Situation Assessment of Blood Centres Bangladesh · Centres in Bangladesh ... The designations...
92
Situation Assessment of Public and Private Blood Centres in Bangladesh
Transcript of Situation Assessment of Blood Centres Bangladesh · Centres in Bangladesh ... The designations...

Situation Assessment of Public and Private Blood Centres in Bangladesh

1
Situation Assessment of Public and Private Blood Centres in Bangladesh
Directorate General of Health Services, Ministry of Health and Family Welfare, Bangladesh. In collaboration with the World Health Organization and the OPEC Fund for International Development (OFID). This report is the product of a ongoing collaboration between the World Health Organization (WHO) and the OPEC Foundation for International Development (OFID); and the Ministry of Health and Family Welfare, Bangladesh.
World Health Organization 2012 This health information product is intended for a restricted audience only. The designations employed and the presentation of the material in this health information product do not imply the expression of any opinion whatsoever on the part of the World Health Organization concerning the legal status of any country, territory, city or area or of its authorities, or concerning the delimitation of its frontiers or boundaries. Dotted lines on maps represent approximate border lines for which there may not yet be full agreement. The mention of specific companies or of certain manufacturers’ products does not imply that they are endorsed or recommended by the World Health Organization in preference to others of a similar nature that are not mentioned. Errors and omissions excepted, the names of proprietary products are distinguished by initial capital letters. The World Health Organization does not warrant that the information contained in this health information product is complete and correct and shall not be liable for any damages incurred as a result of its use.

2

i
Table of Contents
Executive Summary ii
1. Background 1
2. Assessment 5
3. Method of Assessment 6
4. Questionnaire Development 6
5. Field Testing 7
6. Sample Determination 7
7. Data Collection 8
8. Supervision 8
9. Data Analysis 8
10. Results 9
11. Discussion 43
a) Organization and management of blood transfusion services in Bangladesh 43
b) National blood donation and collection practices 43
c) National practices in screening of donated blood 44
d) Blood component preparation 44
e) Inventory of blood and blood products and status of the blood cold chain 44
f) Pre‐transfusion practices in hospitals 44
g) Transfusion monitoring and post‐transfusion practices in hospitals 45
12. Conclusion 45
13. Recommendation 47
14. Proposed Action Plan 49
15. Limitations 51
16. Acknowledgements 51
ANNEX I: Assessment Questionnaires 52
Section A: Organization and Management 54
Section B: Blood Donors & Blood Collection 60
Section C: Screening for Transfusion Transmissible Infections (TTI) 63
Section D: Blood Group Serology and Compatibility Testing 64
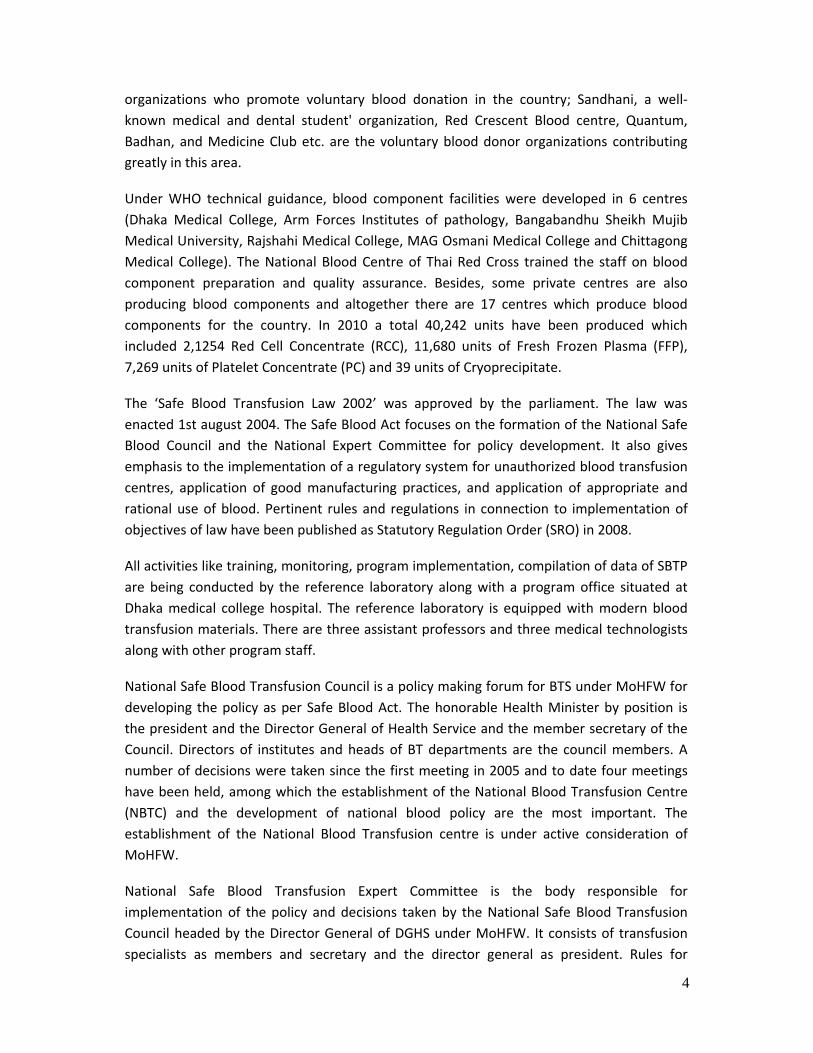
Section E: Blood Component Preparation 65
Section F: Blood Storage, Transportation, Inventory & Distribution 67
ANNEX‐2: List of blood transfusion centres and hospitals surveyed 75
List of Data Collectors 75
Types of Surveyed Blood Centres 75
List of Blood Centres at District Hospitals 76
ANNEX‐3: Status of Selected Indicators 79
ANNEX‐4: Table of Selected Health and Socio‐economic Indicators 81

ii
Executive Summary Blood Transfusion Service is considered as a major part of the public sector healthcare
setting. The service requires quality for safe blood collection and its use for the patients.
This report presents the results of situation assessment of blood centres in public and
private sectors in Bangladesh. The assessment was carried out in 2011 by experts of blood
transfusion and program management personnel of Directorate General of Health Service
under the Ministry of Health in collaboration with the World Health Organization (WHO)
and the OPEC Fund for International Development (OFID). The objective of the assessment
was to review the situation of the existing blood transfusion services that has been
established in public and private sectors in Bangladesh, identify gaps and develop a set of
recommendations. There are 253 centres in the country and the mainstay of the assessment
was a large site survey covering 109 selected blood centres of these 253 centres, from seven
administrative divisions of the country. These include public medical colleges, public
institutes, district hospitals, Upazila health complexes, standalone private blood centres,
private medical colleges, private hospitals and non‐governmental blood centres.
The methodology applied in the assessment was a combination of a desk review of policy
documents and looking into the status of organizational management, quality system,
training, blood donor recruitment, blood collection, screening for Transfusion Transmissible
Infections (TTI), serology and compatibility procedures, blood component preparation,
blood storage system, transportation, inventory and distribution. Assessment of the status
of transfusion process in the hospital, pre‐transfusion procedure, clinical use of blood and
management of the service at central level have been also carried out simultaneously. The
blood transfusion services in Bangladesh are managed and regulated by the Ministry of
Health under the guidelines of Safe Blood Transfusion ACT, a legal framework for blood
safety. The National Safe Blood Transfusion Council has the role of an advisory body and the
National Expert Committee is an implementing body for provision of the services. Setting up
any private blood centres requires licensing from the Directorate General of Health Service,
Ministry of Health.
The Safe Blood Transfusion Program (SBTP), a unit of the Ministry of health supports 203
centres by providing equipment, regular supply of kits, reagents, blood bags and training.
66.8% (169) of blood transfusion centres belonging to the public sector are integrated
within the hospitals and located in seven divisions in the country. 5.6% (14) of centres are
operated by the Ministry of Defense and 7.91% (20) of centres are supported by the
national program but privately operated. In the private sector, 19.76% (50) of blood centres
are integrated into the medical college and the specialized hospitals, and also include
standalone blood centres. Each of these centres collects, stores and tests the blood. The
blood transfusion services are coordinated nationally by the Safe Blood Transfusion Program
and give services through the 203 blood centres. There was significant shortage of trained
staff in each centre and almost all blood centres surveyed reported to have a shortage of

iii
adequate premises, supplies and equipment. Except for two NGO blood centres, all centres
reported to have collected blood from patient’s relatives and friends, showing that 85% of
blood is collected from relatives/family blood donors and only 15% of blood is donated by
voluntary non‐remunerated blood donors. No paid donors were registered during the
assessment. No donors were recruited below the age limit of 18; 80% of donors belonged
with the age range of 18‐ 24 and 20% with the age range of 25‐44. No donation has been
recorded between the ages 44‐60.
In public and private centres, donor assessments were done according to defined donor
selection criteria and 95% of the centres have shown hemoglobin test to be performed by
the hemoglobin scale method. Follow up of sero‐reactive donors were not observed for
blood donor management. SOPs for different processes essential for blood transfusion i.e.
for blood screening, ABO & RhD, blood storage, blood component preparation and waste
management were non‐existent in majority of the centres. Only in two centres, one private
hospital and one private medical college, SOPs were these available and reported as
implemented. The system of standard and comprehensive documentation was found only in
two public medical college blood centres. In the private sector, documentation was
available only in two private medical colleges and in two private hospitals. No centre
maintained records of the whole range of procedures carried out. Basic data for patients’
blood grouping were maintained in almost all surveyed centres but were not found in a
uniform format. Similarly the donor blood grouping registers were available but not
complete in district, Upazila or in medical colleges hospitals of both the public and private
sectors. Laboratory documents for patient’ and donor blood grouping and cross matching
were found incomplete in the district and Upazila health complexes. These reflect scanty
information that could have been generated for the assessment and moreover, most of the
vital statistics were missing due to shortage of manpower, according to responders.
The data shows that public centres received most of the training organized by the Safe
Blood Transfusion Program as a national training. Out of all district hospitals only 38%
responded that they have adequate staff. Out of 14 public medical colleges only 36% and in
Upazila 73% have responded that there is adequate staff. Others, in the public sector
responded that the staff crisis is considered as one of the major challenges to running the
centres smoothly. Screening of all donated blood for markers of five TTI (HIV, HBV, HCV,
syphilis and malaria) is mandatory in Bangladesh and 100% donations are screened in all
centres except for 20% of district hospitals, 55% of Upazila health complexes, 23% of private
medical colleges, 29% of private hospitals and17% of standalone blood centres which do not
routinely perform malaria testing. In 98% of the centres, blood screening is carried out using
rapid tests. All centres reported to perform blood screening for HIV, HBV, HCV and syphilis.
This shows that the prevalence of TTI markers is below 1%. Post‐donation screening was
reported in as much as 70% of the surveyed centres, and rest of the centres only did pre‐
donation screening of donors with no screening of donated blood after the blood donation.

iv
There were no protocol nor algorithm developed and followed for reactive results in either
of the centres under assessment. Initial reactive samples were reported as re‐tested by the
same kits; no confirmatory facilities have been seen in any of the visited centres. Only 21%
of public medical colleges, 50% of private medical colleges and 80% of public institutes
reported to run internal quality control during routine testing of TTI.
With regards to External Quality Assessment (EQAS), three public medical colleges and one
NGO blood centre reported participation in such a program organized by the Public Health
Institute of Thailand. There were records of blood donation deferrals for TTI markers but no
other data were available. A blood donor data base was available in NGO blood centres. In
public centres there was provision of bulk procurement of kits under the Safe Blood
Transfusion Program as well as facilities for validation of kits before their use in centres. All
centres reported to have experienced critical supply of blood bags and run out of kits for the
12 last months on several occasions. All private sector and 10% of public sector purchased
kits and reagents locally and no validation of these kits was done. 2% of district hospitals,
43% of public medical colleges, 20% of public institutes, 50% of private medical colleges,
57% of private hospital centres and 100% of NGO blood centres reported to produce blood
components equal to 10% of total blood collection. 55% of components were produced by
the public sector and 45% by the private sector respectively. On average, district hospitals
received 93% of blood collected by the centres themselves, 3% from NGO blood centres and
5% from standalone blood centres. In medical colleges, 85% of the blood is collected by the
by centres based in the medical colleges and rest 10% is received from NGO blood centres
and 5% from standalone blood centres. Patient relatives were reported responsible for
transportation of the blood to the patients.
There is wide variation of use of blood grouping techniques using both forward and reverse
method. 100% of blood centres in district hospitals, public medical colleges and public
institutes used slide method for ABO blood grouping and 18% of district hospitals, 8% of
Upazila health complexes, 21% of public medical colleges, 80% of public institutes, 83% of
private medical colleges, 71% of private hospitals, and 17% of standalone blood centres
reported to carry out reverse grouping along with forward grouping. RhD typing is
performed using slide method and cross matching at room temperature. Only one NGO
blood centre reported to have performed cross matching by indirect antiglobulin method.
Compatibility testing was reported to be carried out and completed by using donor cells and
patients serum in 100% of cases. Significantly no centre reported to perform antibody
screening for patient’s blood samples. Hospital transfusion committees have been
developed in all district hospitals, public medical colleges and public institutes following Safe
Blood ACT. SOPs for blood transfusion process have been developed for completing blood
request forms, drawing and leveling, blood administration but not for transfusion
monitoring and management of transfusion reactions.

v
The country has a post‐graduate degree started in 1972 as diploma (DBS & T) and currently
BSMMU University is providing MD, MTM, DBST and FCPS. Due to extreme shortage of
manpower in the licensing authority and Safe Blood Transfusion Program, regular
supervision and monitoring of the centres were not adequate for 253 blood centres
throughout the country. The assessment shows that a great deal of activities have been
undertaken for improving blood transfusion services in Bangladesh by providing blood
screening facilities, by regulating the private sector, by reducing paid donations, introducing
blood component preparation and containment of TTI markers below 1%. However some
areas need more focus for improvement. The main reasons for the lack of SOPs
development and implementation and inadequate voluntary blood collections are: lack of
comprehensive planning; failures in the delivery system and absence of adequate
manpower. The blood transfusion services in Bangladesh thus need more attention from the
top level to prioritize for restructuring and development of a comprehensive strategy
following the Safe Blood Act. This includes:
National standards for blood transfusion services to be developed for uniform
practices. Training should be comprehensive for both the public and private sectors
and more emphasis should be given to the importance of SOPs, Quality assurance,
importance of documentation for monitoring and evaluation, stock management, TTI
algorithms, following standard practices for serology, compatibility testing and pre
and post donation counseling.
Facilities of medical colleges’ centres in the public sector need to be strengthened
for confirmatory testing for TTI markers. A medical college should be designated as
regional blood centre to conduct training, data compilation for the division, support
confirmatory testing, conduct motivational and blood collection programs with NGO
and set up a haemovigilance system.
There should be provision for adequate and appropriate manpower and equipment
in each centre and adequate refrigerators should be provided for segregation of
blood units.
The quality of TTI testing and serology should be assessed under EQAS with the
Reference Laboratory (RL) or WHO recommended collaborating centres.
There is urgent need for development of strategic planning for voluntary blood
donation under National Expert Committees. Efforts should be made to develop a
policy for joint collaboration of BT department of medical colleges and non‐
government blood donor organizations for need‐based blood collection and
motivational programs.
The Safe BT Council together with National experts should make efforts for the
development of National Blood Screening Algorithms.
Local hospital authorities should be oriented about blood safety and encouraged to
allocate adequate space for BT centres especially in district hospitals. Hospital Blood

vi
Transfusion Committees should be oriented and given responsibility to set and
define transfusion indications, transfusion alternatives, bedside practices and
evaluation of transfusion outcomes including transfusion reactions (haemovigilance).
Regional medical college BT departments should be strengthened with adequate
manpower and budget allocations made to initiate supervision and monitoring of BT
centres in both sectors.
National expert committee members and experts of higher institutes should visit the
different BT centres under the monitoring program to support SBTP in the
establishment of quality services throughout the country.
The Reference Laboratory (RL) should function as a national confirmation and
reference centre to provide independent responses on repeat reactive TTI donor
samples. It should have appropriate and validated confirmation testing facilities in
place such as Western Blot technology, Nucleic Acid Amplification Technology (NAT)
and PCR as well as competent staff with adequate training to perform the tests. The
RL should also monitor training activities in regional centres and compile the TTI data
as reported from regional centres.
The reference laboratory should update the national data and report to national
authorities. The centre should also have advanced training on quality assurance and
EQAS, and perform research. It should have a mechanism of networking with the
regional centres.

