Sittitavornwong_2009_Seminars-in-Orthodontics
27
Evaluation of Obstructive Sleep Apnea Syndrome by Computational Fluid Dynamics Somsak Sittitavornwong, Peter D. Waite, Alan M. Shih, Roy Koomullil, Yasushi Ito, Gary C. Cheng, and Deli Wang The amelioration of obstructive sleep apnea syndrome (OSAS) by maxilloman- dibular advancement (MMA) surgery can be predicted by analyzing anatomical airway changes with 3-dimensional (3D) geometrical reconstruction and com- putational fluid dynamics. Computer Enabling Technology Lab (ETLab) and Computational Simulation Lab (CSLab) can be used to analyze anatomic airway change for previously operated patients with a clinical cure of OSAS. MMA surgery reduces airway resistance and pressure effort (gradient) of OSAS by increasing the dimension of the airway. ETLab has been used to reconstruct the upper airway as a 3D computer model (bone and soft tissue surrounding the pharyngeal airway) from existing helical computed tomography scan format of OSAS patients. ETLab can compare and construct the geometry with numerical meshes of the airway between pre- and postoperative MMA by the use of bioengineering software. This technology uses high-fidelity computation fluid dynamic simulations, developed at the CSLab, for prediction and analysis of the flow field in the airway for pre- and postoperative MMA. It is possible to use the simulation to predict the likely success of future treatment and develop a prognostic factor. The soft- and hard-tissue mesh is used to determine the pre- and postoperative differences in the facial and pharyngeal tongue base for soft-tissue change associated with hard-tissue movement. This correlation predicts the amount of surgical movement necessary to create an adequate airflow. These results help define the surgical techniques in OSAS for more precise identification of upper airway anatomical features. This process corre- lates the area and pressure change at the velopharynx, oropharynx, and retro- glossal space of the upper airway by the ETLab. Results can compare with polysomnogram and cure rates. 3D computer analysis can be used to test flow dynamics in the human airway for surgical treatment of OSAS. (Semin Orthod 2009;15:105-131.) Published by Elsevier Inc. O bstructive sleep apnea syndrome (OSAS) is one of the most common sleep disorders 1 which is an important public health problem. 2-7 The syndrome is now recognized as being very prevalent, and current epidemiologic data indi- cates that sleep apnea syndrome is second only to asthma in the prevalence league table of chronic respiratory disorders. 8 Furthermore, there is increasing evidence that sleep apnea syn- drome is associated with a considerable number of adverse sequelae, both behavioral and physical. Behavioral consequences include daytime sleep- iness, impaired concentration, and neuropsy- chological dysfunction, whereas physical conse- Department of Oral and Maxillofacial Surgery, The University of Alabama at Birmingham, Birmingham, AL (S.S., P.D.W.). Department of Mechanical Engineering, The University of Ala- bama at Birmingham, Birmingham, AL (A.M.S., R.K., Y.I., G.C.C.). Department of Hematology and Oncology, The University of Ala- bama at Birmingham, Birmingham, Alabama (D.W.). Address correspondence to Deli Wang, PhD, Hematology and Oncology, The University of Alabama at Birmingham, Birmingham, AL; E-mail: [email protected] Published by Elsevier Inc. 1073-8746/09/1502-0$30.00/0 doi:10.1053/j.sodo.2009.01.005 105 Seminars in Orthodontics, Vol 15, No 2 (June), 2009: pp 105-131
-
Upload
roberto-rinaldi -
Category
Documents
-
view
219 -
download
5
description
Somsak Sittitavornwong, Peter D. Waite, Alan M. Shih, Roy Koomullil, Yasushi Ito, Gary C. Cheng, and Deli Wang 105 Seminars in Orthodontics, Vol 15, No 2 (June), 2009: pp 105-131 106 Sittitavornwong et al After several decades of computer development, computer-aided engineering (CAE) has become a matured technology that plays an important role in the engineering community for design, 107 Evaluation of OSAS by Computational Fluid Dynamics 108 Sittitavornwong et al
Transcript of Sittitavornwong_2009_Seminars-in-Orthodontics

ESSY
o
b
b
OA
valuation of Obstructive Sleep Apneayndrome by Computational Fluid Dynamics
omsak Sittitavornwong, Peter D. Waite, Alan M. Shih, Roy Koomullil,asushi Ito, Gary C. Cheng, and Deli Wang
The amelioration of obstructive sleep apnea syndrome (OSAS) by maxilloman-
dibular advancement (MMA) surgery can be predicted by analyzing anatomical
airway changes with 3-dimensional (3D) geometrical reconstruction and com-
putational fluid dynamics. Computer Enabling Technology Lab (ETLab) and
Computational Simulation Lab (CSLab) can be used to analyze anatomic airway
change for previously operated patients with a clinical cure of OSAS. MMA
surgery reduces airway resistance and pressure effort (gradient) of OSAS by
increasing the dimension of the airway. ETLab has been used to reconstruct the
upper airway as a 3D computer model (bone and soft tissue surrounding the
pharyngeal airway) from existing helical computed tomography scan format of
OSAS patients. ETLab can compare and construct the geometry with numerical
meshes of the airway between pre- and postoperative MMA by the use of
bioengineering software. This technology uses high-fidelity computation fluid
dynamic simulations, developed at the CSLab, for prediction and analysis of the
flow field in the airway for pre- and postoperative MMA. It is possible to use the
simulation to predict the likely success of future treatment and develop a
prognostic factor. The soft- and hard-tissue mesh is used to determine the pre-
and postoperative differences in the facial and pharyngeal tongue base for
soft-tissue change associated with hard-tissue movement. This correlation
predicts the amount of surgical movement necessary to create an adequate
airflow. These results help define the surgical techniques in OSAS for more
precise identification of upper airway anatomical features. This process corre-
lates the area and pressure change at the velopharynx, oropharynx, and retro-
glossal space of the upper airway by the ETLab. Results can compare with
polysomnogram and cure rates. 3D computer analysis can be used to test flow
dynamics in the human airway for surgical treatment of OSAS. (Semin Orthod
2009;15:105-131.) Published by Elsevier Inc.
OwTpctctdaBi
Department of Oral and Maxillofacial Surgery, The Universityf Alabama at Birmingham, Birmingham, AL (S.S., P.D.W.).
Department of Mechanical Engineering, The University of Ala-ama at Birmingham, Birmingham, AL (A.M.S., R.K., Y.I., G.C.C.).
Department of Hematology and Oncology, The University of Ala-ama at Birmingham, Birmingham, Alabama (D.W.).
Address correspondence to Deli Wang, PhD, Hematology andncology, The University of Alabama at Birmingham, Birmingham,L; E-mail: [email protected]
Published by Elsevier Inc.1073-8746/09/1502-0$30.00/0
cdoi:10.1053/j.sodo.2009.01.005
Seminars in Orthodontics, Vol 15, N
bstructive sleep apnea syndrome (OSAS) isone of the most common sleep disorders1
hich is an important public health problem.2-7
he syndrome is now recognized as being veryrevalent, and current epidemiologic data indi-ates that sleep apnea syndrome is second onlyo asthma in the prevalence league table ofhronic respiratory disorders.8 Furthermore,here is increasing evidence that sleep apnea syn-rome is associated with a considerable number ofdverse sequelae, both behavioral and physical.ehavioral consequences include daytime sleep-
ness, impaired concentration, and neuropsy-
hological dysfunction, whereas physical conse-105o 2 (June), 2009: pp 105-131

qpahcpv
whpasapdoporeTi
utlhlTcablct
(tmtsabdanat
oa
tpantpt
sahosiwMdmsprw
tOac(TtaiMsstloisaatatm
fors
106 Sittitavornwong et al
uences include cardiovascular disorders,articularly hypertension. The combination ofcute and chronic hemodynamic effects in OSASave been associated with increased risk of myo-ardial infarction, cerebrovascular accidents, hy-ertension, congestive heart failure, and motorehicle crashes.4,9-16
Population-based studies suggest that 2% ofomen and 4% of men older than 50 years of ageave symptomatic obstructive sleep apnea.17 Ap-roximately 1 in 5 adults has at least mild OSASnd 1 in 15 adults has OSAS of moderate or worseeverity.7 The prevalence of OSAS increases withge, with a 2-to 3-fold greater prevalence in olderersons (�65 years) compared with those in mid-le age (30 to 64 years).7 It is estimated that 98%f adults with OSAS lack a specific upper airwayathology of an obstructing nature, such as benignr malignant neoplastic lesions originating in pha-yngeal structures or inflammatory or metabolicnlargement of pharyngeal soft tissue structures.18
his disorder is associated with significant morbid-ty and even some mortality.19
Various surgical procedures for OSAS includevulopalatopharyngoplasty, laser midline glossec-omy and lingualplasty, inferior sagittal mandibu-ar osteotomy and genioglossal advancement withyoid myotomy and suspension, maxillomandibu-
ar osteotomy and advancement, and tracheotomy.hese surgical procedures for OSAS are aimed atreating more space in the breathing airway. Theyre not indicated for central apneas or hypopneasecause the underlying pathophysiology is more
ikely to be related to abnormalities of chemore-eptor function and central control mechanismshan to obstruction of the upper airway.
Bixler et al20 stated that central sleep apneaapnea caused by episodic pauses in respira-ory effort rather than airway collapse) is found
ost often in the older age group. In view ofhis consideration, nocturnal assessment of re-piratory and sleep parameters is essential for
proper evaluation of existing sleep-relatedreathing disorders21 before surgery. Full car-iorespiratory polysomnography (PSG) allowscomplete evaluation to determine whether
octurnal respiratory disturbances are associ-ted with upper airway obstruction or are cen-ral in nature.
Many studies have shown that nasal continu-us airway pressure (nCPAP) therapy is highly
ccepted (35-80% of users).22,23 Unfortunately, ahe long-term compliance with nCPAP is re-orted in the literature to be poor.24 Surgeryppears to be an effective and adequate alter-ative for those patients who do not want to
olerate nCPAP therapy their entire life or foratients for whom nCPAP is not an optimalreatment due to anatomical abnormalities.22,23
In treating OSAS, it is important to detect theeverity of the disease and site of occlusion in theirway for each patient. Objective testing can beelpful in confirming the diagnosis and excludingther sleep disorders that might be causing theymptoms. Clinical indications for upper airwaymaging are evolving for patients being treatedith dental appliances and upper airway surgery.any studies25-28 have attempted to assess and pre-
ict physical pathologies and outcome of treat-ent for OSAS; however, it is difficult to demon-
trate, predict and compare the anatomy of theharynx in patients with OSAS. This difficulty is aesult of the complex 3-dimensional aspect of air-ay anatomy.
Anatomic abnormalities of the pharynx arehought to play a role in the pathogenesis ofSAS. Upper airway imaging modalities to detect
natomic abnormalities include nasopharyngos-opy, cephalometrics, computed tomographyCT), and magnetic resonance imaging (MRI).hese imaging modalities have been used to study
he effect of respiration, weight loss, dental appli-nces, and upper airway surgery on elimination ormprovement of upper airway obstruction. The
RI and CT allow quantification of the airway andurrounding soft tissue structures in 3 dimen-ions.27,29-46 Upper airway imaging is a powerfulechnique for the study of the mechanisms under-ying the pathogenesis, biomechanics, and efficacyf treatment options in patients with OSAS. Imag-
ng studies provide significant insight into thetatic and dynamic structure, function of the upperirway and soft-tissue structure during wakefulnessnd sleep.37-39,43,44 Unfortunately, it is still difficulto understand and predict pathophysiology of theirway in OSAS; consequently, additional diagnos-ic tests are to needed to guide treatment recom-
endations.High-quality diagnostic imaging can be used
or a clinical predictor in OSAS.47 The authorsf many studies27,28,48-58 have attempted to accu-ately quantify the dimensions, configurations,ites of obstruction, and collapsibility of upper
irways. In recent years, sleeping fiber optic en-
dldsptw
taagtap
MshtpapOthi
ttaasaopd
ptgatTllna1pI9
aOpgp3denigrsp
a2jtletntislOmarbsfcmslwSSthdo
E
Aca
107Evaluation of OSAS by Computational Fluid Dynamics
oscopy has been used as an effective method toocate the obstruction site. However, this proce-ure can be a disturbance to normal sleep and isometimes refused by examinees. Because mostatients prefer radiological examinations rather
han invasive ones, radiology could be an idealay to locate the obstructive site in OSAS.27,33,59
Mueller’s maneuver is a diagnostic techniqueo detect airway narrowing. It is performed byttempting to inhale against pinched-off nosend closed mouth with a fiberoptic nasopharyn-oscope in place. The resulting negative inspira-ory pressure will cause the walls of the upperirway to collapse in the narrowed airway. Aositive test is suggestive of OSAS.
Terris, et al60 explored the reliability of theueller’s maneuver and found that the severity of
leep-disordered breathing based on the apneaypopnea index (AHI) is correlated positively with
he Mueller’s maneuver. Hsu et al47 used a com-uter-assisted quantitative video endoscopic upperirway analysis to compare static and dynamic up-er airway morphology between patients withSAS and normal subjects. With this technology,
hey were able to predict which patients wouldave OSAS and confirmed the Mueller test find-
ngs.47
The upper airway begins at the nose and ends athe larynx. Therefore, a complete assessment ofhe upper airway evaluates the entire length of thisnatomic region, including the bony frameworknd soft tissue. Although office assessment of thesetructures does not necessarily mimic the appear-nce of behavior of these structures during physi-logical sleep, the office examination can give im-ortant information as to the site of obstructionuring sleep that can help direct therapy.61
Li et al52 stated the value of 3D-CT scan inroviding the surgeon with anatomic informa-
ion relevant in planning the upper airway sur-ery and monitoring its outcome. The geometrynd caliber of the upper airway in apneic pa-ients differs from those in nonapneic ones.62
he apneic airway is smaller and is narrowedaterally. Oda et al56 evaluated the pharyngo-aryngeal region with 3D-CT in the OSAS andon-OSAS patient. The volume of the upperirway changed mildly between 9.2 cm3 and1.56 cm3 in the expiration and inspirationhase in a non-OSAS individual while sleeping.t fluctuated moderately between 3.74 cm3 and
.91 cm3 in a habitual snorer and changed rcutely between 2.73 cm3 and 16.01 cm3 in anSAS patient. As anatomic abnormalities of theharynx are thought to play a role in the patho-enesis of OSAS, Li et al52 stated that the retro-alatal space is the most relevant upper airwayD-CT scan parameter identified in sleep disor-ered breathing patients and the decreased lat-ral dimension of the retropalatal space is sig-ificantly associated with a compromised airway
n sleep-disordered breathing subjects. After sur-ery the increased lateral dimension of the ret-opalatal space is thought to be one of the rea-ons for the decrease in AHI found duringostoperative polysomnographic studies.
Schwab et al62 used MRI to study the upperirway and surrounding soft-tissue structures in1 normal subjects, 21 snorer/mild apneic sub-
ects, and 26 patients with OSAS. They reportedhat at minimum airway area, thickness of theateral pharyngeal muscular walls, rather thannlargement of the parapharyngeal fat pads, washe predominant anatomic factor causing airwayarrowing in apneic subjects. The fat pad size at
he level of the minimum airway was not greatern apneic than normal subjects. Shintani et al58
uggested dynamic MRI is useful to detect theevel of occlusion during sleep and the severity of
SAS and that this detection can assist in treat-ent. In addition, they found the severity of AHI
nd oxygen saturation (SpO2) are significantly cor-elated with the width of the airway space at thease of the tongue and hypopharynx. By usingtatistic pressure-area relationships, Isono et al38
ound that the passive pharynx is more narrow andollapsible in sleep-apneic patients than inatched controls. This is consistent with the other
tudies.58,63 The retropositioned mandible will al-ow the tongue to impinge on the pharyngeal air-ay and decrease the air flow during sleep.hintani et al58 reported the severity of AHI andpO2 are significantly correlated with the width ofhe airway space at the base of the tongue andypopharynx. Therefore, AHI and SpO2 can pre-ict and interpret the outcomes of pre- and post-perative OSAS.
ngineering Background
fter several decades of computer development,omputer-aided engineering (CAE) has becomematured technology that plays an important
ole in the engineering community for design,

