Sleep Apnea and Heart Failure (2001-06-13)
80
Sleep Apnea in Heart Failure Update on Prevalence and Treatment Options S. Javaheri, M.D., FCCP Professor Emeritus of Medicine, University of Cincinnati, College of Medicine Medical Director, Sleepcare Diagnostics Cincinnati, Ohio Indianapolis, 8/2007
-
Upload
medicineandfamily -
Category
Health & Medicine
-
view
1.325 -
download
0
Transcript of Sleep Apnea and Heart Failure (2001-06-13)

Sleep Apnea in Heart Failure Update on Prevalence and Treatment Options
S. Javaheri, M.D., FCCP
Professor Emeritus of Medicine, University of Cincinnati, College of Medicine Medical Director, Sleepcare Diagnostics Cincinnati, OhioIndianapolis, 8/2007

Disclosures
I am a consultant and/or have received grant and/or honoraria
and/or travel expenses from:
BI, Cardiac Concept, Cephalon,
GSK, Respironics, Res Med,
Sanofi-Aventis and Takeda

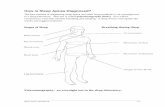
ObstructiveObstructive ApneaApnea
Normal AirwayNormal Airway Obstructed AirwayObstructed Airway

Polysomnographic Breathing Disorders Event
Rib cage
Obstructive apnea
Abdomen
Ribcage
Airflow



Interaction Between Sleep and Heart Pathology
Primary
Secondary
Sleep Apneas & Hypopneas
Secondary
Primary
Cardiovascular Pathology

Polysomnographic Breathing Disorders Event
Rib cage
Abdomen
Ribcage
Airflow
Central apnea


Hunter- Cheyne-Stokes Breathing in SHF

Su
rviv
al %
Months Javaheri et al, JAAC,2007
( N=32 )
( N=56 )

Prevalence of Sleep Apnea inRecent Prospective Studies of SHF
Canada (07) (13)
China (07) (12)
Germany (07) (16)
N Zealand (05) (11)
US (06) (5)
n
%AHI
≥ 10/hr%
β blockers
%AHI
≥ 15/hr
8010
80
30
%OSA
%CSA
2137
46
15
71
68
4749
2612
25
53
52 85
287100
126
56
700
Country (y) (Ref)
9028 43203
54 8037 17102
Germany (07) (15)
Germany (07) (19)
71
UK (07) (18) 7838 1555 53
33 19 8533 19

Complex sleep apnea
The new kid on the block
or
the old guy in the background

Prevalence of Sleep Apnea in Prospective Studies of SHF
• CPAP-resistant Central Sleep Apnea (CSA)– A large number of Patients with Systolic Heart failure – Patients with Atrial Fibrillation– Patients on Opioids– Neuromuscular Disease
• CPAP-emergent CSA– Over-titration – Sleep Fragmentation ( Post-arousal )– S/P UPPP
Complex Sleep ApneaCPAP-resistant CSA and CPAP-emergent CSA

Hunter- Cheyne-Stokes Breathing in SHF






SleepApnea &Hypopnea
H/R
PCO2
Arousals
Ppl
O2 Delivery
RV Afterload
SVR/Others
Changes in R&LVentricular Preload &Afterload
Lung H2O
Vasoconstriction
Thrombosis
Inflammation
OrganDysfunction
Hypoxic & HypercapnicPulmonaryVasoconstriction
EndothelialDysfunctionSyndrome
SympatheticActivation
Transmural P. ofL&R ventricles, and PulmonaryMicrovascular Bed
SA/H: Mechanisms Contributing to Cardiovascular Disease

CSA as a Predictor of Mortality in SHF
• N = 114 eligible
• N = 100 Enrolled
• N = 12 with OSA Excluded
• N = 88
N = 88 : 32 with AHI <5 ; 56 with AHI ≥5/hr
Median F/U : 51 months
Javaheri et al , J Am Coll Cardiol (May, 2007)

Demographic and cardiovascular parameters in 88 heart failure patients
without and with central sleep apnea Variable AHI<5/hr AHI ≥5/hr P
Number 32 56
Age, y 62 67 0.02
BMI, kg/m2 28 26 0.09
SBP, mm Hg 127 119 0.06
DSP, mm Hg 72 70 0.09
Heart rate, n/min 78 80 0.48

