Lobular Breast Cancer: Common Problems in Diagnosing LCIS in Core
Upload
deepak-ningombamCategory
view
217download
0
8/3/2019 SledgeJr 2002 Current Problems in Cancer
http://slidepdf.com/reader/full/sledgejr-2002-current-problems-in-cancer 1/54
Angiogenesis and AntiangiogenicTherapy
What makes a cancer a cancer? What allows a cancer to grow? What
allows a cancer to spread outside its organ of origin? What allows
it to colonize the hostile environment of a distant site? These are,
as all will recognize, simple questions with inordinately complex an-
swers. The malignant phenotype has been the subject of decades of study,
and we have glimpsed its broad outlines only in recent years.
Growth of solid tumors in both the primary and metastatic sites depends
on angiogenesis, the formation of new blood vessels, to nourish the
tumor. In pioneering work by Folkman,1 cancer cells implanted in
vascular sites in animals grew rapidly and formed large tumors. In
contrast, cells implanted in avascular sites were unable to form tumor
masses 1 to 2 mm in size. This work led Folkman1 to hypothesize that
angiogenesis was obligatory for tumor growth.
It has become increasingly certain that angiogenesis, or new blood
vessel formation, plays a central role in the malignant phenotype. As we
will discuss, angiogenesis is activated early in carcinogenesis. The
presence of new blood vessels allows for the growth of local tumors,
offers them a royal road to other parts of the body, and feeds their growth
in distant sites. Unsurprisingly, then, new blood vessel formation has been
shown to be an important prognostic factor in many tumors in human
beings.
This realization has led to the novel and important concept of angio-
genesis as a potential therapeutic target (indeed, targets, as we shall
discuss below). This therapeutic potential is now approaching practical
realization in the clinic, with the reasonable expectation of commercially
available products in coming years. Therapeutic targeting is based to a
significant extent on our growing understanding of the biologic factors
relating to angiogenesis. Although the excitement surrounding this
approach is certainly justified by the ubiquity and centrality of angiogen-
esis to the metastatic phenotype, the development of these novel agents iscertainly not lacking in potential concerns regarding drug resistance.
Curr Probl Cancer 2002;26:1-60.
0147-0272/2002/$35.00 0 56/1/122105
doi:10.1067/mcn.2002.122105
6 Curr Probl Cancer, January/February 2002

8/3/2019 SledgeJr 2002 Current Problems in Cancer
http://slidepdf.com/reader/full/sledgejr-2002-current-problems-in-cancer 2/54
The Process of AngiogenesisBlood vessel formation consists of two related but separate processes,
vasculogenesis and angiogenesis. Vasculogenesis, which occurs duringembryogenesis, involves the differentiation of endothelial cells from
precursor angioblasts and the subsequent formation of a capillary plexus.
Angiogenesis consists of the formation of new capillaries through
sprouting or splitting from preexisting vessels (both embryonic and
adult).
Under physiological conditions, angiogenesis involves initial activation,
including sequential basement membrane degradation, cell migration,
extracellular matrix invasion, endothelial cell proliferation, and capillarylumen formation. The newly formed microvasculature matures through
the process of resolution, which includes inhibition of proliferation,
basement membrane reconstitution, and junctional complex formation.2
In addition, newly formed vasculature recruits periendothelial cells
(pericytes for small capillaries and smooth muscle cells for larger vessels)
to provide support. These periendothelial support cells are known to act
as a survival factor for endothelial cells.3,4
Physiological vascularization and angiogenesis are tightly regulatedprocesses, governed by specific paracrine signals. Although many regu-
lators of vascularization and angiogenesis have been identified (Table 1),
gene knockout studies in mice have identified a few receptor tyrosine
kinase complexes as being crucial for normal vascular development.
These include the vascular endothelial growth factor receptors (VEGF-R1
and R-2, also known as Flt-1 and Flk-1/KDR), and Tie-1 and Tie-2.
Each of these knockouts results in embryonic lethality with vascular
defects (reviewed in Hanahan5). VEGF-R2 knockouts lack endothelialcells and a developing hematopoietic system, suggesting that VEGF-R2
plays an important role in conversion of angioblasts to endothelial cells.
VEGF-R1 appears crucial to the formation of functional vascular tubules
but knocking it out does not affect the abundance of endothelial cells.
Tie-2 knockouts lack mature vessels, branching networks, and proper
organization into larger and smaller vessels. Tie-1 signaling is thought to
be involved in control of fluid exchange across capillaries and in
hemodynamic stress resistance. Unsurprisingly, as discussed below, thesephysiologically important receptor tyrosine kinase complexes, in conjunc-
tion with their ligands, often play an important role in pathologic
angiogenesis.
In contrast to what is seen with physiological angiogenesis, tumor
microvessels frequently lack complete endothelial linings and basement
Curr Probl Cancer, January/February 2002 7

8/3/2019 SledgeJr 2002 Current Problems in Cancer
http://slidepdf.com/reader/full/sledgejr-2002-current-problems-in-cancer 3/54
membranes. They tend to be highly irregular and tortuous, with arterio-
venous shunts and blind ends being common. Blood flow through tumors
tends to be sluggish, and the tumor associated vessels leakier than
normal.6 Many (although by no means all) tumor vessels lack a support-
ing pericyte structure.3
Regulators of AngiogenesisThe presence of an angiogenic process implies the existence of
regulators of the process. These regulators, both positive and negative,
have been increasingly well characterized in recent years, and occur in
astonishing numbers (Table 1). In malignancy in human beings, the
balance between positive and negative regulators may play a crucial role
TABLE 1. Natural positive and negative regulators of angiogenesis
Positive regulators
VEGF (vascular endothelial growth factor)
Basic and acidic FGF (fibroblast growth factor)
Transforming growth factor
Transforming growth factor-1
Platelet-derived growth factor
Insulin-like growth factor
Angiogenin
Thymidine phosphorylase
Angiopoietin-1
Epidermal growth factor
HER-2/neu
Interleukin-8Leptin
Hepatocyte growth factor/scatter factor
Hypoxia-induced factor 1
Cyclooxygenase-2
Negative regulators
Angiostatin
Endostatin
2-Methoxyestradiol
Thrombospondin-1
Platelet factor IV
Tissue inhibitors of metalloproteinasesInterferon-
Angiopoietin-2
Troponin-1
Retinoic Acid
Interleukin-12
Vasostatin
Prolactin
Prostate specific antigen
8 Curr Probl Cancer, January/February 2002

8/3/2019 SledgeJr 2002 Current Problems in Cancer
http://slidepdf.com/reader/full/sledgejr-2002-current-problems-in-cancer 4/54
in angiogenesis and tumor progression.7 Although it is impossible to
discuss all of these regulators in detail, we will focus on several in eachcategory that have proved especially important from a biologic or
therapeutic standpoint.
Positive Regulators of AngiogenesisVascular Endothelial Growth Factor. VEGF plays an important role in
cancers in human beings. In breast cancer, VEGF is detectable at the
transition from atypical hyperplasia to ductal carcinoma in situ, suggest-
ing that its occurrence precedes tumor invasion and metastasis.8-10
Similarly, VEGF expression is found in preneoplastic Barrett’s esopha-gus.11 In contrast, VEGF expression does not occur in dysplastic
adenomas of the colon and only becomes apparent with the advent of
mucosal involvement of colorectal cancers.12
Numerous studies have examined the relationship of VEGF to clinical
outcome in cancers in human beings, particularly breast cancer (Table 2).
In general, these trials have suggested that VEGF is associated with
impaired outcome in patients with early-stage cancers, being associated
with worsened relapse-free and overall survival. The largest of thesetrials, recently reported by Linderholm et al13 at the 2001 American
Society of Clinical Oncology Meetings, suggested that VEGF is an
independent prognostic factor in breast cancer for both relapse-free and
overall survival in multivariate analysis. Its presence is correlated with
larger tumor size, steroid receptor negativity, the presence of mutant p53,
TABLE 2. Negative prognostic value of VEGF
Investigator PatientsNodal
StatusMethod
High vs low VEGF
(P value)
RFS OS
Toi 1994325 103 N/N IHC .039 NR
Toi 1995326 328 N/N IHC .01 NR
Obermair 199789 89 N/N IMA NS NR
Relf 1997237 64 N/N RNase .03 NR
Linderholm 200113 1307 N/N ELISA .034 .0017
Eppenberger 199847 305 N/N ICMA .001 NR
Gasparini 1999328 301 N IMA .05 .05
Gown 2001329 123 N4 IHC NR .006
Gasparini
330
260 N
IMA .001 .001Eppenberger 199847 190 N ICMA .04 NR
RFS , Relapse free survival; OS , overall survival; N , lymph node positive; N , lymph node
negative; IHC , immunohistochemistry; ICMA, chemiluminescence immunosorbent assay; IMA,
chemiluminescence immunoassay; ELISA, enzyme-linked immunosorbent assay, RNase ,
ribonucleotide protection assay, NS , not significant; NR , not reported.
Curr Probl Cancer, January/February 2002 9

8/3/2019 SledgeJr 2002 Current Problems in Cancer
http://slidepdf.com/reader/full/sledgejr-2002-current-problems-in-cancer 5/54
and poor tumor differentiation. In addition, Linderholm’s data suggest
that VEGF production is associated with an increased risk of brain and
visceral metastasis, a finding confirmed by Foekens et al.
14
Although perhaps best studied in breast cancer, the number of cancers
in which VEGF tissue expression has been correlated with impaired
prognosis is truly impressive and includes (but probably is not limited to)
bladder cancer,15 esophageal cancer,16 gastric cancer,17 prostate cancer,18
acute myelogenous leukemia,19 head and neck cancer,20,21 soft tissue
sarcoma,22 osteosarcoma,23 non-small cell lung cancer,24-27 papillary
thyroid cancer,28 cervical cancer,29,30 ovarian cancer,31 pancreatic can-
cer,
32
and glioma.
33
The literature surrounding this association is as vastas it is confusing, with great variation in technique, reagents, and scoring.
A significant number of these trials are characterized by small numbers of
patients and varying disease stage and histopathologic type. Taken
together, they represent impressive support for the relationship between
VEGF expression and patient outcome, yet are of uncertain value for the
practicing clinician.
Although most studies of the prognostic effects of the VEGFs have
focused on the parent (VEGF) ligand, emerging evidence suggests that
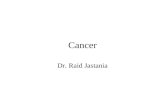
VEGF-B and VEGF-C may play a role in breast cancer (Fig 1). VEGF-B,
like VEGF, acts as a ligand for VEGFR-1, although not (unlike VEGF)
for VEGFR-2. In vitro data suggest that activation of VEGFR-1 by
VEGF-B is only weakly mitogenic for endothelial cells. A recent
publication by Gunningham et al34 suggests that VEGF-B over-expres-
sion is associated with lymph node metastasis but not angiogenesis. This
trial was not powered to determine the effect of VEGF-B expression on
overall survival.
VEGF-C is the ligand for VEGFR-3. This ligand-receptor complex isbelieved to play a role in lymphangiogenesis. Karpanen et al35 have
recently demonstrated that VEGF-C transfection of MCF-7 breast cancer
cells promoted the growth of tumor-associated lymphatic vessels, which
in the tumor periphery were commonly infiltrated with the tumor cells.
Related experiments in an orthotopic model demonstrated that VEGF-C
overexpression resulted in significantly enhanced metastasis to regional
lymph nodes and to lungs; the degree of tumor lymphangiogenesis was
highly correlated with the extent of lymph node and lung metastases.36 Itis unsurprising that VEGF-C is expressed in many invasive breast
cancers37 and that its overexpression is associated with lymphatic vessel
invasion and (in one small study) disease-free survival.38
Angiopoietin/Tie-2. The angiopoietin/Tie-2 ligand-receptor complex
also plays an important role in physiologic and pathologic angiogenesis,
10 Curr Probl Cancer, January/February 2002

8/3/2019 SledgeJr 2002 Current Problems in Cancer
http://slidepdf.com/reader/full/sledgejr-2002-current-problems-in-cancer 6/54
as discussed above. The regulation of the angiopoietins and Tie-2 are stillbeing elucidated. HER-2 signaling up-regulates angiopoietin-2, which
disrupts endothelial cell adherens junctions.39 Angiopoietin-1 is inversely
related to thymidine phosphorylase expression in human breast cancer.40
Angiopoietins and their receptor Tie-2 are expressed in numerous
human cancers, including prostate cancer,41 glioma,42 gastric cancer,43
non-small cell lung cancer,44 and breast cancer,45,46 and have been
reported to have prognostic significance in some of these cases,46
although they have not yet been well characterized. Fibroblast Growth Factor. Fibroblast growth factor (FGF), although
commonly expressed in many cancers (especially basic FGF), has either
no prognostic effect whatsoever, or may be associated with slightly better
overall prognosis.13,47-51 This lack of negative prognostic effect may be
due in part to direct effects of FGF on the cancer cells; bFGF has been
Fig 1. VEGF and VEGF receptors. In addition to the parent VEGF ligand, several other related ligandshave been identified. In turn, these ligands are recognized by several transmembrane receptortyrosine kinases shown above.
Curr Probl Cancer, January/February 2002 11

8/3/2019 SledgeJr 2002 Current Problems in Cancer
http://slidepdf.com/reader/full/sledgejr-2002-current-problems-in-cancer 7/54
shown to induce apoptosis (by down-regulating Bcl-2) and increase the
chemosensitivity of breast cancer cells in vitro.52,53
Integrins. Integrins are cell surface adhesion receptors. The v3
integrin is the most promiscuous member of the integrin family, allowing
endothelial cells to interact with a wide variety of extracellular matrix
components. In the mid 1990s Brooks et al54 established that v3
integrin is up-regulated in proliferating endothelial cells, and antibodies to
this integrin affect angiogenesis without affecting normal pre-existing
blood vessels. From a mechanistic standpoint, v3 integrin is required
for sustained mitogen-activated protein kinase activity during angiogen-
esis.
55
Integrins may function as endothelial cell survival factors bypreventing anoikis by enhancing binding to the extracellular matrix. In
addition, integrins may function in concert with VEGF to promote
endothelial cell survival.4 Antagonists to v3 integrin promote tumor
regression in preclinical models by inducing apoptosis of tumor blood
vessels.56,57
In spite of these interesting observations, v3 integrin has not been
well studied in human cancers, primarily because of the lack of a readily
available reagent for use with formalin-fixed, paraf fin-embedded tissue.
Gasparini et al have demonstrated that increased vascular expression of
v3 integrin is associated with a greater relapse rate in early stage breast
cancer.82,311,317,328
Negative Regulators of AngiogenesisPerhaps unsurprisingly, the first regulators of angiogenesis to be
discovered were positive regulators. More recently, however, several
negative regulators of angiogenesis have been discovered. The impor-
tance of these negative regulators for normal physiology is self-evident;negative feedback loops are necessary to prevent uncontrolled prolifera-
tion of blood vessels. The importance of negative regulators in cancer is
perhaps less obvious for existing macroscopic tumors, which by definition
have already undergone an “angiogenic switch.” The presence of uncon-
trolled growth and the development of progressive metastasis would seem
to imply a failure of negative regulation. As we will describe below, the
story is somewhat more complicated.
Angiostatin. Angiostatin is a 38-kDa plasminogen fragment generatedby several proteases. Originally described by O’Reilly et al58 as an
inhibitor of angiogenesis in Lewis lung carcinoma, it inhibits capillary
endothelial cell proliferation and induces endothelial cell apoptosis in
vitro and tumor growth in vivo (in multiple preclinical models). In
addition, it binds ATP synthase on the surface of endothelial cells, a
12 Curr Probl Cancer, January/February 2002

8/3/2019 SledgeJr 2002 Current Problems in Cancer
http://slidepdf.com/reader/full/sledgejr-2002-current-problems-in-cancer 8/54
mechanism that has been tied to its other actions.59 Recent data suggest
that the cytotoxic effects are limited to proliferating endothelial cells.60
Its role in human cancers is poorly documented. A recent study of patients with non small cell lung cancer suggests that tumor expression of
angiostatin is (as might be expected) associated with improved clinical
outcome.61 Prostatic cancers generate angiostatin-like fragments, and
their generation is associated with tumor grade (by Gleason scoring).62
Elevated levels of angiostatin are detectable in the urine of patients with
cancer, although their prognostic import is unknown.63
Endostatin. Endostatin is a 20-kDa C-terminal fragment of collagen
XVIII that potently inhibits angiogenesis in vitro and in vivo.
64
It isgenerated by proteolytic cleavage of the parent collagen by multiple
proteases.65 It affects multiple endothelial cell functions, including
modulation of plasminogen activation, disassociation of focal adhesions,
and disassembly of actin stress fiber networks66; it alters the intracellular
calcium signaling response to VEGF and bFGF.67 Endostatin binds to
tropomyosin, and a peptide blocker of this binding inhibits endostatin’s
growth-inhibitory activity in vivo.68 Endostatin rapidly down-regulates
many genes in exponentially growing endothelial cells, including imme-
diate early response genes, cell cycle-related genes, and genes regulating
apoptosis inhibitors, mitogen-activated protein kinases, focal adhesion
kinase, G-protein-coupled receptors mediating endothelial growth, a
mitogenic factor, adhesion molecules, and cell structure components.69
Endostatin’s role in human cancer is not well examined. In the ovary,
endostatin gene expression is higher in ovarian cancer than in normal
ovaries, and high endostatin expression is associated with impaired
prognosis.70 In contrast, in hepatocellular carcinoma increased expression
of collagen XVIII (endostatin’s precursor) is associated with smallertumor size and improved prognosis.71 Serum levels of endostatin have
been measured in breast cancer, clear cell renal carcinoma, and soft tissue
sarcoma, with variable results: increased plasma endostatin levels are
associated with improved prognosis in premenopausal breast cancer and
impaired prognosis in sarcoma.72-74
Thrombospondin. Thrombospondins are a multigene family of 5
secreted glycoproteins involved in the regulation of cell proliferation,
adhesion, and migration. They are widely distributed in the extracellularmatrix of numerous tissues. Two members of the thrombospondin family,
namely TSP-1 and TSP-2, are naturally occurring inhibitors of angiogen-
esis.75 Preclinical evidence suggests that stromal TSP-2 may act as a
natural inhibitor of chemically induced carcinogenesis and early tumor
formation.76
Curr Probl Cancer, January/February 2002 13

8/3/2019 SledgeJr 2002 Current Problems in Cancer
http://slidepdf.com/reader/full/sledgejr-2002-current-problems-in-cancer 9/54
The role of the thrombospondins as prognostic factors is currently being
defined. In several tumors, low thrombospondin levels have been asso-
ciated with either increased measures of angiogenesis or progressivedisease stage and impaired prognosis. These include cervical cancer,77
colorectal cancer,78,79 bladder cancer,80 and glioma.81 In contrast, ele-
vated thrombospondin levels have been reported to have either no effect
on prognosis in some tumors (for example, in breast cancer82) or even to
be associated with increased angiogenesis and impaired prognosis (for
example, in endometrial cancer83).
Angiogenesis in Carcinogenesis and
Tumor ProgressionThe role of angiogenesis in the malignant phenotype has been studied
both at a preclinical and a clinical level. It is clear from these studies that
angiogenesis is crucial to the early development of many cancers.
Preclinical transgenic mouse models (reviewed by Hanahan and Folk-
man84) suggest that new blood vessel formation occurs after initial tumor
initiation but before the development of invasive tumors. Studies from the
clinic have confirmed this observation: premalignant lesions of breast,
cervix, and melanocytes all demonstrate increased microvessel density.84
Breast cancer provides a representative clinical example of what has
been termed the “angiogenic switch” in cancer. Stromal microvessel
density increases significantly during the transition from atypical hyper-
plasia to ductal carcinoma in situ of the breast,85,86 and this transition is
associated with increased epithelial cell production of the proangiogenic
factors VEGF, VEGF-C, hypoxia-inducible factor-1 (which regulates
VEGF production), and placental-derived endothelial cell growth factor
(PD-ECGF).8,9,37,86
After the transition from atypical hyperplasia to ductal carcinoma in
situ, increasing angiogenesis appears to be associated with virtually every
step of tumor progression. Comedo ductal carcinomas in situ, for
instance, have higher microvessel density measurements than noncomedo
ductal carcinomas in situ.87,88 Similarly, microinvasive cancers have
higher microvessel densities than noninvasive cancers.85 The angiogenic
ability of a primary invasive tumor and of its lymphatic metastases (as
assessed by microvessel density) is correlated.89
Angiogenesis and MetastasisFrom a teleologic standpoint, angiogenesis is important not only
because it offers the growing cancer nutrients, but also because it offers
cancer cells a route to distant sites and a means of growing in those sites.
14 Curr Probl Cancer, January/February 2002