adpmppdangrpudmovflbcsm
hnfiedBngarTeglriamfftcmsfN
tm
gpBgfiompmfemmcttteqFsmststTce
gebwmLtatshmhaad
sfCt
108 Sittitavornwong et al
nalyses, and performance predictions.64,65 Theevelopment is especially significant during theast 2 decades when computer hardware perfor-ance-cost ratio has increased constantly. This
rovides the computational engineers with com-uting resources that was unimaginable just aecade ago. The enabling technologies associ-ted with CAE involve the scientific disciplines ofumerical geometry modeling, numerical mesheneration, scientific visualization, virtual envi-onment technology, and high-performancearallel computing. They enable the use of sim-lation disciplines such as computational fluidynamics (CFD) and computational structureechanics (CSM), which use numerical meth-
ds to solve the governing equations that pro-ide high-fidelity computational simulations ofuid flow transport phenomena and structureehaviors.66 Such computational technologiesan benefit the medical communities in under-tanding hemodynamics and mechanics of hu-an biological systems as well.65,67
To enable these computational technologies,owever, the first step is to generate high-qualityumerical meshes while maintaining geometrydelity. There have been many numerical geom-try algorithms presented during the past fewecades, such as the cubic spline, Hermit spline,ezier spline, and B-spline.68 Among them, theon-uniform rational B-spline (NURBS) hasained great popularity in the CAE communitynd is the de facto industry standard for theepresentation and design of a geometry.69
here are major benefits of representing geom-try in NURBS. First, NURBS retains the strongeometrical properties, such as the convex hulls,ocal control, and affine maps (invariant underegular geometrical transformation, such as scal-ng, rotating, and translating). NURBS provides
unified mathematical basis and can representany analytic geometries accurately. NURBS
ormulations for curves and surfaces can beound in many publications. However, most ofhe applications associated with mesh-basedomputational technologies are mainly 3D volu-etric applications. Therefore, we not only de-
cribe NURBS formulations in curves and sur-aces, but also demonstrate applications usingURBS volumetric formulations.70
Mesh generation is a step preceeding compu-ational simulations. It is important to have
eshes of high quality while maintaining high n
eometry fidelity so the numerical simulationrocess can be steady, robust, and accurate.ased on the numerical algorithms, the mesheneration techniques generally can be classi-ed into either structured, unstructured, hybrid,r generalized meshes.71-73 For these types ofeshes, major algorithms, such as elliptic, hy-
erbolic and algebraic methods for structuredeshes, Delaunay, and advancing front methods
or unstructured meshes, have been publishedxtensively. Delaunay triangulation is a mathe-atical and geometrical technique used toodel 3D structures. The mesh generation pro-
ess for a complex configuration, however, is stillime-consuming and challenging. Particularly,he quality of meshes plays an essential role inhe computational simulations as it affects thefficiency in convergence and accuracy. Low-uality elements induce numerical errors.71
or a complex configuration, it might take sub-tantial effort and time to create high-qualityeshes. This is especially true when applying
tructured mesh topology for complex geome-ry. The flexibility of unstructured meshes is es-ential for 3D complex geometry to shortenurnaround time in a design or analysis process.herefore, unstructured meshes in this study be-ause the geometry of the upper airway is inher-ntly complex.
The enabling and computational technolo-ies have proven track records in sophisticatedngineering applications to demonstrate theirenefits in revealing the physical phenomenaithout trial and error and expensive experi-ents.74-78 The Computer Enabling Technologyab (ETLab) and CFD79 enable all capabilities
o enhance the innate abilities in both physicalnd mental realms to participate in certain ac-ivities. In physiology and medicine, some re-earchers80-82 tried to simulate the airflow in theuman respiratory system and found significantedical implications and applications. The CAE
as enabled surgeons to characterize the staticnd dynamic morphology of the subjects’ upperirway and to derive reliable indicators to pre-ict OSAS.55,83
In view of these considerations, the OSAStudy model and airway simulation could be per-ormed by the collaboration of the ETLab andSLab. These study applications can greatly help
he medical community to understand the dy-
amics and behaviors of a human body as well as
dCcdm
P
OpmrcsgaOcq(aTmfamTavdntahs
datypstsirimoppt
TlaEatvpiit
fmrstcblmpattrcsCtdlfahqcaln
ivntsorosf
109Evaluation of OSAS by Computational Fluid Dynamics
esign a medical treatment. This technique usesFD to predict the presence, severity, and out-omes of OSAS by the use of CT scans and PSGata of adult OSAS patients who underwentaxillomandibular advancement (MMA).
reliminary Studies
ur previous studies30,36,84-87 have reviewed theathophysiologic nature of OSAS and its currentanagement. By standard treatment and our
eviews, the examination should begin with cal-ulation of the body mass index (BMI) and mea-urement of the neck size. A neck circumferencereater than 17 inches is highly correlated withpnea.88 It has been shown that patients withSAS have a shorter cranial base and a smaller
ranial base flexure angle. Sleep apneics fre-uently have a cranial base length of 76.5 mmnormal, 83.3 mm) and a cranial base flexurengle of 122 degrees (normal, 129 degrees).36,89
hese measurements may cause airway impinge-ent and obstruction. Clinicians should care-
ully examine all aspects of the nose and evalu-te any septal deviation, turbinate hypertrophy,asses, polyps, or collapse of the nasal valve.90
he oral examination should document tonguend palate size. Normally, the uvula should beisible with phonation. A long palate is one thatescends below the base of the tongue and can-ot be directly seen. Such a palate may be rela-
ive in macroglossia and further compromise theirway. The nasal pharynx, oral pharynx, andypopharynx can best be evaluated by endo-copic pharyngoscopy.
The goals of upper airway examination areirected at identification of traditional sitesnd causes of obstruction—tonsils, ectopichyroids, radiation fibrosis, vocal chord paral-sis, and lymphoma.90 One should also try toredict the site of obstruction during sleep,uch as retrognathia, which allows the tongueo fall backward during supine sleep and ob-truct the airway. Another important goal is todentify areas in which surgery might reduceesistance, increase size, or decrease collaps-bility of the airway. Rational surgical treat-
ent should be directed at eliminating thebstruction without creating functional im-airment. Because nasopharyngoscopy is im-ortant in the evaluation of the upper airway,
he Mueller maneuver should be performed. lo reiterate a positive Mueller’s maneuver isateral collapse of the airway when the patientttempts to inhale with the nose obstructed.91
ndoscopy can easily evaluate the shape of theirway at various locations. Retroposition ofhe mandible and tongue will produce a trans-erse airway that is diminished in the anteriorosterior dimension.92 Nasal obstruction by
tself is seldom the cause of OSAS, but it canncrease negative pharyngeal pressure, leadingo obstruction and collapse.93
Assessment of the upper airway can be per-ormed by physical examination, endoscopy,
anometry, computed tomography, magneticesonance imaging, acoustic reflection, andomnofluoroscopy, but cephalometric evalua-ion provides a simple, inexpensive, readily ac-essible, and valuable method of screening. Theenefits of cephalometry are its allowance of
ongitudinal comparison over time and treat-ent and its allowance of the comparison of
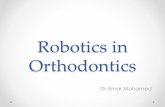
opulations.94 It is also useful for measuringirway changes in a patient before and afterreatment. Waite et al84,87 performed compara-ive preoperative and postoperative cephalomet-ic radiographs after MMA surgery, and clini-ians can easily see a dramatic increase in theize of the posterior airway space (Fig 1).hanges in the posterior airway space are
hought to increase the pharyngeal volume andecrease the airway resistance. However, cepha-
ometric radiographs are not the best methodor evaluating the pharyngeal air space. Therere patients with severe apnea who appear toave a normal cephalometric analysis and ade-uate posterior airway spaces. The limitations ofephalometry are that it is only 2-dimensionalnd not dynamic. It is not yet possible to calcu-ate the amount of MMA needed to create theecessary change in the posterior airway space.
There are examples in our study87,95,96 of anncrease in normal airway space because of ad-ancement surgery and the elimination of ap-ea. Because surgery is a major modality in the
reatment of OSAS and because MMA has beenhown to be one of the most effective surgicalptions, we have continued and observed theesponses of our treatment in OSAS patients. Inur previous study of OSAS in 20 consecutiveubjects undergoing MMA, we used the CT scansor pre- and postoperative evaluation. We ana-
yzed preoperative and postoperative scans by
mwt1Ttla
tbaicceal
Fsahm
FscsvsmN
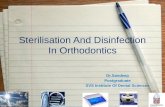
Figure 2. Method for measurements of the (A) a
110 Sittitavornwong et al
easuring the anteroposterior and lateral air-ay dimensions (Fig 2) starting at the level of
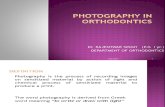
he hard palate (level 1) and then caudally every0-mm until the level of the hyoid bone (levels 8).here are significant enlargements in anteropos-
erior and lateral dimension (Figs 3 and 4) at allevels except level 4 in anteroposterior dimensionnd level 8 in lateral dimension (P � 0.05).
During MMA surgery, muscles, ligaments andendons attached to the jaw are not detachedut equally advanced and straightened with thedvancement of their bony origins. This resultsn a modification of pharyngeal and palatal mus-les, as well as the lingual and suprahyoid mus-les. Within the pharynx, skeletal expansion andnlargement of the pharyngeal soft-tissue tube ischieved. The effectiveness of MMA is mostikely a combination of a change in tension in
igure 3. Change in anteroposterior airway dimen-ions starting at the level of the hard palate (level 1)nd then caudally every 10 mm until the level of theyoid bone (level 8). There are significant enlarge-ents at all levels except level 4.
igure 1. Superimposed cephalometric tracing showskeletal advancement of maxilla and mandible with in-rease in size of posterior airway. Reprinted with permis-ion from Waite PD, Shetter SM: Maxillomandibular ad-ancement surgery: A cure for obstructive sleep apneayndrome. In: Waite PD, ed. Oral and Maxillofacial Treat-ent of Obstructive Sleep Apnea. Maxillofac Surg Clinorth Am 7:327-336, 1995.
nteroposterior and (B) lateral of the airway.

