnotasaferalternativetosmokingnoristhereevidencetosuggestthatitiseffectiveinhelpingsmokersquit.(Fiore,2008)
Intervention for smoking cessation.Theaddictivepropertiesofnicotinemakeitdifficultformostsmokerstoquitwithoutsometypeofassistance.Becauseobstetriciansandotherprenatalcarecliniciansseetheirpatientsregularlyduringpregnancy,theyareinauniquepositiontoprovidethatassistancethoughbehavioralstrategiesdesignedtohelppregnantwomenquitsmoking.Pregnancyisaprime“teachablemoment”inhealthcare.Womenaremorelikelytoquitsmokingduringpregnancythenatanyothertimeintheirlives(USDHHS2001).Amother-to-beisgenerallyhighlymotivatedtodowhatshecantohaveahealthybaby.Clinicianscantapintothatmotivationtohelpparentsachievelong-termhealthylifestylechangesforthemselvesandtheirfamilies.
Althoughastandardizedpregnancy-specificsmokingcessationinterventionbyclinicianshasbeenshowntoimprovequitratesamongsmokers,itisgenerallynotintegratedintoregularprenatalvisits(Fiore1995,Jaen1997,Kreuter2000,Prochazka2000,Sippel1999,Thorndike1998).Ina2001surveyofsmokinginterventionpracticesbyobstetrician-gynecologists,nearlyallcliniciansreportedthatthey“always”askedaboutsmokingstatus(93%)andadvisedpatientstoquit(90%);however,fewrespondentsofferedtoassistpatientswithcessation(28%)orfollowedupwithpregnantpatients(24%)(Grimley2001).Cliniciansmaybeunawarethattheirprovisionofbriefcounselingsessionsusingpregnancy-specificself-helpmaterialscanincreasecessationrates(Dolan-Mullen1999).
Recommendationsforpregnancy-specificsmokingcessationinterventionsarebasedontheresultsofrandomizedclinicaltrialsofvariouscessationmethodsforpregnantsmokers.Ameta-analysispreparedforthe2008USPublicHealthService(PHS)Treating Tobacco Use and Dependence: A Clinical Practice Guidelineconcludedthatperson-to-personpsychosocialinterventionsaremoreeffectivethanminimaladvicetoquit.Cessationratesare80%higher(OR1.8,CI1.4-2.3)forpregnantsmokerswhoreceivecounseling(seeStudies of Smoking Cessation Intervention for Pregnant Patients,Appendix,page28).Evenpregnancy-specific,self-helpmaterialsaloneincreasecessationrateswhencomparedtousualcare.Theguidelinesalsorecommendthattobaccodependenceinterventionstakeplacenotonlyatthefirstprenatalvisit,butthroughoutpregnancy.
4 5

Abrief,fivestepinterventionprogram,referredtoasthe“5A’s”model,isrecommendedinclinicalpracticetohelppregnantwomenquitsmoking(Fiore2008,Melvin2000,ACOG2010).The5A’sincludethefollowing:
• Askabouttobaccouse.
• Advisetoquit.
• Assesswillingnesstomakeaquitattempt.
• Assistinquitattempt.
• Arrangefollow-up.
ThisapproachwasoriginallypublishedbytheNationalCancerInstituteandhasbeenreviewedandupdatedbyseveralgovernmental,academic,andprivateeducationgroups(Glynn1990,Melvin2000,Fiore2008).Althoughsomeprofessionalorganizationsendorseathree-stepprocess“Ask,advise,andrefer,”thismethodhasnotbeenproventobeeffectiveinpregnancy.
ThePHSpublication,TreatingTobaccoUseandDependence:AClinicalPracticeGuideline,2008Updatedescribesthe5A’sinterventionindetailandprovidesachapteraboutspecialpopulations,includingpregnantwomen(Fiore2008).ThePHSguidelineapproachessmokingasachroniccondition,similartodiabetesorhypertension,andstressestheneedforregular,consistentcounseling.Thisperspectiveacknowledgesthedifficultyinquittingsmokingandremainingabstinentgiventheaddictivepropertiesofcigarettes.Alloftherecommendationsthatformedthebasisforthe5A’sapproachwereratedaccordingtothequalityandquantityofempiricalsupportingevidenceinthemedicalliterature(Table1).Drawingonthe5A’sapproach,theAmericanCollegeofObstetriciansandGynecologistspublishedaCommitteeOpinionthatincludesinterventionstepsspecificallydesignedforpregnantwomen(ACOG2010).InformationfromthePHSguideline,theAmericanCollegeofObstetriciansandGynecologist’scommittee
EVIDENCE-BASED GUIDELINES: THE 5 A’S opinion,andadditionalinformationpublishedinthemedicalliteratureabouthowtousethe5A’sapproachhasbeenconsolidatedinthisguidetoprovideclinicianswithacompleteresourceforhelpingpregnantpatientsquitsmoking(Fiore2008,Melvin2000,ACOG2010).
The5A’sapproachtosmokinginterventionfollowsaspecificprotocol,oralgorithm,withsomescriptedmaterial.Thesuggestedlanguagecanbeadaptedtotheclinician’spersonalstyleandthepatient’sindividualneeds.Ifthe5A’sareintegratedintoexistingroutines,thetimecommitment–measuredinminutes–ismanageablewithinaclinicalsettingandisfaroutweighedbythepotentialforreducingthesubstantialriskthatsmokingposestomothersandtheirbabies(Hartmann2000).The5A’sapproachissummarizedinaquickreferenceguideonpage16.
FIRST A: ASK – 1 MINUTEAsk the patient about her tobacco use at every first prenatal visit, document it as a vital sign, and track smoking status at every visit.(Fiore,1995)
Screeningfortobaccouseshouldoccurautomaticallyaspartoftheinitialhistory.Societalstigmaaboutsmoking,especiallyduringpregnancy,maycausesomepatientstofeeluncomfortableaboutdiscussingwhethertheysmokeandhowmuch.Infact,somedatasuggestthatfrom13%to26%ofpregnantsmokersmaynotdisclosethattheysmokewhenaskedaboutitasapartofaroutineclinicalinterview(Boyd1998).Themannerinwhichcliniciansaskaboutsmokingstatusduringtheinitialinterviewcandramaticallyimprovetheaccuracyoftheresponse(seeHow to Intervene,Appendix,page24).Ratherthanaskingthepatientayes/noquestionsuchas“Doyousmoke?”amultiplechoiceresponseshouldbeusedtoimprovedisclosureandprovideusefulinformationforcounseling.Thisapproachimprovesdisclosureby40%forallwomenincludingthoseofvariousethnicbackgrounds(Dolan-Mullen1991).Forexample:
Question: Which of the following statements best describes your cigarette smoking?
A. Ihaveneversmoked,orIhavesmokedfewerthan100cigarettesinmylifetime.
B. IstoppedsmokingbeforeIfoundoutIwaspregnant,andIamnotsmokingnow.
C. IstoppedsmokingafterIfoundoutIwaspregnant,andIamnotsmokingnow.
D. Ismokesomenow,butIcutdownonthenumberofcigarettesIsmokesinceIfoundoutIwaspregnant.
E. Ismokeregularlynow,aboutthesameasbeforeIfoundoutIwaspregnant(Dolan-Mullen1994).
Aquestionaboutsmokingstatuscanbeincludedinageneralwrittensurveyaboutpatienthealththatisprovidedtothepatientbeforevisitingtheclinician,butsomecliniciansprefertoaskaboutsmokingstatusaspartofthepatientinterview.Themultiple-choiceresponseformathasbeenshowntobeeffectivewhetherdeliveredverballyorinwrittenform(Dolan-Mullen1991).Whenquestioningadolescentpatientsaboutsmokingstatus,keepinmindthatyoungpatientscanbecomeaddictedveryquicklyandarealreadyestablishedsmokersbythetimetheyhavesmoked100cigarettes(ResearchTriangleInstitute2001).
Somecliniciansusephysiologicmarkerssuchasurinetestsorbloodsamplestodeterminewhetherapatientissmoking.The“goldstandard”forvalidatedself-reportedsmokingstatusisblood,urine,orsalivacotininelevels.Expiredcarbonmonoxideisanotherwaytodeterminesmokingstatus.Testingisunnecessaryforimplementingasuccessfulcounselinginterventionintheclinicalsettingandisgenerallyreservedforuseinclinicaltrials.Ithasbeensuggested,however,thattestingandcommunicationofresultscanbeusedasamotivationaltoolforsomesmokers.Expiredcarbonmonoxidetestingmayprovideatangibleincentivetoquitsmoking–forexample,forsomepatients,blowing“cleanair”mayreinforcetheidea
TA
BL
E 1
TREATING TOBACCO USE AND DEPENDENCE 2008: PREGNANCY RECOMMENDATIONS WITH STRENGTH-OF–EVIDENCE RATINGS (FIORE 2008)
Recommendation:Becauseof the serious risks of smoking to thepregnant smoker and thefetus, whenever possible pregnant smokers should be offered person-to-person psychosocialinterventionsthatexceedminimaladvicetoquit.Strength of evidence = A*.
Recommendation: Although abstinence early in pregnancy will produce the greatestbenefits to the fetus and expectant mother, quitting at any point in pregnancy can yieldbenefits. Therefore, clinicians should offer effective tobacco dependence interventions topregnant smokers at the first prenatal visit as well as throughout the course of pregnancy.Strength of evidence = B†.
*A:Multiplewell-designedrandomclinicaltrials,directlyrelevanttotherecommendation,yieldedaconsistentpatternoffindings.
†B:Someevidencefromrandomizedclinicaltrialssupportedtherecommendations,butotherscientificsupportwasnotoptimal.
6 7
thattoxinsarebeingeliminatedfromtheirbodies(Hartmann2000).
Smokingisoneofonlyafewimportantriskfactorsthatcanbemodifiedandshouldthereforebetrackedasavitalsignateveryvisit,justasbloodpressurewouldbetracked(Fiore,1995).IdeasfordocumentingsmokingstatusandusingothersupplementarytoolsarepresentedinTable2.
SECOND A: ADVISE – 1 MINUTEAdvise all tobacco users to stop using tobacco.
Advicetoquitshouldbeclear,strong,andpersonalizedwithunequivocalmessagesaboutthebenefitsofquittingforboththepatientandher
baby.Aneffectivewaytostartthediscussionaboutquittingistosay,“Mybestadviceforyouandyourbabyisforyoutoquitsmoking.”
Additionaladvicecanthenbetailoredtothepatient’ssituationandtheirresponsestothemultiplechoice“Ask”Question,usingpositivelanguageandfocusingonthepositivebenefitsofquitting.Althoughcliniciansarekeenlyawareofthedangersmokingposestoinfantsandthelong-termhealthrisksformothers,itiscommonforpatientstominimizerisks.
Focusingonbadoutcomessuchaslowbirthweightordeliverycomplicationsmaybeineffectiveforpatientswhobelievetheyarenotatrisk,especiallyiftheyorpeopletheyknowhavehaduncomplicated,
healthypregnancieswhilesmoking.Describingthegoodthingsthepatientcandoforherselfandherbabybyquittingsmokingappealstoherdesiretobeagoodmother.Table3includesexamplesofbenefitsofquittingthatclinicianscanusewhenadvisingpatients.
Patientsmaydoubtthatcliniciansunderstandhowdifficultitistoquit.Acknowledgingbarrierstoquittingwhileprovidingencouragementmaymakethepatientmorereceptivetoadvice.Youmay
alsowishtoincludeapersonalreasonforquittingidentifiedbythepatientherself.
Thefollowingstatementisanexampleofhowtoacknowledgethedifficultyofquittingwhileofferingencouragement:“IknowI’maskingyoutodosomethingthattakesalotofeffort,butmybestadviceforyouandyourbabyistoquitsmoking.Ialsoseefromyourpatientquestionnairethatyouhaveahistoryofbronchitisandasthma.Quittingsmokingwillhelpyoufeelbetterandprovideahealthierenvironmentforyourbaby”(Hartmann2000).