8/3/2019 SledgeJr 2002 Current Problems in Cancer
http://slidepdf.com/reader/full/sledgejr-2002-current-problems-in-cancer 10/54
The relationship of angiogenesis to distant metastasis in patients with
breast cancer entered the modern era in 1991 with the seminal study by
Weidner et al
90
in the New England Journal of Medicine. Previousinvestigators had examined the invasion of tumor blood vessels by cancer
cells and correlated such vascular or lymphatic invasion with outcome,
with widely varying results. Weidner et al,90 in contrast, measured the
blood vessel content of human breast cancers and argued that microvessel
density (MVD) was directly correlated with clinical outcome. Numerous
other authors have followed their lead in breast cancer (Table 2) and in
other malignancies.
In general, the results of MVD analyses have suggested that increasingMVD is associated with impaired prognosis for patients with metastatic
breast cancer, both with regards to relapse-free and overall survival
(Table 3). Not all studies concur with this conclusion. The conflicting
results obtained may be due to differences in study sample size (which
vary widely), differences in technique, or (although this seems unlikely)
the inadequacy of the underlying hypothesis.
Technique differences abound. First, the means of identifying tumor
blood vessels is based on the type of antibody used in the assay.
Numerous endothelial cell markers (eg, CD31, CD34, factor VIII-related
antigen, CD101, Tie-2) have been studied, and these markers vary with
regard to which endothelial cells are delineated.
Second, pathologists vary tremendously in their counting measures for
tumor endothelial cells. Weidner et al90 originally suggested visual counts
of tumor microvessel “hot spots,” the portion of a given tumor with the
(subjectively determined) greatest number of tumor microvessels. “Hot
spot” analysis has the biologic rationale of examining the portion of the
tumor with the greatest concentration of new blood vessels and thereforepresumably detecting the clonal populations with the greatest potential for
metastasis. However, “hot spot” analysis is inherently subjective and
obviously subject to selection bias. In addition, de Jong et al91 have
demonstrated that it will affect outcome of “hot spot” analysis, depending
on which tumor block is used and which portion of a given tumor block
is examined.91
Because of these concerns, investigators have used several other
variations of measuring microvessel density, including counts with a grid(so-called Chalkley counts)92-95 and computer-assisted image analy-
sis.92,96 Comparison of these techniques has suggested that they may be
more reproducible than standard “hot spot” analysis.
Third, MVD counting is subject to all of the usual technical problems
associated with immunohistochemical technique, such as antigen preser-
Curr Probl Cancer, January/February 2002 15

8/3/2019 SledgeJr 2002 Current Problems in Cancer
http://slidepdf.com/reader/full/sledgejr-2002-current-problems-in-cancer 11/54
vation, investigator experience, and intraobserver and interobserver vari-
ability. Interobserver reproducibility has varied significantly in various
publications where it has been examined.97-99
Although MVD studies support a prognostic effect for increasing
microvessel density in breast cancer, the very real technical concerns limit
the usefulness of MVD as a routine prognostic indicator. The 1999 reviewby the College of American Pathologists of prognostic factors considered
MVD to fall into category III (“factors not suf ficiently studied to
demonstrate their prognostic value”) as a prognostic factor.100 In the
absence of larger studies that use standardized methods, this seems a
reasonable judgment.
TABLE 3. Negative prognostic value of tumor microvessel density in breast cancer
Investigator PatientsNodal
status AntibodyCounting
method
High vs low
MVD
(P value)
RFS OS
Weidner 199190 49 N/N FVIII “Hot spot” .003 NR
Weidner 1992304 165 N/N FVIII “Hot spot” .001 .001
Hall 1992305 87 N/N FVIII “Hot spot” NS NS
Obermair 1994306 106 N/N FVIII “Hot spot” .0002 NR
Fox 1995307 211 N/N CD31 Chalkley NR .05
Toi 1995308 328 N/N FVIII “Hot spot” .00001 NR
Ogawa 1995309 155 N/N FVIII “Hot spot” .025 .01
Axelsson 1995
97
220 N
/N
FVIII “Hot spot” NS NSMorphopoulas 1996310 160 N/N FVIII “Hot spot” NS NS
Gasparini 1998311 531 N/N CD31 “Hot spot” .05 .05
Kumar 1999269 106 N/N CD105 “Hot spot” .0362 .0029
CD34 NS NS
Tynninen 1999312 84 N/N FVIII “Hot spot” NS NR
Hansen 200094 836 N/N CD34 Chalkley .05 NR
Vincent-Salomon313 685 N/N FVIII “Hot spot” NS NS
Bosari 1992314 88 N FV “Hot spot” .01 NF
32 N NS NS
Van Hoef 1993315 93 N FVIII “Hot spot” NS NS
Fox 1994316
109 N CD31 Chalkley .01 .028Gasparini 1994317 254 N CD31 “Hot spot” .0004 .047
Bevilacqua 1995318 211 N CD31 “Hot spot” .0001 .044
Inada 1995319 110 N FVIII “Hot spot” .05 .05
Obermair 1995306 230 N FVIII “Hot spot” .05 NR
Costello 1995320 87 N FVIII “Hot spot” NS NS
Karaiossifidi 1996320 52 N FVIII “Hot spot” .05 NR
Heimann 1996322 167 N CD34 “Hot spot” .018 NR
Ozer 1997323 35 N FVIII “Hot spot” .034 NR
Medri 2000324 378 N FVIII “Hot spot” NS NS
RFS , relapse free survival, OS , overall survival, N
, lymph node positive, N
, lymph nodenegative; NS , not significant; NR , not reported.
16 Curr Probl Cancer, January/February 2002

8/3/2019 SledgeJr 2002 Current Problems in Cancer
http://slidepdf.com/reader/full/sledgejr-2002-current-problems-in-cancer 12/54
Angiogenesis and Tumor DormancyPatients may harbor micrometastatic cancers for prolonged periods
before the emergence of overt metastatic disease. The following possibleexplanations for such tumor dormancy have been suggested: (1) tumor
dormancy simply may represent the natural history of slowly-dividing
tumors, in which overt metastatic disease is the temporal “tip of the
iceberg” (in essence, pseudodormancy); (2) tumor dormancy may repre-
sent a cancer composed of nondividing tumor cells that eventually begin
dividing as a result of a mutation event favoring progressive growth; (3)
tumor dormancy may represent the presence of tumors composed of
normally dividing cells whose progressive growth (as opposed to celldivision) is inhibited by some external force (eg, immune surveillance).
Recent clinical and laboratory data have suggested that angiogenesis
may play a role in tumor dormancy. Examinations of scar line recurrences
in patients with breast cancer have suggested that true tumor dormancy is
a real event; that is, that the “tip of the iceberg” theory cannot explain the
clinical behavior of micrometastatic disease.101 Second, laboratory data
from the study of angiogenesis have suggested a synthesis of the second
and third explanations offered above. Micrometastatic cancer cellscontinue dividing at a normal pace during their dormant phase, but such
cell division is balanced by cell death.102 Tumor growth, as opposed to
cell division, is held in check by the absence of new blood vessel
formation suf ficient to support the progressive growth of the cancer.
It has recently been suggested that tumor dormancy is an active rather than
a passive event, in that its maintenance results from tumor production of the
natural inhibitor angiostatin, which prevents development of new blood
vessel formation.103
Tumor dormancy presumably ends as the result of mutational events that allow new blood vessel formation. The active
maintenance of tumor dormancy by such mechanisms implies the strategy of
inducing tumor dormancy as a means of treating micrometastatic cancers. Of
note, this view of tumor dormancy has been challenged (or at least qualified)
by Guba et al,104 who demonstrated the presence of single dormant
microscopic metastatic cells independent of angiogenesis inhibition (al-
though such inhibition was also noted in their model system).
Angiogenesis in Hematologic MalignanciesOne of the more fascinating outcomes of research involving angiogen-
esis involves its role in hematologic malignancies. Such a role is not
readily intuitive, given the fact that hematologic malignancies are literally
bathed in blood, either in the marrow or in the peripheral circulation. In
Curr Probl Cancer, January/February 2002 17

8/3/2019 SledgeJr 2002 Current Problems in Cancer
http://slidepdf.com/reader/full/sledgejr-2002-current-problems-in-cancer 13/54
recent years, however, investigators have demonstrated that angiogenesis
plays an important role in the development and progression of these
cancers.As with solid tumors, the evidence supporting a role for angiogenesis
(reviewed by List105) comes both from studies of microvessel density
and from studies of proangiogenic growth factors, particularly VEGF.
Increased microvessel density is seen in the marrow of patients with
acute myelogenous leukemia, acute lymphocytic leukemia, chronic
myelogenous leukemia, small lymphocytic lymphoma, multiple my-
eloma, idiopathic myelofibrosis, and myelodysplatic syndromes.19,106-
110 Increased microvessel density has been correlated with impairedclinical outcome in multiple myeloma107,111 and idiopathic myelofi-
brosis.110,112
Studies of VEGF have provided a particularly interesting view into the
role of angiogenesis in hematologic malignancies. Several hematologic
malignancies have been demonstrated to produce VEGF, which may be
measured either in the minor cells themselves or in the serum of patients
with these malignancies. In some of these malignancies VEGF expression
has been correlated with impaired clinical outcome. These include acutemyelogenous leukemia19 and non-Hodgkin’s lymphoma.113 In addition,
there is now growing evidence that several hematologic malignancies
express receptors for VEGF (both VEGF receptor-1 [R-1] and receptor-2
[R-2]), raising the possibility that the VEGF/VEGF receptor axis may
serve as an autocrine pathway in some tumors.114,115
Dias et al116 have recently studied this role. The HL-60 promy-
elomonocytic leukemia cell line (expressing both VEGF and VEGF
R-2) was inoculated into sublethally irradiated NOD-SCID mice, andthen treated with monoclonal antibodies directed against either human
or murine VEGF R-2. This approach allowed the investigators to
examine the respective roles of the stromal (murine) and leukemic
(human) VEGF/VEGF R-2 pathways. Of note, although both antibod-
ies retarded progression of the leukemia in this model, neither was
capable of curing the treated animals. In contrast, the combination of
both antibodies resulted in cure of the animals. These data suggest that
both paracrine and autocrine VEGF R-2 pathways (and, perhaps, bothstromal-mediated angiogenesis and VEGF-stimulated tumor growth)
play a role in the progression of this tumor. To date there are no
published trials of agents targeting either VEGF or VEGF R-2 in
patients with leukemia, although such trials are in development for a
number of such agents.
18 Curr Probl Cancer, January/February 2002

8/3/2019 SledgeJr 2002 Current Problems in Cancer
http://slidepdf.com/reader/full/sledgejr-2002-current-problems-in-cancer 14/54
Therapeutic Implications of Angiogenesis
Chemotherapeutics as AntiangiogenicsOncologists may have been unknowingly administering antiangiogenic
therapy for years.117 Tamoxifen, initially believed to be merely a
competitive inhibitor of estradiol, may have estrogen-independent mech-
anisms of action.118 Tamoxifen inhibits VEGF-stimulated and FGF-
stimulated embryonic angiogenesis in the chick chorioallantoic mem-
brane model. This effect was not reversed by excess estradiol, suggesting
that the antiangiogenic mechanism is not dependent on estradiol concen-
tration or estrogen receptor content.
119,120
Treatment with tamoxifenresulted in a more than 50% decrease in the endothelial density of viable
tumor and an increase in the extent of necrosis in MCF-7 tumors growing
in nude mice.121 The inhibition of angiogenesis was detected before
measurable effects on tumor volume.122 Using differential display tech-
nology to assess gene expression in tumor and normal breast tissue from
two patients, Silva et al123 reported that brief treatment with tamoxifen
resulted in down-regulation of CD36, a glycoprotein receptor for matrix
proteins thrombospondin-1 and collagen types I and IV. Throm-
bospondin-1 is involved in hematogenous tumor dissemination, invasion,
and angiogenesis; thus down-regulation of CD36 represents a potential
mechanism for the observed antiangiogenic effect.
Several chemotherapeutic agents used routinely in breast cancer treat-
ment have known antiangiogenic activity.124-130 Maximal antiangiogenic
therapy typically requires prolonged exposure to low drug concentrations,
exactly counter to the maximum tolerated doses administered when
optimal tumor cell kill is the goal.131 Three recent reports confirm the
importance of dose and schedule. In all 3 the combination of low,frequent-dose chemotherapy plus an agent that specifically targets the
endothelial cell compartment controlled tumor growth much more effec-
tively than the cytotoxic agent alone. An “antiangiogenic schedule” (170
mg/kg every 6 days) of cyclophosphamide was more effective than the
conventional maximum tolerated dose (150 mg/kg every other day for 3
doses every 21 days) in Lewis lung carcinoma and L1210 leukemia
models; the antiangiogenic schedule was 3 times more effective in
controlling growth of chemotherapy-resistant Lewis lung carcinoma andEMT-6 breast cancer cell lines.132 The addition of the angiogenesis
inhibitor, TNP-470, to the antiangiogenic cyclophosphamide schedule
induced endothelial cell apoptosis within tumors, an effect that preceded
apoptosis of drug-resistant Lewis lung carcinomas. Low-dose vinblastine
(0.75 mg/m2 intraperitoneal with 1 mg/m2 /d continuous infusion for 3
Curr Probl Cancer, January/February 2002 19

8/3/2019 SledgeJr 2002 Current Problems in Cancer
http://slidepdf.com/reader/full/sledgejr-2002-current-problems-in-cancer 15/54
weeks followed by 1.5 mg/m2 intraperitoneal twice per week) plus an
antibody against the VEGF-receptor-2 controlled growth of neuroblas-
toma xenografts during 210 days of therapy.
133
Similar findings havebeen reported with carboplatin plus a VEGF-neutralizing antibody.134
Thus far only few clinical trials have tested “antiangiogenic” schedules
of chemotherapy, so-called “metronomic therapy.”135 Nonetheless, the
limited clinical evidence available is intriguing. Remissions can be
induced, albeit infrequently, in patients resistant to taxane therapy
administered on an every 3-week basis by altering the drug schedule.
Specifically, Fennelly et al136 reported that 4 of 13 patients with ovarian
cancer, who had received and subsequently relapsed from prior paclitaxeltherapy, responded when treated with increasing doses of paclitaxel
administered weekly. Moreover, 2 of these patients had progressed while
receiving paclitaxel. Prolonged infusion paclitaxel (140 mg/m2 over 96
hours) induced responses in 7 of 26 patients who had relapsed within a
median of 1 month from prior short taxane infusions.137
The European Organization for Research and Treatment of Cancer
studied 2 cyclophosphamide, methotrexate, and 5-fluorouracil (CMF)
regimens: a classic 28-day regimen incorporating daily oral cyclophos-
phamide for 14 days and a modified intravenous schedule with bolus
cyclophosphamide every 3 weeks. Overall response rate and survival
clearly favored the classic regimen.138 Although generally viewed as a
test of dose intensity (the classic regimen delivered higher total doses of
both cyclophosphamide and 5-fluorouracil), this study may also be
considered as a test of an “antiangiogenic” versus bolus schedule. A phase
II study of low-dose methotrexate (2.5 mg twice daily for 2 days each
week) and cyclophosphamide (50 mg daily) in patients with previously
treated metastatic breast cancer found an overall response rate of 19%(the conditions of an additional 13% of patients were stable for 6
months). Serum VEGF levels decreased in all patients continuing to
receive therapy for at least 2 months but did not correlate with re-
sponse.139
Angiogenesis as Predictive Factor Angiogenesis appears well established as a prognostic factor. More
recent studies suggest that it may also function as a predictive factor. Toiet al140 have provided evidence that VEGF expression is associated with
a phenotype of hormone resistance. Similarly, Foekens et al14 have
suggested that tumor levels of VEGF represent a predictive, as well as a
prognostic, factor both for hormonal therapy and chemotherapy. Exam-
ining a group of 845 patients in whom VEGF had been measured in the
20 Curr Probl Cancer, January/February 2002

8/3/2019 SledgeJr 2002 Current Problems in Cancer
http://slidepdf.com/reader/full/sledgejr-2002-current-problems-in-cancer 16/54
primary tumor cytosol and who then had development of a recurrence
during follow-up, they demonstrated that high tumor VEGF levels were
associated with impaired response to hormonal therapy with tamoxifenand to chemotherapy with 5-fluorouracil, adriamycin, and cyclophos-
phamide (FAC) or CMF. In addition, high VEGF levels were associated
with short progression-free and overall survival.
Why might this be the case? Recent data from Pidgeon et al141 suggest
that VEGF may inhibit apoptosis not only in tumor endothelial cells, but
in breast cancer cells as well. This protection against apoptosis in breast
cancer cells has recently been shown to be mediated at least in part
through the neuropilin receptor, for which VEGF acts as a ligand.
142
Thebelief that VEGFs effects, mediated through the classic receptors Flt-1
and KDR, are limited to endothelial cells is no longer tenable.
Targeting AngiogenesisOur burgeoning understanding of angiogenesis has fostered the devel-
opment of agents targeting specific steps in the angiogenic cascade, many
of which have entered the clinic (Table 4). Part of the very real
enthusiasm surrounding these reagents is due to the large variety of
potential targets, in contrast to the relatively small number of targets of
standard chemotherapy (Table 5). A detailed list of agents in clinical
development can be obtained from the Angiogenesis Foundation
(http://www.angiogenesis.org) or from the National Cancer Institute
(http://cancernet.nci.nih.gov). Although the number of ongoing phase I
and II trials has grown rapidly, few have been reported in the peer-
reviewed literature; no phase III trials (with the exception of matrix
metalloproteinase inhibitors) have been completed. Rather than an ex-
haustive review of all agents currently in clinical testing, we haveconceptually grouped agents into several categories: protease inhibitors,
which either directly inhibit or otherwise interfere with the action of
proteases critical for invasion, growth factor/receptor antagonists, which
thwart signaling of proangiogenic growth factors, endothelial toxins,
which specifically target endothelial antigens, and natural inhibitors,
which stimulate or mimic substances known to naturally inhibit angio-
genesis. The clinical experience with representative agents in each
category will be reviewed. Protease Inhibitors. Degradation of the basement membrane and
surrounding stroma by the matrix metalloproteinases (MMPs) is cru-
cial for direct tissue invasion and angiogenesis. Inhibition of the
MMPs decreases angiogenesis in preclinical systems and mouse
xenografts.143-149 Marimastat is a low molecular weight peptide mimetic
Curr Probl Cancer, January/February 2002 21

