
Slide Pediatric Tuberculosis
112
Pediatric Tuberculosis 9/20/2010 1
-
Upload
fenny-rahmadani -
Category
Documents
-
view
17 -
download
3
description
slide
Transcript of Slide Pediatric Tuberculosis

Pediatric Tuberculosis
9/20/2010 1

Definition
Tuberculosis is a disease due to Mycobacterium tuberculosisinfection with systemic spread thus
9/20/2010 2
infection with systemic spread thus can affect almost all organs, and the most frequent site is in the lung, which usually as the site of primary infection

Tuberculosis
The reaction of the tissues of the human host to the presence and multiplication of
9/20/2010 3
human host to the presence and multiplication of Mycobacterium tuberculosis or Mycobacterium bovis

History
• ancient Egypt : gibbus
• 1882, Koch, identification
• management : sanatorium, collapse treatment
9/20/2010 4
treatment
• Chemotherapy :– PAS – 1943 – Lehmann
– Streptomycine – 1945 - Waksman & Schats
– Isoniazid – 1952 – Domagk
– Rifampicine - 1957

Magnitude of problem
• TB one of the oldest diseases of human
• remains one of the deadliest diseases in the world
• 8 million of new cases yearly
9/20/2010 5
• 8 million of new cases yearly
• 3 million death yearly
• 20-40% population is infected
• reemergence, global emergency
The secret
Why TB is so strong and robust?
• the secret: specific characters of the bacilli
9/20/2010 6
• special issues:
hematogenic spread
infection vs disease
primary vs post-primary

The main problems
• Diagnosis
– Clinical manifestations : not specific �
both over/under diagnosis & over/under treatment
9/20/2010 7
– diagnostic specimen : difficult to obtain
– TB infection or TB disease ? � no
diagnostic tool to distinguish
• Adherence / compliance
– Drug discontinuation � treatment failure

Etiology
9/20/2010 8
Etiology

The bacilli• Mycobacterium tuberculosis• Mycobacterium bovis
features:
� slender, often slightly curved, rods
9/20/2010 9
� aerobic, non-motile, non-spore forming
� acid fail to wash the stain out � acid fast bacilli
�Mycobacteria : found in environments, some strictly human pathogen (M tb, bovis), others animal pathogen and opportunistic pathogens in human (atypical mycobacteria)

TB bacilli
9/20/2010 10
TB bacilli

M tuberculosisCharacteristics :
1. live in weeks in dry condition
2. no endotoxins, no exotoxins
3. hematogenic spread
9/20/2010 11
3. hematogenic spread
4. grows slowly (24-32 hr)
5. non specific clinical manifestation
6. aerob, organ predilection - lung
7. wide spectrum of replication: dormant

Transmission
9/20/2010 12
Transmission

Transmission ...
• airborne human to human transmission by droplet nuclei
• adult pulmonary TB: cough, sneeze, speak, or sing
9/20/2010 13
sing
• droplet nuclei : contain 2-3 bacilli, small size (1-5µ) keep in the air for long period
• inhalation, reach alveoli
• middle and lower lobes

TB droplet nuclei
9/20/2010 14

Transmission factors:
• doses / numbers
• concentration in the air
• virulence
9/20/2010 15
• virulence
• exposure duration
• host immune state

Infection source
• Known source of infection, has
diagnostic value
• Shaw (1954), level of infectiousness :
9/20/2010 16
• Shaw (1954), level of infectiousness :– AFB (+) : 62.5 %
– AFB (-), M tb (+) : 26.8 %
– AFB (-), M tb (-) : 17.6 %

Transmission rate (Shaw ’54)
adultTB patient
9/20/2010 17
AFB(+)AFB(-)
culture(+)culture(-)CXR (+)
65% 26% 17%