tetAottMiasTaiefmotag
smp
tttomsrcsvwavtts
O
T
AgmScOn
Fic(l
T
�oAM
111Evaluation of OSAS by Computational Fluid Dynamics
he suprahyoid and velopharyngeal muscles,ven if the mechanical enlargement of the pos-erior airway space contributes to that effect.dvancement of the maxilla pulls the soft tissuef the palate forward and upward. It also pullshe palatoglossal muscles forward and increasesongue support. Waite et al87,95,96 found that
MA enlarges the entire velopharynx by elevat-ng the tissues attached to the maxilla, mandible,nd hyoid and results in increased tension onuprahyoid and velopharyngeal musculature.hese studies shows airway enhancement in thenteroposterior and lateral dimensions as antic-pated by forward advancement of the facial skel-ton.87,95,96 This confirms that MMA is very ef-ective because it increases the upper airway at
ultiple levels. This mechanism, as proposed bythers,57,97,98 is consistent with our finding thathe geometry of the airway changes remarkablyfter MMA. Subsequently, investigations have be-un to evaluate the changes in the posterior airway
igure 4. Change in lateral airway dimensions start-ng at the level of the hard palate (level 1) and thenaudally every 10 mm until the level of the hyoid bonelevel 8). There are significant enlargements at allevels except level 8.
able 1. Long-Term Mean Results for MMA with OS
Parameters Measured Preoperative
Mx. advance 102.1 mmMd. advance 118.8 mmPAS 8.6 mmBMI 32.5kg 96.6AHI 44.3Arousal index 31.3Desaturation events � 90% 114Longest event 50 sLow oxygen 72%Total obstructive hypopnea 120
, change; Mx., maxilla; Md., mandible; PAS, posterior airwxygen desaturations � 90%. Reprinted with permission from
cure for obstructive sleep apnea syndrome. In: Waite PD, ed. Oraxillofac Surg Clin North Am 7:327-336, 1995.pace by 3D MRI.62 Again, it appears that advance-ent of the tongue and widening of the lateral
illars occurs with mandibular advancement.Waite et al96 found significant correlation of
he results, such as AHI, arousal index, desatura-ion events �90%, longest event, low oxygen, andotal obstructive hyponea between pre- and post-perative MMA for 16 OSAS patients at 5 to 39onths after surgery (Table 1). All these results
upport MMA treatment and can be used for indi-ect interpretation of the outcome. MMA is suc-essful because it enlarges the posterior airwaypace at multiple levels which are generally in-olved in cases of apnea. Maxillary advancementill flare the alar base, open the nasal valve, anddvance and support the palate. Mandibular ad-ancement will increase the tongue space, supporthe tongue and pull it forward, and preventongue impingement on the posterior airwaypace.96
Waite and Shettar96 published a report of 71SAS patients who underwent MMA and received
able 2. Results of MMA for OSAS96
Results AHI DesaturationNumber ofPatients
Percent ofTotal (%)
Excellent � 10 � 0 20 28.2Good � 10 � 20 26 36.6Satisfactory � 20 � 20 15 21.1Poor � 20 � 20 10 14.1
HI, apnea hypopnea index; Desaturation, number of oxy-en desaturations below 90%, n � 71. Reprinted with per-ission from. Reprinted with permission from Waite PD,
hetter SM: Maxillomandibular advancement surgery: Aure for obstructive sleep apnea syndrome. In: Waite PD, ed.ral and Maxillofacial Treatment of Obstructive Sleep Ap-ea. Maxillofac Surg Clin North Am 7:327-336, 1995.
t 5 to 39 Months96
Postoperative � P Value
110.4 mm 8.3 mm � 0.001129.2 mm 10.3 mm � 0.001
16.4 mm 7.8 mm � 0.00431.9 0.6 NS95.0 1.6 NS
9.5 34.8 � 0.0015.5 25.8 � 0.001
15 99 � 0.00226 s 24 s � 0.00188% 24% � 0.0135 85 � 0.01
ace; AHI, apnea hypopnea index; Desaturation, number ofte PD, Shetter SM: Maxillomandibular advancement surgery:
AS a
ay spWai
al and Maxillofacial Treatment of Obstructive Sleep Apnea.

psraswsa
bw4fmvoweTtsamatdo
uifIait
twfl
tcMTWaitvcAnrsdOrm
ttrtrpcsCfgHtsn
SC
(pfta
o
TMC
n*WgPS1
112 Sittitavornwong et al
ostsurgical polysomnography. On the basis of auccess criterion of an AHI less than 10, the cureate was 65%. If an AHI less than 20 is consideredsuccess, the cure rate for MMA is 86%. Table 2
hows the response of OSAS patients who under-ent MMA and also shows that if success is de-
cribed as a AHI of less than 10 then 64.8%chieved at least a good-to-excellent result.
Successful treatment of OSAS by MMA haseen reported by many centers throughout theorld. Waite and Shettar reported on a study96 of2 patients with OSAS. All patients were evaluatedor the purpose of correlating surgical advance-
ent with change in posterior airway space area,olume, and resistance (Table 3). With the previ-usly stated limitations in mind, cephalometricsere obtained preoperatively, immediately postop-ratively, and at least 1 month after the procedure.he length of the airway space was defined from
he lowest point of the pterygoid fissure and ba-ion to a line through C4 and the hyoid bone. Therea of the space was calculated by serial diametereasurements every 5 mm. The volume of the
irway is calculated by (area) � (length). Resis-ance was calculated by (length) � (K constant)ivided by radius.4 The radius is one-half the meanf the total diameter measurements.
In all 42 cases, the airway area (cm2) and vol-me (cm3) enlarged whereas the resistance signif-
cantly decreased. The mean resistance changedrom 28.72 preoperatively to 10.47 postoperatively.t appears that MMA increases the upper airwaynd decreases the resistance. Changes in air flow arenversely proportional to the resistance, and resis-
able 3. Mean Posterior Airway Changes AfterMA for 42 Patients With OSAS Measured byephalometry
Mean mandibular advancement 8.69 mmMean maxillary advancement 7.49 mmMean preoperative length 8.88 mm*Mean postoperative length 8.70 mm*Mean preoperative volume 9.69 mLMean postoperative volume 16.93 mLMean preoperative resistance 28.72Mean postoperative resistance 10.47
� 42.No significant difference. Reprinted with permission fromaite PD, Shetter SM: Maxillomandibular advancement sur-
ery: A cure for obstructive sleep apnea syndrome. In: WaiteD, ed. Oral and Maxillofacial Treatment of Obstructiveleep Apnea. Maxillofac Surg Clin North Am 7:327-336,995.
ance is inversely proportional to the radius raised to a
he fourth power. Therefore, a small change in air-ay diameter produces a significant increase in airow.
There is much evidence that supports MMAreatment for OSAS. Li et al99 reviewed long-termlinical results of OSAS and demonstrated thatMA achieves long-term cure in most patients.his was supported by the study of Nimkarn andaite30 (Table 4). The relatively large maxillary
dvancements observed in these subjects (approx-mately 7.5 mm) seem to be relatively stable overhe long term. In the mandible, the average ad-ancement was approximately 10 mm, with thehin segment being advanced an additional 4 mm.gain, this seemed to be relatively stable with aegligible amount of postsurgical instability occur-ing. The long-term postsurgical position was nottatistically significantly different from the imme-iate postsurgical position for any variable (t test).nly gonion vertical demonstrated a significant cor-
elation between the amounts of surgical advance-ent.The results of this study are of interest because
hey indicate that large surgical advancement ofhe maxilla and mandible in OSAS patients areelatively stable over the long term. The findings ofhis study were supported by Conradt et al.29 Theyeported postoperative success which has beenroven to be stable over a long period (2-year). Inonclusion, MMA is safe and effective and ithould be presented as an alternative option toPAP. When prolonged CPAP maintenance and
ollow-up over a lifetime are considered, sur-ical therapy is also found to be cost effective.owever, the correlation of hard with soft-
issue changes and the airflow in the airwaypace has not been reported because apnea isot a simple problem of tubular physics.
cientific Methodology forFD Study of the Airway in OSAS
Editor’s note: The mathematical and engineeringrinciples in the following are included in an ef-
ort to completely present the rationale for thisechnology. It is understood that it is of limitedpplication for the clinical orthodontist.)
In an effort to develop and test the applicationf computer ETLab in the analysis of the anatomic
irway, the authors created 2 planning steps.
1MR
dafrlrst
hctmpogo
sMip
cfics
poafrwsH
drvdaecsnas
2M
Tprgpc
T
*rps llofac
113Evaluation of OSAS by Computational Fluid Dynamics
) Reconstruction of Facial Geometry andesh (Preprocessor for Geometryeconstruction and Mesh Generation)
Reconstruction of facial geometry from 3D-CTata. All 3D-CT scans of the cases, including pre-nd postoperative MMA, are transformed to sur-ace geometry of the face and airway for the ste-eoscopic models. The anatomical references andandmarks are reidentified on these models. As aesult, it is possible to compare the data of thesetereoscopic models between pre- and postopera-ive MMA.
The changing of facial soft-tissue profile. This stepelps the clinician determine and predict theorrelation of changing surgical bone and softissue after MMA (horizontal advancement of
axilla and mandible). With these numbers ofercent changes between bone and soft tissue,ne can compare the numbers of polysomno-ram (AHI, SpO2, BMI) and interpret for theutcome of correlation.
The changing of upper airway region. With statictereoscopic displays of pre- and postoperativeMA, the alteration of airway dimension (select-
ng area, volume) of the airway are recorded, com-ared, and correlated with the polysomnograms.
On the basis of our previous study, many of theases had an AHI greater than 40, which is classi-ed as severe OSAS.36,96 Consequently, severeases are then selected for the CFD simulation
able 4. Surgical Movements and Postsurgical Instab
Landmark Mean Surgical Movement (mm)
PNS horizontal 7.3 � 2.3ANS horizontal 7.4 � 2.0A point horizontal 7.5 � 2.2UIA horizontal 9.0 � 2.9LIA horizontal 10.0 � 2.8B Point Horizontal 9.6 � 2.8Pg horizontal 13.8 � 5.2Me horizontal 11.4 � 5.0Gonion horizontal 5.8 � 3.8PNS vertical 1.1 � 1.4ANS vertical 0.5 � 2.9Mx 1 vertical 0.7 � 2.1Md 1 vertical 2.4 � 3.5Pg vertical 0.3 � 4.5Me vertical 4.0 � 2.5Gonion vertical �1.7 � 3.9
Significant correlation (�0.7 or � �0.7) for the mean suepresents posterior or superior movement and a positive vermission from Nimkarn Y, Miles PG, Waite PD: Maxillyndrome patients: Long-term surgical stability. J Oral Maxi
tudy. Models for dynamic stereoscopic displays of (
re- and postoperative MMA are used for the studyf the airflow simulation. The tidal volume indults which is normally 5 to 7 mL/kg100 is usedor the volume of simulating airflow. The usual I:Eatio100 (inspiration time/expiration time) of 1:2ill be a number for setting stimulation. Peak pres-
ure at the end of inspiration (Ppeak) at � 15 cm2O is monitored.63
The dimension (diameter, area, and volume inifferent levels) of pre-/postoperative airway areecorded and compared using the technology de-eloped by ETLab. The CFD simulations are con-ucted to obtain velocity and impedance of theirflow through various pre-/postoperative geom-tries of upper airway. Impedance in the airwayan be visualized as the opposition to airflow in ainusoidal wave fashion. The correlation of theumber between PSG, dimension of airway, andirflow properties are analyzed with the use oftatistics.
) Visualization of Geometricalesh and Airflow Simulation
he variable numbers of fluid dynamics are theressure gradient (�p), airflow resistance, flowate, volume and diameter of airway at the re-ion of the affected airway level, such as retro-alatal and retroligual areas. These numbers areompared with the number of polysomnogram
of Skeletal Landmarks30
ost-Surgical Instability (mm) T Test Correlation
0.4 � 1.8 0.53 �0.520.7 � 2.2 0.25 �0.57
0.43 � 1.6 0.52 �0.601.1 � 2.0 0.25 �0.46
�0.1 � 2.1 0.95 �0.36�0.7 � 2.9 0.54 �0.08�0.1 � 3.9 0.96 �0.49
0.3 � 3.8 0.87 �0.12�0.7 � 3.8 0.58 �0.50
0.3 � 1.1 0.56 �0.190.0 � 2.2 1.00 �0.550.7 � 1.6 0.35 �0.250.8 � 2.2 0.49 �0.370.3 � 3.6 0.85 �0.451.0 � 2.0 0.25 �0.202.1 � 3.6 0.07 �0.71*
l movements and postsurgical instability, a negative valuerepresents anterior or inferior movement. Reprinted withdibular advancement surgery in obstructive sleep apneaSurg 53:1414-1418, 1995; discussion:1418-1419.
ility
P
rgicaalueoman
AHI, SpO2, BMI) and interpreted for the corre-