8/3/2019 SledgeJr 2002 Current Problems in Cancer
http://slidepdf.com/reader/full/sledgejr-2002-current-problems-in-cancer 17/54
TABLE 4. Representative anti-angiogenic agents currently in clinical trials
Agent Phase Patient population Combination therapy
Æ-941 (Neovastat) II MyelomaIII Renal cell
III IIIa/IIIb nonsmall cell Platinum-based
chemotherapy RT
Angiostatin I All solid tumors
I All solid tumors RT
Avastin (rhuMab VEGF) I Advanced head and neck 5-fluorouracil
hydroxyurea RT
II Relapsed myeloma Thalidomide
II Colorectal 5-fluorouracil
leucovorin
II Renal cell, cervical, ovarian,lymphoma,
II Hormone-refractory prostate Docetaxel, estramustine
II Hematologic malignancies Cytarabine, mitoxantrone
II Breast vinorelbine
II Ib-IIIa resectable nonsmall
cell
Neoadjuvant paclitaxel
carboplatin
II Inflammatory breast Neoadjuvant docetaxel
doxorubicin
II/III Colorectal 5-fluorouracil
leucovorin CPT-ll
II/III Nonsmall cell Paclitaxel carboplatin
II/III Breast Paclitaxel
III Breast Capectabine
III Advanced colorectal Oxaliplatin 5-
fluorouracil
leucovorin
BMS-275291 I/II HIV-related Kaposi’s
sarcoma
II Ia-IIIa breast Chemotherapy or
tamoxifen
II/III Nonsmall cell Paclitaxel carboplatinCarboxyamodotriazole I All solid tumor and
lymphoma
Paclitaxel
II Renal cell, ovarian
COL-3 I/II Advanced solid tumors,
glioma
II HIV-related Kaposi’s
sarcoma
Celecoxib I/II Cervical Cisplatin 5-fluorouracil
RT
II Colorectal 5-fluorouracil
leucovorin CPT-11
EMD-121974 I All solid tumors
I/II Glioma
Endostatin I/II All solid tumors
IM-862 II Ovarian Paclitaxel carboplatin
II Colorectal 5-fluorouracil
22 Curr Probl Cancer, January/February 2002

8/3/2019 SledgeJr 2002 Current Problems in Cancer
http://slidepdf.com/reader/full/sledgejr-2002-current-problems-in-cancer 18/54
TABLE 4. (Continued)
Agent Phase Patient population Combination therapy
Interleukin-12 I/III HIV-related Kaposi’ssarcoma Liposomal doxorubicin
Marimastat III Small cell lung
2-methoxyestradiol I Breast, all solid tumors
I Breast Docetaxel
II Hormone-refractory
prostate, myeloma
RPI-4610 II Renal cell
Soy isoflavone II Breast
Squalamine II Ovarian Carboplatin
II Glioma RT
SU-5416 I/II All solid tumors, glioma,hematologic malignancies
I All solid tumors Paclitaxel
I/II Soft tissue sarcoma Neoadjuvant RT
I/II Colorectal CPT-11
II Renal cell Interferon alfa-2b
II Hormone-refractory prostate Dexamethasone
III Colorectal 5-fluorouracil
leucovorin CPT-11
Suramin II Myeloma
Thalidomide I Glioma Topotecan
I/II Melanoma Temozolomide
II Myelodysplastic syndromes,
colorectal, ovarian,
uterine sarcoma,
endometrial, chronic
lymphocytic leukemia, low
grade lymphoma,
hepatocellular
II Ovarian Carboplatin
Hormone-refractory prostate Docetaxel
II Myeloma PrednisoneII Chronic lymphocytic
leukemia
Fludarabine
II Nonsmall cell Carboplatin CPT-11
II Low grade lymphoma,
hepatocellular
Interferon-alfa
II Hepatocellular Doxorubicin
chemoembolization
III Nonsmall cell Carboplatin paclitaxel
RT
III Myeloma Dexamethasone
cyclophosphamide
etoposide cisplatin
III Renal cell Interferon alfa-2b
III Prostate Hormone ablation
RT, Radiation therapy.
Source: http://cancernet.nci.nih.gov
Curr Probl Cancer, January/February 2002 23

8/3/2019 SledgeJr 2002 Current Problems in Cancer
http://slidepdf.com/reader/full/sledgejr-2002-current-problems-in-cancer 19/54
containing a hydroxyamate group that chelates the zinc atom of the active
site if the MMPs. Marimastat inhibits a broad spectrum of the MMPs and
has activity in multiple human tumor xenograft models.150 Phase I trials
identified musculoskeletal syndromes including arthralgia/arthritis, ten-
donitis, and bursitis as the dose-limiting toxicity with biologically active
levels achieved in patients with advanced malignancy with doses ranging
from 5 to 10 mg administered 2 times daily.151
Although not predicted to induce substantial clinical response in
patients with well-established bulky tumors, long-term therapy with an
MMP inhibitor may delay or eliminate tumor regrowth after initial
surgical excision or systemic chemotherapy. Two recently completed
trials evaluated marimastat in breast cancer. ECOG-2196 measured timeto progression in patients with metastatic cancers whose conditions were
responding or stable after initial chemotherapy randomized to treatment
with either marimastat or placebo. ECOG-2196 recently closed to accrual;
preliminary results were expected in late 2001. In a limited institution
phase II pilot study, 63 patients with early stage breast cancer received
marimastat at 1 of 2 dose levels either after doxirubicin-based chemo-
therapy or concomitantly with tamoxifen. Musculoskeletal toxicity re-
sulted in significant dose reductions and limited chronic administration todoses yielding plasma levels below the target range.152
BMS-275291 is a peptidomimetic MMP inhibitor that contains a
chemically novel mercaptoacyl zinc-binding group. BMS-275291 inhibits
a broad spectrum of MMPs without inhibiting the sheddases, related
metalloproteinases which regulate proinflammatory cytokine and cyto-
TABLE 5. Chemotherapy versus antiangiogenic therapy: targets of opportunity
Chemotherapy targets
DNA
Topoisomerases
Microtubules
Antiangiogenesis targets
Circulating Ligands
Receptor Tyrosine Kinases
Integrins
Cell adhesion markers
Proteases
Membrane glycoproteins
Enzymes
DNAMicrotubules
Adapted from: Kerbel RS. Clinical trials of antiangiogenic drugs: opportunities, problems, and
assessment of initial results. J Clin Oncol 2001;18(Suppl.):45s-51s.
24 Curr Probl Cancer, January/February 2002

8/3/2019 SledgeJr 2002 Current Problems in Cancer
http://slidepdf.com/reader/full/sledgejr-2002-current-problems-in-cancer 20/54
kine receptor shedding from the cell surface. BMS-275291 preserves the
homeostasis of tumor necrosis factor- and other proinflammatory
cytokine and cytokine receptors hypothesized to play a role in the doselimiting arthritis/arthralgia seen with other MMP inhibitors. A similar
adjuvant pilot trial is ongoing with this agent.
Proangiogenic Growth Factor/Receptor Antagonists. Angiogenesis
requires stimulation of vascular endothelial cells through the release of
angiogenic peptides including VEGF. An antibody directed against
VEGF inhibited the growth of several human tumors in animal mod-
els153,154; a humanized recombinant version of this antibody has entered
clinical trials. RhuMAb-VEGF was well tolerated and produced theexpected decrease in free plasma VEGF levels in a multicenter phase I
trial of 25 patients. Three patients had tumor-related bleeding episodes,
including an intracranial hemorrhage into an unrecognized cerebral
metastasis in a patient with hepatocellular carcinoma. Although no
objective responses were seen, 14 patients had stable disease at evaluation
on day 72.155 A dual-institution phase II study of rhuMAb-VEGF in
patients with previously treated metastatic breast cancer has recently been
completed with 75 patients in 3 successive dose cohorts, 3 mg/kg (n 18), 10 mg/kg (n 41), and 20 mg/kg (n 16) every other week. Overall
the conditions of 17% of patients were responding or stable at 22 weeks;
3 patients continued to receive therapy without progression for 12
months. Therapy was generally well tolerated with mild hypertension and
proteinuria in several patients; no significant bleeding episodes were
noted.156
Inhibition of the VEGF receptor tyrosine kinase domain (Flk-1 and
Flt-1) also represents a fruitful therapeutic target. The critical role of Flk-1 in tumor angiogenesis was demonstrated by use of a dominant-
negative Flk-1 transfectant. Eight of 9 tumor cell lines with dominant
negative Flk-1 showed growth inhibition and reduced MVD in athymic
mice.157 A synthetic inhibitor of the Flk-1 kinase has been developed
(SU-5416) that inhibits VEGF-dependent growth of endothelial cells
without altering tumor growth in vitro. Systemic administration of
SU-5416 inhibited the growth of human tumors in mice without apparent
toxicity.158,159
SU-5416 was well tolerated in a phase I clinical trial withdose-limiting toxicity being a severe migraine syndrome with headache
and projectile vomiting.160,161 Coadministration of SU-5416 did not alter
pharmacokinetics of either agent and produced no unexpected toxicity.162
A phase III trial in colorectal cancer, as well as multiple disease-specific
phase II trials are ongoing. ZD6474, an oral inhibitor of the Flk-1 tyrosine
Curr Probl Cancer, January/February 2002 25

8/3/2019 SledgeJr 2002 Current Problems in Cancer
http://slidepdf.com/reader/full/sledgejr-2002-current-problems-in-cancer 21/54
kinase that also inhibits the epidermal growth factor receptor tyrosine
kinase, has also entered clinical development.163
Ribozymes are small RNA elements with specific catalytic activity.Angiozyme is a synthetic ribozyme designed to cleave the messenger
RNA for the VEGF Flt-1 receptor. Preclinical studies confirmed inhibi-
tion of both primary tumor growth and metastasis.164-167 A phase I study
in patients with refractory solid tumors found limited toxicity and no
evidence of drug accumulation. Immunohistochemical staining of acces-
sible tumor samples found variable VEGF Flk-1 and Flt-1 expression
with Angiozyme localized to tumor endothelial cells.167 Multiple disease-
specific phase II studies are underway.PNU-145156E (formerly FCE26644), a sulfonated distamycine A
derivative, is a noncytotoxic molecule whose antitumor activity is exerted
through the formation of a reversible complex with growth/angiogenic
factors.168,169 In vitro PNU-145156E did not modify the cytotoxicity
induced by several chemotherapeutic agents. However, in vivo, at the
optimal dose of each compound, the antitumor activity was significantly
increased in all combinations, with no associated increase in general
toxicity. In healthy mice treated with cyclophosphamide or doxorubicin,
the addition of PNU-145156E did not enhance the myelotoxic ef-
fect.170,171 In phase I testing PNU-145156E induced an unpredictable and
short-lasting decrease in antithrombin III levels without effects on serum
FGF or VEGF concentrations.172
Endothelial Toxins. The antiangiogenic antibiotic TNP-470 (AGM-
1470) inhibits endothelial cell proliferation and entered clinical trials
nearly a decade ago.173-175 Phase I studies found reversible dose-
dependent neurologic toxicity; only one transient objective response was
reported, although several patients had stabilization of disease.176,177 Thehalf-life of TNP470 was extremely short with practically no drug
detectable an hour after treatment suggesting alternate treatment sched-
ules might be required for maximal activity.178,179
Disruption of endothelial cell chemotaxis and migration interferes with
angiogenesis. The integrins, particularly v3 integrin, provide critical
attachment between the migrating endothelial cell and the extracellular
matrix180; v3 integrin also localizes MMP-2 to the membrane of
endothelial cells in the leading podosomes of new vessels providingcarefully targeted matrix destruction.181 Moreover, immunohistochemical
studies of clinical specimens from ocular pathologies suggest that both
v3 and v5 integrins are of importance for endothelial cell function in
angiogenic neovascular disease.182 Antibodies that block v3 integrin
inhibit angiogenesis and tumor growth in vitro56 and in vivo.57 A
26 Curr Probl Cancer, January/February 2002

8/3/2019 SledgeJr 2002 Current Problems in Cancer
http://slidepdf.com/reader/full/sledgejr-2002-current-problems-in-cancer 22/54
humanized monoclonal antibody against v3 integrin, vitaxin was well
tolerated and showed some activity in a phase I trial.183 Phase II trials are
ongoing.Specific antibodies used to characterize the vitronectin receptors v3
integrin and v5 integrin in vitro were used to study the function of these
integrins in vivo.184 RGD (arg-gly-asp) epitope is critical for the function
of many 1 integrins and is the same epitope that v3 integrin recognizes
in its extracellular matrix ligands. This has led to the development of a
family of RGD-containing peptides that can serve as potent and selective
inhibitors of the vitronectin receptors. EMD 121974 is the inner salt of a
cyclized pentapeptide c-[Arg-Asp-DPhe-(NMeVal)] with significant an-tiangiogenic activity in a variety of preclinical in vitro and in vivo models.
Phase I trials of EMD 121974 are ongoing.
Resting endothelial cells are normally quiescent; proliferation increases
dramatically in the leading podosomes of new capillaries. The protein
endoglin is expressed much more strongly in growing tumor microvas-
culature than in the vasculature of surrounding normal tissues. Antibodies
directed against endoglin decreased tumor growth in mice xeno-
grafts.185,186 Antiendoglin antibodies complexed to deglycosylated ricin
A chain produced long-lasting complete remission of preformed tumors
in immunocompromised mice.187,188
Natural Inhibitors. The exact mechanism of action of angiostatin
remains unclear; however, angiostatin binds ATP-synthase on the surface
of endothelial cells inducing endothelial cell apoptosis.59,189,190 A phase
I study of recombinant human angiostatin treated patients with refractory
solid tumors with doses ranging from 15 to 240 mg/m2 as a daily
10-minute intravenous infusion. No dose-limiting toxicity or changes in
coagulation factors were identified. Pharmacokinetics were linear, withdose-proportionate increases in both peak concentration and total expo-
sure. Antibodies to rhu-angiostatin were identified in 2 of 15 patients and
did not appear clinically significant. No objective responses were re-
ported, although some patients had measurable decreases in urine bFGF
and VEGF levels.191 Treatment with angiostatin increases sensitivity to
radiation in preclinical models,192,193 providing support for an ongoing
phase I trial of angiostatin with radiation.
Endostatin, a 20-kD proteolytic fragment of collagen XVIII, hasantiangiogenic activity similar to angiostatin.194 Endostatin has a highly
basic region with significant af finity for heparin, suggesting that binding
to heparin sulphate proteoglycans involved in growth factor signaling
may be partly responsible for its activity.195 In addition endostatin binds
to tropomyosin in vitro and to tropomyosin-associated microfilaments in
Curr Probl Cancer, January/February 2002 27

8/3/2019 SledgeJr 2002 Current Problems in Cancer
http://slidepdf.com/reader/full/sledgejr-2002-current-problems-in-cancer 23/54
endothelial cells; a peptide that mimics the endostatin-binding epitope of
tropomyosin blocks endostatin antitumor activity. Thus disruption of
microfilament integrity seems central to endostatin activity.
68
Phase I studies of endostatin have recently been reported.196-198 Patients
with refractory solid tumors received daily bolus infusions ranging from
15 to 300 mg/m2 with no apparent toxicity. Pharmacokinetics were
linear199; endostatin treatment had no effect on physiological wound
healing.200 Correlative studies found dose-dependent decreases in tumor
associated blood flow with oxygen 15-labeled positron emission tomog-
raphy (PET) scanning and dynamic computed tomography imaging,
increased tumor apoptosis and decrease in peripheral blood endothelialcell colony-forming precursors.
A naturally occurring metabolite of estradiol, 2-methoxyestradiol
(2ME2), has a dual mechanism of action: (1) as an antiproliferative drug
acting directly on the tumor cell compartment and (2) as an antiangio-
genic drug acting on tumor vasculature. In vitro, 2ME2 exhibits antipro-
liferative activity in tumor cell lines with IC50 values generally in the
submicromolar to low micromolar range independent of the estrogen
responsiveness of the cell line. In vivo, 2ME2 is effective in xenograft
and metastatic disease models.201-204 The antiangiogenic activity of
2ME2 has been demonstrated in vivo in corneal micropocket202 and
chorioallentoic membrane systems,205 as well as by the observation of
reduced tumor vasculature in 2ME2-treated mice. In vitro, 2ME2 inhibits
tubule formation in bovine microvascular endothelial cells stimulated by
basic fibroblast growth factor201 and the proliferation of human umbilical
vein endothelial cells.206 Several mechanisms of action have been
suggested, including induction of apoptosis, possibly through the activa-
tion of p53,207 and slowing the rate, but not the degree, of tubulin(de)polymerization inhibited by 2ME2 treatment in certain cell lines208
and inhibition of superoxide dismutase resulting in increased oxidative
stress.209
Preliminary results of an ongoing phase I study of 2ME2 in patients
with previously treated metastatic breast cancer have been reported.210
No dose-limiting toxicity was identified with doses ranging from 200 to
1000 mg once daily. Metabolism was variable with a half-life of
approximately 10 to 12 hours. Conversion to 2-methoxyestrone, aninactive metabolite, was significant, with 2ME1 concentrations generally
10-fold higher than 2ME2 levels. No objective responses were produced,
although prolonged disease stabilization was achieved in several patients.
Changes in VEGF and basic fibroblast growth factor levels were
inconsistent. Accrual continues with a twice-daily dosing schedule. A
28 Curr Probl Cancer, January/February 2002

8/3/2019 SledgeJr 2002 Current Problems in Cancer
http://slidepdf.com/reader/full/sledgejr-2002-current-problems-in-cancer 24/54
phase I study of 2ME2 in combination with docetaxel in patients with
newly diagnosed metastatic breast cancer completed accrual in late 2001
but has not yet been reported.
Conceptual Approaches to Antiangiogenic Therapy Antiangiogenic agents may be conceptually divided into 2 general
categories. What might be called “vasculotoxins” have a direct toxic
effect on proliferating endothelium, inducing endothelial apoptosis and
cell death. Assuming that a given number of endothelial cells are required
to support a population of tumor cells and that some more-or-less fixed
ratio between the two exists, the vasculotoxins might be expected to havea multiplier effect in tumors in human beings. As such they may produce
clinical responses similar to traditional antineoplastics; standard drug
development and clinical trials may be appropriate.
Conversely, we might term “vasculostatins” agents that merely prevent
further new blood vessel formation without directly damaging the
existing microvasculature. Such vasculostatins may require prolonged
administration to induce and maintain tumor dormancy. Classic phase II
trials of the vasculostatins in patients with well-established tumors may
result in few (if any) objective responses without refuting the theoretical
basis for their use. As such, delayed responses would be expected;
prolonged stable disease might well be considered a “win” for such
agents.
Successful development of antiangiogenic therapy, particularly the
vasculostatins, will require a new conceptual approach to clinical re-
search: biologically active rather than maximal tolerated dose, long-term
rather than intermittent therapy, and induction of minor dormancy rather
than tumor cell kill. Current testing of new clinical agents in the phase IIsetting regularly focuses on overall response rate; agents failing to pass
some level of response determined a priori are frequently discarded. This
may represent a strategic error for agents that only prevent further tumor
growth; progression-free survival may represent the preferred end point
for such agents. Alternatively, it may be necessary and appropriate for
some agents to move quickly into a randomized trial once appropriate
safety concerns have been met.211
Hahnfeldt et al212 have explored a model of tumor growth underangiogenic signaling. This model considers growth of the tumor vascu-
lature to be explicitly time dependent (rather than dependent on tumor
volume) and to be under the control of distinct positive and negative
signals arising from the tumor. Overall the model parallels Gompertzian
kinetics with tumor growth slowing as tumor size increases. Tumor
Curr Probl Cancer, January/February 2002 29

8/3/2019 SledgeJr 2002 Current Problems in Cancer
http://slidepdf.com/reader/full/sledgejr-2002-current-problems-in-cancer 25/54
growth eventually reaches a plateau as the action of stimulators of
vascular growth is offset by the increasing production of vascular
inhibitors by the primary tumor. Antiangiogenic therapies act to lowerthis plateau tumor size, it is hoped to a level compatible with asymptom-
atic host survival. Importantly, the final tumor size is dependent only on
the balance of positive and negative angiogenic factors and is independent
of tumor size at the start of treatment. The model also predicts initial
tumor growth with some inhibitors of angiogenesis (particularly angio-
statin) before stabilization at the plateau size is achieved. This early
growth could easily be interpreted (perhaps misinterpreted) as treatment
failure unless surrogate markers of angiogenesis are used to guidetherapy. If such a model is a correct approximation of clinical reality, then
clinical trialists (and their patients) will need to learn to tolerate the
prospect of initial disease progression. This will not be a comfortable
prospect for many.
Potential Strategies for Thwarting Resistance toAntiangiogenic Therapy
Initial Assumptions and Clinical RealitiesAntiangiogenic therapy was initially proposed as being a therapy
“resistant to resistance.”213 This concept was based on both theoretical
expectations and preclinical observations. From a theoretical standpoint,
cancer cell mutational events form the basis of resistance to cancer
chemotherapy; endothelial cells, lacking the genetic plasticity of malig-
nant tissues, should be unable to develop resistance to antiangiogenic
therapy. Observations in animal models of antiangiogenic therapy seem to
support this hypothesis; treatment of mice bearing a variety of tumors(Lewis lung carcinoma, T241 fibrosarcoma, or B16F10 melanoma) with
endostatin until tumor regression is followed by regrowth cessation of
therapy. Retreatment with endostatin following regrowth results in a
repeat of tumor regression (and eventual tumor disappearance), suggest-
ing that drug resistance does not develop.214
The clinical reality of human tumors is something different. Although
occasional trials have demonstrated some modest evidence of clinical
ef ficacy (eg, VEGF-targeting therapies in breast, lung, and colorectalcancers and thalidomide in myeloma), there is currently no suggestion in
the clinical literature that antiangiogenic therapies represent the therapeu-
tic “home run” initially hoped for. The problem of resistance continues.
The discussion above is not meant to imply that antiangiogenic therapy
will prove fruitless, nor that resistance will occur to all patients in all
30 Curr Probl Cancer, January/February 2002

