Small-Diameter Implant Placement: A Case Report - Steven T
4
88 DENTALCETODAY.COM • SEPTEMBER 2013 INTRODUCTION How often do patients arrive at your office so dissatisfied with their lower denture that they are carrying it in their purse or shirt pocket? Whether it is a full or partial denture, a poorly fitting mandibular prosthetic can generate a variety of quality-of-life concerns. Fear of the denture becoming loose or falling out may lead to avoidance of certain foods as well as insecurities about laughing, smiling, or even talking. These issues can lead to changes in diet, avoidance of social situations, and isolation among this patient population. Treatment plans that call for implant-sup- ported prosthetics (ISP) can address the quali- ty-of-life concerns that stem from a poorly fit- ting denture, while providing patients the self-confidence and security they are seeking. Traditional implants can be a suitable choice for prosthetic retention; however, the use of small-diameter implants (SDIs) has expanded the patient base that is eligible for implant-retained prosthetic treatment. Im- portantly, studies demonstrate that survival rates between SDIs and their standard-width counterparts are similar, and that SDIs can be a suitable choice for prosthetic retention. 1 In an ideal situation, patients who present with denture-related concerns will have existing anatomy to facilitate the successful SDI osseointegration that can lead to a well-sup- ported prosthetic. However, fully or partially edentulous patients often do not demon- strate the bone width or quality that is need- ed. 2,3 Augmentation of existing bone is often necessary. In these cases, ridge augmentation via bone grafting can help generate addition- al high-quality bone structure. Background As documented in the dental literature, tra- ditional implants generally require approx- imately 6 mm of mandibular bone facial- lingually for successful osseointegration as well as 10 mm of bone height in the coro- nal-apical direction. 2,3 Small-diameter im - plants can be placed in as little as 3 to 4 mm of facial-lingual bone width with one mm of surrounding bone, as well as 10 mm of bone height in the coronal-apical direc- tion. 2,3 However, when a patient presents with a knife-edged mandib ular ridge, as well as concurrent insufficient bone to sup- port even SDIs, a well-structured treatment plan is needed that takes into account mandibular ridge alteration as well as bone augmentation. As demonstrated in the case report below, a combination of autologous harvested bone with allograft or xenograft bone granules can be used with a support- ing resorbable membrane to supplement existing bone structure. Surgically flatten- ing the knife-edged ridge creates a platform, providing sufficient bone width and sur- rounding bone structure to successfully maintain SDIs and their accompanying overdenture. The article to follow is the second in a series of 7 articles to appear in Dentistry Today; the first article, “Improving Existing Dentures With Mini Implants: Idealizing a Knife-Edged Mandibular Ridge,” was pub- lished in the magazine’s February 2013 issue. Future articles will address: (1) extraction of mandibular anterior teeth, modifying the interproximal bone, then immediate place- ment of SDIs in the interproximal bone fol- lowed by bone grafting/membrane place- ment, then fabrication of a lower denture; (2) placement of SDIs in a mandibular ridge with minimum vertical bone height; (3) SDI denture stabilization in the maxillary arch; (4) technique for relining dentures that con- tain implant housings; and (5) SDI utiliza- tion for removable partial stabilization. CASE REPORT Diagnosis and Treatment Planning A 65-year-old woman in excellent health with an unremarkable medical history pre- sented to our office carrying her mandibu- lar, 7-unit, anterior fixed partial denture (FPD) in her hand. She was mostly edentu- lous in the mandibular arch except for the abutment teeth that had retained the FPD as well as the remains of her left canine (Figure 1). Following a thorough clinical and radi- ographic examination, it was determined that the aforementioned teeth could not be saved. The patient, who coordinated prison ministries for a living with her husband, engaged frequently in public speaking and needed a prosthetic solution that prioritized function and stability. She was terrified of having a nonimplant-supported lower den- ture because of stories she had heard about lower denture instability; specifically, a friend of hers whose denture had fallen out of her mouth while she was laughing! Steven T. Cutbirth, DDS Small-Diameter Implant Placement: A Case Report Managing the Thin Knife-Edged Mandibular Ridge With Bone Grafting continued on page 90 Figure 1. Preoperative photo. Figures 2a and 2b. Patient presented with a knife-edged mandibular ridge. IMPLANTS a b dentalCEtoday.com Go online to earn credit for reading this CE article.* ce ce
