Taking a Deep Breath, Smoking Cessation and Diagnosed Mental

Smoking Cessation for Persons with Mental Illness

O V E R V I E W | 1
Why is a smoking cessation toolkit for persons with mental illnesses needed?
They need to quit.Consumersneedtobealiveto“recover”frommentalillnesses.Smokingcessationisakeycomponentofconsumer-driven,individualizedtreatmentplanning.
They want to quit.Peoplewithmentalillnesseswanttoquitsmokingandwantinformationaboutcessationservicesandresources.(Morrisetal,2006)
They can quit.Peoplewithmentalillnessescansuccessfullyquitusingtobacco.(Evinsetal.,2005;Georgeetal.,2002).Significantevidenceshowsthatsmokingcessationstrategieswork.
Note: Throughoutthistoolkittheterms“tobaccouse”and“smoking”areusedinterchangeably.Althoughwedonotspecificallyaddressspit-tobaccouse,thetoolkitisgenerallyapplicabletospit-tobaccousers.
“I’d love to quit – I just don’t know how.”– John, age 45

O V E R V I E W | 2
Alarming StatisticsApproximately 7.7 percent of Colorado’s adult population has a major mental illness.1
Forty-onepercentoftheseindividualsusetobacco.Theprevalenceofsmokingamongpeoplewithmentalillnessesisstartling.
By diagnosis:Majordepression 45-50percentBipolarmooddisorder 50-70percentSchizophrenia 70-90percent
Americanswithmentalillnessesrepresentanestimated44.3percentofthetobaccomarket.2
Americanswithmentalillnessesarenicotinedependentatratesthataretwotothreetimeshigherthanthegeneralpopulation.3
Becausepeoplewithmentalillnessesusetobaccoatgreaterrates,theysuffergreatersmoking-relatedmedicalillnessesandmortality.4
About this toolkitWho is this toolkit for?Thistoolkitwasdevelopedforabroadcontinuumofmentalhealthproviders.Materialsareintendedfordirectproviders,aswellasadministratorsandbehavioralhealthorganizations.
How do I use this toolkit?Thetoolkitcontainsavarietyofinformationandstep-by-stepinstructionabout:•Lowburdenmeansofassessingreadiness toquit•Possibletreatments•ReferraltoColoradocommunityresources
1] Morris et al., 20062] Grant et al., 2004, Lasser et al., 20003] Grant et al., 2004, Lasser et al., 20004] Grant et al., 2004

Quick FactsMental Illnesses and Tobacco Use
• 7.1%oftheU.S.populationhasapsychiatricillness;however,thispopulation consumesover34.2%ofallcigarettes.(Grantetal.,2004)
• IntheU.S.,personswithmentalillnessesrepresentanestimated44.3%ofthetobacco marketandarenicotinedependentatratesthatare2-3timeshigherthanthegeneral population.(Grantetal.,2004;Lasser,2000)
• InColorado,approximately7.7%oftheadultpopulationhasamajormentalillnessand 41%oftheseindividualsusetobacco.(Gieseetal.,2003)
• Smokingcessationisakeycomponentofconsumer-driven,individualizedtreatment planning.(Morrisetal.,2006)
• Personswithmentalillnesseswanttoquitsmokingandwantinformationoncessation servicesandresources.(Morrisetal.,2006)
• Personswithmentalillnessescansuccessfullyquitusingtobacco.(Evinsetal.,2005; Georgeetal.,2002)
• SmokingquitratesforindividualswithpsychiatricillnessareNOTsignificantlylower thanthegeneralpopulation.(el-Guebalyetal.,2002)
• Becausepersonswithmentalillnessesusetobaccoatgreaterrates,theysuffergreater smoking-relatedmedicalillnessesandmortality.(Grantetal.,2004)
References:
El-GuebalyN,CathcartJ,CurrieSetal(2002).Smokingcessationapproachesforpersonswithmentalillnessoraddictivedisorders.Psychiatric Services,53(9):1166-1170.
EvinsAE,MaysVk,RigottiNA,etal.(2001).Apilottrialofbupropionaddedtocognitivebehavioraltherapyforsmokingcessationinschizophrenia.Nicotine Tobacco Research,3(4):397-403.
GeorgeTP,VessicchioJC,TermineAetal.(2002b).Aplacebo-controlledstudyofbupropionforsmokingcessationinschizophrenia.Biological Psychiatry,52(1):53-61.
GieseA,MorrisC,OlincyA(2003).Needsassessmentofpersonswithmentalillnessesfortobaccoprevention,exposure,reduction,andcessation.ReportpreparedfortheStateTobaccoEducationandPreventionPartnership(STEPP),ColoradoDepartmentofPublicHealthandEnvironment.
GrantBF,HasinDS,ChouPS,StinsonFS,DawsonDA(2004).NicotinedependenceandpsychiatricdisordersintheUnitedStates:resultsfromthenationalepidemiologicsurveyonalcoholandrelatedconditions.Archives General Psychiatry,61(11):1107-1115.
LasserK,BoydW,WoolhandlerS,etal(2000).Smokingandmentalillness:apopulationbasedprevalencestudy.Journal of the American Medical Association,284:2606–2610.
MorrisCD,GieseJJ,DickinsonM,Johnson-NagelN.(2006).PredictorsofTobaccoUseAmongPersonsWithMentalIllnessesinaStatewidePopulation.Psychiatric Services,57:1035-1038.
TobaccoDisparitiesInitiativesoftheStateTobaccoEducationandPreventionPartnership(STEPP),ColoradoDepartmentofPublicHealthandEnvironmentwww.cdphe.state.co.us/pp/tobacco/tobaccohome.asp

Smoking and mental illnesses: nicotine effects and other considerationsPeoplewithmentalillnesses:•usetobaccoathigherrates• arelesslikelytosucceedatcessationattempts•accessgeneralmedicalservicesandother communityresourcesrelativelyinfrequently• strugglewithstigmaonseverallevels•generallyexperienceagreaterburdenofmorbidity andmortalitythantheoverallpopulation.
Why do they smoke more?Researchersbelievethatacombinationofbiological,psychologicalandsocialfactorscontributetoincreasedtobaccouseamongpersonswithmentalillnesses.
Biological predispositionPersonswithmentalillnesseshaveuniqueneurobiologicalfeaturesthatmayincreasetheirtendencytousenicotine,makeitmoredifficulttoquitandcomplicatewithdrawalsymptoms.
Nicotineaffectstheactionsofneurotransmitters(e.g.dopamine).Forexample,peoplewithschizophreniawhousetobaccomayexperiencelessnegativesymptoms(lackofmotivation,driveandenergy).
Nicotineenhancesconcentration,informationprocessingandlearning.(Thisisespeciallyimportantforpersonswithpsychoticdisordersforwhomcognitivedysfunctionmaybeapartoftheirillnessorasideeffectofantipsychoticmedications).
Otherbiologicalfactorsincludenicotine’spositiveeffectsonmood,feelingsofpleasureandenjoyment.
Someevidencesuggeststhatsmokingisassociatedwithareducedriskofantipsychotic-inducedParkinsonism.
T O B A C C O U S E a n d M E N T A L I L L N E S S | 3
Tobacco use and mental illness

T O B A C C O U S E a n d M E N T A L I L L N E S S | 4
Psychological considerations•Tobaccousemaytemporarilyrelievefeelings oftensionandanxietyandisoftenusedtocope withstress.•Peopledevelopadailyroutineofsmoking.
Social considerations•Peoplemaysmoketofeel“partofagroup.”•Smokingisoftenassociatedwithsocialactivities.•Personswithmentalillnessesmaynothavealot ofactivitiestokeepthembusy.Whenthey’re bored,theymaysmokemore.•Thesiteofasocialactivitymaysupport tobaccouse.
Stigma•Providersoftenthinkthatpeoplewithmental illnessesareunabletoquitsmoking.•Symptommanagementoftentakesprecedence overpreventivehealthmeasures.
Specific mental disordersWhataresomeconsiderationsforsmokingcessationinregardtospecificmentaldisorders?
DepressionAmongpatientsseekingsmokingcessationtreatment,25-40percenthaveahistoryofmajordepressionandmanyhaveminordysthymicsymptoms.
Depressionhasbeenshowntopredictpoorersmokingcessationrates.Considerstartingorrestartingpsychotherapyorpharmacotherapyfordepressioninpatientswhostatethatdepressionintensifiedwithcessationorthatcessationcauseddepression.
Cognitivebehavioraltherapyfordepressionandantidepressantshasbeenfoundtoimprovesmokingcessationratesinthosewithahistoryofdepressionorsymptomsofdepression.
Forasmokerwithahistoryofdepressioncurrentlytakingantidepressantmedication,itisimportanttonotethatsomeantidepressantlevelswillincreasewithsmokingcessation.
Stress is a big trigger for me. I don’t know how to deal with stress.
– Cathi, age 32
What I did to keep from craving cigarettes for a while is just to keep busy, being with people, and talking and playing games and working and things like that. That’s what helped me.
– Robert, age 43

SchizophreniaPersonswithschizophreniawhosmokemaybelessinterestedintobaccocessation,makingstrategiestoenhancemotivationtoquitespeciallyimportant.
Whenmentalhealthconsumerswithschizophreniadotrytostop,manyareunsuccessful;thus,intensivetreatmentsareappropriateevenwithearlyattempts.
Thehighprevalenceofalcoholandillicitdrugabuseinconsumerswithschizophreniacaninterferewithsmokingcessation.
Thebloodlevelsofsomeantipsychoticscanincreasedramaticallywithcessation.Nicotinewithdrawalcanmimictheakathisia,depression,difficultyconcentratingandinsomniaseeninconsumerswithschizophrenia.
Other psychiatric disordersThereisinsufficientinformationtomakespecificrecommendationsabouttailoringtreatmentofsmokingcessationtotheneedsofsmokerswithotherpsychiatricdisorders.
Ingeneral,whenmentalhealthconsumersmakeanattemptatsmokingcessation,theyshouldbefollowedcloselytomonitorformoreseverenicotinewithdrawal,exacerbationoftheirpsychiatricdisorderandpossiblesideeffectsduetocessation-inducedincreasesinmedicationlevels.
Methylphenidate(Ritalin)andd-amphetamine(Dexedrine),stimulantscommonlyprescribedforbehavioralproblemsassociatedwithattentiondeficithyperactivitydisorder(ADHD)increaseratesofsmokingandthereinforcingeffectsofsmoking.Methylphenidateandd-amphetamineuseinearlylifeleadstoincreasedoddsofdailysmokinglaterinlife.
Tobacco industry targetingBy1977,smokerswerebecominga“downscalemarket.”RJReynoldsnotedthatlesseducated,lowerincome,minoritypopulationsweremoreimpressionable/susceptibletomarketingandadvertising.Tobaccocompaniesbegantargetingthesepopulations.Free cigarettes were distributed to homeless shelters, mental hospitals and homeless service organizations.Cigaretteswerepurchasedforthementallyillandhomelesssothatconsumerswouldsmoke“clean”cigarettes,notdirtycigarettesbutts.
Thetobaccoindustryhastargetedpsychiatrichospitalsforsalespromotionsandgiveaways.Theyhavemadefinancialcontributionstohomelessveteranorganizations,usingrelationshipstoadvancetheirpoliticalagenda.
T O B A C C O U S E a n d M E N T A L I L L N E S S | 5
I’ve been schizophrenic since I was 14. I was told more less when I went to the hospitals that cigarettes help control certain areas in my brain and the way we function out in society. I more or less became more of a smoker because I was told it would help me with my illness. I was taught more about it helping my illness than I was about cancer and stuff like that. – Marc, age 24