8/3/2019 SledgeJr 2002 Current Problems in Cancer
http://slidepdf.com/reader/full/sledgejr-2002-current-problems-in-cancer 26/54
settings. Rather it is meant to suggest that the justified enthusiasm over a
novel therapeutic modality should not blind us to the very real challenges
facing this modality. Resistance is not a new problem, but rather onefaced by physicians for multiple diseases, both oncologic and infectious.
Antiangiogenic resistance is one thread of the larger fabric of drug
resistance in cancer therapy. The lessons learned in combating other types
of drug resistance, offer hope that we might be able to overcome
resistance to antiangiogenic therapies. In addition, an understanding of
issues specific to antiangiogenesis resistance suggests possibilities for
ameliorating or bypassing resistance.
Means of Thwarting Resistance to Antiangiogenic Therapy
Use Standard Therapies with Antiangiogenic Intent. Chemotherapeu-
tic agents have long been developed on the basis of the concept of
maximum tolerated dose, and with the assumption that the cancer cells are
the sole— or at least primary—target. Recent preclinical studies call these
assumptions into question. Numerous chemotherapeutic agents have
antiangiogenic activity, and this activity may occur at levels far lowerthan those required to kill cancer cells.117 Recent data have suggested that
the use of long-term low-dose chemotherapy (so-called “metronomic
therapy”) may be potently antiangiogenic, although this effect seems most
pronounced when the chemotherapeutic agent is combined with an
antiangiogenic agent.132,215
Use of chemotherapeutics to target the tumor vasculature has the
advantage of using agents that are already commercially available. The
disadvantages of this approach are equally real. For virtually all of thechemotherapeutic agents said to have antiangiogenic activity, we have no
idea of the drug doses and schedules that will optimize an antiangiogenic
effect. Similarly, if the concentration X time aspects of “antiangiogenic
chemotherapy” differs significantly from those of “antitumor chemother-
apy,” we may be faced with the dilemma of not knowing which approach
to forego.
Combine Antiangiogenic Agents with Standard Chemotherapy Regi-
mens. An iteration on the use of chemotherapeutic agents as antiangio-genic therapy involves the combination of chemotherapeutics with
antiangiogenic agents. This approach has an extensive preclinical basis
for support, with multiple antiangiogenic agents and multiple chemother-
apeutic agents showing evidence of combinatorial activity.124,132,215-217
The mechanistic rationale for many of these combinations is poorly
Curr Probl Cancer, January/February 2002 31

8/3/2019 SledgeJr 2002 Current Problems in Cancer
http://slidepdf.com/reader/full/sledgejr-2002-current-problems-in-cancer 27/54
understood and not intuitive. Both radiotherapy and chemotherapy
depend on an effective blood supply for therapeutic ef ficacy.
One angiogenic factor that has been extensively examined with regardto its potential interactions with chemotherapeutic agents is VEGF. VEGF
is antiapoptotic for endothelial cells via several pathways, including
induction of expression of the antiapoptotic proteins Bcl-2 and A1,
activation of the PI 3-kinase/Akt signaling pathway, stimulation of NO
and PGI2, and increased FAK tyrosine phosphorylation.218 This survival
function may play a role in the protection of tumor endothelial cells
against the antiangiogenic effects of commonly used chemotherapeutic
agents. Sweeney et al
124
have recently demonstrated that VEGF protectsendothelial cells against docetaxel, an effect reversed by anti-VEGF
monoclonal antibody.
Recent data suggest that the antiapoptotic effects of VEGF may not be
limited to endothelial cells. Neuropilin-1, a receptor important in neuronal
guidance, has recently been found to act as a receptor for VEGF219 and
is highly expressed by some tumor cells.220 In these, VEGF acts as an
antiapoptotic factor, potentially protecting tumor cells against chemother-
apeutic agents.142 It is reasonable to expect that, both from the aspect of
antineoplastic and antiangiogenic activities, the combination of chemo-
therapeutic agents with agents targeting VEGF will allow one to increase
therapeutic ef ficacy.
Combine Antiangiogenic Agents with Each Other. If, as has been
suggested above, tumor progression is associated with tumor acquisition
of increasing numbers of proangiogenic factors, then the use of multiple
antiangiogenic agents targeting this multiply redundant process simulta-
neously seems a reasonable means of thwarting resistance to individual
agents. This approach is, of course, not unique to antiangiogenic therapy,having previously been used for chemotherapy, antimicrobial therapy,
and antiviral therapy. The combination of antiangiogenic agents has been
used in preclinical models with success, such as interferon and TNP-
1470,221 and angiostatin with endostatin.222 The major barriers to the use
of such combinations in clinical practice will likely be regulatory and
commercial.
Combine Antiangiogenic Agents with Other Biologics. Many of the
substances regulating angiogenesis are not solely proangiogenic. Forinstance, epidermal growth factor receptors and HER-2 both regulate
VEGF in human tumors, and their blockade reduces VEGF production
and angiogenesis.223-231 Given this plethora of indirect influences on
angiogenesis, might we be able to use the combination of biologic agents
targeting growth factor receptors such as EGFR and HER-2 as a means of
32 Curr Probl Cancer, January/February 2002

8/3/2019 SledgeJr 2002 Current Problems in Cancer
http://slidepdf.com/reader/full/sledgejr-2002-current-problems-in-cancer 28/54
inhibiting angiogenesis? More specifically, might we be able to combine
antiangiogenic agents with anti-growth factor receptor agents as a means
of overcoming resistance? This strategy has been shown in preclinicalmodels to be an effective antitumor strategy232 and is currently under
examination by use of combinations of antiangiogenic agents and
trastuzumab in patients with HER-2-positive breast cancer.
Conversely, antiangiogenic agents might offer a means of overcoming
resistance to growth factor-targeting agents. Recent data from Vitoria-
Petit et al233 suggest that increased production of VEGF represents one
mechanism by which tumor cells escape control with an anti-EGFR
monoclonal antibody therapy. The combination of a VEGF-targetingagent with an anti-EGFR agent might prevent this mechanism of
resistance to growth factor receptor therapy.
Use Antiangiogenic Therapy as Adjuvant Therapy. It is a rare therapy
that is more effective for large tumors than for small. Tumor progression,
as we have argued above, implies drug resistance for antiangiogenics as
for other anticancer agents. One means of thwarting the development of
drug resistance associated with tumor progression is to treat cancers when
they are small rather than large in volume. The adjuvant setting (or,
similarly, a minimal residual disease setting) is the logical place to
accomplish this goal.
The use of antiangiogenics as adjuvant therapy has its own potential
barriers. Physicians are frequently loath to use agents in the adjuvant
setting until there is evidence of activity in an advanced disease setting.
The toxicity of long-term antiangiogenic therapy remains largely unex-
plored, as is the toxicity of combinations of chemotherapy with antian-
giogenic therapy. At a minimum, it would seem reasonable to require of
an antiangiogenic therapy being considered as adjuvant therapy that it canbe administered on a long-term basis with established safety and
acceptable pharmacokinetics. For instance, we might require that a matrix
metalloproteinase inhibitor could be given safely for a year at levels
above the range required for successful inhibition of trough serum
metalloproteinase enzyme activity. Such a trial has already been con-
ducted for the matrix metalloproteinase inhibitor marimistat in the
adjuvant breast cancer setting.152
Use Antiangiogenic Therapy as Targeted Therapy. Antiangiogenictherapy has been viewed to date essentially as another form of chemo-
therapy: a general therapy given on a population basis, rather than as a
targeted therapy given to patients with specific molecular targets. It is
reasonable to ask whether we can call failure to respond to a therapy
“drug resistance” if the target at which the therapy is aimed is not present
Curr Probl Cancer, January/February 2002 33

8/3/2019 SledgeJr 2002 Current Problems in Cancer
http://slidepdf.com/reader/full/sledgejr-2002-current-problems-in-cancer 29/54
in the tumor. For instance, although VEGF is an important, perhaps
obligatory, part of new blood vessel formation for many cancers, it
certainly is not the only proangiogenic factor. Indeed, it is likely to be of little importance to the growth of some individual tumors or even entire
classes of tumors. If a patient’s tumor fails to respond to an anti-VEGF
approach, is the tumor resistant or is the therapy merely misguided?
This is a practical, as well as, a semantic issue. If insensitivity due to
lack of therapeutic target equates with resistance at the patient level, than
proper targeting is the means of overcoming such resistance. Targeted
therapy requires specific molecular targets. Ideally these targets should be
biologically relevant (in the sense of being crucial to the tumor’smalignant phenotype), clinically measurable, and definably correlated
with clinical benefit. Examples that fit into such criteria include estrogen
receptor or HER-2 for breast cancer, c-kit for GIST (gastrointestinal
stromal tumors), or bcr-abl for chronic myelogenous leukemia.
At present we are unable to point to any targeted antiangiogenic
therapy. But it is clear that such targeting is at least potentially realizable.
Proangiogenic factors, such as VEGF, and endothelial markers such as
v3 integrin, are clinically measurable. It is reasonable, as part of the
development of phase III proof-of-concept trials for such agents, to
require mandatory tissue collection for such testing. We lack validated
assays for most of the therapeutic targets, but the availability of tissues for
testing has a way of stimulating the development of such assays.
Soluble Measures of AngiogenesisCorrelative laboratory studies assessing biologically meaningful inter-
mediate endpoints of angiogenesis are a necessity. Unfortunately, the
correlation between intermediate endpoints, angiogenesis and biologicalactivity remains unproven. In spite of the wealth of laboratory data, direct
clinical evidence linking antiangiogenic activity, changes in tumor
microvessel density and objective tumor response is lacking. In addition
to the need to establish the clinical relevance of antiangiogenic activity,
the development of reliable surrogate markers of angiogenesis that could
guide therapy without repeated tissue samples is urgently needed.
Although as yet no clear standard has emerged, the search for reliable
surrogates of antiangiogenic activity has focused on two main areas:soluble factors and imaging of the tumor vasculature.
VEGF is a highly conserved, homodimeric, secreted, heparin-binding
glycoprotein whose dominant isoform has a molecular weight of
45,000.234,235 VEGF produces a number of biologic effects, including
endothelial cell mitogenesis and migration, induction of proteinases
34 Curr Probl Cancer, January/February 2002

8/3/2019 SledgeJr 2002 Current Problems in Cancer
http://slidepdf.com/reader/full/sledgejr-2002-current-problems-in-cancer 30/54
leading to remodeling of the extracellular matrix, increased vascular
permeability and vasodilation, immune modulation via inhibition of
antigen-presenting dendritic cells, and maintenance of survival for newlyformed blood vessels by inhibiting endothelial cell apoptosis. VEGF
expression is regulated by hypoxia via molecular pathways similar to
those regulating erythropoietin gene expression.236 The biologic effects
of VEGF are mediated through binding and stimulation of two receptors
on the surface of endothelial cells: Flt-1 (fms-like tyrosine kinase) and
KDR (kinase domain region). Although multiple angiogenic factors are
commonly expressed by invasive human breast cancers, the 121-amino
acid isoform of VEGF predominates.
237
VEGF has been measured in sera and is typically detected at higher
levels in patients with breast cancer than in healthy volunteers.238,239
Higher serum concentrations have also been found in those patients with
stage III compared with stage I or II breast cancer.240 Serum concentra-
tions of VEGF may primarily reflect platelet count rather than tumor
burden, limiting interpretation of these results.241-243 VEGF can also be
easily measured in urine with urinary levels unaffected by platelet
count.244 Elevated urinary VEGF concentrations predicted recurrence of
bladder cancer in one reported study by Crew et al (J Urol 1999;161:
799-804). Additionally, urine VEGF levels increased in patients with
progressive disease during treatment with thalidomide.245 As urine VEGF
excretion may be affected by renal function, normalization on the basis of
urine creatinine has been suggested.246,247 Although previous attempts to
correlate single pretreatment VEGF levels with response to therapy248
and the ability of serial measurements to predict response249 in patients
with metastatic breast cancer have been disappointing, neither of these
preliminary studies directly assessed angiogenesis.Tumorigenesis and progression to metastatic disease are accompanied
by changes in the expression of cell adhesion molecules.250 Though the
major physiologic role of VCAM-1 appears to be in the adhesion of
leukocytes to endothelium during acute inflammatory states, a role in the
adhesion of malignant cells during the process of metastasis has been
demonstrated.251,252 VCAM-1 is transiently expressed on endothelial
cells in response to stimulation by various cytokines, including VEGF,253
interleukin-3, interleukin-4,254 and tumor necrosis factor-.255-257
VCAM-1 plays an integral role in angiogenesis. Human recombinant
soluble VCAM-1 induces chemotaxis of human endothelial cells in vitro
and angiogenesis in vivo in the rat corneal micropocket assay. Both the in
vitro chemotactic activity and the in vivo angiogenic activity of rheuma-
toid synovial fluid was blocked by antibodies to soluble VCAM-1.258
Curr Probl Cancer, January/February 2002 35

8/3/2019 SledgeJr 2002 Current Problems in Cancer
http://slidepdf.com/reader/full/sledgejr-2002-current-problems-in-cancer 31/54
Messenger RNA for VCAM-1 has been identified in juvenile rheumatoid
arthritis synovium; the level of expression was significantly higher than in
synovium from patients with osteoarthritis.
259
Human dermal microvas-cular endothelial cells transplanted into severe combined immunodefi-
cient mice on biodegradable polymer matrixes differentiate into func-
tional microvessels that anastomose with the mouse vasculature. The
newly formed microvessels express multiple markers of angiogenesis
including CD31, CD34, intercellular adhesion molecule 1, and
VCAM-1.260
Soluble VCAM-1 has been detected in the sera of patients with
rheumatoid arthritis,
261
and pancreatic, colon, prostate, and kidney cellcancers.262-264 Increased concentrations of serum soluble VCAM-1 were
detected in patients with breast cancer compared with patients with
benign breast disease, further supporting its role.265,266 In a recently
reported pilot study, serum VCAM-1 levels were more tightly correlated
with breast cancer microvessel density than serum VEGF levels. Al-
though initial levels in patients with known metastatic disease were not
predictive of response, levels quickly rose in patients whose disease
progressed but decreased or remained stable in responding patients.249
Similar results were found in a phase II study evaluating razoxane, an
antiangiogenic topoisomerase II inhibitor, in patients with metastatic
renal cell carcinoma. Serum VCAM-1 levels and urinary VEGF levels
rose significantly after one cycle in patients with progressive disease but
not in those with stable disease.244 Endoglin (CD105), a receptor for
transforming growth factor 1 and 3 in vascular endothelial cells, is
significantly up-regulated in areas of active angiogenesis.186,267
Endoglin endothelial mesenchymal signaling and is required for normal
vascular development.268 Antiendoglin antibodies have produced com-plete remissions in xenograft models.187,188 Endoglin expression in breast
tumors is associated with a poor prognosis269; plasma levels of soluble
endoglin correlate with metastasis in many solid tumor including breast
cancer.270,271 Changes in endoglin levels with antiangiogenic therapy has
not been reported.
The MMP family of enzymes degrade molecules of the basement
membrane and extracellular matrix and are critical for the process of
cellular movement and invasion.272 The gelatinases (MMP-2 andMMP-9) have received particular attention as a result of their ability to
degrade type IV collagen and the correlation of expression with tumor
angiogenesis.145 Overall expression of the gelatinases has been associated
with grade and stage of breast cancer273,274; increased serum levels are
found in patients with metastatic disease. Given the central role of these
36 Curr Probl Cancer, January/February 2002

8/3/2019 SledgeJr 2002 Current Problems in Cancer
http://slidepdf.com/reader/full/sledgejr-2002-current-problems-in-cancer 32/54
peptides in the angiogenic process, decreases in serum levels should
theoretically correlate with changes in tumor MVD and may predict
response to antiangiogenic therapy. This hypothesis has not yet beentested prospectively.
FGF is also commonly produced by breast cancers and can be measured
in tumor cytosols,50 serum, and urine. Similar to VEGF, FGF levels are
increased in patients with breast cancer238,275 and may predict surviv-
al.276,277 The correlation of serial FGF measurements with changes in
tumor microvasculature has not been reported but was not predictive of
response to other systemic treatments in one pilot study.278 Other soluble
factors including interleukin-6
279
and tumor necrosis factor- remainunder investigation.280
Imaging Tumor VasculatureAssessment of tumor blood flow by color-flow Doppler ultrasonography
(CDUS) did not correlate with tumor microvessel density in one small
study,281 but nonetheless was an independent predictor of survival.282
Other investigators, however, found a significant correlation between
CDUS images and microvessel density; increased blood flow as detected
by CDUS was predictive of lymph node metastasis in this pilot study.281
The potential of this technique to monitor the effect of therapy was shown
by investigators at the Royal Marsden Hospital. Thirty-four patients with
large or centrally located breast tumors were followed with clinical
examination, B-mode ultrasonography, and CDUS. Changes in vascular-
ity as measured by CDUS images were concordant with changes in tumor
size at more than 75% of the time points assessed. Perhaps more striking,
changes were apparent by CDUS at least 4 weeks before any change in
tumor size was detected by physical examination or B-mode ultrasonog-raphy in 40% of patients.283
Use of ultrasonography to measure breast tumor vasculature has been
hampered by the technical imitations of traditional clinical ultrasonogra-
phy (2 to 10 MHz).284 Low-velocity flow within the central region of a
tumor and increased peripheral perfusion is common. Traditional ultra-
sound can not readily distinguish these regional variations because the
low-velocity flow approximates the tissue motion velocity. Modifications
to clinical ultrasonography including laser Doppler flow measure-ments,285 use of encapsulated microbubbles as contrast agents,286 and
high-frequency Doppler limitations of traditional clinical ultrasonography
(2 to 10 MHz) are anticipated.284 Low-velocity flow within the central
region of a tumor and increased peripheral perfusion is common.
Traditional ultrasonography can not readily distinguish these regional
Curr Probl Cancer, January/February 2002 37