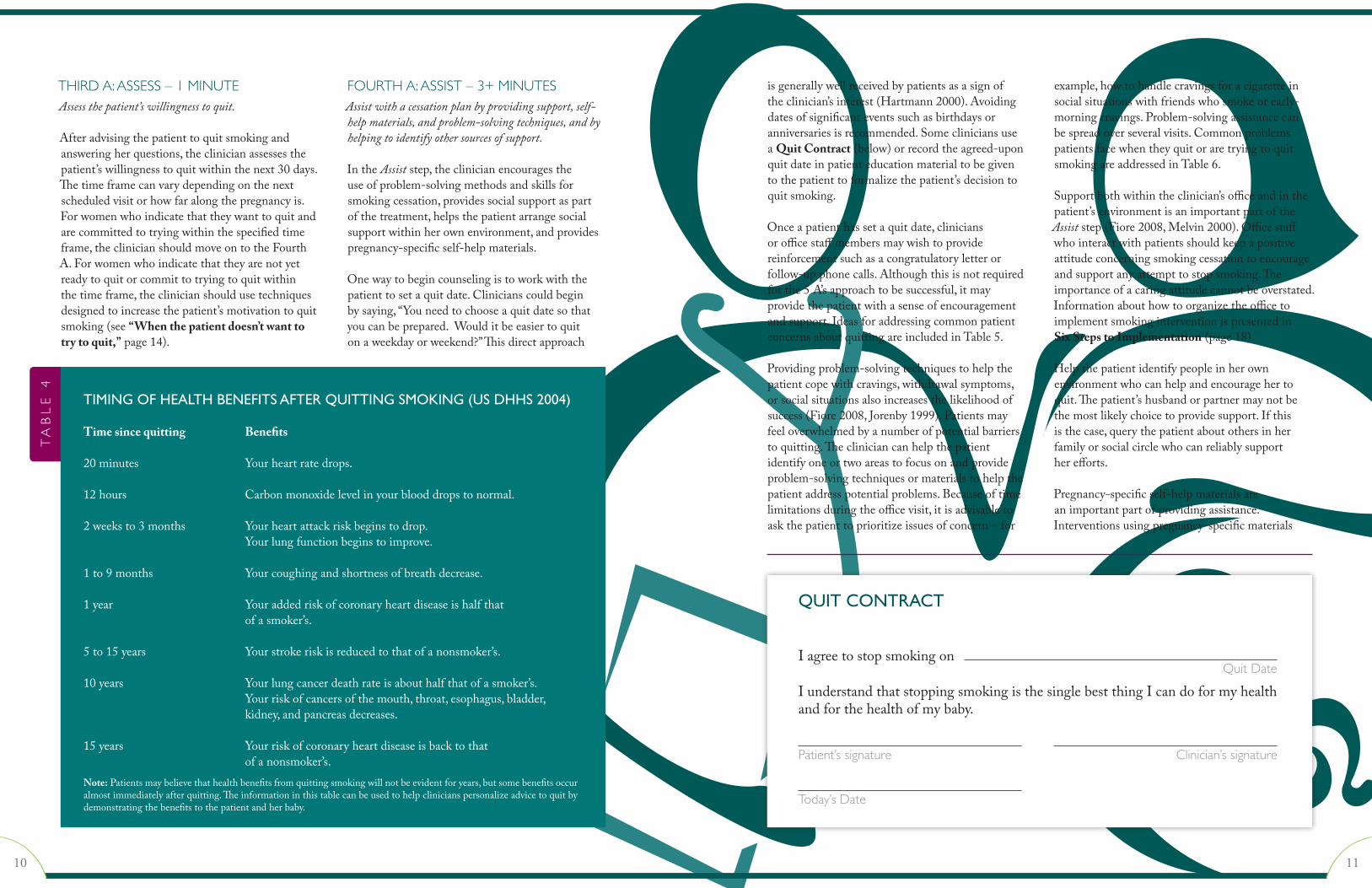
Apatientmayhavetheimpressionthatittakesalongtimeafterquittingbeforeherhealthorthehealthofherbabyimproves,butbenefitsbeginimmediately.Table4delineateshowquicklybeneficialhealthchangesoccurafterquittingsmoking(USDHHS2004).OtherpatientquestionsorconcernsaboutquittingsmokingandsampleresponsesareincludedinTable5.
Somewomenwillreducethenumberofcigarettestheysmokeratherthantryingtoquitcompletely,butsmokingevenasmallnumberofcigarettesisassociatedwithdecreasedinfantbirthweight.Ifapatientsuggestscuttingdownasastrategy,theclinicianshouldletherknowthatwhilesmokingfewerthanfivecigarettesinadaymayreducerisk,quittingisthebestthingshecandoforherselfandherbaby(England2001).
Theimportanceofcommunicatingunequivocaladvicetoquitcannotbeoverstated,butadmonishingthepatientisineffective.Ifyoustatethatyourbestadviceisforthepatienttoquit,youhavecommunicatedclearlywithoutmakingthepatientfeelcriticized(Hartmann2000).
Advise all recent quitters to remain smoke-free.Ifthepatientindicatesthatsherecentlyquitsmoking(answersBorCtothequestionaboutcigarettesmoking),congratulateherfornotsmoking,andreiteratetheimportanceofstayingsmoke-freeandavoidingsituationswhereothersaresmoking.Letherknowthatyouwillbeaskinghowsheisdoingatfuturevisits.
TA
BL
E 2
Ask
• Program a reminder into your EMRsystemtoscreenfortobaccouse
• Use the standardized multiple-choicequestiontoaskpatientsaboutsmokingstatus
• Recordsmokingstatusasavitalsigninthepatientrecord(Fiore1995)
Advise
• Provide pregnancy-specific educationalmaterials about health risks and thebenefitsofquittingformotherandbaby
Assess
• Refer toa calendar tohelp thepatientchooseaspecificquitdate
Assist
• Write out a “Prescription to Quit,”including a quit date and cessationresources (e.g. 1-800-QUIT NOW,www.smokefree.gov)
• Fax a referral to thequitlinewhile thepatientisintheoffice
• Signa“QuitContract”betweenpatientandclinician
• Provide a patient diary or phoneapplication for recording smokingtriggers prior to quitting or problemsandsuccessafterquitting
• Practice a “no smoking” dialog thepatientcanusewithfamilyandfriends
Arrange
• Program a reminder into your EMRsystemto follow-uponsmokingstatusateveryprenatalvisit
• Send a congratulatory letter from theofficeifapatientquits
Note:Thetoolsassociatedwitheachstepofthe 5 A’s approach are not required for theintervention to work, but some cliniciansandsomeofficestaffmembersusethemforinformation-gathering and organization aswellasforpatientsupport.
SUPPLEMENTARY TOOLS FOR THE 5 A’S APPROACH
TA
BL
E 3 POSITIVE EFFECTS OF
SMOKING CESSATION DURING PREGNANCY
When you stop smoking...
• yourbabywill getmoreoxygen, evenafterjustonedayofnotsmoking
• your baby is less likely to havebronchitisandasthma
• thereislessriskthatyourbabywillbeborntooearly
• thereisabetterchancethatyourbabywillcomehomefromthehospitalwithyou
• youwillbelesslikelytodevelopheartdisease, stroke, lung cancer, chroniclungdisease,andother smoke relateddiseases
• youwillbemorelikelytolivetoknowyourgrandchildren
• youwillhavemoreenergyandbreathemoreeasily
• youwillhavemoremoneythatyoucanspendonotherthings
• yourclothes,hair,andhomewillsmellbetter
• yourfoodwilltastebetter
• youwillfeelgoodaboutwhatyouhavedoneforyourselfandyourbaby
8 9
THIRD A: ASSESS – 1 MINUTEAssess the patient’s willingness to quit.
Afteradvisingthepatienttoquitsmokingandansweringherquestions,theclinicianassessesthepatient’swillingnesstoquitwithinthenext30days.Thetimeframecanvarydependingonthenextscheduledvisitorhowfaralongthepregnancyis.Forwomenwhoindicatethattheywanttoquitandarecommittedtotryingwithinthespecifiedtimeframe,theclinicianshouldmoveontotheFourthA.Forwomenwhoindicatethattheyarenotyetreadytoquitorcommittotryingtoquitwithinthetimeframe,theclinicianshouldusetechniquesdesignedtoincreasethepatient’smotivationtoquitsmoking(see“When the patient doesn’t want to try to quit,”page14).
FOURTH A: ASSIST – 3+ MINUTESAssist with a cessation plan by providing support, self-help materials, and problem-solving techniques, and by helping to identify other sources of support.
IntheAssiststep,theclinicianencouragestheuseofproblem-solvingmethodsandskillsforsmokingcessation,providessocialsupportaspartofthetreatment,helpsthepatientarrangesocialsupportwithinherownenvironment,andprovidespregnancy-specificself-helpmaterials.
Onewaytobegincounselingistoworkwiththepatienttosetaquitdate.Clinicianscouldbeginbysaying,“Youneedtochooseaquitdatesothatyoucanbeprepared.Woulditbeeasiertoquitonaweekdayorweekend?”Thisdirectapproach
isgenerallywellreceivedbypatientsasasignoftheclinician’sinterest(Hartmann2000).Avoidingdatesofsignificanteventssuchasbirthdaysoranniversariesisrecommended.SomecliniciansuseaQuit Contract(below)orrecordtheagreed-uponquitdateinpatienteducationmaterialtobegiventothepatienttoformalizethepatient’sdecisiontoquitsmoking.
Onceapatienthassetaquitdate,cliniciansorofficestaffmembersmaywishtoprovidereinforcementsuchasacongratulatoryletterorfollow-upphonecalls.Althoughthisisnotrequiredforthe5A’sapproachtobesuccessful,itmayprovidethepatientwithasenseofencouragementandsupport.IdeasforaddressingcommonpatientconcernsaboutquittingareincludedinTable5.
Providingproblem-solvingtechniquestohelpthepatientcopewithcravings,withdrawalsymptoms,orsocialsituationsalsoincreasesthelikelihoodofsuccess(Fiore2008,Jorenby1999).Patientsmayfeeloverwhelmedbyanumberofpotentialbarrierstoquitting.Thecliniciancanhelpthepatientidentifyoneortwoareastofocusonandprovideproblem-solvingtechniquesormaterialstohelpthepatientaddresspotentialproblems.Becauseoftimelimitationsduringtheofficevisit,itisadvisabletoaskthepatienttoprioritizeissuesofconcern–for
example,howtohandlecravingsforacigaretteinsocialsituationswithfriendswhosmokeorearly-morningcravings.Problem-solvingassistancecanbespreadoverseveralvisits.CommonproblemspatientsfacewhentheyquitoraretryingtoquitsmokingareaddressedinTable6.
Supportbothwithintheclinician’sofficeandinthepatient’senvironmentisanimportantpartoftheAssiststep(Fiore2008,Melvin2000).Officestaffwhointeractwithpatientsshouldkeepapositiveattitudeconcerningsmokingcessationtoencourageandsupportanyattempttostopsmoking.Theimportanceofacaringattitudecannotbeoverstated.InformationabouthowtoorganizetheofficetoimplementsmokinginterventionispresentedinSix Steps to Implementation(page18).
Helpthepatientidentifypeopleinherownenvironmentwhocanhelpandencouragehertoquit.Thepatient’shusbandorpartnermaynotbethemostlikelychoicetoprovidesupport.Ifthisisthecase,querythepatientaboutothersinherfamilyorsocialcirclewhocanreliablysupportherefforts.
Pregnancy-specificself-helpmaterialsareanimportantpartofprovidingassistance.Interventionsusingpregnancy-specificmaterials
TA
BL
E 4
TIMING OF HEALTH BENEFITS AFTER QUITTING SMOKING (US DHHS 2004)
Time since quitting Benefits
20minutes Yourheartratedrops.
12hours Carbonmonoxidelevelinyourblooddropstonormal.
2weeksto3months Yourheartattackriskbeginstodrop. Yourlungfunctionbeginstoimprove.
1to9months Yourcoughingandshortnessofbreathdecrease.
1year Youraddedriskofcoronaryheartdiseaseishalfthat ofasmoker’s.
5to15years Yourstrokeriskisreducedtothatofanonsmoker’s.
10years Yourlungcancerdeathrateisabouthalfthatofasmoker’s. Yourriskofcancersofthemouth,throat,esophagus,bladder, kidney,andpancreasdecreases.
15years Yourriskofcoronaryheartdiseaseisbacktothat ofanonsmoker’s.Note:Patientsmaybelievethathealthbenefitsfromquittingsmokingwillnotbeevidentforyears,butsomebenefitsoccuralmostimmediatelyafterquitting.Theinformationinthistablecanbeusedtohelpclinicianspersonalizeadvicetoquitbydemonstratingthebenefitstothepatientandherbaby.
QUIT CONTRACT
Iagreetostopsmokingon
IunderstandthatstoppingsmokingisthesinglebestthingIcandoformyhealthandforthehealthofmybaby.