Readiness to quit and stages of changeTheStagesofChangeModel(alsoknownastheTranstheoreticalModel)illustratedbelowisusefulinrecognizingthatnicotinedependenceisachronic,relapsingdisorderwithmosttobaccousersinthegeneralpopulationrequiringfivetosevenattemptsbeforetheyfinallyquitforgood.Manypatientsdonotrealizethatitusuallytakesseveralattemptstostopusingtobaccoandwillneedmotivationtoattempttoquitiftheyhavebeenunsuccessfulinthepast.Itisusefultothinkoftobaccocessationasaprocessratherthananevent.
Onceapersonhasbeenidentifiedasatobaccouser,hisorherreadinesstoquitcanbedetermined.Thisisimportantbecausetobaccouserswhoarenotconsideringquittingappeartoneeddifferentinterventionsthanthosewhoareambivalentaboutquittingorthosepresentlyinterestedinquitting.TobaccousersinthePrecontemplationstage(notconsideringquitting)canbemovedtotheContemplationstagebyaskingconsumerstoconsiderthenegativeconsequencesoftobaccouseforthemandtheadvantagesoftobaccocessation(thisinformationhastobepersonalized).Itisworthwhiletoactivelyencouragequittingandoffersupportandtreatmentaswellasconveyingthemessagethatpersonswithmentalillnessescansuccessfullyquitusingtobacco.
Stages of change•Precontemplation:Nochangeisintendedinthe foreseeablefuture.Theindividualisnotconsidering quitting.•Contemplation:Theindividualisnotpreparedtoquitat present,butintendstodosointhenextsixmonths.•Preparation:Theindividualisactivelyconsidering quittingintheimmediatefutureorwithinthenext month.•Action:Theindividualismakingovertattemptstoquit. However,quittinghasnotbeenineffectforlongerthan sixmonths.•Maintenance:Theindividualhasquitforlongerthan sixmonths.
A S S E S S M E N T a n d I N T E R V E N T I O N P L A N N I N G | 7
Assessment and intervention planning

A S S E S S M E N T a n d I N T E R V E N T I O N P L A N N I N G | 8
The 5 A’s: Ask, Advise, Assess, Assist and ArrangeTheU.S. Public Health Service Clinical Practice Guideline: Treating Tobacco Use and Dependenceprovideshealthcarecliniciansastrategyforsmokingcessationtreatmentthatisbuiltaroundthe“5A’s”(Ask,Advise,Assess,AssistandArrange).Knowingthatprovidershavemanycompetingdemands,the5A’swerecreatedtokeepstepssimple.
Onthefollowingpagesyouwillfindasummaryoftheseeasilyimplementedsteps.
TheGuidelinerecommendsthatallpeopleenteringahealthcaresettingshouldbeaskedabouttheirtobaccousestatusandthatthisstatusshouldbedocumented.Providersshouldadvisealltobaccouserstoquitandthenassesstheirwillingnesstomakeaquitattempt.Personswhoarereadytomakeaquitattemptshouldbeassistedintheeffort.Followupshouldthenbearrangedtodeterminethesuccessofquitattempts.
Thefull5A’smodelismostappropriateforagenciesandorganizationsthathavetobaccocessationmedicationsand/orbehavioralservicesavailableforconsumers.Foragenciesandorganizationsthatdonothavetobaccocessationservicesreadilyavailable,werecommendtheuseofthefirsttwoA’s(askandadvise)andthenrefertoavailablecommunityservices.Thefull5A’smodel,aswellastheabbreviatedask-advise-refermodelarepresentedintheflowchartandtablesatthebackofthisbook.
A S K
AD
VI S
E
AS
SESSASSIS
T
AR
RA
NG
E
Tobacco dependenceand use (current or former)
is a chronic relapsingcondition that requires
repeated interventions and a systematic approach.
If you have limited time:ASK ADVISE REFER
Strategies for Implementation
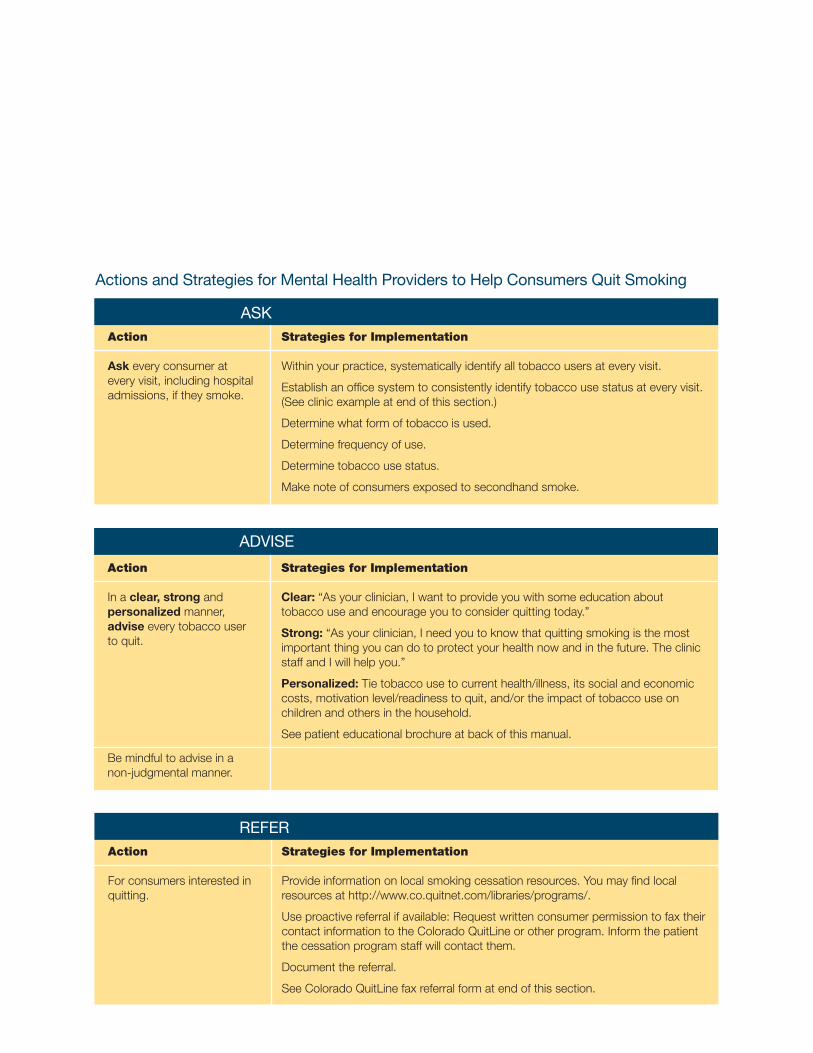
Clear:“Asyourclinician,Iwanttoprovideyouwithsomeeducationabouttobaccouseandencourageyoutoconsiderquittingtoday.”
Strong:“Asyourclinician,Ineedyoutoknowthatquittingsmokingisthemostimportantthingyoucandotoprotectyourhealthnowandinthefuture.TheclinicstaffandIwillhelpyou.”
Personalized:Tietobaccousetocurrenthealth/illness,itssocialandeconomiccosts,motivationlevel/readinesstoquit,and/ortheimpactoftobaccouseonchildrenandothersinthehousehold.
Seepatienteducationalbrochureatbackofthismanual.
Action
Inaclear, strong andpersonalizedmanner, adviseeverytobaccousertoquit.
Bemindfultoadviseinanon-judgmentalmanner.
Action
Forconsumersinterestedinquitting.
Strategies for Implementation
Provideinformationonlocalsmokingcessationresources.Youmayfindlocalresourcesathttp://www.co.quitnet.com/libraries/programs/.
Useproactivereferralifavailable:RequestwrittenconsumerpermissiontofaxtheircontactinformationtotheColoradoQuitLineorotherprogram.Informthepatientthecessationprogramstaffwillcontactthem.
Documentthereferral.
SeeColoradoQuitLinefaxreferralformatendofthissection.
Action
Askeveryconsumerateveryvisit,includinghospitaladmissions,iftheysmoke.
Strategies for Implementation
Withinyourpractice,systematicallyidentifyalltobaccousersateveryvisit.
Establishanofficesystemtoconsistentlyidentifytobaccousestatusateveryvisit.(Seeclinicexampleatendofthissection.)
Determinewhatformoftobaccoisused.
Determinefrequencyofuse.
Determinetobaccousestatus.
Makenoteofconsumersexposedtosecondhandsmoke.
Actions and Strategies for Mental Health Providers to Help Consumers Quit Smoking
A S S E S S M E N T a n d I N T E R V E N T I O N P L A N N I N G | 9
ASK
REFER
ADVISE