lfi
aMfsstt1ttieregmAraa
S
Tse
Cw
114 Sittitavornwong et al
ation outcomes. The postprocessor for the flow-eld visualization, feature extraction are detailed.
To obtain retrospective data. our study chartsre reviewed for OSAS patients who receivedMA surgery. The inclusion criteria were as
ollows: (1) completion of a polysomnographictudy before and a minimum of 6 months afterurgery; (2) a standardized helical CT scan withhe patient’s trago-canthal line perpendicular tohe ground while the end of expiration taken in-month preoperative and 6-month postopera-ive MMA; and (3) a preoperative AHI greaterhan 25 events per hour on attended PSG. PSGs performed with the use of 2-channel electro-ncephalography (EEG; C3-A2, O2-A1), left andight electroencephalogram (EO6), submentallectromyogram, body position, electrocardio-ram, oronasal airflow (nasal pressure of ther-ista) with respiratory events defined by themerican Academy of Sleep Medicine.101 The
eferences of points and lines on facial and neckreas are defined and are used for measurementnd statistical correlations.
election of Anatomic Landmarks
he facial and neck landmarks of the airway areelected and defined mathematically, acknowl-
Figure 5. Facial landmarks of hard tissue.
dged and defined.
Cephalometric Landmarks102
ephalometric landmarks are used in junctionith imaging obtained during CT scanning.
Hard tissue part (Fig 5)
S (sella): the point of sella tursicaNa (nasion): the point of frontonasal sutureCo (condylion): the highest and most poste-
rior point of the mandibular condylePo (porion): the central point on upper bor-
der of external auditory meatusOr (orbitale): the lowest point of the orbitA (subspinale): the most concave point be-
tween the anterior nasal spine (ANS) andmaxillary alveolar process
B (submentale): the most concave point ofmandibular alveolar process
Go (gonion): the lowest and furthermost ofmandibular angle—the half-divided angleof ramus and mandibular plane
ANS: the most anterior of maxilla on thepalatal plane
PNS (posterior nasal spine): the most poste-rior of maxilla on the palatal plane
Pog (pogonion): the most anterior of thechin convexity
Me (menton): the lowest point of the man-dibular symphysis
Gn (gnathion): the lowest and most anteriorpoint of the chin—the half-divided angleof Na-Pg plane and Go-Me plane
Angulations and distance
Hard tissue part (Fig 5)FH-SN: the angle between the
Frankfort horizontal and SNplanes
Co-Gn: the distance from the Co-toGn-points
Co-A: the distance from the Co-toA-points
SN-MP: the angle between the SN andGo-Me planes
Soft-tissue part (Fig 6)
A (glabella): the most prominence of midsag-ittal plane of the forehead
B (eye): the point between the AC plane andperpendicular line of the orbit
C (subnasale): the junction of nasal alar base
and upper lip
Imh
115Evaluation of OSAS by Computational Fluid Dynamics
D (upper vermillion border): the midpoint ofvermillion border of the upper lip
E (stomion): the junction of upper and lower lipsF (lower vermillion border): the midpoint of
vermillion border of the lower lipG (soft-tissue pogonion): the junction of the
perpendicular line from Pog to N-Pog planeH (soft-tissue menton): the junction of the half-
divided angle of N-Pog and Go-Me planeI (throat point): the junction of the chin and
neck lines(UFH) upper facial plane: the plane from the
A-point (glabella) to C-point (subnasale)Lower facial plane (lower facial height [LFH]):
the plane form the C-point (subnasale) toG-point (soft pogonion)
FH: Frankfort horizontal planeSN: Sella-nasion planeMP: Mandibular plane
Soft-tissue part (Fig 6)
NLA (nasolabial angle): the angle betweenthe nasal alar base and upper lip at C-point(subnasale)
FCA (facial contour angle): the angle be-
Figure 6. Facial landmarks of soft tissue.
tween the AC and GC planes
UFH (upper facial height): the distance fromthe eye to the C-point (subnasale), on theAC plane
LFH: the distance from the C-point (subna-sale) to the H-point (soft-tissue menton)on the CG plane
ULL (upper lip length): the distance fromthe C-to E-points on the CG plane
LLL (lower lip length): the distance from theE-to H-points on the CG plane
TL (throat length): the distance from the I(throat point) to H points (soft-tissue men-ton)
LCTA (lip chin throat angle): the angle be-tween the HI and FG planes
Modified Cephalometric Landmarks54
n addition to conventional cephalometric land-arks, modified landmarks are obtained to en-
ance the data quality.Reference landmarks (Fig 7A)
AH: the most anterior and superior point onthe body of the hyoid bone, representingthe inferior part of the tongue
Ba (basion): the most postero-inferior pointon the clivus
pm: Pterygomaxillare: the intersection be-tween the nasal floor and the posteriorcontour of the maxilla
GE: the genial tubercle, representing themost posterior point of the mandibularsymphysis and the anteroinferior part ofthe tongue
V: vallecula, the intersection of epiglottis andthe base of the tongue
T: the tip of the tongueH: the most superior point of the tongue in
relation to the line from V to TLPW: lower pharyngeal wall, intersection of a
perpendicular line from V with the poste-rior pharyngeal wall
MPW: middle pharyngeal wall, intersection ofa perpendicular line from U with the pos-terior pharyngeal wall
U: tip of the uvula, the most posteroinferiorpoint of the uvula
UPW: upper pharyngeal wall, intersection ofthe pterygomaxillare-basion (pm-Ba) line
and the posterior pharyngeal wall
FLpDom
116 Sittitavornwong et al
FH: Frankfort horizontal, the line betweenthe porion (Po) and orbitale (Or)
pm-U: the line between the pm and uvula (U)NL: nasal line, the line between the ANS
igure 7. (A) Landmarks of pharyngeal airway. (B)inear measurements of the pharyngeal airway. Re-rinted with permission from Wolford L, Hilliard F,ugan D: Surgical Treatment analysis in patients withbstructive sleep apnoea syndrome. II. Soft tissueorphology. J Laryngol Otol 103:293-297, 1989.
and pm
Linear measurements (Fig 7B)
V-T: the distance from V to T, tongue lengthH-VT: the perpendicular distance from H to
the line connecting V and T, tongueheight
pm-UPW: the distance from pm to UPW, na-sopharyngeal airway space
U-MPW: the distance from U to MPW, oro-pharyngeal airway space
V-LPW: the distance from V to LPW hypopha-ryngeal airway space
PASmin: the minimal distance between thebase of the tongue and the posterior pha-ryngeal wall, posterior airway space
pm-U: the distance from pm to U, length ofthe soft palate
SPT: the maximal thickness of the soft palatemeasured perpendicular to the pm-U-line
CL: contact length between the dorsal con-tour of the tongue and the soft palate
V-FH: the perpendicular distance from V toFH, the vertical position of vallecula
V-cc: the distance from V to the cervical co-lumna, measured parallel to FH, the hori-zontal position of Vallecula
Angular measurementsNL/pm-U the inclination of the length axis
of the soft palate relative to thenl line
V-T/FH the inclination of the length axisof the tongue relative to the FHline
Volume measurements
TV: volume of tongue—the lower part of thetongue is reduced to a geometrical poly-gon where the boundaries are defined byline segments connecting the followingpoints, V, AH, GE, and T. The upper partof the tongue area is defined as the dorsaland superior contour of the tongue from Vthrough H to T
SPV: volume of soft palate—measures along theanterior and posterior contour of the softpalate. The superior outline is a line throughpm perpendicular to the pm-u-line
OV: oral volume—includes tongue volumeand extends superiorly to the outline ofthe soft and hard palate
OPV: oropharyngeal volume—includes OV and
the area defined by the point pm, UPW,
R
tmrvppssrfqo
1MRTtfibtt
Wmtocaitrltsa
acfmfi
tSvtibdsetTmwraieoatr
F
WcctkTr
117Evaluation of OSAS by Computational Fluid Dynamics
LPW and V along the posterior pharyngealwall and the dorsal outline of the tongue,including the soft palate volume, SPV
atiosTV/OV � Relationship between the tongue
and oral volumeTV/OPV � Relationship between tongue
and the oropharyngeal volumeSPV/OV � Relationship between the soft
palate and oral volumeSPV/OPV � Relationship between soft
palate and the oropharyngeal volume
The pre-/postoperative 3D-CT scans are thenransformed to 3D geometry reconstruction and
esh generation in the next step. The geometryeconstruction and mesh generation is a scientificisualization for high-performance parallel com-uting. The patient’s trago-canthal line is kept per-endicular to the ground at expiration. Thereforeome landmarks of the nonsurgical bones, such askull base and upper-facial third areas are used foreferencing and superimposing. The surgical-af-ected areas, including bone and soft tissue, areuantified and compared between pre- and post-perative MMA.
) Reconstruction of Facial Geometry andesh (Preprocessor for Geometryeconstruction and Mesh Generation)his preprocessing step in numerical simula-
ions is a critical step, because the geometricaldelity and mesh quality can greatly affectoth the convergence of numerical calcula-ions and, more importantly, the accuracy ofhe result.
Reconstruction of Facial Geometry From3D-CT Scan
hen an image dataset is acquired, there can beany factors103,104 that affect its quality other
han the resolution. The noise in the dataset isne of the issues that must be addressed. This issuean be mitigated through the use of mathematicallgorithms on the raw data provided by the imag-ng systems. To use the image data for segmenta-ion and surface extraction, noise can be selectivelyemoved through the careful application of se-ected 3D imaging filters. It is important to keephe use of such filtering to an absolute minimumo the resulting image is as coherent to the original
s possible while attempting to remove only noisend other unneeded information. It has been dis-overed that using a 3D median convolution filterollowed by light 3D Gaussian blur filter removes
ost undesirable noise while still maintaining a highdelity to the original.
To extract the desired geometry of the airway,he 3D image data must then be segmented.urfaces defined by a radical shift in the scalaralues in the image volume are relatively simpleo segment. Examples of these types of surfacesnclude bone boundaries in CT data and theoundary between flesh and air in CT or MRIata. However, this process requires the re-earch team members from both medical andngineering schools to work closely to ensurehat proper surface information are extracted.he National Library of Medicine Insight Seg-entation and Registration Toolkit (ITK; http://ww.itk.org)105 provides many advanced noiseeduction and segmentation algorithms whichre leveraged with for this work. Demonstratedn Fig 8A and B is the preliminary result toxtract the boundary surfaces for the geometryf interest. This example indicates the appropri-te approaches as suggested; however, moreime and effort are needed to enhance the algo-ithms to extract the geometry more accurately.
For a NURBS curve of order k, as shown inig 8s, it can be expressed as follows:
C (u) ��i�0
n
wipiNik(u)
�i�0
n
wiNik(u)
(1)
here pi (i � 0, . . . , n) denotes the deBoorontrol polygon and the wi are the weights asso-iated with each control point. The Ni
k�u� Nik�u� is
he normalized B-Spline basis function of orderand is defined recursively over a knot vector� Ti (i � 0 . . . n � k) by the recurrence
elations as shown in the following equation.
Nik(u) �
(u � Ti)Nik�1(u)
Ti�k�1 � Ti
(Ti�k � u)Ni�1k�1(u)
�Ti�k � Ti�1
(2)