1
1. Background A major step in implementing such an integrated blood safety strategy is the need for an
effective assessment. It should focus firstly on obtaining information on policy and national
operations (organizational and managerial) within facilities. Secondly, information should be
collected about managerial and technical parameters regarding blood and blood products in
individual facilities along with total “vein‐to‐vein" transfusion. An effective assessment will
enable responsible ministries to have a comprehensive view of all aspects of the national
blood program and to identify gaps relevant to the implementation of the recommended
integrated strategy on blood safety. Key findings and additional information gathered will
help to advocate and develop strategies to strengthen the national blood program. The
implementation of and progress towards set targets can be monitored by periodic repeat
assessments using the same tools.
Bangladesh is a densely populated small country of approximately 156 million people. The
country is one of the largest deltas of the world with a total area of 147,570 sq. km (56,977
square miles). Being a low‐lying country it stretches between 20º34' and 26º38' north and
longitudinally between 88º01' and 92º41' east. It is mostly surrounded by Indian Territory
(West Bengal, Tripura, Assam and Meghalaya), except for a small strip in the southeast by
Myanmar. Bay of Bengal lies on the south.
From the administrative point of view, Bangladesh is divided into seven administrative
divisions (Dhaka, Chittagong, Rajshahi, Khulna, Barisal, Sylhet and Rangpur), 64 districts, six
city corporations, 308 municipalities, 482 Upazila and 4498 unions. At national level, the
Ministry of Health & Family Welfare (MoHFW) is responsible for policy, planning and
decision making at macro level. Under MoHFW, there are four Directorates, viz., Directorate
General of Health Services, Directorate General of Family Planning, Directorate of Nursing
Services and Directorate of Drug Administration. The rural population constitutes the
majority (65.4%) of the population; but the urban population is increasing and is currently
34.6%. The number of people living per square kilometer is 939. Male to female ratio is
105:100. The two major religions practiced in Bangladesh are Islam (88.3%) and Hinduism
(11%). Other religious groups include Buddhists and Christians. Gross National Product per
capita income is US$ 1550 (2009). Dhaka is the capital city of the country. The health care
service has been extended up to Upazila level. Distribution of public health care services
and facilities follow similar patterns of administrative tiers, viz. national (mostly capital‐
based in Dhaka), regional (in divisions), district, Upazila, union and ward.
Primary health care (PHC), including family planning services in the urban area (city
corporations and municipalities), is provided by the Ministry of Local Government; and in
the rest of the country by the Ministry of Health and Family Welfare (MoHFW). Provision of
secondary and tertiary cares, in both urban divisional directorates with necessary staff and
rural areas, is the sole responsibility of MoHFW. The primary level hospital care begins with
the 418 Upazila health complexes (153 are 50‐beds and the rest are 31‐beds) with a range

2
of 31 to 50 beds. The 62 district hospitals (59 Sadar district hospitals and two general
hospitals) are the secondary level hospitals which provide health care in several specialties
with a range of 50 to 375 beds. The tertiary level hospitals are multidisciplinary medical
colleges and institutes hospitals with a range of 250 to 1700 beds. At national level there
are post‐graduate, specialized hospitals with ranges of 100 to 600 beds. There are four
types of static health facilities at union level. These are Rural Health Centres (RHC, 10‐bed
hospitals), Union Sub‐Centres (USC), Union Health and Family Welfare Centres (UHFWC)
and Community Clinics (CC). There are 18 governmental medical colleges and 41 private
medical colleges.
The Government of Bangladesh is implementing the program throughout the healthcare
services provided to the people from grass root to central level. The program is entitled
Health, Nutrition and Population Sector Program (HNPSP), launched 1998 and extended to
June 2010. It was further extended from 2011 to 2016 as Health Population and Nutrition
Sector Development Program (HPNSDP). The HPNSDP covers 38 Operational Plans (OP)
implemented by 38 Line Directors and 14 Projects/Programs; Safe Blood Transfusion
Program is one of them. The Implementing Agency of the program is the Ministry of Health
and Family Welfare (MoHFW) with its attached departments.
Blood Transfusion Service (BTS) of Bangladesh was established in 1950 at the Dhaka medical
college hospital. A few blood transfusion centres opened later in the then 18 districts.
During that period BT activities were mostly limited to only basic grouping and cross
matching. More than 70% of annual demands for blood were collected from paid donors till
2001. No blood was screened as mandatory be it in public or private sector. Due to the
immense threat of HIV, the government was convinced and committed to ensuring that all
patients had access to enough appropriate safe blood and blood products (free from HIV,
viral hepatitis and other Transfusion Transmissible Infections (TTI)) whenever needed by
hospitals. Under the National AIDS Committee (NAC) on HIV/AIDS, the Blood Transfusion
subcommittee (BTSC) was formed to plan Safe Blood Transfusion throughout the country.
The committee prepared a three‐year plan. The Ministry of Health and Family Welfare
approved the plan and started implementation of National Safe Blood Transfusion Program
with the support of UNDP in 1999.
The main objectives of the program were: 1) Establishment of a Reference Laboratory and
of blood screening facilities in 99 blood transfusion centres with the provision of reagent
kits and equipment for the detection of HIV, hepatitis‐B, hepatitis‐C, syphilis and malaria. 2)
Training of doctors and technologists and 3) Enhancement of voluntary blood donation
through motivation programs and IEC campaigns. A training module was prepared.
However, in 2004 UNDP support was taken over by World Bank and DFID, involving WHO to
provide the technical assistance for development of component facilities and the
implementation of quality standards under HAPP (HIV/AIDS Prevention Project). In addition,
technical assistance of WHO was reinforced by WHO collaborating centre of National Blood

3
Centre of Thailand. WHO provided support at the National Blood Centre for procurement of
equipment and reagents and facilitating overseas training, continuous on‐site technical
support through the international centre of excellence WHO Collaborating Centre (WHO
CC).
The Blood transfusion service in Bangladesh is under control of the Directorate General of
Health services (DGHS) and is coordinated by the National Safe Blood Transfusion Program.
Each blood transfusion centre is integrated within the hospital at tertiary (medical colleges,
institutes and specialized hospitals) and secondary (district hospitals) levels. However there
are blood transfusion centres at primary level hospitals called “Upazila health complexes”.
Today there are 203 blood transfusion centres enlisted, supported and coordinated by the
National Safe Blood Transfusion Program.
The private sector (50 centres) is being operated by hospital‐based blood transfusion
centres and also by standalone blood centres regulated by licensing authorities. Each centre
either in the public or private sector reports monthly on blood screening for five TTI and
blood components to the reference laboratory of the Safe Blood Transfusion Program.
However, there are no national or regional BTS in the country. The National Safe Blood
transfusion program has been delegated authority to act as resource mobilization for
procurement of equipment, kits, reagents and blood bags for the enlisted centres and
training of manpower.
Blood screening facilities developed in 99 blood transfusion centres in the year of 2000
include all public medical colleges, district hospitals, combined military hospitals, medical
institutes, Red Crescent blood centres and others as well as two non‐governmental medical
college hospitals. From 2008 to 2010 104 new centres were developed in Upazila health
complexes and in other hospitals. Today, there are officially a total of 203 blood screening
centres. Over a total of 2,440,096 units of blood screened for TTI between 2000 and 2010,
129 HIV, 21,715 HBV, 3,182 HCV, 2,800, syphilis and 1,149 malaria reactive cases were
detected, maintaining TTI prevalence almost below 1%. Most of TTI screening is done on
rapid tests. Only in some centres of the private sector is blood screening is performed by
ELISA.
Approximately 600,000 units of blood are required yearly in Bangladesh. This estimate is
based on year 2010 throughout the country as reported by public and private blood
transfusion centres. There are mainly two types of blood donors in Bangladesh which are
relative/replacement blood donors and voluntary blood donors. The report of SBTP (2010)
shows that 70% of blood is collected from directed or relative blood donors the rest being
from voluntary blood donors. The blood donation system in Bangladesh is not a centralized
system as all blood transfusion centres, mostly hospital based, collect, process and
distribute blood. There is no nationally designated organization for recruitment of voluntary
blood donors either in the public or private sectors. However there are a few philanthropic
4
organizations who promote voluntary blood donation in the country; Sandhani, a well‐
known medical and dental student' organization, Red Crescent Blood centre, Quantum,
Badhan, and Medicine Club etc. are the voluntary blood donor organizations contributing
greatly in this area.
Under WHO technical guidance, blood component facilities were developed in 6 centres
(Dhaka Medical College, Arm Forces Institutes of pathology, Bangabandhu Sheikh Mujib
Medical University, Rajshahi Medical College, MAG Osmani Medical College and Chittagong
Medical College). The National Blood Centre of Thai Red Cross trained the staff on blood
component preparation and quality assurance. Besides, some private centres are also
producing blood components and altogether there are 17 centres which produce blood
components for the country. In 2010 a total 40,242 units have been produced which
included 2,1254 Red Cell Concentrate (RCC), 11,680 units of Fresh Frozen Plasma (FFP),
7,269 units of Platelet Concentrate (PC) and 39 units of Cryoprecipitate.
The ‘Safe Blood Transfusion Law 2002’ was approved by the parliament. The law was
enacted 1st august 2004. The Safe Blood Act focuses on the formation of the National Safe
Blood Council and the National Expert Committee for policy development. It also gives
emphasis to the implementation of a regulatory system for unauthorized blood transfusion
centres, application of good manufacturing practices, and application of appropriate and
rational use of blood. Pertinent rules and regulations in connection to implementation of
objectives of law have been published as Statutory Regulation Order (SRO) in 2008.
All activities like training, monitoring, program implementation, compilation of data of SBTP
are being conducted by the reference laboratory along with a program office situated at
Dhaka medical college hospital. The reference laboratory is equipped with modern blood
transfusion materials. There are three assistant professors and three medical technologists
along with other program staff.
National Safe Blood Transfusion Council is a policy making forum for BTS under MoHFW for
developing the policy as per Safe Blood Act. The honorable Health Minister by position is
the president and the Director General of Health Service and the member secretary of the
Council. Directors of institutes and heads of BT departments are the council members. A
number of decisions were taken since the first meeting in 2005 and to date four meetings
have been held, among which the establishment of the National Blood Transfusion Centre
(NBTC) and the development of national blood policy are the most important. The
establishment of the National Blood Transfusion centre is under active consideration of
MoHFW.
National Safe Blood Transfusion Expert Committee is the body responsible for
implementation of the policy and decisions taken by the National Safe Blood Transfusion
Council headed by the Director General of DGHS under MoHFW. It consists of transfusion
specialists as members and secretary and the director general as president. Rules for

5
management of public and private blood centres have been developed in 2008 as SRO 145.
As per rule public blood centres may collect revenue through imposing charges for blood
screening, cross matching and other routine investigations. 50% of the collected funds are
kept for purchasing kits and reagents in case of interrupted supply of consumables from the
central procurement unit. This system has empowered each blood centre to perform
routine activities without interruption. Remuneration of staff working in public blood
transfusion centres may be taken from the charges collected as per SRO by this mechanism.
However all blood centres are authorized to collect fees of 250/‐ BDT for blood screening in
general hospital and charge for 350/‐ for others. As mentioned, 50% of the money collected
is diverted to hospitals to be used by blood banks and 50% are distributed as incentives to
the blood transfusion centre staff.
A Draft National Policy prepared and approved by the National Safe Blood Transfusion
Council is yet to be approved by the cabinet. The major areas cover all the areas of Safe
Blood Transfusion Act. This includes strategies for development of the National Blood
Program with establishment of the National Blood Transfusion Centre, plan of actions for
the improvement of the whole BTS, strategies for staff educational and training programs,
strategies for blood screening and donor management and policy for the role of NGOs in
voluntary non‐remunerated donor recruitment programs. It also focuses on the needs for
implementing and enforcing appropriate regulations necessary to ensure high quality BTS in
the private and public sectors. Emphasis is also placed in the draft policy on the
development of standard operating procedures (SOPs) and guidelines for appropriate use of
blood, introduction of advanced technology, and development of a uniform management
information system for the blood program in all blood transfusion centres.
The main goal of the assessment was to develop a National Action Plan for establishment of
quality standards for BTS. The scopes of the assessment were to collect data of activities of
the existing blood transfusion service in the public and private sectors, physical inspections
of the BTSs, in‐depth data review and extraction, cross checking of the data with registers,
discussions with key responders and medical technologists of the blood transfusion centres.
The assessment also included a review of the manpower challenges, logistics and
equipment, clinical transfusion practices, activities and coordination of voluntary blood
donor organization; the existing local constraints and management perspective towards the
National Policy and ACT and rules for Safe Blood Transfusion; to reiterate the
implementation of standards and SOPs as well as management issues for quality BTS,
orientation of the different aspects of variables and importance of indicators identifying
existing key capacities and additional capacities needed to reach such objectives.
2. Assessment
A national consultative meeting was held on 1 to 2 November 2010 in Dhaka, in
collaboration with WHO and OFID, the Ministry of Health, and all other stakeholders in the

6
blood safety program in the country. Thirty‐five participants from the ministry of health,
Safe Blood Transfusion Program, blood transfusion experts of hospital based BTSs,
representatives of Red Crescent blood centres and non‐governmental blood centres, WHO
officials from country office and blood safety experts from WHO‐HQ, Geneva, attended the
meeting. During the brief inaugural session, the national authorities and the stakeholders
were introduced to the scope and objectives of the WHO/OFID joint project on ‘Prevention
of Transfusion Transmitted HIV/AIDS and hepatitis’ in four developing countries namely
Bangladesh, Nepal, Bhutan and Pakistan. The meeting concluded with excellent outcomes in
identification of local and national barriers in the country.
The priority activities, role and responsibility of stakeholders also discussed the
implementation of the proposed blood safety project of WHO/OFID/ Ministry of Health
(MoH), Bangladesh. It was prioritized that an assessment should be carried out for existing
BTSs in Bangladesh for review and updating of national standards, introduction of
algorithms for TTI testing, implementation of Standard Operating Procedures (SOPs),
protocol for haemovigilance, waste management, training needs for laboratory staff on TTI
testing and quality management. It was recommended that assessment of BTS in the public
and private sectors would enable an in‐depth look to identify gaps to make action plan on
blood safety by exploring the constraints that preclude establishing quality of blood
screening, to identify the needs for strengthening the laboratory and training, to enable
responsible stakeholders to have a comprehensive view of all aspects of the national blood
program for developing strategic action plans.
3. Method of Assessment
The assessment process used is consistent with the process and steps presented in the WHO
frameworks for situation assessment used in most countries for BTS. Accordingly the WHO
questionnaire has been modified by the expert group of transfusion medicine and the
management personnel involved in the national BTS of Bangladesh, considering the country
context. The process of development of a questionnaire has been reviewed and revised by
the WHO National expertise for its suitability and fitting for the purpose of data collection.
The assessment begun with the existing assets (structures, management, practices and
critical facilities) pertinent to identify weaknesses and strengths for decision makers to
elaborate the relevant action plan
Step 1: Identify challenges for a quality blood screening and characteristics.
Step 2: Prepare a profile for each important area.
Step 3: The findings were evaluated to identify the gaps.
Step 4: Preparing a scenario for policy makers to develop action plans for each area.
4. Questionnaire Development
The consultative meeting was held 17‐19 January 2011 for development of the
questionnaire. The stakeholders were given an introduction of WHO BTS framework of