Action
Assesswillingnesstomakeaquitattemptwithinthenext30days.
Determinewiththepatientthecostsandbenefitsofsmokingforhimorher.
Determinewherethepatientisintermsofthereadinesstochangemodel.
Assesspastquitattemptsandpast/currentpsychiatricsymptomsforconsumerswantingtoquit.
Strategies for Implementation
Assessreadinessforchange.Gotop.7tolearnhowtoassessreadinessforchange.
Iftheconsumerisreadytoquit,proceedtoAssist(below)and/orarrangeformoreintensiveservicestohelpwiththequittingprocess.
Iftheconsumerwillparticipateinanintensivetreatment,deliversuchatreatmentorrefertoanintensiveintervention(Arrange).
Iftheconsumerisn’treadytoquit,don’tgiveup.Providerscangiveeffectivemotivationalinterventionsthatkeepconsumersthinkingaboutquitting.Conductamotivationalinterventionthathelpsconsumersidentifyquittingaspersonallyrelevantandrepeatmotivationalinterventionsateveryvisit.
Foraddressingtobaccocessationwithtobaccousersunwillingtoquit,pleaseproceedtothe5R’sonpage12.
Fortheconsumerwhoiswillingtoquit:
Obtainasmokinghistoryandassessexperiencewithpreviousquitattempts:• Reasonsforquitting.• Anychangeinpsychiatricfunctioningwhenheorshetriedtostop?• Causeofrelapse(wasthisduetowithdrawalsymptomsorincreased psychiatricsymptoms?)• Howlongdidheorsheremainabstinent?• Priortreatmentintermsoftype,adequacy(dose,duration),complianceand consumer’sperceptionofeffectiveness.• Expectationsaboutfutureattemptsandtreatments.
Determinewhetherthereareanypsychiatricreasonsforconcernaboutwhetherthisisthebesttimeforcessation:• Istheconsumerabouttoundergoanewtherapy?• Istheconsumerpresentlyincrisis,oristhereaproblemthatissopressingthat timeisbetterspentonthisproblemthanoncessationatthisvisit?
• Whatisthelikelihoodthatcessationwouldworsenthenon-nicotinepsychiatric disorder?Andcanthatpossibilitybediminishedwithfrequentmonitoring,useof nicotinereplacementtherapyorothertherapies?
• Whatistheconsumer’sabilitytomobilizecopingskillstodealwithcessation? Ifthecopingskillsarelow,wouldtheconsumerbenefitfromindividualorgroup behaviortherapy?
• Istheconsumerhighlynicotinedependentordoestheconsumerhaveahistory ofrelapseduetowithdrawalsymptomsorincreasedpsychiatricsymptoms?Ifso, whichmedicationmightbeofhelp?
Increasingreadiness/motivation:Ifaconsumerwithpsychiatricillnessisnotreadytomakeaquitattempt,enhancemotivationanddealwithanticipatedbarrierstocessation.• Useproblemsolvingstrategies.• Increasemonitoringoftobaccouse.• Employbehavioraltherapyand/ornicotinereplacementtherapy.• Addressfearsofwithdrawalsymptomsorofworseningpsychiatricproblems.
A S S E S S M E N T a n d I N T E R V E N T I O N P L A N N I N G | 1 0
ASSESS

Action
Helptheconsumerwithaquitplan.
Recommenduseofapprovednicotinereplacementtherapy(NRT)and/orcounseling
Strategies for Implementation
Set a quit date,ideallywithintwoweeks.
Tellfamily,friendsandcoworkersaboutquittingandrequestunderstandingandsupport.
Anticipatetriggersorchallengestoplannedquitattempt,particularlyduringthecriticalfirstfewweeks.Theseincludenicotinewithdrawalsymptoms.Discusshowtheconsumerwillsuccessfullyovercomethesetriggersorchallenges.
Removetobaccoproductsfromtheenvironment.Priortoquitting,consumershouldavoidsmokinginplaceswheretheyspendalotoftime(e.g.work,home,car).
Forconsumerswithcognitivedifficulties(e.g.memoryorattentiondeficits)duetomentalillness,havethemwritedowntheirquitplan,sotheycanrefertoitlater.
RecommendtheuseofNRTmedicationstoincreasecessationsuccess.Discussoptionsforaddressingbehavioralchanges(e.g.cessationclasses,individualcounseling,telephonecoachingfromtheColoradoQuitLine)Encouragepatientswhoarereadytoquitthattheirdecisionisapositivestep.
A S S E S S M E N T a n d I N T E R V E N T I O N P L A N N I N G | 1 1
ASSIST
Action
Schedulefollow-upcontact.
Strategies for Implementation
Timing.Followupcontactshouldoccursoonafterthequitdate,preferablywithinthefirstweek.Asecondfollow-upcontactisrecommendedwithinthefirstmonth.Schedulefurtherfollow-upcontactsasneeded.
Actionsduringfollow-upcontact:
Congratulate success!
Iftheconsumerhasrelapsed,reviewthecircumstancesandelicitrecommitmenttototalabstinence.• Remindpatientthatalapsecanbeusedasalearningexperience.• Identifyproblemsalreadyencounteredandanticipatechallengesinthe immediatefuture.• AssessNRTuseandproblems.• Consideruseorreferraltomoreintensivetreatment.• Give positive feedback about the patient’s attempts to quit. Individuals often cut down substantially on their tobacco use before quitting, and this harm reduction needs to be recognized and congratulated.
ARRANGE

A S S E S S M E N T a n d I N T E R V E N T I O N P L A N N I N G | 1 2
The 5 R’s: Addressing Tobacco Cessation for the Tobacco User Unwilling to Quit(From Treating Tobacco Use and Dependence. Quick Reference Guide for Clinicians, October 2000. U.S. Public Health Service. www.surgeongeneral.gov/tobacco/tobaqrg.htm)
The“5R’s”Relevance,Risks,Rewards,RoadblocksandRepetition,aredesignedtomotivatesmokerswhoareunwillingtoquitatthistime.
Smokersmaybeunwillingtoquitduetomisinformation,concernabouttheeffectsofquittingordemoralizationbecauseofpreviousunsuccessfulquitattempts.Therefore,afteraskingabouttobaccouse,advisingthesmokertoquitandassessingthewillingnessofthesmokertoquit,itisimportanttoprovidethe“5R’s”motivationalintervention.
RelevanceEncouragetheconsumertoindicatewhyquittingispersonallyrelevant,asspecificallyaspossible.Motivationalinformationhasthegreatestimpactifitisrelevanttoaconsumer’smedicalstatusorrisk,familyorsocialsituation(e.g.,havingchildreninthehome),healthconcerns,age,genderandotherimportantpatientcharacteristics(e.g.,priorquittingexperience,personalbarrierstocessation).
RisksAsktheconsumertoidentifypotentialnegativeconsequencesoftobaccouse.Suggestandhighlightthosethatseemmostrelevanttothem.Emphasizethatsmokinglow-tar/low-nicotinecigarettesoruseofotherformsoftobacco(e.g.,smokelesstobacco,cigarsandpipes)willnoteliminatetheserisks.
Examplesofrisksare:
•Acuterisks:Shortnessofbreath,exacerbationof asthma,harmtopregnancy,impotence,infertility andincreasedserumcarbonmonoxide.
•Longtermrisks:Heartattacksandstrokes,lung andothercancers(larynx,oralcavity,pharynx, esophagus,pancreas,bladder,cervix),chronic obstructivepulmonarydiseases(chronicbronchitis andemphysema),longtermdisabilityandneed forextendedcare.
•Environmentalrisks:Increasedriskoflungcancer andheartdiseaseinspouses;higherratesof smokinginchildrenoftobaccousers;increased riskforlowbirthweight,SuddenInfantDeath Syndrome,asthma,middleeardiseaseand respiratoryinfectionsinchildrenofsmokers.
Every time I need a pack of cigarettes, that’s taking money out of my pocket. You can see everybody around here, people that aren’t smoking, look how much money they have. People that are smoking are pretty much broke. If I could quit smoking, I’d have more money to spend.
– James, age 37

A S S E S S M E N T a n d I N T E R V E N T I O N P L A N N I N G | 1 3
RewardsAsktheconsumertoidentifypotentialbenefitsofstoppingtobaccouse.Suggestandhighlightthosethatseemmostrelevanttotheconsumer.
Examplesofrewardsfollow:• Improvedhealth•Foodtastesbetter• Improvedsenseofsmell•Moneysaved•Betterselfimage•Home,car,clothing,breathsmellbetter•Nomoreworryingaboutquitting•Setagoodexampleforchildren•Havehealthierbabiesandchildren•Nomoreworryingaboutexposingothers tosmoke•Feelbetterphysically•Performbetterinphysicalactivities•Reducewrinkling/agingofskin
RoadblocksAsktheconsumertoidentifyimpedimentstoquittingandnoteelementsoftreatment(problemsolving,medications)thatcouldaddressbarriers.
Typicalbarriersmightinclude:•Withdrawalsymptoms•Fearoffailure•Weightgain•Lackofsupport•Depression•Enjoymentoftobacco
RepetitionRepeatmotivationalinterventionseverytimeanunmotivatedconsumervisitstheclinicsetting.Tobaccouserswhohavefailedinpreviousquitattemptsshouldbetoldthatmostpeoplemakerepeatedquitattemptsbeforetheyaresuccessful.
Cultural ConsiderationsCulturalissuesshouldalsobeconsideredforthoseindividualsofdiverseracialandethnicbackgroundsastobaccocessationassessmentandservicesareoffered.
RecommendationsKeyfindingsfromtheSurgeonGeneral’sreport:(1998SurgeonGeneral’sReport,TobaccoUseAmongU.S.Racial/EthnicMinorityGroups)
Inthefourracial/ethnicgroupsstudied(AfricanAmerican,AmericanIndian/AlaskaNative,AsianAmerican/PacificIslanderandHispanic),AfricanAmericanmenbearoneofthegreatesthealthburdens,withdeathratesfromlungcancerthatare50percenthigherthanthoseofCaucasianmen.
Ratesoftobaccorelatedcancers(otherthanlungcancer)varywidelyamongmembersofracial/ethnicgroups.TheyareparticularlyhighamongAfricanAmericanmen.
Tobaccouseamongadolescentsfromracialandethnicminoritygroupshasbeguntoincreaserapidly,threateningtoreversetheprogressmadeagainstlungcanceramongadultsintheseminoritygroups.CigarettesmokingamongAfricanAmericanteenshasincreased80percentoverthelastsixyears–threetimesasfastasamongwhiteteens.
Thehighleveloftobaccoproductadvertisinginracial/ethnicpublicationsisproblematicbecausetheeditorsandpublishersofthesepublicationsmaylimittheleveloftobaccousepreventionandhealthpromotioninformationincludedintheirpublications.
Well, the first thing is you have to decide is that you’re really committed to doing it and then you try over and over and over until you finally get there, and eventually you get there. But it takes a lot of time and it’s not easy.
– Sandy, age 37