8/3/2019 SledgeJr 2002 Current Problems in Cancer
http://slidepdf.com/reader/full/sledgejr-2002-current-problems-in-cancer 33/54
variations because the low-velocity flow approximates the tissue motion
velocity. Modifications to clinical ultrasonography including laser Dopp-
ler flow measurements, use of encapsulated microbubbles as contrastagents, and high-frequency Doppler scanning (20 to 100 MHz) to
improve quantitative measurement of the tumor microvasculature are
intriguing but as yet unproven in the clinic.
Positron Emission Tomography (PET) uses small doses of radiophar-
maceuticals to depict and quantify biochemistry rather than measure static
anatomic structures. The most commonly used agent in clinical PET
imaging is 2-(18F)Fluoro-2-Deoxyglucose (FDG). As a glucose analog,
FDG measures the uptake and phosphorylation of glucose as an indicatorof metabolic activity. Sequential PET imaging with FDG predicted
response to primary chemotherapy in 3 small pilot trials.287-289 Popular
tracers to quantify blood flow include technetium 99m technetium
sestamibi, thallium 201, and 15O-labeled water. The 99mTc sestamibi and
201Tl are taken up so avidly by most tissues that levels predominantly
reflect relative blood flow. Although 99mTc sestamibi and 201Tl have
gained widespread acceptance for assessment of myocardial perfusion,
markedly increased uptake in tumors has also been demonstrated.290,291
Yoon et al292 evaluated 99mTc sestamibi uptake and washout in 31
patients with untreated primary breast cancer. Both early and late
tumor-to-normal breast ratios correlated well with tumor MVD.292 The15O-labeled water has a short half-life (2 minutes), mandating cyclotron
production near the PET facility. However, 15O-labeled water can
quantify perfusion (milliliters/gram/minute) in all body tissues including
breast cancer. A small pilot study in patients with breast cancer using15O-labeled water found increased blood flow associated with the tumor
compared with surrounding normal breast tissue but did not attempt anycorrelation with histologic study or microvessel density.293 Absolute
tumor-associated blood volume can be calculated by use of carbon
11-labeled carbon monoxide, either as an inhaled gas or mixed with
whole blood ex vivo.294 The 15O-labeled oxygen has been used to
measure changes in tumor oxygen metabolism during therapy.295 Several
novel PET imaging strategies are currently in development to quantify
tumor hypoxia, proliferation index, apoptosis, receptor/ligand interac-
tions, and angiogenesis-related gene expression.296
Magnetic resonance imaging (MRI) has been used to evaluate tumor-
associated vasculature with either intrinsic or contrast-enhanced methods.
Intrinsic methods use pulse sequences that detect the motion of water in
the vascular bed297,298 or the distortion of the magnetic field by
deoxyhemoglobin.299,300 Intrinsic contrast methods rely solely on intra-
38 Curr Probl Cancer, January/February 2002

8/3/2019 SledgeJr 2002 Current Problems in Cancer
http://slidepdf.com/reader/full/sledgejr-2002-current-problems-in-cancer 34/54
vascular red blood cells and are not affected by changes in vascular
permeability but have a lower contrast-to-noise ratio limiting resolution.
Dynamic contrast enhanced MRI with small molecular contrast media
that equilibrate quickly between blood and the extracellular space is
dependent on the tumor MVD, vascular permeability (K21) and the
transfer constant (Ktrans permeability-surface area product per unit
volume of tissue). Such quantitative MRI parameters have been correlated
with tumor MVD and VEGF expression in several studies (Table 6).
Macromolecular contrast agents quantitatively assay microvascular
hyperpermeability and therefore produce an increased signal-to-noise
ratio. In a pilot study of 32 patients, tumors with the most intense early
signal enhancement and rapid contrast washout (high signal enhancement
ratio) had the highest MVD.301 A similar contrast-enhanced method
correlated well with changes in tumor necrosis and increasing vascular
permeability after treatment with tamoxifen302 or a monoclonal antibodydirected against VEGF.303
Future Prospects and ConclusionsAngiogenesis clearly represents a central theme in the genesis and
progression of human cancers. Will it represent a central therapeutic
TABLE 6. Contrast Enhanced MR parameters compared to angiogenesis in breast cancer
Investigator
No.
tumors(B:M)
MR
parameter VEGF MVD
Comparisons with MVD
(unless otherwise
noted)
r P
Buada331 20:51 steepest slope – CD34 0.83 .001
Stomper332 23:25 max. – FVIII NR .02
amplitude
Buckley333 0:40 enhancement – FVIII 0.47 .002
at 1 minute
Hulka334 36:21 extraction – FVIII 0.36 .01
flow product
Ikeda
335
29:61 K
trans
– NR 0.89
.01Knopp336 20:7 K21 IHC CD31 K21/VEGF,
0.52
.05
MVD/VEGF() NS
MVD/VEGF(),
0.71
.07
Matsubayashi337 4:31 rim IHC ND VEGF, NR .008
enhancement
B , benign; M , malignant; NS , not significant; NR , not reported; IHC , immunohistochemistry;
ND , not done; K trans, permeability surface area product per unit volume of tissue; K 21
, vascular
permeability.
Curr Probl Cancer, January/February 2002 39

8/3/2019 SledgeJr 2002 Current Problems in Cancer
http://slidepdf.com/reader/full/sledgejr-2002-current-problems-in-cancer 35/54
approach in years to come? Although it is too early to claim victory for
the antiangiogenics, it is not too soon to predict the successful integration
of some form of antiangiogenic therapy into routine clinical practice. Tobelieve otherwise would be to assume that angiogenesis is both biologi-
cally crucial and therapeutically unimportant, an unlikely paradox.
The major barriers to the use of antiangiogenic therapies—practical and
psychological—are real. For many human cancers we lack a good sense
of which angiogenic factors are crucial (crucial in the sense that the tumor
cannot survive or grow without the factor). For many tumors the
redundancy of proangiogenic factors may prove a barrier to individual
treatments. The existence of resistance will result in the death of earlyhopes of a therapy “resistant to resistance.” The presence of well-
established vascular networks in large tumors may render our normal
fashion of testing novel agents (beginning with the most refractory tumors
and progressing to the smallest, least treated tumors) a prescription for
therapeutic failure. Antiangiogenic therapies may have hidden toxicities
that may be related to mechanism or drug class, toxicities that may only
become apparent with prolonged exposure. These barriers, although real,
should not blind us to the promise of this therapy. We are still in the
beginning of a revolution, not at its end.304-337
REFERENCES1. Folkman J. What is the evidence that tumors are angiogenesis dependent? J Natl
Cancer Inst 1990;82:4-6.
2. Pepper M, Mandriota S, Vassalli J, et al. Angiogenesis-regulating cytokines:
activities and interactions. Curr Top Microbiol Immunol 1996;213(pt 2):31-67.
3. Eberhard A, Kahlert S, Goede V. Heterogeneity of angiogenesis and blood vessel
maturation in human tumors: implications for antiangiogenic tumor therapies.Cancer Res 2000;60:1388-93.
4. Liu W, Ahmad S, Reinmuth N, et al. Endothelial cell survival and apoptosis in the
tumor vasculature. Apoptosis 2000;5:323-8.
5. Hanahan D. Signaling vascular morphogenesis and maintenance. Science 1997;
277:48-50.
6. Brown JM, Giaccia AJ. The unique physiology of solid tumors: opportunities (and
problems) for cancer therapy. Cancer Res 1998;58:1408-16.
7. Liotta LA, Steeg PS, Stetler-Stevenson WG. Cancer metastasis and angiogenesis:
An imbalance of positive and negative regulation. Cell 1991;64:327-336.
8. Bos R, Zhong H, Hanrahan C, et al. Levels of hypoxia-inducible factor-1a duringbreast carcinogenesis. J Natl Cancer Inst 2001;93:309-13.
9. Heffelfinger S, Miller M, Yassin R, et al. Angiogenic growth factors in preinvasive
breast disease. Clin Cancer Res 1999;5:2867-76.
10. Guidi A, Schnitt S, Fischer L, et al. Vascular permeability factor (vascular
endothelial growth factor) expression and angiogenesis in patients with ductal
carcinoma in situ of the breast. Cancer 1997;80:1945-53.
40 Curr Probl Cancer, January/February 2002

8/3/2019 SledgeJr 2002 Current Problems in Cancer
http://slidepdf.com/reader/full/sledgejr-2002-current-problems-in-cancer 36/54
11. Couvelard A, Paraf F, Gratio V, et al. Angiogenesis in the neoplastic sequence of
Barrett’s oesophagus: Correlation with VEGF expression. J Pathol 2000;192:14-8.
12. Kondo Y, Arii S, Furutani M, et al. Implication of vascular endothelial growth
factor and p53 status for angiogenesis in noninvasive colorectal carcinoma. Cancer
2000;88:1820-7.
13. Linderholm B, Lindh B, Beckman L, et al. The prognostic value of vascular
endothelial growth factor (VEGF) and basic fibroblast growth factor (bFGF) and
associations to first metastasis site in 1307 patients with primary breast cancer. Proc
Am Soc Clin Oncol 2001;20:4a (abstract 13).
14. Foekens J, Peters H, Grebenchtchikov N, et al. High tumor levels of vascular
endothelial growth factor predict poor response to systemic therapy in advanced
breast cancer. Cancer Res 2001;61:5407-14.
15. Quan Z, Wu K, Wang J, et al. Association of p53, p16, and vascular endothelialgrowth factor protein expressions with the prognosis and metastasis of gallbladder
cancer. J Am Coll Surg 2001;193:380-3.
16. Shih C, Ozawa S, Ando N, et al. Vascular endothelial growth factor expression
predicts outcome and lymph node metastasis in squamous cell carcinoma of the
esophagus. Clin Cancer Res 2000;6:1161-8.
17. Ichikura T, Tomimatsu S, Ohkura E, et al. Prognostic significance of the expression
of vascular endothelial growth factor (VEGF) and VEGF-C in gastric carcinoma.
J Surg Oncol 2001;78:132-7.
18. West A, O’Donnell M, Charlton R, et al. Correlation of vascular endothelial growth
factor expression with fibroblast growth factor-8 expression and clinico-pathologicparameters in human prostate cancer. Br J Cancer 2001;85:576-83.
19. Aguayo A, Estey E, Kantarjian H, et al. Cellular vascular endothelial growth factor
is a predictor of outcome in patients with acute myeloid leukemia. Blood
1999;94:3717-21.
20. Smith B, Smith G, Carter D, et al. Prognostic significance of vascular endothelial
growth factor protein levels in oral and oropharyngeal squamous cell carcinoma.
J Clin Oncol 2000;18:2046-52.
21. Mineta H, Miura K, Ogino T, et al. Prognostic value of vascular endothelial growth
factor (VEGF) in head and neck squamous cell carcinomas. Br J Cancer 2000;83:775-81.
22. Yudoh K, Kanamori M, Ohmori K, et al. Concentration of vascular endothelial
growth factor in the tumour tissue as a prognostic factor of soft tissue sarcomas.
Br J Cancer 2001;84:1610-5.
23. Lee Y, Tokunaga T, Oshika Y, et al. Cell-retained isoforms of vascular endothelial
growth factor (VEGF) are correlated with poor prognosis in osteosarcoma. Eur J
Cancer 1999;35:1989-93.
24. Yuan A, Yu C, Kuo S, et al. Vascular endothelial growth factor 189 mRHA isoform
expression specifically correlates with tumor angiogenesis, patient survival, and
postoperative relapse in non-small-cell lung cancer. J Clin Oncol 2001;19:432-41.25. Han H, Silverman J, Santucci T, et al. Vascular endothelial growth factor
expression in stage I non-small cell lung cancer correlates with neoangiogenesis
and a poor prognosis. Ann Surg Oncol 2001;8:72-9.
26. Yuan A, Yu C, Chen W, et al. Correlation of total VEGF mRNA and protein
expression with histologic type, tumor angiogenesis, patient survival and timing of
relapse in non-small-cell lung cancer. Int J Cancer 2000;89:475-83.
Curr Probl Cancer, January/February 2002 41

8/3/2019 SledgeJr 2002 Current Problems in Cancer
http://slidepdf.com/reader/full/sledgejr-2002-current-problems-in-cancer 37/54
27. Sheng H, Aoe M, Doihara H, et al. Prognostic value of vascular endothelial growth
factor expression in primary lung carcinoma. Acta Medica Okayama 2000;54:119-
26.
28. Klein M, Vignaud J, Hennequin V, et al. Increased expression of the vascular
endothelial growth factor is a pejorative prognosis marker in papillary thyroid
carcinoma. J Clin Endocrinol Metab 2001;86:656-8.
29. Cheng W, Chen C, Lee C, et al. Vascular endothelial growth factor and prognosis
of cervical carcinoma. Obstet Gynecol 2000;96:721-6.
30. Loncaster J, Cooper R, Logue J, et al. Vascular endothelial growth factor (VEGF)
expression is a prognostic factor for radiotherapy outcome in advanced carcinoma
of the cervix. Br J Cancer 2000;83:620-5.
31. Shen G, Ghazizadeh M, Kawanami O, et al. Prognostic significance of vascular
endothelial growth factor expression in human ovarian carcinoma. Br J Cancer2000;83:196-203.
32. Seo Y, Baba H, Fukuda T, et al. High expression of vascular endothelial growth
factor is associated with liver metastasis and a poor prognosis for patients with
ductal pancreatic adenocarcinoma. Cancer 2000;88:2239-45.
33. Oehring R, Miletic M, Valter M, et al. Vascular endothelial growth factor (VEGF)
in astrocytic gliomas—a prognostic factor? J Neuro-Oncol 1999;45:117-25.
34. Gunningham S, Currie M, Han C, et al. VEGF-B expression in human primary
breast cancers is associated with lymph node metastasis but not angiogenesis.
J Pathol 2001;193:325-32.
35. Karpanen T, Egeblad M, Karkkainen M, et al. Vascular endothelial growth factorC promotes tumor 1ymphangiogenesis and intralymphatic tumor growth. Cancer
Res 2001;61:1786-90.
36. Skobe M, Hawighorst T, Jackson D, et al. Induction of tumor lymphangiogenesis
by VEGF-C promotes breast cancer metastasis. Nature Med 2001;7:192-8.
37. Valtola R, Salven P, Heikkila P, et al. VEGFR-3 and its ligand VEGF-C are
associated with angiogenesis in breast cancer. Am J Pathol 1999;154:1381-90.
38. Kinoshita J, Kitamura K, Kabashima A, et al. Clinical significance of vascular
endothelial growth factor-C (VRGF-C) in breast cancer. Breast Cancer Res Treat
2001;66:159-64.39. Carter W. HER2 signaling—induced microvessel dismantling. Surgery 2001;130:
382-7.
40. Currie M, Gunningham S, Han C, et al. Angiopoietin-1 is inversely related to
thymidine phosphorylase expression in human breast cancer, indicating a role in
vascular remodeling. Clin Cancer Res 2001;7:918-27.
41. Wurmbach J, Hammerer P, Sevinc S, et al. The expression of angiopoietins and
their receptor Tie-2 in human prostate carcinoma. Anticancer Res 2000;20:5,217-
20.
42. Ding H, Roncari L, Wu X, et al. Expression and hypoxic regulation of angiopoi-
etins in human astrocytomas. Neuro-Oncology 2001;3:1-10.43. Etoh T, Inoue H, Tanaka S, et al. Angiopoietin-2 is related to tumor angiogenesis
in gastric carcinoma: possible in vivo regulation via induction of proteases. Cancer
Res 2001;61:2145-53.
44. Takahama M, Tsutsumi M, Tsujiuchi T, et al. Enhanced expression of Tie2, its
ligand angiopoietin-1, vascular endothelial growth factor, and CD31 in human
non-small cell lung carcinomas. Clin Cancer Res 1999;5:2506-10.
42 Curr Probl Cancer, January/February 2002

8/3/2019 SledgeJr 2002 Current Problems in Cancer
http://slidepdf.com/reader/full/sledgejr-2002-current-problems-in-cancer 38/54
45. Hayes AJ, Huang WQ, Yu J, et al. Expression and functon of angiopoietin-1 in
breast cancer. Br J Cancer 2000;83:1154-60.
46. Peters K, Coogan A, Berry D, et al. Expression of Tie2/Tek in breast tumour
vasculature provides a new marker for evaluation of tumour angiogenesis. Br J
Cancer 1998;77:51-6.
47. Eppenberger U, Kueng W, Schlaeppi J, et al. Markers of tumor angiogenesis and
proteolysis independently define high- and low-risk subsets of node-negative breast
cancer patients. J Clin Oncol 1998;16:3129-36.
48. Blanckaert V, Hornez L, Hebbar M, et al. Distribution and prognostic value of the
fibroblast growth factor-2 low-af finity binding sites in human breast cancer.
Anticancer Res 2000;20:3913-8.
49. Blanckaert V, Hebbar M, Louchez M-M, et al. Basic fibroblast growth factor
receptors and their prognostic value in human breast cancer. Clin Cancer Res1998;4:2939-47.
50. Colomer R, Aparicio J, Montero S, et al. Low levels of basic fibroblast growth
factor (bFGF) are associated with a poor prognosis in human breast carcinoma. Br J
Cancer 1997;76:1215-20.
51. Yiengou C, Gomm J, Coope R, et al. Fibroblast growth factor 2 in breast cancer:
occurrence and prognostic significance. Br J Cancer 1997;75:28-33.
52. Maloof P, Weng Q, Wang H, et al. Overexpression of basic fibroblast growth factor
(FGF-2) downregulates Bcl-2 and promotes apoptosis in MCF-7 human breast
cancer cells. Breast Cancer Res Treat 1999;56:153-67.53. Fenig E, Livnat T, Sharkon-Polak S, et al. Basic fibroblast growth factor potentiates
cisplatinum-induced cytotoxicity in MCF-7 human breast cancer cells. J Cancer
Res Clin Oncol 1999;125:556-62.
54. Brooks PC, Clark RA, Cheresh DA. Requirement of vascular integrin alpha v beta
3 for angiogenesis. Science 1994;264:569-71.
55. Eliceiri B, Klemke R, Stromblad S, et al. Integrin alphavbeta3 requirement for
sustained mitogen-activated protein kinase activity during angiogenesis. J Cell Biol
1998;140:1255-63.
56. Brooks P, Montgomery A, Rosenfeld M, et al. Integrin avb3 antagonists promote
tumor regression by inducing apoptosis of angiogenic blood vessels. Cell 1994;79:
1157-64.
57. Brooks PC, Stromblad S, Klemke R, et al. Antiintegrin alpha v beta 3 blocks human
breast cancer growth and angiogenesis in human skin. J Clin Invest 1995;96:1815-
22.
58. O’Reilly MS, Holmgren L, Chen C, et al. Angiostatin induces and sustains
dormancy of human primary tumors in mice. Nat Med 1996;2:689-92.
59. Moser TL, Kenan DJ, Ashley TA, et al. Endothelial cell surface F1-F0 ATP
synthase is active in ATP synthesis and is inhibited by angiostatin. Proc Natl Acad
Sci USA 2001;98:6656-61.60. Hari D, Beckett M, Sukhatme V, et al. Angiostatin induces mitotic cell death of
proliferating endothelial cells. Molec Cell Biol Res Commun 2000;3:277-82.
61. Volm M, Mattern J, Koomagi R. Angiostatin expression in non-small cell lung
cancer. Clin Cancer Res 2000;6:3236-40.
62. Migita T, Oda Y, Naito S, et al. The accumulation of angiostatin-like fragments in
human prostate carcinoma. Clin Cancer Res 2001;7:2750-6.
Curr Probl Cancer, January/February 2002 43