7
situation assessment tools. Later the resource persons reviewed the draft questionnaire.
The group remarked that some questions might not be relevant to the country context of
Bangladesh. The questions were considered important as they would reflect the actual
situation in the country while filling the global database questionnaire every year. The group
finally presented the draft, revised and finalized questionnaires.
5. Field Testing On 25th January 2011, a field test was conducted in the blood transfusion centre of NICVD
(National Institute of cardiovascular Disease) at Dhaka. The group consisted of two experts
from Dhaka medical college hospital and DGHS took part in the field test of the assessment
tool. The team briefed the procedure of field testing and their findings. The field testing was
successful with regards to the preset questions of part one and part two and the responder
Assistant Professor was able to give the expected responses for most of the questions asked.
The team recommended that questions related to yearly statistics/data were not collected
during this short period of interview and recommended that these data should be collected
separately by sending the formats to the centre before the assessors’ visits. This would
reduce the time taken for assessment during the busy hours of the centre and the assessor
would only verify and cross check the prepared data as per format provided beforehand.
The team also recommended some modification and rephrasing of questions for
understanding and clarification.
6. Sample Determination
As per WHO framework for assessment, monitoring and evaluation of the blood transfusion
services (FRAME) the number of blood centres and health facilities to be assessed depends
on the objective of the assessment; it was advised that attempt must be made to cover as
many facilities as possible in doing such an assessment. In general, it is recommended that a
minimum of 30% of hospitals (and other health facilities) that received blood from the blood
centres must be covered when the number of such facilities exceeds 100 and all of such
facilities if the number is less than 100. The sampling methods should be decided and
agreed by the assessment team beforehand.
From the report of safe BT program the total number of centres was 203 including blood
transfusion centres in public medical colleges, institutes, arm forces institutes, specialized
hospitals, district hospitals and Upazila health complexes. It was also reported that there
were 50 licensed blood centres in the private sector. It was decided to have an assessment
of all centres, but due to limitation of resources and time constraints the program manager
decided to visit 59 centres in the first phase and 50 centres in the 2nd phase. Altogether 109
centres were selected for assessment which covered at least 43% of total blood centres out
of 253 centres throughout the country. The centres were selected purposely in the
stratification of public medical colleges, public institutes, private hospitals, district hospitals,
Upazila health complexes, standalone centres, NGO blood centres and others.

8
7. Data Collection The data collectors were selected among medical doctors from DGHS and Safe Blood
Transfusion Program and senior level medical technologists from Safe Blood Transfusion
Program. Six teams were constituted with two members in each. The teams that collected
the data up to district hospital level were blood transfusion experts and administrative
experts from DGHS. However the team that collected data from Upazila level centres i.e.
primary level hospitals were senior medical technologists having working experience in
monitoring blood centres. The collection of data started in two phases from February to
May 2011 and from July to September 2011. 109 centres were selected which include 14
public medical colleges, six private medical colleges, five institutes of the public sector and
seven specialized hospitals of the private sector, 50 district hospitals, 11 Upazila health
complexes, two NGO blood centres, six standalone blood centres and other eight centres.
The data were collected by the preset questionnaire through face to face interviews and on‐
spot inspections of facilities, modes of management of different sized hospitals, discussions
with the local authorities, laboratory procedures, equipment and facilities, laboratory
records and registers and discussions with blood transfusion staff and clinicians in the
hospitals. The teams also reviewed the relevant documents, Safe Blood Transfusion ACT
2002, Rules (SRO) and Draft National Blood Policy. Discussions were held with the program
manager and line director, while experts of the reference laboratory, reviewed the yearly
reports (January 10 to December10) during data collection. 27 facilities were visited in
Dhaka city and the rest were outside and situated on average 250 kilometres from the
capital city.
8. Supervision The assessment was initiated jointly by WHO and the program manager of BAN BCT. Dr MK
Zaman Biswas, national professional officer (epidemiology), Dr Murad Sultan, technical
officer, blood safety, Dr Aminul Hasan DPM BAN BCT, DGHS and Dr Mazharul Hoque, DPM,
SBTP coordinated data collection, monitored and supervised the assessment process.
9. Data Analysis The submitted data sheets were checked by a WHO technical officer for verification. Some
responses were verified with responders as required. After verification the data sheet were
given to data entry operator and to statisticians. A data field was created as per variable of
interest and data were entered in the SPSS system for analysis. Mr Hafizur Rahaman, Mr
Muhiuddin Ahmed and Mr Golam Kibria Nury in consultation with the technical officer
prepared the database in SPSS. The entries were crossed checked and invalid entries
discarded. The WHO technical officer assisted in cleaning and verifying the data. Total data
of 109 surveyed centres were entered in SPSS. All data were displayed in tables with
frequency distribution and graphical presentations were developed. The technical officer,
the national consultant of blood safety and the national professional officer in epidemiology
and Dr Nazmul jointly analysed the data against the variables and indicators of interest.

9
10. Results
The following are the figures and tables that have been created on the number variables
used in the pre‐set questionnaires for the survey of blood centres. The whole questionnaire
contains three parts. Part‐1 includes organization and management, quality system,
training, equipment & supplies, regulation, health safety, conditions of premises, blood
donors & blood collections, screening of transfusion transmissible infections, blood group
serology and compatibility testing, blood component preparation, blood storage
transportation and inventory distribution. Part two refers to the transfusion process in the
hospital which includes pre‐transfusion procedures, SOPs and records, staff training, clinical
use of blood, and appropriate use of blood. Part three deals with the assessment of policy
and management at the central administrative level and include national policy and
coordination, national standards and guidelines, monitoring and assessment at national
level, training, contingency plan and preparedness for disasters. The data indicate numbers
of blood units, sources of blood by donor types, male/female blood donors, units collected
in fixed and mobile sites, number of new donors, number of TTI markers, number and
percentage of initial reactive samples, number of repeat reactive samples, types of blood
components used, types of patients that received the components. The results are reflected
in frequency distribution. As mentioned, the findings are represented according to the
questionnaires used to obtain the information from 109 locations.
Part‐1 Types of centre f %
District Hospital 50 45
Upazila Health Complex 11 10
Public Medical College 14 13
Private Medical College 6 6
Private Hospital 7 6
Public Institute 5 5
Standalone Blood Centre 6 6
NGO Blood Centre 2 2
Others 8 7
Total 109 100
Table 1: Types of centres surveyed
Out of 109 centres 50 were district hospitals, 11 were Upazila health complexes, 14 public
medical colleges, six private medical colleges, seven private hospitals, five public institutes
in Dhaka city, six standalone private blood centres, two non‐governmental, Bangladesh Red
Crescent blood centre and Quantum Foundation Blood Bank. Other centres included blood
centres in combined military hospitals and paramilitary forces, blood centres in the family
planning and BGB (Border Guard of Bangladesh) hospital.

10
Figure 1Distribution of blood centres
Figure 1 shows that 80% of the centres belong to the public sector (ministry of health and
other ministry) including medical colleges, institutes, district hospitals and Upazila health
complexes, combined military and paramilitary hospitals. 12% of the centres belong to the
private sector. Only 6% of the surveyed centres were standalone blood centres.
Almost 73% of total blood centres belong to Ministry of health and 18% to the private
sector. However a few centres also get support from Safe Blood Transfusion Program.
Figure 2 Organization and management of blood transfusion services

11
Figure 3 Delegation of function
In Bangladesh the BTS is a mixed type system. Public centres are exempted from license
where private centres require license from Directorate General of Health Services (DGHS).
All centres directly report to National Safe Blood Transfusion authorities. With respect to
delegation of authority, none of centres responded to delegate blood transfusion for other
organizations. All centres surveyed are attached to hospitals except the standalone blood
centres (6).
Figure 4 Types of centres supported by International Organizations
Delegation of Functions to other Organizations
0
10
20
30
40
50
60
70
80
90
100
District Hospital
Upazila Health Complex
Public Medical College
Private
Medical
College
Private
Hospital
Public
Institute
Standalone
Blood
Centre
NGO Blood Centre
Others
Yes
NO

12
The assessment revealed that blood centres are operated by their own resources. One
Upazila reported to have received some logistic support from an international organization
like UNICEF. However, Red Crescent blood centres reported to get financial support from
several international organizations.
Figure 5 Blood centres that receive support from National Safe Blood Transfusion Program
It has been mentioned that 99 blood centres were enlisted under the Safe Blood Transfusion
Program in 1999 when the program was first launched. That includes all public medical
colleges, institutes and district hospitals and combined military hospitals and specialized
hospitals like children hospitals. Besides, some private medical colleges like Bangladesh
Medical College Hospital, national medical hospitals, Red Crescent blood centres,
Thalassaemia Foundation Hospital, Holy Family Red Crescent Hospital were also enlisted in
the program. These enlisted centres get regular supply of kits, reagents and blood bags from
Safe Blood Transfusion Program. In addition, the enlisted centres do receive opportunities
for training organized by Safe Blood Transfusion Program. From the assessment it has been
noted that 100 Upazila health complexes received basic blood transfusion equipment and
laboratory furniture but the function is yet to be started in all of them. During assessment
one Upazila blood centre reported to be non‐functional.

13
Figure 6 Sources of funds for operation of blood centres
All public centres received funds from the government. The public centres reported to
collect funds from charge recovery as fees for investigation of blood screening and other
serological tests. Red Crescent reported to receive funds from different donor agencies. The
proportion of funds from different sources were not calculated and recorded as per data
requirement.
Figure 7 Status of quality standards.
The questionnaire for assessing quality standards included whether the centre has a quality
policy, organizational structure, job descriptions and availability of a quality manager. The
data revealed that out of 109 centres only one of the private sector centres could show
quality policy and informed to have received accreditation. Though organization structures
were present in most of the centres surveyed, it appeared that it concerned the centre as a

14
whole and not the blood centre. However, written job descriptions were not observed in
any of the surveyed centres. For the reason mentioned above, only in one centre (APPOLO
Hospital), the survey team could find a quality manager as the centre received JCI (Joint
Commission Accreditation).
Figure 8 Status of SOPs in different types of blood centres
Figure 9 Status of SOPs in different types of blood centres
The team looked for SOPs on seven different essential processes including SOPs for blood screening,
ABO and RhD blood grouping, blood storage, SOPs for blood component preparation and waste
management. Only in two centres‐one private hospital and one private medical college, SOPs were
found and reported implemented.

15
Figure 10 Status of records maintained in different types of centres
Figure 11 Status of records maintained in different types of centres

16
Figure 12 Status of records maintained in different types of centres
Documentation is an important feature of BTS for tracking and other routine purposes. The survey
questionnaire included information on 13 types of documents covering all aspects of BT activities.
Standard and comprehensive systems of documentation were found only in two public medical
college blood centres. In the private sector it was comprehensive only in two private medical
colleges and in two private hospitals. The data collected reveal that record maintenance of
transfusion activities is not well organized and uniform. No centre kept records of the whole range
of documents as required. Data also revealed that basic data for patients’ blood grouping were
maintained in almost all surveyed centres but not in a uniform format. Similarly, the donor blood
grouping registers were available but not complete in district, Upazila or in medical college hospitals
of both the public and private sectors.
Laboratory documents such as cross matching were found in brief and along with patient blood
grouping, donor blood grouping as seen in district and Upazila health complexes. In most of the
district hospitals only three registers were found for the whole documentation of BTS. This reflects a
paucity of information and most of the vital statistics were missing leading to possible improper
monitoring and evaluation. Most of the responders knew the types and formats of documents
required from their training program manuals. Lack of maintenance of documents according to
responders is mostly due to shortage of manpower. All the data were recorded manually by the
medical technologists working in the centres. It has been revealed that none of the centres has a
designated person for data management except in one non‐governmental blood centre. In private
hospitals like Apollo reported to keep data along with centralized laboratory information system
(LIMS) from where data could be retrieved for reporting purposes.

17
T raining
0
1020
30
4050
60
70
8090
100
In‐S ervice Training National Training International Training
DH (50) UHC (11) PMC (14) P rMC (6) P rH (7) P Int (5) S BC (6) NGOBC (2) O (8)
Figure 13 Status of training in transfusion centres
The data show that Public centres received most of the training organized by Safe Blood Transfusion
Program as a national training. Most of the training conducted was basic training to develop
laboratory skills.
Figure 14 Status of staff in blood centres
Out of all district hospitals only 38% responded that they have adequate staff. Out of 14 public
medical colleges only 36% and in Upazila 73% have adequate staff. Others in public sector
responded that the staff crisis is considered one of the major challenges to run the centres. Only in
an NGO run centre adequate staff is present. All remaining centres declared to have shortage of staff.

18
Figure 15 Status of equipment
During the assessment, a list of equipment was shown to each of the centres. None of the centres
responded that they have all the equipment as per list provided.
Figure 16 Mechanism of procurement
With regard to procurement of equipment all public centres indicated that almost all major
equipment is purchased by a central procurement unit upon request from Safe Blood Transfusion
Program whereas in private centres, equipment are purchased locally by the centre itself. Five public
medical colleges purchased equipment locally in addition to central procurement. One private
medical hospital and one NGO blood centre have received some equipment as grants from donor
agencies.

19
Figure 17 Status of training on equipment maintenance
In response to whether the centre provides training to its staff –almost all centres under assessment
responded negatively. In most of the cases the responders mentioned that the vendor provided on
spot training when the equipment were purchased and installed. All centres under assessment
reported to have equipment maintenance program. The system and practice of stock controls were
not developed in either of the centres surveyed. However, it was observed in surveyed centres with
varying degree.
Figure 18 Status of procurement of critical supplies
The questionnaires included specific questions as to whether the centre has developed a system for
procurement of critical items for blood transfusion centres including blood bags, kits and reagents. It
has been reported that blood bags were the critical supplies generally supplied from Central Medical
Store and Deport (CMSD), Institutes of Public Health (IPH) and Safe Blood Transfusion Program (SBTP)
in the public sector – however not adequate enough to meet the demands of the enlisted centres. In
the private sector purchases are made from local market. SBTP generally arranged validation of kits

20
before distribution and use by the centres. There is no validation system for blood bags purchased
from local market. Only the bags produced in IPH were reported to be validated.
Figure 19 Status of out of stock critical supplies in different blood centres (blood bags, test
kits and reagents)
During assessment almost all centres reported to have experienced all types of critical supply run
out. It has been shown that a significant portion of the public centres always suffered from
shortages of blood bags where they have no other option than buy through the end user. Shortage
of kits and blood group reagents happened to be regular; a major part of public centres suffered
shortage with different degrees: 36% of public medical colleges 44% of district hospitals and more
markedly 74% of Upazila health complexes and 4% of the public institutes. The private sector
reported to keep critical supply ready but has experienced shortages however not in significant
proportions. In the public system there is an ad hoc arrangement to buy kits, reagents, and others
from local market through funds collected as “investigation fees”, as reported by the responders.
Figure 20 Status of regulation /licensing

21
As mentioned by law, the private blood centres require licensing prior to run a centre
whereas public centres do not. The data show that all centres under the private sector
obtained licenses. However in response to inspection by licensing authorities, only 50% of
private medical colleges and 43% of private hospitals and 100% of NGO blood centres
reported inspections by the licensing authorities.
Figure 21 Status of health and safety programme
Figure 21 shows that this area is quite neglected in both sectors. No records of program
activities have been shown in the public sector in this regard. Some public blood centres
have received training on health and safety program but no documentation was available
Data revealed that health and safety program started in some private medical colleges and
private hospitals at their own initiative and as an effort to the requirement of accreditation
from different international agencies.
Figure 22 Status of suitable premises in the centres

22
There was significant shortage of spaces in districts hospital and Upazila health complexes
surveyed. In district hospitals blood transfusion activities and routine pathology services
were seen functioning from the same room, without any separation between the sections.
Shortage of space was seen in the standalone blood centres as well as in the private medical
colleges and private hospitals. Significantly two NGO blood centres have all types of rooms
as reported and observed during the assessment.
Figure 23 Status of suitable premises in the centres
Figure 24 Status of access to differ utilities
Access to facilities like internet, telephone was available in both public and private sectors.
Access to power supply varied from centre to centre and most of the public centres have
access to central supply from the hospital where it is located.