A S S E S S M E N T a n d I N T E R V E N T I O N P L A N N I N G | 1 4
Recommendations for Mental Health CliniciansWhenworkingwithpersonswithmentalillnesseswhoarealsoofdiverseracial/ethnicbackgrounds,thementalhealthclinicianshould:
•Ask,Advise,Assistand/orReferallpatientswithregardtotobaccocessation.Thereisacriticalneedto delivereffectivetobaccodependenceeducationandinterventionstoethnicandracialminoritieswith mentalillnesses.
•Usecessationinterventionsthathavebeeneffectiveforpersonswithmentalillnesses(e.g.NRTorbuproprion incombinationwithindividualorgroupcounselingthatemploysmotivationalinterviewingorcognitive- behavioralstrategies).Avarietyofsmokingcessationinterventions(includingscreening,clinicianadvice, self-helpmaterialsandthenicotinepatch)havebeenproveneffectivefortobaccocessationinminority populations.
•Beculturallyappropriate,reflectingthetargetedracial/ethnicgroups’culturalvalues.Thismayincreasethe smoker’sacceptanceoftreatment.
•Conveycessationcounselingorself-helpmaterialsinalanguageunderstoodbythesmoker.
ResourcesFormoreinformationabouttobaccouseandinterventionforracial/ethnicpopulationsinColorado,pleaseseethefollowingonlineresources:
ColoradoTobaccoDisparitiesStrategicPlanningWorkingGroup:http://ctdsp.amc.org/
ColoradoStateStateTobaccoEducationandPrevention(STEPP):http://steppcolorado.com
ColoradoMinorityHealthForumforInformationonReducingHealthDisparitiesinColorado:http://www.coloradominorityhealthforum.org/

Example for Clinic Screening for Tobacco Use
From the U.S. Department of Health & Human Serviceshttp://www.surgeongeneral.gov/tobacco/tobaqrg.pdf
ACTION STRATEGIESforIMPLEMENTATION
Implementanoffice-widesystem Expandvitalsignstoincludetobacco thatensuresthat,foreverypatientat useoruseanalternativeuniversal everyclinicvisit,tobacco-usestatus identificationsystem. isqueriedanddocumented.
VITALSIGNS
BloodPressure:
Pulse: Weight:
Temperature: RespiratoryRate:
TobaccoUse(circleone):CurrentFormerNever
• Repeatedassessmentisnotnecessaryinthecaseoftheadultwhohasneverused tobaccoorhasnotusedtobaccoformanyyears,andforwhomthisinformationis clearlydocumentedinthemedicalrecord.
• Alternativestoexpandingthevitalsignsaretoplacetobacco-usestatusstickerson allpatientchartsortoindicatetobacco-usestatususingelectronicmedicalrecords orcomputerremindersystems.

Key findingsSmokingcessationmodelsforpersonswithmentalillnessesgenerallycombinenicotinereplacementtherapy(NRT)withCognitiveBehavioralTherapy(CBT),atypeofpsychotherapythatfocusesonchangingdysfunctionalthoughts,emotionsandbehavior.
CBTprogramsthatproducethemostsuccessfulquitratesforthementalhealthpopulationgenerallyhavegroupsofapproximately8-10individualsthatmeetonceaweekfor7-10weeks.
ConsumerswithschizophreniaseemtohavethehighestsuccesswhenCBTiscombinedwithNRTandstrategiestoenhancemotivation.ArandomizedcontrolstudybyBakeretal.(2006)foundthatatallfollow-upperiods,asignificantlyhigherproportionofsmokerswithapsychoticdisorderwhocompletedalltreatmentsessionswerecurrentlyabstinent,relativetoacomparisongroupofpersonsreceivingcareasusual,(pointprevalencerates:3months,30.0%vs.6.0%;6months,18.6%vs.4.0%;12months18.6%vs6.6%).Smokerswhocompletedalleighttreatmentsessionswerealsomorelikelytohaveachievedcontinuousabstinenceatthreemonths(21.4%vs.4.0%).
Thereisastrongdose-responserelationbetweenthesessionlengthofperson-to-personcontactandsuccessfultreatmentoutcomes.Intensiveinterventionsaremoreeffectivethanlessintensiveinterventionsandshouldbeusedwheneverpossible.
Haugetal.(2005)foundthatforpeoplewithdepression,smokingcessationwasbestpredictedbystageofchange,withthoseinpreparationenteringtreatmentmorequicklythancontemplatorsorprecontemplators.Thevariablesmostassociatedwithacceptingtreatmentwerenotseverityofsymptoms,butrathercurrentuseofpsychiatricmedicationsandperceivedabilitytosucceedinquitting.
S M O K I N G C E S S A T I O N T R E A T M E N T | 1 5
Smoking cessation treatment for persons with mental illnesses

S M O K I N G C E S S A T I O N T R E A T M E N T | 1 6
Components of Successful Intensive Intervention Programs:Intensivecessationinterventionsshouldincludethefollowing(fromtheU.S.DepartmentofHealthandHumanServices,2000):
AssessmentAssessmentsshouldensurethattobaccousersarewillingtomakeaquitattemptusinganintensivetreatmentprogram.Otherassessmentscanprovideinformationusefulincounseling(e.g.stresslevel,presenceofpsychiatricsymptoms,stressors,othercomorbidity).Personswithmentalillnesseswhoareattemptingtoquitsmokingshouldbecarefullyassessedandmonitoredfordepressionandotherpsychiatricsymptomsateveryofficevisit.
Program clinicians Multipletypesofcliniciansareeffectiveandshouldbeused.Onecounselingstrategywouldbetohaveamedical/healthcarecliniciandelivermessagesabouthealthrisksandbenefitsanddeliverpharmacotherapy,andbehavioralhealthcliniciansdeliveradditionalpsychosocialorbehavioralinterventionslikecognitivebehavioraltherapy(CBT).
Program intensity Becauseofevidenceofastrongdose-responserelationship,theintensityoftheprogramshouldbe:•Sessionlength–longerthan10minutes.•Numberofsessions–4ormore.•Totalcontacttime–longerthan30minutes.
Program formatEitherindividualorgroupcounselingmaybeused.Proactivetelephonecounselingalsoiseffective.Useofadjuvantself-helpmaterialisoptional.Follow-upassessmentinterventionproceduresshouldbeused.
Type of counseling and behavioral therapies Counselingandbehavioraltherapiesshouldinvolvepracticalcounseling(problemsolving/skillstraining),aswellasintra-treatmentandextra-treatmentsocialsupport.
PharmacotherapyEverysmokershouldbeencouragedtousepharmacotherapies,exceptinthepresenceofspecialcircumstances.Specialconsiderationshouldbegivenbeforeusingpharmacotherapywithselectedpopulations(e.g.pregnancy,adolescents).Theclinicianshouldexplainhowthesemedicationsincreasesmokingcessationsuccessandreducewithdrawalsymptoms.Thefirst-linepharmacotherapyagentsinclude:bupropionSR,nicotinegum,nicotineinhaler,nicotinenasalsprayandthenicotinepatch.(SeePharmacotherapiesSectiononp.19andlaminatedsheetatbackofthismanual).

