Smile: Every PT can treat a Why did I choose this topic ...
10
[email protected] 4/17/2021 You may not copy or reuse the information without permission of Dr. Joni Barry 1 Smile: Every PT can treat a person after facial nerve injury (competently) Joni G Barry PT, DPT Professor ABPTS Neurologic Certified Specialist [email protected] Why did I choose this topic? What is my experience with this population Plan for the session • Review of facial nerve and muscle of facial expression • Discussion of common diagnoses affecting the facial nerve and the medical/surgical management • PT evaluation and management of facial nerve injuries • I welcome questions/e-mails at anytime Muscles of Facial Expression Innervated by the Facial Nerves (CN VII) so when this nerve is damaged it is essentially a peripheral nerve injury • Each Facial Nerve has 7,000 motor fibers (and 3,000 that go to some of our taste buds) 4 Copyrights apply Copyrights apply From UpToDate®
Transcript of Smile: Every PT can treat a Why did I choose this topic ...

[email protected] 4/17/2021
You may not copy or reuse the information without permission of Dr. Joni Barry 1
Smile: Every PT can treat a
person after facial nerve injury
(competently)
Joni G Barry PT, DPTProfessorABPTS Neurologic Certified Specialist
Why did I choose this topic?
What is my experience with this population
Plan for the session
• Review of facial nerve and muscle of facialexpression
• Discussion of common diagnoses affectingthe facial nerve and the medical/surgicalmanagement
• PT evaluation and management of facialnerve injuries
• I welcome questions/e-mails at anytime
Muscles of Facial Expression
Innervated by the Facial Nerves (CN VII)
so when this nerve is damaged it is essentially a peripheral nerve injury
• Each Facial Nerve has 7,000 motor fibers(and 3,000 that go to some of our tastebuds)
4
Copyrights apply Copyrights apply
From UpToDate®

[email protected] 4/17/2021
You may not copy or reuse the information without permission of Dr. Joni Barry 2
Muscles of Facial Expression23+ pairs of skeletal muscle in our face have differences from our typical skeletal muscles, most notably are:1. Don’t attach to bone but embedded in skin2. They can stay viable several years without
innervation3. They get input from both the motor cortex
and the emotional side of your brain– which comes in handy later in therapy
4. They lack muscle spindle5. Small motor units
Common diagnoses with Facial Nerve injury
• Bell’s Palsy– (including Shingles/Ramsey Hunt Syndrome)
• Acoustic Neuroma
• Trauma
Bell’s Palsy• Common clinical condition affecting 20-30 per
100,000 people per year• Can occur in any age group, most common
between 15-45• Cause is uncertain, animal models show a role of
viruses• Some have latent Herpes virus reactivated, or
Shingles from a history of Chicken Pox• Inflammation in the auditory canal creates
compression initially causing demyelination but itcan lead to axonal degeneration
• People with DM and pregnant women have anincreased incidence
Copyrights apply
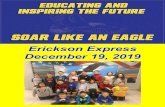
Bell’s Palsy phenomenon seen with his attempted eye closure
Clinical Manifestations
• Rapidly developing facial paralysis/paresis
• Decreased resting tone of face (droopingeye and mouth, decreased/absentnasolabial fold)
• Eye doesn’t close (cornea at risk)
• Decreased tearing
• Some taste buds involved
• Stapedius muscle (sensitive to loud noise)

[email protected] 4/17/2021
You may not copy or reuse the information without permission of Dr. Joni Barry 3
Medical Management• Diagnosis
– mostly clinical presentation– Differentiating LMN (Bell’s palsy) from UNM (stroke)
look at upper face which has bilateral input frommotor cortex
– Can do EMG after a week to determine the extent ofthe damage
• Only demyelination (faster recovery)• Axonal damage (will take longer and possibly incomplete)
• Treatment:– Steroids ASAP and often anti-virals– protection of cornea– Potential surgical decompression if recurrence
Which patient had a stroke and who has Bell’s palsy?
Copyrights apply From UpToDate®
Prognosis• 94% with incomplete involvement and get a
complete recovery over a period of days to weeks• 75% with complete involvement recover normal
function• Recovery is slower & sometimes incomplete if
nerve needs to regenerated (1 mm/day or 1 inch/month)
• Then may get some unwanted movements –synkinesis and increased facial tone
• Worse prognosis for those with Ramsey Huntsyndrome or those with other conditions such asDM
Synkinesis• Extra unwanted contraction or synchronization of
some facial muscle when trying to use others• Commonly an eye closing when your smile or the
mouth getting pulled when closing your eyes orraising your eyebrows
• Platysma can pull down when you try to smile• People can also have a feeling of tightness and
discomfort at rest (almost the opposite of whatthey started with)
• It can be managed in part with Botox injections butalso neuromuscular re-education
• http://bellspalsy.ws/residual-effects/
Acoustic Neuromas
• Typically originate in the internal auditorycanal and tumor grows into thecerebellopontine angle eventuallycompressing the facial nerve and encroachingon the brainstem
• Clinical Manifestation– Unilateral sensorineural hearing loss– Tinnitus, vertigo, unsteadiness– Facial weakness, numbness, trouble swallowing– Eventual obstruction of 4th ventricle– Symptoms from pressure on brainstem