23
Figure 25 Status of activities for blood donation
This figure shows 11 types of activities. All centres in both public and private sectors recruit
and collect blood from donors. NGO blood centres reported to undertake almost 100% of
activities for blood donor education and donor counseling as well as education materials for
blood donors and have dedicated units for blood donor programs. This was significantly
absent from the rest of the private and public centres. Only 54% of district hospitals and
9% of Upazila health complexes have regular physicians to look at blood donors. Although
all centres responded that they have trained donor recruitment staff, materials for donor
education and donor pre‐counseling persons were not adequately available.
Figure 26 Status of manpower for blood collection

24
Figure 27 Status of manpower for blood collection
Data shows that 17% of standalone blood centres and 45% of the Upazila health complexes
have the trained personnel for assessing the suitability of blood donors. All other centres
show to have trained personnel as well.
Figure 28 Blood donor selection strategies
The data show that there was a mixed type of recruitment strategies in the different centres.
It has been noted that changes in recruitment strategies were being adopted in public
medical colleges as well as in private centres. The private blood centres and hospitals prefer
to perform pre‐donation screening of donors due to high prevalence of seroreactivity. On
the other hand NGO blood centres during camp collection usually selected the post
donation blood screening. None of the centres have developed a system to follow‐up sero‐

25
reactive blood donors. With regards to pre donation Hb measurement none of the centres
responded to have performed it routinely. All centres followed the national criteria for
blood donors suitability observed available in all centres surveyed. Except for two NGO
blood centres none of the surveyed centres reported to observe World Blood Donor Day.
Figure 29 Method of assessment of blood donor suitability
Figure 29 shows the results of different methods used to assess blood donors’ suitability. All
centres responded to use the blood donor assessment form supplied from SBTP as well as
the form printed by the centres. Only 36% of public medical colleges, 20% of public
institutes, 100% of NGO blood centres reported to hold pre donation counseling and
interviews routinely before blood donation. None of the standalone blood centres under
assessment reported to hold such activities during routine blood donation. 82% of district
hospitals and 55% of Upazila health complexes reported to undertake regular physical
checks of the blood donor before donation, however all other centres reported to carry out
the physical check in 100% of blood donors.
Method for haemog lobin es timation
0
1020
30
4050
60
70
8090
100
P ortable colorimeter Haemoglobin colour s cale Other
DH (50) UHC (11) PMC (14) P rMC (6) P rH (7) P Int (5) S B C (6) NGOBC (2) O (8)
Figure 30 Method for Hb estimation
Figure 30 shows that estimation of Hb was observed only by use of colour scale technique.

26
Figure 31 Cumulative data of blood collection by 109 centres as surveyed
The data show a yearly total of 165816 units of whole blood collected by the centres which
represents 43% of total blood centres in the country. This shows that 15% of blood is
collected from voluntary blood donors and 85% from relatives/family blood donors.
Donationby L oc ation
0
1020
30
4050
60
70
8090
100
S tatic Mobile
DH (50) UHC (11) PMC (14) P rMC (6) P rH (7) P Int (5) S BC (6) NGOBC (2) O (8)
Figure 32 Donations by location
Figure 32 shows that NGO blood centres have the scope to collect blood in equal
proportions from fixed and mobile sites, whereas some district hospitals, public medical
colleges and public institutes reported to have blood collections done through door
Cumulative Data of Blood Collection by 109 Surveyed Centers
0
20000
40000
60000
80000
100000
120000
140000
160000
180000
200000
Total No. of blood donors
No. of voluntary non‐remunerated blood
donors
No. of familyreplacement donors
No. of paid blooddonors
33,406 (20.15%)
132,410 (79.85%)
165,816
0

27
campaign which represents on average 10% of collections from mobile sites. On enquiry
NGO and standalone blood centres have mobile site donations on different national days.
On a turnover basis blood collection was high in public centres in fixed sites though NGO
blood centres have shown to have higher numbers of blood donations in mobile sites.
Outdoor blood collections were not observed in Upazila health complexes surveyed. Even
such an initiative was observed in standalone blood centres as well.
Donation by Age Group
0
80
20
00
10
20
30
40
50
60
70
80
90
100
under 18 years old 18- 24 years old 25-44 years old 46-60 years old
Per
centa
ge
Figure 33 Donation by age groups
The data show there were no paid donors registered during the assessment in any centre.
The male/female ratio of the blood donors was not calculated as the data were not
recorded in the centres according to the standard format. The records from the centres
have shown that no single donor was recruited below the age limit of 18 ; 80% of donors
belonged to age limits between 18 to 24 and 20% of donors belonged to age limits between
25 to 44. No donation was recorded between the age from 44‐60 in the surveyed centres.

28
Number of donor deferrals
0
1020
30
40
5060
70
8090
100
No. deferrals dueto low
haemoglobin
No. of deferralsdue to their
medicalconditions
No. of deferralsdue to high-risk
behaviour
No. of deferralsdue to travel and
other reasons
No. of deferralsdue to other
reasons ( TTI )
Nu
mb
er
of
Do
no
rs1,657 (100% )
Figure 34 Number of blood donor deferrals
During donor assessment, deferrals were noted in the centres. However in all centres there
were records of blood donation deferrals due to sero‐reactive TTI markers, with no other
reasons recorded for deferrals. The figure shows that 100% of donations were deferred due
to presence of TTI markers.
B lood donation , reac tion rec ord
0102030405060708090
100
One s tandard volume of
donation routinely
collec ted
Autologous (pre‐
depos itory) blood
donation
Only s terile , s ingle
us e plas tic blood
collec tion bags
R ecords of advers e
blood donor reac tions
S ys tem of obtaining
donor's feedback and
complains
DH (50) UHC (11) PMC (14) P rMC (6) P rH (7) P Int (5) S BC (6) NGOBC (2) O (8)
Figure 35 Blood donation, donor reactions and others
Figure 36 shows that all centres under assessment reported to collect 450ml of blood from
the donors routinely and to use blood bags. None of the centres reported to have started
autologous blood transfusion and there were no reports available in either of the centres
for adverse donor reactions, however they responded to have observed vaso‐vagal
reactions during blood donation. No system has been found adapted to record and
entertain blood donors for feedback/ complaints either in public or private centres.

29
B lood Donor Data B as e
0
10
20
30
40
50
60
70
80
90
100
B lood donor databas e Budget line item for the donor programme
DH (50) UHC (11) PMC (14) P rMC (6) P rH (7) P Int (5) S BC (6) NGOBC (2) O (8)
Figure 36 Status of blood donor data base
This figure shows the presence of blood donor data bases. The data show that only in two
NGO blood centres donor databases were manual and included all donor profiles, status of
blood screening and time for next call for blood donation. Moreover, the mentioned NGO
blood centres had the specific budget to develop other sections which was absent in the
other centres. The data revealed that none of the surveyed centres has shown records for
new blood donors each year. NGO blood centres however reported to have the data but not
calculated as per specific format required for the assessment.
Figure 37 Blood collection by apheresis
Out of 109 centres surveyed only one public institute has record of blood collection for
platelet components collected by apheresis. The remaining centres do not have components
collection by apheresis.
Collection of Blood through Apheresis Procedure
0 10 20 30 40 50 60 70 80 90
100
District Hospital
Upazila Health
Complex
PublicMedical
College
PrivateMedical
College
PrivateHospital
PublicInstitute
Standalone Blood Centre
NGO Blood Centre
Others
Yes NO

30
S ys tem to follow up s ero ‐reac tive blood donors
0102030405060708090
100
Results are confirmed by
further tes ts
C onfirmation is done at the
centre
C onfirmation is done at a
reference laboratory
Donor is notified
DH (50) UHC (11) PMC (14) P rMC (6) P rH (7) P Int (5) S BC (6) NGOBC (2) O (8)
Figure 38 System to follow up sero‐reactive blood donors
S ys tem to follow up s ero ‐reac tive blood donors
0102030405060708090
100
P os t‐donation couns elling is
conducted
at the centre referred to another centre
DH (50) UHC (11) PMC (14) P rMC (6) P rH (7) P Int (5) S BC (6) NGOBC (2) O (8)
Figure 39 System to follow up sero‐reactive blood donors
Figures 38 and 39 shows the different aspects of management of donors, who are sero‐
reactive for TTI markers. Each of the centres orally reported to provide post donation
counseling to blood donors in each case but no protocol was evidenced. Most of the public
centres reported to refer the sero‐reactive blood donors from district to medical colleges
and to other private diagnostic centres for confirmation. However no feedback results were
registered in the centres. Confirmatory testing was not available in the centres and most of
blood donors were informed only of ELISA tests for TTI markers when available. There are
no national guidelines or written instructions available for processing blood donor deferrals
for further evaluations.

31
Figure 40 Status of TTI screening in the surveyed centres
Figure 40 shows that screening of five TTI tests mandatory in Bangladesh were carried out in
100% of centres except in 20% of district hospitals, 55% of Upazila health complexes, 23% of
private medical colleges, 29% of private hospitals, and 17% of standalone blood centres
which did not perform malaria testing routinely as evidenced from the assessment.
Quality as s es s ment of T T I tes ting .
0102030405060708090
100
Algorithm for trans fus ion
transmis s ible infec tions
IQC s amples us ed in each
run
P artic ipate in an E QAS for
TTI tes ting
P erform repeat tes ting in
cas e initial reacting blood
s ample
DH (50) UHC (11) PMC (14) P rMC (6) P rH (7) P Int (5) S B C (6) NGOBC (2) O (8)
Figure 41 Status of quality control system for TTI markers
Figure 41 shows varieties of information on quality system for TTI markers. The assorted
data from the assessment show that none of the surveyed centres (109) has the algorithms
for TTI markers; internal quality control (IQC) was not observed in district hospitals and
Upazila health complexes. Only 21% of public medical colleges, 50% of private medical
colleges, 80% of public institutes reported to run IQC during routine testing of TTI. All NGO
blood centres reported to run IQC during testing. With regards to External Quality
Assessment (EQAS) three public medical colleges and one NGO blood centre reported to
have participated in such a program organized by the Public Health Institute of Thailand.

32
Figure 42 Equipment for storage of test kits and blood samples
Figure 42 shows that all kits are kept in temperature monitored refrigerators in 72% district
hospitals, 35% in Upazila heath complexes, 100% in public and private medical colleges
hospitals and institutes whereas temperature monitored refrigerators for samples storage
were absent in varying degrees in all but NGO blood centres.
Screening of blood donations by Elisa Method
0
10
20
30
40
50
60
70
80
90
100
HIV I and II Hepatitis B Hepatitis C
DH (50) UHC (11) PMC (14) PrMC (6) PrH (7) PInt (5) SBC (6) NGOBC (2) O (8)
Figure 43 Method of blood screening by ELISA
Figure 43 shows that all surveyed centres carried out TTI testing using rapid method except in two
private hospitals and two NGO BC where ELISA and CLIA were seen to be carried out in addition to
rapid testing.
Temperature‐monitored Equipment for Samples, Kits and Reagents
0
20
40
60
80
100
Test kits/ Reagents Samples
DH (50) UHC (11) PMC (14) PrMC (6) PrH (7) PInt (5) SBC (6) NGOBC (2) O (8)

33
Figure 44 Status of repeat testing for initial reactive blood samples
All centres reported to perform repeat testing for initially reactive cases using the same type
of kits. The practice of repeat testing was absent in Upazila health complexes. It was 100% in
public and private medical colleges and institutes and NGO blood centres. The data also
revealed that no centre stored or archived reactive blood samples for look back studies.
S tatus of blood c omponent produc tion
0102030405060708090
100
Red cell components P latelets F res h froz en plasma
component
C ryoprec ipitate
component
Any other component
DH (50) UHC (11) PMC (14) P rMC (6) P rH (7) P Int (5) S BC (6) NGOBC (2) O (8)
Figure 45 Status of blood component production
Repeat testing of initial reacting blood samples
0
10
20
30
40
50
60
70
80
90
100
DH (50) UHC (11)
PMC(14)
PrMC(6)
PrH (7) PInt (5) SBC (6) NGOBC (2)
O (8)
Percentage

34
Only 2% of district hospitals reported to produce blood components, 43% of public medical
colleges, and 20% of public institutes, 50% of private medical colleges, 57% of private
centres and 100% of NGO blood centres reported to produce blood components. This
figures show that 10% of collected whole blood is converted into blood components by 17
centres in both public and private centres which represent 7% of the total (253 centres)
throughout the country. None of the surveyed centres reported to have quality control
programs for blood components and no centre reported to have a plasma fractionation
plant.
Figure 45 Relative production of blood components
This figure shows that 55% of RCC 26% of FFP and 20% of PRP are produced and distributed.
S tatus of B lood C omponent produc tion by apheres is
0
1020
30
4050
60
70
8090
100
Apheres is red cells Aphers is platelets Apheres is plasma
DH (50) UHC (11) PMC (14) P rMC (6) P rH (7) P Int (5) S B C (6) NGOBC (2) O (8)
Figure 46 Types of centres producing blood components by Apheresis

35
QC programme for blood components
0102030405060708090
100
District
Hospital
Upazila
Health
Complex
Public
Medical
College
Private
Medical
College
Private
Hospital
Public
Institute
Standalone
Blood
Centre
NGO Blood
Centre
Others
Yes NO
Figure 47 Quality control programme for blood components
None of the centres has a QC program for blood components

36
Part 2 Assessing the transfusion process in the hospital
Following data are responses to part two of the questionnaire related to pre‐transfusion
practices in the hospitals. It is to be mentioned that all blood centres surveyed are
integrated within hospitals except for standalone blood centres which are not.
Cold Chain
0102030405060708090
100
Blood storage operating
within pre defined
temperature
DH (50) UHC (11) PMC (14) PrMC (6) PrH (7) PInt (5) SBC (6) NGOBC (2) O (8)
Figure 48 Blood cold chain management
All centres reported to keep blood in temperature monitored centres except for Upazila
health complexes and standalone blood centres where no such system has been developed.
Stock control
0102030405060708090
100
Are SOPs on transport of
blood and blood products
in use at the center
Stand by generator to
provide power to the blood
storage equipment?
Is there a mechanism for
monitoring stock of blood
and components
Hospital accepted back
into the stock of the center
for reissue
DH (50) UHC (11) PMC (14) PrMC (6) PrH (7) PInt (5) SBC (6) NGOBC (2) O (8)
Figure 49 Stock control
None of the centres has developed SOPs for blood components or blood transportation. The
system of stock control monitoring was not adequately developed both in public and private
sectors except in the NGO blood centres where stock control of blood bags was available. All
centres in the public sector responded that they have mechanisms for accepting the units of