Fctkt
pl
a
tsb
Flapbalcczeaoaslolladpa2brlpop3rarprrmb1
118 Sittitavornwong et al
Ni1(u) � �1, if Ti � u � Ti�1
0, otherwise
T � Ti i � 0, 1, . . . , n � k
or the knot vector T, it contains the nonde-reasing knot values with the multiplicity k forhe knot value 0 and 1 on both ends of thenot vector so the NURBS curve can be usedo interpolate the first and last control points
l
0 and pn. For example, a knot vector T can beisted as following:
T � �0, 0, . . . 0, Tk, . . . , Tn, 1, 1, . . . , 1�
nd
Ti � Ti�1.
A NURBS surface (Fig 8B) is actually theensor product of the NURBS curve definition ashown in Eq. (1). It can assume the form aselow:
igure 8. Facial landmark location. 1 & 7, right andeft lateralciliary points located above most lateralspect of eyebrows; 2 & 6, right and left superciliaryoints located above most superior aspect of eye-rows; 3 & 5, right and left interciliary points locatedbove medial aspect of eyebrows; 4, midnose pointocated on midline of nasal bridge in line with medialanthi; 9 & 10, right and left infraorbital points lo-ated on infraorbital notches; 8 & 11, right and leftygomatic points located on outer orbital region,quidistant below the lateral canthi as 1 and 7 arebove; 12 & 16, right and left maxillary points locatedn cheek one quarter distance between right and leftla and right and left temporomandibular joint, re-pectively; 13 & 15, right and left lateral alar pointsocated on lateral alar rims; 14, nasal tip point locatedn nasal tip; 17 & 18, right and left nasolabial points
ocated on nasolabial fold, midway between right andeft ala and commissures, respectively; 19 & 26, rightnd left cheek points located on cheek one-quarteristance between right and left commissures and tem-oromandibular joints, respectively; 21 and 24 right,nd left commissure points located on commissures;0 & 25, right and left mid-cheek points located 2 cmetween points 19 through 21 and 24 through 26,espectively; 22 & 23, right and left upper lip pointsocated on peaks of Cupid’s bow; 28, mid-lower lipoint; 27 & 29, right and left lower lip points locatedn middle of lower lip vermillion halfway betweenoints 21 through 28 and 24 through 28, respectively;2, mid-chin point located 2 cm below point 28; 31 & 33,ight and left chin points located 2 cm lateral to point 32nd 2 cm below points 27 and 29, respectively; 30 & 34,ight and left lateral chin points located 2 cm lateral tooints 31 and 33 and 2 cm below points 27 and 29,espectively. Reprinted with permission from Noo-eyazdan M, Trotman CA, Faraway JJ: Modeling facialovement. II. A dynamic analysis of differences caused
y orthognathic surgery. J Oral Maxillofac Surg 62:1380-386, 2004.106 (Color version of figure is available on-
ine.)
WiwdaT
tfcmtcpoubtstcatmptifs
tssptmmopttptpsaN
cgt
catTisbpio
mrp6mnaaiccopcafcoa
pbvnsop
ttcfcsow
119Evaluation of OSAS by Computational Fluid Dynamics
S (u, v) ��i�0
m
�j�0
n
wijpijNik1(u)Nj
k2(v)
�i�0
m
�j�0
n
wijNik1(u)Nj
k2(v)(3)
here pij is a 3D NURBS control point net, and� 0 . . . m, j � 0 . . . n, wij are the weights associatedith each control point. The Ni
k1�u� and Njk2�v�
enote the normalized basis functions of order k1
nd k2 over 2 kt vectors T1 � Ti, I � 0 . . . m and2 � Tj, j � 0 . . . n.
The basis functions are defined recursively inhe same way as in the curve. NURBS surfaceormulation thus provides a strong mathemati-al foundation to correspond the facial land-arks with the control points, which allows the
o interpolation of the displacement of cervi-ocraniofacial skeletal reference points. Map-ing a dense NURBS surface control point netn the patient’s pre- and postoperative face issed to calculate the transformation matricesetween these 2 sets of control points to identifyhe deformation. Such deformation data aretored in a database as supplemental informa-ion to predict the postoperative geometryhange based on preoperative 3D scanned im-ges and statistical values from literature. Theransformation matrices are then applied to
ove control Points pij in each region. Onceij are obtained, the facial surface covered byhis NURBS surface patch are interpolated us-ng Eq. (3), and blended with rest of the staticacial surface region to regain the entire facialoft-tissue surface.
The geometry reconstruction approach to ex-ract the facial surface is used as well as skeletaltructure for pre- and postoperative patient data-ets to determine the change of facial landmarkoints with respect to the skeletal change due to
he MMA procedure. To calculate the transfor-ation matrices more precisely for these land-ark points, a NURBS surface patch is placed
ver the facial region that covers these landmarkoints. Comparisons of the pre- and postopera-
ive NURBS surface are conducted to calculatehe offset of each control point. The landmarkoints are projected onto these NURBS surfaces
o interpolate the offset of these landmarkoints. As shown in Figs 9 and 10, the NURBSurface can be used properly for this purpose asresult of the many important properties of a
URBS surface, including local control (ie, the thange of a control point will only affect theeometry nearby, not propagating throughhe entire surface).
With these processes, all 3D-CT scans of OSASases, including pre- and postoperative MMA,re transformed to surface geometrical mesh ofhe face and airway for the stereoscopic models.he anatomical references and landmarks are
dentified on these models. Therefore, it is pos-ible to compare the data of these static modelsetween pre- and postoperative MMA. At thisoint, attention is focused on 2 areas: the chang-
ng of facial soft-tissue profile and the changingf the upper airway region.
The changing of facial soft-tissue profile. The landarks of facial and neck areas are defined and
epresented on the 3D geometrical modeling ofre- and postoperative MMA. Preoperative and-month postoperative MMA in 3D geometricalodeling are analyzed and compared in facial/
eck soft-tissue dimensional change and pre-nd postoperative pharyngeal airway volume, tossess whether there is a correlation between thencrease in pharyngeal airway space and de-rease in AHI. The average facial/neck soft-tissuehange is expressed as percentage of dento-osse-us movement by superimposing of the pre- andostoperative images (Fig 11). These numbers ac-urately predict the postoperative facial appear-nce of the patient who undergoes MMA. Wol-ord et al102 reported the facial soft-tissuehanges and expressed as percentage of dento-sseous movement for advancement of maxilland mandible by using cephalogram (Fig 12).
This step helps the clinician determine andredict the correlation of changing surgicalone and soft tissue after MMA (horizontal ad-ancement of maxilla and mandible). With theseumbers of percent changes between bone andoft tissue, it is possible to compare the numbersf polysomnogram (AHI, SpO2, BMI) and inter-ret for the co-relation outcomes.
The changing of the upper airway region. Withhe geometry extracted, it is possible to calculatehe volume of airspace and area of any givenross sections. Such information is very usefulor quantitative comparison. Polyhedron volumealculation can be achieved by the summing ofigned volumes of tetrahedra defined by correctlyriented triangles and an arbitrary point,107 whichill allow the development of a new algorithm
hat allows the researcher to calculate the vol-

uwat
(
zt
cuoaavv
bfic
atpt
Fhlt
120 Sittitavornwong et al
me of the airway between two selected planesithin the region of interest. The volume of theirway can be obtained by the volume of a closedriangulated mesh as following formulation108:
Consider a tetrahedron V0V1V2V3, where Vi
i � 0, 1, 2, 3) denotes each vertex, Vi � (xi, yi,
igure 9. A NURBS surface patch is mapped onto aypothetical human face, and the control point new
ocation can be calculated based on the surface per-urbation. (Color version of figure is available online.)
Figure 10. NURBS control points and the ass
i). The signed volume of the signed volume ofhe tetrahedra is
Volume�Vo V1 V2 V3 �
�1
6det�
1 1 1 1
xo x1 x2 x3
yo y1 y2 y3
zo z1 z2 z3
� (4)
The volume of a closed triangulated mesh Man be computed as the sum of the signed vol-mes of tetrahedra, each of which is defined byne of the triangular faces Fi � VFi0VFi1VFi2 andn arbitrary point V. The triangular faces aressumed to be counterclockwise oriented asiewed from the outside of the closed mesh. Theolume of the closed mesh is
Volume�M�� �
triangle Fi
Volume�V VFi0VFi1
VFi2 � (5)
To avoid computational error, V is chosen toe the center of M. Figure 13A and B shows theocusing area of the airway that we are interestedn that will be applied as with the volume of alosed triangulated mesh as above.
With this step explanation, the changing areand volume of the airway geometry can be de-ermined. Figures 14 and 15 show the pre- andostoperative MMA of the same patient in an-eroposterior and lateral direction subsequently.
ociated geometry for A-curve, B surface.