Pathogenesis
9/20/2010 18
Pathogenesis

Location of primary focus
in 2,114 cases, 1909-1928
Location %Lung 95.93
Intestine 1.14
Skin 0.14
9/20/2010 19
Skin 0.14
Nose 0.09
Tonsil 0.09
Middle ear (Eustachian tube) 0.09
Parotid 0.05
Conjunctiva 0.05
Undetermined 2.41

droplet nuclei inhalation
alveoli ingestion by PAM’S
intracellular replicationof bacilli
destructionof bacillidestruction of PAM’S
Tubercle formation Hilar lymph nodesLymphogenic spread
primary focus lymphangitis lymphadenitis
9/20/2010 20Figure. Pathogenesis of primary tuberculosis
hematogenic spread
multiple organs remote focidisseminated primary TB
acute hematogenicspread
occult hematogenicspread
primary
complex
CMI

Incubation period
• first implantation � primary complex
• 4-6 weeks (2-12 weeks) � incubation period
• first weeks: logaritmic growth, : 103-10
4 �
elicit cellular response
9/20/2010 21
elicit cellular response
• end of incubation period:
– primary complex formation
– cell mediated immunity
– tuberculin sensitivity
�������� PrimaryTB infection has established

lymphadenitis
lymphangitis
Pathogenesis ...Pathogenesis ...
9/20/2010 22
primary focus

Hematogenous spread
• during incubation period, before TB infection establishment:
– lymphogenic spread
– hematogenic spread
9/20/2010 23
–hematogenic spread
• hematogenic spread (HS):
–occult HS
–acute generalized HS

Occult HS
• most common
• sporadic, small number
• no immediate clinical manifestation
• remote foci in almost every organ
9/20/2010 24
• remote foci in almost every organ
• rich vascularization: brain, liver, bones & joints, kidney
• including: lung – apex region
• CMI (+): silent foci - dormant, potential for reactivation

TB hematogenous spread
9/20/2010 25

Acute HS
• less common
• large number
• immediate clinical manifestation: disseminated TB
9/20/2010 26
disseminated TB
• milliary TB, meningitis TB
• tubercle in same size, special appearance in CXR

Miliary TB
9/20/2010 27
Miliary TB

Primary complex
• end of incubation period
• TB infection establishment
• tuberculin sensitivity (DTH)
• cell mediated immunity
9/20/2010 28
• cell mediated immunity
• end of hematogenic spread
• end of TB bacilli proliferation
• small amount, live dormant in granuloma
• new exogenous TB bacilli: destroyed / localized

Tuberculin skin test
9/20/2010 29
Tuberculin skin test

Tuberculin test
TB infection
cellular immunity
9/20/2010 30
delayed type hypersensitivity
tuberculin reaction

Tuberculin
StrengthPPD S
SeibertPPD RT23
first 1 TU 1 TU
9/20/2010 31
first 1 TU 1 TU
intermediate(standard dose)
5-10 TU 2-5 TU
second 250 TU 100 TU

Tuberculin delivery
1. Mantoux : intradermal injection
2. Multiple puncture :
9/20/2010 32
• Heaf, special apparatus with 6 needles
• Tine, disposable, 4 needles
3. Patch test

Tuberculin
Mantoux 0.1 ml PPD intermediate strength
location : volar lower arm
reading time : 48-72 h post injection
measurement : palpation, marked, measure
9/20/2010 33
report : in millimeter, even ‘0 mm’
Induration diameter :
� 0 - 5 mm : negative
� 5 - 9 mm : doubt
� > 10 mm : positive

Mantoux
tuberculin
9/20/2010 34
tuberculin
skin test

9/20/2010 35

9/20/2010 36

9/20/2010 37

Pengukuran Uji tuberkulin
9/20/2010 38

9/20/2010 39

Tuberculin positive
1. TB infection :
� infection without disease / latent TB infection
� infection and disease
9/20/2010 40
� infection and disease
� disease, post therapy
2. BCG immunization
3. Infection of Mycobacterium atypic

AnergiPatient with primary complex do not give reaction to TST due to supression of CMI :
• Severe TB: miliary TB, TB meningitis
• Severe malnutrition
• Steroid, long term use
9/20/2010 41
• Steroid, long term use
• Certain viral infection: morbili, varicella
• Severe bacterial infection: typhus abdominalis, diphteria, pertussis
• Viral vaccination: morbili, polio
• Malignancy: Hodgkin, leukemia, ...

