Sleep apnea and aortic dissectiondownloads.hindawi.com/journals/crj/1995/254831.pdf · CASE REPORT...
6
CASE REPORT Sleep apnea and aortic dissection PATRICK J HANLY MD FRCPC, DAVID FORD MSc Sleep Laboratory, Department of Medicine, The Wellesley Hospital, Toronto, Ontario PJ HANLY, D FORD. Sleep apnea and aortic dissection. Can Respir J 1995;2(1):69-73. ,\ 62-year-old man presented with obstructive slee p apnea, congestive heart failure and Cheyne-Stokes respira ti on. Further evaluation revealed a chronic dissecting aneurysm of the aorta causing vcna ca val obstruction. Surgical correc- tion or the aneurysm dramatica ll y improved ventricular fun c ti on w it h resolution of Cheyne -Stokes respiration. Na- sal continuous positive airway pressure corrected the ob - structive sleep apn ea and as ociated clinical features. The cardiopulmonary interactions between sleep apnea and aor- tiL· dissection are discussed. Key Words : Aortic a11e11rrs1 11. Chen 1 e- S1okcs respim1io11. Sl ff p apnea C I-J l'.Y E-STOKES RESPIRATI ON (CS R) IS A FORM OF CEN- tral sleep apnea caused by periodic changes in respira- tory dr ive ( I). It is characteristically seen in patients with evere congestive heart failure (2) and has not been reported in association with aortic aneurysm. Obstructive sleep apnea (OSA ) is caused by upper airway in stabi lity dur ing sleep and may co nt ribute to left ventricular dys fu nct ion in pa ti ents with rn-cxistin g heart di sease (3 ). A case of a patient who had CSR due to vcna caval obstruction associated with a dissect- ing ancury~m of' the ascending aorta is presented. The patient also had OSA. which may have contributed to the develop - ment or hi~ aort ic di ssection. Apnee du sommeil et dissection aortique RESUME : Un homme de 62 ans presentait unc apnee du so mmeil obstructive, une insu llisancc cardiaque et une res- piration de Cheyne-Stokes. Un examen plus approfondi a revelc un anevri me chroniq ue dissequant de l'ao rt e causant une obstruction de la vei ne cave . Une chirurgie corTectivc de J'anevrisme a considerablernent ameliore la fonction ventriculaire et a resolu la respiration de Cheyne-Stoke . La pre sion positive continue administree par voie nasale a corrige l'apnee du somrneil obstructive ainsi que Jes syrnp- t6me s qu i y etaien t asso cies . Les int eract io ns ca rdio- pulrnonaires de l'apnee du somme il ct de la dissectinn aortique sont examinees. CASE PRESENTATION History: A 62 -y ea r- old mal e presented with a l ong history of OSA and a recen t hi story of congestive heart failure. He reported very loud, habitual snoring and excessive daytime sleep iness for 40 years. Initially. he had passive sleepiness but it became so severe that he had frequent road tra ff ic accidents and disco ntinued dr iv ing. His wife had witnessed apneas dur in g sleep t or 20 years. The patient had been obese a ll his life and. on presentation, weighed 15 3 kg with a body mass index of 46 kg/ 111 2 . He reported drinking 6 to 8 oz of alcoho l per day for several years_ The pa ti ent had bee n treated for hypertensinn !'or IO yea rs. Corre.,po111f, , 11ce <1n d rep ri111s: Dr Par rick Han ly. Suite 247 18. Th e \Vl'l/esley Hospita l. 160 We ll es /er Sreet Eu.,t, Toron r o. Ontario M.f.Y 113. l'ele11hmH' I 41 6) 926-4865 Can Respir J Vol 2 No 1 Spring 1995 69
Transcript of Sleep apnea and aortic dissectiondownloads.hindawi.com/journals/crj/1995/254831.pdf · CASE REPORT...

CASE REPORT
Sleep apnea and aortic dissection
PATRICK J HANLY MD FRCPC, DAVID FORD MSc
Sleep Laboratory, Department of Medicine, The Wellesley Hospital, Toronto, Ontario
PJ HANLY, D FORD. Sleep apnea and aortic dissection. Can Respir J 1995;2(1):69-73.
