Slide 1 - Clinical Immunology Society
42
م ي ح ر ل ا ن م ح ر ل ه ا ل ل م ا س ب م ي ح ر ل ا ن م ح ر ل ه ا ل ل م ا س ب
-
Upload
many87 -
Category
Technology
-
view
563 -
download
0
description
Transcript of Slide 1 - Clinical Immunology Society

بسم الله الرحمن بسم الله الرحمن الرحيمالرحيم

Immunological Basis of
Gastrointestinal Disorders
Maha A. El BassuoniAss.Prof. of Clinical Pathology
Faculty of Medicine , Menoufiya University, EGYPT

The immune System
The cells and molecules responsible for immunity
constitute the immune system.
The immune system has to be able to respond to protect the human body from a very large number of foreign antigens introduced at any site.

Mucosal Immune System The mucosal immune The mucosal immune
system is recognized by system is recognized by differences from its differences from its systemic counterpart.systemic counterpart.
It is recognized that the It is recognized that the mucosal immune mucosal immune response is also distinct, response is also distinct, largely focused on largely focused on suppressing immunity suppressing immunity rather than promoting it.rather than promoting it.


Gut Associated Lymphoid Tissue(GALT)

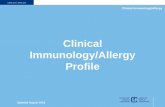
Structure of Secretory IgA
It consists of at least two IgA molecules covalently linked by a J chain and the secretory component, which is added as the antibody crossed the mucosal epithelial cells into the lumen..

Gastrointestinal Organs Disorders
A. Gastrointestinal Disorders
B. Pancreatic Disorders
C. Hepatobiliary Disorders
D. Orodental Disorders

A. Gastrointestinal Disorders1. Food -Induced Gastrointestinal Disorders
I. Gluten-sensitive Enteropathy Celiac Disease

Endomysial antibodies on smooth muscleEndomysial antibodies on smooth muscle
A. Gastrointestinal Disorders1. Food -Induced Gastrointestinal Disorders
I. Gluten-sensitive Enteropathy Celiac Disease
Laboratory Investigation:Laboratory Investigation: Hypoalbuminemia Hypoalbuminemia
hypoproteinemiahypoproteinemia
Iron, folate, and, vB12 Iron, folate, and, vB12 deficiency.deficiency.
PT prolongedPT prolonged
circulating IgA and IgG to circulating IgA and IgG to gliadin gliadin
IgA antibody to endomysium IgA antibody to endomysium has higher sensitivity and has higher sensitivity and specificity specificity

Allergy is an immunological phenomena
refers to certain diseases in which immune responses to environmental antigens causes tissue inflammation and organ dysfunction.
Hypersensitivity and Sensitivity used as synonyms for allergy.
A. Gastrointestinal Disorders1. Food -Induced Gastrointestinal Disorders
II. Gastrointestinal food allergy diseases

A. Gastrointestinal Disorders1. Food -Induced Gastrointestinal Disorders
II. Gastrointestinal food allergy diseases
a. Dietary Protein-Induced Proctitis/Proctocolitis eosinophilic infiltration and occasionally lymph-nodular
hyperplasia. b. Dietary Protein Enteropathy T cell responses
c. Dietary Protein Enterocolitis milk-specific T cell response
d. Immediate Gastrointestinal Hypersensitivity mediated by IgE antibody
e. Eosinophilic Gastroenteropathiesboth cell-mediated and IgE antibody-mediated

d. Immediate Gastrointestinal Hypersensitivity Allergy testingAllergy testing
In vitro testsIn vitro tests Tests for IgE Abs (RAST).Tests for IgE Abs (RAST). Tests for IgG Abs .Tests for IgG Abs . Tests for Immune complex.Tests for Immune complex. Tests for Lymphocyte Tests for Lymphocyte
stimulationstimulation
Antigen cross links IgE on mast cells in tissues Mast Cell Degranulation
II. Gastrointestinal food allergy diseases

A. Gastrointestinal Disorders
2. Chronic Atrophic Gastritis
Normal AtrophicNormal Atrophic

A. Gastrointestinal Disordes
2. Chronic Atrophic Gastritis Autoimmune Atrophic Gastritis (Type A)

A. Gastrointestinal Disordes
2. Chronic Atrophic Gastritis Autoimmune Atrophic Gastritis Types of intrinsic factor antibodies