TB infection & TB disease
• TB infection: CMI can control infection
– primary complex
– tuberculin sensitivity (DTH)
– cell mediated immunity
9/20/2010 42
– cell mediated immunity
– no clinical or radiological manifestation
• TB disease: CMI failed to control TB infectionTB infection + clinical and/or radiological manifestation

TB classification (ATS/CDC modified)
Class Contact Infection Disease Manage ment
0 - - - -
1 - -
9/20/2010 43
1 + - - proph I
2 + + - proph II?
3 + + + therapy

TB Natural history overviewprimary TB infection
primary TB disease latent infection
9/20/2010 44
no diseasepost primary TB
respiratory TBnon respir TB
new infection

Pathology
9/20/2010 45
Pathology

Pathology
• complicated pathogenesis �varied pathology
�clinical manifestation
�radiologic appearance
9/20/2010 46
�radiologic appearance
• lung represent
• tubercle, granuloma, tuberculoma, fibrosis, fistula, cavity, atelectasis
• complication of primary focus: so many possibilities

Lesions of pulmonary TB
• Parenchym: primary focus, pneumonia, atelectasis, tuberculoma, cavitary
• Lymph node: hilar, paratracheal, mediastinal
• Airway: air trapping, endobronchial TB,
9/20/2010 47
• Airway: air trapping, endobronchial TB, bronchial stenosis, fistula, bronchiectasis
• Pleura: effusion, fistula, empyema, pneumothorax, hemothorax
• Blood vessels: milliary, hemorrhage

tubercle formationresolution
primary focus
PathologyPathology
remote focireg lymph node
milliary seed
9/20/2010 48
calcification
2nd lung lesions
caseation
liquefaction
granuloma
tuberculoma
cavity
erodes airway
compresses airway
rupt to pleura rupt to airway bronchiectasis
fibrosis
br pl fistula

Clinical
9/20/2010 49
Clinical

Clinical types of pediatric TB
• Infection: TST (+), clinical (-), radiographic (-)
• Disease:– Pulmonary:
• primary pulmonary TB
• milliary TB
• pleuritis TB
9/20/2010 50
• pleuritis TB
• progr primary pulm TB: pneumonia, endobr TB
– Extrapulmonary:• lymph nodes
• brain & meninges
• bone & joint
• gastrointestinal
• other organs

Clinical manifestation
• vary, wide spectrum
• factors:
– TB bacilli: numbers, virulence
9/20/2010 51
– TB bacilli: numbers, virulence
– host: age, immune state
• clinical manifestation
– general manifestation
– organ specific manifestation

General manifestation
• chronic fever, subfebrile
• anorexia
• weight loss
9/20/2010 52
• weight loss
• malnutrition
• malaise
• chronic recurrent cough, think asthma!
• chronic recurrent diarrhea
• others

Organ specific
• Respiratory : cough, wheezing, dyspnea
• Neurology : convulsion, neck stiffness,
SOL manifestation
• Orthopedic : gibbus, crippled
9/20/2010 53
• Orthopedic : gibbus, crippled
• Lymph node : enlarge, scrofuloderma
• Gastrointestinal: chronic diarrhea
• Others

9/20/2010 54

9/20/2010 55

9/20/2010 56

9/20/2010 57

9/20/2010 58

9/20/2010 59

9/20/2010 60

Complications of focus
1. Effusion
2. Cavitation
3. Coin shadow
Complications of nodes
1. Extension to bronchus
2. Consolidation
3. HyperinflationMENINGITIS OR MILIARY
in 4% of children infected
under 5 years of ageLATE COMPLICATIONS
Renal & SkinMost after 5 years
BRONCHIAL EROSION
Most children
become tuberculin
sensitive
3-9 months
9/20/2010 61Miller FJW. Tuberculosis in children, 1982
A minority of children
experience :
1. Febrile illness
2. Erythema Nodosum
3. Phlyctenular Conjunctivitis 1 2 3 4 5 6
BONE LESIONMost within
3 years
24 months
Resistance reduced :
1. Early infection
(esp. in first year)
2. Malnutrition
3. Repeated infections :
measles, whooping cough
streptococcal infections
4. Steroid therapy
infection
12 months
DIMINISHING RISK
But still possible
90% in first 2 yearsGREATEST RISK OF LOCAL & DISEMINATED LESIONS
Development Of Complex
4-8 weeks 3-4 weeks fever of onset
PRIMARY COMPLEXProgressive HealingMost cases
Uncommon under 5 years of age25% of cases within 3 months75% of cases within 6 months
3-9 monthsIncidence decreasesAs age increased

