Sleep and sleep disorders
73
Sleep and sleep disorders Andy Montgomery
description
Sleep and sleep disorders. Andy Montgomery. Talk Outline. Normal Sleep Diagnosing sleep disorders Insomnia Hypersomnia Parasomnias Circadian sleep rhythm disorders Psychiatric disorders and sleep Pharmacology and sleep. Normal sleep. 1/3 of adult lives asleep Role poorly understood - PowerPoint PPT Presentation
Transcript of Sleep and sleep disorders

Sleep and sleep disorders
Andy Montgomery

Talk Outline
• Normal Sleep• Diagnosing sleep disorders• Insomnia• Hypersomnia• Parasomnias• Circadian sleep rhythm disorders• Psychiatric disorders and sleep• Pharmacology and sleep

Normal sleep
• 1/3 of adult lives asleep
• Role poorly understood
• Sleep deprivation consequences– Cognitive impairment– Hormonal rhythm disturbance– Rebound after deprivation

Normal sleep
• Quantity– 7-8 hours– <6 increased reports dissatisfaction
• Control by 2 processes– Circadian process– Homeostatic process

The Circadian process
• 24 hour cycle– Many cells and organs
• Principle time-keeper:– Supra-chiasmatic nucleus
• Influenced by light and temperature• Some sleep disorders associated with genetic
variant • Determines owl/lark

The homeostatic process
• Aka recovery drive to sleep• Increases in proportion to time awake
• 2 processes interact– Generates
• Post-lunch dip• mid-evening activity
• Other influences– Arousal, relaxation, anxiety

Physiology of sleep control
• Orexin (hypocretin)– Peptide hormone– Promotes wakefulness
• Wakefulness– Ascending arousal system dominant
• Sleep– Inhibition of arousal systems

Sleep structure
• Polysomnography– Simultaneous record
• EEG• Muscle activity• Eye movements
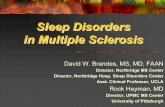
• 4-5 cycles – Quiet sleep alternating with REM
• Increased duration through night

Hypnogram

Sleep structure:quiet sleep
• 4 stages• 1: dozing “just resting eyes”• 2: deeper, occasional jerks, reduced HR &RR• 3&4: slow HR & RR
• EEG• Progressive slow synchronous activity
– Reduced cortical arousal– Increased thalamo-cortical synchrony

Sleep structure:REM
• Rapid onset
• EEG “awake”
• Jerky eye movements
• Muscle paralysis
• Autonomic arousal
• Usually several short wakenings

Stage EEG Eye movt EMG
Wake Low-amp, mixed some alpha
Many varied, usually fast
High
1 Low amp, mainly irregular theta
Slow rolling lateral movt
Slightly lowered
2 Sleep spindles, K complexes low amp theta
None Lowered
3 High amp delta,K complexes
None Low
4 As 3 None Low
REM Low amp irregular, saw-toothed
Rapid jerky, lateral
absent

Age variants
• 24 hour rhythm– Develops at 3/12
• High levels REM in childhood
• Aging– Time awake increases– Slow wave reduces– GH release reduces

Dreaming
• Only remembered if REM followed by wakefulness
• Occurs in – REM
• Bizarre, storyline
– Slow wave

Sleep and cognition
• Sleep enhances memory consolidation
• Transfer from short-term to long-term memory– Dependent on hippocampal activity– Sleep deprivation associated with reduced
hippocampal neurogenesis

Sleep disorders
• Diagnosis– Take sleep history– Questionnaires and diaries can be helpful– Sleep centres: polysomnography, actigraphy, video
recording
• Classified in ICD 10 and DSM IV– 3 categories
• Insomnia• Hypersomnia• Parasomnia

Questions to ask
• Time:– Bed, getting up, ?regular pattern– Falling asleep
• Waking episodes
• Quality (Pittsburgh Sleep Quality Index)
• How many bad nights/week?