A. Gastrointestinal Disordes
2. Chronic Atrophic Gastritis Autoimmune Atrophic Gastritis
Diagnosis of autoimmune gastritis however, it can be ascertained histologically:
(1) Antiparietal and anti-IF antibodies in the serum.
(2) Achlorhydria and hypergastrinemia
(3) serum v. B12 levels, usually low.
Anti-Parietal Cells (Rat stomach)

A. Gastrointestinal Disordes
2. Chronic Atrophic Gastritis Gastric autoantibodies
ConditionParietal Cell Antibody
Intrinsic Factor Antibody
Pernicious Anemia Serum 90%IgG – 65%IgA – 25% IgG
Gastric Juice 70%IgA
Blocking Type 70% , IgG Binding Type 35% IgA
Relatives of patients with PA
30% <1%
Other autoimmune diseases Thyroid disease Diabetes mellitus Addison's disease
20% 5%
Iron Deficiency anemia 25% <1%
Healthy Adults Females >60 years
<20 years10%
2%
<1%
<1%

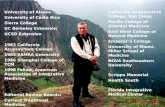
A. Gastrointestinal Disorders 3.Human immunodeficiency Virus Enteropathy
HIV infection HIV is one of the group of viruses known as
retroviruses.
When HIV infects a human cell, its RNA has to be converted to DNA.
It exerts its effect both directly, through infection of the intestinal cells and indirectly through impairment of the intestinal immune response.
The antigenicity of various components provides a means for detection of antibody, and the basis for most HIV testing.

HIV Virus Lifecycle

Gastrointestinal Disorders 4.Whipple's Disease
DiagnosisDiagnosis microscopic examination of microscopic examination of
specimens. The established specimens. The established cultivation of the bacterium and cultivation of the bacterium and the isolation from infected the isolation from infected intestinal biopsies intestinal biopsies
PCR analysis, which has high PCR analysis, which has high sensitivity and specificity. sensitivity and specificity.

A. Gastrointestinal Disorders
5. Inflammatory Bowel Diseases I. Crohn's Disease II. Ulcerative colitis

A. Gastrointestinal Disorders
5. Inflammatory Bowel Diseases

A. Gastrointestinal Disorders
5. Inflammatory Bowel Diseases I. Crohn's Disease II. Ulcerative colitis

A. Gastrointestinal Disorders
5. Inflammatory Bowel Diseases I. Crohn's Disease II. Ulcerative colitis
Enteric bacterial flora has been reported in both animal models and IBD patients.
In animal models Oslon et al have reported that CD4+CD45RBloCD25+ regulatory T cells (Treg cells) prevent colitis induced by transferring effector CD4+CD45RBhiCD25 – T cells into SCID mice through mechanisms involving TGF-ß and IL-10.
Based on the cytotoxicity findings Sauberman et al. postulate that in mice the stimulation of NKT cells through antigen presented to these cells by CD1d-bearing DCs or epithelial cells (MHC class1-like).
The stimulated NKT cells, then
begin to produce IL-13, they become capable of lysing epithelial cells, leads to epithelial cell loss and ulceration.

B. Pancreatic Disorders
Autoimmune pancreatitis is uncommon and accounts for less than 1% of cases of chronic pancreatitis.
local expression and release of TGF-ß, enhances synthesis of extracellular matrix proteins, (collagens, fibronectin).
MCP-1mRNA IL–8 and ENA mRNA in centroacinar ducts.
Laboratory tests
↓ serum amylase and lipase only during acute attacks of pancreatitis, usually early in the course of the disease.
↓ concentrations of serum trypsin are relatively specific for advanced chronic pancreatitis. (not sensitive enough)
ANA test Fecal tests (Steatorrhea a
manifestation of advanced disease) Pancreatic function tests

C. HEPATOBILIARY DISORDERS
1. LIVER DISORDERS I. Viral HepatitisII. Autoimmune Hepatitis
2. BILIARY DISORDERS I. Primary Biliary Cirrhosis (PBC) II. Primary Sclerosing Cholangitis (PSC)