Pemeriksaan mikrobiologis
• Memastikan D/ TB
• Hasil negatif tidak menyingkirkan D/ TB
• Hasil positif : 10 - 62 % (cara lama)
9/20/2010 62
• Hasil positif : 10 - 62 % (cara lama)
• Cara :
– cara lama,
– radiometrik,
– PCR

Radiology, serology , ...
9/20/2010 63
Radiology, serology , ...

Imaging diagnostic
• routine : chest X ray
• on indication : bone, joint, abdomen
• majority of CXR non suggestive TB
9/20/2010 64
• majority of CXR non suggestive TB
• pitfall in TB diagnostic

Radiographic picture
• primary complex: lymph node enlargement
• milliary
• atelectasis
• cavity
9/20/2010 65
• cavity
• tuberculoma
• pneumonia
• air trapping - hyperinflation
• pleural effusion
• honeycombs – bronchiectasis
• calcification, fibrosis

do not always help, particularly in small childrenat times can be confusing
some cases: extensive disease from radiography � clinical exam revealed little or nothing
Radiographic picture
9/20/2010 66
� clinical exam revealed little or nothing
more confusing � superadded bacterial
pneumonia (+)
Osborne CM et.al. Arch Dis Child 1995;72:369-74

• No radiographic picture is typical of TB
• Many lung diseases have similar radiographic appearances mimicking PTB
• Cannot distinguish active pulmonary TB –inactive PTB – previously treated TB
Radiographic picture
9/20/2010 67
inactive PTB – previously treated TB
• May not detect early stages of TB disease– under-reading
– over-reading
– intra-individual inconsistency
Vijayan VK. Indian J Clin Biochem 2002;17(2):96-100.

Commonly found: enlargement of hilar/paratracheal nodes � sometimes difficult to interpret � requires thorax CT with contrast
Radiographic picture
9/20/2010 68
Thorax CT reveals enlargement of lymph node in 60% children with TB infection and normal Chest röntgenogram
Delacourt C et.al. Arch Dis Child 1993;69:430-2.

100
60
80
100
Over diagnosis TB by CXR
Over-diagnosis
9/20/2010 69
32
0
20
40
Diagnosed by X-
ray alone
Actual cases

Sensitivity: 19 – 68%
Specificity: 40 – 98%
Disadvantages
Depends on:Type of antigen usedType of infection
Serology
9/20/2010 70
Disadvantages
results affected by factors such as
- age
- history of BCG vaccination
- exposure to atypical Mycobacteria
- unable to differentiate between infection and disease
Khan EA and Starke JR. Emerg Infect Dis 1995;1:115-23.
Polymerase chain reaction
• PCRPCRPCRPCRfrom gastric aspirate ���� diagnosis of TB in children Sensitivity: 44 – 90%Specificity: 94 – 96,8%Compared to MTB culture
9/20/2010 71
Compared to MTB cultureLodha R et.al. Indian J Pediatr 2004;71:221-7.
PCR technique using primer containing IS6110 ����better results
Khan EA and Starke JR. Emerg Infect Dis 1995;1:115-23.
May help in early detection of resistant strain of MTBLodha R et.al. Indian J Pediatr 2004;71:221-7.

• Detection of interferon- γ (QuantiFERON-TB)
comparable with TST to detect latent TB infection
Advantages- less affected by BCG vaccination- can discriminates responses due to nontuberculous
Interferon γ
9/20/2010 72
- can discriminates responses due to nontuberculous mycobacteria
- avoids variability and subjectivity associated with placing and reading TST
The utility of QFT in predicting the progression to active TB has not been evaluated
Mazurek GH et.al. MMWR Dispatch 2002;51.