SRBD in 88 heart failure patients without and with central sleep apnea
Variable AHI<5/hr AHI ≥5/hr
AHI, n/hr 2 35
CAI, n/hr 0.6 23
OAI, n/hr 0.1 0.5
CAHI, n/hr 2 32
OAHI, n/hr 0.2 1

Cardiovascular parameters in 88 heart failure patients
without and with central sleep apnea Variable AHI<5/hr AHI ≥5/hr P
LVEF, % 27 22 0.006
RVEF, % 49 43 0.048
Atrial fibrillation,% 6 20 0.1 NHYA Class I,% 25 9 0.09
NHYA Class II, % 53 55 0.09
NHYA Class III, % 22 36 0.09

The Predictors of mortality in SHF
Three Variables, RVEF, AHI and DBP
Independently Correlated with Survival:
RVEF (HR=0.97, P=0.003)
AHI (HR=2.14, P=0.02)
DBP (HR=0.96, P=0.02)

90
6259 60 60 59
45 44
36 35 35 36
0
10
20
30
40
50
60
70
80
90
100
AHI<5 VS >=5 AHI<10 VS >=10 AHI<15 VS >=15 AHI<20 VS >=20 AHI<25 VS >=25 AHI<30 VS >=30
Med
ian
Su
rviv
al
Less than cutoff point Greater or equal to cutoff point
44
36353536
45
P=0.0190
P=0.0162 P=0.02
59
P=0.00360
P=0.00260
P=0.00259
Med
ian
su
rviv
al (
mo
nth
s)
AHI<5 VS ≥5 AHI<10 VS≥10 AHI<15 VS ≥15 AHI<20 VS ≥20 AHI<25 VS ≥25 AHI<30 VS≥30
■ Less than the cutoff point■ Greater or equal than the cutoff point
0
10
20
30
40
50
60
70
80
90
100
Javaheri et al, JAAC, 2007

Prevalence of Sleep apnea Stable Systolic Heart Failure
Prospective Studies
Variable
Apnea-Hypopnea Index > 15/hr
Central Sleep Apnea
Obstructive Sleep Apnea
Range, %
47 - 49
15 - 46
12 - 53

Prevalence of SRBD in Systolic Heart Failure
100 out of 114 consecutive patients
– 68% with AHI ≥ 5/h ; 49% with AHI ≥ 15/h
– 56% CSA
– 12% OSA
– Javaheri, Ann Intern Med, 1995, Circulation 1998– and Int J cardiol 2006

Prevalence of Sleep Apnea in Prospective Studies of SHF
68
4947
68 71 70
82
53
0
20
40
60
80
100
%
CanadaUS NZ ChinaGermanyDCM ICM
AHI ≥5/hr AHI ≥10/hr AHI ≥15/hr
Germany

Prevalence of Sleep Apnea in Prospective Studies of SHF
12
37
2621
53
15
20
37 3835
32
46
17
37
0
10
20
30
40
50
60
%
OSA CSA
CanadaUS NZ ChinaGermany
DCM ICM Germany

Heart Failure in U.S.
• 1.5–2% of population (5 million)
• 6–10% of population >65 y old
• 400,000–700,000 new cases annually
• 20 million with asymptomatic cardiac impairment
• 11 million physician office visits annually
• 3.5 million hospitalizations annually
• Leading cause of hospitalization in people >65 y
• 250,000 deaths annually (direct and indirect)
• $27 billion (annual cost), 2003
• $8–15 billion per for hospitalization

Mortality Trends in Heart Failure U.S.
• Framingham Study (2002)
59% in men and 43% in women
• Olmsted Study (2004)
43%
• Worcester (2007)
79%

Treatment of CSA in SHF(No Guidelines)
1. Promote sleep hygiene
2. Avoiding ETOH and benzodiazepines
3. Optimization of medical thereapy of CP functions
lockers vs- melatonin secretion
4. Treatment algorithm for CSA
5. Treatment of RLS/PLM

Optimize Therapy:
ACEI; ß-Blockers; Diuretics; Digoxin; CRT
SRBD Eliminated
Persistent SRBD
Follow-up Clinically
Consider Treatment
Cardiac TransplantationMedications
TheophyllineNocturnal Nasal Oxygen
Acetazolamide
APSSV HFV
Medical Devices
nCPAPMandibular
AdvancementCardiacPacing