37
blood supplied to the ward of the same hospital but not outside the hospital. It uses criteria
though not written when the blood is returned back to the blood centre when not used. In
private medical colleges and in private hospitals the same rule is followed where blood
issued within the hospital is accepted if returned, under certain criteria. However, NGO and
standalone blood centres never accept blood units once supplied from the blood centres
even if returned within half an hour of issue.
Figure 50 Facilities for storage of blood and blood products
In clinical ward there were no separate refrigerators for transit storage of blood. All hospital
blood centres used blood bank refrigerators for transit storage of blood. Only five Upazila
health complexes and standalone blood centres reported to use domestic refrigerators for
blood storage.
Figure 51 Provision of separate storage
Provison of separate storage
0
1020
3040
50
6070
8090
100
Quarantine/ untested units Ready for issue Discarded units
DH (50) UHC (11) PMC (14) PrMC (6) PrH (7) PInt (5) SBC (6) NGOBC (2) O (8)

38
In response to facilities for separate storage like quarantine, ready for use and discarded
units, 4% of district hospitals, 7% of public medical colleges, 100% of NGO blood centres
have separate facilities.
Figure 52 Source of blood in hospitals
Except for two NGO blood centres all others reported to receive blood from different
sources arranged by the patients’ relatives. On average district hospitals received 93% of
blood collected by the centres themselves, 3% from NGO blood centres and 5% from
standalone blood centres. In medical colleges 85% of the blood is collected by the centres,
and the remaining 10% are from NGO blood centres and 5% from standalone blood centres.
Patient relatives were reported responsible for the transportation of blood to the patients.
There were no transport boxes seen being used in public and private medical colleges and
hospitals. Picnic type boxes were common transportation for blood in one centre.
Source of Blood in Hospitals
0 10 20 30 40 50 60 70 80 90
100
District Hospital (50)
Upazila Health Complex (11)
Public Medical College (14)
Private
Medical
College (6)
Private
Hospital
(7)
Public
Institute (5)
Standalone
Blood
Centre (6)
NGO Blood Centre (2)
Others (8)
Blood from other centers Blood from NGO blood centers
Blood from Private blood centers Collected by Centre

39
Figure 53 Status of compatibility testing
Compatibility testing was reported to be carried out in all centres surveyed. On inquiry all
centres responded to carry compatibility testing by using donor cells and patients serum in
100% of cases. There were mixed responses to ABO cell /serum grouping and RhD typing
during cross matching. Significantly no centre reported to perform antibody screening for
patients’ blood samples before any compatibility testing.
Methods used for the ABO (Red cell) grouping
0102030405060708090
100
District
Hospital
Upazila
Health
Complex
Public
Medical
College
Private
Medical
College
Private
Hospital
Public
Institute
Standalone
Blood
Centre
NGO Blood
Centre
Others
Forward Grouping Forward + Reverse
Figure 54 Methods of ABO grouping
The data show that 100% of blood centres in district hospitals, public medical colleges,
public institutes use slide method for ABO blood grouping and 18% of district hospitals, 8%
of Upazila health complexes, 21% of public medical colleges, 80% of public institutes, 83% of
private medical colleges, 71% of private hospitals, and 17% of standalone blood centres
under survey reported to carry out reverse grouping along with forward grouping. RhD
typing using slide method has been seen in all centres.

40
Figure 55 ABO grouping techniques
Figure 56 Methods of RhD grouping

41
Figure 57 Techniques of cross matching
The data show that all surveyed centres reported to perform cross matching at room
temperature. Only one NGO blood centre reported to perform cross matching by indirect
Coombs method as well. None of the centres carried out cross matching in addition to the
two methods.
Transfusion Process
0
10
20
30
40
50
60
70
80
90
100
Transport boxes used for
blood transportation
Demand of f blood and
shortage of supply
Separate storage areas
for cross matched and
uncrossed matched blood
and components
Use of domestic
refrigerator for storage of
blood and blood
products
System to check the
patient's previous
transfusion records as
part of the compatibi lity
testing
DH (50) UHC (11) PMC (14) PrMC (6) PrH (7) PInt (5) SBC (6) NGOBC (2) O (8)
Figure 58 Transfusion process
Data show that none of the centres has facilities for segregating cross matched and other
blood units. All centres reported to keep the previous transfusion records as part of
compatibility testing.
Hospital Transfusion Committee
0 10 20 30 40 50 60 70 80 90 100
District Hospital
Upazila Health Complex
Public Medical College
PrivateMedicalCollege
PrivateHospital
PublicInstitute
StandaloneBloodCenter
NGO Blood Center
Others

42
Figure 59 Hospital transfusion committee
The data show that hospital transfusion committees have been developed in all district
hospitals, public medical colleges and public institutes as per rules of Safe Blood ACT.
Figure 60 standard operating procedures for the transfusion process
The figure shows that SOPs for blood transfusion process were developed for completing
blood request forms, drawing and leveling, blood administration but not for transfusion
monitoring and management of transfusion reactions. There were no national guidelines
developed for clinical indications for transfusion, such as Maximum Blood Ordering
Schedules (MSBOS), safe blood administration, transfusion reactions. However, during
assessment, most of the responders could not show the data because such data were not
recorded in the centres. Only in two centres the Red Crescent blood centre and Quantum
blood centre have extensive data. But they were not calculated and recorded according to
the requirement assessment. For example, these two centres have records of new donors
but the number could be not be ascertained as new. Data for the use of blood components
were not available as per types of patients in any of the surveyed hospitals.
Standard operating procedures (SOPs) or local written instructions
0 10 20 30 40 50 60 70 80 90
100
Completing the blood request form
Drawing and labelling the pre-transfusion
blood sample
Collecting blood andblood products from
the blood bank
Storage of blood andblood products prior to
transfusion
Administeringblood/components,including patient id
check
Monitoring the patient before, during and
after the transfusion
Managing andrecording transfusion
reaction
Percentage

43
11. Discussion
a) Organization and management of blood transfusion services The Blood Transfusion Service in Bangladesh has been reorganized since 2000 with the
implementation of the National Program Safe Blood Transfusion under the Ministry of Health and
Family welfare. To regulate and improve the service Safe Blood Act 2002 was approved by the
parliament. Safe Blood Transfusion Program is the only implementing authority that has been
dealing with facilities development in blood centres up to Upazila level hospitals by providing the
logistics, manpower training and regular monitoring. There is National Safe Blood Transfusion
Council constituted under the Ministry of Health to direct the National Safe Blood Transfusion
Program to develop policy, guidelines and implement the projects for improvement of BTS. Besides,
there is an expert committee constituted of the Directorate of Health services for implementation of
the resolutions taken in National Safe Blood Council meeting. The overall management of the blood
transfusion centres through the health care system is coordinated and implemented by the National
Safe Blood Transfusion Program. The assessment does not reflect the whole scenario of BTS in the
country but only partially. However, the data represent 43% (109) of the total (253) centres in the
country, which is significant.
Each of the centres under survey, collects, processes, screens and distributes blood to the hospital
where it is located. Thus there is no central collection system throughout the country. Requirement
of licensing is mandatory for the private sector and inspection by licensing authorities was found
inadequate. There is no regular system of supervision of transfusion service and no program for
implementing quality service. The hospital transfusion committees formed in all public blood centres
need activation for addressing and resolving various management issues at the local level. The
shortage of manpower in each of the public centres appears to be a major constraint for the
implementation of activities. This is applicable to the national program, where there is shortage of
manpower to conduct regular supervision and monitoring of the centres. However, there is scope
for development of an expert team under the national expert committee to visit the centres on a
regular basis for implementing quality standards in the BTS as a decentralized system.
b) National blood donation and collection practices From the assessment it is noted that blood collection in BTS is mainly hospital‐based, fixed site
collection. The data show that 15% of blood is collected from voluntary blood donors and 85% from
relative/family blood donors and that there were no paid donors in any of the surveyed centres.
However, there is lack of coordination between the voluntary blood donor organization and the
public sector for blood collection and utilization. No national blood donation strategy is yet
formulated and no strategic program is yet implemented at national level. The promotion for
voluntary blood donation was found inadequate at the national level. No national blood donor data
base is yet to be developed for recruitment of blood donors. It is also seen that pre‐donation
haemoglobin estimation is not practiced in any of the 109 centres; furthermore, all centres maintain
records of donor deferrals due to sero‐reactive TTI markers but not for other reasons. Reliance on
replacement donors as a source of blood is seen in all centres. Such donors usually have a higher
frequency of infectious disease markers. It is urgent to develop a panel of voluntary donors whose
blood is available for any patient. For the recruitment of voluntary blood donors a major effort
should be made to develop a national program with an emphasis on training and motivation of

44
young people regarding their eventual responsibility in this matter. Blood donor publicity in adults
should be targeted towards middle and upper class persons who have better health standards. This
could be done in conjunction with various NGOs. A collaborating blood collection program based on
governmental and NGO should be considered under the frame of policy development.
c) National practices in screening of donated blood It has been reported that all blood transfusion centres under survey performed 100% blood
screening for HIV, HBV, HCV and syphilis. All screening tests for viral markers are done using rapid
method and only a few centres perform ELISA tests. However, the quality assessment of TTI testing
was found inadequate. No facilities for confirmatory testing for repeat reactive markers have even
been reported. Blood donor management, donor notification and deferral are poorly developed in
the BTS in either of the systems. Besides, in district blood centres and in the private sector blood is
screened as pre‐donation technique however data for sero‐reactive TTI markers were not recorded
in the national screening data. How many of them later become false reactive? Or true negative?
These data were not available. Single test strategy is being followed for screening in Bangladesh. Due
to non‐ availability of referral system most of the sero‐reactive blood donors were not enlisted and
followed up systematically to final confirmation. For the same reason no algorithms have been
started for blood screening for confirmation for initial reactive and repeat reactions as well as for
blood donor notification. There is a general lack of quality control and assurance in all laboratories
and in spite of imparted training the concept has not been institutionalized neither in the district
hospitals nor in medical colleges and hospital blood centres in both the sectors. There is an urgent
need to upgrade serological techniques and to implement SOPs in all transfusion processes.
d) Blood component preparation From the assessment it has been learnt that 17 centres throughout the country are producing blood
components which convert 10% of total blood collection into blood components. There is no plasma
fractionation plant in the country. However, quality control of blood components is yet to be
developed in either sector. Use of blood components is not seen as widely practiced in most of the
centres; this is due to lack of facilities and lack of orientation on the rational use of blood and blood
components and in some centres blood component machines were seen not functioning.
e) Inventory of blood and blood products and status of the blood cold chain From the assessment it is seen that in most of the blood centres single type refrigerators are used
and all units (cross matched, uncross matched, screened and unscreened blood) were kept in the
same refrigerator. It is reported that 4% of district hospitals, 7% of public medical colleges, and 100%
of NGO blood centres have separate facilities for quarantine, ready for use and discarded units. This
reflects an inadequate storage system for maintaining an appropriate cold chain for blood and blood
products. Furthermore, in the public sector no cold chain system was used during transportation of
blood from blood centre to the clinical wards of same hospitals. Only in two of private hospitals’ cold
boxes were used for transportation of blood.
f) Pre‐transfusion practices in hospitals It is to be recalled here that in Bangladesh, blood centres are integrated to each of the hospitals
except for the standalone blood centres of the private sector. Due to shortage of blood, each of the
hospital collects blood from other sources. Except for two NGO blood centres, all centres reported to
receive blood from different sources arranged by patient’s relatives. On average district hospitals

45
received 93% of blood collected by the centres themselves 3% from NGO centres and 5% from
standalone blood centres. In medical colleges 85% of blood was collected by the centres and the
remaining 10% from NGO blood centres and 5% from standalone blood centres. Patient’s relatives
have been reported responsible for transportation of blood to the patients. Consequently, not all
centres are sufficient to meet the requirements for their own respective hospitals. The assessment
revealed that 100% of blood centres in district hospitals, public medical colleges, public institutes
use slide method for ABO grouping and 18% of district hospitals, 8% of Upazila health complexes,
21% of public medical colleges, 80% of public institutes, 83% of private medical colleges, 71% of
private hospitals, and 17% of standalone blood centres reported to carry out reverse grouping along
with forward grouping. RhD typing is done using slide method in all centres. Compatibility testing
was reported to be carried out in all surveyed centres. All carry compatibility testing by using donor
cells and patients serum which does not meet the standard criteria for compatibility testing.
Most of the responders particularly mentioned that manpower shortage is one of the reasons for
not maintaining the standards for testing. Blood centres are always under pressure to supply blood
within a short period of time in most of the cases. No centre reported to perform antibody screening
for patient’s blood samples before any compatibility testing. Centres surveyed reported to perform
cross matching at room temperature. Only one NGO blood centre reported to perform cross
matching by indirect Coombs. Apart from that none of the centres carried out cross matching in
addition to the two methods described. Quality standards for blood grouping, serology and
compatibility testing need urgent attention for maintaining SOPs. The assessment revealed that
none (except only two private hospitals) of the centres have ever developed SOPs for core
laboratory process which is one of the challenges for Safe Blood Transfusion Program. The
assessment revealed that hospital transfusion committees have been developed in all districts
hospitals, public medical colleges and public institutes as per rules of Safe Blood ACT. However,
these committees need more orientation about the clinical transfusion process monitoring.
g) Transfusion monitoring and post‐transfusion practices in hospitals It is noted that written instructions for the blood transfusion processes were developed for
completing blood request forms, drawing and leveling. However, there were no such protocols or
instructions for blood administration, transfusion monitoring and management of transfusion
reactions. No haemovigilance protocols have been developed in either of the centres. It is to be
mentioned here that blood ordering schedule is also not developed in any of the hospitals visited.
12. Conclusion Good progress has been made in Bangladesh, but the pace now should be quickened in view of
establishing a quality system in the country, particularly addressing the huge need for blood due to
improving medical services and the expansion of the population. However, in spite of imparted
training, workshop on clinical use of blood, monitoring of the centres by SBTP and DGHS, the
implementation of SOPs was not observed in any of the surveyed centres. The basic procedures of
blood typing, cross matching, with exception of a few centres are not followed as per standards
which poses great threat to quality service.
The numbers of documents for pre‐transfusion records of patients were scarce and a high variation
of format of documentation as well as number of registers to keep vital records related to donor

46
traceability and patients’ transfusion were observed. Similarly, registers for blood donation, cross
matching and laboratory procedures were not uniformly followed and documented in centres
according to SRO of BTS. Similarly, in the clinical transfusion settings of the visited centres none of
centres could produce documents or registers for transfusion monitoring and recording adverse
transfusion reactions. As reported, blood screening kits were procured by each centre when the
supply from SBTP was inadequate and none of the public centres showed any documents for critical
supply of test kits or blood bags purchased by using local funds. All public centres reported staff
shortage and showed constraints in delivering quality service especially in medical colleges and
district hospitals.
Over the past decade since the creation of SBTP, blood collection and donor recruitment has only
changed from paid donation system to donations by relatives and there is rarely any stock seen in
public centres of blood collected from voluntary donation and no stocks of blood were seen in the
Upazila health complexes during the survey. Nonetheless, Safe Blood Transfusion Program has been
successful in lowering the rate of TTI markers in blood donors (below 1%) through the introduction
of mandatory blood screening backed by the Safe Blood Act. The isolated success would need to be
consolidated through gap analysis and lessons learnt between the sector wide program and the
findings of the assessment. The SBTP from the very outset focused on prevention of TTI, rather than
total improvement of coordinated BTS. Consequently, time bound strategic planning like immediate,
midterm and long term action plans need to be formulated and implemented. The experts
recommended assessment of all centres in order to get more information. The questionnaires set
which was prepared and developed after consultation was exhaustive however many of the
responses were not well registered due to paucity of systematic records; in many instances it was
also difficult to retrieve full information within the short period of time allowed for assessment.
The assessment findings can serve as input for formulating a capacity development response for
capacities that could be strengthened and optimize the already strong and well founded ones. It can
also set the baseline for continuous monitoring and evaluation of progress against relevant
indicators and help create a solid foundation for long‐term planning, implementation and
sustainable results. The collected data can be used, for instance, when preparing national action
plans for blood transfusion services and implementation strategies. In the context of any of the
situations just described, the collected data will act as a catalyst for action, confirm priorities and
provide insight into operational hurdles experienced in the last program from 2000 to 2010. It is to
be noted that the conducted assessment opened an opportunity to educate and update program
personnel and the responders at the centres on the importance of data series required for updating
the global data base of blood safety. The assessment has introduced and put emphasis on use of
benchmark which needs to be considered for adaptation and implementation of quality assurance. It
was learned from the assessment that the blood transfusion service (2000 and onward) in
Bangladesh had been largely successful in establishing mandatory blood screening in public and
private sectors, initiating blood components production, institutionalizing training, data collection,
and regulation of private blood centres. The assessment has encouraged prioritizing the use of
different indicators.