,\ 62-year-old man presented with obstructive sleep apnea, congestive heart failure and Cheyne-Stokes respirati on. Further eval uation revea led a chron ic dissecting aneurysm of the aorta causing vcna ca va l obstruction. Surgical correction or the aneurysm dramatica ll y improved ventricu lar fun ction wit h resolution of Cheyne-Stokes respiration. Nasa l continuous positive airway pressure corrected the obstructive sleep apnea and as ociated clinical features. The card iopulmonary interactions between sleep apnea and aortiL· dissection are d iscussed.
Key Words : Aortic a11e11rrs111. Chen 1e-S1okcs respim1io11. Slffp apnea
C I-J l'.Y E-STOKES RESPIRATION (CS R) IS A FORM OF CEN
tral sleep apnea caused by periodic changes in respiratory drive ( I). It is characterist ically seen in pat ients with evere congestive heart failure (2) and has not been reported
in association with aort ic aneurysm . Obstruct ive sleep apnea (OSA ) is caused by upper airway instabi lity during sleep and may cont ribu te to left ventricular dys fu nct ion in patients with rn-cxisting heart di sease (3 ). A case of a patient who had CSR due to vcna caval obstruction assoc iated with a dissecting ancury~m of' the ascending aorta is presented. The patient a lso had OSA. which may have contributed to the development or hi~ aort ic di ssection.
Apnee du sommeil et dissection aortique
RESUME : Un homme de 62 ans presentai t unc apnee du sommei l obstructive, une insu llisancc cardiaque et une respiration de Cheyne-Stokes. Un examen plus approfondi a reve lc un anevri me chronique dissequant de l'aorte causant une obstruction de la vei ne cave. Une chi rurgie corTect ivc de J'anevrisme a considerablernent amel iore la fonc tion ventricula ire et a resolu la respiration de Cheyne-Stoke . La pre sion positive continue admin istree par voie nasale a corrige l'apnee du somrnei l obstructive ai nsi que Jes syrnpt6mes qu i y etaien t assoc ies . Les interact io ns ca rdiopu lrnonaires de l'apnee du sommeil ct de la di ssectinn aortique sont exami nees.
CASE PRESENTATION History: A 62-year-old male presented with a long his tory of OSA and a recent hi story of congestive heart failure . He reported very loud, habitual snoring and excessive daytime sleep iness for 40 years. Initially. he had passi ve sleepiness but it became so severe that he had frequen t road traffic accidents and d iscontinued driv ing. His wife had witnessed apneas during sleep tor 20 yea rs. The patient had been obese all his life and. on presentation, weighed 153 kg wit h a body mass index of 46 kg/1112
. He reported drinking 6 to 8 oz of alcohol per day for several years_
The patient had been treated for hypertens inn !'or IO years.
Corre.,po111f,,11ce <1nd repri111s: Dr Par rick Hanly. Suite 247 18. The \Vl'l/esley Hospita l. 160 Welles /er Sreet Eu.,t, Toron ro. Ontario M.f.Y 113. l'ele11hmH' I 416) 926-4865
Can Respir J Vol 2 No 1 Spring 1995 69

HANLY AND F ORD
TABLE 1 Overnight polysomnography at presentation and 13 months following surgery, on and off nasal CPAP
Before After surgery, After surgery, sur~ry off CPAP on CPAP
TST(h) 4.87 2.3 3.6 Sleep efficiency (%) 81 76 94 Stage 1 ,2 (% TST) 98 86 69
SWS (%TST) 0 14 4
REM(% TST) 2 0 27
AHi (/h) 61 43 3
PLM (/h) 62 20 17 AR (/h) 53 26 14 Sa02 (TST) 82 85 92 !CO2 (TST) 34 43 44
AHi Apnea-hypopnea index: AR Arousal index: CPAP Continuous positive airway pressure; PLM Periodic leg movement index; REM Rapid eye movement sleep; Sa(k (TST) Mean oxygen saturation during TST; Stage 1. 2 Stage 1 and 2 non-rapid eye movement sleep; SWS Slow wave sleep; tC(k (TST) Mean transcutaneous PC(k in mmHg during TST; TST Total sleep time
