Slip-knot suspension technique: A fail-safe microanastomosis for small-caliber vessels
3
The most common technical error associated with microvascular anastomotic failure is accidentally snagging the opposite wall and including it in the stitch, thereby reducing the vessel lumen diameter or occluding it altogether. A sim- ple, safe microsuturing technique is described that combines the use of the slip-knot and the suspension technique in a procedurethat allows direct visual inspection of suture placement from first to last stitch. This technique is ap- plicable to end-to-end and end-to-side microvascular anastomoses, for thick- walled ducts such as the vas deferens and the fallopian tube, and in laparo- scopic suturing. MICROSURGERY 13:lOO-102 1992 SLIP-KNOT SUSPENSION TECHNIQUE: A FAIL-SAFE MICROANASTOMOSIS FOR SMALL-CALIBER VESSELS ZOLTAN SZABO, Ph.D., LUDOVICO STELLINI, M.D., ELLIOTT H. ROSE, M.D., MARK S. ELLIS, D.P.M., and BUFORD H. BURCH, M.D. T h e success of a microvascular anastomosis is highly de- pendent on technical skill, use of atraumatic technique, op- timal visualization, fine instruments, and sutures. However, under less than optimal conditions, whether due to surgical inexperience, poor instrumentation, or a compromised sur- gical field, the slip-knot suspension technique is advanta- geous in that it allows for avoidance or correction of tech- nical errors and therefore increases the chances for a successful anastomosis. Anastomotic failure may be caused by many factors. The most common technical error leading to failure is com- plete or partial occlusion of the vessel lumen by including a portion of the posterior vessel wall in an anterior stitch, i.e., “catching the back wall.”’ This type of error is often caused by “blind stitch” placement. The slip-knot suspension technique is less complex than similar anastomotic and allows visualization of the vascular lumen from first to last stitch, eliminating the need to place the last stitches of the anastomosis blindly. The last few stitches are left in a loose suture loop and are tied securely but are not cinched down (Fig. 1). Inspection is possible, and incorrectly placed sutures can simply be From the Microsurgical Research Institute, San Francisco, CA (Z.S.); lstituto Ortopedico Toscano, Florence, Italy (L.S.); Division of Plastic and Reconstruc- tive Surgery, Department of Plastic Surgery, Mount Sinai Medical Center, New York, NY (E.H.R.); Riverside, CA (M.S.E.);Department of Surgery, Tulane University School of Medicine, New Orleans, LA and Veterans Administration Medical Center, Alexandria, LA (B.H.B.). Acknowledgments: The authors express their appreciation to Albert Rath, MD, for his insightfulness. Address reprint requests to Zoltan Szabo, PhD, FICS, at the Microsurgical Research Institute, 153 States Street, San Francisco, CA 94114. Received for publication September 18, 1991; revision accepted October 28. 1991. removed and replaced. The stitches can be cinched down to approximate tissue edges properly by converting the square knot to its adjustable configuration, sliding it into position and relocking it. MATERIALS AND METHODS Sprague-Dawley rats, males (450-500 g) and females (350-400 g), were anesthetized, and the femoral arteries and veins were dissected and prepared, in the usual fashion using atraumatic technique^.^ In the slip-knot suspension technique for both end-to- end and end-to-side anastomoses, vessels are sutured in a fashion that approximates one-half of the vessel circumfer- ence, leaving the remaining one-half open to inspect for error. If an offending stitch is found, it is replaced properly. END-TO-END MICROANASTOMOSIS (FIG. 2A-F)’-’ Stitches were placed, in the standard fashion, at the 12, 6, 3, 4, and 5 o’clock positions of the vessel., completing the first half.’ The vessel was rotated 180” and the lumenal surface was inspected for technical errors, in particular the snagging of an intimal surface. If any offending stitches were detected, they were excised and replaced properly prior to continuing. The remaining half of the vessel was sutured in the same fashion as the first half, with one ex- ception. Instead of tying the stitches down, they are tied, with the normal square knot, leaving a loose suture loop (1-2 mm). The vessel lumen was then checked for stitches that may have caught the posterior wall. If any were found, they were corrected. After thorough inspection, the pretied square knots were then converted to the adjustable configuration referred to as the “slip-knot” (Fig. 2A, B) and the suture 0 1992 Wiley-Liss, Inc.