A3cto(pt
Omsnbhsvvtrefid
SD
OeCffliepacaiephp2e
Ftp
Fcm
121Evaluation of OSAS by Computational Fluid Dynamics
fter airway geometry reconstruction fromD-CT scans, it is possible to see the remarkablehanges in the static stereoscopic displays. Withhe static stereoscopic displays of pre- and post-perative MMA, the changing of dimensionsarea, volume) of the airway are recorded, com-ared, and elicited with the PSG data correla-
ion.
Generation of Numerical Mesh Model
nce the geometry of interest is extracted, nu-erical meshes must be generated before CFD
imulations can take place. This requires theumerical mesh generation algorithms to be ro-ust for complex biological geometry so thatigh quality meshes can be produced. Demon-trated in Fig 16 are the high-quality surface andolume meshes generated using direct 3D ad-ancing front method.109 This is the algorithmhat is used for mesh generation as it providesobust and high quality meshes. Such mesh gen-ration is used for next step simulations of flow-elds using sophisticated computational fluid
igure 11. Superimposition of pre- and post-opera-ive 3D-CT scan of MMA will be measured and ex-ressed as percentage of dentoalveolar movement.
ynamics software developed at CSLab. i
electing Cases for Computational Fluidynamics (CFD)
CFD-Based Flow Solver
nce the geometry of the object of interest isxtracted and the associated mesh is generated,FD-based numerical simulations can be per-
ormed to analyze the transport phenomena ofow through the airway. The CFD-based numer-
cal simulation is conducted by solving the gov-rning equations that describe the transporthenomena of continuum fluid flows, such asir. The governing equation consists of a set ofoupled nonlinear equations, such as continuitynd Navier-Stokes equations.66 The geometry ofnterest is very complex, deriving an analytic (ie,xact) solution of the governing equation is im-ractical. Hence, numerous numerical methodsave been developed to solve for the set of cou-led nonlinear governing equations. There aremajor approaches used to solve the governing
quations: pressure-based and density-based
igure 12. Wolford et al102 stated the facial soft tissuehange expressed as percentage of dentoosseousovement for advancement of maxilla and mandible
ndividually.

msass
pdosu
Fd
F ng a(
122 Sittitavornwong et al
ethods. The pressure-based method, whicholves pressure as one of the dependent vari-bles and obtains density from the equation oftate, is widely used to solve the low-to-mediumpeed incompressible and compressible flow, es-
igure 14. (A) Pre- and (B) postoperative MMA im
igure 13. Preliminary result of (A) volume renderiColor version of figure is available online.)
emonstrate lateral enhancement of the airway.
ecially for the internal flow. In contrast, theensity-based method, which solves density asne of the dependent variables and obtains pres-ure from the equation of state, is most oftensed to solve the compressible high-speed flow,
of the OSAS patient with subtraction 3D-CT scan
nd (B) extracting surfaces for geometry of interest.
ages

ehosst3cs
ioqdmsngr
Fd way.
F
123Evaluation of OSAS by Computational Fluid Dynamics
specially for the external flow. Each methodas its strengths and weaknesses. In grid topol-gy, there are 2 major approaches used in CFDolvers: structured grid and unstructured gridolvers. The structured grid flow solvers use ei-her quadrilateral (for 2D) or hexahedral (forD) mesh to discretize (that is, to convert aontinuous space into an equivalent discretepace for easier calculation) the flow domain of
igure 15. (A) Pre- and (B) postoperative MMA imemonstrate anteroposterior enhancement of the air
igure 16. High quality surface and volume meshes for a fem
nterest such that indexes of the mesh are inrder. The unstructured grid flow solvers useuadrilateral and triangular (for 2D) or tetrahe-ral, hexahedral, prism, and pyramid (for 3D)esh to represent the computational domain
uch that the mesh indexes are not in order (orot in a structured manner). The structuredrid flow solver has good numerical accuracy inesolving the viscous boundary layer but is inef-
of the OSAS patient with subtraction 3D-CT scan
agesoral artery. (Color version of figure is available online.)

fiunlbehctsta
sbI
deeisteisrhcfsar
Ffa
124 Sittitavornwong et al
cient in modeling complex geometries. Thenstructured grid flow solver in contrast has aumerical dissipation problem in the viscous
ayer if the triangular or tetrahedral mesh is usedut is very efficient in handling complex geom-try problems. Researchers have developed aybrid grid or generalized grid technology toombine the strength of both grid topologies. Inhe present study, we used 2 in-house CFD flowolvers, UNIC and HYB3D, to simulate flowhrough pre- and postoperative upper airwaynd explore their suitability.
The UNIC code is an unstructured grid pres-ure based Navier-Stokes flow solver, developedy Dr Y.S. Chen of Engineering Sciences,nc.110,111 The UNIC code has been well vali-
igure 17. Study of hemodynamics in the femoral aemoral artery, (B) shear stress of the artery surface, a
nd exit planes. (Color version of figure is available onlinated and used to simulate a great variety ofngineering problems ranging from internal toxternal flows and incompressible to compress-ble flow. One of the examples is the numericalimulation of flood flow through a femoral ar-ery, as shown in the Fig 17. Numerous submod-ls were incorporated in the code to model var-ous physics and transport phenomena. Theseubmodels include (1) finite-rate and equilib-ium chemistry for combustion, (2) conjugateeat transfer for coupling heat convection andonduction, (3) 2-equation eddy viscosity modelsor turbulence effects, (4) both the heterogeneouspray model with Eulerian/Lagrangian approachnd the homogeneous spray model with the Eule-ian/Eulerian approach and real-fluid property
using UNIC code. (A) Geometry and mesh of theC) pressure of the artery surface and vectors at inlet
rterynd (
e.)

mm(efpudmfited
oecvtggfccctalooi
netvaifsbbtutsctuursTippgtuba
m
T
A
125Evaluation of OSAS by Computational Fluid Dynamics
odels for liquid spray flow, (5) the finite volumeethod for solving radiation transport equation
RTE), (6) solving translational and vibrationalnergy equations for thermal nonequilibrium ef-ect, and (7) porosity model for flow through aorous media, etc. In addition, the UNIC codeses parallel computing with PVM112 or MPI113
omain decomposition with Metis114 and flexibleesh adaptation to enhance its computational ef-ciency. We believe the UNIC code is as compu-
ationally efficient as any CFD codes and hasquipped appropriate models to resolve the un-erlying physics of flow through airway.
The density-based flow solver HYB3D, devel-ped by Koomullil,115,116 is designed for a gen-ralized grid framework and is used to simulateomplex geometry problems with ease. Finite-olume schemes for solving an integral form ofhe Navier-Stokes equations are well suited foreneralized grids because a typical generalizedrid is an agglomeration of polygons with a dif-erent number of sides. Hence, HYB3D uses aell-centered, finite volume scheme in whichell-averaged flow variables are stored at the cellenter. The inviscid numerical flux passinghrough the cell faces is calculated with Ro’spproximate Riemann solver117 as an exact so-ution for a linearized Riemann problem. Higher-rder accuracy in the spatial discretization isbtained with a linear reconstruction of the prim-
tive variables by use of the values of those in the
able 5. Demographic and Raw Data Describing the
Case Age Sex Pre-BMI (kg/m2) Post-BMI (kg/m
1 56 M 28 292 54 F 45 443 46 M 26 294 56 M 33 355 30 M 38 396 57 M 29 277 55 M 33 338 45 F 54 559 56 F 16 16
10 48 M 42 4511 57 M 26 2712 60 M 27 2713 38 M 32 3114 38 M 32 3115 52 M 28 2716 29 F 42 4317 48 F 41 4818 32 M 41 4019 56 F 30 3120 38 F 34 36
HI, apnea hypopnea index.
eighboring cells. With use of the Taylor’s seriesxpansion, the flow variables are extrapolated tohe cell-faces from either side of the face and thosealues are used to solve the Riemann problem. Tovoid spurious values near the regions where theres a sharp jump in the flow variables, a limiterunction is used. The limiter function is con-tructed to satisfy the monotonicity principle andasically ensures that the extrapolated values lieetween the maximum and minimum values ofhe variable in the surrounding cells and the cellnder consideration. The temporal integration of
he governing equations is achieved by an implicitcheme in which the numerical flux crossing theell face is a function of the primitive variables athe next time level. The numerical accuracy of thensteady simulations has been improved with these of Newton iterations.118 The matrix systemesulting from the aforementioned equation isolved with the symmetric Gauss Seidel method.o handle larger grids, a parallel simulation strategy
s developed. In this approach, the grid is decom-osed into different blocks with the public domainrogram METIS. The graph of the grid is used in therid decomposition process. The information acrosshe grid interfaces is passed between different blockssing a message-passing interface, MPI. Hence, weelieve the UNIC code is an efficient and appropri-te flow model for simulating flow through airway.
On the basis of our previous study (Table 5),ost cases (17 of 20) have an AHI greater than 40,
ent Population
Pre-AHI Pre-SpO2 (%) Post-AHI Post-SpO2 (%)
47.4 83 7 9299.6 56 11 9127.2 81 38.2 8843.3 94 6.6 95
107.9 86 28.8 8841 84 38.3 8828 88 5.8 85
134 88 15 8347 87 5 8960 55 16 79
100 87 47 7856 88 27 8751 68 35 8355 80 55 8543 75 1.6 82
122.2 75 5.9 8663 75 6.5 96
130 84 7 96102 87 5.7 8726.8 88 9 98
Pati2)

wctitaest
iadctglos
2AFETas
igobacpdanedrbncflt
Sssob
Fpo
126 Sittitavornwong et al
hich are classified as severe OSAS cases. We de-ided to select only severe cases for CFD simula-ion. Each case was selected at the same probabil-ty. The tidal volume in adults which is normally 5o 7 mL/kg100 is used for the volume of simulatingirflow. The usual I:E ratio100 (inspiration time/xpiration time) of 1:2 is the number for settingtimulation. Peak pressure at the end of inspira-ion (Ppeak) at � 15 cm H2O is monitored.63
The dimension (diameter, area, and volumen different levels) of pre-/postoperative airwayre recorded and compared with the technologyeveloped by ETLab. The CFD simulations areonducted to obtain velocity and impedance ofhe airflow through various pre-/postoperativeeometries of upper airway (Fig 18). The corre-ation of the number between PSG, dimensionf airway and airflow properties is analyzed withtatistics.
) Visualization of Geometrical Mesh andirflow Simulation (Postprocessor for thelow-Field Visualization and Featurextraction)o facilitate the CFD simulations of airway, pre-nd postoperative airway geometries must be con-
igure 18. (A) Anteroposterior view, and (B) lateraatient demonstrate the airway and direction of snline.)
tructed based on the CT data, followed by numer- o
cal mesh generation to represent the discretizedeometry. The CFD-based flow solvers and centerf numerical simulations need to equip the capa-ility of solving the low-speed compressible flowccurately and efficiently handling problems withomplex geometries. Stereoscopic visualizationrovides researchers rich visual cues to better un-erstand the complex geometry and flow fieldssociated with the upper airway. The variableumbers of fluid dynamics are the pressure gradi-nt (�p), airflow resistance, flow rate, volume andiameter of airway at the interesting level, such asetropalatal and retrolingual areas. These num-ers are compared with the number of polysom-ogram (AHI, SpO2, BMI) and interpreted for theorrelation outcomes. The postprocessor for theow-field visualization, feature extraction are de-
ailed next.
Postprocessing Algorithms
cientific visualization algorithms, such as iso-urfaces and streamlines, can provide the re-earchers better understanding and explorationf simulated results. These techniques haveeen developed and are relative mature technol-
w of pre-operative MMA images of the same OSASation airflow. (Color version of figure is available
l vieimul
gies. The in-house developed visualization soft-