Seven years prev ious ly. he developed viral pericardit is and ~1
sma ll pericardia! effusion. wh ich was detected by echocardiography. This was compl icated hy atrial fibrillation , which was successfully cardioverted. Over the past few months. he dcve loped increasi ng shortness of breath and peripheral edema. His medications included furosem iJe, digox in. amiloride, ena lapri l and allopurinol. Physical examination: The patient was a morb idly obese male . He had atria l fibrillat ion wit h a ventricul ar response of 150 beats/min . Blood pressure was 140/80 mmHg. Neck circumference was 51 cm and he had a large uvu la and crowded oropharynx . Cardiovascula r exam inati on revealed an e levated j ugular venous pressure. disp laced le ft ventricular apex beat and severe. bilatera l leg edema. Overnight polysomnography: Electroencephalogram (EEG), c lcctro-oculogram (EOG) and submental clectromyogram (EMG ). airflow, movement of the chest and abdomen (Respi trace ). arterial oxygen satu ration (Sa02, by Ohmeda Biox 3740 pulse ox irneter) , transcuta neous ?CO2 and e lectrocardiogr:irn (ECG ) were all monitored. Movement of' the left and right leg were recorded independent ly from the anterior tibia lis EMG via surface e lectrodes. A ll variables were continuously recorded on a po lygraph (Model 78E. Grass Instruments. Massac husetts) at a paper speed of I 0 mm/s. Transcutaneous partial pressure of carbon dioxide (?CO2 ) was disp layed on a slow recorder (paper sp1.:ed 20 cm/h) synchronized to the Grass polygraph.
Polysomnograms were scored manually and sleep stage, and arousa ls were determined by establi shed criteria us ing the EEG. EOG and EMG (4). Period ic leg movement. were scored if they occurred independently of an arousal from sleep and were part o f a series or fo ur or more consecutive move ments las ti ng 0.5 to 5 .0 s wit h an intermovement interval of 5 10 90 s (5 ). CSR was defined as periodic breathing wit h centra l apnea or hypopnea al ternat ing with hyperpnea in a crescendo/descrescendo pattern . and the duration o r CSR
70
EEG),,.,.,...,.,,.~.N,,\J.i.µNly...,.,r".~•/\___..,.,.,~,.--\~_,,..,,,,, EEG""'"-.;,,,~i,f.Jr,A-.'f.,"""'-.~~,..._,,,,.,..__.._,J..,.,._,,,~,,.,, ....... ,,.\~ EQG .................... ~,........,, .... ..,,.-'-r~v ',·.,·····'·· .. 1,),~ ... \---·-.,. .... Y .. , .... ..,_,r.,""'-"-.,1"' . .., ..... .,,, ... _,,._._,.,,."',J, ... .
EMG--~~V~ RAT'.......-~~~~~~~.---~~~~~~~ ~~--LAT'~~~~~-~~~~~~~~~~~~~~
,_r •
ABO -- .... ,,,.--.._,.- ... /', "'. ., • --..J "'~ --v-1~ r-..... ,.. ,,__,\. __ ~
--- " \s/ \. \ \ Jv . 1\/\.i, SUM
FLOW ~ - ____..... -o~--- --~- -~ -- TIME (minutes) ---~----~---1.0
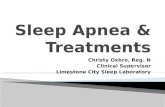
Figure I) 011c 111i11111e rif 11011rar1id eye 111m·c111c111 .1/cc1i dc111011s1ru1-i11g paradoxical hrea1h i11g fo //ou·cd /J.1· /1_1·1wrp11ca iri1/1 11 crescemloldccrcscel/(/o 11a11cr11. EEC l:Jcctm c11cep lw fngro111 ; L'O , £/cc1m-oculogra111 ; EMC Su////1c1110 / e/cc/m111yo1!J<llll ; RAT w1d LAT Righi a11d lefi a111erior 1i/Jia/i.1· EMC; CW Ches/ ll'u lf 111m ·e-111e111; ABD Abdo111i11al 11 •af/ 11101 'C111c111; SUM S11lll rf CW olld AB!): EKG £/curocardiugrw11; Sa02 Ox\'ge11 sat1maioll: FLOW Ai1:flou· {I / //OS I' {/li ef 11 /(} //(/t
was expressed as a percentage of the total s leep time (TST). Mean oxygen saturation during sleep was cale ulated by averaging the high and low Sa0 2 for each 30 s epoch . Mean transcutaneous ?CO2 (1C02) duri ng sleep was calculated from the average 1C02 over 36 s intervals.