S M O K I N G C E S S A T I O N T R E A T M E N T | 1 7
Behavioral Interventions for Smoking CessationUseofbriefpsychosocialinterventions,self-helpandsupportivetherapyhavebeenshowntobeeffectivewithgeneralmedicalpatientsbutmaynotbesufficientforconsumerswithpsychiatricproblems(APA,1996).Additionally,peoplewithmentalillnessesoftenhavefewersocialsupportsandcopingskills.Therefore,intensivebehavioraltherapyshouldbeconsideredforthesepeopleevenintheearlyquitattempts.Whenpossible,thementalhealthprovidershouldelicitconsumerpreferencesaboutgrouporindividualtherapy.Ifaconsumerhasaspecificissuethatmightunderminetobaccocessation(e.g.problemswithassertiveness),thementalhealthprovidermightworkonthisissueinindividualtherapywhiletheconsumeralsoattendsgrouptherapyfortobaccocessation.
Cessationprogramsforpeoplewithmentalillnessesincludeabout7-10sessions.Typically,thereis• anintroductiontotobaccohistoryandprevalence ofuse•educationaboutthepropertiesofnicotine,health effectsofnicotineandaddictivenatureofnicotine• areviewofthereasonswhypeoplesmoke•educationaboutwaysonecanquitsmoking,use ofmedicationanddevelopmentofaquitplan.
Asnotedabove,additionalsessionsareusefulforaddressingissuesthatarepertinenttopersonswithmentalillnesses(i.e.,developingcopingskillsforstressandanxiety).
TheSANEprograminAustralia(Strasser,2001)isoneeffectivegroupcounselingprogramforpersonswithschizophrenia.Itinvolvesteachingproblemsolvingskillsandcognitive-behavioraltechniquestoaidsmokingreductionandcessationmaintenance.Thegroupconsistsof10sessions,runbytwotrainedfacilitators.Thecontentconsistsofthefollowing:• IntroductiontotheProgram•ReasonstoQuit•BenefitsofQuitting•UnderstandingWhyWeSmokeandWays ofQuitting•WithdrawalSymptoms•SocialSupport•DealingwithStressandAnxiety•CopingwithDepression•AssertivenessTraining•AngerManagement•Smoke-FreeLifestyle•DealingwithHighRiskSituations
More Elements of Successful CounselingFurtherelementsofsuccessfulcounselingandsupportiveinterventionsareoutlinedinthefollowingtables(U.S.DepartmentofHealthandHumanServices,2000).
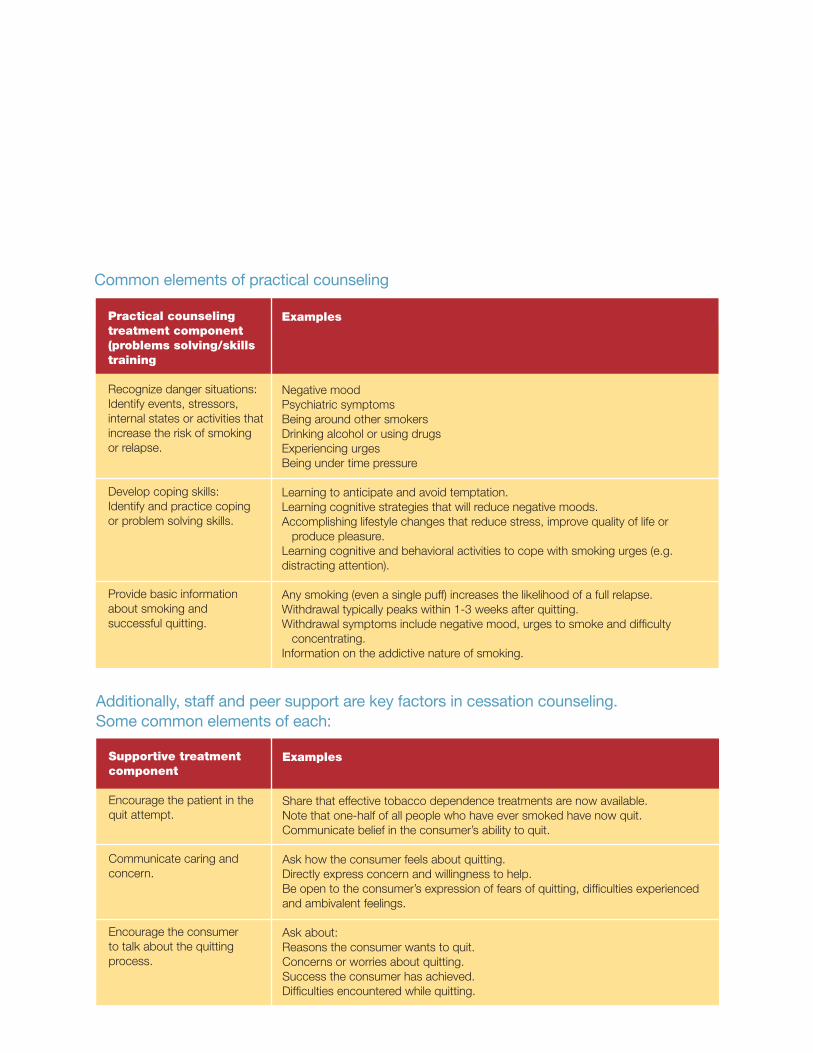
Practical counseling treatment component (problems solving/skills training
Recognizedangersituations:Identifyevents,stressors,internalstatesoractivitiesthatincreasetheriskofsmokingorrelapse.
Developcopingskills:Identifyandpracticecopingorproblemsolvingskills.
Providebasicinformationaboutsmokingandsuccessfulquitting.
Examples
NegativemoodPsychiatricsymptomsBeingaroundothersmokersDrinkingalcoholorusingdrugsExperiencingurgesBeingundertimepressure
Learningtoanticipateandavoidtemptation.Learningcognitivestrategiesthatwillreducenegativemoods.Accomplishinglifestylechangesthatreducestress,improvequalityoflifeorproducepleasure.Learningcognitiveandbehavioralactivitiestocopewithsmokingurges(e.g.distractingattention).
Anysmoking(evenasinglepuff)increasesthelikelihoodofafullrelapse.Withdrawaltypicallypeakswithin1-3weeksafterquitting.Withdrawalsymptomsincludenegativemood,urgestosmokeanddifficultyconcentrating.Informationontheaddictivenatureofsmoking.
Common elements of practical counseling
S M O K I N G C E S S A T I O N T R E A T M E N T | 1 8
Additionally, staff and peer support are key factors in cessation counseling. Some common elements of each:
Supportive treatment component
Encouragethepatientinthequitattempt.
Communicatecaringandconcern.
Encouragetheconsumertotalkaboutthequittingprocess.
Examples
Sharethateffectivetobaccodependencetreatmentsarenowavailable.Notethatone-halfofallpeoplewhohaveeversmokedhavenowquit.Communicatebeliefintheconsumer’sabilitytoquit.
Askhowtheconsumerfeelsaboutquitting.Directlyexpressconcernandwillingnesstohelp.Beopentotheconsumer’sexpressionoffearsofquitting,difficultiesexperiencedandambivalentfeelings.
Askabout:Reasonstheconsumerwantstoquit.Concernsorworriesaboutquitting.Successtheconsumerhasachieved.Difficultiesencounteredwhilequitting.

Common elements of eliciting peer support and other resources
S M O K I N G C E S S A T I O N T R E A T M E N T | 1 9
Supportive treatment component
Trainconsumersinsupportsolicitationskills.
Promptsupportseeking.
Arrangeoutsidesupport.
Examples
Showvideotapesthatmodelskills.Practicerequestingsocialsupportfromfamily,friendsandcoworkers.Aidconsumerinestablishingasmoke-freehome.
Helpconsumeridentifysupportiveothers.Calltheconsumertoremindhimorhertoseeksupport.Informconsumersofcommunityresourcessuchasquitlines.
Mailletterstosupportiveothers.Callsupportiveothers.Inviteotherstocessationsessions.Assignconsumerstobe“buddies”foroneanother.
Prescribing Cessation MedicationsUtilizethefrequencyofmentalhealthtreatmentvisitsasanopportunityformonitoringprogressinsmokingcessation.Additionally,smokingcessationstrategiesshouldbeintegratedandcoordinatedwithtreatmentsformentalillnesses.
Sincepeoplewithmentalillnessesappeartohavemorewithdrawalsymptomswhentheystopsmokingthanthegeneralpopulation,theuseofnicotinereplacementtherapy(NRT)eveninearlycessationattemptsisrecommended.
TheoptimaldurationofNRTisnotknown.Someindividualsappeartorequirelong-termuseofNRT(e.g.,≥6months),butalmostallindividualseventuallystopusingNRTandthedevelopmentofdependenceonNRTisrare.Thus,patientpreferenceshouldbethemajordeterminateforthedurationofNRT(American Psychiatric Association Practice Guidelines 2006: Treatment of Patients with Substance Use Disorders,2ndEdition,p54).
Cliniciansshouldcloselymonitoractionsorsideeffectsofpsychiatricmedicationsinsmokersmakingquitattempts.
DepressionConsiderbuproprionandnortriptylineforconsumerswithdiagnosesofdepression.Bupropion-SRhasbeendemonstratedtobethemosteffectiveindepressedpatients.Patientswhousebupropion-SRduringasmokingcessationprogramaremorelikelytobeabstinentatthequitdate.However,relapseishighfollowingthediscontinuationoftreatment(Evins,etal.,2005;George,etal.,2002).Additionally,bupropion-SRhashadadverseaffectsonpatientswithbipolardisorderand/orahistoryofeatingdisorders.Itshouldnotbeusedinthesepopulations(McNeill,2004).Additionalresearchonsmokerswithahistoryofdepressionsuggeststheusefulnessofthenicotinetransdermalpatch(Thorsteinssonetal.,2001)andnicotinegum(Kinnunenetal.,1996)forshort-termsmokingcessation.
StronglyconsiderbehavioraltherapiessuchasCognitiveBehavioralTherapy(CBT),assmokerswithdepressionarelikelytofailwithmoreminimalinterventions(Brownetal,2001).ImprovedcessationoutcomeswiththeadditionofCBThavebeenreportedfornortriptylineandnicotinegum(Halletal.,1998,1994).

S M O K I N G C E S S A T I O N T R E A T M E N T | 2 0
SchizophreniaSmokingcessationprogramsthatusethenicotinetransdermalpatch(NTP)demonstratethehighestquitratesforpatientswithschizophrenia(Williams&Hughes,2003)asitaidsinwithdrawalsymptoms.WhentreatmentincludestheuseofNRTinpatientswithschizophrenia,Dalacketal.(1999)foundthatdyskinesiasdecreasedduringabstinenceintheplacebopatchcondition,butincreasedduringabstinenceintheactivepatchcondition.
NRTisassociatedwithsmokingcessationratesof27percentto42percentinsmokerswithschizophrenia(Addingtonetal.,1998;Chouetal.,2004;Georgeetal.,2000).Also,useofnicotinenasalspray,whichproducesthehigherplasmalevelsofnicotine,isassociatedwiththereductionofwithdrawalandcraving(Williamsetal.,2004).
Incontrolledtrials,pharmacologicaltreatmentwithsustained-release(SR)bupropionhasbeenefficaciousinpromotingabstinenceinpersonswithschizophrenia.Treatment-seekingsmokershaveshownsuccess(withshort-termabstinenceratesof11percentto50percent)withacombinationofbupropionSRandcognitive-behavioraltherapy(CBT)atboththe150mg/day(Evinsetal.,2001)andthe300mg/daydoses(Evinsetal.,2005;Gerogeetal.,2002).Bupropiontreatmentalsoseemstoreducethenegativesymptomsofschizophrenia(Weinberberetal.,2006).
Patientstreatedwithatypicalantipsychoticagents,suchasclozapine(Clozaril),smokeless(Georgeetal.,1995;McEvoyetal.,1999,1995)andhaveaneasiertimequitting(Georgeetal.,2002,2000)thanthosetreatedwithtypicalantipsychoticmedications.However,smokingcessationcancauseachangeinplasmaconcentrationsofpsychotropicagentsduetoadecreaseintheinductionofcytochromeP4501A2(Weinbergeretal.2006).Antipsychoticmedicationswhosemetabolismisaffectedbysmokinginclude:clozapine(Clozaril),fluphenazine
(Modecate),haloperidol(Haldol),andolanzapine(Zyprexa).Therefore,monitoringmedicationsideeffectsmaybeneededduringthefirstmonthafterquitting(Kalmanetal.,inpress;ZiedonisandGeorge,1997).Themetabolismofrisperidone(Risperdal)andquetiapine(Seroquel)doesnotappeartobeaffectedbysmoking(Strasser,2001).
Bipolar DisorderGlassmanetal.(1993)foundthatpersonswithbipolardisorder(BD)mayalsobeatriskforrecurrenceofdepressivesymptomsduringsmokingcessation.Interestingly,personswithBDshowageneticlinkagetothea7nAChRnicotinicreceptorlocusonchromosome15similartothatfoundforpersonswithschizophrenia(Leonardetal.,2001).Todate,therehavebeennoempiricallybasedtreatmentspublishedforsmokerswithBD(Weinberger,etal,2006).UseofNTPissuggestedforthispopulation.
Anxiety DisordersAlthoughpatientsreportthatsmokingreducesdepressionandanxiety,chronicnicotineuseinanimalstudiesispositivelycorrelatedwithincreasedanxiety(Irvineetal.2001).Itisuncleartowhatextentsmokersexperiencewithdrawalsymptomsandmisinterpretareductioninnicotinewithdrawalasanxietyrelief(ZiedonisandWilliams,2003).Cinciripiniandcolleagues(1995)foundthatsmokerswithhighlevelsoftraitanxietyreceivingbuspirone(BuSpar)versusplaceboweremorelikelytohaveremainedabstinentattheendofthetrialbutnotatfollow-up.AsnotedbyWeinbergeretal.,(2006),aplacebo-controlledstudybyHertzbergetal.(2001)ofbupropionSRforsmokerswithposttraumaticstressdisorder(PTSD)foundthatbupropionwaswelltoleratedandresultedinhigherratesofsmokingcessation(60percent)ascomparedtotheplacebo(20percent).