-
Upload
zoltan-szabo -
Category
Documents
-
view
213 -
download
1
Transcript of Slip-knot suspension technique: A fail-safe microanastomosis for small-caliber vessels

The most common technical error associated with microvascular anastomotic failure is accidentally snagging the opposite wall and including it in the stitch, thereby reducing the vessel lumen diameter or occluding it altogether. A sim- ple, safe microsuturing technique is described that combines the use of the slip-knot and the suspension technique in a procedure that allows direct visual inspection of suture placement from first to last stitch. This technique is ap- plicable to end-to-end and end-to-side microvascular anastomoses, for thick- walled ducts such as the vas deferens and the fallopian tube, and in laparo- scopic suturing.
MICROSURGERY 13:lOO-102 1992
SLIP-KNOT SUSPENSION TECHNIQUE: A FAIL-SAFE MICROANASTOMOSIS FOR SMALL-CALIBER VESSELS ZOLTAN SZABO, Ph.D., LUDOVICO STELLINI, M.D., ELLIOTT H. ROSE, M.D., MARK S. ELLIS, D.P.M., and BUFORD H. BURCH, M.D.
T h e success of a microvascular anastomosis is highly de- pendent on technical skill, use of atraumatic technique, op- timal visualization, fine instruments, and sutures. However, under less than optimal conditions, whether due to surgical inexperience, poor instrumentation, or a compromised sur- gical field, the slip-knot suspension technique is advanta- geous in that it allows for avoidance or correction of tech- nical errors and therefore increases the chances for a successful anastomosis.
Anastomotic failure may be caused by many factors. The most common technical error leading to failure is com- plete or partial occlusion of the vessel lumen by including a portion of the posterior vessel wall in an anterior stitch, i.e., “catching the back wall.”’ This type of error is often caused by “blind stitch” placement.
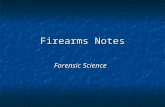
The slip-knot suspension technique is less complex than similar anastomotic and allows visualization of the vascular lumen from first to last stitch, eliminating the need to place the last stitches of the anastomosis blindly. The last few stitches are left in a loose suture loop and are tied securely but are not cinched down (Fig. 1). Inspection is possible, and incorrectly placed sutures can simply be
From the Microsurgical Research Institute, San Francisco, CA (Z.S.); lstituto Ortopedico Toscano, Florence, Italy (L.S.); Division of Plastic and Reconstruc- tive Surgery, Department of Plastic Surgery, Mount Sinai Medical Center, New York, NY (E.H.R.); Riverside, CA (M.S.E.); Department of Surgery, Tulane University School of Medicine, New Orleans, LA and Veterans Administration Medical Center, Alexandria, LA (B.H.B.).
Acknowledgments: The authors express their appreciation to Albert Rath, MD, for his insightfulness.
Address reprint requests to Zoltan Szabo, PhD, FICS, at the Microsurgical Research Institute, 153 States Street, San Francisco, CA 94114.
Received for publication September 18, 1991; revision accepted October 28. 1991.
removed and replaced. The stitches can be cinched down to approximate tissue edges properly by converting the square knot to its adjustable configuration, sliding it into position and relocking it.
MATERIALS AND METHODS Sprague-Dawley rats, males (450-500 g) and females
(350-400 g), were anesthetized, and the femoral arteries and veins were dissected and prepared, in the usual fashion using atraumatic technique^.^
In the slip-knot suspension technique for both end-to- end and end-to-side anastomoses, vessels are sutured in a fashion that approximates one-half of the vessel circumfer- ence, leaving the remaining one-half open to inspect for error. If an offending stitch is found, it is replaced properly.
END-TO-END MICROANASTOMOSIS (FIG. 2A-F)’-’
Stitches were placed, in the standard fashion, at the 12, 6, 3, 4, and 5 o’clock positions of the vessel., completing the first half.’ The vessel was rotated 180” and the lumenal surface was inspected for technical errors, in particular the snagging of an intimal surface. If any offending stitches were detected, they were excised and replaced properly prior to continuing. The remaining half of the vessel was sutured in the same fashion as the first half, with one ex- ception. Instead of tying the stitches down, they are tied, with the normal square knot, leaving a loose suture loop (1-2 mm).