Quit Date
Clinician’s signaturePatient’s signature
Today’s Date
10 11
havebeenfoundtoimprovequitratescomparedwithinterventionsthatdonotincludeself-helpmaterials(Melvin2000,Windsor1985).Pregnancyrelatedself-helpmaterialsshouldreinforcecounselingofferedintheAssiststep,includepregnancyspecifictechniquestohelpthepatientquit,andpromotebenefitsgainedfromquitting.Materialsshouldbereadilyavailableandproducedinaformatthatcanbeusedinthepatient’senvironment.Printmaterialsmaybemoreaccessiblethanvideotapesoraudiotapes,forexample.(SeeResources for Clinicians and Patients, Appendix,pages26-27.)
Thesmokingcessationquitline,1-800-QUITNOW,offersstatespecificresourcesandprogrammedcounselingsessionsforcallers.SomequitlineservicesprovidecounselinginbothSpanishandEnglishandofferservices24hoursaday,7daysaweek.Manystatesofferapregnancyspecificquitprotocolwithcounselorstrainedtoaddressprenatalsmokingandpostpartumrelapseatkeyintervalsspecifictothepregnancy,butallstatequitlinesmaynotofferequallyeffectivecounseling
methods.Aproviderfaxreferraloptionmayalsobeprovidedsothatoncethepregnantwomansignsarelease,quitlinecounselorscallherandarrangecontinuedtelephonecounselingsessions.Whenthecounselorinitiatesthecalltothepregnantsmoker,itisaproactiveapproach.Inareactiveapproachtheinitiativetocallmustcomefromthesmoker.Ameta-analysisofsixty-fivetrialsfoundproactivetelephonecounselingofthreeormorecallstobemoreeffectivethanaminimalinterventionthatwouldincludeself-helpmaterialsandbriefadvice(Stead2006).
Assisting Heavy SmokersPregnantwomenwhosmokemorethanapackadayandareunabletoquitafterparticipatinginthebehavioralinterventionapproachpresentedinthismodulemayneedadditionalassistance.Moreintensivecounselingcanhelpsomewomenandshouldbeofferedevenifareferralisneeded.Telephonequitlineservicescanbeespeciallyhelpfultoheavysmokerswhoaretryingtoquit.
FIFTH A: ARRANGE – 1+ MINUTESArrange follow up to monitor smoking status and provide support.
Thefinalandongoingstepinthe5A’sapproachistoarrangefollow-up.Follow-upvisitsshouldincluderepeatassessmentsofsmokingstatus.Forpatientsattemptingtoquit,thesevisitsshouldallowtimetomonitortheirprogress,reinforcethestepstheyaretakingtoquit,andpromote
problem-solvingskills.Providingencouragementandpositivereinforcementfortheireffortsisimportanttomaintainmotivation.Patientswhoarestillsmokingshouldbeadvisedtoquitateachopportunity(seeSecond A: Advise,page8).Thosewhoareheavysmokersorwhocontinuetorelapsemayneedmoreintensivebehavioralcounseling.
Changestotheofficesettingandpoliciescanfacilitateimplementationofthe5A’sintoroutine
TA
BL
E 5
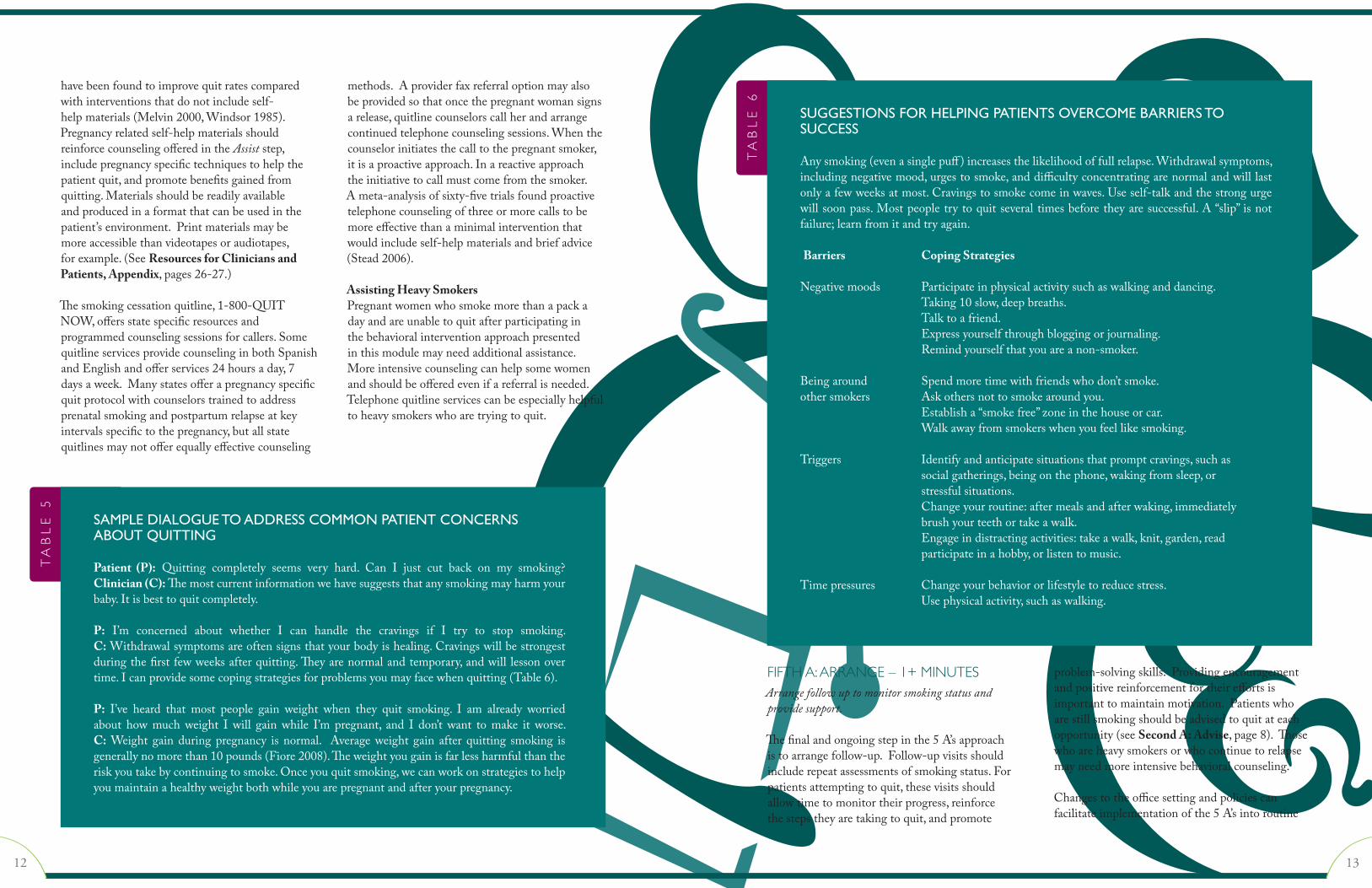
SAMPLE DIALOGUE TO ADDRESS COMMON PATIENT CONCERNS ABOUT QUITTING
Patient (P): Quitting completely seems very hard. Can I just cut back on my smoking?Clinician (C):Themostcurrentinformationwehavesuggeststhatanysmokingmayharmyourbaby.Itisbesttoquitcompletely.
P: I’m concerned about whether I can handle the cravings if I try to stop smoking.C:Withdrawalsymptomsareoftensignsthatyourbodyishealing.Cravingswillbestrongestduringthefirstfewweeksafterquitting.Theyarenormalandtemporary,andwilllessonovertime.Icanprovidesomecopingstrategiesforproblemsyoumayfacewhenquitting(Table6).
P: I’ve heard that most people gain weight when they quit smoking. I am already worriedabout how much weight I will gain while I’m pregnant, and I don’t want to make it worse.C:Weight gainduringpregnancy isnormal. Averageweight gain after quitting smoking isgenerallynomorethan10pounds(Fiore2008).Theweightyougainisfarlessharmfulthantheriskyoutakebycontinuingtosmoke.Onceyouquitsmoking,wecanworkonstrategiestohelpyoumaintainahealthyweightbothwhileyouarepregnantandafteryourpregnancy.
TA
BL
E 6
SUGGESTIONS FOR HELPING PATIENTS OVERCOME BARRIERS TO SUCCESS
Anysmoking(evenasinglepuff )increasesthelikelihoodoffullrelapse.Withdrawalsymptoms,includingnegativemood,urgestosmoke,anddifficultyconcentratingarenormalandwilllastonlyafewweeksatmost.Cravingstosmokecomeinwaves.Useself-talkandthestrongurgewillsoonpass.Mostpeopletrytoquitseveraltimesbeforetheyaresuccessful.A“slip”isnotfailure;learnfromitandtryagain.
Barriers Coping Strategies
Negativemoods Participateinphysicalactivitysuchaswalkinganddancing. Taking10slow,deepbreaths. Talktoafriend. Expressyourselfthroughbloggingorjournaling. Remindyourselfthatyouareanon-smoker.
Beingaround Spendmoretimewithfriendswhodon’tsmoke.othersmokers Askothersnottosmokearoundyou. Establisha“smokefree”zoneinthehouseorcar. Walkawayfromsmokerswhenyoufeellikesmoking.
Triggers Identifyandanticipatesituationsthatpromptcravings,suchas socialgatherings,beingonthephone,wakingfromsleep,or stressfulsituations. Changeyourroutine:aftermealsandafterwaking,immediately brushyourteethortakeawalk. Engageindistractingactivities:takeawalk,knit,garden,read participateinahobby,orlistentomusic.
Timepressures Changeyourbehaviororlifestyletoreducestress. Usephysicalactivity,suchaswalking.
12 13

care.Implementingatobaccouseridentificationsystem,dedicatingstafftodelivertobaccocessationtreatment,educatingallstaff,andprovidingresourcesarechangesrecommendedinthe2008ClinicalPracticeGuidelines.InformationabouthowtoorganizetheofficetoimplementsmokinginterventionispresentedinSix Steps to Implementation(page18).
PHARMACOLOGIC INTERVENTIONPregnantpatientsshouldtrytoquitsmokingwithoutusingpharmacologicagents.The5A’sapproachhasbeenshowntobeaneffectivebehavioralstrategyforsmokingcessation.
Pharmacologicaidssuchasnicotinereplacementtherapy(NRT),bupropion,andvareniclinehavenotbeensufficientlytestedforefficacyandsafetyinpregnantpatientsandshouldnotbeusedasfirst-linesmokingcessationstrategiesforthesepatients.Evidenceisinconclusivethatsmokingcessationmedicationsboostabstinenceratesinpregnantsmokers.Inaddition,U.S.clinicaltrialswithsufficientpowertodeterminestatisticalsignificancehavebeenpulledorendedduetodataorsafetymonitoringissues(Fiore2008).
Ifpharmacotherapyisconsideredforpregnantsmokerswhoareunabletoquitsmokingbyothermeans,itisimportantthewomandemonstratearesolvetoquitsmokingandtounderstandthebenefitsandrisksoftheuseofthemedicationtoherselfandherfetus.Cliniciansshouldcarefullyreviewpatientinformation,drugsideeffectprofiles,andcurrentinformationinmedicalliteraturewhenrecommendingpharmacologicaids.
Sinceantidepressantsmarketedforsmokingcessation,suchasbupropion,carryrisksofadverseeffectsincluding:increasedriskforsuicide,insomniaandrhinitis.Pregnantpatientswhochoosetousesmokingcessationmedicationsshouldbecloselysupervised.
Concomitant Alcohol UseApregnantsmokerwhoalsousesalcoholshouldbeencouragedtodiscontinuebothcigarettesand
alcoholandbeofferedcounselingusingthe5A’sapproach.InformationaboutrisksassociatedwithalcoholuseduringpregnancyshouldbeaddedtotheAdvisestep,andspecificstrategiesforabstainingfromalcoholshouldbediscussedintheAssiststep(Melvin2009).
WHEN THE PATIENT DOESN’T WANT TO TRY TO QUIT: MOTIVATIONAL INTERVENTIONSApatientwhodeclinestomakeaquitattemptduringtheAdvisestepmayhavereasonsfornotquittingthatsheisunableorunwillingtoexpress,orshemaythinktherisksdonotapplytoher.The2008ClinicalPracticeGuidelinesstatethatMotivationalInterventionsareeffectivewithStrengthofEvidence=B(SeeStrength of Evidence. Appendix,page27).Onetypeofintervention,otherwiseknownas5R’s,isoftenused:relevance,risks,rewards,roadblocks,andrepetition(Table7)(Fiore2008).Itisunnecessarytoaddressallofthe5R’sinasinglevisit;rather,considertheoneortwothatarerelevant,dependingonthepatient’scommentsduringtheAdviseandAssesssteps.Ifshesaysshedoesn’tthinkshecanquitinthenext30days“becausemyhusbandsmokesandheisn’treadytoquit,too,”or,“Idon’tthinkIneedtoquitbecauseIsmokedthelasttimeIwaspregnantandmybabyisfine,”usetheappropriate
“R”tohelp.Inthefirstexample,considertheroadblockpresentedbythiswoman’shusband’ssmoking,andinthesecond,denialofrisk.(SeeACOG,2009).