47
13. Recommendations The infrastructure of blood transfusion services especially in district hospitals under the public
sector needs more attention in providing physical space required for proper functioning of the
blood centres. The blood transfusion services should be separated from diagnostic
laboratories. Each blood centre in district and Upazila health complexes should also have
suitable facilities and preferably separated from pathology departments.
There should be deputation of additional staff such as medical technologists in each blood
centre. Medical officers working in blood centres should get frequent training along with
medical technologists on procurement, SOPs, quality assurance, record keeping,
documentation, stock management, TTI algorithms, standard practices for serology,
compatibility testing, and pre‐ and post‐donation counseling.
The overall management personnel in each centre require management training and training
on quality management for implementing SOPs in BTS.
Safe Blood Transfusion Program should consider training for the private sector so that the
uniform standards are being followed in each centre, which would assist the licensing
authority to conduct regular monitoring and supervision of standards.
National standards should be developed for blood transfusion including SOPs. National
authority should train the personnel on the basis of national standards of blood transfusion.
The national voluntary blood donation program should be structured with participation of
potential stakeholders and policy should be adopted for GOVT–NGO collaboration for
organizing motivational and blood collection programs to build up blood stocks in the centres.
There should be policy adopted for equal distribution and exchange of blood between public
and private sectors in order to have optimum utilization of blood.
Regional basis blood collection should be initiated jointly by medical colleges and voluntary
blood donor organizations for more blood components production and replacing the use of
whole blood in all cases.
Safe Blood Transfusion Program with collaboration of reference laboratory should take
initiative for the development of TTI algorithms and conduct regular quality of TTI testing and
serology with recommended WHO collaborating centres.
Regional medical colleges should be strengthened with adequate facilities and manpower for
acting as regional referral centres for confirmatory testing of TTI markers.
National guidelines should be developed for blood donor deferral, confirmatory testing,
management and notification.
Clinicians need more orientation on rational use of blood and should be encouraged to
develop SOPs for blood administration, monitoring transfusion and reporting hazards of blood
transfusion.
Local level hospitals transfusion committees should be oriented proactively in developing
local blood transfusion guidelines for monitoring and supervision of BTS including
development of haemovigilance protocols.

48
There should be provision for adequate and appropriate equipment in each centre and
adequate refrigerators provided for segregation of units of blood before and after testing.
Members of national expert committee and experts of higher institutes should visit the
different types of centres under monitoring program to support SBTP in establishing quality
services in a large number of centres throughout the country.
The Reference Laboratory (RL) should function as a national confirmation centre to provide an
independent opinion on repeat reactive TTI donor samples. It should have appropriate and
validated confirmation testing facilities in place such as Western blot technology, Nucleic Acid
Amplification Technology (NAT), PCR, CLIA and competent staff with adequate training to
perform the tests. RL should also monitor training activities in regional centres and compile
data of TTI and blood components, update the national data and report to national authority.
Besides, the centre should take any advance training, like quality assurance, EQAS and
research. It should have a networking system with regional centres.

49
14. Proposed Action Plan
Activities / Timeline Month
1 2 3 4 5 6 7 8 9 10 11 12
1 .Situation Assessment
Assess the existing facilities/ practices and
identify gaps for screening donated blood
2. Develop National Action Plan and
Baseline indicators
Develop national action plan (workshop)
Develop baseline indicators
3. Review / develop national standards,
strategies and algorithms
Develop / Review and revise National
Blood Policy, National Guidelines,
Strategies, SOPs and related documents
Dissemination of the above guidelines to
stakeholders and regular CME for updates
4. Develop equipment, reagent
management system
Review procedures in current use in the
procurement of equipment and
kits/reagents
Develop a system (procurement guideline)
for development and evaluation of
specification for blood banking logistics
including reagents/kits/blood bags;
printing of the guideline & dissemination
Streamline evaluation procedure for
procurement of equipment/kits/reagents
5. Identify, designate and build capacity of
national reference laboratory
Establishment of regulatory mechanism for
Blood Banking (EQAS, Proficiency Panel
Preparation and validation, Evaluation of
diagnostic kits/ reagents/ blood bags/blood
bank equipment; import/export of
reagents/kits)
Training for staff in management of
NEQAS, Proficiency panel preparation, TTI
screening,

50
Activities / Timeline Month
1 2 3 4 5 6 7 8 9 10 11 12
6. Capacity Building
Develop capacity on investigation of
transfusion reactions and haemovigilance
protocol
Training of staff in Transfusion medicine
(Fellowship)
Networking of Central, Regional, District
and Hospital based Blood centres Review
Meetings* and monitoring
7. Training for laboratory personnel
Hands on training on TTI screening
Hands on training on waste management
Hands on training on proper use of the
SOPs
8. Training and support to develop quality
systems
Develop Quality Policy and manual
Hands on training workshop on quality
assured screening of donated blood
including IQC, QA, EQAS, Waste
Management
Development and distribution of SOPs
Training workshop for recording, reporting
and maintenance of Blood Banking
information system
9. Strengthen information management
systems
Develop and operationalize a web based
Information Management System
Expansion of the web based Blood Banking
Information Management System linking
with MIS.
Technical support for maintenance of
Blood Banking data management system
Regular evaluation of the program
Implementation by experts of MoHP/WHO
country office/ HQ through visits, review
meetings, etc.

51
15. Limitations The used toolkit was very comprehensive and it would have been very useful for introduction of
WHO framework for monitoring. However, the assessment suffered a considerable time due to non‐
availability of data collectors for conduction of the assessment. There were other administrative
problems in the program management like changes of program managers which ultimately led to
delay in timely conducting of the assessment. Due to considerable number of variables the analysis
by SPSS also took time to prepare the final report.
16. Acknowledgements The assessment has been successfully completed with the assistance of Safe Blood Transfusion
Program team and resource persons of DGHS under the leadership of program director, program
manager and deputy program manager of BAN‐BCT and SBTP. During the visits of the centres,
responders cordially supported the team in inspection of the centres showing the records and
statistics which greatly contributed in the assessment. It is nevertheless to acknowledge the
technical assistance of WHO country office, Dr Neelam Dhingra, WHO HQ, Dr Rajesh Bhatia, SEARO,
WHO for which such assessment could have been conducted. Dr MK Zaman Biswas, National
Professional officer (epidemiology), Dr Murad Sultan, technical officer, blood safety, national
consultants CSR, EHA and data analyst and statistician are greatly appreciated for their contribution
in making the assessment successful. Dr SM Alamgir, Dr Muzaddeed Ahmaed, Dr Syeda Masooma
Rahman, Dr Enamul Haque, Dr Zahidur Rahim and Dr Selina Khatun of WHO and Dr Md Ashadul
Islam of blood transfusion and Dr Mazharul Hoque, DPM, SBTP, Dr Aminul Hassan, DMP, DGHS have
been acknowledged for their continuous and pro‐active support that enlightened with valuable
guidance during the assessment. Collaboration and support of OFID is highly appreciated.
References 1. Aide Mémoire: Blood Safety, 2002
2. WHO Aide Mémoire: Good Policy Making Process for blood safety and availability, 2008
3. WHO Aide Mémoire: Quality System for Blood Safety, 2002
4. WHO Aide Mémoire: Safe Blood Components, 2005
5. WHO Aide Mémoire: Clinical Use of Blood, 2003
6. WHO, Framework for Assessment, Monitoring and Evaluation of the Blood Transfusion
Services, 2010
7. Safe Blood transfusion Act 2002
8. Safe Blood Transfusion Rules 2008
9. Screening Report of Safe Blood Transfusion 2010
10. Bangladesh Health Bulletin, 2011

52
ANNEX I: Assessment questionnaires
The assessment tool for Blood Transfusion at Public and Private sector
DGHS and WHO
Name of the DATA collectors with Designation with contact number:
………………………………………………………………………………….
………………………………………………………………………………….
………………………………………………………………………………….
Date of visit: …………………………..
Date of Reporting and submission: …………………………
Signature: ……………………………
Center Code …………. . . . . . . . . . . . . . . . . . District…………………………. . Division ………………………. .

53
Part 1: Assessing the blood centre1
General information about the Centre
Name of the facility
Address
City/ town
District
Name of officer in‐charge
Designation
E‐mail Telephone
Fax Other
Date of report ‐
Reporting period: From To
Name of responder/s
With contact number
Signature
Type of blood centre
National Blood Centre
Regional/ Provincial Blood Centre
District level Blood Centre/Blood Bank
Other (Please specify)
.
1 It can be standalone blood center that collects, screens, processes and distributes blood or a hospital‐based blood center that collects, screens, processes and issues (or distributes) blood. Hospital blood banks that only store blood and check compatibility should not be regarded as a blood center.

54
Section A: Organization and Management
General management
1 Under which management responsibility does the blood centre operate (please tick):
[1] Public (under MOHFW)
[2] Public (other than MOHFW)
[3] Non‐governmental/non‐profit organizations
such as the National Red Cross Society
[4] Private Blood centre
2 What type facility does the centre belong to? (please tick)
[1] Standalone blood centre
[2] Hospital based blood centre
[3] Hospital based blood bank (as part of the laboratory)
[4] Other (Please specify)
3 Is the National authority (SBTP) supporting the blood centre? Yes No
If yes,
Types of support
Financial : Yes No
Reagent : Yes No
Blood Bag : Yes No
Equipment : Yes No
Others specify :
Quality System
4
Does the centre have a quality policy? Yes No
If yes, please obtain a copy
A document that defines the goals and objectives of a blood transfusion service or blood
centre with regard to quality, a commitment to meeting stated requirements, and an
undertaking to drive continuous improvement throughout its activities.
It must be suitable for the organization and provide a framework for establishing,
communicating and monitoring performance against agreed quality objectives.
5 Does the centre have an organizational structure indicating authority, responsibility and
reporting relationships? Yes No
If yes, please provide a copy of the organigram.
6 Are there written job descriptions for all positions within the department /centre?
Yes No

55
7 Has the centre appointed a person responsible for quality management?
Yes No
The appointed, responsible and authorized individual within an organization with the
responsibility for developing and managing the quality system
8 Does the centre have Standard Operating Procedures (SOPs) or local written instructions
for following areas of the centre? (Please tick as appropriate)
Yes No
[1] Blood donors selection
[2] Blood collection and donor care
[3] Blood component preparation (RCC, FFP, PRP)
[4] Screening for TTI
[5] Blood group serology and Cross matching
[6 ] Waste management
9 Do the centre maintain records of the following: (Please tick as appropriate)
Yes No
[1]Blood donors selection
[2]Blood collection and donor care
[3]Blood component preparation
[4 ]Screening for TTI
[5]Waste management
[6] Patient blood grouping register
[7]Donor blood group register
[8]Cross Matching register
[9]Blood Supply register
[10]Blood Stock register
Training
10
How many staff work in the centre in following categories and how many of them have
been trained during the reporting period? (Please specify numbers)
Category of Staff Total
number
of staff
In‐service
training
(departmental
on blood
transfusion)
National
training
course/work
shop (SBTP)
International
training
course/worksho
p SBTP)
Professor
Associate professor
Assistant Professor
Consultant
Medical officer
Medical
Technologist

56
Nurse
Counsellor
Administrative staff
Others specify
11 Does the centre have adequate staff for its operations2?
Equipment & Supplies
12 Please provide information on the availability and functioning of the equipment in the
centre based on the list at the end of the section.
13 Does the centre have adequate equipment for its work?3 Yes No
How are equipment procured?
Please tick as appropriate
Yes No
[1]Purchased locally by the
centre
[2]Purchased centrally or
through upper level agencies
[3]Donated by international
development agencies/donor
countries
14
[4]Other (please specify)
15 Does the centre provide staff training of the use of equipment? Yes No
16 Does the centre have a program for equipment maintenance?
Yes No
17 How key supplies4 in the centre were purchased?
Please tick () whenever applicable.
Yes No
[1] Purchased locally at the centre?
[2] Purchased centrally or through upper level
agencies
[3] Evaluated before procurement?
[4] Validation of kits, reagent and blood bag
carried out? If yes
2 this question should be answered based on the national criteria if there is one, otherwise the answer can only reflect the perceptions of the directors/managers of the blood center 3 Same as above

57
Whether in practice
(reagent, kits and blood bag)
18 Is there a system of stock control for the critical supplies? Yes No
If yes
Blood
Logistics Blood Bag
Kits
Reagent
Others specify
Critical stock items are all items that directly or indirectly affect the ability to collect, test,
process and distribute blood and blood products
19 Have any of following supplies run out in the last 12 months?
Yes No
(Please tick and indicate number of days affected without supply)
Item No Yes If yes, please indicate
number of days
[1]Blood bags
[2]TTI kits
[3] Blood Grouping
Reagents
[4]Others (Pl.
specify)
Regulation
20
Is the centre registered/ licensed (private organization)? Yes No
20. 1 If yes, under what national body/ authority/ agency is the centre registered /licensed?
_________________
21
Is the centre inspected for the purpose of registration / license? Yes No
If yes,
21. 1 When was the last inspection carried out?
_____________ Date/month/year
Health and Safety
22 Is there a program for Health and Safety in the centre? Yes No
Detailed information on the program
4 Key supplies include blood bags, TTI test kits, blood group serology reagents, etc.

58
Premises
23 Does the centre have suitable premises for5:
Yes No
[1]Donor selection and collection
[3]Blood processing and testing
[4]Storage and distributing
[5] Wash room /Bath room for donors
[6]. Store room
[7] Room for Blood Transfusion staff
[8] Autoclave
24 Does the centre have access to:
Yes No
[1]Continuous water supply
[2]Power supply
[3]Transportation system
[4] telephone
[5]fax
[6]internet
5 The questions should be adapted based on the country‐specific guidelines about work area regulations.

59
Equipment in the blood centre6:
Equipment Number
expected
Number
available
Number
functioning
Donor beds/couches
Weighing scale
Blood collection monitor (bio Mixture)
Sphygmomanometers
Tube sealers
Container for safe disposal of sharps
Oxygen supply equipment (e.g. cylinder)
PC with accessories and software
bench top centrifuge for samples
Blood transportation box
Double pan balance
Cell washer centrifuge
Binocular microscopes
Laboratory thermometers
ELISA plate washers
ELISA plate reader
Automatic pipette
pH Meter
Autoclaves machine
Water bath
Incubators
Hot Air ovens
Deep freezer‐750C‐80 0C
Plasma extractors
Platelet incubator and shaker
Haematology autoanalyzer
Refrigerated centrifuges
Haemocue/instrument for Hb Estimation
Voltage stabilizers
Distill water Plant
Blood bank refrigerator
6 The list of equipment should be adapted to be used for the blood centres in various levels in the country where assessment is conducted. If a national standard for the equipment requirement at various level of blood services is available, this list should be based on the standards.