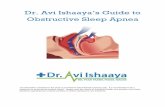
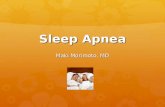
The overn igh t sleep st udy revealed severe sleep apnea. period ic leg movements during s leep and rap id atri a l fibri llation (Table I). During nonrapiJ eye movemen t (NREM ) sleep, there were features hoth of OS J\ , man ifested by rib cage paradox , and CSR wit h a classic crescendo/decrescendo appearance (Figure l ). During rapiJ eye movemen t (REM ) sleep, apneas were clearly ob tructive without ev idence of CSR (Figure 2 ). Apneas were 30 to 40 s long during NREM sleep and up to 65 s long during the brief peri od o f REM slee p. They were assoc iated with seve re hypoxcm ia a nd sleep d isruptio n. T ranscu taneous ?CO2 was low duri ng both wakefulness anJ sleep. The patient was im med iately placed on nasa l continuous posit ive airway pressu re (CPAP) and a repeat s leep study de monstrated that IO cmH20 nasal CPAP corrected upper ai rway obstruction anJ maintained satisfactory oxygen saturat ion Juring sleep. Fu rthermore. once the uppe r airway was stabilized by na al PAP. CSR became more appare nt wi th a typica l crescendo/dec rescendo appearance (Figure 3). Th is occurreJ on ly duri ng NREM sleep and was assoc iated with mi Id oxygen desaturation to between 85 and 90%. The patient continued to have frequen t periodic leg movements during sleep and rapid atrial fibri llation. Pulmonary function : Spirometry showed a vit al capacity of 3.~ L (78% predicted). and a forced expiratory vo lume in I s (FEY 1) of 2.54 L (88% predicted). w ith a normal inspiratoryexpiratory fl ow-volume loop. Lung volumes (body plcthysmography) were: total lung capaci ty 5 .74 L (87% predicted ).
Can Respir J Vol 2 No 1 Spring 1995

EEG--~~..r-EEG._:,.'J.,.,/•..,,.._. __ ~~~ EOG·--· .... .,r '· . . r; .r... .... : .. ~.,..\_.. ",'Y"·~.-./~._ ,, ... ,r..,, . .1,/~ .. J"-·~./\ ,v\,,,, •. ~-,.~,,., EMO- · · ---.---- ·'. .. i ---·------~~,._._...,._____,,___ RAT~...._~~--~~--~----~~--~ LAT--·-··-+ -
cw ABD
SUM
FLOW 0 -· .
- _____ j\J,._r,-..r,._,~
- TIME (minutes) ~ .0
Figure 2 ) 011e 111i11111e of mpid ne 111 m·e111e111 sleep de111011.11ra1i11g obs1mc1il·,· 111111m. l:'FG Elcr-1roe11 cephalogra111; EOG Electru-ont· logrw 11: L'M(; Su/1111 e11wl electro111_rngm111: RAT and LAT Right <1llll lefl a111crior 1ihi11/is F:MC: CW hes/ 1rn /l 11w1•e111t'III; ABD Abdo111i-1111I mill 11101 ·e111e111: SUM S11111 of' W a11d ABD: EKG Elec1rornrdiogn 1111: Sa02 Oxygm sa111rutio11: FLOW Airfl ,m· at nose a11d 1//() !(/ /,
funct ional residu al capacity 2.97 L (77% predic ted ). and re sidual volu me 2.30 L (93'/o pred ic ted) : exp iratory reserve Yol ume was 48% of pred icteu. presumably due to the pa-1 il' nt's morbid obes ity . Single-breath carhon monox ide uptake was 20.9 mL/mi n/mmHg (78% pred icted). and 98'7£predicted when correcteJ for single-breath lung volume. Arterial oxygen saturation by ear oximetry was 95 % at re.,t with no L·hange du ring sta ir cl imbing. Cardiac function: A 12- leaJ ECG revealed at ria l 11bril la t ion with a ven tricular rate o r 150 beats/min. Transthoracic echocartli ography revea led a Ji lated le rt ven tricle with severe global hypokinesis. Left ventricular ejection fraction was est imateJ between 20 and 30'/c, (normal greater than 60%). T his was confi rmed hy radi onuc li de ang iography. which revealeJ a left ventricu lar eject ion fraction of 16%. In aJJ ition, echocan.liography rl' vea led that the ascending aorta was Ji lated, and aortic d issection was suspected . Radiology: Chest radiography showed caruiomegaly and an anterior med iast inal mass (Figure 4). Further eval uat ion by computerized tomography confirmed the presence o r a very large dissect ing ane urys m in the ascend ing aorta . Operation: Surgical repair was recommended since it was felt there was a signific1nt risk or aortic rupture . Fol lowing a midli ne sternotorny. a 12 u11 d issecting aneurysm of the ascending aorta was rou nJ that was compress ing the vena cava and displac ing the heart inferiorly and lateral ly to the left. The su rgeon al so reported evidence of old pericard itis . A Dacron tube graft replaced the abnormal aorta, and once the aneurysm was removed, the heart moved back to a normal position. Patho logica l exam inat ion (11' the resected aorta subsequent ly revealed a J ouble-barre l lumen w ith fibro intimal hyperplasia cons istent with chron ic metl ial wall dissection.