Ifthepatientremainsuninterestedinquittingafterthe5R’s,clinicianscankeepcommunicationlinesopenbyendingthetalkwithastatementsuchas,“Iunderstandthatyouarenotreadytoquit,butwouldyouthinkaboutitforournextvisit?”Patientswillcontinuetolistentoclinicianadviceevenwhentheyareunpreparedtoactonit.Smokingistooimportantnottomention.The5R’smayhelpapatientidentifypersonalreasonstoquitthatcanmotivatehertoeventuallytrytoquitsmoking.
TA
BL
E 7
Relevance.Encouragethepatienttodiscusswhy quitting may be personally relevant –for example, because there are children inthehome–tohelpheridentifymotivationalfactors on her own.The idea is to link themotivation to quit to the patient’s personalsituation,beingasspecificaspossible.
Risks.Toensurethatthepatientunderstandstherisktoherownhealthandtoherbaby’shealthifshecontinuestosmoke,askhertoidentify potential negative consequences.Onewaytobeginthispartofthediscussionis to ask, “Although you do not want to orare not ready to quit now, what have youheard about smoking during pregnancy?” Ifthepatient seemsunawareof the risks, thisisagoodtimetogiveherpregnancy-specificinformation.Apatientwhohashadahealthychild while smoking may be unconvincedof the need to quit.This is an opportunityto reiterate the benefits of quitting for thispregnancyand for thechildorchildrenshealreadyhas.Also,sheneedstobeawarethateachpregnancyisdifferentandsheisdifferentaswell:older,smokinglonger,mayhaveanewchronicdisease.Theabsenceofcomplicationsin apreviouspregnancydoesnotguaranteefuturepregnanciesfreeoftrouble.
Rewards. Ask the patient to describe howquittingsmokingmightbenefitherandherfamily.Dependingonhersituation,shemayneedsomeexamples,suchas,“Youwillhavemoreenergytotakecareofyourselfandyour
newbaby,”or“You’llsetagoodexampleforyourchildrenandtheirfriends”(seeTable3).The patient’s history and comments abouther smoking behavior can provide valuableinformation to create a checklist of factorsthat will increase her motivation to quit –for example, saving money, taking the babyhomefromthehospitalwithher,protectinga child who has asthma, less time requiredfor smoking-related doctors’ visits, vanity(healthierskin,absenceofodor),andpleasingfamilyandfriends.
Roadblocks.Mostpatientscaneasilyidentifybarrierstoquitting.Reassurethepatientthatassistance is available to help her overcomeroadblocks such as withdrawal symptoms,weightgain,anothersmokerinthehouse,andemotional consequences. Problem-solvingstrategies and tools, including information,can be applied to many situations onceroadblocksareidentified(seeTable6).
Repetition. Follow up at each visit to seeif the patient has changed her mind aboutundertaking a quit attempt. Tell patientswho have tried to quit and relapsed thatmostpeoplemakerepeatedattemptstoquitbeforetheyaresuccessful,thatshecanlearnfrom repeated quit attempts, and each newattempt increases the likelihoodofquitting.For a patient who does not respond to the5R’sintervention,itmaybeusefultoprovideinformation about how to get help if shechangeshermind.
Relevance Patientidentifiesmotivationalfactors.Risks Patientidentifiespotentialnegativeconsequencesofcontinuedsmoking.Rewards Patientdescribeshowquittingwouldbenefitherandherfamily.Roadblocks Patientidentifiesbarrierstoquitting.Repetition Repeatateveryvisitforpatientswhosmoke.
THE 5 R’S
14 15
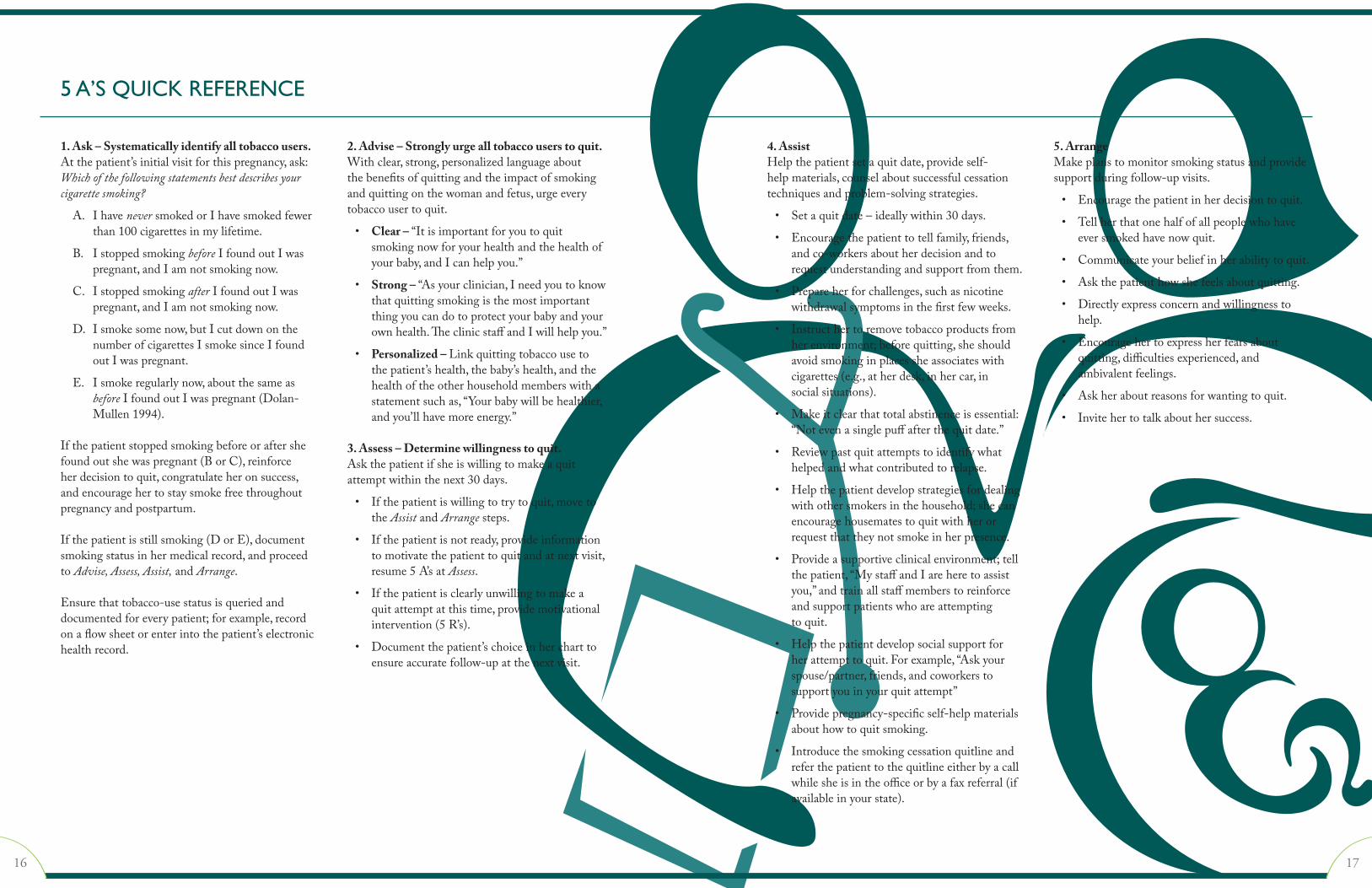
1. Ask – Systematically identify all tobacco users.Atthepatient’sinitialvisitforthispregnancy,ask:Which of the following statements best describes your cigarette smoking?
A. IhaveneversmokedorIhavesmokedfewerthan100cigarettesinmylifetime.
B. IstoppedsmokingbeforeIfoundoutIwaspregnant,andIamnotsmokingnow.
C. IstoppedsmokingafterIfoundoutIwaspregnant,andIamnotsmokingnow.
D. Ismokesomenow,butIcutdownonthenumberofcigarettesIsmokesinceIfoundoutIwaspregnant.
E. Ismokeregularlynow,aboutthesameasbeforeIfoundoutIwaspregnant(Dolan-Mullen1994).
Ifthepatientstoppedsmokingbeforeoraftershefoundoutshewaspregnant(BorC),reinforceherdecisiontoquit,congratulateheronsuccess,andencouragehertostaysmokefreethroughoutpregnancyandpostpartum.
Ifthepatientisstillsmoking(DorE),documentsmokingstatusinhermedicalrecord,andproceedtoAdvise, Assess, Assist,andArrange.
Ensurethattobacco-usestatusisqueriedanddocumentedforeverypatient;forexample,recordonaflowsheetorenterintothepatient’selectronichealthrecord.
2. Advise – Strongly urge all tobacco users to quit.Withclear,strong,personalizedlanguageaboutthebenefitsofquittingandtheimpactofsmokingandquittingonthewomanandfetus,urgeeverytobaccousertoquit.
• Clear – “Itisimportantforyoutoquitsmokingnowforyourhealthandthehealthofyourbaby,andIcanhelpyou.”
• Strong – “Asyourclinician,Ineedyoutoknowthatquittingsmokingisthemostimportantthingyoucandotoprotectyourbabyandyourownhealth.TheclinicstaffandIwillhelpyou.”
• Personalized – Linkquittingtobaccousetothepatient’shealth,thebaby’shealth,andthehealthoftheotherhouseholdmemberswithastatementsuchas,“Yourbabywillbehealthier,andyou’llhavemoreenergy.”
3. Assess – Determine willingness to quit.Askthepatientifsheiswillingtomakeaquitattemptwithinthenext30days.
• Ifthepatientiswillingtotrytoquit,movetotheAssistandArrangesteps.
• Ifthepatientisnotready,provideinformationtomotivatethepatienttoquitandatnextvisit,resume5A’satAssess.
• Ifthepatientisclearlyunwillingtomakeaquitattemptatthistime,providemotivationalintervention(5R’s).
• Documentthepatient’schoiceinhercharttoensureaccuratefollow-upatthenextvisit.
4. AssistHelpthepatientsetaquitdate,provideself-helpmaterials,counselaboutsuccessfulcessationtechniquesandproblem-solvingstrategies.
• Setaquitdate–ideallywithin30days.
• Encouragethepatienttotellfamily,friends,andco-workersaboutherdecisionandtorequestunderstandingandsupportfromthem.
• Prepareherforchallenges,suchasnicotinewithdrawalsymptomsinthefirstfewweeks.
• Instructhertoremovetobaccoproductsfromherenvironment;beforequitting,sheshouldavoidsmokinginplacessheassociateswithcigarettes(e.g.,atherdesk,inhercar,insocialsituations).
• Makeitclearthattotalabstinenceisessential:“Notevenasinglepuffafterthequitdate.”
• Reviewpastquitattemptstoidentifywhathelpedandwhatcontributedtorelapse.
• Helpthepatientdevelopstrategiesfordealingwithothersmokersinthehousehold;shecanencouragehousematestoquitwithherorrequestthattheynotsmokeinherpresence.
• Provideasupportiveclinicalenvironment;tellthepatient,“MystaffandIareheretoassistyou,”andtrainallstaffmemberstoreinforceandsupportpatientswhoareattemptingtoquit.
• Helpthepatientdevelopsocialsupportforherattempttoquit.Forexample,“Askyourspouse/partner,friends,andcoworkerstosupportyouinyourquitattempt”
• Providepregnancy-specificself-helpmaterialsabouthowtoquitsmoking.
• Introducethesmokingcessationquitlineandreferthepatienttothequitlineeitherbyacallwhilesheisintheofficeorbyafaxreferral(ifavailableinyourstate).
5. ArrangeMakeplanstomonitorsmokingstatusandprovidesupportduringfollow-upvisits.
• Encouragethepatientinherdecisiontoquit.
• Tellherthatonehalfofallpeoplewhohaveeversmokedhavenowquit.
• Communicateyourbeliefinherabilitytoquit.
• Askthepatienthowshefeelsaboutquitting.