Transcript of Small-Diameter Implant Placement: A Case Report - Steven T

88
DENTALCETODAY.COM • SEPTEMBER 2013
INTRODUCTIONHow often do patients arrive at your office sodissatisfied with their lower denture thatthey are carrying it in their purse or shirtpocket? Whether it is a full or partial denture,a poorly fitting mandibular prosthetic cangenerate a variety of quality-of-life concerns.Fear of the denture becoming loose or fallingout may lead to avoidance of certain foods aswell as insecurities about laughing, smiling,or even talking. These issues can lead tochanges in diet, avoidance of social situations,and isolation among this patient population.Treatment plans that call for implant-sup-ported prosthetics (ISP) can address the quali-ty-of-life concerns that stem from a poorly fit-ting denture, while providing patients theself-confidence and security they are seeking. Traditional implants can be a suitable
choice for prosthetic retention; however, theuse of small-diameter implants (SDIs) hasexpanded the patient base that is eligible forimplant-retained prosthetic treatment. Im -portantly, studies demonstrate that survivalrates between SDIs and their standard-widthcounterparts are similar, and that SDIs can bea suitable choice for prosthetic retention.1 Inan ideal situation, patients who present withdenture-related concerns will have existinganatomy to facilitate the successful SDIosseointegration that can lead to a well-sup-ported prosthetic. However, fully or partiallyedentulous patients often do not demon-strate the bone width or quality that is need-ed.2,3 Augmentation of existing bone is oftennecessary. In these cases, ridge augmentationvia bone grafting can help generate addition-al high-quality bone structure.
BackgroundAs documented in the dental literature, tra-ditional implants generally require approx-imately 6 mm of mandibular bone facial-lingually for successful osseointegration aswell as 10 mm of bone height in the coro-nal-apical direction.2,3 Small-diameter im -plants can be placed in as little as 3 to 4 mmof facial-lingual bone width with one mmof surrounding bone, as well as 10 mm of
bone height in the coronal-apical direc-tion.2,3 However, when a patient presentswith a knife-edged mandib ular ridge, aswell as concurrent insufficient bone to sup-port even SDIs, a well-structured treatmentplan is needed that takes into accountmandibular ridge alteration as well as boneaugmentation. As demonstrated in the casereport below, a combination of autologousharvested bone with allograft or xenograftbone granules can be used with a support-ing resorbable membrane to supplement
existing bone structure. Surgically flatten-ing the knife-edged ridge creates a platform,providing sufficient bone width and sur-rounding bone structure to successfullymaintain SDIs and their accompanyingoverdenture. The article to follow is the second in a
series of 7 articles to appear in DentistryToday; the first article, “Improving ExistingDentures With Mini Implants: Idealizing aKnife-Edged Mandibular Ridge,” was pub-lished in the magazine’s February 2013 issue.Future articles will address: (1) extraction ofmandibular anterior teeth, modifying theinterproximal bone, then immediate place-ment of SDIs in the interproximal bone fol-lowed by bone grafting/membrane place-ment, then fabrication of a lower denture; (2)placement of SDIs in a mandibular ridgewith minimum vertical bone height; (3) SDIdenture stabilization in the maxillary arch;(4) technique for relining dentures that con-tain implant housings; and (5) SDI utiliza-tion for removable partial stabilization.
CASE REPORTDiagnosis and Treatment Planning
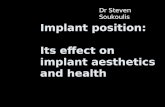
A 65-year-old woman in excellent healthwith an unremarkable medical history pre-sented to our office carrying her mandibu-lar, 7-unit, anterior fixed partial denture(FPD) in her hand. She was mostly edentu-lous in the mandibular arch except for theabutment teeth that had retained the FPD aswell as the remains of her left canine (Figure1). Following a thorough clinical and radi-ographic examination, it was determinedthat the aforementioned teeth could not besaved. The patient, who coordinated prisonministries for a living with her husband,engaged frequently in public speaking andneeded a prosthetic solution that prioritizedfunction and stability. She was terrified ofhaving a nonimplant-supported lower den-ture because of stories she had heard aboutlower denture instability; specifically, afriend of hers whose denture had fallen outof her mouth while she was laughing!