S M O K I N G C E S S A T I O N T R E A T M E N T | 2 1
Also,inastudyofveteranswithpost-traumaticstressdisorderwhoweresmokersMcFallandcolleagues(2005)foundthatsmokerswhoreceivedtobaccotreatmentintegratedwiththeirpsychiatriccarewerefivetimesmorelikelythansmokerswhoreceivedseparatetreatmenttoreportabstinencefromsmokingninemonthsafterthestudy.ThesmokersreceivingtheintegratedtreatmentweremorelikelytouseNRTandtoreceivemoresmokingcessationsessions.Additionally,cognitivebehavioraltherapytechniquesthatincorporatecognitiverestructuringandexposuretherapytohelppersonslearntotolerateandbecomemorecomfortablewithphysicalsensationsmaybehelpfultopersonswithanxietydisorders(Morissetteetal.,2007).
Substance Use DisordersNotsurprisingly,concurrentuseofalcoholand/orotherdrugsisanegativepredictorofsmokingcessationoutcomesduringsmokingcessationtreatment(Hughes,1996).Long-termquitratesofsmokersinearlyrecoverfromsubstanceusedisorders(SUDs)arelow,atapproximately12percent(Kalman,1998;Sussman,2002).However,personswithapasthistoryofalcoholismdonodiffersignificantlyfromcontrolsubjectsintobaccotreatmentoutcomes(Hayfordetal.,1999).
Thecombinedeffectsofco-occurringsubstanceabuseandsmokingbehaviorsappeartosignificantlyinfluencethehighratesofsmokingcessationtreatmentfailure(Weinbergeretal.,2006).Therearefewstudiesofpharmacotherapeuticinterventionsforsmokinginsubstanceabusers,butsomeevidenceexistssuggestingthatnicotinereplacementandbehavioralapproachesareeffective(Burlingetal.,1996;Shoptawetal.,1996).Areviewoftobaccocessationstudiesbyel-Guebalyetal.(2002)foundthatquitratesrangedfromsevenpercentto60percentaftertreatmentandfrom13percentto27percentat12months.Todate,thereareno
publishedcontrolledstudiesusingbupropionSRinsmokerswithco-occurringSUDs,althoughthesestudiesareinprogress(Weinbergeretal.2006).
Thetimingofsmokingcessationtreatmentforsubstanceabusersremainscontroversial(Weinbergeretal,2006).Somestudiesfoundthatconcurrenttreatmentforsmokingandotherdrugsappearsnottobeassociatedwithincreaseduseofalcoholorotherdrugs(Burlingetal.,2001;Kalmanetal.,2004,2001).Josephetal.(2004)foundthatwhilepatientsinalcoholtreatmentareinterestedinsmokingcessation,participateintreatment,anddemonstratesuccess,theydidnotshowanybenefitfromconcurrenttobaccocessationtreatment.Infact,Josephetal.foundthatdrinkingoutcomeswereworsewithconcurrenttobaccotreatment,suggestingthattobaccocessationinterventionsshouldbeprovidedtopatientsafterintensivealcoholtreatmenthasbeencompleted.
Most relapses occur soon after a person quits smoking, yet some people relapse months or even years after the quit date. Relapse prevention programs can take the form of either minimal (brief) or prescriptive (more intensive) programs.
Components of Minimal Practice Relapse PreventionTheseinterventionsshouldbepartofeveryencounterwithaconsumerwhohasquitrecently.Congratulateeveryex-tobaccouserundergoingrelapsepreventiononanysuccess.Stronglyencouragethemtoremainabstinent.Whenencounteringarecentquitter,useopen-endedquestionsdesignedtoinitiateconsumerproblemsolvingsuchas“Howhasstoppingtobaccousehelpedyou?”Encouragetheconsumer’sactivediscussionofthetopicsbelow:
•Thebenefits,includingpotentialhealthbenefitsthatthe consumermayderivefromcessation.•Anysuccesstheconsumerhashadinquitting(duration ofabstinence,reductioninwithdrawal,etc.).•Theproblemsencounteredorthreatsanticipatedto maintainingabstinence(e.g.,depression,weightgain, alcoholandothertobaccousersinthehousehold).
Components of Prescriptive Relapse PreventionDuringprescriptiverelapseprevention,aconsumermightidentifyaproblemthatthreatenshisorherabstinence.Specificproblemslikelytobereportedbyconsumersandpotentialresponsesfollow:
Lack of support for cessation•Schedulefollow-upvisitsortelephonecallswith theconsumer.•Helptheconsumeridentifysourcesofsupportwithin hisorherenvironment.•Refertheconsumertoanappropriateorganizationthat offerscessationcounselingorsupport.
R E L A P S E P R E V E N T I O N | 2 3
Relapse prevention

R E L A P S E P R E V E N T I O N | 2 4
Negative mood or depressionIfsignificant,providecounseling,prescribeappropriatemedications,orrefertheconsumertoaspecialist.
Strong or prolonged withdrawal symptomsIftheconsumerreportsprolongedcravingorotherwithdrawalsymptoms,considerextendingtheuseofanapprovedpharmacotherapyoradding/combiningmedicationstoreducestrongwithdrawalsymptoms.
Weight gain•Recommendstartingorincreasingphysical activity;discouragestrictdieting.•Reassuretheconsumerthatsomeweightgain afterquittingiscommonandappearstobe self-limiting.•Emphasizetheimportanceofahealthydiet.•Maintaintheconsumeronpharmacotherapy knowntodelayweightgain(e.g.,bupropionSR, nicotine-replacementpharmacotherapies, particularlynicotinegum).•Referconsumertoaspecialistorprogram.
Flagging motivation / feeling deprived•Reassureconsumerthatthesefeelings arecommon.•Recommendrewardingactivities.•Probetoensurethattheconsumerisnot engagedinperiodictobaccouse
Emphasize that beginning to smoke (even a puff) will increase urges and make quitting more difficult.
Notes
____________________________________
____________________________________
____________________________________
____________________________________
____________________________________
____________________________________
____________________________________
____________________________________
____________________________________
____________________________________
____________________________________
____________________________________
____________________________________
____________________________________
____________________________________
____________________________________
____________________________________
____________________________________

L I T E R A T U R E R E V I E W | 3 3
Literature reviewIndividual Studies
Yr of Pub
2001
1998
2006
1996
2001
2000
Author
Acton,G.,Prochaska,J.,etal.
Addington,J.,el-Guebaly,N.,etal.
Baker,A.,Richmond,R.,Haile,M.,etal.
Borrelli,B.,Niaura,R.,etal.
Brown,R,,Kahler,C.,Niaura,R.,etal
Combs,D.&Advokat,C.
Article Name
Depressionandstagesofchangeforsmokinginpsychiatricoutpatients
Smokingcessationtreatmentforpatientswithschizophrenia
Arandomizedcontrolledtrialofasmokingcessationinterventionamongpeoplewithapsychoticdisorder
DevelopmentofMDDduringsmoking-cessationtreatment
Cognitive-behavioraltreatmentfordepressioninsmokingcessation
Antipsychoticmedicationandsmokingprevalenceinacutelyhospitalizedpatientswithchronicschizophrenia
Setting/ContactType
Outpatientpsychiatricresearchcenter;Survey
Outpatientpsychiatricresearchcenter;Facetoface
Outpatientmentalhealthclinicsorresearchcenter;Facetoface
Facetoface
Facetoface
Inpatient;Facetoface
Volume # /Issue #
AddictiveBehaviors,26(5)
AmericanJofPsychiatry,155(7)
AmericanJofPsychiatry,163(111)
JofClinicalPsychiatry,57(11)
JofConsulting&ClinicalPsych,69
SchizophreniaResearch,46(2-3)
Intervention
Correlationalstudy:205psychiatricoutpatientscompletedmeasuresofdepression(PRIME-MDandBDI-II)
50schizophrenicoutpatientsweredividedinto5groupswhometfor7weeklysmokingcessationprogramsessions
298regularsmokerswithapsychoticdisorderwererandomlyassignedtoatreatmentconditionconsistingof8individualonehoursessionsofmotivationalinterviewingandcognitivebehavioraltherapyorcontrol(treatmentasusual)
144non-depressedSstooktheBDIandtheHamiltonRatingScaleforDepression;txwasfluoxetine
Smokersw/MDDrandomizedtostandardCBTsmokingcessationtxorsmokingcessationtx+CBTtreatmentfordepression
Schizophrenicpatientswhosmokedandwereeitherreceivingatypicalantipsychotic(n=15),clozapine(n=6),oranotheratypicalantipsychotic(n=18)
Results
PatientswhohadneversmokedshowedlowerratesofMDDthanthosewhohadsmoked;patientsinearlystagesofchangedidnotshowmoreMDDordepressivesymptoms,butshowedmorenegativethoughtsaboutabstinence;suggestbuildingsmokingcessationinterventionsbasedonthetranstheoreticalmodelofchangeforusew/psychiatricpops.
42%ofpatientshadstoppedsmokingattheendofthegroupsessions,16%remainedabstinentat3mo,and12%at6mo.;nochangesineitherposornegsymptomsofschizophrenia.
Asignificantlyhigherproportionofsmokerswhocompletedalltreatmentsessionsstoppedsmokingateachofthefollow-uptimesthancontrols(pointprevalenceratesat3months:30%vs6%;6months:18.6%vs4%;12months18.6%vs4%).
5SsmetthresholdcriteriaforMDD.
SmokerwithrecurrentMDDandheavysmokerswhoreceivedCBT-Dweresignificantlymorelikelytobeabstinentthaninstandardtreatment.
Clozapinewasassociatedwithasignificantlylowerincidenceofsmokingthaneithertypicaldrugsorotheratypicalantipsychotics.