60
Pharmaceutical refrigerator
Air conditioner
Blast freezer

61
Section B: Blood Donors & Blood Collection
25 Are following activities undertaken by the centre (please tick)?
Activities Yes No
Blood donor recruitment
Pre‐donation counselling
Blood collection from donors
Note:
If your answer to all the above is "No", skip section "B" of the questionnaire completely.
If your answer to any of the above is "Yes", please answer all relevant questions on that topic.
26 Does the centre have dedicated unit and staff for the blood donor program? Yes No
27 Is there a physician in the centre with responsibility for medical matters such as donor
health and safety? Yes No
28 Does the centre have trained donor recruitment staff? Yes No
29
Is there a specific budget line item for the donor program? Yes No
30 Are educational materials for donor information available?
Yes No
If yes, at what level were these materials developed
By the centre_________; Regional/____________________; national_______________.
31 Are there criteria for assessing the donor suitability to give blood?
Yes No
32 How do you assess donor suitability? (Please tick.)
Method Yes No
[1]Donor questionnaire
[2]pre‐donation counselling & interview
[3]Physical check
[4]Other, specify
33 Does the centre estimate donor's haemoglobin or haemtocrit before donation?
Yes No

62
34 Is there a blood donor database/registry in the centre? Yes No
34. 1 If yes, how is it maintained?
Manual Electronically
35 Among the total number of DONATIONS from voluntary non‐remunerated blood donors
who donate during the period, how many are from new donors
Please indicate the number of DONATIONS that were collected in different locations. (last
one year)
Nº
‐ Static location
‐ Mobile sites
36
Is only one standard volume of donation routinely collected in the centre?
Yes No
36. 1 If yes, what is the standard volume of a whole blood unit collected in the centre?
36. 2 If different volumes are routinely collected in the centre, please indicate the number
of BLOOD DONATIONS different volumes?
Volume of Collection (ml) Nº (write "E" if it s estimated)
37 Does the centre collect blood through apheresis procedures?
Yes No
38 Does the centre collect autologous (pre‐depository) blood donation?
Yes No
If yes, please indicate the total number of autologous DONATIONS (pre‐depository) collected
in the centre during the reporting period.

63
39 Are records of adverse blood donor reactions maintained?
Yes No
39. 1 Please indicate the number of donations with adverse reactions for the reporting
period? You may give an estimated% if the exact number cannot be provided.
Type of reactions Number of donations with
adverse reactions
%
[1]Total
[1. 1]Mild reaction
[1. 2]Modest reaction
[1. 3]Severe 40 Is there a system to follow up sero‐reactive blood donors (please tick)?
Yes No
40. 1 If yes, answer the following by ticking as appropriate
Yes No
[1]Results are confirmed by further tests
[1. 1]Confirmation is done at the centre
[1. 2]Confirmation is done at a reference
laboratory
[2]Donor is notified
[3]Post‐donation counselling is
conducted
[3. 1]at the centre
[3. 2]referred to another centre
40. 2 If donor counselling is conducted in the centre, is it conducted by trained personnel?
Yes No

64
Section C: Screening for Transfusion Transmissible Infections (TTI)
41 Does the centre screen the donated blood for following TTI (please tick)?
Screening for Yes No
HIV I and II
Hepatitis B
Hepatitis C
Syphilis
Malaria
Note:
If your answer to all the above is "No", skip all questions of section "C".
If your answer to any of the above is "Yes", please answer all relevant questions on
that screening test.
42 Does the centre have an algorithm for screening donated blood for transfusion
transmissible infections?
Yes No
42.1 If yes, please provide a more detailed description of the algorithm (Document of
procedures and Protocol for testing and interpretation of result specially for initial reactive
case, repeat reactive case and confirmatory testing)
43 Does the centre participate in an external quality assessment scheme (EQAS) for TTI
testing?
Yes No
44 Are test kits/reagents and samples stored in temperature‐monitored equipment?
Yes No
[1]Test kits/ Regents
[2]Samples
45 [1] Please indicate percentage of donations screened for transfusion transmissible
infections (TTI) during 2010 (Jan‐December).
TTI markers %
[1] HIV I and II
[2]Hepatitis B
[3]Hepatitis C
[4]Syphilis
[5]Malaria 46 Are different types of test methods (such as simple/Rapid and ELISA methods) used for the
screening of blood donations for TTI?
Yes No

65
46. 1 If yes, please indicate the types of test methods used in the centre and the total
number of donations tested by each method during the reporting period:
Test method used (please tick) and the number of donations tested
by the different method
Infection
markers Simple/Rapid
Test
ELISA Other, specify
Used No. Used No. Used No.
[1]HIV I/II
[2]Hepatitis B
[3]Hepatitis C
[4]Syphilis
[5]Malaria
[6]Others,
specify
47 Does the centre perform repeat testing in case of initial reacting blood sample
48 Are reactive results in the screening tests confirmed (either by the centre or through
reference laboratories)? If yes, please indicate the number of donations that were positive
in the confirmatory test.
49 Does the centre keep records of screening tests performed for TTI marker by different type
of voluntary non‐remunerated donations? (Voluntary donors are new and repeat)
Yes No
Others, specify
Section D: Blood Group Serology and Compatibility Testing
50 Which of following tests were performed on blood donations for determination of ABO
and Rh (D) groups and what techniques were followed? (Please tick)
Red cell/
Forward
Grouping
Serum/
Reverse
Grouping
RhD
Grouping
[1]Slide
[2]Tube
[3]Micro‐plate
[4]Column agglutination

66
[5]Magnetic bead technology
[6]Others
51 Do you perform irregular antibodies screening on blood donations?
Yes No
52 Does the centre participate in an external quality assessment scheme (EQAS) for Blood
Grouping Serology assay? (see the EQAS for TTI)
Yes No
52. 1 If yes, at which level does the centre participate in EQAS?
Level Please tick.
International
National
Regional/
provincial
Local 53 Does the centre provide compatibility testing for other hospitals/clinics?
Yes No
If yes, what is the total number of cross‐match procedures performed by the centre?
Section E: Blood Component Preparation
54 Does the centre prepare blood components?
Yes No
Note:
If your answer to all the above is "No", skip this section ("B") of the questionnaire
completely.
If your answer to any of the above is "Yes", please answer all relevant questions on
that topic.
55 What is the number of whole blood donations that were separated into component during
the reporting period?
(number of donations)
56 What type of components does the centre prepare? How many units were prepared during
the reporting period?
Please tick “yes or “no” and, if the answer “yes” is chosen, indicate the total units of blood
components prepared during the reporting period.
56. 1 Whole blood derived components
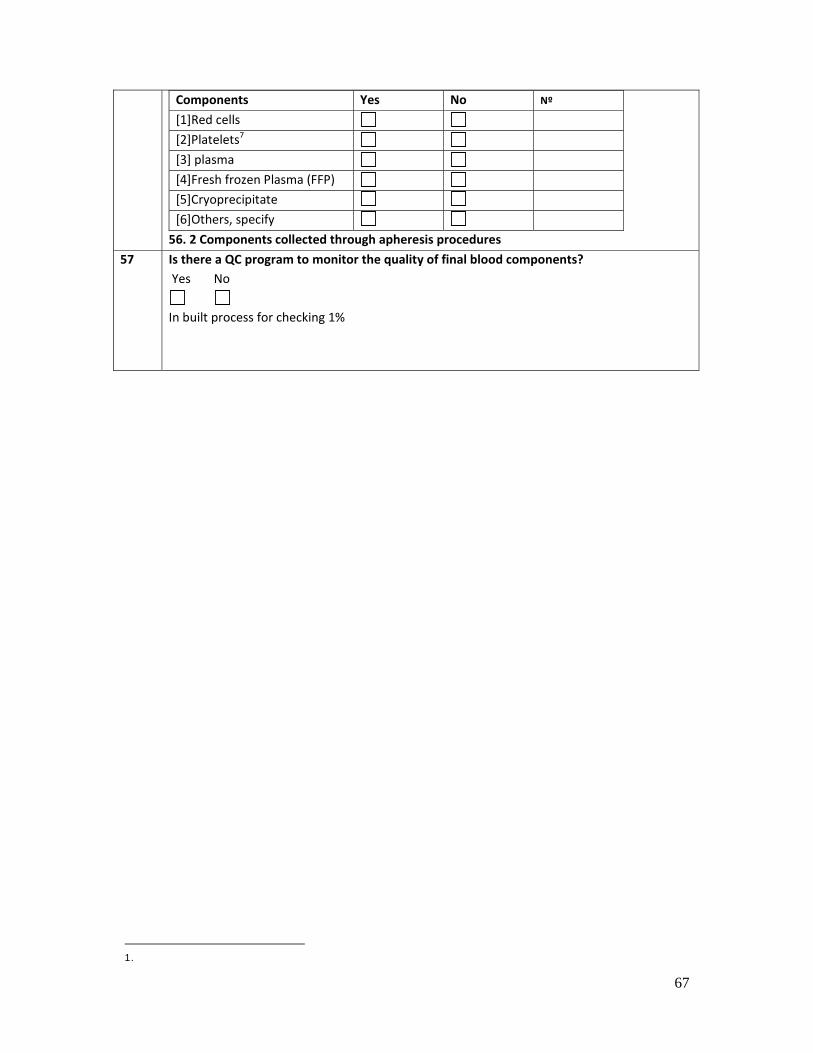
67
Components Yes No Nº
[1]Red cells
[2]Platelets7
[3] plasma
[4]Fresh frozen Plasma (FFP)
[5]Cryoprecipitate
[6]Others, specify
56. 2 Components collected through apheresis procedures
57 Is there a QC program to monitor the quality of final blood components?
Yes No
In built process for checking 1%
1.
68
Section F: Blood Storage, Transportation, Inventory & Distribution
58 Is blood storage operating within the pre‐defined temperatures for storage of blood and
blood components according to the SRO?
Yes No
WB +20C to + 6 0C
Platelet concentrate +200C to + 24 0C
FFP (fresh Frozen Plasma‐300C
Cryoprecipitate‐300C
59 Is the temperature of the blood storage equipment in the centre monitored?
Yes No
If yes, describe how it is monitored.
Temperature chart
Report of inspection
60 What types of freezers does the centre use for storage of blood or blood products?
Yes No
[1] Blood Bank Refrigerator
[2] domestic refrigerator for whole blood/red cell
[3] domestic freezer for FFP/Cryoprecipitate
If yes, please provide the number of domestic refrigerators and freezers used and (if possible)
the estimated percentage of blood/blood components stored in the domestic refrigerators or
freezers.
(Is the temperature monitored? How is it monitored?)
61 Does the centre have separate storage areas for following purposes?
Yes No
[1] Quarantine/ untested units
[2] Ready for issue to patients
[3] Discarded units
62
Does the centre use equipment for blood transportation? Please tick "Yes" or "No"
appropriately. If "yes" is ticked, indicate the numbers of equipment the centre have for
transportation?
Yes No Number
[1] Picnic type boxes
[2] locally made boxes
[3] Standard cold boxes
[4] Refrigerated vehicle
[5] Other, specify

69
63 Is the temperature of blood monitored during transportation?
Yes No
If yes, describe how it is monitored.
64 Do you have stand‐by generator to provide power to the blood storage equipment?
Yes No
65 Is there a mechanism for monitoring stock of blood and components?
Yes No
If yes, please describe how the stock of blood and components are monitored
66 Please provide the total units of blood and blood components distributed during the
reporting period
Units
[1]Whole blood
[2]Red cells
[3]Platelets
[4]Fresh frozen Plasma (FFP)
[5]Cryoprecipitate
[6]Others, specify
67
Is the blood not used by the transfusing hospital accepted back into the stock for reissue?
Yes No
If yes
67. 1, what is the total number of units (whole blood or red blood cells) accepted back in
the stock during the reporting period?
67. 2 Are there criteria to receive blood back for stock rotation?
Yes No
Written document or SOP for Criteria or condition indicating under which it will be accepted
and not accepted)

70
68 Do you maintain records of the following: (Please tick as appropriate)
Yes No
[1]Request blood and components for transfusion
[2]Drawing and labelling the pre‐transfusion blood sample
[3]Collecting blood and blood products from the blood bank
[4]Storage of blood and blood products prior to transfusion
[5]Administering blood/components, including patient id check
[6]Monitoring the patient before, during and after the transfusion
[7]Managing and recording transfusion reaction
69 Which of these are available or used as alternatives to blood transfusion?
Yes No
[1]Crystalloids
[2]Colloid
[3]No information available
70 Is there a system for monitoring post transfusion incidence or reactions in the health
facility?
Yes No
[1] system for monitoring post transfusion incidence
[2] system for monitoring post transfusion reactions
71 What was the number of serious adverse transfusion incidents or reactions reported
during the reporting period?
[1] Number of serious adverse transfusion incidents
[2] Number of serious adverse transfusion reactions

71
72 Do the medical records in the facility permit differentiation of blood usages for any of the
following categories of patients requiring multiple transfusions?
Yes No
72 1 If yes, please specify the number of the patients and number of blood, blood
components and blood products transfused in the reporting period.
Condition No of
patients
Whole
blood
Red
Cells
Platelets FFP Crpt
[1] Thalassaemia
[2] Haemophilia
[3] Sickle Cell
Anaemia
[4] Aplastic Anaemia
[5] Haematological
and other
malignancies
[6] Chronic renal
failure
[7] Others
(Specify)…………..
…………………….

72
IN PLACE (Tick) Policy and management at the central administrative level
Yes No
National Policy and coordination
1
Is there a unit within the MoH (or other government department) with responsibility for overseeing blood transfusion activity?
If yes, name of the unit: ___________________
Name of the officer in charge_________________
2 Is there a designated national blood program manager?
3 Is a national quality manager/officer nominated ?
4 Is a national blood donor program manager/officer nominated?
5 Is there a national blood policy?
If yes, Year of adoption_________________________
Please obtain a copy
6 Is there a national strategy or strategic plan?
If yes, has its implementation been initiated?
7 Is there specific national legislation covering safety and quality of blood transfusion?
If yes, obtain the document reference number and a copy.
8 Has the Ministry of Health constituted a national body responsible for policy development and decision making for blood transfusion?
If yes, please provide a list showing the membership of this body.
9 Are there (national) expert panel (s) to advice on technical and medical issues related to transfusion safety, availability and quality?
10 Is there a national reference centre? (Is there a national blood transfusion service?)?
If yes, what was the year of its establishment? ___
11 Has the government delegated any responsibility for NBTS/blood transfusion services to a nongovernmental organization?
If yes, name of the organization(s):‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐,
Roles of the organization (s)‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐
12 Is there a national strategy for the provision of fractionated plasma products?
13 Please indicate how fractionated plasma products are supplied in the country? Please tick. [1] Importing from abroad [2] Fractionation in‐country by the public (not‐for‐profit) sector

73
[3] Contract fractionation by a profit making organization [4] Other, specify
14 Is a specific budget provided for the national blood program?
Are there specific budget line item for
(1) national supervision
(2) training
(3) donor recruitment
(3) equipment maintenance and spare parts
(4) other, please specify
15 Is there a national cost recovery policy/system for the blood centre/blood transfusion services?
If yes, obtain detailed information.
National standards and guidelines
16 Are there national standards/guidelines for: [1] Criteria for assessing the suitability of donors for blood donation [2] Standardized donor interview questionnaire [3] Blood collection [4] Technical specification for blood components [5] Preparation of Blood and Blood components [6]Testing of Blood donated for TTI [7] Storage of Blood and Blood Components [8] Transportation of Blood and Blood Components [9]Issue of Blood [10]Quality management for blood transfusion services
[11]Waste management in blood transfusion services?
[12]Occupational health and hygiene to prevent the transmission of blood borne infections
17
Are there national standards/guidelines for: [1]Clinical indications for transfusion [2]Standardized blood request form [3]Maximums blood ordering schedules (MSBOS) [4]Pre‐transfusion testing [5]Safe Blood administration [6]Transfusion reaction form
Monitoring and Assessment at the National Level

74
18 Is there a system of centralized data collection and analysis for the blood transfusion services in the countries
19.1 If yes, how frequent are the national data collection and analysis conducted?
19 Is scheduled supervision program available for:
(1) blood centre
(2) blood banks in hospitals or other health facilities
When was the latest supervisory visit? What activities are conducted during the supervisory visits?
Is there a standard supervision checklist? If yes, pl provide a copy?
20 Is there a national external quality assessment scheme for blood group serology? If yes, please provide the name of the provider, or how it is provided:________________
21 Is there a national haemovigilance system? If yes, please provide the start year______________ and the number of participating facilities_____________________
22
Mechanism for the regulation of the blood centre/blood transfusion services?
(A) Is there a system for mandatory registration or licensing of blood transfusion services?
(B) Is there a system of regular inspection of the blood transfusion services?
(C) Do the inspectors have specialized training?
(D) Is there a national regulatory authority for blood transfusion services? If yes, name of regulatory authority_____________________________
Equipment and supplies
23 Is procurement of equipment conducted centrally at the national level?
24
Is there a separate budge line item for equipment maintenance and spare parts?
25
Is there a national inventory maintained for equipment and spare parts
26 Is there a national program to evaluate test kits and reagents used for blood transfusion?
If yes, who conducts the evaluation? ________________________

75
Education and training
27 At the national level, is there a program to provide continuing education for personnel involved in blood transfusion?
If yes, obtain more detailed information, such as providers/organizer/fields.
28 During the reporting period, how many national training courses were provided? Please fill in the following tables
Major purpose of the training No. of courses organized
Total No. of participants
[1] Donor education, recruitment, and selection
[2] Blood collection and donor care
[3] Quality management
[4] Laboratory practices and skills relating to blood safety
[5] Processing and component preparation
[6] Cold chain management (storing, handling, transportation)
[7] Transfusion and blood utilization
[8] Blood administration procedures
[9] Bio‐safety and waste management
[10] Blood service management
[11] Others, please specify_____________
29 Are there educational programs in blood transfusion medicine/science leading to a nationally recognized university degree/diploma?