Can Respir J Vol 2 No 1 Spring 1995
Sleep apnea and aortic dissection
EEG-.,,._-.Jr,~._,..,~._...,.,..,;~ EEG..,....,',t-,i..,.-,.,.,,,.,_.~,·~.,.,..J.~"'•1'VJi·,~ ~,-· EOG--' .. 1.""""'-·,,._,___,..._----.,/~
EMu------RAT·-------~~~~~.......-~~~w--~~ LAT--- -- - ~ llP' -~
cw '!\( (\
ABD---~~ J\.J\J\J,.,\J \J1~ 1\ ' ', !\ /\ \ ( I\
SUM f\.; ', "1' ' I I \J '\__
EKG .... ·11ll.l(IJ.J!,JJ,1(1J,wl.JJ.ll,l(~~ll,l(il,l(ill\!Wil,u1JUU1J1uw1uuw111u1wu1uHHu1uuwmuw~llJ.ll,l(JJµ -- 100 - - - ----Sa02 (%) so
o-~-~~----·TIME (minutes) ~---- -~~~1.0
Figure 3) One 111i11 111e o( 11011 mpid ere 1110 1·e111e111 sleeJ) on na.rn l co111 i1111u11s positil ·,· ainl'II_\' pressure de111011s1ra1i11g ce111ra l 11p11ea fo ll01 1·ed b1' /1_1pe17meu 11'i1h a c/'/'s ,·nuloldecresce11 do pal/em. EEC Electroe11ce11lw log rw 11: EOG Ell'.-t rtHIClflog m111: EMC S11 /m1rn111I electro111rogrw11: RA T (1/ 1(1 LAT Right a11d le.ft anlerior tihialis EMC: CW Chest ll'all 111 m ·,,111e,11: AfJD Abd,m1i11ul 1m ll 11 111 1·e111e11 1: S UM Sum of CW mu/ AfJD: EKG E/ec1rornnliogm111: Su(h 0.rrg{'// Silllfratirm
Progress: Postoperat ively. the pat ient diureseJ rapid ly anJ there was a ma rked reduction in his faci al size. In re trospect. it was apparent that he had sign ificant superior vena caval obstruct ion. He reverted spontaneous ly to sinus rhythm. Resting rad ionucl ide ,mg iography two weeks foll owing surgery revea led a le ft ventri cu lar ejection fraction o r 549'1' with persistent left ventricu lar en large ment. He was discharged from hospita l 25 days fo llowing his surgery on .:nalapril I 0 mg Jaily, enteric coated acetyl sa licylic acid. anJ sa lt and ca lorie restriction. Congest ive heart fa il ure hatl resolved and he did not requi re d iure tic therapy.