Questions to ask
• Naps during day• Mood• Motor activity during sleep• Behaviour during sleep• Day-time somnolence (Epworth sleepiness
scale)• Snoring• Use of drugs

Investigations
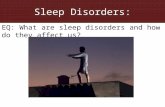
• Actigraphy– Monitors movement via wrist band– Can be used over days- weeks– Sleep- less movement
• Overnight video recording

Actigraphy

Polysomnography
• Terms– Time in bed– Sleep onset (to stage 1 or 2)– Sleep onset latency– Sleep period: onset to wake– Total sleep time– Number of wakenings– Sleep efficiency (total sleep/time in bed)– Wake after sleep onset– REM onset latency– Time in each sleep stage

Insomnia
• Major public health problem
• 10-15% adults persistent insomnia– Low quality of life– Increased absenteeism– Physical illness– Mental illness

Insomnia
• Symptoms– Too little– Too long to go to sleep– Poor quality– Unrefreshing– Impaired daytime function
• Daytime sleepiness uncommon (circadian rhythm disorder)

Insomnia
• Two main types:– Sleep onset insomnia– Sleep maintenance insomnia

Insomnia - precipitating factors
Sleep wake cycle•jet lag•Shift work•Irregular routine
Psychological stress•Bereavement•Increased arousal•Worry about alarm•Noise•children
Psychiatric disorder•Depression •anxiety
Pharmacological-blocker•AD•Caffeine•Alcohol•Stimulants•Withdrawal
Physical•Pain•Pregnancy•Illness (cardio/resp)•Urinary
Short term insomnia

Insomnia- perpetuation
Short term insomnia
Long term insomnia
Anxiety about sleep
Good sleep
Poor sleep habitsGood sleep habits

Insomnia- treatment
• Establish primary diagnosis
• Acknowledge distress
• Treat precipitating factors/primary cause
• Educate about trigger factors and reassure
• Establish good sleep habits

Insomnia- treatmentHypnotics
• Act at GABA-A benzodiazepine receptor
– Generally safe and effective in short term
– SE• Muscle relaxation• Memory impairment• Ataxia
– Potentiated by EtOH– Avoid long term px

Insomnia- other drugs
• Sedative AD– Mirtazapine– Agomelatine
• Melatonin
• Anti-histamines

Psychological treatments
• Sleep hygiene– Regular hours– Daytime exercise– Morning daylight exposure– Reduced daytime napping– Avoid stimulants– Bed-time routine

Psychological treatments
• Behavioural techniques– Stimulus control
• Avoid clock watching• Don’t watch TV• Don’t stay in bed if awake
– Sleep restriction– Relaxation training

Psychological treatments
• Cognitive techniques– CBT
• Avoid negative thoughts associated with not sleeping
– Rehearsal and planning session– Paradoxical intent

Sleep restriction

Hypersomnia
• Feeling sleepy during day– Distinct from tired
• 37% adults a few days a month• 16% a few days / week• Main causes
– Fragmentation of sleep• Obstructive sleep apnoea
– Intrusion of sleep phenomena into wake• narcolepsy
– Disturbed circadian rhythm.

Obstructive sleep apnoea: symptoms
• Excessive daytime sleepiness• Loud snoring• Interruptions of breathing
– Resumes with loud gasp, violent movement
• Marital problems• Dry mouth, sore throat, headache• Depression
• Present in 0.5% men BMI >25

Obstructive sleep apnoea: treatment
• Weight loss
• Continuous positive pressure ventilation
• Consider modafinil if remain sleepy during day

Narcolepsy
• 3-4/10,000
• HLA DQB1*0602 (18-35% in controls)
• Symptoms– Sudden onset sleep– Sleepiness– Cataplexy– Hypnogogic/pompic hallucinations– Poor nocturnal sleep

Narcolepsy
• Cause– Lack of orexin neurones/release in
hypothalamus– Possible cross-reaction autoimmune disorder
after infection in adolescence
• Diagnosis– Clinical picture– Reduced REM latency