• Directlyexpressconcernandwillingnesstohelp.
• Encouragehertoexpressherfearsaboutquitting,difficultiesexperienced,andambivalentfeelings.
• Askheraboutreasonsforwantingtoquit.
• Invitehertotalkabouthersuccess.
5 A’S QUICK REFERENCE
16 17

The5A’sapproachisdesignedtoincorporatesmokingcessationmessagesintoroutineclinicalcareofpregnantwomeneffectivelybutquickly.Likeanysustainedprogram,however,itiseasiertoimplementandmoreeffectivewhenmorethanonestaffmemberisinvolved.Thesuccessofasmokingcessationinterventionismorelikelyifthepatientsensesinvolvementandencouragementfromeveryonesheencountersduringaclinicvisit.
Thelevelofstaffinvolvementdependsonthesizeofthepracticeorclinic.Itisimportant,therefore,toclearlyestablishthetasksinvolvedinaninterventionprogramandassignresponsibilities.Thesixstepslistedherearedesignedtoassisttheclinicianandotherstaffmembersinsettingupasmokingcessationprogramintheclinic.
STEP 1. DEVELOP ADMINISTRATIVE COMMITMENTEverypersononthestaffplaysacriticalroleinasmokingcessationinterventionprogram.Tobeeffective,aninterventionprogrammustbefullysupportedbyallstaffmemberswhowillhaveresponsibilityforanyaspectofcareforthepatient,record-keeping,orderingmaterials,orotheraspectsofimplementation.Reviewingbackgroundinformationaboutthehealthconsequencesofsmokingforpregnantpatientsandtheirbabiesandtheimportanceofquittingcanhelpthestaffunderstandhowcriticalitistohelppatientsquitsmoking.Brieflyexplainingthatthe5A’sinterventionhasbeenproveneffectivemayhelpmotivatestafftobecomeinvolved(see5 A’s Quick Reference,page16).
SIX STEPS TO IMPLEMENTATION
STEP 2. INVOLVE STAFF EARLY IN THE PROCESSStaffmembersmayexpressconcernaboutintroducingadditionaltasksintothecareroutineintheoffice.Itishelpfulatthispointtoestimatethenumberofpatientsyourpracticeislikelytoseebasedonthegeographicanddemographiccharacteristicsofyourpatientpopulation.Thisnumberisoftenlowerthananticipated,whichcanhelprelieveconcernsaboutworkload.Alsoevaluatewhatyourpracticeiscurrentlydoingtoidentifyandtreatpregnantsmokers.
Invitingparticipationintheplanningprocesswillpermitstaffmemberstocontributeideasandfeelasenseofownership.Addressingproblemsandanticipatingneedsmayresultinsmootherintroductionofthe5A’sapproach.Also,staffmemberswhoroutinelydealwithpatientsmayprovidevaluableinsightintohowthe5A’sapproachwillbereceivedbypatientsandcanoffersuggestionsaboutimplementation.Duringtheplanningprocess,itishelpfultofollowthesesteps:
• Provideanoverviewofthe5A’sapproach,andthenrevieweachstepseparately.
• Emphasizethatencouragementbystaffmembershasbeenshowntohelppatientsquitsmoking.
• Invitestaffmemberstoaskquestionsandexpressconcerns.
• Identifybarrierstoimplementationateachstepandconsidersolutions.
• Useinputfromthestafftodeveloparealisticimplementationplan,includingpatientoutreach,useofnewmedia,andwaystomeasureandmonitorsuccess.
• Determinethestaffmeetingformatformonitoringprogressoftheimplementationplan.
• Underscorethattheskillsstaffmembersgaininusingthe5A’sapproachwillbeusefulinscreening,treating,anddocumentingotherkindsofriskssuchasalcoholanddrugmisuse.
Stafftrainingisaseparatestep.Duringinitialplanning,anoverviewoftheinterventionisadequate.Attheinitialmeeting,emphasizethattheimplementationofthe5A’sapproachintothecareroutinewillbemonitored,andregularstaffmeetingswillprovideanopportunitytodiscusswhatisworkingwellandwhatneedsimprovement.Ifanystaffmemberssmoke,thismightbetherighttimetoofferthemassistanceinquittingsmokingthemselves.
STEP 3. ASSIGN ONE PERSON TO COORDINATE AND MONITOR IMPLEMENTATIONHavingonepersoncoordinateplanningandimplementationoftheinterventionisrecommendedtoensurethattasksdon’tgetoverlooked.Someonewhoisprimarilyresponsiblefortheprogramcanbeavailabletoanswerstaffquestions,troubleshootproblems,arrangefortrainingusingthismanualorothersourcesofinformation,andmonitorimplementationoftheprogram.Thisindividualcanalsoorderself-helpandotherrelatedmaterials,assurestaffreadyaccesstothematerials,andidentifyreferralsourcesformoreintensivecounselingorcounselingforotherdruguse.Dependingonthenumberofstaffmembersinanofficeandtheirresponsibilities,thecoordinatormayormaynotberesponsibleforeveryaspectoftheintervention.Specificassignmentscanbemadeonceallstaffmembersaretrained.
STEP 4. PROVIDE TRAININGStaffshouldbetrainedaboutthe5A’s,the5R’s,andtheimportanceofsupportingthepatient’sefforttoquit.Informationsuchasthisresourceguidecanhelpstaffmembersunderstandthe5A’sapproachandanticipatepatientneeds.AdditionaltrainingresourcesforprovidersareavailablethroughtheorganizationslistedinResources for Clinicians and Patients(Appendix,pages26-27).Additionaltrainingisnotrequiredtoimplementasuccessfulinterventionprogram,however.
18 19
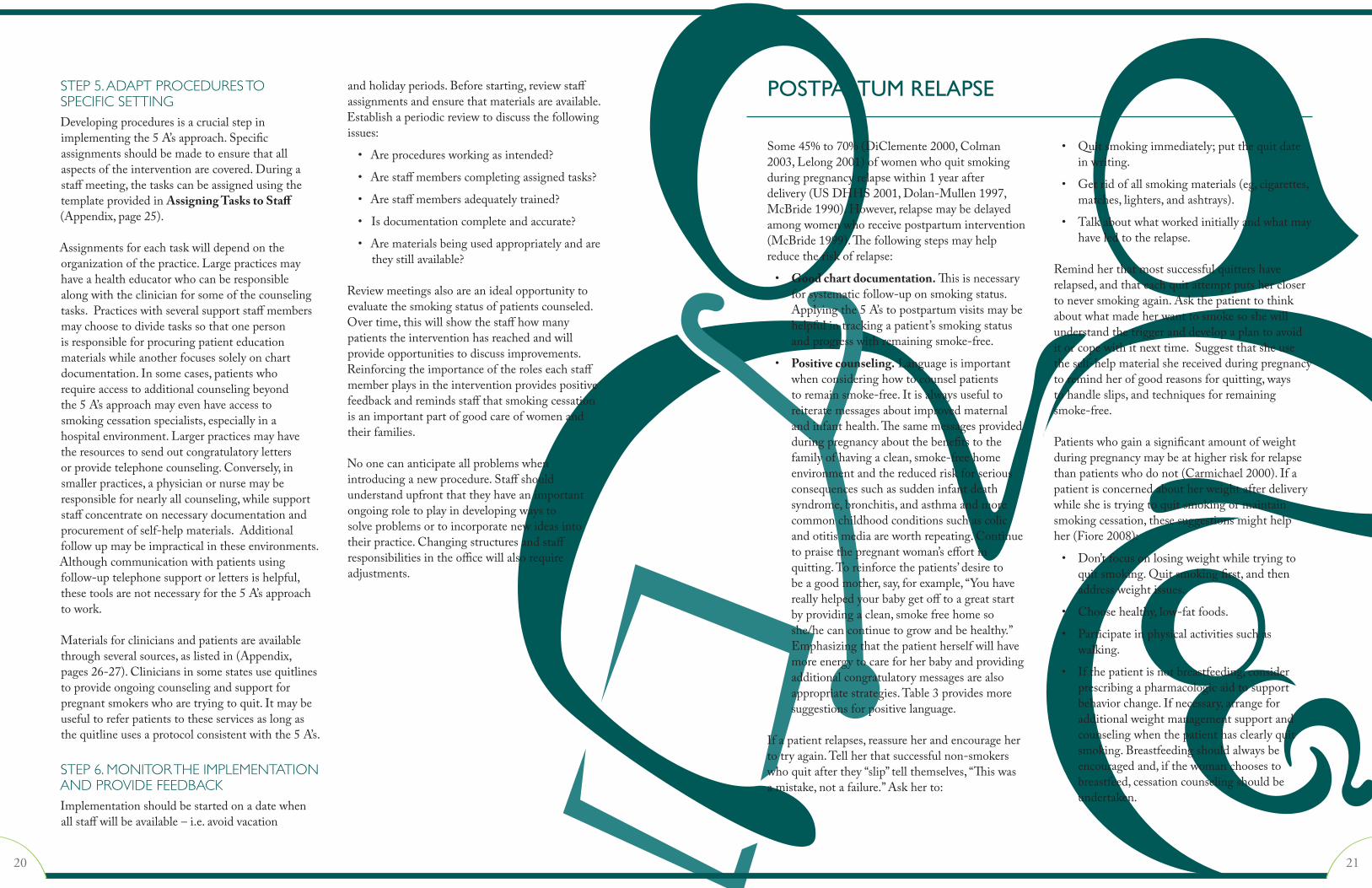
STEP 5. ADAPT PROCEDURES TO SPECIFIC SETTINGDevelopingproceduresisacrucialstepinimplementingthe5A’sapproach.Specificassignmentsshouldbemadetoensurethatallaspectsoftheinterventionarecovered.Duringastaffmeeting,thetaskscanbeassignedusingthetemplateprovidedinAssigning Tasks to Staff(Appendix,page25).
Assignmentsforeachtaskwilldependontheorganizationofthepractice.Largepracticesmayhaveahealtheducatorwhocanberesponsiblealongwiththeclinicianforsomeofthecounselingtasks.Practiceswithseveralsupportstaffmembersmaychoosetodividetaskssothatonepersonisresponsibleforprocuringpatienteducationmaterialswhileanotherfocusessolelyonchartdocumentation.Insomecases,patientswhorequireaccesstoadditionalcounselingbeyondthe5A’sapproachmayevenhaveaccesstosmokingcessationspecialists,especiallyinahospitalenvironment.Largerpracticesmayhavetheresourcestosendoutcongratulatorylettersorprovidetelephonecounseling.Conversely,insmallerpractices,aphysicianornursemayberesponsiblefornearlyallcounseling,whilesupportstaffconcentrateonnecessarydocumentationandprocurementofself-helpmaterials.Additionalfollowupmaybeimpracticalintheseenvironments.Althoughcommunicationwithpatientsusingfollow-uptelephonesupportorlettersishelpful,thesetoolsarenotnecessaryforthe5A’sapproachtowork.
Materialsforcliniciansandpatientsareavailablethroughseveralsources,aslistedin(Appendix,pages26-27).Cliniciansinsomestatesusequitlinestoprovideongoingcounselingandsupportforpregnantsmokerswhoaretryingtoquit.Itmaybeusefultoreferpatientstotheseservicesaslongasthequitlineusesaprotocolconsistentwiththe5A’s.
STEP 6. MONITOR THE IMPLEMENTATION AND PROVIDE FEEDBACKImplementationshouldbestartedonadatewhenallstaffwillbeavailable–i.e.avoidvacation
andholidayperiods.Beforestarting,reviewstaffassignmentsandensurethatmaterialsareavailable.Establishaperiodicreviewtodiscussthefollowingissues:
• Areproceduresworkingasintended?
• Arestaffmemberscompletingassignedtasks?
• Arestaffmembersadequatelytrained?
• Isdocumentationcompleteandaccurate?
• Arematerialsbeingusedappropriatelyandaretheystillavailable?
Reviewmeetingsalsoareanidealopportunitytoevaluatethesmokingstatusofpatientscounseled.Overtime,thiswillshowthestaffhowmanypatientstheinterventionhasreachedandwillprovideopportunitiestodiscussimprovements.Reinforcingtheimportanceoftheroleseachstaffmemberplaysintheinterventionprovidespositivefeedbackandremindsstaffthatsmokingcessationisanimportantpartofgoodcareofwomenandtheirfamilies.
Noonecananticipateallproblemswhenintroducinganewprocedure.Staffshouldunderstandupfrontthattheyhaveanimportantongoingroletoplayindevelopingwaystosolveproblemsortoincorporatenewideasintotheirpractice.Changingstructuresandstaffresponsibilitiesintheofficewillalsorequireadjustments.