Over the next year. he cont inued to use IO cmH20 nasa l CP P during sleep. There was a dramatic improvement in his sleep qual ity and dayti me function w ith complete reso lut ion or hypcrsomnolence. Although he remained obese, hi s weight fe ll to 118 kg (body mass index 38.5 kg/m~l with a reduction in his nec k circumference to 47 cm. Cl inical ly. he rrn1ained free o f heart fail ure although atrial ribrill ation returned, requiring treatment with d igox in and amiodarone. which converted him to normal sinus rhy thm. He maintained norma l left ven tricular systol ic function although he had pers isten t impairment of lert ventricu lar diastoli c fun ct ion. which was attribu ted to hypertension anJ previous caruiac hi story . Overnight polysomnography was repeated 13 mon ths fo llowing repai r or his aortic ane urysm (Table I ). T he study was pe1formed on and off nasal CPAP. Off nasal CPAP, he conti nueJ to have signific.1nt OSA with assoc iated hypoxemi a anJ sleep d isru ption. Howe ver, there was no ev idence o f CSR and tC02 wa, clevateJ compared with the relat ive hypocapn ia he experienced duri ng the fi rst sleep study. During the second part of the st udy. his OSA was con-ected by 10 cmH20 nasa l CPAP. The pat ient re mains well three years fo llowing his init ia l presenta tion.
71

HANLY AND FORD
Figure 4) /'n '"/'Cmli1 ,. 1io.1?1'mc1111erior (left) a11d /arer,il right) 111<'.1/ ,,uliogml'hs de111011srrati11g cardio111egu/_1· 1111</ " large l/1/ lerior l/l('(/ia .11 i11a l 11,a.1s
DISCUSSION The patien t described he re had cl iniL·,d and polysonmo
graphic evide nce of both OSA and CSR . The long history o r loud snoring, witnessed apneas and excess i v1.: dayti me sleepi
ness are cons isten t wi th OSA. and the recent his tory o f congestive heart failure pred isposed the patient to de velop CSR. Al though in termittent paradoxical breath ing was pre
sent throughou t the s leep study. obstruc ti ve apnea was most obvious duri ng REM s leep (Figure 2 ). the sleep stage du ring which upper airway occl usion is most likely to occur. CSR was only seen during stage I and 2 NREM s leep (Figure I) and became more obvious once the upper airway was stabilized by nasa l CPAP (Figure 3). The pathogenesis of CSR is close ly re lated to destabil izatio n of" the metabolic control system. which is the primary regulator or venti lat ion during NREM sleep (6) . Hence. the rel ationshi p between sleep stage and s leep-disordered breathing in our patient is cons istent
with the current understand ing o f the pathogenes is o r these two d ifferen t fo rms o f s lee p apnca.
T he uni que feature of this case is the potent ial interactio n between sleep apnea and aortic d issec tio n and the ro le they may have played in each others · pathogenesis. It has be n proposed by m1r c ardiovascubr colleagues that the pat ient·s aortic di ssect ion started during the episode of acute pericardi tis seven years prev ious ly . In addit ion. he was hyperte nsive.
which is a know n ri , k fac tor for the deve lopment o f aort ic di ssection. Howeve r, the re was also clinical a nd po lyso mnographic ev idence of OSA which. hi storica ll y. had been presen t for 40 years. Obstructive apnea is associated with large negative intratho rac ic pressure swings due to force d inspirati on against an occluded upper airway (7). Each apnea
generates a substant ial pressure g rad ient across the le ft ventricle and aort ic wall. Obstruc ti ve apneas are also known to cause acut e elevation o f system ic blood pressure during sleep (8 ). It is possib le that this repetitive increase in the pressure grad ient across the aortic wall and the inte rmittent rise in systemic blood pressure over many years may have extended
72
the aortic dissec ti on that commenced duri ng the episode of acute pericard iti s .
In addi tion to OSA. the patiL'.11! al so had polysomnograph ic ev idence llf CSR (Figures l and 3 ). Si nce the pat ient also had congcsti ve heart fa il ure. it is reasonable to assume that his CSR was caused by le ft ventricular dysfunction. T he re were many risk factors fo r the deve lopment of le rt ve ntri cular dysfunction in this patient includi ng hyperten
sion. obesity. alcohol consum pt io n and prev ious perica rdi tis (l)). In additi on, OS A may have exacerbated pre-ex isting left
\ entricubr dysfunction Ol although it is un like ly to have caused it de novu ( 10). However. we believe that the most significant GtUSL' of impaired left ve ntric ular functi on was ve na ca val obstruction caused by a large d issecting aneurysm of the ascending aorta. It is likely that venous return was
cri tically reduced not only by compression o f the vcna cava but also by di sp lacement o f the heart. T his was supported hy the in traoperati w findi ngs, clinical features o f su perio r vcna caval obstruct ion and the rapid cliniL·al and echocardiographic improvement fo l lowing surgery. The pal ien t · s con t i 11 -
ued improvemen t and the absen e of CSR three YL'ars fol lowing surge ry furt he r support these suggest ions.