8/3/2019 SledgeJr 2002 Current Problems in Cancer
http://slidepdf.com/reader/full/sledgejr-2002-current-problems-in-cancer 39/54
63. Cao Y, Veitonmaki N, Keough K, et al. Elevated levels of urine angiostatin and
plasminogen/plasmin in cancer patients. Int J Nuclear Med 2000;5:547-51.
64. O’Reilly MS, Boehm T, Shing Y, et al. Endostatin: an endogenous inhibitor of
angiogenesis and tumor growth. Cell 1997;88:277-85.
65. Ferreras M, Felbor U, Lenhard T, et al. Generation and degradation of human
endostatin proteins by various proteinases. FEBS Lett 2000;486:247-51.
66. Kuo C, Farnebo F, Yu E, et al. Comparative evaluation of the antitumor activity of
antiangiogenic proteins delivered by gene transfer. Proc Natl Acad Sci USA
2001;98:4605-10.
67. Jiang L, Jha V, Dhanabal M, et al. Intracellular Ca(2) signaling in endothelial
cells by the angiogenesis inhibitors endostatin and angiostatin. Am J Physiol-Cell
Physiol 2001;280:C1140-50.
68. MacDonald NJ, Shivers WY, Narum DL, et al. Endostatin binds tropomyosin: apotential modulator of the antitumor activity of endostatin. J Biol Chem 2001;276:
25190-6.
69. Shichiri M, Hirata Y. Antiangiogenesis signals by endostatin. FASEB J 2001;15:
1044-53.
70. Hats K, Fujiwaki R, Nakayama K, et al. Expression of the endostatin gene in
epithelial ovarian cancer. Clin Cancer Res 2001;7:2405-9.
71. Musso O, Rehn M, Theret N, et al. Tumor progression is associated with a
significant decrease in the expression of the endostatin precursor collagen XVIII in
human hepatocellular carcinomas. Cancer Res 2001;61:45-9.
72. Kuroi K, Tanaka C, Toi M. Circulating levels of endostatin in cancer patients.Oncology Rep 2001;8:405-9.
73. Feldman A, Tamarkin L, Paciotti G, et al. Serum endostatin levels are elevated and
correlate with serum vascular endothelial growth factor levels in patients with stage
IV clear cell renal cancer. Clin Cancer Res 2000;6:4628-34.
74. Feldman A, Pak H, Yang J, et al. Serum endostatin levels are elevated in patients
with soft tissue sarcoma. Cancer 2001;91:1525-9.
75. de Fraipont F, Nicholson A, Feige J, et al. Thrombospondins and tumor angiogen-
esis. Trends Molec Med 2001;7:401-7.
76. Hawighorst T, Velasco P, Streit M, et al. Thrombospondin-2 plays a protective rolein multistep carcinogenesis: a novel host antitumor defense mechanism. EMBO J
2001;20:2631-4.
77. Kodama J, Hashimoto I, Seki N, et al. Thrombospondin-1 and -2 messenger RNA
expression in invasive cervical cancer: correlation with angiogenesis and prognosis.
Clin Cancer Res 2001;7:2826-31.
78. Maeda K, Nishiguchi Y, Kang S, et al. Expression of thrombospondin-1 inversely
correlated with tumor vascularity and hematogenous metastasis in colon cancer.
Oncol Reports 2001;8:763-6.
79. Tokunaga T, Nakamura M, Oshika Y, et al. Thrombospondin 2 expression is
correlated with inhibition of angiogenesis and metastasis of colon cancer. Br JCancer 1999;79:354-9.
80. Grossfeld G, Ginsberg D, Stein J, et al. Thrombospondin-1 expression in bladder
cancer: association with p53 alterations, tumor angiogenesis, and tumor progres-
sion. J Natl Cancer Inst 1997;89:219-27.
81. Kazuno M, Tokunaga T, Oshika Y, et al. Thrombospondin-2 (TSP2) expression is
inversely correlated with vascularity in glioma. Eur J Cancer 1999;35:502-6.
44 Curr Probl Cancer, January/February 2002

8/3/2019 SledgeJr 2002 Current Problems in Cancer
http://slidepdf.com/reader/full/sledgejr-2002-current-problems-in-cancer 40/54
82. Gasparini G, Toi M, Biganzoli E, et al. Thrombospondin-1 and -2 in node-negative
breast cancer: correlation with angiogenic factors, p53, cathepsin D, hormone
receptors and prognosis. Oncol 2001;60:72-80.
83. Seki N, Kodama J, Hashimoto I, et al. Thrombospondin-1 and -2 messenger RNA
expression in normal and neoplastic endometrial tissues: correlation with angio-
genesis and prognosis. Int J Oncol 2001;19:305-10.
84. Hanahan D, Folkman J. Patterns and emerging mechanisms of the angiogenic
switch during tumorigenesis. Cell 1996;86:353-64.
85. Santinelli A, Baccarini M, Colanzi P, et al. Microvessel quantitation in intraductal
and early invasive breast carcinomas. Anal Quant Cytol Histol 2000;22:277-84.
86. Brown L, Guidi A, Schnitt S, et al. Vascular stroma formation in carcinoma in situ,
invasive carcinoma, and metastatic carcinoma of the breast. Clin Cancer Res
1999;5:1041-56.87. Guidi AJ, Fischer L, Harris JR, et al. Microvessel density and distribution in ductal
carcinoma in situ of the breast. J Natl Cancer Inst 1994;86:614-9.
88. Zolota V, Gerokosta A, Melachrinou M, et al. Microvessel density, proliferating
activity, p53 and bcl-2 expression in in situ ductal carcinoma of the breast.
Anticancer Res 1999;19:3269-74.
89. Arapandoni-Dadioti P, Giatromanolaki A, Trihia H, et al. Angiogenesis in ductal
breast carcinoma: comparison of microvessel density between primary tumour and
lymph node metastasis. Cancer Lett 1999;137:145-50.
90. Weidner N, Semple J, Welch W, et al. Tumor angiogenesis and metastasis-
correlation in invasive breast carcinoma. N Engl J Med 1991;324:1-8.91. de Jong JS, van Diest PJ, Baak JP. Heterogeneity and reproducibility of microvessel
counts in breast cancer. Lab Invest 1995;73:922-6.
92. Fox S, Leek R, Weekes M, et al. Quantitation and prognostic value of breast cancer
angiogenesis: comparison of microvessel density, Chalkley count, and computer
image analysis. J Pathol 1995;177:275-83.
93. Hansen S, Grabau D, Rose C, et al. Angiogenesis in breast cancer: a comparative
study of the observer variability of methods for determining microvessel density.
Lab Invest 1998;78:1563-73.
94. Hansen S, Grabau D, Sorensen F, et al. The prognostic value of angiogenesis byChalkley counting in a confirmatory study design on 836 breast cancer patients.
Clin Cancer Res 2000;6:139-6.
95. Hegde P, Brenski A, Caldarelli D, et al. Tumor angiogenesis and p53 mutations:
prognosis in head and neck cancer. Arch Otolaryngol Head Neck Surg 1998;124:
80-5.
96. Kohlberger P, Obermair A, Sliutz G, et al. Quantitative immunohistochemistry of
factor VIII-related antigen in breast carcinoma: a comparison of computer-assisted
image analysis with established counting methods. Am J Clin Pathol 1996;105:
705-10.
97. Axelsson K, Ljung B, Moore D, et al. Tumor angiogenesis as a prognostic factorfor invasive ductal breast carcinoma. J Natl Cancer Inst 1995;87:997-1008.
98. Rubin M, Buyyounouski M, Bagiella E, et al. Microvessel density in prostate
cancer: lack of correlation with tumor grade, pathologic stage, and clinical
outcome. Urology 1999;53:542-7.
99. Miralbell R, Tolnay M, Bieri S, et al. Pediatric medulloblastoma: prognostic value
of p53, bcl-2, Mib-1, and microvessel density. J Neuro-Oncol 1999;45:103-10.
Curr Probl Cancer, January/February 2002 45

8/3/2019 SledgeJr 2002 Current Problems in Cancer
http://slidepdf.com/reader/full/sledgejr-2002-current-problems-in-cancer 41/54
100. Fitzgibbons P, Page D, Weaver D, et al. Prognostic factors in breast cancer: College
of American Pathologists Consensus Statement 1999. Arch Pathol Lab Med
2000;124:966-78.
101. Karrison T, Ferguson D, Meier P. Dormancy of mammary carcinoma after
mastectomy. J Natl Cancer Inst 1999;91:80-5.
102. Holmgren L, O’Reilly M, Folkman J. Dormancy of micrometastases: balanced
proliferation and apoptosis in the presence of angiogenesis suppression. Nature
Med 1995;1:149-53.
103. O’Reilly M, Holmgren L, Chen C, et al. Angiostatin induces and sustains dormancy
of human primary tumors in mice. Nature Med 1996;2:689-92.
104. Guba M, Cernaianu G, Koehl G, et al. A primary tumor promotes dormancy of
solitary tumor cells before inhibiting angiogenesis. Cancer Res 2001;61:5575-9.
105. List A. Vascular endothelial growth factor signaling pathway as an emerging targetin hematologic malignancies. The Oncologist 2001;6(suppl. 5):24-31.
106. Perez-Atayde A, Sallan S, Tedrow U, et al. Spectrum of tumor angiogenesis in the
bone marrow of children with acute lymphoblastic leukemia. Am J Pathol
1997;150:815-21.
107. Aguato A, Kantarjian H, Manshouri T, et al. Angiogenesis in acute and chromic
leukemias and myelodysplastic syndromes. Blood 2000;96:2240-45.
108. Ridell B, Norrby K. Intratumoral microvascular density in malignant lymphomas of
B-cell origin. APMIS 2001;109:66-72.
109. Rajkumar S, Leong T, Roche P, et al. Prognostic value of bone marrowangiogenesis in multiple myeloma. Clin Cancer Res 2000;6:3111-6.
110. Pruneri G, Bertolini F, Soligo D, et al. Angiogenesis in myelodysplastic syndromes.
Br J Cancer 1999;81:1398-1401.
111. Sezer O, Niemoller K, Eucker J, et al. Bone marrow microvessel density is a
prognostic factor for survival in patients with multiple myeloma. Ann Hematol
2000;79:574-7.
112. Mesa R, Hanson C, Rajkumar S, et al. Evaluation and clinical correlations of bone
marrow angiogenesis in myelofibrosis with myeloid metaplasia. Blood 2000;96:
3374-80.
113. Bertolini F, Paolucci M, Peccatori F, et al. Angiogenic growth factors and
endostatin in non-Hodgkin’s lymphoma. Br J Haematol 1999;106:504-9.
114. Bellamy W, Richter L, Sirjani D, et al. Vascular endothelial growth factor is an
autocrine promoter of abnormal localized immature myeloid precursors and
leukemia progenitor formation in myelodysplastic syndromes. Blood 2001;97:
1427-34.
115. Hayashibara T, Yamada Y, Miyanishi T, et al. Vascular endothelial growth factor
and cellular chemotaxis: a possible autocrine pathway in adult T-cell leukemia cell
invasion. Clin Cancer Res 2001;7:2719-26.
116. Dias S, Hattori K, Heissig B, et al. Inhibition of both paracrine and autocrineVEGF/VEGFR-2 signaling pathways is essential to induce long-term remission of
xenotransplanted human leukemias. Proc Natl Acad Sci USA 2001;98:10857-62.
117. Miller K, Sweeney C, Sledge G. Redefining the target: Chemotherapeutics as
antiangiogenics. J Clin Oncol 2001;19:1195-206.
118. Wiseman H. Tamoxifen: new membrane-mediated mechanisms of action and
therapeutic advances. Trends Pharmacol Sci 1994;15:83-9.
46 Curr Probl Cancer, January/February 2002

8/3/2019 SledgeJr 2002 Current Problems in Cancer
http://slidepdf.com/reader/full/sledgejr-2002-current-problems-in-cancer 42/54
119. Gagliardi A, Collins DC. Inhibition of angiogenesis by antiestrogens. Cancer Res
1993;53:533-5.
120. Gagliardi AR, Hennig B, Collins DC. Antiestrogens inhibit endothelial cell growth
stimulated by angiogenic growth factors. Anticancer Res 1996;16:1101-6.
121. Haran EF, Maretzek AF, Goldberg I, et al. Tamoxifen enhances cell death in
implanted MCF7 breast cancer by inhibiting endothelium growth. Cancer Res
1994;54:5511-4.
122. Linder C, Bystrom P, Engel G, et al. Correlation between basic fibroblast growth
factor immunostaining of stromal cells and stromelysin-3 mRNA expression in
human breast carcinoma. Br J Cancer 1998;77:941-5.
123. Silva ID, Salicioni AM, Russo IH, et al. Tamoxifen down-regulates CD36
messenger RNA levels in normal and neoplastic human breast tissues. Cancer Res
1997;57:378-81.124. Sweeney C, Miller K, Sissons S, et al. The antiangiogenic property of docetaxel is
synergistic with a recombinant humanized monoclonal antibody against vascular
endothelial growth factor or 2-methoxyestradiol but antagonized by endothelial
growth factors. Cancer Res 2001;61:3369-72.
125. Belotti D, Nicoletti I, Vergani V, et al. Paclitaxel (Taxol), a microtubule affecting
drug, inhibits tumor induced angiogenesis. Proc Am Assoc Cancer Res 1996;37:57
[Abstract 397].
126. Schirner M, Hoffmann J, Menrad A, et al. Antiangiogenic chemotherapeutic
agents: characterization in comparison to their tumor growth inhibition in human
renal cell carcinoma models. Clin Cancer Res 1998;4:1331-6.127. Benbow U, Maltra R, Hamilton J, et al. Selective modulation of collagenase 1 gene
expression by the chemotherapeutic agent doxorubicin. Clin Cancer Res 1999;5:
203-8.
128. Lau D, Young L, Xue L, et al. Paclitaxel: an angiogenesis antagonist in a metastatic
breast cancer model [abstract]. Proc Am Soc Clin Oncol 1998;17:107.
129. Klauber N, Parangi S, Flynn E, et al. Inhibition of angiogenesis and breast cancer
in mice by the microtubule inhibitors 2-methoxyestradiol and taxol. Cancer Res
1997;57:81-6.
130. Iigo M, Shimamura M, Sagawa K, et al. Characteristics of the inhibitory effect of mitoxantrone and pirarubicin on lung metastases of colon carcinoma 26. Jpn J
Cancer Res 1995;86:867-72.
131. Slaton JW, Perrotte P, Inoue K, et al. Interferon-alpha-mediated down-regulation of
angiogenesis-related genes and therapy of bladder cancer are dependent on
optimization of biological dose and schedule. Clin Cancer Res 1999;5:2726-34.
132. Browder T, Butterfield C, Kraling B, et al. Antiangiogenic scheduling of chemo-
therapy improves ef ficacy against experimental drug-resistant cancer. Cancer Res
2000;60:1878-86.
133. Klement G, Baruchel S, Rak J, et al. Continuous low-dose therapy with vinblastine
and VEGF receptor-2 antibody induces sustained tumor regression without overttoxicity. J Clin Invest 2000;105:R15-R24.
134. Wild R, Ghosh K, Dings R, et al. Carboplatin differentially induces the VEGF
stress response in endothelial cells: potentiation of anti-tumor effects by combina-
tion treatment with antibody to VEGF [abstract]. Proc Am Assoc Canc Res
2000;41:307.
135. Hanahan D, Bergers G, Bergsland E. Less is more, regularly: metronomic dosing
Curr Probl Cancer, January/February 2002 47

8/3/2019 SledgeJr 2002 Current Problems in Cancer
http://slidepdf.com/reader/full/sledgejr-2002-current-problems-in-cancer 43/54
of cytotoxic drugs can target tumor angiogenesis in mice [comment]. J Clin Invest
2000;105:1045-7.
136. Fennelly D, Aghajanian C, Shapiro F, et al. Phase I and pharmacologic study of
paclitaxel administered weekly in patients with relapsed ovarian cancer. J Clin
Oncol 1997;15:187-92.
137. Seidman AD, Hochhauser D, Gollub M, et al. Ninety-six-hour paclitaxel infusion
after progression during short taxane exposure: a phase II pharmacokinetic and
pharmacodynamic study in metastatic breast cancer. J Clin Oncol 1996;14:1877-84.
138. Engelsman E, Klijn J, Rubens R, et al. “Classical” CMF versus a 3-weeekly
intravenous CMF schedule in postmenopausal patients with advanced breast
cancer. Eur J Cancer 1991;27:966-70.
139. Rocca A, Colleoni M, Masci G, et al. Low dose oral methotrexate and cyclophos-
phamide in metastatic breast cancer: an attempt to exploit the antiangiogenicactivity of common chemotherapeutics. Proc Am Soc Clin Oncol 2001;20:30a.
140. Toi M, Bando H, Kuroi K. The predictive value of angiogenesis for adjuvant
therapy in breast cancer. Breast Cancer 2000;7:311-4.
141. Pidgeon G, Harmey J, Foley D, et al. Vascular endothelial growth factor (VEGF)
upregulates Bcl-2 and inhibits apoptosis in human and murine mammary adeno-
carcinoma cells. Br J Cancer 2001;85:273-8.
142. Bachelder R, Crago A, Chung J, et al. Vascular endothelial growth factor is an
autocrine survival factor for neuropilin-expressing breast carcinoma cells. Cancer
Res 2001;61:5736-40.143. Fisher C, Gilbertson-Beadling S, Powers EA, et al. Interstitial collagenase is
required for angiogenesis in vitro. Developmental Biol 1994;162:499-510.
144. Low J, Johnson M, Bone E, et al. The matrix metalloproteinase inhibitor batimastat
(BB-94) retards human breast cancer solid tumor growth but not ascites formation
in nude mice. Clin Cancer Res 1996;2:1207-14.
145. Kurizaki T, Toi M, Tominaga T. Relationship between matrix metalloproteinase
expression and tumor angiogenesis in human breast carcinoma. Oncol Rep
1998;5:673-7.
146. Taraboletti G, Garofalo A, Belotti D, et al. Inhibition of angiogenesis and murine
hemangioma growth by Batimastat, a synthetic inhibitor of matrix metalloprotein-
ases. J Natl Cancer Inst 1995;87:293-8.
147. Tamargo RJ, Bok RA, Brem H. Angiogenesis inhibition by minocycline. Cancer
Res 1991;51:672-5.
148. Fife RS, Sledge GW Jr. Effects of doxycycline on in vitro growth, migration, and
gelatinase activity of breast carcinoma cells. J Lab Clin Med 1995;125:407-11.
149. Sledge GW, Qulali M, Goulet R, et al. Effect of matrix metalloproteinase inhibitor
batimastat on breast cancer regrowth and metastasis in athymic mice. J Natl Cancer
Inst 1995;87:1546-50.
150. Steward WP, Thomas AL. Marimastat: the clinical development of a matrixmetalloproteinase inhibitor. Expert Opin Investig Drugs 2000;9:2913-22.
151. Wojtowicz-Praga S, Low J, Dickson R, et al. Pharmacokinetics (PK) of marimastat
(BB-2516), a novel matrix metalloproteinase inhibitor administered orally to
patients with metastatic lung cancer. Proc Am Soc Clin Oncol 1996;15:490
[Abstract 1565].
152. Miller K, Gradishar W, Schucter L, et al. A randomized Phase II pilot trial of
48 Curr Probl Cancer, January/February 2002

8/3/2019 SledgeJr 2002 Current Problems in Cancer
http://slidepdf.com/reader/full/sledgejr-2002-current-problems-in-cancer 44/54
adjuvant marimastat in patients with early breast cancer. Proc Am Soc Clin Oncol
2000;19:96a.
153. Warren RS, Yuan H, Matli MR, et al. Regulation by vascular endothelial growth
factor of human colon cancer tumorigenesis in a mouse model of experimental liver
metastasis. J Clin Invest 1995;95:1789-97.
154. Kim KJ, Li B, Winer J, et al. Inhibition of vascular endothelial growth:
factor-induced angiogenesis suppresses tumour growth in vivo. Nature 1993;362:
841-4.
155. Gordon MS, Margolin K, Talpaz M, et al. Phase I safety and pharmacokinetic study
of recombinant human anti-vascular endothelial growth factor in patients with
advanced cancer. J Clin Oncol 2001;19:843-50.
156. Sledge G, Miller K, Novotny W, et al. A phase II trial of single-agent rhuMAb
VEGF (recombinant humanized monoclonal antibody to vascular endothelialgrowth factor) in patients with relapsed metastatic breast cancer. Proc Am Soc Clin
Oncol 2000;19:3a [abstract 5c].
157. Millauer B, Longhi MP, Plate KH, et al. Dominant-negative inhibition of Flk-1
suppresses the growth of many tumor types in vivo. Cancer Res 1996;56:1615-20.
158. Fong TA, Shawver LK, Sun L, et al. SU5416 is a potent and selective inhibitor of
the vascular endothelial growth factor receptor (FIk-1/KDR) that inhibits tyrosine
kinase catalysis, tumor vascularization, and growth of multiple tumor types. Cancer
Res 1999;59:99-106.
159. Shaheen R, Davis D, Lin W, et al. Antiangiogenic therapy targeting the tyrosinekinase receptor for vascular endothelial growth factor receptor inhibits the growth
of liver metastasis and induces tumor and endothelial cell apoptosis. Cancer Res
1999;59:5412-6.
160. Rosen L, Kabbinavar F, Rosen P, et al. Phase I trial of SU5416, a novel
angiogenesis inhibitor in patients with advanced malignancies. Proc Am Soc Clin
Oncol 1998;17:218a.
161. Rosen L, Mulay M, Mayers A, et al. Phase I dose-escalating trial of SU5416, a
novel angiogenesis inhibitor in patients with advanced malignancies. Proc Am Soc
Clin Oncol 1999;18:161a.
162. Overmoyer B, Robertson K, Persons M, et al. A phase I pharmacokinetic and
pharmacodynamic study of SU5416 and doxorubicin in inflammatory breast cancer.
Proc Am Soc Clin Oncol 2001;20:99a [abstract 391].
163. Basser R, Hurwitz H, Barge A, et al. Phase I pharmacokinetic and biological study
of the angiogenesis inhibitor ZD6474 in patients with solid tumors. Proc Am Soc
Clin Oncol 2001;20:100a.
164. Sandberg JA, Bouhana KS, Gallegos AM, et al. Pharmacokinetics of an antiangio-
genic ribozyme (ANGIOZYME) in the mouse. Antisense Nucleic Acid Drug Dev
1999;9:271-7.
165. Sandberg J, Parker V, Blanchard K, et al. Pharmacokinetics and tolerability of anantiangiogenic ribozyme (ANGIOZYME) in healthy volunteers. J Clin Pharmacol
2000;40:1462-9.
166. Sandberg J, Sproul C, Blanchard K, et al. Acute toxicology and pharmacokinetic
assessment of a ribozyme (ANGIOZYME) targeting vascular endothelial growth
factor receptor mRNA in the cynomolgus monkey. Antisense Nucleic Acid Drug
Dev 2000;10:153-62.
Curr Probl Cancer, January/February 2002 49