Narcolepsy
• Treatment– Education– Day-time naps– Drugs
• Daytime sleepiness– Modafinil/dexamphetamine
• Cataplexy– 5HT enhancing drug: SSRI, clomipramine
• Night-time sleep disruption– Sodium oxybate

Other causes of daytime sleepiness
• Idiopathic hypersomnia
• Kleine-Levine syndrome– Rare, reversible disorder– Hypersomnia +/- excessive eating &
hypersexuality– Onset adolescence– Typical duration 4-8 years– ? autoimmune

Parasomnias
• Unusual behaviours occurring during sleep
• Exacerbated by anxiety
• Variable drug treatments

Night terrors
• Recurrent episodes of abrupt waking usually first 1/3 of night
• Intense fear and autonomic arousal
• Unresponsive to comforting
• No detailed recall
• Significant distress

Night terrors
• Occur in 30-40% children
• Generally resolve with aging
• Can recur at times of stress
• Comorbidity with anxiety common
• Often run in families

Night terrors
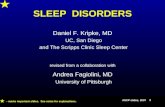
• Cause– Genetic component– Incomplete arousals from SW sleep
• Treatment– Clonazepam– Paroxetine (immediate effect)

Night terrors hypnogram

Parasomnias -SWS
• Sleep walking– Automatic behaviour– No recall– 15-20% lifetime prevalence
• Confusional arousals– Semi-purposeful movements
• Sleep bruxism• Sleep talking

Parasomnias -REM
• Nightmares– Wake oriented (vs night terrors)– Association with depression and PTSD– Psychological treatment
• Guided imagery- rehearse happy endings
• Sleep paralysis– Waking with fear, foreboding, unable to move– Common-25% experience– Treatment- good sleep hygiene

Parasomnias -REM behaviour disorder
• Violent, short duration • Several episodes/night• Can wake • Remembers dream
– Violent unpleasant content
• Strong association with subsequent IPD OR LBD (45-85%)
• Made worse by AD• Treat by making sleep environment safe

Circadian rhythm sleep disorders
• Jet lag– Worse for travel east (natural clock 24.5hr)– Melatonin may help
• Delayed sleep phase syndrome– Unable to sleep before 2-3AM– Preferred wake time after 10 AM– Causes insomnia and sleepiness on work days
• Advanced sleep phase disorder– rare

Circadian rhythm sleep disorders
• Non 24hr circadian sleep disorder– Sleep pattern advances daily– Most common in congenitally blind
• Irregular sleep wake rhythm – Seen in dementia- ? Loss of melatonin
neurons in SCN
• Shift work sleep disorder

Sleep and depression
• Sleep disturbance common in depression– Almost 100% some disturbance
• Depression common in insomnia*– 14-21% c/o insomnia depressed– 9% c/o hypersomnia depressed– 1% no sleep problem depressed– Depression most common diagnosis
associated with insomnia
*Epidemiologic study of sleep disturbances and psychiatric disorders. An opportunity for prevention?JAMA. 1989 Sep 15;262(11):1479-84.

Sleep complaints in mood disorders
• Initial insomnia• Frequent/extended wakening• EMW• Vivid dreams, -ve emotional content• Lack of adequate rest
• Hypersomnia (BPAD depressed, SAD)
• Reduced sleep (mania)
(MDD)

Subjective effects of AD on sleep
• Few good studies– Mismatch between subjective sleep and
objective measure– AD may affect subjective sleep

Polysomnography findings: MDD
• Initiation and maintenance– ↑sleep latency– Frequent awakenings– EMW
• Reduced SWS– Absolute and relative– Fewer delta waves
• REM– Reduced REM latency– ↑REM in first half night– More eye movements

Polysomnography in at-risk population
• Two 1st degree relatives with MDD
– Reduced SWS in first NREM sleep cycle
– Increased REM density first REM period
J Affect Dis 2001 62:33-