Some45%to70%(DiClemente2000,Colman2003,Lelong2001)ofwomenwhoquitsmokingduringpregnancyrelapsewithin1yearafterdelivery(USDHHS2001,Dolan-Mullen1997,McBride1990).However,relapsemaybedelayedamongwomenwhoreceivepostpartumintervention(McBride1999).Thefollowingstepsmayhelpreducetheriskofrelapse:
• Good chart documentation.Thisisnecessaryforsystematicfollow-uponsmokingstatus.Applyingthe5A’stopostpartumvisitsmaybehelpfulintrackingapatient’ssmokingstatusandprogresswithremainingsmoke-free.
• Positive counseling.Languageisimportantwhenconsideringhowtocounselpatientstoremainsmoke-free.Itisalwaysusefultoreiteratemessagesaboutimprovedmaternalandinfanthealth.Thesamemessagesprovidedduringpregnancyaboutthebenefitstothefamilyofhavingaclean,smoke-freehomeenvironmentandthereducedriskforseriousconsequencessuchassuddeninfantdeathsyndrome,bronchitis,andasthmaandmorecommonchildhoodconditionssuchascolicandotitismediaareworthrepeating.Continuetopraisethepregnantwoman’seffortinquitting.Toreinforcethepatients’desiretobeagoodmother,say,forexample,“Youhavereallyhelpedyourbabygetofftoagreatstartbyprovidingaclean,smokefreehomesoshe/hecancontinuetogrowandbehealthy.”Emphasizingthatthepatientherselfwillhavemoreenergytocareforherbabyandprovidingadditionalcongratulatorymessagesarealsoappropriatestrategies.Table3providesmoresuggestionsforpositivelanguage.
Ifapatientrelapses,reassureherandencouragehertotryagain.Tellherthatsuccessfulnon-smokerswhoquitafterthey“slip”tellthemselves,“Thiswasamistake,notafailure.”Askherto:
• Quitsmokingimmediately;putthequitdateinwriting.
• Getridofallsmokingmaterials(eg,cigarettes,matches,lighters,andashtrays).
• Talkaboutwhatworkedinitiallyandwhatmayhaveledtotherelapse.
Remindherthatmostsuccessfulquittershaverelapsed,andthateachquitattemptputsherclosertoneversmokingagain.Askthepatienttothinkaboutwhatmadeherwanttosmokesoshewillunderstandthetriggeranddevelopaplantoavoiditorcopewithitnexttime.Suggestthatsheusetheself-helpmaterialshereceivedduringpregnancytoremindherofgoodreasonsforquitting,waystohandleslips,andtechniquesforremainingsmoke-free.
Patientswhogainasignificantamountofweightduringpregnancymaybeathigherriskforrelapsethanpatientswhodonot(Carmichael2000).Ifapatientisconcernedaboutherweightafterdeliverywhilesheistryingtoquitsmokingormaintainsmokingcessation,thesesuggestionsmighthelpher(Fiore2008):
• Don’tfocusonlosingweightwhiletryingtoquitsmoking.Quitsmokingfirst,andthenaddressweightissues.
• Choosehealthy,low-fatfoods.
• Participateinphysicalactivitiessuchaswalking.
• Ifthepatientisnotbreastfeeding,considerprescribingapharmacologicaidtosupportbehaviorchange.Ifnecessary,arrangeforadditionalweightmanagementsupportandcounselingwhenthepatienthasclearlyquitsmoking.Breastfeedingshouldalwaysbeencouragedand,ifthewomanchoosestobreastfeed,cessationcounselingshouldbeundertaken.
POSTPARTUM RELAPSE
20 21
ACOG(AmericanCollegeofObstetriciansandGynecologists).Motivational interviewing: a tool for behavior change. ACOGCommitteeOpinionNo.423.ObstetGynecol2009;113:243-6.
ACOG(AmericanCollegeofObstetriciansandGynecologists).Smoking cessation during pregnancy. ACOGCommitteeOpinion#471.ObstetGynecol2010;166:1241-4.
Adams,E.,F.Ayadi,etal.Smoking among Medicaid insured mothers: What are the neonatal costs. HealthCareFinancingReview2004;26:105-118.
AyadiMF,AdamsEK,MelvinCL,etal.Costs of a smoking cessation counseling intervention for pregnant women: comparison of three settings. PublicHealthRep2006;121:120-6.
BoydNR,WindsorRA,PerkinsLL,LoweJB.Quality of measurement of smoking status by self-report and saliva cotinine among pregnant women. MaternChildHealthJ1998;2:77-83.
CarmichaelSL,AhluwaliaIB.Correlates of postpartum smoking relapse. Results from the Pregnancy Risk Assessment Monitoring System (PRAMS). AmJPrevMed2000;19:193-6.
Colman,G.J.andT.Joyce.Trends in smoking before, during, and after pregnancy in ten states. AmJPrevMed.2003;24:29-35.
DiClemente,C,Dolan-MullenP,etal..The process of pregnancy smoking cessation: implications for interventions. TobControl2000;9Suppl3:III16-21.
DiFranzaJR,LewRA.Morbidity and mortality in children associated with use of tobacco products by other people. Pediatrics1996;97:560-8.
Dolan-MullenPD,CarbonariJP,TabakER,GlendayMC.Improving disclosure of smoking by pregnant women. AmJObstetGynecol1991;165:409-13.
Dolan-MullenP,RamirezG,GroffJY.A meta-analysis of randomized trials of prenatal smoking cessation interventions. AmJObstetGynecol1994;171;1328-34.
Dolan-MullenPD,RichardsonMA,QuinnVP,ErshoffDH.Postpartum return to smoking: Who is at risk and when. AmJHealthPromot1997;11:323-30.
Dolan-MullenPD.Maternal smoking during pregnancy and evidence-based intervention to promote cessation. PrimCare1999;26:577-589.
DrewsCD,MurphyCC,Yeargin-AllsoppM,DecoufleP.The Relationship between idiopathic mental retardation and maternal smoking during pregnancy. Pediatrics1996;97:547-53.
EnglandLJ,KendrickJS,WilsonHG,MerrittRK,GargiulloPM,ZahniserSC.Effects of smoking reduction during pregnancy on the birth weight of term infants. AmJEpidemiol2001;154:694-701.
FioreMC,JorenbyDE,SchenskyAE,SmithSS,BauerRR,BakerTB.Smoking status as the new vital sign: Effect on assessment and intervention in patients who smoke. MayoClinProc1995;70:209-13.
REFERENCES
FioreMC,JaenCR,BakerTB,etal.Treating Tobacco Use and Dependence: 2008 Update. Clinical Practice Guideline. Rockville, MD: U.S.DepartmentofHealthandHumanServices.PublicHealthService.May2008.
GlynnTJ,ManleyMW.How to help your patients stop smoking: A National Cancer Institute manual for physicians. Washington,DC;SmokingandTobaccoControlProgram,DivisionofCancerPrevention,NationalCancerInstitute,USDepartmentofHealthandHumanServices,November1990,NIHpublication90-3064.
GoldenbergRL,Dolan-MullenP.Convincing pregnant patients to stop smoking. ContempObGyn2000;11:34-44.
GrimleyDM,BellisJM,RaczynskiJM,HenningK.Smoking cessation counseling practices: A survey of Alabama obstetrician-gynecologists. SouthMedJ2001;94:297-303.
HartmannKE.Clear and concise interventions for smoking cessation. HospPhysician2000;36:19-27.
JaenCR,StangeKC,TumielLM,NuttingP.Missed opportunities for prevention: Smoking cessation counseling and the competing demands of practice. JFamPract1997;45:348-54.
JorenbyDE,FioreMC.The Agency for Health Care Policy and Research smoking cessation clinical practice guideline: basics and beyond. PrimCare1999Sep;26:513-28.
KreuterMW,ChhedaSG,BullFC.How does physician advice influence patient behavior? Evidence for a priming effect. ArchFamMed2000;9:426-33.
Lightwood,JM,Phibbs,CS,etal.Short-term health and economic benefits of smoking cessation: low birth weight. Pediatrics1999;104:1312-20.
Lelong,N,KaminskiM,etal.Postpartum return to smoking among usual smokers who quit during pregnancy. EurJPublicHealth2001;11(3):334-9.
LumleyJ,OliverS,WatersE.Interventions for promoting smoking cessation during pregnancy. CochraneDatabaseSystRev2000;CD001055.
MakinJ,FriedPA,WatkinsonB.A comparison of active and passive smoking during pregnancy: Long-term effects. NeurotoxicolTeratol1991;13:5-12.
McBrideCM,CurrySJ,LandoHA,PiriePL,GrothausLC,NelsonJC.Prevention of relapse in women who quit smoking during pregnancy. AmJPublicHealth1999;89:706-11.
McBrideCM,PiriePL.Postpartum smoking relapse. AddictBehav1990;15:165-8.
MelvinCL,Dolan-MullenP,WindsorRA,WhitesideHPJr,GoldenbergRL.Recommended cessation counseling for pregnant women who smoke: A review of the evidence. TobControl2000;9(supplIII):iii80-iii84.
MelvinCL,RayburnWF.Substance Use. In: Nolan TE, editor. Precis: An update in obstetrics and gynecology, primary and prevention care. Washington,DC:AmericanCollegeofObstetriciansandGynecologists;4thed.2009.:81-6.
ProchazkaAV.New developments in smoking cessation. Chest2000;117(4Suppl1):169S-175S.
ResearchTriangleInstitute.Report Series Reveals Findings from Youth Tobacco Survey. July 23, 2001. Availableat:http://www.rti.org/news.cfm?nav=386&objectid=A7585181-E83E-49D5-B864FF4E36D713B7.AccessedAugust31,2010.
SippelJM,OsbornML.BjornsonW,GoldbergB,BuistAS.Smoking cessation in primary care clinics. JGenInternMed1999;14:670-6.
SteadLF,PereraR,LancasterT.Telephone counselling for smoking cessation. CochraneDatabaseofSystematicReviews2006,Issue3.Art.No.:CD002850.DOI:10.1002/14651858.CD002850.pub2.
ThorndikeAN,RigottiNA,StaffordRS,SingerDE.National patterns in the treatment of smokers by physicians. JAMA1998;279:604-8.
USDepartmentofHealthandHumanServices.Women and Smoking: A Report of the Surgeon General. 2001. Availableat:http://www.cdc.gov/tobacco/data_statistics/sgr/2001/index.htm.AccessedAugust31,2010.
USDepartmentofHealthandHumanServices.The Health Benefits of Smoking Cessation: A report of the Surgeon General. 2004. Availableat:http://www.cdc.gov/tobacco/data_statistics/sgr/2004/posters/20mins/index.htm.AccessedSeptember3,2010.
WakschlagLS,LaheyBB,LoeberR,GreenSM,GordonRA,LeventhalBL.Maternal smoking during pregnancy and the risk of conduct disorder in boys. ArchGenPsychiatry1997;54:670-6.
WindsorRA,CutterG,MorrisJ,etal.The effectiveness of smoking cessation methods for smokers in public health maternity clinics: A randomized trial. AmJPublicHealth1985;75:1389-92.
Continuingthe5A’sapproachafterawomangivesbirthhelpshercontinuehereffortstoquitsmokingormaintainsmokingcessation.Italsoreinforcesyourconcernabouthersmokingstatusandyourinterest,asherclinician,inhelpinghertoquitsmoking.Forpatientswhorelapse,revisitthe5A’sandcontinuetostatethepositiveeffectsofquitting(seeTable3).Reassurethepatientwhohasrelapsedofyourcontinuedassistanceinherattemptstoquit.
Forpostpartumsmokers,severalpharmacologicsmokingcessationaidsareavailable,includingnicotinereplacementproductssuchasgum,patches,
lozenge,nasalsprayandinhalers.Bupropion(anantidepressant)andvareniclinearealsoprescribedassmokingcessationaidsbecausetheyhavebeenshowntohelppatientscopewithnicotinewithdrawalsymptoms.However,theFDAhasplacedblack-boxwarningsonallantidepressantsandvareniclineastheiruseincreasestheriskofsuicide,particularlyinadolescentsandyoungadults.Usersmustbefollowedcloselyforsuicidalideation.Postpartumsmokerswhoarebreastfeedingshouldcheckwiththeirpediatricianpriortoinitiatingpharmacologicsmokingcessationaids.