8/3/2019 SledgeJr 2002 Current Problems in Cancer
http://slidepdf.com/reader/full/sledgejr-2002-current-problems-in-cancer 45/54
167. Weng D, Usman N. Angiozyme: a novel angiogenesis inhibitor. Curr Oncol Rep
2001;3:141-6.
168. Ciomei M, Pastori W, Mariana M, et al. New sulfonated A distamycin A
derivatives with bFGF complexing activity. Biochem Pharmacol 1994;47:295-302.
169. Zamai M, Caiolfa VR, Pines D, et al. Nature of interaction between basic fibroblast
growth factor and the antiangiogenic drug 7,7-(Carbonyl-bis[imino-N-methyl-4, 2-
pyrrolecarbonylimino[N-methyl-4,2-pyrrole]-carbonylimino])bis-(1, 3-naphthalene
disulfonate). Biophys J 1998;75:672-82.
170. Possati L, Campioni D, Sola F, et al. Antiangiogenic, antitumoural and antimeta-
static effects of two distamycin A derivatives with anti-HIV-1 Tat activity in a
Kaposi’s sarcoma-like murine model. Clin Exp Metastasis 1999;17:575-82.
171. Sola F, Capolongo L, Moneta D, et al. The antitumor ef ficacy of cytotoxic drugs is
potentiated by treatment with PNU 145156E, a growth-factor-complexing mole-cule. Cancer Chemother Pharmacol 1999;43:241-6.
172. deVries E, Groen H, Wynendaele W, et al. PNU-145156E - a novel angiogenesis
inhibitor in patients with soldi tumors: an update of a phase I and pharmacokinetic
study. Proc Am Soc Clin Oncol 1999;18:161a.
173. McLeskey S, Zhang L, Trock B, et al. Effects of AGM-1470 and pentosan
polysulphate on tumorigenicity and metastasis of FGF-transfected MCF-7 cells.
Br J Cancer 1996;73:1053-62.
174. Sasaki A, Alcalde RE, Nishiyama A, et al. Angiogenesis inhibitor TNP-470 inhibits
human breast cancer osteolytic bone metastasis in nude mice through the reduction
of bone resorption. Cancer Res 1998;58:462-7.175. Singh Y, Shikata N, Kiyozuka Y, et al. Inhibition of tumor growth and metastasis
by angiogenesis inhibitor TNP-470 on breast cancer cell lines in vitro and in vivo.
Breast Cancer Res Treat 1997;45:15-27.
176. Bhargava P, Marshall JL, Rizvi N, et al. A phase I and pharmacokinetic study of
TNP-470 administered weekly to patients with advanced cancer. Clin Cancer Res
1999;5:1989-95.
177. Stadler WM, Kuzel T, Shapiro C, et al. Multi-institutional study of the angiogenesis
inhibitor TNP-470 in metastatic renal carcinoma. J Clin Oncol 1999;17:2541-5.
178. Logothetis CJ, Wu KK, Finn LD, et al. Phase I trial of the angiogenesis inhibitorTNP-470 for progressive androgen-independent prostate cancer. Clin Cancer Res
2001;7:1198-203.
179. Dezube BJ, Von Roenn JH, Holden-Wiltse J, et al. Fumagillin analog in the
treatment of Kaposi’s sarcoma: a phase I AIDS Clinical Trial Group study. AIDS
Clinical Trial Group No. 215 Team. J Clin Oncol 1998;16:1444-9.
180. Brooks PC, Clark RAF, Cheresh DA. Requirement of vascular integrin vv3 for
angiogenesis. Science 1994;264:569-71.
181. Brooks PC, Silletti S, von Schalscha TL, et al. Disruption of angiogenesis by PEX,
a noncatalytic metalloproteinase fragment with integrin binding activity. Cell
1998;92:391-400.182. Friedlander M, Theesfeld C, Sugita M, et al. Involvement of integrins avb3 and
avb5 in ocular neovascular disease. Proc Natl Acad Sci USA 1996;93:9764-9.
183. Gutheil J, Campbell T, Pierce J, et al. Phase I study of vitaxin, an antiangiogenic
humanized monoclonal antibody to vascular integrin v3. Proc Am Soc Clin
Oncol 1998;17:215a.
184. Cheresh D, Spiro R. Biosynthetic and functional properties of an Arg-Gly-Asp
50 Curr Probl Cancer, January/February 2002

8/3/2019 SledgeJr 2002 Current Problems in Cancer
http://slidepdf.com/reader/full/sledgejr-2002-current-problems-in-cancer 46/54
directed receptor involved in human melanoma cell attachment to vitronectin.
J Biol Chem 1987;262:17703-11.
185. Thorpe PE, Burrows FJ. Antibody-directed targeting of the vasculature of solid
tumors. Breast Cancer Res Treat 1995;36:237-51.
186. Burrows FJ, Derbyshire EJ, Tazzari PL, et al. Up-regulation of endoglin on
vascular endothelial cells in human solid tumors: implications for diagnosis and
therapy. Clin Cancer Res 1995;1:1623-34.
187. Seon B, Matsuno F, Haruto Y, et al. Long-lasting complete inhibition of human
solid tumors in SCID mice by targeting endothelial cells of tumor vasculature with
antihuman endoglin immunotoxin. Clin Cancer Res 1997;3:1031-44.
188. Matsuno F, Haruto Y, Kondo M, et al. Induction of lasting complete regression of
preformed distinct solid tumors by targeting the tumor vasculature using two new
anti-endoglin monoclonal antibodies. Clin Cancer Res 1999;5:371-82.189. Griscelli F, Li H, Bennaceur-Griscelli A, et al. Angiostatin gene transfer: inhibition
of tumor growth in vivo by blockage of endothelial cell proliferation associated
with a mitosis arrest. Proc Natl Acad Sci USA 1998;95:6367-72.
190. Moser TL, Stack MS, Asplin I, et al. Angiostatin binds ATP synthase on the surface
of human endothelial cells. Proc Natl Acad Sci USA 1999;96:2811-6.
191. DeMoraes E, Fogler W, Grant D, et al. Recombinant human angiostatin: a phase I
clinical trial assessing safety, pharmacokinetics and pharmacodynamics. Proc Am
Soc Clin Oncol 2001;20:3a.
192. Mauceri HJ, Hanna NN, Beckett MA, et al. Combined effects of angiostatin andionizing radiation in antitumour therapy. Nature 1998;394:287-91.
193. Gorski DH, Mauceri HJ, Salloum RM, et al. Potentiation of the antitumor effect of
ionizing radiation by brief concomitant exposures to angiostatin. Cancer Res
1998;58:5686-9.
194. O’Reilly M, Boehm T, Shing Y, et al. Endostatin: an endogenous inhibitor of
angiogenesis and tumor growth. Cell 1997;88:277-85.
195. Hohenester E, Sasaki T, Olsen BR, et al. Crystal structure of the angiogenesis
inhibitor endostatin at 1.5 A resolution. EMBO J 1998;17:1656-64.
196. Eder J, Clark J, Supko J, et al. A phase I pharmacokinetic and pharmacodynamic
trial of recombinant endostatin. Proc Am Soc Clin Oncol 2001;20:70a.
197. Thomas J, Schiller J, Lee F, et al. A phase I pharmacokinetic and pharmacodynamic
study of recombinant human endostatin. Proc Am Soc Clin Oncol 2001;20:70a.
198. Herbst R, Tran H, Mullani N, et al. Phase I clinical trial of recombinant human
endostatin in patients with solid tumors: pharmacokinetic, safety and ef ficacy
analysis using surrogate endpoints of tissue and radiologic response. Proc Am Sco
Clin Oncol 2001;20:3a.
199. Fogler W, Song M, Supko J, et al. Recombinant human endostatin demonstrates
consistent and predictable pharmacokinetics following intravenous bolus adminis-
tration to cancer patients. Proc Am Soc Clin Oncol 2001;20:69a.200. Mundhenke C, Thomas J, Neider R, et al. Endothelial cell kinetics in skin wounds
and tumors of patients receiving endostatin. Proc Am Soc Clin Oncol 2001;20:70a.
201. Fotsis T, Zhang Y, Pepper MS, et al. The endogenous oestrogen metabolite
2-methoxyoestradiol inhibits angiogenesis and suppresses tumour growth. Nature
1994;368:237-9.
202. Klauber N, Parangi S, Flynn E, et al. Inhibition of angiogenesis and breast cancer
Curr Probl Cancer, January/February 2002 51

8/3/2019 SledgeJr 2002 Current Problems in Cancer
http://slidepdf.com/reader/full/sledgejr-2002-current-problems-in-cancer 47/54
in mice by the microtubule inhibitors 2-methxyestradiol and taxol. Cancer Res
1997;57:81-6.
203. Schumacher G, Kataoka M, Roth J. 2-methoxyestradiol induces apoptosis in human
pancreatic cancer cell lines and inhibits tumorgenicity in vivo [abstract]. Proc Am
Assoc Cancer Res 1998;39:602.
204. Schumacher G, Kataoka M, Roth J, et al. Potent antitumor activity of 2-me-
thoxyestradiol in human pancreatic cancer cell lines. Clin Cancer Res 1999;5:
493-9.
205. Yue T, Wang X, Louden C, et al. 2-methoxyestradiol, an endogenous estrogen
metabolite, induces apoptosis in endothelial cells and inhibits angiogenesis:
possible role for stress-activated protein kinase signaling pathway and Fas
expression. Molec Pharmacol 1997;51:951-62.
206. Reiser F, Way D, Bernas M, et al. Inhibition of normal and experimentalangiotumor endothelial cell proliferation and cell cycle progression by 2-me-
thoxyestradiol. Proc Soc Exp Biol Med 1998;1998:211-6.
207. Seegers J, Lottering M, Grobler C, et al. The mammalian metabolite, 2-me-
thoxyestradiol, affects p53 levels and apoptosis induction in transformed cells but
not in normal cells. J Steroid Biochem Mol Biol 1997;62:253-67.
208. Attalla H, Makela TP, Adlercreutz H, et al. 2-Methoxyestradiol arrests cells in
mitosis without depolymerizing tubulin. Biochem Biophys Res Commun 1996;228:
467-73.
209. Huang S, DeGuzman A, Bucana CD, et al. Nuclear factor-kappaB activity
correlates with growth, angiogenesis, and metastasis of human melanoma cells innude mice. Clin Cancer Res 2000;6:2573-81.
210. Miller K, Haney L, Pribluda V, et al. A phase I safety, pharmacokinetic, and
pharmacodynamic study of 2-methoxyestradiol in patients with refractory meta-
static breast cancer [abstract]. Proc Am Soc Clin Oncol 2001;20:43a.
211. Korn EL, Arbuck SG, Pluda JM, et al. Clinical trial designs for cytostatic agents:
are new approaches needed? J Clin Oncol 2001;19:265-72.
212. Hahnfeldt P, Panigrahy D, Folkman J, et al. Tumor development under angiogenic
signaling: a dynamical theory of tumor growth, treatment response, and postvas-
cular dormancy. Cancer Res 1999;59:4770-5.213. Kerbel RS. A cancer therapy resistant to resistance. Nature 1997;390:335-6.
214. Boehm T, Folkman J, Browder T, et al. Antiangiogenic therapy of experimental
cancer does not induce acquired drug resistance. Nature 1997;390:404-7.
215. Klement G, Baruchel S, Rak J, et al. Continuous low-dose therapy with vinblastine
and VEGF receptor-2 antibody induces sustained tumor regression without overt
toxicity. J Clin Invest 2000;105:R15-24.
216. Teicher B, Sotomayor E, Huang Z. Antiangiogenic agents potentiate cytotoxic
cancer therapies against primary and metastatic disease. Cancer Res 1992;52:6702-
704.
217. Teicher BA, Holden SA, Jui-Tsai C, et al. Minocycline as a modulator of chemotherapy and hyperthermia in vitro and in vivo. Cancer Lett 1994;82:17-25.
218. Zachary I. Signaling mechanisms mediating vascular protective actions of vascular
endothelial growth factor. Am J Physiol Cell Physiol 2001;280:C1375-86.
219. Sokor S. Neuropilin in the midst of cell migration and retraction. Int J Biochem Cell
Biol 2001;33:433-7.
220. Sokor S, Takashima H, Miao G, et al. Neuropilin-1 is expressed by endothelial and
52 Curr Probl Cancer, January/February 2002

8/3/2019 SledgeJr 2002 Current Problems in Cancer
http://slidepdf.com/reader/full/sledgejr-2002-current-problems-in-cancer 48/54
tumor cells as an isoform-specific receptor for vascular endothelial growth factor.
Cell 1998;92:735-45.
221. Brem H, Gresser I, Grosfeld J, et al. The combination of antiangiogenic agents to
inhibit primary tumor growth and metastasis. J Ped Surg 1993;28:1253-7.
222. Scappaticci F, Smith R, Pathak A, et al. Combination angiostatin and endostatin
gene transfer induces synergistic antiangiogenic activity in vitro and antitumor
ef ficacy in leukemia and solid tumors in mice. Mol Ther 2001;3:186-96.
223. O-charoenrat P, Rhys-Evans P, Modjtahedi H, et al. Vascular endothelial growth
factor family members are differentially regulated by c-erbB signaling in head and
neck squamous carcinoma cells. Clin Exp Metastasis 2000;18:155-61.
224. Rak J, Yu J, Klement O, et al. Oncogenes and angiogenesis: signaling three-
dimensional tumor growth. J Invest Dermatol 2000;5:24-33.
225. Yen L, You X, Al Moustafa A, et al. Heregulin selectively upregulates vascularendothelial growth factor secretion in cancer cells and stimulates angiogenesis.
Oncogene 2000;19:3460-9.
226. Koukourakis M, Giatromanolaki A, O’Byrne K, et al. Bcl-2 and c-erbB-2 proteins
are involved in the regulation of VEGF and of thymidine phosphorylase angiogenic
activity in non-small-cell lung cancer. Clin Exp Metastasis 1999;17:545-54.
227. Maity A, Pore N, Lee J, et al. Epidermal growth factor receptor transcriptionally
up-regulates vascular endothelial growth factor expression in human glioblastoma
cells via a pathway involving phosphatidylinositol 3'-kinase and distinct from that
induced by hypoxia. Cancer Res 2000;60:5879-86.
228. Bruns C, Solorzano C, Harbison M, et al. Blockade of the epidermal growth factorreceptor signaling by a novel tyrosine kinase inhibitor leads to apoptosis of
endothelial cells and therapy of human pancreatic carcinoma. Cancer Res 2000;
60:2926-35.
229. Perrotte P, Matsumoto T, Inoue K, et al. Anti-epidermal growth factor receptor
antibody C225 inhibits angiogenesis in human transitional cell carcinoma growing
orthotopically in nude mice. Clin Cancer Res 1999;5:257-65.
230. Goldman C, Kim J, Wong W, et al. Epidermal growth factor stimulates vascular
endothelial growth factor production by human malignant glioma cells: a model of
glioblastoma multiforme pathophysiology. Mol Biol Cell 1993;4:121-33.231. Clarke K, Smith K, Gullick W, et al. Mutant epidermal growth factor receptor
enhances induction of vascular endothelial growth factor by hypoxia and insulin-
like growth factor-1 via a PI3 kinase dependent pathway. Br J Cancer 2001;84:
1322-9.
232. Ciardiello F, Bianco R, Damiano V, et al. Antiangiogenic and antitumor activity of
anti-epidermal growth factor receptor C225 monoclonal antibody in combination
with vascular endothelial growth factor antisense oligonucleotide in human GEO
colon cancer cells. Clin Cancer Res 2000;6:3739-47.
233. Viloria-Petit A, Crombet T, Jothy S, et al. Acquired resistance to the antitumor
effect of epidermal growth factor receptor-blocking antibodies in vivo: a role foraltered tumor angiogenesis. Cancer Res 2001;61:5090-101.
234. Dvorak HF, Detmar M, Claffey KP, et al. Vascular permeability factor/vascular
endothelial growth factor: an important mediator of angiogenesis in malignancy
and inflammation. Int Arch Allergy Immunol 1995;107:233-5.
235. Ferrara N, Davis-Smyth T. The biology of vascular endothelial growth factor.
Endocrinol Rev 1997;18:1-22.
Curr Probl Cancer, January/February 2002 53

8/3/2019 SledgeJr 2002 Current Problems in Cancer
http://slidepdf.com/reader/full/sledgejr-2002-current-problems-in-cancer 49/54
236. Blancher C, Moore J, Talks K, et al. Relationship of hypoxia-inducible factor
(HIF)-1alpha and HIF-2alpha expression to vascular endothelial growth factor
induction and hypoxia survival in human breast cancer cell lines. Cancer Res
2000;60:7106-13.
237. Relf M, LeJeune S, Scott P, et al. Expression of the angiogenic factors vascular
endothelial cell growth factor, acidic and basic fibroblast growth factor, tumor
growth factor -1, platelet-derived endothelial cell growth factor, placenta growth
factor, and pleiotrophin in human primary breast cancer and its relation to
angiogenesis. Cancer Res 1997;57:963-9.
238. Dirix LY, Vermeulen PB, Pawinski A, et al. Elevated levels of the angiogenic
cytokines basic fibroblast growth factor and vascular endothelial growth factor in
sera of cancer patients. Br J Cancer 1997;76:238-43.
239. Salven P, Maenpaa H, Orpana A, et al. Serum vascular endothelial growth factor isoften elevated in disseminated cancer. Clin Cancer Res 1997;3:647-51.
240. Yamamoto Y, Toi M, Kondo S, et al. Concentrations of vascular endothelial growth
factor in the sera of normal controls and cancer patients. Clin Cancer Res
1996;2:821-6.
241. Verheul H, Hoekman K, Luykx-de Bakker S, et al. Platelet: Transporter of vascular
endothelial growth factor. Clin Cancer Res 1997;3:2187-90.
242. Wynendaele W, Derua R, Hoylaerts M, et al. Vascular endothelial growth factor
measured in platelet poor plasma allows optimal separation between cancer patients
and volunteers: a key to study an angiogenic marker in vivo? Ann Oncol
1999;10:965-71.243. Adams J, Carder P, Downey S, et al. Vascular endothelial growth factor (VEGF) in
breast cancer: comparison of plasma, serum, and tissue VEGF and microvessel
density and effects of tamoxifen. Cancer Res 2000;60:2898-905.
244. Braybrooke JP, O’Byrne KJ, Propper DJ, et al. A phase II study of razoxane, an
antiangiogenic topoisomerase II inhibitor, in renal cell cancer with assessment of
potential surrogate markers of angiogenesis. Clin Cancer Res 2000;6:4697-704.
245. Eisen T, Boshoff C, Mak I, et al. Continuous low dose Thalidomide: a phase II
study in advanced melanoma, renal cell, ovarian and breast cancer. Br J Cancer
2000;82:812-7.246. Honkanen EO, Teppo AM, Gronhagen-Riska C. Decreased urinary excretion of
vascular endothelial growth factor in idiopathic membranous glomerulonephritis.
Kidney Int 2000;57:2343-9.
247. Kitamoto Y, Matsuo K, Tomita K. Different response of urinary excretion of VEGF
in patients with chronic and acute renal failure. Kidney Int 2001;59:385-6.
248. Zon R, Neuberg D, Wood W, et al. Correlation of plasma VEGF with clinical
outcome in patients with metastatic breast cancer [abstract]. Proc Am Soc Clin
Oncol 1998;17:185.
249. Byrne G, Blann A, Venizelos J, et al. Serum soluble VCAM: a surrogate marker of
angiogenesis [abstract]. Breast Cancer Treat Res 1998;50:330.250. Zelinski D, Zantek N, Stewart J, et al. EphA2 overexpression causes tumorigenesis
of mammary epithelial cells. Cancer Res 2001;61:2301-6.
251. Rice GE, Bevilacqua MP. An inducible endothelial cell surface glycoprotein
mediates melanoma adhesion. Science 1989;246:1303-6.
252. Zetter BR. Adhesion molecules in tumor metastasis. Semin Cancer Biol 1993;4:
219-29.
54 Curr Probl Cancer, January/February 2002