76
ANNEX‐2: List of blood transfusion centres and hospitals surveyed
List of Data Collectors
Dr Md Mumtaz Uddin Bhuiyan, Director hospital, DGHS
Dr MAJ Musa, Deputy Director Planning, DGHS
Dr Md. Mazharul Hoque, Assistant professor, DPM SBTP
Dr Lutfor Kabir, Deputy Director, Hospital DGHS
Dr Md Alamgir Ahmed, Assistant Director, DGHS
Dr Shamsuzzaman, Assistant Director, DGHS
Dr Md Nazmul Haque, Assistant Director
Dr Aminul Hassan, DPM BAN BCT, DGHS
Dr Masum, DPM, DGHS
Prof. Dr Husne Ara Begum, Blood Transfusion Department , DMCH, Dhaka
Dr Moon Mon Rahman, Assistant Prof, Blood Transfusion, NITOR, Sher‐e‐Bangladesh Nagar
Dr Hosne Ara, Associate professor, Blood Transfusion Dept., DMCH, Dhaka
Dr Munshi Md Habib Ullah, Associate prof., Blood Transfusion, SSMC, Dhaka
Dr Zereen Mosfeqa Rahman, Blood Transfusion, NICVD, Sher‐e‐Bangla Nagar, Dhaka
Dr Syeeda Masooma Rahman, Assistant professor, SBTP
Dr Farhana Islam, Blood Transfusion, NIDCH, Mohakhali, Dhaka
Dr Md Khairul Islam, Blood Transfusion NITOR, Sher‐e‐Bangla Nagar, Dhaka
Dr Sheikh Daud Adnan, Assistant Prof Blood Transfusion, NICVD, Dha
Dr Mizanur Rahman, Assistant Professor, Blood Transfusion, SSMC, Dhaka
Dr Zubaida Nasreen, EMO Blood Transfusion, DMCH, Dhaka
Dr Daulatun Nahar, Associate professor, Safe Blood Transfusion Program, DMCH, Dhaka
Dr Md Asadul Islam, Associate Professor, Transfusion Medicine, BSMMU, Dhaka
Md Faruque , Medical Technologist Lab , SBTP
Shakhawat Hossain , Medical Technologist Lab , SBTP
Md Mollah Amirul Islam Medical Technologist Lab , SBTP
Types of surveyed Blood Centres
Centre Type Number of Centres
District Hospital 50
Upazila Health Complex 11
Public Medical College 14
Private Medical College 6
Private Hospital 7
Public Institute 5
Standalone Blood Centre 6
Standalone NGO Blood Centre 2
Others 8
Total 109

77
List of Blood Centres at District Hospital
Sl Name of Centre
1 Adhunik Sadar Hospital, Bagerhat
2 Adhunik Sadar Hospital, Feni
3 Adhunik Sadar Hospital, Kishoregong
4 Adhunik Sadar Hospital, Magura
5 Adhunik Sadar Hospital, Rajbari
6 Adhunik Sadar Hospital, Thakurgaon
7 Barisal Sadar Hospital
8 Chittagong Sadar Hospital
9 General Hospital Noakhali
10 General Hospital, Jamalpur
11 General Hospital, Jessore.
12 General Hospital, Kushtia.
13 General Hospital, Meherpur.
14 General Hospital, Narayanganj.
15 General Hospital, Pabna.
16 General Hospital, Patuakhali.
17 General Hospital, Rangamati.
18 General Hospital, Sirajgonj
19 General Hospital, Tangail.
20 Modernized Sadar Hospital, Jhalokati
21 Mohammad Ali Sadar Hospital, Bogra
22 Sadar Hospital, Bandarban
23 Sadar Hospital, Barguna
24 Sadar Hospital, B‐Baria
25 Sadar Hospital, Bhola
26 Sadar Hospital, Brahmanbaria
27 Sadar Hospital, Chandpur
28 Sadar Hospital, Chapai Nowabgonj
29 Sadar Hospital, Comilla
30 Sadar Hospital, Cox's Bazar
31 Sadar Hospital, Faridpur
32 Sadar Hospital, Gaibandha
33 Sadar Hospital, Gazipur
34 Sadar Hospital, Gopalgonj
35 Sadar Hospital, Habiganj
36 Sadar Hospital, Hobigonj
37 Sadar Hospital, Jhenaidah
38 Sadar Hospital, Jhenaidah
39 Sadar Hospital, Khulna
40 Sadar Hospital, Laxmipur
41 Sadar Hospital, Madaripur
42 Sadar Hospital, Munshigonj

78
Sl Name of Centre
43 Sadar Hospital, Narile
44 Sadar Hospital, Natore
45 Sadar Hospital, Nilphamari
46 Sadar Hospital, Panchagor
47 Sadar Hospital, Sariatpur
48 Sadar Hospital, Satkhira.
49 Sadar Hospital, Sunamgonjl
50 Shahid Shamsuddin Sadar Hospital
51 Blood Banks Quantum Foundation, Dhaka
52 Red Crescent Blood Centre, Dhaka
53 Anser & VDPHospital, Gazipur
54 Azimpur Maternity Hospital Dhaka
55 BBF Hospital, Peelkhana Dhaka
56 CMH, Bogra Cantonment, Bogra.
57 CMH, Chittagong Cantonment, Chittagong.
58 CMH, Comilla Cantonment, Comilla.
59 CMH, Rangpur Cantonment, Rangpur.
60 Port authority Hospital
61 AFIP, Dhaka Cantonment, Dhaka
62 National Institute of Cancer Hospital Dhaka
63 National Institute of kidney Hospital Dhaka
64 NIDCH, Mohakhali, Dhaka
65 IC& MH Matuil Dhaka
66 Chittagong Medical College Hospital, Chittagong
67 Comilla Medical College Hospital, Comilla.
68 Dhaka Medical College Hospital, Dhaka
69 Dinajpur Medical College Hospital, Dinajpur
70 Faridpur Medical College Hospital, Faridpur
71 Khulna Medical College Hospital, Khulna
72 MAG Osmani Medical College Hospital, Sylhet
73 Mymensingh Medical College Hospital, Mymensingh
74 Rajshahi Medical College Hospital, Rajshahi
75 Rangpur Medical College Hospital, Rangpur
76 S.Sh.Medical College Hospital, Sher‐e‐Bangla Nagar, Dhaka
77 Shaheed Ziaur Rahman Medical College Hospital, Bogra
78 Sher‐e‐Bangla Medical College Hospital, Barisal
79 Sir Salimullah Medical College Hospital
80 Ad‐din Hospital
81 Appolo Hospitals
82 Dhaka Shishu Hospital
83 Lab Aid Hospital
84 National Heart Foundation Hospital Dhaka
85 Square Hospital

79
Sl Name of Centre
86 United Hospital, Dhaka
87 Bangladesh Medical College Hospital Dhaka
88 BIRDEM Hospital, Dhaka
89 Holy family Red Crescent Medical College Hospital
90 Kwaza Younis Ali Medical College
91 National Medical College Hospital, Dhaka
92 Sikder Womens Medical College and Hospital, Dhaka
93 Brati Blood Bank Chata Kalibari, Ankur, Tangail
94 Crossmatch Blood Centre, Dhaka
95 Dhaka City Blood Bank and transfusion Centre, Dhaka
96 Fatema memorial Diagnostic Medical Services, Dhaka
97 New Save Life Blood Bank and Diagnostic Centre, Comilla
98 Shebika Blood Bank, Dhaka
99 Bheramara Upazila Health Complex
100 Borolekha Upazila Health Complex, Moulivi Bazzar Sylhet
101 Chaugasha UHC
102 Fakirhat UHC, Bagherhat, Khulna
103 Gurudashpur Upazila Health Complex
104 Kolapara UHC
105 Loha Gora UHC
106 Parshuram Upazila Health Complex
107 Patnitala UHC
108 Sakhipur Upazila Health Complex
109 Shibgonj Upazila Health Complex
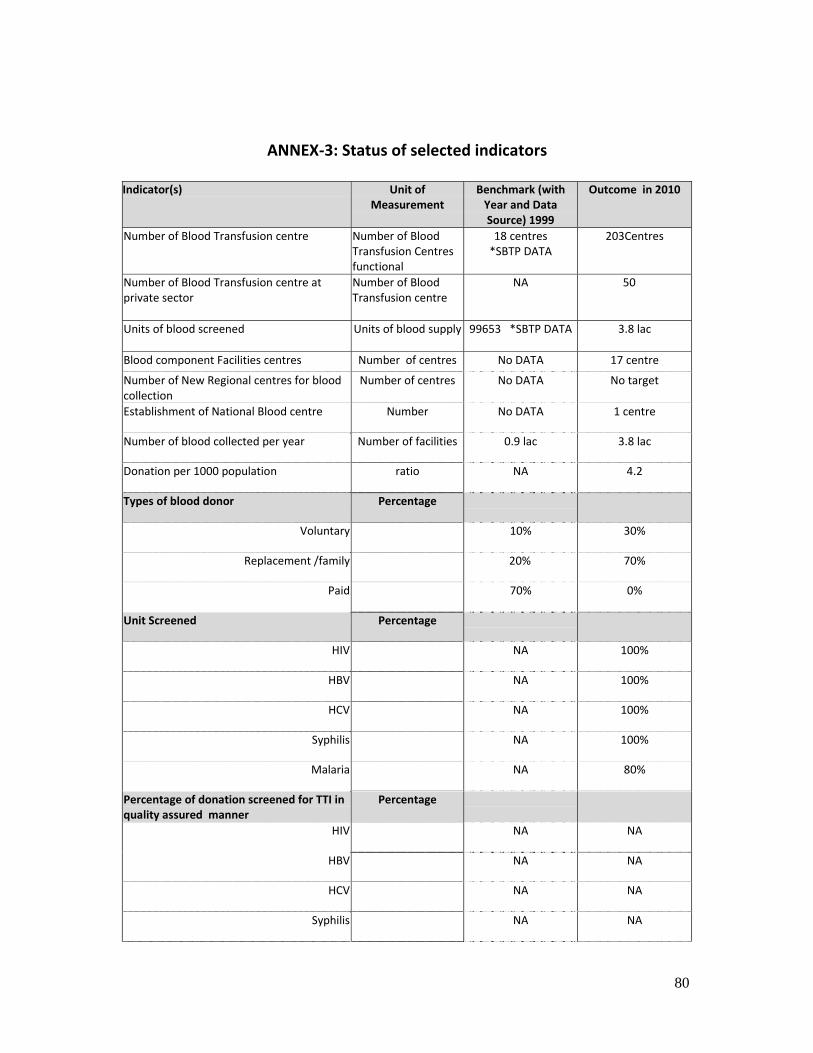
80
ANNEX‐3: Status of selected indicators
Indicator(s) Unit of
Measurement Benchmark (with Year and Data Source) 1999
Outcome in 2010
Number of Blood Transfusion centre Number of Blood Transfusion Centres functional
18 centres *SBTP DATA
203Centres
Number of Blood Transfusion centre at private sector
Number of Blood Transfusion centre
NA 50
Units of blood screened
Units of blood supply 99653 *SBTP DATA 3.8 lac
Blood component Facilities centres Number of centres No DATA 17 centre
Number of New Regional centres for blood collection
Number of centres No DATA No target
Establishment of National Blood centre Number No DATA 1 centre
Number of blood collected per year Number of facilities 0.9 lac 3.8 lac
Donation per 1000 population ratio NA 4.2
Types of blood donor Percentage
Voluntary 10% 30%
Replacement /family 20% 70%
Paid 70% 0%
Unit Screened Percentage
HIV NA 100%
HBV NA 100%
HCV NA 100%
Syphilis NA 100%
Malaria NA 80%
Percentage of donation screened for TTI in quality assured manner
Percentage
HIV NA NA
HBV NA NA
HCV NA NA
Syphilis NA NA

81
Malaria NA NA
Prevalence of TTI in blood donation Percentage
HIV NA 0.002%
HBV NA 0.862%
HCV NA 0.097%
Syphilis NA 0.047%
Malaria NA 0.01%
Percentage of units discarded due to TTI Percentage NA 0.99%
Number of staff trained on national standard , guidelines, algorithm and SOPs on screening of blood for TTI
Number NA NA

82
ANNEX‐4: Table of selected health and socio‐economic indicators
Name of indicator Source
A. ADMINISTRATION
Division 7 Bangladesh
City corporation 9 datasheets
Metropolitan city 4
Municipality 308
District 64
Upazila 483
Union 4,501
Ward 40,509
Village (approximately) 87,310
Household 25,490,822
B. EDUCATION and ECONOMY
Per capita GDP (in US$) 2010‐11 664
GDP growth rate (%) 2009‐10 6
Bangladesh Economic Review 2010
C. DEMOGRAPHY
Total 142. 32 BBS 2011
Male 71. 26
Population (in million) (2011 Census)
Female 71. 06
D. HEALTH STATUS
Infant mortality rate (per 1000 live
births)
39 SVRS 2009,
BBS
Maternal mortality ratio (per
100,000 live births)
194 BMMS 2010
Neonatal mortality rate (per 1,000
live births)
28 SVRS 2009,
BBS
E. HEALTH SERVICES PROVISION
Government hospitals at Upazila 463 DGHS 2011
Government hospitals of secondary 120
Total no. of government hospitals 583
No. of non‐government hospitals
(Regd. by DGHS)
2,501
No. of beds in MOHFW
(functioning)
39,639

83
Name of indicator Source
No. of beds in private sector (Regd.
by DGHS)
42,237
No. of registered physicians 53,063 BMDC 2011
Estimated no. of doctors available
in the country
43,537
Doctors working under MOHFW 38%
Doctors working under other org. 3%
HRD Data
Sheet 2011
Health Bulletin 2011, Page‐5