C. HEPATOBILIARY DISORDERS
1. LIVER DISORDERS I. Viral Hepatitis HAV & HEV
Epidemics by contaminated water or food suorce
Acute HEV infection Pregnant female in 3rd trimester 25% risk of mortality

C. HEPATOBILIARY DISORDERS
1. LIVER DISORDERS I. Viral Hepatitis HBV & HDV
Progress to cirrhosisFlare of HBV and FHF

C. HEPATOBILIARY DISORDERS
1. LIVER DISORDERS I. Viral Hepatitis HCV
85% chronic casesAssociated with autoimmune hepatitis

C. HEPATOBILIARY DISORDERS
1. LIVER DISORDERS II. Autoimmune Hepatitis

C. HEPATOBILIARY DISORDERS
1. LIVER DISORDERS II. Autoimmune Hepatitis
Autoantibodies: Autoimmune hepatitis type 1 is characterized by positive ASMA and ANA.
Type 2 marked by a positive anti–LKM-1 antibody.
Type 3 is marked by a positive anti-SLA antibody.
Anti SLAAnti SLA
Anti-actinAnti-actin
Laboratory diagnosis

C. HEPATOBILIARY DISORDERS
1. LIVER DISORDERS II. Autoimmune Hepatitis
Laboratory Diagnosis Hypergammaglobulinemia ↑AST and ALT ↑S. bilirubin and ALP Hypoalbuminemia and prolongation of PT Other common laboratory abnormalities
mild leucopenia Normochromic anemia Coombs-positive hemolytic anemia Thrombocytopenia

C. HEPATOBILIARY DISORDERS
2. BILIARY DISORDERS

C. HEPATOBILIARY DISORDERS
2. BILIARY DISORDERS
I. Primary Biliary Cirrhosis

C. HEPATOBILIARY DISORDERS
2. BILIARY DISORDERS
I. Primary Biliary Cirrhosis
Elevation of : ALT AST ALP GGTP.
Lipid levels (HDL) and cholesterol levels may be increased .
Elevated bilirubin level Prolonged PT Decreased albumin level
The hallmark of the disease is the presence of AMAs in the sera.
AMAs found in 90-95% of patients and have a specificity of 98%.
AMA

C. HEPATOBILIARY DISORDERS
2. BILIARY DISORDERS
II. Primary Sclerosing Cholangitis

C. HEPATOBILIARY DISORDERS
2. BILIARY DISORDERS II. Primary Sclerosing Cholangitis
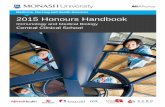
Laboratory Diagnosis: Increased ALP and total bilirubin, Increased transaminases Hypergammaglobulinemia, P-ANCA (65-85% of cases) ANA, (ASMA), anti-cardiolipin
autoantibodies Anti-mitochondrial autoantibodies
(AMA) are negative
P-ANCA

D. ORODENTAL DISORDERS
1. Inflammatory Periodontal Diseases
I. Gingivitis and periodentitis polymorph induced damage, complement induced damage (through IgG (IgG2). peripheral T cell reactivity to plaque antigens
II.Juvenile Periodontitis defects in granulocyte or monocyte function conventional.

D. ORODENTAL DISORDERS
2. Recurrent Aphthous Ulceration Raised level of circulating antibody to saline
extract of fetal oral mucous membrane.
These antibodies may be a response to exposed tissue antigen that previously been protected from immune system. (Ag against oral mucous membrane, epithelial cells. or viral Ags).
CMI proved by an infiltrate of lymphocyte

D. ORODENTAL DISORDERS
3.Oral Candidiasis A threshold number of systemic CD4+ cells to protect the oral
mucosa together with the status of local immunity. HIV infected persons with and without OPC had a Th2-type
salivary cytokine profile suggestive of susceptibility to Candida infection
GM-CSF are important in the generation of effective immunity to GM-CSF are important in the generation of effective immunity to C. albicansC. albicans. . .
4. Oral Hairy Leukoplakia There is correlation of diminished CD4+ T lymphocyte count to
the occurrence of the lesions.