22 23

HOW TO INTERVENE
5 A’s Step Action
Askaboutsmoking
• Useamultiple-responseformatasshowninFirst A: Ask(page7).
• Don’task,“Doyousmoke?”or“Youdon’tsmoke,doyou?”
• Indicatesmokingstatusclearlyinthepatient’schartsothatitcanbereadilynotedatfollow-up.
Advisetoquit
• Emphasizethatsmokingisoneofthemostimportantchangesthepatientcanmake.
• Emphasizethebenefitsofquitting(Table3).
• Usepositivelanguage;admonishmentmaybeintimidatingordiscouraging.
Assesswillingnesstoquit• Askpatientifsheiswillingtomakeaquitattemptinthenext30days.
• ConsiderformalizingtheagreementusingaQuit Contract(page11).
Ifpatientiswillingtoquit,Assistherwiththeprocess
• Brieflycounselthepatientandprovidesupportforherattempttoquit.
• Suggestwaystoovercomebarriers(Table6).
• Helpthepatientidentifysomeoneinherenvironmentwhocanprovideencouragement.
• Providepregnancy-specificself-helpmaterials(seeResources for Clinicians and Patients,pages26-27)
Ifthepatientisnotwillingtoquit,explorewhy
• Usethe5R’s(seeWhen the Patient Doesn’t Want to Try to Quit: The 5 R’s,page14).
• Ifthepatienttriedtoquitbeforeandrelapsed,explorewhatdidnotwork.
• Reassurethepatientthatitgenerallytakesseveralattemptstoquitsuccessfully.
• Donotadmonishthepatient;beopenandapproachable.
Arrangefollow-up• Assesssmokingstatusatsubsequentvisits.
• Ifpatientcontinuestosmoke,encouragecessationandrepeatassistance.
STAFF TASK ASSIGNMENTS
Task Who Will Do It Where
Ask
1.Askpatientaboutsmoking.
2.Labelpatientsmokingstatusinsidechart.
Advise
1.Advisethepatienttoquit.
Assess
1.Assesswillingnessofpatienttotrytoquitwithinaspecifiedtimeframe.
2.Assesspreviousquitattempts.
3.Assessbarrierstoquitting(5R’s).
Assist
1.Helpthepatientsetaquitdate.
2.Provideself-helpmaterials.
3.Provideproblem-solvinginformation.
4.Provideadditionalmaterialssuchasquit-smokingcontract,patientdiaries.
Arrange follow up
1.Documentsothatsmokingstatusischeckedatthenextvisit.
2.Followupbytelephone(optional).
3.Sendcongratulatoryletters(optional).
4.Askaboutsmokingstatusatnextvisit.
Administrative support
1.Orderandkeepmaterialsstocked.
2.Compilefollow-upresults.
3.Monitorstaffcompliancewithprotocol.
APPENDIX: HOW TO INTERVENE APPENDIX: ASSIGN TASKS TO STAFF
24 25

FROM ACOG:Motivational Interviewing: A Tool For Behavioral ChangeACOGCommitteeOpinion#423
Smoking Cessation During PregnancyACOGCommitteeOpinion#471(2010)
• Singlecopiesavailablewithoutcharge;pleaseincludename,affiliation,andmailingaddresswithrequesttowww.acog.org.
• Toorderapackageof25,calltheACOGDistributionCenterat800-762-ACOG,ext882ororderonlineatsales.acog.com.
OTHER RESOURCES: Thefollowingarelistedforinformationpurposesonly.ListingofthesesourcesandwebsitesdoesnotimplytheendorsementofACOG.Thislistisnotmeanttobecomprehensive.Theinclusionorexclusionofasourceorwebsitedoesnotreflectthequalityofthatsourceorwebsite.Pleasenotethatwebsitesaresubjecttochangewithoutnotice.
Treating Tobacco Use And DependenceClinicalPracticeGuidelinesfromtheAgencyforHealthcareResearchandQuality(AHRQ).Topreviewgotowww.ahrq.gov;underthe“ClinicalInformation”headingclickon“ClinicalPracticeGuidelines”linkandlookunderTobaccoCessation.Toorderprintcopies,telephone800-358-9295.
FREE CME Smoking Cessation During Pregnancy ProgramAnonlineprogramforprovidertrainingonsmokingcessationduringpregnancyisconsistentwiththeUSPHS2008Guidelines:TreatingTobaccoUseandDependence.Itisinteractive,canbeusedinsegmentsandprovidesfreeCMEs/CEUsforphysicians,nurses,dentistsanddentalhygienists:musom.marshall.edu/medctr/med/tobaccocessation/pregnancyandsmoking/login.aspx
Smoke-Free FamiliesTheNationalPartnership(2002-2008)wasacollaborationofmorethan30organizationsfundedbyTheRobertWoodJohnsonFoundation.Archivedproductsincludingclinicalpracticeresources,technicalassistancetools,andpatientmaterialsareavailableontheNationalTobaccoCessationCoalition’swebsite(www.tobacco-cessation.org/sf/index.htm).
Need Help Putting Out That Cigarette?A28-pagepatientself-helpguide.Toordermultiplecopies,call800-762-ACOG,ext.882.CanalsobedownloadedfromNationalPartnershipforSmokefreeFamilieswebsite(www.tobacco-cessation.org/sf/patient.htm).Click“selectEnglishorSpanishforbooklet,”andclick“Printed/web-basedmaterialsthatwillhelpyouinyourquitattempt.”
www.smokefree.govWebsitecontainsanonlinestep-by-stepcessationguide,telephonequitlines,instantmessagingservice,andpublicationsthatcanbedownloaded,printedorordered.CreatedbytheTobaccoControlResearchBranchoftheNationalCancerInstitute.
1-800-QUIT NOWToll-freetelephonenumberconnectsyoutocounselingandinformationaboutquittingsmokinginyourstate.
Note:Contactyourstatepublichealthdepartmentdivisionofsmokingcessationtolearnwhetheryourstateoffersatoll-freetelephonesupportprogramandotherservicestohelpsmokersquit.
APPENDIX: RESOURCES FOR CLINICIANS APPENDIX: RESOURCES FOR PATIENT/CONSUMERS
EveryrecommendationmadebytheClinicalPracticeGuidelinePanelbearsastrength-of-evidenceratingthatindicatesthequalityandquantityofempiricalsupportfortherecommendation.Theratingsandtheirdescriptionsarelistedbelow(Fiore2008).
Rating Description
A Multiplewell-designedrandomizedclinicaltrials,directlyrelevanttotherecommendation,yieldedaconsistentpatternoffindings.
B
Someevidencefromrandomizedclinicaltrialssupportedtherecommendation,butthescientificsupportwasnotoptimal.Forinstance,fewrandomizedtrialsexisted,thetrialsthatdidexistweresomewhatinconsistent,orthetrialswerenotdirectlyrelevanttotherecommendation.
C ReservedforimportantclinicalsituationsinwhichthePanelachievedconsensusontherecommendationintheabsenceofrelevantrandomizedcontrolledtrials.
APPENDIX: STRENGTH OF EVIDENCE
26 27
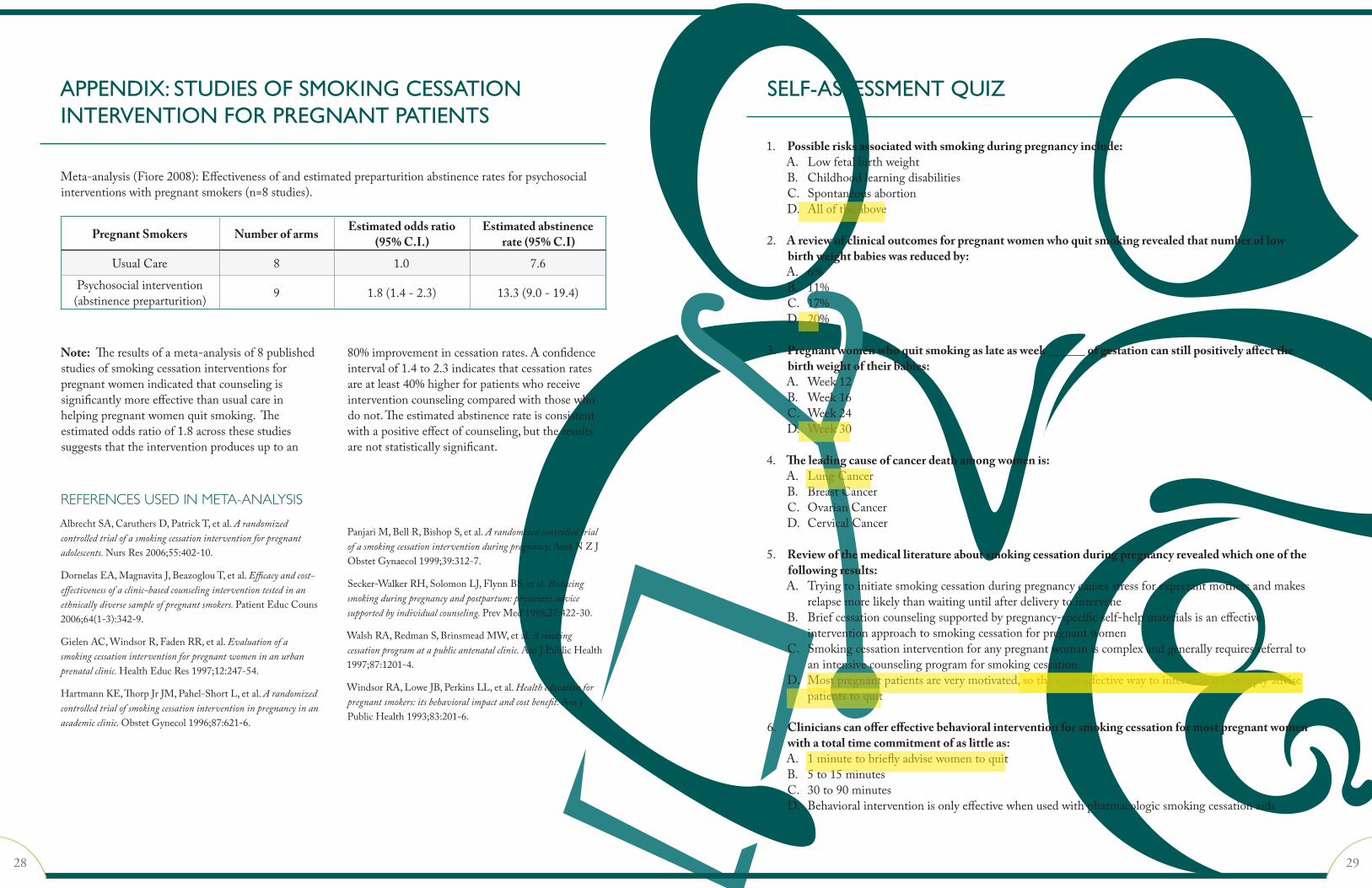
Meta-analysis(Fiore2008):Effectivenessofandestimatedpreparturitionabstinenceratesforpsychosocialinterventionswithpregnantsmokers(n=8studies).
Pregnant Smokers Number of arms Estimated odds ratio (95% C.I.)
Estimated abstinence rate (95% C.I)
UsualCare 8 1.0 7.6
Psychosocialintervention(abstinencepreparturition) 9 1.8(1.4-2.3) 13.3(9.0-19.4)
Note:Theresultsofameta-analysisof8publishedstudiesofsmokingcessationinterventionsforpregnantwomenindicatedthatcounselingissignificantlymoreeffectivethanusualcareinhelpingpregnantwomenquitsmoking.Theestimatedoddsratioof1.8acrossthesestudiessuggeststhattheinterventionproducesuptoan
80%improvementincessationrates.Aconfidenceintervalof1.4to2.3indicatesthatcessationratesareatleast40%higherforpatientswhoreceiveinterventioncounselingcomparedwiththosewhodonot.Theestimatedabstinencerateisconsistentwithapositiveeffectofcounseling,buttheresultsarenotstatisticallysignificant.
REFERENCES USED IN META-ANALYSIS
AlbrechtSA,CaruthersD,PatrickT,etal.A randomized controlled trial of a smoking cessation intervention for pregnant adolescents. NursRes2006;55:402-10.
DornelasEA,MagnavitaJ,BeazoglouT,etal.Efficacy and cost-effectiveness of a clinic-based counseling intervention tested in an ethnically diverse sample of pregnant smokers. PatientEducCouns2006;64(1-3):342-9.
GielenAC,WindsorR,FadenRR,etal.Evaluation of a smoking cessation intervention for pregnant women in an urban prenatal clinic. HealthEducRes1997;12:247-54.
