SLE and cardiovascular manifestations
40
http:// cardiologysearch.blogspot.i n/ http://cardiologysearch.blogspot.in/ http:// cardiologysearch.blogspot.in/
-
Upload
sujit-sahu -
Category
Health & Medicine
-
view
1.055 -
download
1
description
for more cardiology ppts visit regularly
Transcript of SLE and cardiovascular manifestations

http://cardiologysearch.blogspot.in/
http://cardiologysearch.blogspot.in/
http://cardiologysearch.blogspot.in/

Cardiac disease is common among patients with systemic lupus erythematosus (SLE) as
pericardial, myocardial, valvular and coronary artery involvement
http://cardiologysearch.blogspot.in/

http://cardiologysearch.blogspot.in/

http://cardiologysearch.blogspot.in/

http://cardiologysearch.blogspot.in/

Pericardial involvement is the Pericardial effusion
pericarditis
second most common echocardiographic lesion in SLE, and
most frequent cause of symptomatic cardiac disease.
http://cardiologysearch.blogspot.in/

Conduction defects,
Represent a sequel of active or past pericarditis and/or myocarditis
noted in 34 to 70 % of patients with SLE.
First-degree heart block may be seen and is often transient
http://cardiologysearch.blogspot.in/

Congenital heart block may be part of the neonatal lupus syndrome.
The resting heart rate may correlate with disease activity.
Study 14 of 15 patients with a resting heart rate above 90 beats/min had active disease
http://cardiologysearch.blogspot.in/

Mitral valve involvement is most common;
Mild to moderate regurgitant murmur may be heard but most patients remain asymptomatic
Mitral valve prolapse in 25 percent of cases.
Verrucous endocarditis — Libman-Sacks (verrucous) endocarditis
http://cardiologysearch.blogspot.in/

MYOCARDITIS
uncommon,
asymptomatic manifestation of SLE
prevalence of 8 to 25 % in different studies
http://cardiologysearch.blogspot.in/

Acute myocarditis
infiltration of the myocardium with mononuclear cells.
Resolution of the inflammation leads to fibrosis that may be manifested clinically as dilated cardiomyopathy.
http://cardiologysearch.blogspot.in/

1. Coronary artery involvement is the most recent cardiovascular manifestation to be recognized in SLE
2. seen in 2 – 16 % of patients with SLE 3. can lead to acute myocardial
infarction in young women.
In some cases, thrombi rather than coronary disease is responsible for the ischemia .
Coronary artery vasculitis is rare.
http://cardiologysearch.blogspot.in/

Other coronary artery manifestations -
Coronary arteritis,
Aneurysms,
Vasospasm
Embolic phenomenonhttp://cardiologysearch.blogspot.in/

Presentation
Angina,
Myocardial infarction,
Sudden death
Responsible for 0.3 % deaths.
http://cardiologysearch.blogspot.in/

http://cardiologysearch.blogspot.in/

Pathogenesis
http://cardiologysearch.blogspot.in/

RiskFactors
http://cardiologysearch.blogspot.in/

Most striking feature of CAD in SLE is the predilection for young premenopausal
women.
Manzi and colleagues lupus women aged 35 to 44 years were
over 50 times more likely to have an MI as compared to controls.
http://cardiologysearch.blogspot.in/

modifiable risk factor for occlusive vascular disease in both general and lupus populations.
Elevated homocysteine levels have been reported in 15% of lupus patients
Associated with cardiovascular events subclinical atherosclerosis
http://cardiologysearch.blogspot.in/

http://cardiologysearch.blogspot.in/

43 yr old female
A known case of SLE
ANA positive
On steroids
http://cardiologysearch.blogspot.in/

OBESITY
SYSTEMIC HYPERTENSION
ANEMIA
Acid peptic disease
Hypothyroidism
Nephropathy
Hemorrhoids
http://cardiologysearch.blogspot.in/

Old IWMI
CAG-2003 Mild CAD Mild LAD and RCA disease
http://cardiologysearch.blogspot.in/

Acute coronary syndrome
AWMI – delayed presentation
Not Thrombolised
Patient managed and stabilized
Taken for CAGhttp://cardiologysearch.blogspot.in/

Right dominant system
Two vessel disease
Significant proximal LAD disease
Critical mid RCA disease
Major diagonal diseasehttp://cardiologysearch.blogspot.in/

Hypokinetic IVS, apical segments. Anterolateral segments
Mild LV dysfunction
EF -65 %
Grade I – diastolic dysfunction
http://cardiologysearch.blogspot.in/

Advised
CABG SURGERY with grafts to Distal LAD Major diagonal Distal RCAORPCI to LAD and RCA- IF considered
high risk for CABGhttp://cardiologysearch.blogspot.in/

Discussed with CT surgeons and anesthetists
Due to Presence of high risk profile Symptomatic status – class III symptoms Nephropathy – high creatinine values, cr -
2.7 mg%
Patient taken for PCIhttp://cardiologysearch.blogspot.in/

Drug eluting stent placed in
LAD -SUPRALIMUS CORE STENT RCA - ENDEAVOR STENT
Patient was started on antiplatelets
http://cardiologysearch.blogspot.in/

http://cardiologysearch.blogspot.in/

http://cardiologysearch.blogspot.in/

Patient developed GI –bleeding
Coffee ground vomitting
Profound hypotension
Patient became unconscious
http://cardiologysearch.blogspot.in/

Blood transfusion
Fluid replacement
Inotrops – dopamine. Adrenaline infusion
started
Patient ABG - desaturationhttp://cardiologysearch.blogspot.in/

Patient connected to mechanical ventilator
Antiplatelets stopped- inspite of DES
Continuous Pantoprazole infusion started
http://cardiologysearch.blogspot.in/

Active bleeding stopped - after 3 days
Hemodynamic stability attained
CLOPIDOGREL antiplatelet- started after 3 days
Aspirin also restarted by 5 dayshttp://cardiologysearch.blogspot.in/

Patient improved in 5 days
Shifted to ward and discharged
http://cardiologysearch.blogspot.in/

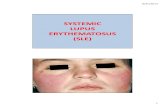
Blood disorder NSAIDS – used for different symptoms in
SLE▪ Increase bleeding
Corticosteroids – produce peptic ulcer
Thrombocytopenia – increase bleeding▪ Autoimmune ▪ Drug induced
Antiphospholipid antibody – increase thrombosis▪ Increase chance of stent thrombosishttp://cardiologysearch.blogspot.in/

Bleeding Bleeding Stent
thrombosis
Anti platelets
http://cardiologysearch.blogspot.in/

http://cardiologysearch.blogspot.in/

Kindly send your suggestions to improve this site
Visit us regularly for updates
Send your articles/ ppt/pdf to publish in this site .
http://cardiologysearch.blogspot.in/