Diagnosis
9/20/2010 73
Diagnosis

Prognostic factors
A. TB bacilli :– virulence
– infection dose
B. Patient :– general condition
9/20/2010 74
– general condition
– age
– nutritional state
– coinfection: morbili, pertussis
– genetic
– stress; physically (trauma, surgery) or mentally

The main problems
• Diagnosis– Clinical manifestations : not specific �both over/under diagnosis & over/under treatment
– diagnostic specimen : difficult to obtain
9/20/2010 75
– diagnostic specimen : difficult to obtain
– No other definitive diagnostic tools
– TB infection or TB disease ? � no diagnostic tool to distinguish
• Adherence / compliance– Drug discontinuation � treatment failure

Diagnosis1. Tuberculin skin test
2. Chest X ray
3. Clinical manifestation
4. Microbiologic
9/20/2010 76
5. Pathology
6. Hematological
7. Known infection source
8. Others : serologic, lung function, bronchoscopy

Clinical setting management
Suspect TB
proveTB
Mantoux test
9/20/2010 77
proveTB infection positive negative
not TB
Seek other etiologies
completed: Ro, labDiagnosis TB
treatment

Practical clinical approach to Ped TB
• Scoring system
�Stegen, 1969
�Smith, Marquis, 1981
9/20/2010 78
�Migliori dkk, 1992
�WHO, 1994
• Algorithm
�IDAI, 1998, 2002

Algorithm for Early Detection and Referral for Childhood
Tuberculosis in Indonesia
Suspected TB:• Close contact with adult with AFB sputum (+) • Early reaction of BCG (in 3-7 days)• Weight loss with no apparent cause, or underweight with no
improvement in 1 month with adequate nutritional support (failure to thrive)
• Prolonged/recurrent fever with no apparent cause• Cough more than 3 weeks
9/20/2010 79
• Cough more than 3 weeks• Specific enlargement of superficial lymph node• Scrofuloderma• Flychten conjunctivitis• Tuberculin test positive (> 10 mm)• Radiological findings suggestive TB
If > 3 positive Next page

Considered TB
Give anti-TB therapyObservation in 2 months
Clinical response (+) No clinical response/worsening
TB
Continue anti-TB therapy
Not TB MDR TB
Refer to hospital
9/20/2010 80
Continue anti-TB therapy Refer to hospital
Reevaluation in Referral Hospital:Clinical signsTuberculin testRadiological findingsMicrobiology and serology examinationHistopatology examinationDiagnostic procedure and therapy according to each hospital’s protocol
ATTENTIONPresence of any dangerous signs:• Seizure• Decreased level of consciousness• Neck stiffnessOr signs such as:• Spinal tumor/lump• Limping • Dam board phenomenon � Send to hospital UKK Pulmonologi –IDAI. Jakarta;2002.

Encountered problem
• Increasing demands of TB drugs for Pediatric TB
• Increasing diagnosis of Pediatric
9/20/2010 81
TB using the IDAI algorhitm
• Over diagnosis ?
• Need improvement � IDAI scoring system

Proposed IDAI scoring system
Feature 0 1 2 3 Score
Contact not clear reported, AFB(-)
- AFB(+)
TST - - - positive
BW (KMS) - <red line, BW�
severe malnutrition
-
9/20/2010 82
BW� malnutrition
Fever - unexplained - -
Cough <3weeks >3weeks - -
Node enlargemnt
- >1 node, >1cm,painless
- -
Bone,joint - swelling - -
CXR normal sugestive - -

Notes for IDAI scoring system• Diagnosis by doctor
• BW assessement at present
• Fever & cough no respons to standard tx
• CXR is NOT a main diagnostic tool in children
• All accelerated BCG reaction should be evaluated
9/20/2010 83
• All accelerated BCG reaction should be evaluated with scoring system
• TB diagnosis total score >5
• Score 4 in under5 child or strong suspicion, refer to hospital
• INH prophylaxis for AFB(+) contact with score <5