HartmannKE,ThorpJrJM,Pahel-ShortL,etal.A randomized controlled trial of smoking cessation intervention in pregnancy in an academic clinic. ObstetGynecol1996;87:621-6.
PanjariM,BellR,BishopS,etal.A randomized controlled trial of a smoking cessation intervention during pregnancy. AustNZJObstetGynaecol1999;39:312-7.
Secker-WalkerRH,SolomonLJ,FlynnBS,etal.Reducing smoking during pregnancy and postpartum: physician’s advice supported by individual counseling. PrevMed1998;27:422-30.
WalshRA,RedmanS,BrinsmeadMW,etal.A smoking cessation program at a public antenatal clinic. AmJPublicHealth1997;87:1201-4.
WindsorRA,LoweJB,PerkinsLL,etal.Health education for pregnant smokers: its behavioral impact and cost benefit. AmJPublicHealth1993;83:201-6.
APPENDIX: STUDIES OF SMOKING CESSATION INTERVENTION FOR PREGNANT PATIENTS
1. Possible risks associated with smoking during pregnancy include:A. LowfetalbirthweightB. ChildhoodlearningdisabilitiesC. SpontaneousabortionD. Alloftheabove
2. A review of clinical outcomes for pregnant women who quit smoking revealed that number of low birth weight babies was reduced by: A. 6%B. 11%C. 17%D. 20%
3. Pregnant women who quit smoking as late as week ______ of gestation can still positively affect the birth weight of their babies: A. Week12B. Week16C. Week24D. Week30
4. The leading cause of cancer death among women is: A. LungCancerB. BreastCancerC. OvarianCancerD. CervicalCancer
5. Review of the medical literature about smoking cessation during pregnancy revealed which one of the following results: A. Tryingtoinitiatesmokingcessationduringpregnancycausesstressforexpectantmothersandmakes relapsemorelikelythanwaitinguntilafterdeliverytointerveneB. Briefcessationcounselingsupportedbypregnancy-specificself-helpmaterialsisaneffective interventionapproachtosmokingcessationforpregnantwomenC. Smokingcessationinterventionforanypregnantwomaniscomplexandgenerallyrequiresreferralto anintensivecounselingprogramforsmokingcessationD. Mostpregnantpatientsareverymotivated,sothemosteffectivewaytointerveneistosimplyadvise patientstoquit
6. Clinicians can offer effective behavioral intervention for smoking cessation for most pregnant women with a total time commitment of as little as: A. 1minutetobrieflyadvisewomentoquitB. 5to15minutesC. 30to90minutesD. Behavioralinterventionisonlyeffectivewhenusedwithpharmacologicsmokingcessationaids
SELF-ASSESSMENT QUIZ
28 29
user
Highlight
user
Highlight
user
Highlight
user
Highlight
user
Highlight
user
Highlight
user
Highlight
user
Highlight

7. Some women do not disclose that they smoke when asked because of the societal stigma associated with smoking. What strategy can clinicians use to improve disclosure rates when asking about smoking status during an initial patient interview? A. Mostpatientsconcealtheirsmoking,sothereisnoreliablewaytoobtaininformationaboutsmoking statuswithoutusingphysiologicmarkerssuchasurinetestsorexpiredcarbonmonoxideB. Describingindetailthepoorclinicaloutcomesforchildrenofmotherswhosmokecanmotivatea smokertoaskforhelpC. Veryfewwomenconcealtheirsmokingstatusfromphysicians,sosimplyaskingthepatient,“Doyou smoke?”isthemoststraightforwardstrategyD. Usingamultiple-choiceformatwithrelativeresponses,suchas“IstoppedsmokingafterIfoundoutI waspregnant”improvesdisclosurerates
8. Tracking smoking status as a vital sign, in the same way blood pressure is monitored, for example, is important because: A. SmokingisoneofthefewriskfactorsthatcanbemodifiedduringpregnancyB. Recordingtheinformationasavitalsigninthecharthelpstracksmokingstatusforfollow-up atfuturevisitsC. AskingpatientsaboutsmokingstatusateachvisitincreasesthelikelihoodofasuccessfulinterventionD. Alloftheabove
9. Which statement about pharmacologic intervention for pregnant smokers is not true? A. ThenicotinereplacementpatchexposesthefetustoasteadydoseofnicotineB. Studiesto-datehavenotdemonstratedthesafetyorefficacyofpharmacotherapyduringpregnancyC. ThereisnocircumstanceinwhichapharmacologicaidisappropriateforapregnantsmokerD. BupropionandVareniclinehavebeenlabeledwithblackboxwarningsforincreasedsuiciderisk
10. Using the 5 R’s to expose reasons a pregnant patient may choose not to try to quit smoking should be repeated how often? A. AteveryvisitaslongasthepatientisstillsmokingB. AfterdeliverywhenpharmacotherapycanbeofferedC. Onlyonce;repeatingtheprocesstoooftencouldcausethepatienttobecomeirritatedD. Onceattheinitialassessmentandoncemorebeforethe30thweekofpregnancy
11. Which statement about office staff involvement in the 5 A’s smoking cessation approach is accurate? A. Onlythephysiciantreatingthepatientshouldbeinvolvedininterventionbecausethepatientmay beembarrassedabouthersmokingB. Staffmembersinvolvedinimplementingasmokingcessationprogramintheofficemustattend extensive,ongoingtrainingfromabehavioralmodificationspecialisttoensurethattheintervention programwillbeeffectiveC. Anofficeinterventionprogramisreallyonlyfeasibleinalargesettingwithpatienteducation providersonstaffD. The5A’sinterventioncanbeadaptedaccordingtotheofficesizeandtheavailabilityofstaff
12. What percentage of women who quit smoking during pregnancy relapse within 1 year after delivery? A. 10%to35% C.45%to70%B. 25%to50% D.60%to85%
13. If a patient relapses, what should the clinician do? A. InstructthepatienttoquitimmediatelyandputthequitdateinwritingB. TellthepatientthatmostsuccessfulquittershaverelapsedC. InstructthepatienttogetridofallsmokingmaterialsD. Alloftheabove
14. Which is the recommended approach for women who are concerned about weight gain if they quit smoking? A. Quitsmokingfirst,andthenaddressweightissuesB. Makeacompletelifestylechangeatonetimeusingthe5A’stoquitsmokingandinitiatingadiet forweightcontrolC. Addressweightissuesfirstasamotivatingstrategy,andthenaddresssmokingcessationD. Gainingweightduringpregnancyisnormal,sotellthepatientnottobeconcernedaboutit
15. Which statement about the cost of smoking cessation intervention is true? A. Thecost-effectivenessofsmokingcessationcannotbemeasuredaccuratelyB. Initiatingsmokingcessationinterventionhasbeenshowntobeverycostly,butitisanecessary partofimprovinghealthoutcomesC. Tobaccodependenceinterventionsarecosteffectivebecausetheyreducethenumberof lowbirth-weightbabies,perinataldeaths,anduseofnewbornintensivecareunitsD. Ingeneral,thehigherthecostofasmokingcessationinterventionmethod,thegreateritssuccess
16. When advising a patient to quit, which is the recommended attitude to use as presented in the 5 A’s approach? A. Gentlyremindthepatientthatsocietywillviewherasa“badmother”ifshedoesn’tquitB. Offerthepatienteducationalpamphletsabouttheeffectsofsmokingandwaittoseeifshe asksaboutquittingC. Inastricttone,provideacompletelistofthehealthriskstowhichsheisexposingherchild soshewillknowyouareseriousaboutherquittingD. Usepositivelanguageandfocusonthebenefitsofquittingforherbabyandherself
17. Which strategy about assisting patients to quit is recommended in the 5 A’s approach? A. Alwaysmakesurethefatherofthechildisinvolvedinthepatient’squit-smokingefforts; heismostlikelytoprovidethebestsupportforthepatientB. Encouragethepatienttokeepherattemptstoquitsmokingtoherselfsootherswon’tpressureherC. HelpthepatientidentifysomeonewhocanprovideencouragementandsupportD. Theclinicianandofficestaffaretheonlypeoplewhoshouldbeinvolved
18. What is the best response to the patient who asks if she can just cut down on her smoking? A. “Ifyoucanreduceyoursmokingto5cigarettesperday,thatisadequatetoreducerisk.”B. “Yourgoalshouldbetotryandquitcompletely.”C. “Ifcuttingbackisthebestyoucando,thatisadequateduringpregnancy.Icanprescribe pharmacologicaidstohelpyouquitcompletelyafterdelivery.”D. “Anyreductionyoumakeinsmokingisgoodforyouandyourbaby.”
30 31
user
Highlight
user
Highlight
user
Highlight
user
Highlight
user
Highlight
user
Highlight
user
Highlight
user
Highlight
user
Highlight
user
Highlight
user
Highlight
user
Highlight
user
Highlight
user
Highlight
user
Highlight

19. The first option on the multiple-choice response format to determine smoking status states: I have never smoked, or I have never smoked more than 100 cigarettes in my lifetime. What should clinicians consider when dealing with adolescents? A. Adolescentscanbeaddictedquicklyandbeestablishedsmokersbythetimetheyhavesmoked 100cigarettesB. Adolescentsdonotbecomeaddictedaseasilyasadults,soevensmoking200cigarettesdoesnot establishthepatientasasmokerC. VirtuallyalladolescentswhosmokewillconcealitandrespondthattheyhaveneversmokedD. Itisbestnottousethisformatwhentreatingadolescentsandusephysiologictestinginstead todeterminesmokingstatus
20. What strategy should the clinician follow to assist a patient after she has decided to quit smoking? A. Discussconcernsthepatienthasaboutquittingsmokingandhelpherdevelop problem-solvingstrategiesB. Ifthepatienthastriedtoquitsmokingbeforeandrelapsed,reviewwhathelpedandwhat contributedtorelapseC. Tellthepatientthathergoalmustbetoquitcompletely:“Notevenapuff ”D. Alloftheabove
Foreachquestion,pleasecircletheletterthatcorrespondswiththecorrectanswer.Ascoreof70%correctisrequiredtoobtainamaximumof3 AMA PRA Category 1 Credits™.
CMEactivitiesmustbefreeofcommercialbiasfororagainstanyproduct.Inthisregardhowwouldyouratethisactivity? ExcellentGoodFairPoor
HowwouldyouratetheoverallqualityofthisCMEactivity?ExcellentGoodFairPoorDoyouplantomakeanychangesinyourpracticeasaresultofthisCMEactivity?YesNoIfyes,pleasespecify:
Pleasetypeorprintlegiblyinthespacesbelow.Thisinformationwillbeusedtoprocessandmailyourcertificate.
Pleaseratefromexcellent(4)topoor(1)howwellthisactivitypreparedyoutomeeteachofthefollowingobjectives.
4 3 2 1Employevidence-basedguidelinesforsmokingcessationduringpregnancy
EffectivelyfollowuponpatientswhoarereluctanttoquitsmokingRecognizewhentousepharmacologicintervention
EstablishasmokingcessationprograminthepracticesettingCounselpatientsaboutpostpartumrelapse
AddresspatientconcernsaboutquittingHelppatientsovercomebarrierstosuccess
Providepatient-orientedinformationsourcesonsmokingcessation
1. abcd
2. abcd
3. abcd
4. abcd
5. abcd
6. abcd
7. abcd
8. abcd
9. abcd
10. abcd
11. abcd
12. abcd
13. abcd
14. abcd
15. abcd
16. abcd
17. abcd
18. abcd
19. abcd
20. abcd
ToreceiveCMEcredit,pleasemailcompletedanswersheetto:ACOG,Women’sHealthIssues,P.O.Box96920,Washington,DC20090-6920OrFAXto:Women’sHealthIssues@202-484-3917
Expiration Date: September 1, 2013
A CLINICIAN’S GUIDE TO HELPING PREGNANT WOMEN QUIT SMOKING ANSWER SHEET AND EVALUATION FORM
E-mail Address
Phone
City
Street Address
Full Name
Specialty
Fax
State
Degree
ZIP
32 33
user
Highlight
user
Highlight
user
Highlight
user
Highlight
user
Highlight
user
Highlight
user
Highlight
user
Highlight
user
Highlight
user
Highlight
user
Highlight
user
Highlight
user
Highlight
user
Highlight
user
Highlight
user
Highlight
user
Highlight
user
Highlight
user
Highlight
user
Highlight
user
Highlight
user
Highlight
user
Highlight
user
Highlight
user
Highlight

Support for this publication provided in part by these institutions:


