ws(vpmwbecsusoElwufi
hvawmcviepamsivfdt
S
DaadTcoattf
sa
mtbdcluwtMmTjfcb
is4ttFpgba
OauccAspfPcs(tipa
ct
127Evaluation of OSAS by Computational Fluid Dynamics
are at ETLab, Goggle,119 uses the popular open-ource visualization library Visualization ToolkitVTK)120 to provide these powerful and ad-anced visualization functionalities. We alsorovide the new algorithm to Goggle so thatean pressure at a user-defined locationithin the domain of interest can be obtainedy inserting a cutting plane into the domain,xtracting the pressure distribution on thisutting plane, and obtaining its mean pres-ure. Goggle can be tailored for this study tonderstand the important features of medicalignificance. This software also can be operaten the stereoscopic display system available atTLab so that medical and engineering col-
aborators can analyze the results in real timeith the benefit of rich visual cues to betternderstand the complex geometry and floweld associated with the upper airway.
The key aspect of this step is to bring togetherigh-fidelity models, user interaction, and 3Disualization into the same virtual space creatingmodel that acts like it is real. The goal of thisork is to create a physically driven model that isore than a static visualization of data (virtual
ardboard). That is, the goal is to create airtual model of a real furnace that respondsn the same way as a real furnace. This willnable the user to interact with the virtuallant in the same manner as the real plant. Tochieve this long-term goal, a number of stepsust be implemented. In the first steps pre-
ented here, the visualization, data, and usernteraction all need to be integrated into theirtual model. This model then provides a plat-orm for future inclusion of real time, physics-riven interaction permitting user query andesting of designs.
tatistical Analysis
escriptive statistics (including mean, range,nd standard deviation) are used to describell measurements acquired from 3D-CT scanata from 20 cases in our previous study.hese measurements include dimensionalhanges of facial soft-tissue profiles, dento-osse-us movements, area and volume of the upperirway in pre- and postoperative MMA condi-ions. The location with the minimum area ofhe upper airway in pre- and postoperative MMA
or each OSAS case is identified through de- acriptive analysis. Distribution of each variable islso evaluated.
On the basis of 3D-CT scan data for measure-ents, a paired t test or Wilcoxon signed-rank
est is used to compare the individual changesetween pre- and postoperative MMA, includingimensions of the facial soft tissue profile, per-entage of the dento-osseous movement at eachandmark, area at each selected location of thepper airway, and volume of whole upper air-ay. A summary statistic also is used to compare
he changes between pre- and postoperativeMA for anteroposterior and lateral dimensionseasured at the different levels of the airway.he significant level for statistical tests is ad-
usted by multiple comparisons using the Bon-feroni correction method. The overall signifi-ant level for statistical inference is controlled toe 0.05.
According to our previous study, the major-ty (17 of 20) of OSAS cases are classified asevere cases (AHI before MMA is greater than0). In the future, clinicians will have thisechnology to evaluate the effect of MMAreatment for OSAS by using CFD simulation.or simulated CFD data, it is possible to com-are the numbers of fluid dynamics—pressureradient (�p), airflow resistance, and flow rateetween pre- and postoperative MMA at therea of interest.
To address the hypothesis that the cure ofSAS by MMA surgery can be predicted by
nalyzing anatomical airway changes with these of 3D geometrical reconstruction andomputational fluid dynamics, the variableorrelations of OSAS clinical studies (such asHI, SpO2 and BMI) and geometrical dimen-
ional measurements of the facial soft tissuerofiles, area, and volume of the upper airway
rom 3D CT scan data were evaluated with theearson correlation coefficient or Spearmanorrelation coefficient. The correlations andignificant changes of OSAS clinical studiesAHI, SpO2, and BMI) and MMA are useful forhe prediction of clinical outcomes in OSAS,ncluding surgical succession, facial soft-tissuerofiles, dimensions, and volume of the upperirway.
In summary, OSAS is a complex disease pro-ess. The most significant forms involve disrup-ion of normal breathing through an abnormal
irway. The airway is a 3D structure with com-
pbtcgnts
R
128 Sittitavornwong et al
lex anatomy and airflow. This new technologyrings complex engineering and mathematicalechnology together to better understand theomplexity of disrupted airflow. The advancesained from this novel application of these tech-ologies offers hope in an attempt to improve
he lives of individuals suffering from obstructiveleep apnea syndrome.
eferences1. Young T, Palta M, Dempsey J, et al: The occurrence of
sleep-disordered breathing among middle-aged adults.N Engl J Med 328:1230-1235, 1993
2. Young T, Peppard PE, Gottlieb DJ: Epidemiology ofobstructive sleep apnea: A population health per-spective. Am J Respir Crit Care Med 165:1217-1239,2002
3. Guilleminault C, Tilkian A, Dement WC: The sleepapnea syndromes. Annu Rev Med 27:465-484, 1976
4. Young T, Peppard P: Sleep-disordered breathing andcardiovascular disease: Epidemiologic evidence for arelationship. Sleep 23:S122-126, 2000 (suppl 4)
5. Young T, Peppard P, Palta M, et al: Population-basedstudy of sleep-disordered breathing as a risk factorfor hypertension. Arch Intern Med 157:1746-1752,1997
6. Tilkian AG, Guilleminault C, Schroeder JS, et al: Sleep-induced apnea syndrome. Prevalence of cardiac ar-rhythmias and their reversal after tracheostomy. Am JMed 63:348-358, 1977
7. Young T, Skatrud J, Peppard PE: Risk factors for ob-structive sleep apnea in adults. JAMA 291:2013-2016,2004
8. Young T, Peppard P: Epidemiology of obstructive sleepapnea, in Breathing Disorders in Sleep. London, W. B.Saunders, 2001, pp 31-43
9. Maekawa M, Shiomi T: Sleep apnea syndrome (SAS)and ischemic heart disease (IHD) [in Japanese]. Nip-pon Rinsho 58:1702-1706, 2000
10. Chin K: Obstructive sleep apnea-hypopnea syndromeand cardiovascular diseases. J Intern Med 43:527-528,2004
11. Beelke M, Angeli S, Del Sette M, et al: Obstructive sleepapnea can be provocative for right-to-left shuntingthrough a patent foramen ovale. Sleep 25:856-862,2002
12. Altin R, Ozdemir H, Mahmutyazicioglu K, et al: Evalu-ation of carotid artery wall thickness with high-resolu-tion sonography in obstructive sleep apnea syndrome.J Clin Ultrasound. 33:80-86, 2005
13. George CF, Sleep: Driving and automobile crashes inpatients with obstructive sleep apnoea/hypopnoea syn-drome. 5. Thorax 59:804-807, 2004
14. George CF, Smiley A: Sleep apnea and automobilecrashes. Sleep 22:790-795, 1999
15. Wu H, Yan-Go F: Self-reported automobile accidentsinvolving patients with obstructive sleep apnea. Neurol-
ogy 46:1254-1257, May 199616. Krieger J, McNicholas WT, Levy P, et al: Public healthand medicolegal implications of sleep apnoea. Eur Re-spir J 20:1594-1609, 2002
17. Strollo PJ, Jr, Rogers RM: Obstructive sleep apnea.N Engl J Med 334:99-104, 1996
18. Sher AE: Surgical management of obstructive sleepapnea. Prog Cardiovasc Dis 41:387-396, 1999
19. Gould GA, Whyte KF, Rhind GB, et al: The sleep hy-popnea syndrome. Am Rev Respir Dis 137:895-898,1988
20. Bixler EO, Vgontzas AN, Ten Have T, et al: Effects ofage on sleep apnea in men. I. Prevalence and severity.Am J Respir Crit Care Med 157:144-148, 1998
21. Peter JH, Becker H, Cassel W, et al: [Diagnosis of sleepapnea: initial experiences with a staged procedure].Pneumologie 43:587-590, 1989 (suppl 1)
22. Kribbs NB, Pack AI, Kline LR, et al: Objective measure-ment of patterns of nasal CPAP use by patients withobstructive sleep apnea. Am Rev Respir Dis 147:887-895, 1993
23. Krieger J, Kurtz D: Objective measurement of compli-ance with nasal CPAP treatment for obstructive sleepapnoea syndrome. Eur Respir J 1:436-438, 1988
24. Schweitzer PK, Chambers GW, Birkermeier N: Nasalcontinuous positive airway pressure (CPAP) compli-ance at six, twelve and eighteen months. J Sleep Res16:186, 1987
25. Faber CE, Grymer L: Available techniques for objectiveassessment of upper airway narrowing in snoring andsleep apnea. Sleep Breath 7:77-86, 2003
26. Marien S, Schmelzer B: Velopharyngeal anatomy insnorers and patients with obstructive sleep apnea. ActaOtorhinolaryngol Belg 56:93-99, 2002
27. Schwab RJ: Upper airway imaging. Clin Chest Med19:33-54, 1998
28. Metes A, Hoffstein V, Direnfeld V, et al: Three-dimen-sional CT reconstruction and volume measurements ofthe pharyngeal airway before and after maxillofacialsurgery in obstructive sleep apnea. J Otolaryngol 22:261-264, 1993
29. Conradt R, Hochban W, Brandenburg U, et al: Long-term follow-up after surgical treatment of obstructivesleep apnoea by maxillomandibular advancement. EurRespir J 10:123-128, 1997
30. Nimkarn Y, Miles PG, Waite PD: Maxillomandibularadvancement surgery in obstructive sleep apnea syn-drome patients: Long-term surgical stability. J OralMaxillofac Surg 53:1414-1418, 1995; discussion:1418-1419
31. Pepin JL, Ferretti G, Veale D, et al: Somnofluoroscopy,computed tomography, and cephalometry in the assess-ment of the airway in obstructive sleep apnoea. Thorax47:150-156, 1992
32. Riley RW, Powell NB: Maxillofacial surgery and obstruc-tive sleep apnea syndrome. Otolaryngol Clin North Am23:809-826, 1990
33. Schwab RJ, Goldberg AN: Upper airway assessment:Radiographic and other imaging techniques. Otolaryn-gol Clin North Am 31:931-968, 1998
34. Shepard JW, Jr, Gefter WB, Guilleminault C, et al:Evaluation of the upper airway in patients with obstruc-
tive sleep apnea. Sleep 14:361-371, 1991
129Evaluation of OSAS by Computational Fluid Dynamics
35. Turnbull NR, Battagel JM: The effects of orthognathicsurgery on pharyngeal airway dimensions and quality ofsleep. J Orthod 27:235-247, 2000
36. Waite PD, Wooten V, Lachner J, et al: Maxillomandibu-lar advancement surgery in 23 patients with obstructivesleep apnea syndrome. J Oral Maxillofac Surg 47:1256-1261, 1989; discussion:1262
37. Isono S: Diagnosis of sites of upper airway obstructionin patients with obstructive sleep apnea [in Japanese].Nippon Rinsho. 58:1660-1664, 2000
38. Isono S, Feroah TR, Hajduk EA, et al: Interaction ofcross-sectional area, driving pressure, and airflow ofpassive velopharynx. J Appl Physiol 83:851-859, 1997
39. Isono S, Morrison DL, Launois SH, et al: Static mechan-ics of the velopharynx of patients with obstructive sleepapnea. J Appl Physiol 75:148-154, 1993
40. Isono S, Remmers JE, Tanaka A, et al: Anatomy ofpharynx in patients with obstructive sleep apnea andin normal subjects. J Appl Physiol 82:1319-1326,1997
41. Isono S, Shimada A, Utsugi M, et al: Comparison ofstatic mechanical properties of the passive pharynxbetween normal children and children with sleep-dis-ordered breathing. Am J Respir Crit Care Med 157:1204-1212, 1998
42. Isono S, Tanaka A, Tagaito Y, et al: Pharyngeal pa-tency in response to advancement of the mandible inobese anesthetized persons. Anesthesiology 87:1055-1062, 1997
43. Launois SH, Feroah TR, Campbell WN, et al: Site ofpharyngeal narrowing predicts outcome of surgery forobstructive sleep apnea. Am Rev Respir Dis 147:182-189, 1993
44. Morrison DL, Launois SH, Isono S, et al: Pharyngealnarrowing and closing pressures in patients with ob-structive sleep apnea. Am Rev Respir Dis 148:606-611,1993
45. Saeki N, Isono S, Tanaka A, et al: Pre- and post-opera-tive respiratory assessment of acromegalics with sleepapnea—Bedside oximetric study for transsphenoidalapproach. Endocr J 47:S61-S64, 2000 (suppl)