Steven T.Cutbirth, DDS
Small-Diameter ImplantPlacement: A Case Report
Managing the Thin Knife-Edged Mandibular Ridge With Bone Grafting
continued on page 90
Figure 1. Preoperative photo.
Figures 2a and 2b. Patient presented with a knife-edged mandibular ridge.
IMPLANTS
a
b
dentalCEtoday.comGo online to earn credit for reading this CE article.*
cece

IMPLANTS90
Finances were also a major concern. Inaddition to these concerns, the patientalso presented the clinical challenge ofa thin, knife-edged man dibular ridge(Figures 2a and 2b) with what wasdeemed to be insufficient bone to sup-port an implant. The recommendation to the pa -
tient was a solution that addressed bothfunctionality as well as financial con-cerns: extraction of the remaining man -dibular teeth and roots followed by fab-rication and placement of an SDI-stabi-lized removable denture. Due to thethin facial-lingual condition of theman dibular bone, however, the patientwas advised that bone grafting could berequired in order to provide adequatelong-term support for the SDIs andprosthetic. The patient, who was satis-fied with the condition of her maxillaryteeth and restorations, eagerly agreedand consented to the presented treat-ment plan for the mandibular arch.
Clinical ProtocolAt the patient’s next visit, the remain-ing lower teeth and roots were ex -tracted (Figure 3). Using a 15 Bard-Parker blade, an incision was madefrom cuspid to cuspid to expose themandibular ridge at the crest of theknife-edged bone. The incision wasextended apically in the first bicuspidarea (Figure 4). Avoiding the inferior
alveolar nerve exiting the mental fora-men, the alveolar bone was exposedby reflecting a full thickness gingivalflap apically along the complete ante-rior arch. The knife-edged ridge wasflattened with a coarse football dia-mond bur (No. 379-023 [BrasselerUSA]) (Figure 5) and rongiers. Thisbony ridge adjustment created a flatplatform for SDI placement. The foot-ball diamond can be used safely witheither high- or low-speed handpieces.High water volume and very lightpressure should be applied if a high-speed device is used. The SDIs do not have to align
exactly with each other upon place-ment, as their housings are designedto allow up to 30° of alignment varia-tion. A surgical guide is not necessary,but if the clinician is uncomfortablevisualizing implant alignment, a vac-uum-formed shim with surgical pilotdrill guide holes may be used to guideSDI placement. It is sometimes diffi-cult to utilize a surgical guide follow-ing gingival flap reflection and ridgemodification. The reflected flapmakes it difficult to seat the surgicalguide, and the bony ridge morphologyhas been changed following ridgemodification.As supported in the dental litera-
ture, four 1.8 x 13 mm SDIs wereplaced (MDI Mini Dental Implants[3M ESPE]) in the flattened ridge tosupport the patient’s denture, stayinganterior to the identified mental fora-
men and leaving at least 7 mm of sepa-ration between implants to accommo-date housings.2-5 Prior to insertion,small indentations were made in thecortical bone at the implant sites witha No. 4 round bur (Figure 6). Theseindentations serve as “stops” to pre-vent the pilot drill from sliding. Pilotholes were then drilled through thecortical plate approximately one quar-ter the length of the threaded implants(Figure 7). On a slow-speed contraangle handpiece connected to an elec-tric motor (AEU 7000 [Asep tico], 0.9%sterile NaCl IV bag [Baxter]), the pilotdrill was moved up and down at slow-to-moderate speed with high waterflow to avoid burning the bone. Each of the 4 SDIs was screwed in
sequentially before proceeding to thenext one. They were inserted first withthe plastic lid of the implant, followedby a finger driver, and finally with awinged thumb wrench (Figures 8a to8c). Figure 9 shows the 4 SDIs solidlyin place but with inadequate facial-coronal bone for long-term stability. Ifthe SDI can be placed completely withthe finger driver, it likely will notosseointegrate and will be lost. Incases where only the finger driver isneeded to completely insert the SDI,
the best course of action is to removethe implant and choose an alternatesite. Implant success rates are veryhigh when the winged thumb wrenchor torque wrench is required to secure-ly screw the SDI into place. Sometimesthere is insufficient vertical space forthe winged thumb wrench, and thetorque wrench, which requires lessspace, may be used to very slowlyscrew the SDI to place. Once placed, anSDI should “ting” and not “thud”when tapped with the handle end of amouth mirror. As was determined during the ini-
tial clinical examination, bone aug-mentation would be necessary in thefacial-coronal region of the lower alve-olar ridge. This augmentation wouldfacilitate successful SDI osseo in -tegration and support for the man -dibular prosthesis. A recent literaturereview by Clementini et al6 of 8 studiesduring the last 17 years demonstratescomparable success rates of implantsplaced in regenerated bone versus pris-tine bone. Also, a study by van der Meijet al7 indicates that an ISP will pre -dictably succeed in mandibular bonethat has underdone augmentation pro-cedures. For this patient, augmenta-
DENTALCETODAY.COM • SEPTEMBER 2013
Figure 3. Lower arch, following extraction ofteeth and roots.