CONCLUSIONS We report a patien t wi th L'Oex ist ing dissec ting aneurysm
uf the aorta and sleep apnea. We bel ieve that vcna caval obstruction assoc iated with the aneurysm caused CSR during sleep. Furthermore, we speculate th at long-standing OSA may have cont ributed to the deve lopment of aortic di ssec tion.
ACKNOWLEDGEMENTS: The authm, than~ LI\ ic' <.i :1r,·i;1 !or typi no the manuscript.
REFERENCES I . Cherniak NS. LongobarJo GS. Cheyne-Stokes breathing: ;111
instab ility in phys iolu~ic conlrul. N Engl J Med 1973:288:952-7 .
Can Respir J Vol 2 No 1 Spring 1995

2. Yamashiro Y. Krygcr M. Sleep in heart failure. Sleep I <)tJJ: 16::i 13-23.
3. Malone S. I.i11 P. Ha ll 0w.1y R. Rutherrord R. Xie A. Hradley TD. Ohstructiw sleep apnca in pati ent;; with dila ted cardiomyopathy: effect s or continuous positive airway prl'ssun:. Lancet 199 1 :338: 1480-4 .
4. Kaks /\.. Red1tschalfrn A. eds . A M,rnual of Standardized Tcrn1inology. Tl·,fo1iques and Scori ng System for Sleep Stages of llu111an Suhjl'l'tS. NIH publi ca ti on no. 204. Be thesda: National Institute· of Neurol ogical Disease and Blindness, 1968.
5 . Ameril'a11 Sleep Disorders Association. The lntcrnati on,11 Classification of Sleep Disorders: Diagnostic and Cndin,t' Manual. l.awn:nce: Allen Press Inc, 1990.
6. 1 lanly P. Zuhl·ri N, Gray R. Pathogenesis of Cheyne-Stokes
Can Respir J Vol 2 No 1 Spring 1995
Sleep apnea and aortic dissection
respiration in patien ts with congesti ve heart l'a ilure: rela tionsh ip to arterial !'CO2. Chest 1993: I O..i: I 079-8+.
7. Ma ,rnne 0 , Belli a Y. Ferrara G. Mil one F. Romano L. Salvaggio A, et al. Transmural pressure measurements . l111porta1Kc in the assessment or pulmonary hypertension in obstruct ive sleep apncas. Chest 1989:95:338-42 .
8. Parish JM . Sheppard JW. Cardiovascular effects of sleep J i orders. Che. t 1990:97 :220-6.
<J. Braunwald E. Clinical manifestations of heart l'ailu re. In : Brau nwald E. ed. Hc.1rt Disca,c. Philadelphia : WB Saunders Co, 1988:47 1-8+.
I 0. Han ly. P. Sasson Z. Zuhcri N. Al<ll'rson M. Ventri l'ular functi on in snorers and patients with obslructivc sleep ap11l·;1. Chest 1992: I 02: I 00-5.
73

Submit your manuscripts athttp://www.hindawi.com
Stem CellsInternational
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
MEDIATORSINFLAMMATION
of
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
Behavioural Neurology
EndocrinologyInternational Journal of
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
Disease Markers
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
BioMed Research International
OncologyJournal of
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
Oxidative Medicine and Cellular Longevity
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
PPAR Research
The Scientific World JournalHindawi Publishing Corporation http://www.hindawi.com Volume 2014
Immunology ResearchHindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
Journal of
ObesityJournal of
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
Computational and Mathematical Methods in Medicine
OphthalmologyJournal of
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
Diabetes ResearchJournal of
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
Research and TreatmentAIDS
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
Gastroenterology Research and Practice
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
Parkinson’s Disease
Evidence-Based Complementary and Alternative Medicine
Volume 2014Hindawi Publishing Corporationhttp://www.hindawi.com