46. Watanabe T, Isono S, Tanaka A, et al: Contribution ofbody habitus and craniofacial characteristics to seg-mental closing pressures of the passive pharynx in pa-tients with sleep-disordered breathing. Am J Respir CritCare Med 165:260-265, 2002
47. Hsu PP, Tan BY, Chan YH, et al: Clinical predictors inobstructive sleep apnea patients with computer-assistedquantitative videoendoscopic upper airway analysis. La-ryngoscope 114:791-799, 2004
48. Abbott MB, Donnelly LF, Dardzinski BJ, et al: Obstruc-tive sleep apnea: MR imaging volume segmentationanalysis. Radiology 232:889-895, 2004
49. Adams GL, Gansky SA, Miller AJ, et al: Comparisonbetween traditional 2-dimensional cephalometry and a3-dimensional approach on human dry skulls. Am JOrthod Dentofac Orthop 126:397-409, 2004
50. Hoffman EA, Gefter WB: Multimodality imaging ofthe upper airway: MRI, MR spectroscopy, and ultra-
fast X-ray CT. Prog Clin Biol Res 345:291-301, 199051. Joseph AA, Elbaum J, Cisneros GJ, et al: A cephalomet-ric comparative study of the soft tissue airway dimen-sions in persons with hyperdivergent and normodiver-gent facial patterns. J Oral Maxillofac Surg 56:135-139,1998; discussion:139-140
52. Li HY, Chen NH, Wang CR, et al: Use of 3-dimensionalcomputed tomography scan to evaluate upper airwaypatency for patients undergoing sleep-disorderedbreathing surgery. Otolaryngol Head Neck Surg 129:336-342, 2003
53. Lowe AA, Gionhaku N, Takeuchi K, et al: Three-dimen-sional CT reconstructions of tongue and airway in adultsubjects with obstructive sleep apnea. Am J OrthodDentofac Orthop 90:364-374, Nov 1986
54. Lyberg T, Krogstad O, Djupesland G: Cephalometricanalysis in patients with obstructive sleep apnoea syn-drome. II. Soft tissue morphology. J Laryngol Otol103:293-297, 1989
55. Martonen TB, Zhang Z, Yu G, et al: Three-dimensionalcomputer modeling of the human upper respiratorytract. Cell Biochem Biophys 35:255-261, 2001
56. Oda M, Suzuka Y, Lan Z, et al: Evaluation of pharyn-golaryngeal region with 3-D computed tomography. IntCongr S 1257:281-287, 2003
57. Schwab RJ, Gefter WB, Hoffman EA, et al: Dynamicupper airway imaging during awake respiration innormal subjects and patients with sleep disorderedbreathing. Am Rev Respir Dis 148:1385-1400, 1993
58. Shintani T, Kozawa T, Himi T: Obstructive sleep apneaby analysis of MRI findings. Int Congr S 1257:99-102,2003
59. Schwab RJ: Imaging for the snoring and sleep apneapatient. Dent Clin North Am 45(4):759-796, 2001
60. Terris DJ, Hanasono MM, Liu YC: Reliability of theMuller maneuver and its association with sleep-disor-dered breathing. Laryngoscope 110:1819-1823,2000
61. Goldberg AN, Schwab RJ: Identifying the patient withsleep apnea: Upper airway assessment and physical ex-amination. Otolaryngol Clin North Am 31:919-930,1998
62. Schwab RJ, Gupta KB, Gefter WB, et al: Upper airwayand soft tissue anatomy in normal subjects and patientswith sleep-disordered breathing. Significance of thelateral pharyngeal walls. Am J Respir Crit Care Med152:1673-1689, 1995
63. Fouke JM, Wolin AD, Strohl KP, Galbraith GM: Elasticcharacteristics of the airway wall. J Appl Physiol 66:962-967, 1989
64. Sharit J: Perspectives on computer aiding in cognitivework domains: Toward predictions of effectiveness anduse. Ergonomics 46:126-140, 2003
65. Gore BF: Human performance cognitive-behavioralmodeling: A benefit for occupational safety. Int J Oc-cup Saf Ergon 8:339-351, 2002
66. Warsi ZUA: Fluid Dynamics: Theoretical and Compu-tational Approaches. Boca Raton, FL, CRC Press, 1998
67. Wong BK, Sellaro CL, Monaco JA: Information systemsanalysis approach in hospitals: A national survey.
Health care Superv 13:58-64, 1995
1
1
1
1
130 Sittitavornwong et al
68. Farin GE: Curves and Surfaces for CAGD: A PracticalGuide (ed 5). San Francisco, CA, Morgan KaufmannPublishers, 2001
69. Piegl LA, Tiller W: The NURBS Book. Berlin,Springer-Verlag, 1997
70. Shih AM, Yu T-Y, Gopalsamy S, et al: Geometry andmesh generation for high fidelity computational Simu-lations using non-uniform Rational B-Splines. Appl Nu-merical Mathematics 55:368-381, 2005
71. Thompson JF, Warsi ZUA, Mastin CW: Numerical GridGeneration: Foundations and Applications. New York,Elsevier, North-Holland, Inc, 1985
72. Pirzadeh S, StructuredBackground grids for generationof unstructured grids by advancing-front method.AIAA. 31:257, 1993
73. Thompson DS, Soni BK: Semistructured grid genera-tion in three dimensions using a parabolic marchingScheme. AIAA. 40:391-393, 2002
74. Newling B, Poirier CC, Zhi Y, et al: Velocity imaging ofhighly turbulent gas flow. Phys Rev Lett 93:154503,2004
75. Pospisil J, Katolicky J, Jicha M: A comparison of mea-surements and CFD model predictions for pollutantdispersion in cities. Sci Total Environ 334-335:185-195,2004
76. Hsia TY, Migliavacca F, Pittaccio S, et al: Computationalfluid dynamic study of flow optimization in realisticmodels of the total cavopulmonary connections. J SurgRes 116:305-313, 2004
77. Bove EL, de Leval MR, Migliavacca F, et al: Computa-tional fluid dynamics in the evaluation of hemody-namic performance of cavopulmonary connectionsafter the Norwood procedure for hypoplastic left heartsyndrome. J Thorac Cardiovasc Surg 126:1040-1047,2003
78. Chang TJ: Numerical evaluation of the effect of traf-fic pollution on indoor air quality of a naturallyventilated building. J Air Waste Manag Assoc 52:1043-1053, 2002
79. Kulmala I: Experimental validation of potential andturbulent flow models for a two-dimensional jet en-hanced exhaust hood. AIHAJ 61:183-191, 2000
80. Pless D, Keck T, Wiesmiller K, et al: Numerical simula-tion of air temperature and airflow patterns in thehuman nose during expiration. Clin Otolaryngol 29:642-647, 2004
81. Muller-Wittig W, Mlynsji G, Weinhold I, et al: Nasalairflow diagnosis—Comparison of experimental studiesand computer simulations. Stud Health Technol In-form 85:311-317, 2002
82. Elad D, Liebenthal R, Wenig BL, et al: Analysis of airflow patterns in the human nose. Med Biol Eng Com-put 31:585-592, 1993
83. Weinhold I, Mlynski G: Numerical simulation of airflowin the human nose. Eur Arch Otorhinolaryngol 261:452-455, 2004
84. Waite PD: Obstructive sleep apnea: A review of thepathophysiology and surgical management. Oral SurgOral Med Oral Pathol Oral Radiol Endod 85:352-361,
199885. Lachner J, Waite PD, Wooten V: Treatment of obstruc-tive sleep apnea with methods of orthognathic surgery[in German]. Dtsch Z Mund Kiefer Gesichtschir 14:272-275, 1990
86. Louis PJ, Austin RB, Waite PD, et al: Soft tissue changesof the upper lip associated with maxillary advancementin obstructive sleep apnea patients. J Oral MaxillofacSurg 59:151-156, 2001
87. Waite PD, Vilos GA: Surgical changes of posterior air-way space in obstructive sleep apnea. Oral MaxillofacSurg Clin North Am 14, 2002:385-399
88. Mathur R, Douglas NJ: Family studies in patients withthe sleep apnea-hypopnea syndrome. Ann Intern Med122:174-178, 1995
89. Steinberg B, Fraser B: The cranial base in obstructivesleep apnea. J Oral Maxillofac Surg 53:1150-1154, 1995
90. Woodson BT: Examination of upper airway, in Waite PD(ed): Oral and Maxillofacial Treatment of Obstructive SleepApnea. Oral Maxillofac Surg Clin North Am 7:257-267, 1995
91. Katsantonis GP, Maas CS, Walsh JK: The predictiveefficacy of the Muller maneuver in uvulopalatopharyn-goplasty. Laryngoscope 99:677-680, 1989
92. Kuna ST, Bedi DG, Ryckman C: Effect of nasal airwaypositive pressure on upper airway size and configura-tion. Am Rev Respir Dis 138:969-975, 1988
93. Lavie P, Fischel N, Zomer J, et al: The effects of partialand complete mechanical occlusion of the nasal pas-sages on sleep structure and breathing in sleep. ActaOtolaryngol 95:161-166, 1983
94. Hans MG, Goldberg J: Cephalometric exam in obstruc-tive sleep apnea. In: Waite PD, ed. Oral and Maxillofa-cial Treatment of Obstructive Sleep Apnea. Oral Max-illofac Surg Clin North Am 7:209-281, 1995
95. Waite PD, Wooten V: Maxillomandibular advancementsurgery for obstructive sleep apnea. J Oral MaxillofacSurg 48:770-771, 1990
96. Waite PD, Shetter SM: Maxillomandibular advance-ment surgery: A cure for obstructive sleep apnea syn-drome. In: Waite PD, ed. Oral and Maxillofacial Treat-ment of Obstructive Sleep Apnea. Maxillofac Surg ClinNorth Am 7:327-336, 1995
97. Li KK, Powell NB, Riley RW, et al: Overview of phase Isurgery for obstructive sleep apnea syndrome. Ear NoseThroat J 78:836-837, 841-835, 1999
98. Li KK, Powell NB, Riley RW, et al: Distraction osteogen-esis in adult obstructive sleep apnea surgery: A prelim-inary report. J Oral Maxillofac Surg 60:6-10, 2002
99. Li KK, Powell NB, Riley RW, et al: Long-term Results ofmaxillomandibular advancement Surgery. Sleep Breath4:137-140, 2000
00. Marino PL: The ICU Book (ed 2). Philadelphia,Lippincott Williams & Wilkins, 1997
01. Sleep-related breathing disorders in adults: Recom-mendations for syndrome definition and measurementtechniques in clinical research. The Report of an Amer-ican Academy of Sleep Medicine Task Force. Sleep22:667-689, 1999
02. Wolford L, Hilliard F, Dugan D: Surgical TreatmentObjective: St. Louis: C.V. Mosby, 1985
03. Russ JC: The Image Processing Handbook (ed 2). Boca
Raton, FL, CRC Press, 1995
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
131Evaluation of OSAS by Computational Fluid Dynamics
04. Kuwahara M: Processing of RI-angiocardiographic im-ages, in Preston K, Onoe M (eds): Digital Processing ofBiomedical Images. New York, Plenum Press, 1976
05. Ibanez L, Schroeder W, Ng L, et al. ITK SoftwareGuide. Kitware, Inc, 2003
06. Nooreyazdan M, Trotman CA, Faraway JJ: Modeling facialmovement. II. A dynamic analysis of differences caused byorthognathic surgery. J Oral Maxillofac Surg 62:1380-1386,2004
07. Schneider PJ, Eberly DH: Geometric Tools for Com-puter Graphics. San Francisco, CA, Morgan KaufmannPublishers, 2003
08. Schneider PJ, Eberly DH: Geometric Tools for Com-puter Graphics. San Francisco, CA, Elsevier SciencePublishing, 2003
09. Ito Y, Shih AM, Soni BK: Reliable isotropic tetrahedralmesh generation based on an advancing front method:paper presented at: Proceedings of the 13th InternationalMeshing Roundtable; September 2004; Williamsburg, VA
10. Chen YS: An unstructured finite volume method forviscous flow computations: paper presented at: 7th In-ternational Conference on Finite Element Methods inFlow Problems; Febr 3-7 1989, Huntsville, AL, Univer-sity of Alabama in Huntsville
11. Shang HM, Shih MH, Chen YS, et al. Flow calculationon unstructured grids with a pressure-based method:paper presented at: Proceedings of 6th InternationalSymposium on Computational Fluid Dynamics; Sept
4-8 1995, 1995; Lake Tahoe, NV12. Geist A, Beguelin A, Dongarra J, et al: PVM: ParallelVirtual Machine. Boston, MIT Press, 1994
13. Gropp W, Lusk E, Skjellum A: Using MPI, PortableParallel Programming with the Message-Passing Inter-face. Boston, MIT Press, 1999
14. Karypis G, Kumar V: METIS: Unstructured graph par-titioning and Sparse matrix Reordering System, Ver-sion 2.0: Minnesota. Department of Computer Science,University of Minnesota, 1995
15. Koomullil RP, Soni BK: Flow Simulation using gener-alized Static and dynamics grids. AIAA. 37:1551-1557,1999
16. Koomullil RP, Thompson DS, Soni BK: Iced airfoilSimulation using generalized grids. J Appl NumericalMathematics 46:319-330, 2003
17. Roe PL, Approximate R, Solvers: Parameter Vector,and difference Schemes. J Comput Phys 43:357-372,1981
18. Whitfield DL, Taylor L: Discretized Newton-RelaxationSolution of high Resolution flux-difference SplitSchemes. AIAA:91-1539, 1991
19. Shih AM, Shum PC, Ross DH: Goggle: A portable,extensible Scientific visualization System for desktopand virtual Reality environment: paper presented at:the Huntsville Simulation Conference, Oct, pp 29-31,2003, 2003; Huntsville, AL
20. Schroeder W, Martin K, Lorensen B: The Visualization
Toookit. Kitware, Inc, 2004