Figure 7. Pilot holes were drilledthrough the cortical plate.
Figure 9. Four SDIs solidly in place but withinadequate facial-coronal bone for long-termstability.
Figure 4. Periodontal flap reflected andmandibular alveolar ridge exposed.
Figure 5. A coarse football diamond bur (No.379-023 [Brasseler USA]) was used to flatten the knife-edged ridge.
Figure 6. A No. 4 round bur was utilized tomake small indentations in the cortical boneto create “stops” for the pilot drill.
continued on page 92
a b c
Figures 8a to 8c. Small-diameter implants(SDIs) (MDI Mini Dental Implants [3M ESPE])were inserted with the plastic lid of theimplant (a), followed by a finger driver (b),and finally with a winged thumb wrench (c).
Small-Diameter Implant Placement...continued from page 88 The laboratory technician uses the housings on
the stone model to verify spacing and fit.

IMPLANTS92
tion was best accomplished utilizing acombination of autogenous bone har-vested from the patient’s chin andfreeze-dried xenograft bone granules.Using a sterile, disposable curved
cortical bone collector (SafescraperTwist [Osteogenics Biomedical]), can-cellous bone was carefully harvestedfrom the chin. The collected shavingsproduced are collected with coagulat-ed blood, and together they demon-strate the low density and porosityneeded for angiogenesis and integra-tion with existing bone (Figure 10).8The collected autologous bone andblood was supplemented with sterilexenograft bone granules (Bio-Oss[Geist lich Bioma terials]), a materialderived from the mineral portion ofbovine bone.9,10 After making multi-ple facial surface cortical plate perfo-rations with a No. 1 round bur to es -tablish bleeding points into the tra-becular bone, the bone graft mixturewas applied to the mandibular alveo-lar ridge (Figures 11a and 11b). A
resorbable mem brane (BioCellect[IMTEC, a 3M Com pany]) covered thegraft (Figure 12). It is important thatthe resorbable membrane have nomemory so it adheres to the shape ofthe bone graft. If the membrane isstiff, suturing the reflected flap overthe membrane will be difficult.The gingival tissue was sutured
passively back into place to coverand protect the bone graft and mem-brane (Figure 13). It is important thegingival flap be deeply reflected api-cally to facilitate passive suturing.Either 3-0 chromic gut (Angiotech) or5-0 poly propylene suture (Prolene[Ethicon 360]) can be used. Prolene isnot dissolvable and must be removedone to 2 weeks postplacement. If pro-lene is left in place much over oneweek the tissue will grow over thesuture, making it difficult to remove,even requiring local anesthesia.Chromic gut su ture dissolves in 1.5to 2 weeks, versus plain gut whichdissolves in 4 to 7 days.Throughout the following 4
months, the patient returned for brieffollow-up visits to check the condi-
tion of the graft, implants, and sur-rounding soft tissues. A chlorhexi-dine gluconate antimicrobial oralrinse (PerioGard [Colgate-Palmolive])was prescribed for patient use be -tween visits to help keep the implantsand tissue plaque free. Bone regenera-tion, osseointegration, and soft-tissuehealing continued without incident.At the patient’s 4-month visit, radi-ographic and clinical examinationrevealed healthy tissue and bonestructure, as well as implants that hadfully integrated with the regeneratedbone (Figures 14a and 14b). When theintegrated SDIs were tapped with amouth mirror handle the sound was“ting” and not “thud.” A customacrylic tray was fabricated for a finalim pression of the patient’s lowerarch. Micrometal housings with spac-ers were placed on the SDIs and pulledin the custom tray with polyetherimpression material (ImpregumPenta Soft [3M ESPE] (Figures 15a and15b). An arbitrary face-bow recordand centric relation occlusal registra-tion record at the estimated verticaldimension were taken for the lab.