Functional imaging: depression• REM
– Increased activation wake vs sleep • Midbrain reticular formation• L hemisphere cortical regions: (DLPFC, FEF)• Limbic/paralimbic regions: (hipp, basal forebrain,
ACC, MPFC)
• NREM– Increased whole brain metabolism

BPAD & dysthymia
• BPAD– Similar findings to MDD (depressed & manic)
• Dysthymia– Minimal changes

Treatment effects
• Pharmacological tx most effective in pt with sleep architecture disturbance
Which depressed patients will respond to interpersonal psychotherapy? The role of abnormal EEG sleep profiles.Am J Psychiatry. 1997 Apr;154(4):502-9.

SSRI effects on REM
• Reduced REM• Increased REM latency• Effects within 2-3 days• effects mediated ↑ synaptic 5HT • ?5HT1A
– 1A knockout mice no effect of citalopram on REM latency
– 5HT1a agonists reduce REM– Tryptophan depletion removes SSRI REM effect

SSRI effects SWS
• Increased time Stage1• Increased awakenings• Increased time awake
• Effects diminish over ~5/7 (except fluoxetine)
• ?5HT2 mediated– Agonists disturb sleep – Antagonists promote sleep

TCA effects
• REM: similar to SSRI
• SWS: – imipramine, clomipramine, desipramine:
increased sleep fragmentation– Amitriptyline: improve sleep healthy
volunteers, not in MDD • ? 5HT2 antagonism effect

MAOI
• REM– Phenelzine complete REM suppression
• 5HT mechanism- reversed by tryp. depl.• ?MAOB effect
– Moclobemide: minimal effect
• SWS– Increased sleep fragmentation

Other AD
• Mianserin– Suppressed REM– Reduced SWS fragmentation (?H1 blockade)
• Mirtazepine, trazadone, nefazadone– Increased REM onset latency– Reduced fragmentation (5HT2 antagonism)
• Reboxetine– Minimal effect on REM or SWS
• Venlafaxine– SSRI like effects

Other AD
• Agomelatine– 5HT2c antagonist
– MT1/ MT2 agonist
– Effective AD (antidepressant efficacy of agomelatine: meta-analysis of published
and unpublished studies BMJ 2014;348:g1888)
– Increased SWS, reduced sleep latency
– No effects on REM latency, total REM or REM densityThe International Journal of Neuropsychopharmacology (Impact Factor: 5.64). 11/2007; 10(5):691-6.

Effects of AD on HAM-D sleep items
Drugs. 2005;65(7):927-47.

Change in perception of sleep quality with nefazadone
Psychiatry Res. 2003 Sep 30;120(2):179-90.

AD adverse effects on sleep
• Restless legs
• Eye-movements in SWS
• Bruxism
• Nightmares
• Withdrawal nightmares

Sleep deprivation effects
• One study– [123I]IBZM SPET– Increased DA release after sleep deprivation

Sleep and schizophrenia
• Rarely predominant complaint
• Disturbance may precede relapse
• Insomnia occasionally very severe
• Studies contradictory– Variety of definitions of schizophrenia– Older patients included – Medicated patients

Unmedicated patients
• Stage 2 latency increased
• Increased nocturnal wakenings
• Reduced sleep efficiency
• ? REM latency reduced

Medicated patients- typical antipsychotics
• Stage 2 latency increased
• Reduced stage 2 & 4
• Total sleep time reduced
• Reduced sleep efficiency
• Reduced REM latency
• Reduced total REM sleep

Medicated patients- atypical antipsychotics I
• Olanzapine– Increased total sleep– Increased sleep efficiency– Reduced stage 2 latency– Reduced total REM
• Risperidone– Minimal data– Increased SWS

Medicated patients- atypical antipsychotics II
• Clozapine– Increased total sleep– Increased sleep efficiency– No effect on REM– ? Rebound insomnia after abrupt stop