Optimize Therapy:
ACEI; ß-Blockers; Diuretics; Digoxin
SRBD Eliminated
Persistent SRBD
Follow-up Clinically
Consider Treatment
Cardiac TransplantationMedications
TheophyllineNocturnal Nasal Oxygen
Acetazolamide
APSSV HFV
Medical Devices
nCPAPMandibular
AdvancementCardiacPacing

Study Design-Inclusion Criteria
• Subjects transplanted between 1995-1999
• At least 5 months post- transplant
• 59 Eligible patients
• 45 Participated (76%)
• 14 Refused (24%)
Javaheri et. al., EHJ, 2004

21
1
7
0
5 4
7
5
10
15
20
0- 5 5- 10 10- 15 15- 20 20- 30 30- 40 40
47% 53%
51%
36%
36%
24%
16%
AHI, no./hr
Nu
mb
er o
f S
ub
ject
s
Javaheri et. al., EHJ, 2004

Demographics and Physical Examination Findings in 45 Heart Transplant Subjects Without Sleep Disorders (Group I, n=15),
With PLM (Group II, n=14)or With Sleep Related Breathing Disorders (Group III, n=16)
Variable
Age, yMale/Female, nHt, cmWt, kgWt gain since transplant, kgBMI, kg/m2
Neck size, cm
Group II 55
12/2179•
909
28•
42.4
Group I 58
13/217685 4
27 41.1
Values are means ± SD; * p<0.05 when compared to Group I; • p<0.05 when compared to Group III.
Group III 58
15/117299*16*
33* 43.9
p 0.7 — 0.03 0.045 0.03
<0.001 0.1

10
20
30
40
50
60
80
HabitualSnoring
ExcessiveDaytime
Sleepiness
UnrefreshedSleep
Restless LegsSyndrome
PhysicalComponent
Scale
MentalComponent
Scale
P=0.02 P=0.002 P=0.03 P=0.04 P=0.01 P=0.7
*
*
*
*
Group I
Group 2
Group 3
0
%%
% %
70
Javaheri et. al., EHJ, 2004

Optimize Therapy:
ACEI; ß-Blockers; Diuretics; Digoxin
SRBD Eliminated
Persistent SRBD
Follow-up Clinically
Consider Treatment
Cardiac TransplantationMedications
TheophyllineNocturnal Nasal Oxygen
Acetazolamide
APSSV HFV
Medical Devices
nCPAPMandibular
AdvancementCardiacPacing

Ap
nea
-Hyp
op
nea
In
dex
(n
/hr)
0
10
20
30
40
50
60
70
80 Changes in AHI with low flow nasal O2 in CSA patientswith heart failure and systolic dysfunction
Room Air
Oxygen
N=9 N=7 N=11 N=7 N=22 N=29Hanly FranklinStaniforthWalsh Andreas Javaheri
p<0.0001
p<0.01
p<0.001
p=0.02
p=0.01
p<0.05
MeansSD

Effects of Supplemental Nasal O2 on CSA in SHF
• Decreases PB and central apneas
• Improves hypnogram
Ar; S1; S2
• Improves exercise capacity
• Decreases sympathetic activity
urinary norepinephrine
SMNA by microneurography
• Increases LVEF
• Improves Quality of life
• Decreases BNP

Optimize Therapy:
ACEI; ß-Blockers; Diuretics; Digoxin ,CRT
SRBD Eliminated
Persistent SRBD
Follow-up Clinically
Consider Treatment
Cardiac TransplantationMedications
TheophyllineNocturnal Nasal Oxygen
Acetazolamide
APSSV HFV
Medical Devices
nCPAPMandibular
AdvancementCardiacPacing

Data of HF Patients Undergoing Theophylline Trial
Placebo
15 15/0
66 175
88 ND
Theo
15 15/0
66 175 88 11 Values are means; ND=not detectable
Javaheri et al., NEJM, 1996, 335, 562-7
Baseline
15 15/0 66 175 89
ND
Variable
NGender, M/FAge, yHt, cmWt, kgTheo, ug/ml

Periodic Breathing at Baseline, With Placebo and Theophylline in 15 HF Patients
Placebo
37 26 2 2
17
Theo
18* 6* 2 1 8* Values are means; * p < 0.05
Javaheri et al., NEJM, 1996, 335, 562-7
Baseline
47 26 2 2
24
Variable
AHI, n/hCAI, n/hOAI, n/hMAI, n/hDBArI, n/h