Diagnosis of TB in children
• If you find the diagnosis of TB in children easy, you probably overdiagnosing TB
• If you find the diagnosis of TB in children difficult, you are not alone
9/20/2010 84
difficult, you are not alone
• It is easy to over-diagnose TB in children
• It is also easy to miss TB in children
• Carefully assess all the evidence, before making the diagnosis
Anthony Harries & Dermot Maher, 1997

Treatment
9/20/2010 85
Treatment

Objectives of treatment
• Rapid reduction of the number
of bacilli
9/20/2010 86
• Preventing acquired drug
resistance
• Sterilization to prevent relapses

Treatment principles
• Drug combination, not single drug
• Two phases :
9/20/2010 87
� Initial phase (2 months) – intensive, bactericidal effect
� Maintenance phase (4 months / more) – ‘sterilizing’ effect, prevent relaps

Smear +Culture +
108
107
106
105
Sensitive organisms Resistant organisms
Nu
mb
er
of
bacil
li p
er
ml
of
sp
utu
m
The ‘fall and rise’ phenomenon
9/20/2010 88
Smear -Culture +
Smear -Culture -
104
103
102
101
100
Start of treatment(isoniazid alone)
Weeks of treatment
0 3 6 9 12 15 18 WHO 78351
Nu
mb
er
of
bacil
li p
er
ml
of
sp
utu
m
Toman K, Tuberculosis, WHO, 1979

Treatment principles
• Long duration � problem of
adherence (compliance)
• Other aspects :
9/20/2010 89
• Other aspects :
�Nutrition improvement
� prevent / search & treat other disease

Hypothetical model of TB therapy
A
B
Pop A = rapidly multiplying (caseum)
Pop B = slowly multiplying (acidic)
Pop C = sporadically multiplying
9/20/2010 90
B
C
Bacteridal activity & ‘sterilizing’ effect
0 1 2 3 4 5 6
Pop C = sporadically multiplying
Months of therapy

DrugsDaily dose
(mg/Kg/day)Adverse reactions
2 Time/week
dose
(mg/Kg/dose))
Isoniazid(INH)
5-15
(300 mg))Hepatitis, peripheral neuritis,
hypersensitivity
15-40
(900 mg))
Rifampicin(RIF)
10-15
(600 mg))
Gastrointestinal upset,skin reaction,hepatitis, thrombocytopenia,
hepatic enzymes, including orangediscolouraution of secretions
10-20
(600 mg)
Dosage of antituberculosis drug
9/20/2010 91
discolouraution of secretions
Pyrazinamide(PZA)
15 - 40
(2 g)Hepatotoxicity, hyperuricamia,
arthralgia, gastrointestinal upset
50-70
(4 g)
Ethambutol(EMB)
15-25
(2,5 g)
Optic neuritis, decreased visualacuity, decreased red-green colour
discrimination, hypersensitivity,gastrointestinal upset
50
(2,5 g)
Streptomycin(SM)
15 - 40
(1 g)Ototoxicity nephrotoxicity
25-40
(1,5 g)
When INH and RIF are used concurrently, the daily doses of the drugs are reduced
National consensus of tuberculosis in children, 2001

Populasi basil TB pada pasien
Kavitas,ekstrasel
Massa kijuDalam makrofag
(intrasel)
Jumlah populasi 107 - 109 104 - 105 104 - 105
9/20/2010 92
RIF, INH
Netral
Metabolisme danperkembang biak
AktifLambat atauintermiten
Lambat
pH Netral/basa Asam
Obat paling efektif(berturut-turut)
INH, RIF,STREP
PZA, RIF, INH

Drug activities upon TB pop
TB Population
Multiplying rate
Drug
activities
A rapidly INH>>SM>
9/20/2010 93
A rapidly INH>>SM>
RIF>EMB
B slowly PZA>>RIF>>
INH
C sporadically RIF>>INH

TB therapy regimen
2 mo 6 mo 9 mo 12mo
INHRIF
9/20/2010 94
RIFPZA
EMBSM
PREDDOT.S !