L I T E R A T U R E R E V I E W | 3 4
Yr of Pub
1990
2002
1999
2005
2004
Author
Covey,L,Glassman,A,etal.
Covey,L,Glassman,A,etal.
Dalack,G.,Becks,L.,etal.
Evins,A.,Cather,C.,etal.
Evins,A.,Rigotti,C.,etal.
Article Name
Depressionanddepressivesymptomsinsmokingcessation
Arandomizedtrialofsertralineasacessationaidforsmokerswithahistoryofmajordepression
Nicotinewithdrawlandpsychiatricsymptomsincigarettesmokerswithschizophrenia
Adouble-blindplacebo-controlledtrialofbupropionsustained-releaseforsmokingcessationinschizophrenia
Two-yearfollow-upofasmokingcessationtrialinpatientswithschizophrenia:Increasedratesofsmokingcessationandreduction
Setting/ContactType
Facetoface
Facetoface
Outpatientpsychiatricresearchcenter;Facetoface
Recruitedfromcommu-nitymentalhealthcenters;Facetoface
Facetoface
Intervention
Investigationintoresultsofabehaviorallyorientedsmokingcessationprogramshowedsmokersw/MDDhistoryhadlowersuccessrates
134smokerswithhistoryofMDDreceivedSertraline(n=68)ormatchingplacebo(n=66)1wkplacebowashout,9wkdouble-blind,placebo-controlledtreatmentphasefollowedbya9daytaperperiod,anda6mo.drugfreefollow-up;allreceivedintensiveindividualcessationcounselingduring9clinicvisits
19outpatientsw/schizophreniaorschizoaffectivedisorder;1dayofadlibitumsmokingfollowedby3daysofacutesmokingabstinencewhilewearing22mg/dayactiveorplacebotransdermalnicotinepatches,withareturnto3daysofsmokingbetweenpatchconditions
bupropion-SRvsplacebo;andCBT
2yrfollow-uptobupropiontxw/CBT
Results
Firstweek–frequencyandintensityofpsychologicalsymptoms,particularlydepressivemood,werehigheramongsmokerswithpastdepression;interventionsshouldattempttopreventdysphoricsymptomsduringacutewithdrawlperiodforMDDsmokers.
Sertralinetxproducedalowertotalwithdrawlsymptomscoreandlessirritability,anxiety,craving,andrestlessnessthanplacebo;howevernosignificantdifferencebetweenthegroups.
Dyskinesiaswerefoundtohavedecreasedduringabstinenceandplacebopatchtreatment,butincreasedduringabstinenceandtheactivepatchconditions.
Ssinbupropiongrpweremorelikelytobeabstinentfortheweekafterthequitdateandattheendoftheintervention;Ssinthebupropiongrphadahigherrateof4-wkcontinuousabstinence(wks8-12)andalongerdurationofabstinence;relapseishighfollowingthediscontinuation.
MoreSswereabstinentatfollowupthanwereabstinentattheendofthetrial;decreasedsmokingduringthetrialwaspredictiveoflatersmokingreduction.
Volume # /Issue #
ComprehensivePsychiatry,31(4)
AmericanJofPsychiatry,159(10)
Neuropsycho-pharmacology,21(2)
JofClinicalPsycho-pharmacology,25(3)
ClinicalPsychiatry,65(3)

L I T E R A T U R E R E V I E W | 3 5
Yr of Pub
1995
2002
2000
1997
1993
1991
2004
Author
George,T.,Sernyak,M.,etal.
George,T.,Vessicchio,J.,etal.
George,T.,Ziedonis,D.,etal.
Ginsburg,J.,Klesges,R.,etal.
Glassman,A.,Covey,L.,etal.
Greeman,M.&McClellan,T.
Haas,A.,Munoz,R.,etal.
Article Name
Effectsofclozapineonsmokinginchronicschizophrenicoutpatients
Aplacebocontrolledtrialofbupropionforsmokingcessationinschizophrenia
Nicotinetransdermalpatchandatypicalantipsychoticmedicationsforsmokingcessationinschizophrenia
Therelationshipbetweenahistoryofdepressionandadherencetoamulti-componentsmoking-cessationprogram
Smokingcessation,clonidine,andvulnerabilitytonicotineamongdependentsmokers
Negativeeffectsofasmoke-freeruleonaninpatientpsychiatryservice
Influencesofmood,depressionhistory,andtreatmentmodalityonoutcomesinsmokingcessation
Setting/ContactType
Facetoface
Facetoface
Facetoface
Facetoface
Facetoface
Inpatient;Facetoface
Facetoface
Intervention
29schizophrenicoutpatients;clozapinetxvsTYPneuroleptics
bupropion-SRvsplacebo
Ssw/schizoorschizoafftreatedw/NTP&w/eitherATYPorTYPantipsychotics;GToftheAmerLungAssnorGTforsmokersw/schizothatemphasizedmotivationenhancement,relapseprevention,socialskillstraining,andpsychoeducation
13wkCBG&randomassignmenttonicotinegum,appetitesuppressantgum,orplacebogum
Clonidine
SmokingbanoninpatientunitsataVeteransAffairsmedicalcenter
549Ss(28%w/historyofMDD);CBTvs.HE
Results
Therewasasigdecreaseinreporteddailyciguseafterclozapinetx.
Bupropion-SRincreasedsmokingabstinencerates;possymp–notaffected,negsympreduced;ATYPuseenhancesmokingcessationresponsestoBUP.
EffectsofNTParemodestinschizophrenicpatients;nodifferenceinGTprograms;ATYPmaybesuperiortoTYPincombinationw/NTPforsmokingcessationinschizophrenicpatients.
GroupCBTisaneffectivesmoking-cessationprogramforwomenwithahistoryofdepressionwhoarenotcurrentlydepressed.
MDDpredicttxfailure;anincreasedriskforpsychiatriccomplicationsaftersmokingcessationwasapparentamongsmokerwithMDD,particularlybipolar.
20-25%ofpatientswhosmokedhaddifficultyadjustingtotherule,andsomepatientsexperiencedmajordisruptionintheirtx.
MDD-RSshadhigherratesofabstinenceinCBTcomparedw/HE,evenwhenthecontributionofmoodandtheinteractionbetweenmoodandanMDDxtxvariablewereincludedinthemodel.
Volume # /Issue #
JofClinicalPsychiatry,56(8)
BiologicalPsychiatry,52(1)
AmericanJofPsychiatry,157(11)
AddictiveBehaviors,22(6)
ClinicalPharmacology&Therapeutics,54(6)
Hospital&Community,42(4)
JConsultClinPsychol,72(4)

L I T E R A T U R E R E V I E W | 3 6
Yr of Pub
1994
1998
1996
2005
Author
Hall,S.M.,Reus,V.I.,MunozR.F.,etal
Hall,S.M.,Reus,V.I.,MunozR.F.,etal
Hall,S.M.,Reus,V.I.,MunozR.F.,etal
Haug,N.A,Hall,S.M.Prochaska,J.J.etal.
Article Name
Cognitive-behavioralinterventionincreasesabstinenceratesfordepressive-historysmokers
NortriptylineandCBTinthetreatmentofcigarettesmoking
Moodmanagementandnicotineguminsmokingtreatment:Atherapeuticcontactandplacebo-controlledstudy
Acceptanceofnicotinedependencetreatmentamongcurrentlydepressedsmokers
Setting/ContactType
Facetoface
Facetoface
Facetoface
Outpatientpsychiatricresearchcenter;Self-reportandstructuredinterviewmeasures
Intervention
149smokers(31%hadahistoryofMDD);allreceived2mg/dayofnicotinegum;MMprovidedin10groupsessionsover8wks;standardtxprovidedin5gpsessionsover8wks
HxofMDDvs.NohxofMDDrandomizedtoNortriptylinevs.placeboandCBTvs.control
Moodmanagement(MM)vs.contact-equivalenthealtheducation(HE);and2mgto0mgofnicotinegumforsmokersw/historyofMDD
Thisstudyreportsonbaselinecharacteristicsassociatedwithacceptanceandrefusalofavailablesmokingtreatmentamongcurrentlydepressedsmokersinapsychiatricoutpatientclinic.Thesample(N=5154)was68%femaleand72%White,withameanageof41.4yearsandaveragesmokingrateof17cigarettes/day.Allparticipantswereassignedtoarepeatedcontactexperimentalcondition;receivedastage-basedexpertsystemprogramtofacilitatetreatmentacceptance;andwerethenofferedsmokingtreatment,consistingofbehavioralcounseling,nicotinepatch,andbupropion
Results
Ssw/MDDweremorelikelytobeabstinentwhentreatedw/MM,andlessangeratbaselinewaspredictiveofabstinence.
Nortriptyline-higherabstinenceratesthanplacebo,independentofdepressionhx.CBT-Moreeffectivefor+hxMDD.Smokerswithhxofdepressionareaidedbymoreintensivepsychosocialtreatments.
MMandHEproducedsimilarabstinencerates:2mggumwasnomoreeffectivethanplacebo;MDDpatientshadagreaterincreaseinmooddisturbanceafterthequitattempt;MDDpatientsmaybebesttreatedbyinterventionsprovidingadditionalsupportandcontact,independentoftheraputiccontact.
Thenumberofdaystotreatmentacceptancewassignificantlypredictedbystageofchange,withthoseinpreparationenteringtreatmentmorequicklythancontemplatorsorprecontemplators.Inalogisticregression,thevariablesmoststronglyassociatedwithacceptingtreatmentwerecurrentuseofpsychiatricmedicationandperceivedsuccessforquitting.Severityofdepressivesymptoms,durationofdepressionhistory,andhistoryofrecurrentdepressionwerenotrelatedtotreatmentacceptance.Findingshaveimplicationsforthepsychiatricassessmentandtreatmentofsmokersinclinicalsettings.Psychiatricmedicationmayplayasignificantroleinsmokingcessationtreatmentacceptancebycurrentlydepressedsmokers.
Volume # /Issue #
JConsultClinPsychol,62(1)
ArchivesGenPsych,55
JofConsulting&ClinicalPsych,64(5)
Nicotine&TobaccoResearch,7(2),(April2005)217–224