Optimize Therapy:
ACEI; ß-Blockers; Diuretics; Digoxin;CRT
SRBD Eliminated
Persistent SRBD
Follow-up Clinically
Consider Treatment
Cardiac TransplantationMedications
TheophyllineNocturnal Nasal Oxygen
Acetazolamide
APSSV HFV
Medical Devices
nCPAPMandibular
AdvancementCardiacPacing

Demographics and Cardiovascular Findings in 12 SHF Patients with Central Sleep Apnea Treated
with Acetazolamide
Variable
Patients, n Age, yBMI, kg/m2
SBP, mm HgDBP, mm HgLVEF, %
Placebo
126626
1136921
ACTZ
126626
1086920
Values are means.Javaheri, AJRCCM, 2006
Baseline
126626
1106719
p
----0.91.00.80.90.5

Variable
AHI, n/h
CAI, n/h
Placebo
57
49
ACTZ
34*†
23*†
Disordered Breathing Events of 12 SHF Patients with Central Sleep Apnea Treated with Acetazolamide
Baseline
55
44
p
0.002
0.004
* p < 0.05 versus baseline † = p < 0.05 versus placebo

Patients’ Perception of Their Sleep Quality and Daytime Symptoms Comparing Acetazolamide
with Placebo
Variable
Sleep qualityWaking up refreshedDaytime fatigueFall asleep
unintentionally
Javaheri, Am J Respir Crit Care Med,2006
Acetazolamide
ImprovedImprovedImproved
Decreased
p
0.0030.0070.020.002


• The Canadian Continuous Positive Airway Pressure for Patients with CSA and Heart Failure trial tested the hypothesis that CPAP would improve the survival rate without heart transplantation of patients who have CSA and heart failure
Background
Continuous Positive Airway Pressure for Central Sleep Apnea and Heart Failure
Bradley TD et al., N Engl J Med 2005;353:2025-33.

• After medical therapy was optimized, 258 patients who had heart failure, were randomly assigned to receive CPAP (128) or no CPAP (130)
• CAHI = 40/hr , LVEF = 25%, age = 63 yr
• Patients were followed for a mean of two yr
Methods
Continuous Positive Airway Pressure for Central Sleep Apnea and Heart Failure
Bradley TD et al., N Engl J Med 2005

Effect of CPAP on the Frequency of Episodes of Apnea and Hypopnea
Bradley TD et al., N Engl J Med 2005
P<0.001
Control group
CPAP group
Time from Randomization (mo)
Ep
iso
des
of
Ap
ne
a a
nd
H
yp
op
ne
a (
no
. pe
r h
r o
f s
lee
p)
50
40
30
20
10
00 3 24

Bradley TD et al., N Engl J Med 2005
Heart-Transplantation-Free Survival
Tra
nsp
lan
tati
on
-fre
e S
urv
ival
(%
)
Time from Enrollment (mo)
Control group(32 events)
CPAP group(32 events)
P=0.54
100
80
60
40
20
00 12 24 36 48 60

Potential Mechanisms of CPAP Failure
1. Hemodynamic Consequences:Effects on RV Function, LV Stroke Volume, BP and CBF. Hemodynamic Effects of Atrial Fibrillation
2. Nonresponsive Patients Importance of Hpocapnia and Failure of PAP Devices to Correct it
Javaheri, JCSM, 2006

The Predictors of mortality in SHF
• N = 88; 32 with AHI <5; 56 with AHI ≥5/hr
• Mean AHI 2/hr vs. 32/hr (CAI = 23/hr)
• Median F/U : 51 months
• RVEF (HR=0.97,P=0.003), AHI (HR=2.14,P=0.01) and DBP (HR=0.96,P=0.02) independently correlated with
survival

RV Systolic dysfunction is a predictor of mortality in SHF
1. Palak, J Am Coll Cardiol, 1983
2. Disalvo, J Am Coll Cardiol, 1995
3. Gavazzi, J Heart Lung Transplant, 1997
4. Mehta, J Am Coll Cardiol, 2001
5. Karatasakis, J Am Cardiol. 1998
6. Meluzin, Int J Cardiol, 2005
7. De Groote, J Am Coll Cardiol, 1998
8. Ghio, J Am Coll Cardiol, 2001