Copyrights apply From UpToDate®
You may not copy or reuse the information without permission of Dr. Joni Barry
4

[email protected] 4/17/2021
You may not copy or reuse the information without permission of Dr. Joni Barry 5
http://med.mui.ac.ir/slide/clinical/ent/AcousticNeuroma.jpg
http://www.anausa.orghttps://www.anausa.org/learn-about-acoustic-neuroma/learn-overview
Prognosis• Majority of cases a cure is achieved with surgical
resection• Also see gamma-knife surgery (radiation) done• Often come out of surgery with permanent hearing
loss on that side and some balance deficits• They try to electrically monitor the facial nerve to
preserve it but at times it has to be sacrificed andother times they still have facial paresis post-op
• If they know the facial nerve was sacrificed in thefuture they may need to do either a CN XII to VIIanastomosis or a facial reanimation surgery
http://www.youtube.com/watch?v=ClrBPO6KULk
Hypoglossal (XII), Trigeminal(V) or cross facial to facial (VII) nerve anastomosis surgery
• Used to restore movement to facial muscles• Have to relearn how to control facial
movements through voluntary tongue orchewing movements
• There was a study published looking atrecovery of 30 patients– Reinnervation occurred 5.5 months post-op– 8 had weights implanted in eyelid; 6 had
tarsorrhaphy– 80% had automatic activation or facial mm with
tongue movements but none had a spontaneoussmile
– 14 had synkinesis; 2 were treated with Botox
Passive facial reanimation
• Surgical techniques create a sling thatholds the facial muscles in a partial smile
• ultimate goal of facial reanimation is torestore resting facial symmetry anddynamic facial motion that mirrors theopposite side as closely as possible
• Can use the temporalis tendon and agracilis free muscle transfer
PT Exam• History
– Acute or Chronic– Etiology– Co-morbidities– What is biggest concern and goals
• Observation of face at rest– Low tone vs. high tone– Any spontaneous blinking on involved side
• Examination of facial expression– Looking for symmetry– Looking for unwanted movement (synkinesis)– Prioritizing eye closure
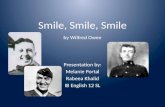
Outcome measures• House-Brackmann scale classification (I – VI)
– Used by physicians– I = Normal & VI = total paralysis
• Facial Grading Scale (Sunnybrook FacialGrading System)– Going through this eval moves easily into a HEP– Gives a score out of 100 that is easy to use when
setting goals
• Can look at other facial expressions• Documentation with photographs or videos

[email protected] 4/17/2021
You may not copy or reuse the information without permission of Dr. Joni Barry 6
Copyrights apply Copyrights apply
Intervention and Plan of Care
• Education• Eye protection• Oral Hygiene• Neuromuscular Re-education
– Early/Acute– Later/Chronic
• Home Exercise Program
• Frequency and Duration of visits
Education Protecting the eye• If they are not able to close the eye there
is risk of corneal damage from dryness orscratching
• Don’t want to just put tape over the eye– Moisture Chamber
– Ointment
• Should not wear contacts

Resting Symmetry -
Compared to normal side
Eye (choose one only)
normal 0
narrow 1 wide 1 eyelid surgery 1
Cheek (naso-lablal lild)
normal 0
absent 2 less pronounced 1 more pronounced 1
Mouth
normal 0
corner dropped 1 corner pulled up/out 1
Tota1O
Resting
D symmetry Total X 5 score
Patient's name
Ox
Date
Symmetry of Voluntary Movement ,-
Standard Expressions
Forehead Wrinkle (FRO)
Gentle eye
closure (OCS)
Open mouth smile (ZYG/RIS)
Snarl (LLA/LLS)
Lip Pucker (OOS/OOI)
Degree of muscle EXCURSION
compared to normal side
-�� � .�CZ, �
f � .!!! .!!! � CZ, Z;- � -� � .... $ c:; � ..§ -� (:) � � � -�� �
-s i ,,,"'f � � � CZ, � �-� 1� CZ,
.!!!$ -$$-,(:) � ''- �
�(:) -� (:) ::s � ��
1 2
1 2
1 2
1 2
1 2
.... !:? -.;; -�� ��
�:} �tJ
3 4
3 4
3 4
3 4
3 4
f� :$
5
5
5
5
5
�� c:; 'qf
!!'i::- .!!!� :)::,, ;!>, .... ;!>,
D
D
D
D
□��Ii:
f�
�� G'qf �, �,
if, � if, "t' "t'
·':::� ,� � CZ, ' CZ,
I �l □
if, "t'
Total
Vol mov't score
Voluntary movement score:
□-Resting symmetry score □-
Total X 4
Synk score
D
D
Synkinesis
Rate the degree of INVOLUNTARY MUSCLE CONTRACTION associated with each expression
·!:? .� .... 't;; tJ �-� tJ �
�!'I.' :$$ ,,,-c::,� �� ·!:? � ,,, ���
tJ .c:;� ,,, �:; ·!:? I � ·� �,,,$ tJ CZ,-� �� ��
-� � � <:j ,ff, :::i lit � �� if, :$ ,ff, ;;
;;f.:: .;s- !it• ,!(, :: � -� <:::, � ...
�$ r:§ I,; (S �
� !i,· !i,· � q• I I ;:, I � � 4'
0 1 2 3 D 0 1 2 3 D 0 1 2 3 D 0 1 2 3 D - -
0 1 2 3 D
Synkinesis score: Total □ Composite score D
Ross, Fradet. Nedzelsk1 1992
You may not copy or reuse the information without permission of Dr. Joni Barry
7