Corticosteroid
• Anti inflammation
• prednison : 1 - 3 mg/kg BB/hari, 3x/hari oral 2 - 4 minggu, tapering off
9/20/2010 95
tapering off
• Indications :
– TB milier
– Meningitis TB
– Pleuritis TB with effusion

Treatment evaluation
• Clear improvement in clinical and supporting examination, especially in the first 2 month
9/20/2010 96
especially in the first 2 month
• Main : clinical
• supporting exam as adjuvant

Treatment evaluation
• Clinical improvement :– Increased body weight
– Increased appetite
– Diminished / reduced symptoms (fever,
9/20/2010 97
– Diminished / reduced symptoms (fever, cough, etc)
• Supporting examination : – Chest X rays : 2 / 6 month (on indication)
– Blood : BSR
– Tuberculin test : once positive, do not needed to repeat !

Treatment failure
• Inadequate response, despite adequate therapy :
– Review the diagnosis, not a TB case ?
9/20/2010 98
– Review the diagnosis, not a TB case ?
– Review other aspects : nutrition, other
disease
– MDR – rarely in children
• Treatment discontinuation

Treatment problems
• The main : compliance / adherence
• The factors :
– Long duration
9/20/2010 99
– Drug side effect
– Initial improvement – misinterpreted by patients /
parents
– Inconvenient health service
– Socio-economic-cultural factors
• The following : drug resistance

DOTS with a SMILE
S : Supervised
M : Medication
S : Supervised
M : Medication
9/20/2010 100
I : In
L : a Loving
E : Environment
(Grange JM, Int J Tuberc Lung Dis 1999; 3:360-362)
I : In
L : a Loving
E : Environment
(Grange JM, Int J Tuberc Lung Dis 1999; 3:360-362)

Treament problem solution: FDC
Fixed dose combination: >2 drugs in one tablet in a fixed dose formulation
• simple dosing
• patient friendly, doctor friendly
9/20/2010 101
• patient friendly, doctor friendly
• increase adherence
• reduce MDR
• easier drug supplying
• easier drug monitoring

FDC tablet formulation
WHO
• H : 30 mg
• R : 60 mg
IDAI
• H : 50 mg
• R : 75 mg
9/20/2010 102
• R : 60 mg
• Z : 150 mg
• R : 75 mg
• Z : 150 mg
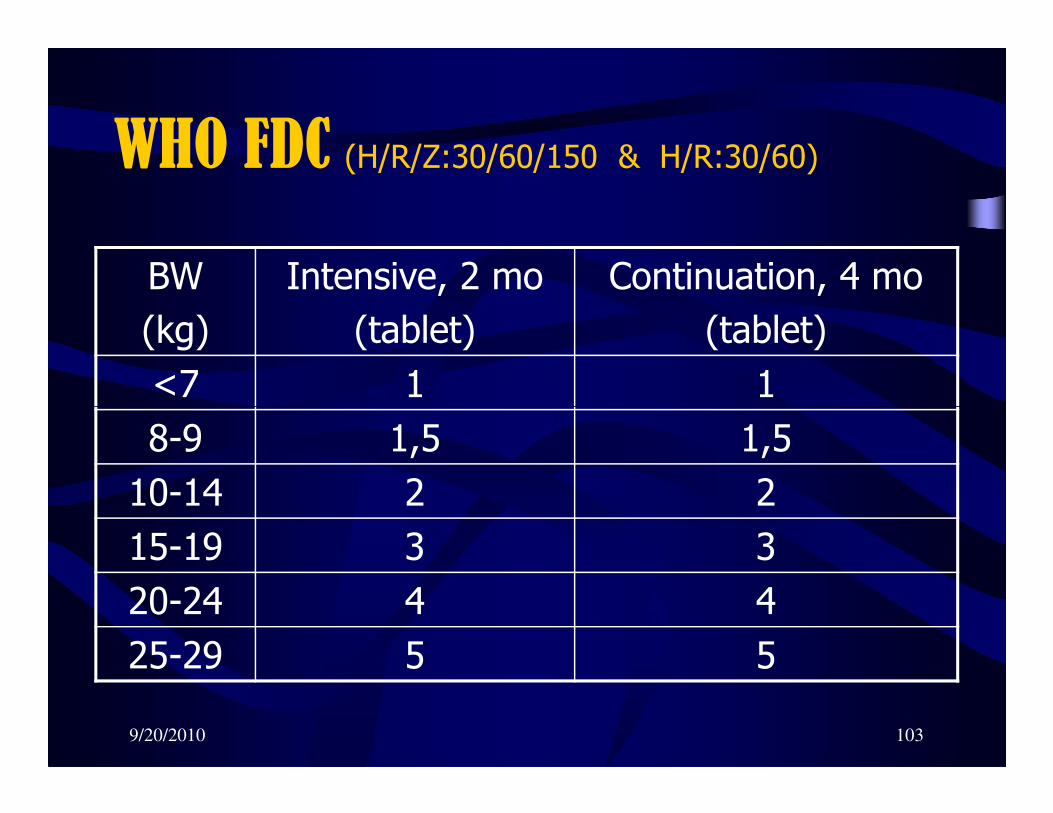
WHO FDC (H/R/Z:30/60/150 & H/R:30/60)
BW
(kg)
Intensive, 2 mo
(tablet)
Continuation, 4 mo
(tablet)
<7 1 1
9/20/2010 103
8-9 1,5 1,5
10-14 2 2
15-19 3 3
20-24 4 4
25-29 5 5