CVD mortality in the elderlyThe lower the DBP the worse
• CV effects of SBP and DBP depend on the age
• In the Fram study, there was a gradual transition from DBP to SBP as the more important predictor of CV mortality
• After age 60 yr, the risk of CHD correlated positively with SBP and negatively with DBP
• After age 60 yr, the lower DBP was associated with a worsening CV prognosis
Franklin et al, Circulation, 2001

The risk with aggressively lowering blood pressure in HTN patients with CAD
• Low DBP and Mortality; Post hoc analysis of INVEST
• N = 22576 patients with CAD, CHF (I,II) and HTN
• The risk for the primary outcome, all-cause death and MI, but not stroke, progressively increased with low diastolic blood pressure.
• Excessive reduction in diastolic pressure should be avoided in patients with CAD who are being treated for hypertension.
• Messerli et al, AIM, 2006

Transplant-free survival in HF patients according to effect of CPAP on CSA
CPAP responders*(AHI at 3 months < 15/hr, n = 57)
CPAP non-respondersCPAP non-responders(AHI at 3 months (AHI at 3 months 15/hr, n = 43) 15/hr, n = 43)
00 66 1212 1818 2424 3030 3636 4242 4848 5454 6060
Time from enrollment (months)Time from enrollment (months)
ControlControl
00
2020
4040
6060
8080
100100
Tra
nsp
lan
t-fr
ee s
urv
ival
(%
)T
ran
spla
nt-
free
su
rviv
al (
%)
*versus control: HR=0.36, *versus control: HR=0.36, p=0.040p=0.040

Optimize Therapy:
ACEI; ß-Blockers; Diuretics; Digoxin
SRBD Eliminated
Persistent SRBD
Follow-up Clinically
Consider Treatment
Cardiac TransplantationMedications
TheophyllineNocturnal Nasal Oxygen
Acetazolamide
APSSV HFV
Medical Devices
nCPAPMandibular
AdvancementCardiacPacing

APSSV in CSA (mean values)
AHI
ArI
PtCO2
45*
67*
32
28*
32*
37*
6
17
34
27*
32*
35
15*
18
35
(n/hr)
(n/hr)
(mm Hg)
BaselineO2
2l/minCPAP 8-11
Bilevel IP:11-15 EP: 5-6
APSSV PI:4-10 EP: 4-6
*Significant vs. APSSV. Teschler et al., AJRCCM, 2001

APSSV in SHF/ CSA
• A randomized parallel trial using Therapeutic and Sub-therapeutic APSSV for one month
• 15 patients with SHF in each group; mean AHI = 20/hr
• AHI decreased to 5/hr in Ther. and 15 /hr in Subther. arm
• In the Ther. arm: Objective (but not subjective) EDS, BNP and urinary metadrenaline excretion decreased
Pepperell et al, AJRCCM, 2003

Studies with ASV in SHFa
Szollosi
Phillips
Pepperell*
Teschler
nAge(Y)
LVEF%
(2006)
(2001)
(2006)
(2003)
Baseline AHIn/hr
14
8
<10
5
Durationnights
30
47
47
25
ASV AHIn/hr
67
69
64
71
32
NR
29
30
1
1
180
30
10
14
12
15
Kasai (2006) 66372 38 14

CPAP vs. APSSV in Patients on Opioids
BaselinePSG
CPAP Final Setting
ADAPT Final Settings
AHI OAI CAI AHI OAI CAI AHI OAI CAI
1 74 45 29 101 0.0 101 6 0.0 0.0
2 17 0.5 3 27 0.0 22 12 0.0 0.0
3 44 4 3 61 0.0 56 1 0.0 0.0
4 83 1 60 34 0.0 33 5 0.0 0.0

Prevalence of Sleep Apnea inRecent Prospective Studies of SHF
Canada (07) (13)
China (07) (12)
Germany (07) (16)
N Zealand (05) (11)
US (06) (5)
n
%AHI
≥ 10/hr%
β blockers
%AHI
≥ 15/hr
8010
80
30
%OSA
%CSA
2137
46
15
71
68
4749
2612
25
53
52 85
287100
126
56
700
Country (y) (Ref)
9028 43203
54 8037 17102
Germany (07) (15)
Germany (07) (19)
71
UK (07) (18) 7838 1555 53
33 19 8533 19

OSA as a Cause of Mortality in SHF (Wang, JAAC, 2007)
N=37
N=113

Treatment of OSA in CHF
• Promote sleep hygiene
• Avoid ETOH , benzodiazepines and Viagra
• Weight loss• Positive airway pressure devices CPAP, bilevel• Mandibular advancement devices• Upper airway procedures• Nocturnal use of supplemental oxygen