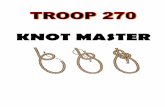
The vessel lumen was then checked for stitches that may have caught the posterior wall. If any were found, they were corrected. After thorough inspection, the pretied square knots were then converted to the adjustable configuration referred to as the “slip-knot” (Fig. 2A, B) and the suture
0 1992 Wiley-Liss, Inc.

Slip-Knot Suspension Technique 101
allows for inspection of any or all stitches prior to comple- tion of the anastomosis. None of the stitches is placed blindly, which improves the chances for success. This is especially important under less than optimal clinical situa- tions.
FAIL-SAFE SUTURING Suspension - Slip-knot technique
Second
Open
> 1.2 rnrn O.D.
First Side
Closed
Figure 1. Suspension slip-knot technique, using loose suture loops that are tied but not cinched down, allowing direct visual inspection of all stitches.
loop was cinched down to approximate the vessel edges (Fig. 2C, D). The slip-knot was then reconverted to its locking configuration (square knot), and the stitch was completed (Fig. 2E, F). Additional flat knots could be placed for added security in thick walled vessels or other ducts.''-'*
END-TO-SIDE ANASTOMOSIS End-to-side anastomoses are accomplished following
the same procedure as that for end-to-end anastomoses.
CONCLUSIONS The slip-knot suspension technique is a simple suturing
technique that utilizes the common square knot. The con- vertibility of the square knot into the slip-knot configuration saves the time and effort involved in untied stay sutures. With the new technique, the stitches are already tied and need only to be cinched down and relocked. The technique
REFERENCES 1. Lidman D, Daniel RK: Evaluation of clinical microvascular anasto-
moses-reasons for failure. Ann Plast Surg 6:2 15, 198 I . 2. Harris GD, Finseth F, Buncke HJ: Posterior-wall-first microvascular
anastomotic technique. Br J Plast Surg 34:47, 1981. 3. Berggren A, Ostrup LT, Lindman, D: Mechanical anastomosis of
small arteries and veins with the unilink apparatus: A histologic and scanning electron microscopic study. Plast Reconstr Surg 80271, 1987.
4. Chen L, Chiu D: Spiral interrupted suturing technique for microvas- cular anastomosis: a comparative study. Microsurgery 7:72, 1986.
5 . Buncke HJ, Chater NL, Szabo Z: The Laboratory Manual of Mi- crovascular Surgery. Wayne, NJ: Davis & Geck, 1975.
6. Szabo 2: Suspension technique for anastomosis of one millimeter blood vessels. Paper presented at the Second Annual International Congress for the Workshop on Laparoscopy and Microsurgical Repair of the Fallopian Tube, American Association of Gynecologic Lap- aroscopists, University of California, Irvine, April, 1978.
7. Szabo Z: Suspension technique for microvascular anastomosis. Paper presented at the IVe Recontre Internationale de Microchirugie, Lyon, France, May, 1978.
8. Szabo Z: Deep anastomotic techniques. Paper presented at the Micro- neurosurgery at the Base of the BrainSecond Workshop and Sym- posium, Microsurgical Research Institute and Bellevue Hospital & Medical Center (NYU), New York, September, 1984.
9. Szabo Z: Microvascular surgical technique today, in Phillips JM (ed): Microsurgery in Gynecology. Downey , CA, American Association of Gynecologic Laparoscopists, 1977, pp 145-152.
10. Szabo Z: Laboratory animal models for microsurgery-Technique for vascular anastomosis and vas deferens anastomosis. Paper presented at the American Association of Laboratory Animal Science Annual Meeting, Anaheim, CA, October, 1977.
11. Szabo Z: Suspension technique for infertility microsurgery. Paper pre- sented at the XXII Congress of the Hungarian Society for Obstetrics and Gynecology, Szeged, Hungary, September, 1984.
12. Estes JM, Longaker MT, Whitby DJ, Lorenz HP, Szabo Z, Adzick NS, Harrison M R Endoscopic creation and repair of fetal cleft lip. Plasi Reconstr Surg (in press).

102 Szabo et al.
Figure 2. A: Square knot being converted to its adjustable slipping configuration. 6: Conversion completed (from the square knot to the slip knot). C: Slip-knot being tightened. D: Slip-knot now cinched down. E: Slip-knot now being reconverted to the square knot. F: Reconversion completed (from the slip knot to the square knot).