IDAI FDC (H/R/Z:50/75/150 & H/R:50/75)
BW
(kg)
Intensive, 2 mo
(tablet)
Continuation, 4 mo
(tablet)
5-9 1 1
9/20/2010 104
5-9 1 1
10-19 2 2
20-33 4 4
Note: BW < 5kg should be referred and need tailored dosing

WHO vs IDAI fdc formulation
• WHO:
– INH: 4-6 mg/kgBW
– BW grouping: too many
– not practical
– hard to remember
9/20/2010 105
– hard to remember
– a gap for BW 30-33 kg
• IDAI
– INH: 5-10 mg/kgBW
– simple BW grouping
– more friendly both for doctor and patient

TraceTraceTraceTrace
Adult TB patient centri-
fugal
9/20/2010 106
Child TBpatient
centri-petal

case finding
centripetal
• trace the source
• adult people
centrifugal
• trace other ‘victims’
9/20/2010 107
• adult people
• close contact
• by chest X ray
‘victims’
• children
• close contact
• by tuberculin

Pencegahan
• Perbaikan sosio ekonomi
• Kemoprofilaksis
• Imunisasi BCG
9/20/2010 108
• Imunisasi BCG

Kemoprofilaksis primer
• Mencegah infeksi
• Anak kontak dengan pasien TB aktif, tetapi
belum terinfeksi (uji tuberkulin negatif)
9/20/2010 109
• Obat : INH 5 - 10 mg/kg BB/hari

Kemoprofilaksis sekunder
Mencegah penyakit TB pada anak yang terinfeksi :
1. Mantoux (+), Rö (-), klinis (-) :• Umur < 5 th
9/20/2010 110
• Umur < 5 th
• Kortikosteroid lama
• Limfoma, Hodgkin, lekemi
• Morbili, pertusis
• Akil baliq
2. Konversi Mt (-) menjadi (+) dalam 12 bl, Rö (-), klinis (-)
Obat INH 5 - 10 mg/kg BB/hari

Imunisasi BCG
• Imunitas spesifik
• Uji tuberkulinmenjadi (+)
• Mt (-) baru BCG
9/20/2010 111
• Mt (-) baru BCG
• Masal : langsung BCG tanpa Mt
• Reaksi lokal : membantu screening

Thank you
9/20/2010 112
Thank you











![Pediatric TB.ppt [Read-Only]ocw.usu.ac.id/course/download/1125-respirologi/mk_res_slide_pediatric_tuberculosis.pdfDefinition Tuberculosis is a disease due to Mycobacterium tuberculosis](https://static.fdocuments.in/doc/165x107/5e2e2442787f592bc114cc64/pediatric-tbppt-read-onlyocwusuacidcoursedownload1125-respirologimkresslidepediatric.jpg)