Finalizing Denture Placement and Alignment
The laboratory technician uses thehousings on the stone model to verifyspacing and fit. Specifically, this stepensures there is adequate space in thedenture base to accommodate thehousings when they are seated on theSDIs and pulled in the mouth withhard acrylic pick-up material at thefinal denture delivery appointment.The laboratory sends the housings backto the dentist once final laboratory pro-cessing of the denture has taken place. It is indeed more trouble to “pull”
the housings in the mouth at the final
DENTALCETODAY.COM • SEPTEMBER 2013
Small-Diameter Implant Placement...continued from page 90
Figure 10. Bone and blood harvested with a(sterile disposable) curved cortical bone collector (Safescraper Twist [OsteogenicsBiomedical]).
Figures 14a and 14b. Clinical (a) and radiographic (b) examination revealed healthy tissueand bone structure as well as implant osseointegration at the 4-month follow-up visit.
Figures 11a and 11b. Cortical plate perforations followed by a mixture of autologous andxenograft bone graduals.
Figure 16. Final mandibular denture. Figure 17. Denture with housings and o-rings.
Figure 12. Resorbable membrane (BioCellect[IMTEC, a 3M Company]) in place to coverthe bone graft.
Figure 13. Gingival tissue sutured passivelyback into place.
a b
Figures 15a and 15b. Micrometal housings with spacers were placed on the SDIs (a) andpulled with polyether impression material that had been placed in the custom tray (b).
a b
a b
...this step ensures there is adequate space in the denturebase to accommodate the housings when they are seated on the SDIs....
Figure 18. The patient was pleased with thefinal outcome.

denture delivery appointment versusprocessing the housings into the den-ture base in the laboratory prior todelivery. The concern is that if the hous-ings are not pulled at the final appoint-ment and the denture is not relined inthe mouth, one cannot be certain all thehousings/o-rings are completely seatedon the SDIs or that the denture is in inti-mate contact with and supported by themandibular ridge. It is essential for thedenture base to be in intimate contactwith the mandibular ridge rather thanvertically supported by the SDIs, whichcould lead to fracturing of the prosthet-ic. The SDIs are intended to prevent hor-izontal and coronal movement of theprosthetic, not support apical load. Ifthe denture “pivots” on an im -plant/housing and is not apically sup-ported by the man dibular/maxillaryridge, then the den ture may fractureacross the implant.Following a “teeth in wax” ap -
pointment to verify teeth placement,the final mandibular denture withhousings and o-rings is pictured inFigures 16 and 17. Note: The patient inthis case declined treatment for her maxil-lary arch, and issues associated with natu-ral teeth opposing a denture, especiallywith implants, will be discussedin a forthcoming article.
DISCUSSIONSmall-diameter implants werechosen for this case because ofthe limited presenting hori-zontal bone, ease of SDI place-ment, and cost concerns. Priorexperience as well as an exam-ination of the dental literatureassured us the SDIs would ade-quately support the patient’sprosthetic. As part of our boneaugmentation procedure, wesupplemented the patient’sharvested bone with xenograftgranules due to their demon-strated biocompatibility andlong-term success in dentalprocedures that require aug-mentation.9,10As with all dental proce-
dures, it is important to pres-ent to patients a full treatmentplan and obtain informed writ-ten consent prior to the start oftherapy. Due to the longer-term nature of dental thera-pies such as the aforemen-tioned that involve implantosseointegration, bone aug-mentation, and tissue healing,patients should demonstratethe ability to physically and
psychologically tolerate in-office proce-dures and follow-up treatment, as wellas suggested at-home regimens to sup-port a successful outcome.