L I T E R A T U R E R E V I E W | 3 7
Yr of Pub
1999
2000
2000
1997
2002
1998
Author
Hayford,K.,Patten,C.,etal.
Keuthen,N.,Niaura,R.,etal.
Lucksted,A.,Dixon,L.,etal.
Martin,J.E.,Calfas,K.J.,PattenCA,etal.
Niaura,R.,Spring,B.,Borelli,B.,etal.
Patten,C.A.,Martin,J.E.,Meyers,M.G.,etal.
Article Name
Efficacyofbupropionforsmokingcessationinsmokerswithaformerhistoryofmajordepressionoralcoholism
Comorbidity,smokingbehaviorandtreatmentoutcome
Afocusgrouppilotstudyoftobaccosmokingamongpsychosocialrehabilitationclients
Prospectiveevaluationofthreesmokinginterventionsin205recoveringalcoholics:One-yearresultsofProjectSCRAP-Tobacco
Multicentertrialoffluoxetineasanadjuncttobehavioralsmokingcessationtreatment
Effectivenessofcognitive-behavioraltherapyforsmokerswithhistoriesofalcoholdependenceanddepression
Setting/ContactType
Facetoface
Facetoface
Facetoface
Facetoface
Facetoface
Facetoface
Intervention
615smokersreceivedplaceboorbupropion-SRat100,150,or300mg/dayfor6wksaftertargetquitdate
120smokers;10wksmokingcessationtrialw/fluoxetine&behavioraltx;62.3%ofSswerediagnosedwithalifetimemood,anxietyorSUD
5focusgroups(6-10Sseach)40clientsinpsychosocialrehabilitationprograms.Discussedprosandconsofsmokingandnotsmoking.
Randomized:standardtreatment(ALAquitprogram+nicoticeanonymousmeetings)(ST),behavioralcounseling+exercise(BEX),orbehavioralcounselingplusnicotinegum(BNIC)
Randomizedto3doseconditions:10weeksofplacebo,30mg,or60mgfluoxetineplus9weeksCBT
Randomized:behavioralcounseling(BC)orBC+CBT
Results
Doseresponseeffectoftxforsmokingcessationwasfound.
Lifetimecomorbiditywasrelatedtohighersmokingratesandnicotinedependence,depressedmoodandgreaterselfreportofanxietyandstress.BaselinescoresontheBDIwererelatedtotxoutcomeforSsw/opositivehistoryofanypsychiatricdisorder,withlowerBDIscoresmorefreqinthosewhowereabstinent.
Resultsindicatethatissuesandneedsthatarespecifictosmokerswhousementalhealthservicesmustbeaddressedinthedevelopmentofsmokingpreventionandcessationinterventionsinpsychosocialrehabilitationandothermentalhealthprograms.
BEX=significantlyhigherquitratesatpost-treatment,notat6or12months.
Analysesassumingmissingdata=smokingobservednotreatmentdifferenceinoutcomes.Pattern-mixtureanalysisthatestimatestreatmenteffectsinthepresenceofmissingdata=enhancedquitratesassociatedwithboththe60-mgand30-mgdoses.
SignificantlymoresmokersinCBTquitatpost-treatmentand12monthfollowup.
Volume # /Issue #
BritishJofPsychiatry,174
Psychotherapy&Psycho-somatics,69(5)
PsychiatricServices,51(12)
JofConsulting&ClinicalPsych,65(1)
JofConsulting&ClinicalPsych,70(4)
JofStudiesonAlcohol,50(3)

L I T E R A T U R E R E V I E W | 3 8
Yr of Pub
2000
1997
2006
2001
1997
Author
Patten,C.A.,Martin,J.E.,Calfas,K.J.,etal.
Rabois,D.,Haaga,D.
Thorndike,F.P.,Friedman-Wheeler,D.G.,Haaga,D.A.
Weiner,E.,Ball,M.P.,Summerfelt,A.,etal
Ziedonis,D.M.,George,T.P.
Article Name
Briefreporteffectofthreesmokingcessationtreatmentsonnicotinewithdrawalin141abstinentalcoholicsmokers
Cognitivecoping,historyofdepression,andcigarettesmoking
Effectofcognitivebehaviortherapyonsmokers’compensatorycopingskills
Effectsofsustained-releasebupropionandsupportivegrouptherapyoncigaretteconsumptioninpatientswithschizophrenia
Schizophreniaandnicotineuse:Reportofapilotsmokingcessationprogramandreviewofneurobiologicalandclinicalissues
Setting/ContactType
Facetoface
Interview
Facetoface
Outpatientpsychiatricresearchcenter;Facetoface
Facetoface
Intervention
Randomizedto12weekprogramofStandardTreatment,behavioralcounselingplusexercise,orbehavioralcounselingplusnicotinegum
TestedpremisethatformerlydepressedsmokersarelackingincognitivecopingskillstaughtinCBT.4groups(depressed/not,smoker/not)completedWORtotestcognitivecoping
RandomizedtoCBTorcomparisonconditionofeducationandscheduledsmokingreduction.(uniquetoCBTconditionwascognitiverestructuringformoodmanagement)
9sessionsofweeklygrouptherapyinconjuctionwithopenlabelbupropiontreatment(150mg/twiceaday)for14weeks
24schizophrenicpatients:Nicotinereplacement,motivationalenhancementtherapy,andrelapsepreventionbehavioraltherapy
Results
Nosignificanteffectoftreatmentonpercentagereductioninsmokingrate.All3groupsshowedsimilaroverallreductionsinsmokingrate.
HxofdepressionassociatedwithsignficantlymorenegativeresponsesonWOR.“Thisstudysuggeststhatpeoplewithahistoryofdepressiontendtolacksuchskillsandmightthereforeespeciallybenefitfromincorporationofcognitivebehaviortherapyprinciplesinsmoking-cessationprograms.”
CBTgroupdidNOTshowmoreimprovementincompensatorycopingskills(measuredbyWaysofResponding).AnonsignificanttrendfavoringCBTwasfoundinpost-treatmentabstinence.
Noneofthesubjectsquitsmoking.However,measuredchangeinexpiredbreathcarbonmonoxidelevelsindicatedreductioninsmoking.
50%completedtheprogram,40%decreaseduseby50%,and13%remainedabstinentfor6months.
Volume # /Issue #
AddictiveBehaviors25(2)
AddictiveBehaviors,22(6)
AddictBehav,Jan18
AmJofPsychiatry,158
SchizophreniaBulletin,23(2)

L I T E R A T U R E R E V I E W | 3 9
Review Articles
Yr of Pub
1992
1998
1999
2002
1995
2003
1993
2001
1998
Author
Dalack,G.W.&Glassman,A.H.
Dalack,G.W.,Healy,D.J.,etal.
Dursun,S.M.&Kutcher,S.
el-Guebaly,N.&Cathcart,J.
Hughes,J.R.&Frances,R.J.
Martinez-Raga,J.&Keaney,F.
Resnick,M.P.
Ziedonis,D.,Krejci,J.,etal.
Ziedonis,D.M.,Wyatt,S.A.,etal.
Article Name
Aclinicalapproachtohelppsychiatricpatientswithsmokingcessation
Nicotinedependenceinschizophrenia:Clinicalphenomenaandlaboratoryfindings
Smoking,nicotineandpsychiatricdisorders:evidencefortherapeuticrole,controversiesandimplicationsforfutureresearch
Smokingcessationapproachesforpersonswithmentalillnessoraddictivedisorders
Howtohelppsychiatricpatientsstopsmoking
TreatmentofnicotinedependencewithbupropionSR:Reviewofitsefficacy,safetyandpharacologicalprofile
Treatingnicotineaddictioninpatientswithpsychiatricco-morbidity
Integratedtreatmentofalcohol,tobacco,andotherdrugaddictions
Currentissuesinnicotinedependenceandtreatment
Volume # /Issue #
PsychiatricQuarterly,63(1)
AmericanJofPsychiatry,155(11)
MedicalHypotheses,52(2)
PsychiatricServices,53(9)
Psychiatric`Services,46(5)
AddictBiol,8(1)
Nicotineaddition:Principlesandmanagement,pp.327o-336(eds:Orleans,C.T.&Slade,J.D.)
Integratedtreatmentofpsychiatricdisorders(ed:Kay,J.)Reviewofpsychiatry,20(2)
Newtreatmentsforchemicaladdictions(eds:McCance-Katz,E.F.&Kosten,T.R.)Reviewofpsychiatryseries.
Conclusions/Discussion
Adiscussionoftheinterfaceofpsychiatricillnessandsmoking,particularlyamongthosechronicallyhospitalizedinpsychiatricinstitutions.Itsuggestsarationalapproachtohelppsychpatientsstopsmoking.
Clinicaldatasuggestthatsmokinginschizophreniaisanattempttoself-medicate(negative)symptoms.Knowledgeontheeffectsofnicotineonschizopatientsmayleadtonewtreatmentforbothdxandtx.
Investigatedthreecomponentsofthesocial-scientific-ethicaldilemmathatresearcherslookingintothepossibletherapeuticeffectsandthemechanismsofactionofnicotineinneuropsychiatricdisorders.
Reviewof24empiricalstudiesofoutcomesofsmokingcessationapproachesusedwithsamplesofpersonswithmentaldisorders.Foundthatthemajorityofinterventionscombinedmedicationandpsychoeducation.
ThisarticlefoundthatbupropionSRappearstobeasafe,well-toleratedandeffectivemedicationincombinationwithsmokingcessationcounsellingforawiderangeofsmokers.
Exploretheuniquecircumstancesofpsychiatricpatients,therelationshipbetweenpsychiatricdisorderandnicotineaddition,andspecialproblemsinpsychiatricinstitutions/recentresearchontheinteractionbetweensmokingcessation,relapse,andmooddisorderisreviewed/discussesinteractionbetweenpsychotropicmedicationsandsmoking.
Empiricalliteratureontheeffectivenessofcombinedtreatmentofspecificsubstanceusedisorders.Reviewof3oftheleadingpsychotherapiescurrentlyinuseinthetreatmentofpatientswithsubstanceabusedisorders:12-step,motivationalenhancementtherapy,andrelapseprevention.
Pharmacotherapiescanbeintegratedwithbehavioralmanagementtechniquesthatareindividualizedtotheneedsofthepatient.

"This course was developed from the public domain document: Smoking Cessation for
Persons with Mental Illnesses: A Toolkit for Mental Health Professionals – University of
Colorado Anschutz Medical Campus: Behavioral Health & Wellness Program.”