8/3/2019 SledgeJr 2002 Current Problems in Cancer
http://slidepdf.com/reader/full/sledgejr-2002-current-problems-in-cancer 50/54
253. Kim II, Moon SO, Kim SH, et al. VEGF stimulates expression of ICAM-1,
VCAM-1 and E-selectin through nuclear factor-kappaB activation in endothelial
cells. J Biol Chem 2001;276:7614-20.
254. Fukushi J, Ono M, Morikawa W, et al. The activity of soluble VCAM-1 in
angiogenesis stimulated by IL-4 and IL-13. J Immunol 2000;165:2818-23.
255. Osborn L, Hession C, Tizard R, et al. Direct expression cloning of vascular cell
adhesion molecule 1, a cytokine-induced endothelial protein that binds to lympho-
cytes. Cell 1989;59:1203-11.
256. Ali S, Kaur J, Patel KD. Intercellular cell adhesion molecule-l, vascular cell
adhesion molecule- 1, and regulated on activation normal T cell expressed and
secreted are expressed by human breast carcinoma cells and support eosinophil
adhesion and activation. Am J Pathol 2000;157:313-21.
257. Gnant MF, Turner EM, Alexander HR. Effects of hyperthermia and turnoutnecrosis factor on inflammatory cytokine secretion and procoagulant activity in
endothelial cells. Cytokine 2000;12:339-47.
258. Koch AE, Halloran MM, Haskell CJ, et al. Angiogenesis mediated by soluble forms
of E-selectin and vascular cell adhesion molecule-1. Nature 1995;376:517-9.
259. Scola MP, Imagawa T, Boivin GP, et al. Expression of angiogenic factors in
juvenile rheumatoid arthritis: correlation with revascularization of human syno-
vium engrafted into SCID mice. Arthritis Rheum 2001;44:794-801.
260. Nor JE, Peters MC, Christensen JB, et al. Engineering and characterization of
functional human microvessels in immunodeficient mice. Lab Invest 2001;81:453-63.
261. Kolopp-Sarda MN, Guillemin F, Chary-Valckenaere I, et al. Longitudinal study of
rheumatoid arthritis patients discloses sustained elevated serum levels of soluble
CD106 (V-CAM). Clin Exp Rheumatol 2001;19:165-70.
262. Kuehn R, Lelkes PI, Bloechle C, et al. Angiogenesis, angiogenic growth factors,
and cell adhesion molecules are upregulated in chronic pancreatic diseases:
angiogenesis in chronic pancreatitis and in pancreatic cancer. Pancreas 1999;18:
96-103.
263. Dosquet C, Coudert MC, Lepage E, et al. Are angiogenic factors, cytokines, and
soluble adhesion molecules prognostic factors in patients with renal cell carci-
noma? Clin Cancer Res 1997;3:2451-8.
264. Lynch DF Jr, Hassen W, Clements MA, et al. Serum levels of endothelial and
neural cell adhesion molecules in prostate cancer. Prostate 1997;32:214-20.
265. Banks RE, Gearing AJ, Hemingway IK, et al. Circulating intercellular adhesion
molecule-1 (ICAM-1), E-selectin and vascular cell adhesion molecule-1
(VCAM-1) in human malignancies. Br J Cancer 1993;68:122-4.
266. Regidor PA, Callies R, Regidor M, et al. Expression of the cell adhesion molecules
ICAM-1 and VCAM-1 in the cytosol of breast cancer tissue, benign breast tissue
and corresponding sera. Eur J Gynaecol Oncol 1998;19:377-83.267. Bodey B, Bodey B Jr, Siegel SE, et al. Over-expression of endoglin (CD105): a
marker of breast carcinoma- induced neo-vascularization. Anticancer Res 1998;18:
3621-8.
268. Li D, Sorensen L, Brook B, et al. Defective angiogenesis in mice lacking endoglin.
Science 1999;284:1534-7.
269. Kumar S, Ghellal A, Li C, et al. Breast carcinoma: vascular density determined
Curr Probl Cancer, January/February 2002 55

8/3/2019 SledgeJr 2002 Current Problems in Cancer
http://slidepdf.com/reader/full/sledgejr-2002-current-problems-in-cancer 51/54
using CD105 antibody correlates with tumor prognosis. Cancer Res 1999;59:856-
61.
270. Li C, Guo B, Wilson PB, et al. Plasma levels of soluble CD105 correlate with
metastasis in patients with breast cancer. Int J Cancer 2000;89:122-6.
271. Takahashi N, Kawanishi-Tabata R, Haba A, et al. Association of serum endoglin
with metastasis in patients with colorectal, breast, and other solid tumors, and
suppressive effect of chemotherapy on the serum endoglin. Clin Cancer Res
2001;7:524-32.
272. Matrisian LM. Metalloproteinases and their inhibitors in matrix remodeling. Trends
Genet 1990;6:121-5.
273. Kossakowska AE, Huchcroft SA, Urbanski SJ, et al. Comparative analysis of the
expression patterns of metalloproteinases and their inhibitors in breast neoplasia,
sporadic colorectal neoplasia, pulmonary carcinomas and malignant non-Hodgkin’slymphomas in humans. Br J Cancer 1996;73:1401-8.
274. Monteagudo C, Merino MJ, San-Juan J, et al. Immunohistochemical distribution of
type IV collagenase in normal, benign, and malignant breast tissue. Am J Pathol
1990;136:585-92.
275. Nguyen M. Angiogenic factors as tumor markers. Invest New Drugs 1997;15:29-
37.
276. Folkman J. Tumour angiogenesis: diagnostic and therapeutic implications. Am
Assoc Cancer Res 1993;34:571-2.
277. Sliutz G, Tempfer C, Obermair A, et al. Serum evaluation of basic FGF in breast
cancer patients. Anticancer Res 1995;15:2675-7.278. Pichon M, Moulin G, Pallud C, et al. Serum bFGF (basic fibroblast growth factor)
and CA 15.3 in the monitoring of breast cancer patients. Anticancer Res
2000;20:1189-94.
279. Nishimura R, Nagao K, Miyayama H, et al. An analysis of serum interleukin-6
levels to predict benefots of medroxyprogesterone acetate in advanced or recurrent
breast cancer. Oncology 2000;59:166-73.
280. Poon RT, Fan ST, Wong J. Clinical implications of circulating angiogenic factors
in cancer patients. J Clin Oncol 2001;19:1207-25.
281. Peters-Engl C, Frank W, Medl M. Tumor flow in malignant breast tumors measuredby doppler ultrasound: an independent predictor of survival [abstract]. Breast
Cancer Treat Res 1998;50:228.
282. Peters-Engl C, Medl M, Mirau M, et al. Color-coded and spectral Doppler flow in
breast carcinomas—relationship with the tumor microvasculature. Breast Cancer
Res Treat 1998;47:83-9.
283. Kedar RP, Cosgrove DO, Smith IE, et al. Breast carcinoma: measurement of tumor
response to primary medical therapy with color Doppler flow imaging. Radiology
1994;190:825-30.
284. Ferrara KW, Merritt CR, Burns PN, et al. Evaluation of tumor angiogenesis with
US: imaging, Doppler, and contrast agents. Acad Radiol 2000;7:824-39.285. Foltz RM, McLendon RE, Friedman HS, et al. A pial window model for the
intracranial study of human glioma microvascular function. Neurosurgery 1995;
36:976-84 discussion 984-5.
286. Chaudhari MH, Forsberg F, Voodarla A, et al. Breast tumor vascularity identified
by contrast enhanced ultrasound and pathology: initial results. Ultrasonics 2000;
38:105-9.
56 Curr Probl Cancer, January/February 2002

8/3/2019 SledgeJr 2002 Current Problems in Cancer
http://slidepdf.com/reader/full/sledgejr-2002-current-problems-in-cancer 52/54
287. Jansson T, Westlin JE, Ahlstrom H, et al. Positron emission tomography studies in
patients with locally advanced and/or metastatic breast cancer: a method for early
therapy evaluation? J Clin Oncol 1995;13:1470-7.
288. Bassa P, Kim EE, Inoue T, et al. Evaluation of preoperative chemotherapy using
PET with fluorine-18- fluorodeoxyglucose in breast cancer. J Nucl Med 1996;37:
931-8.
289. Wahl RL, Zasadny K, Helvie M, et al. Metabolic monitoring of breast cancer
chemohormonotherapy using positron emission tomography: initial evaluation.
J Clin Oncol 1993;11:2101-11.
290. Arslan N, Ozturk E, Ilgan S, et al. 99Tcm-MIBI scintimammography in the
evaluation of breast lesions and axillary involvement: a comparison with mam-
mography and histopathological diagnosis. Nucl Med Commun 1999;20:317-25.
291. Mankoff D, Dunnwald L, Gralow J, et al. Monitoring the response of patients withlocally advanced breast carcinoma to neoadjuvant chemotherapy using {technetium
99m}-sestamibi scintimammography. Cancer 1999;85:2410-23.
292. Yoon JH, Bom HS, Song HC, et al. Double-phase Tc-99m sestamibi scintimam-
mography to assess angiogenesis and P-glycoprotein expression in patients with
untreated breast cancer. Clin Nucl Med 1999;24:314-8.
293. Wilson CB, Lammertsma AA, McKenzie CG, et al. Measurements of blood flow
and exchanging water space in breast tumors using positron emission tomography:
a rapid and noninvasive dynamic method. Cancer Res 1992;52:1592-7.
294. Martin G, Caldwell J, Graham M, et al. Noninvasive detection of hypoxic
myocardium using fluorine-18-fluoromisonidazole and positron emission tomogra-phy. J Nucl Med 1992;33:2202-8.
295. Ogawa T, Uemura K, Shishido F, et al. Changes of cerebral blood flow and oxygen
and glucose metabolism following radiochemotherapy of gliomas: a PET study.
J Comput Assist Tomog 1988;12:290-7.
296. Blankenberg FG, Eckelman WC, Strauss HW, et al. Role of radionuclide imaging
in trials of antiangiogenic therapy. Acad Radiol 2000;7:851-67.
297. Stejskal E. Use of spin echos in a pulsed magnetic-field gradient to study
anisotropic, restricted diffusion and flow. J Chem Phys 1965;43:3597-3603.
298. Yamada I, Aung W, Himeno Y, et al. Diffusion coef ficients in abdominal organsand hepatic lesions: evaluation with intravoxel incoherent motion echo-planar MR
imaging. Radiology 1999;210:617-23.
299. Van Ziji P, Eleff S, Ulatowski J, et al. Quantitative assessment of blood flow, blood
volume and blood oxygenation effects in functional magnetic resonance imaging.
Nat Med 1998;4:159-67.
300. Abramovitch R, Frenkiel D, Neeman M. Analysis of subcutaneous angiogenesis by
gradient echo magnetic resonance imaging. Magn Reson Med 1998;39:813-24.
301. Esserman L, Hylton N, George T, et al. Contrast-enhanced magnetic resonance
imaging to assess tumor histopathology and angiogenesis in breast carcinoma.
Breast J 1999;5:13-21.302. Furman-Haran E, Grobgeld D, Margalit R, et al. Response of MCF7 human breast
cancer to tamoxifen: evaluation by the three-time-point, contrast-enhanced mag-
netic resonance imaging method. Clin Cancer Res 1998;4:2299-304.
303. Pham C, Roberts T, van Bruggen N, et al. Magnetic resonance imaging detects
suppression of tumor vascular permeability after administration of antibody to
vascular endothelial growth factor. Cancer Invest 1998;16:225-30.
Curr Probl Cancer, January/February 2002 57

8/3/2019 SledgeJr 2002 Current Problems in Cancer
http://slidepdf.com/reader/full/sledgejr-2002-current-problems-in-cancer 53/54
304. Weidner N, Folkman J, Pozza F, et al. Tumor angiogenesis: a new significant and
independent prognostic indicator in early-stage breast carcinoma. J Natl Cancer Inst
1992;84:1875-7.
305. Hall N, Fish D, Hunt N, et al. Is the relationship between angiogenesis and
metastasis in breast cancer real? Surg Oncol 1992;1:223-9.
306. Obermair A, Kurz C, Czerwenka K, et al. Microvessel density and vessel invasion
in lymph-node-negative breast cancer: effect on recurrence-free survival. Int J
Cancer 1995;62:126-31.
307. Fox S, Leek R, Weekes M, et al. Quantitation and prognostic value of breast cancer
angiogenesis: comparison of microvessel density, Chalkley count, and computer
image analysis. J Pathol 1995;177:275-83.
308. Toi M, Inada K, Suzuki H, et al. Tumor angiogenesis in breast cancer: its
importance as a prognostic indicator and the association with vascular endothelialgrowth factor expression. Breast Cancer Res Treat 1995;36:193-204.
309. Ogawa Y, Chung Y, Nakata B, et al. Microvessel quantitation in invasive breast
cancer by staining for factor VIII-related antigen. Br J Cancer 1995;71:1297-301.
310. Morphopoulos G, Pearson M, Ryder W, et al. Tumour angiogenesis as a prognostic
marker in infiltrating lobular carcinoma of the breast. J Pathol 1996;180:44-9.
311. Gasparini G, Toi M, Verderio P, et al. Prognostic significance of p53, angiogenesis,
and other conventional features in operable breast cancer: subanalysis in node-
positive and node-negative patients. Int J Oncol 1998;12:1117-25.
312. Tynninen O, von Boguslawski K, Aronen H, et al. Prognostic value of vascular density
and cell proliferation in breast cancer patients. Pathol Res Pract 1999;195:31-7.313. Vincent-Salomon A, Carton M, Zafrani B, et al. Long term outcome of small size
invasive breast carcinomas independent from angiogenesis in a series of 685 cases.
Cancer 2001;92:249-56.
314. Bosari S, Lee A, DeLellis R, et al. Microvessel quantitation and prognosis in
invasive breast carcinoma. Hum Pathol 1992;23:755-61.
315. Van Hoef M, Knox W, Dhesi S, et al. Assessment of tumor vascularity as a
prognostic factor in lymph node negative invasive breast cancer. Eur J Cancer
1993;29A:1141-5.
316. Fox S, Leek R, Smith K, et al. Tumor angiogenesis in node-negative breastcarcinomas—relationship with epidermal growth factor receptor, estrogen receptor,
and survival. Breast Cancer Res Treat 1994;29:109-16.
317. Gasparini G, Weidner N, Bevilacqua P, et al. Tumor microvessel density, p53
expression, tumor size, and peritumoral lymphatic vessel invasion are relevant
prognostic markers in node-negative breast carcinoma. J Clin Oncol 1994;12:454-66.
318. Bevilacqua P, Barbareschi M, Verderio P, et al. Prognostic value of intratumoral
microvessel density, a measure of tumor angiogenesis, in node-negative breast
carcinoma—results of a multiparametric study. Breast Cancer Res Treat 1995;36:
205-17.
319. Inada K, Toi M, Hoshina S, et al. Significance of tumor angiogenesis as anindependent prognostic factor in axillary node-negative breast cancer. Gan To
Kagaku Ryoho 1995;22(Suppl 1):59-65.
320. Costello P, McCann A, Carney D, et al. Prognostic significance of microvessel
density in lymph node negative breast carcinoma. Human Pathol 1995;26:1181-4.
321. Karaiossifidi H, Kouri E, Arvaniti H, et al. Tumor angiogenesis in node-negative breast
cancer: relationship with relapse free survival. Anticancer Res 1996;16:4001-2.
58 Curr Probl Cancer, January/February 2002

8/3/2019 SledgeJr 2002 Current Problems in Cancer
http://slidepdf.com/reader/full/sledgejr-2002-current-problems-in-cancer 54/54
322. Heimann R, Ferguson D, Powers C, et al. Angiogenesis as a predictor of long-term
survival for patients with node-negative breast cancer. J Natl Cancer Inst 1996;88:
1764-9.
323. Ozer E, Canda T, Kurtodlu B. The role of angiogenesis, laminin and CD44expression in metastatic behavior of early-stage low-grade invasive breast carci-
nomas. Cancer Lett 1997;121:119-23.
324. Medri L, Nanni O, Volpi A, et al. Tumor microvessel density and prognosis in
node-negative breast cancer. Int J Cancer 2000;89:74-80.
325. Toi M, Hoshina S, Takayanagi TT. Association of vascular endothelial growth
factor expression with tumor angiogenesis and with early relapse in primary breast
cancer. Jpn J Cancer Res 1994;85:1045-9.
326. Toi M, Inada K, Hoshina S, et al. Vascular endothelial growth factor and
platelet-derived endothelial cell growth factor are frequently coexpressed in highlyvascularized human breast cancer. Clin Cancer Res 1995;1:961-4.
327. Obermair A, Kucera E, Mayerhofer K, et al. Vascular endothelial growth factor
(VEGF) in human breast cancer: correlation with disease-free survival. Int J Cancer
1997;74:455-8.
328. Gasparini G, Toi M, Miceli R, et al. Clinical relevance of vascular endothelial
growth factor and thymidine phosphorylase in patients with node-positive breast
cancer treated with either adjuvant chemotherapy or hormone therapy. Cancer J Sci
Am 1999;5:101-11.
329. Gown A, Rivkin S, Hunt H, et al. Prognostic factor of vascular endothelial growth
factor (VEGF) expression in node-positive breast cancer. Proc Am Soc Clin Oncol2001;20:427a [abstract 1703].
330. Gasparini G, Toi M, Gion M, et al. Prognostic significance of vascular endothelial
growth factor protein in node-negative breast carcinoma. J Natl Cancer Inst
1997;89:139-47.
331. Buadu L, Murakami J, Murayama S, et al. Breast lesions: correlation of contrast
medium enhancement patterns on MR images with histopathologic findings and
tumor angiogenesis. Radiology 1996;200:639-49.
332. Stomper P, Winston J, Klippenstein D, et al. Angiogenesis and dynamic MR
imaging gadolinium enhancement of malignant and benign breast lesions. Breast
Cancer Res Treat 1997;45:39-46.
333. Buckley D, Drew P, Mussurakis S, et al. Microvessel density of invasive breast
cancer assessed by dynamic Gd-DTPA enhanced MRI. J Magn Reson Imaging
1997;7:461-4.
334. Hulka C, Edmister W, Smith B, et al. Dynamic echo-planar imaging of the breast:
experience in diagnosing breast carcinoma and correlation with tumor angiogene-
sis. Radiology 1997;205:837-42.
335. Ikeda O, Yamashita Y, Takahashi M. Gd-enhanced dynamic magnetic resonance
imaging of breast masses. Top Magn Reson Imaging 1999;10:143-51.
336. Knopp M, Weiss E, Sinn H, et al. Pathophysiologic basis of contrast ehancementi b t t J M R I i 1999 10 260 6