Effects of CPAP on Systolic Heart Failure in OSA
• 24 patients with systolic HF and OSA (AHI ~40/h) were randomized to CPAP (n = 12) or a control group (n = 12)
• LVEF increased significantly following one month of CPAP therapy (25% to 34%)
• LVEF did not change significantly in the control group
Kaneko Y et al. N Engl J Med. 2003;348:1233.
CPAP = continuous positive airway pressureHF = heart failureLVEF = left ventricular ejection fraction

A controlled study of mild to moderate OSA (AHI~25, low SaO2~78%) with CPAP (9cm H2O) for 3 months in SHF
VariablesNAHI, n/hrLVEFUNEESSSF36CHF?
Control2121 181.5%21No changeNo change
CPAP1925 35% (P=0.04)10 (P=0.04)3 (P=0.01)ImprovedImproved
No change in BP, Dyspnea, VO2, NYHA, BMI or MedsMansfield et al, Am J Respir Crit Care Med, 2004

CPAP Improves Cardiac Efficiency
Open study of 7 HF /OSA compared to 5 HF/No OSA
Yoshinaga et al; JAAC, 2007
SHF/OSA
LVEFBMI AHIAge
61 37 31 38
SHF/No OSA 62 30 27 3
%Kg/m2 /hryrs

• 2D-ECHO and “C acetate PET (K mono) baseline and 6 W
• K mono = Monoexponential function fit to myocardial clearance
(rate of oxidative metabolism reflecting MVO2)
• Myocardial efficiency: LV WMI = SVI *SBP/K mono)
Yoshinaga et al; JAAC, 2007
Long-term CPAP Improves Cardiac Efficiency

CPAP Improves Cardiac Efficiency
Yoshinaga et al; JAAC, 2007
SVI
Heart rate
SHF/No OSASHF/OSA (CPAP)
59
37
141
60
42
129SBP
58
38
141
42
121
55
WMI
LVEF 38
7.1
0.047
43
8.2
0.039Kmono
43*
8.2*
0.04*
7.0
0.036
44
Base line Base line 6 wk 6 wk
38 43*

Effects of CPAP on LVEF in OSA/SHF
AHI, n / h
Duration
CPAP titration
LVEF, %
n
MansfieldKaneko SmithYoshinaga
6W
30
38
yes
3.5
19 7
3M
35
21
23
yes
NR
36
6W
38
6.2Compliance, h
40
12
4W
25
yes
5.6
Auto
Change in LVEF, % N05 59

Treatment of OSA in CHF
• Promote sleep hygiene.
• Avoid ETOH and benzodiazepines.• Weight loss.• Positive airway pressure devices, CPAP, bilevel.• Mandibular advancement devices.• Upper airway procedures.• Nocturnal use of supplemental oxygen. • Pacing does not improve OSA.

Pacing does not improve OSA
OSA without Heart Failure
1. Pepin et al, Eur Respir J, 2005
2. Luthye et al, Am J Respir Crit Med, 2005
3. Simantrikis et al, NEJM, 2005
OSA with Heart Failure
1. Garrigue et al, NEJM, 2002
2. Gabor et al, Eur Respir J, 2005
3. Pepin et al ,Eur Respir J, 2005

HR /min 64 75
Pacing Does Not Improve OSA
Baseline Pacing
AHI /hr 43 50
CAI /hr 1 2
Minimum SaO2 % 83 84
n=15; BMI=28 kg/m2; LVEF=64 % (5<56 %)
Pepin et al, ERJ;2005

Treatment of OSA in CHF
• Promote sleep hygiene.
• Avoid ETOH and benzodiazepines.• Weight loss.• Positive airway pressure devices, CPAP, bilevel.• Mandibular advancement devices.• Upper airway procedures.• Nocturnal use of supplemental oxygen.

Heart Failure in U.S.
• 1.5–2% of population (5 million)
• 6–10% of population >65 y old
• 400,000–700,000 new cases annually
• 20 million with asymptomatic cardiac impairment
• 11 million physician office visits annually
• 3.5 million hospitalizations annually
• Leading cause of hospitalization in people >65 y
• 250,000 deaths annually (direct and indirect)
• $27 billion (annual cost), 2003
• $8–15 billion per for hospitalization