[email protected] 4/17/2021
You may not copy or reuse the information without permission of Dr. Joni Barry 8
Eye weights (temporary or permanent)
• External eye weights
• Implantable eye weights
• http://www.meddev-corp.com/1%20product/Eyelid%20Closure%20Products/eyelid%20products.htm
Oral Hygiene
• Potential for pocketing of food on involvedside
• Biting cheek
• Trouble drinking or keeping liquids inmouth
Early Neuromuscular Reeducation
Eye Closure difficulties:
• Working around Bell’s Palsy phenomenon
• Focusing on glancing down while trying toclose eye (and once not seeing light)
• Education to wear sunglasses and becautious out in wind when still without afunctional protective blink
Early Neuromuscular Reeducation
• Other muscles of facial expression
• Explore for changes from week to week incases that start with complete loss
• May see differences between trying tovolitionally make expressions vs. moreautomatic and emotional expressions
Neuromuscular Reeducation
• When trying to make expressions likesmiling think:
1. Slow – try to delay good side2. Small – may just go through part of
excursion on good side3. Symmetrical – using a mirror for feedback
can help4. Can also try to tap into the more
automatic emotional input
Some Exercises
• Close mouth smile• Open mouth smile• Pucker• Lip compression• Eyebrow raise• Squint• Wide eyes• Furrowed brow

[email protected] 4/17/2021
You may not copy or reuse the information without permission of Dr. Joni Barry 9
During chronic phase (past 3 months)• Watch for more activity or tightness at rest• Opposite asymmetries from the start• Complaints of tightness and also of
synkinesis• Can introduce moist heat and stretches• Work to gain control of synkinesis
– I tend to give other examples of ability toretrain muscles after reinnervation
• One exercise I add here is keeping mouthclosed and filling cheeks with air
Use of Botox® (FDA approval for this use)
• When to consult with physician for Botox?
• Can be used to weaken uninvolved side toimprove symmetry
• Can be used to tone down synkinesis
• It is a great opportunity to go with thepatient to the appointments
BTX-A: Mechanism of ActionBotulinum toxin acts presynaptically at nerve
terminals to prevent release of acetylcholine.
Result CHEMICAL DENERVATION• Once inside cell, botulinum toxin type A blocks
release of acetylcholine transmitter.This produces functional muscle denervation.
BTX-A: Mechanism of Action• RESPROUTING - In muscles treated
with botulinum toxin type A, chemical denervation of neuromuscular junction stimulates nerve sprouting.
• RE-ESTABLISHING - Single nervesprout establishes new neuromuscularjunction. Muscle tone is restored andspasms return
• Making it necessary to repeatinjections approximatelyevery 3 to 6 months,depending on individualpatient response.
• RESPROUTING - In muscles treated with botulinum toxin type A, chemical denervation of neuromuscular junction stimulates nerve sprouting.
• RE-ESTABLISHING - Single nervesprout establishes new neuromuscularjunction. Muscle tone is restored andspasms return
• Making it necessary to repeatinjections approximatelyevery 3 to 6 months,depending on individualpatient response.
Stretches (go slow repeat a few times each)
1 - Follow a clock-like pattern from close to nose to side of cheek and have thumb in mouth and 1-2 fingers over face and pull slowly until out of mouth pausing and squeezing to tolerance if a knot or tender area felt2 - Can also use thenar eminence and push along Platysma (down side of neck) while turning head up and away
Biofeedback for NMR
• Visual Feedback in a mirror– Works in clinic or with a HEP
• Surface EMG– In clinic if available
• Keying into proprioceptive feeling of facial expressions with unaffected side as a model