CLOSING COMMENTSFor patients presenting with a fullyedentulous lower arch, an SDI-retainedremovable denture can be a secure andfunctional prosthetic solution. Knife-edged ridges pose an additional clinicalchallenge, but can be easily altered, cre-ating a flat “platform” appropriate forSDI placement using the technique pre-sented in this article. When an edentu-lous patient presents with a knife-edgedridge as well as insufficient bone to sup-port an SDI, bone augmentation proce-dures may be necessary and can beaccomplished via autologous bone har-vesting, use of a bone substitute, or acombination of both along with aresorbable membrane barrier. Through use of the above proce-
dures, the patient in this article wasprovided a solution that restoredexcellent functionality, addressedquality-of-life concerns, and restoredthe self-confidence to continue with asuccessful career centered on min-istry and pu blic speaking. She is very
pleased with the final results (Figure18) of her treatment. After 2 years, sheremains confident and satisfied, say-ing that she is able to eat the foods sheenjoys, nev er worries about talking orlaughing, and never even thinksabout her lower denture rising up orfalling out of her mouth. The im -plants are still fully vi able: radiog -raphically bone appears to cover theimplant threads completely, and theystill “ting” versus “thud” when tappedby a metal mirror handle.�
References1. Sohrabi K, Mushantat A, Esfandiari S, et al. How
successful are small-diameter implants? A litera-ture review. Clin Oral Implants Res. 2012;23:515-525.
2. Christensen GJ. Ask Dr. Christensen. Dent Econ.2011;101(8):56.
3. Schoonover L. Predictable stabilization of a lowerdenture. Dent Today. 2012;31:80-83.
4. Erwood I. Denture stabilization with small-diame-ter implants. Dent Today. 2010;29:116-118.
5. Greenstein G, Tarnow D. The mental foramen andnerve: clinical and anatomical factors related todental implant placement: a literature review. JPeriodontol. 2006;77:1933-1943.
6. Clementini M, Morlupi A, Agrestini C, et al.Success rate of dental implants inserted in autol-ogous bone graft regenerated areas: a systemat-ic review. Oral Implantol (Rome). 2011;4:3-10.
7. van der Meij EH, Blankestijn J, Berns RM, et al.The combined use of two endosteal implants andiliac crest onlay grafts in the severely atrophicmandible by a modified surgical approach. Int JOral Maxillofac Surg. 2005;34:152-157.
8. Osteogenics Biomedical. Safescraper TWIST—
Curved version. osteogenics.com/v/product-group/Safescraper-TWIST-Curved-Version/vh.Accessed March 17, 2013.
9. Geistlich Biomaterials. Natural bone regenera-tion for a better quality of life. bio-oss.com.Accessed March 17, 2013.
10. Geistlich Biomaterials. Geistlich Bio-Oss—TheMaster’s Choice. geistlich.com/?dom=2&rub=42.Accessed March 17, 2013.
Dr. Cutbirth practices restorative dentistry inWaco, Tex (wacosedationdentist.com), and isdirector of the Center for Aesthetic RestorativeDentistry (CARD) (centerforard.com) located inDallas, Tex, a hands-on, complex restorativeteaching center for practicing dentists. Hegraduated from Baylor Dental College in 1979,then completed a 2-year oral surgery fel -lowship at Baylor, then was a member of theteaching faculty at the Pankey Institute inFlorida for 20 years. Dr. Cutbirth has lecturedand published extensively on the topics of sys-tematic restoration of the severely worn denti-tion with vertical dimension increase, diagno-sis and treatment of occlusal problems andfacial pain, complex aesthetic restorative den-tistry, ridge modification and bone grafting forsmall-diameter implant utilization, and themost effective/productive dental practice sys-tem. He can be reached at (254) 772-5420 orat [email protected].
Disclosure: Dr. Cutbirth is an occasional lectur-er for 3M ESPE but has received no compen-sation for the writing of this article.
*CEUs for this activity will not beaccepted by AGD for FAGD/MAGD creditas this activity was not developed inaccordance with AGD PACE standards.
IMPLANTS 93