[email protected] 4/17/2021
You may not copy or reuse the information without permission of Dr. Joni Barry 10
Use of electric stimulation or things like acupuncture: the debate…..
• Study on rats in 2019 showed femoral n.responded to brief low frequency ES tonerve stump but facial nerve did not
• J Diels recommends avoiding ES as itdoesn’t speed recovery and has concernit may add to synkinesis
• Cochrane review of Acupuncture for Bell’sPalsy in 2010 concluded they could notmake a conclusion due to inadequatequality of trials found (6 RCT with N=537)
But…….
• Neither is definitively harmful
• If patients feel something like acupunctureis helpful I would not tell them to stop
• If someone wanted to do some ES I wouldsuggest an AC type after 3 months vs. aDC point stimulator acutely
Frequency and duration or PT• If early after Dx of Bell’s palsy or if nerve
monitored and thought to be intact for ANsurgery may educate, protect eye and mouthand wait a few weeks for spontaneousrecovery
• If still impaired reassess every few weeksand by 3 month post watch for signs ofsynkinesis
• Overall every 2 -4 weeks to monitor andprogress HEP– More often if doing EMG biofeedback to retrain
• This may be a perfect population fortelerehab services
References• http://bellspalsy.ws• http://www.anausa.org• https://www.facialretraining.com/• https://facialparalysisfound.wistia.com/medias/8wpu0g8uuv
• https://facialtherapyspecialists.com/
• Jacqueline Diels Nonoperative Facial Rehabilitation in Vestibular Schwannoma: Facial Neuromuscular Retraining. Ch 62 Medical and Surgical Rehabilitation of Vestibular Schwannoma. 2019. Thieme Publshers.
• Tiemstra J, Khatkhate N. Bell’s Palsy Diagnosis and Management. Am Fam Physician 2007;76:997-1002, 1004. Copyright © 2007 American Academy of Family Physicians.https://www.aafp.org/afp/2007/1001/p997.html
• Vestibular schwannoma (acoustic neuroma) UpToDate www.uptodate.com ©2021 UpToDate, Inc.
• Bell’s palsy: Pathogenesis, clinical features, and diagnosis in adults. UpToDate Literature review current through Feb 2021.www.uptodate.com ©2021 UpToDate, Inc.
• Bell's palsy: Treatment and prognosis in adults. UpToDate Literature review current through Feb 2021. www.uptodate.com ©2021 UpToDate, Inc.
References
• Madhok VB, Gagyor I, Daly F, Somasundara D, Sullivan M, Gammie F,Sullivan F. Corticosteroids for Bell's palsy (idiopathic facial paralysis).Cochrane Database of Systematic Reviews 2016, Issue 7.
• Uscategui T, Doree C, Chamberlain IJ, Burton MJ. Corticosteroids as adjuvant to antiviral treatment in Ramsay Hunt syndrome (herpes zoster oticus with facial palsy) in adults. Cochrane Database of SystematicReviews 2008, Issue 3.
• Costa J, Espírito-Santo CC, Borges AA, Ferreira J, Coelho MM, Moore P, Sampaio C. Botulinum toxin type A therapy for hemifacial spasm. Cochrane Database of Systematic Reviews 2005, Issue 1.
• Toffola ED et al. Hypoglossal-facial nerve anastomosis and rehabilitation in patients with complete facial palsy: cohort study of 30 patients followed up for three years. Functional Neurology 2014; 29(3): 183-187
References• Samuel L. Oyer, MD; Jason Nellis, MD; Lisa E. Ishii, MD; Kofi D.
Boahene, MD; Patrick J. Byrne, MD Comparison of Objective Outcomes in Dynamic Lower Facial Reanimation With Temporalis Tendon and Gracilis Free Muscle Transfer JAMA Otolaryngol Head Neck Surg. 2018;144(12):1162-1168.https://www.ncbi.nlm.nih.gov/pmc/articles/PMC6583085/
• https://www.anausa.org/learn-about-acoustic-neuroma/video-library/809-facial-paralysis-the-science-and-art-of-treating-facial-palsy (35 minute presentation by Dr. Rozen on the topic
• Elkatatny A, Abdallah H, Ghoraba D, Amer T, Hamdy T. Hypoglossal Facial Nerve Anastomosis for Post-Operative and Post-TraumaticComplete Facial Nerve Paralysis. Open Access Macedonian Journal of Medical Sciences. 2019 Dec 15; 7(23):3984-3996.
• Raslan A et al. Brief ES Improves Functional Recovery after Femoral but not Facial Nerve Injury in Rats. The Anatomical Record. 2019;302: 1304-1313
• ChenN, ZhouM, HeL, ZhouD, LiN. Acupuncture for Bell's palsy.Cochrane Database of Systematic Reviews 2010, Issue 8.