Single photon emission computed tomography (SPECT) and SPECT/low-dose computerized tomography did...
7
Single photon emission computed tomography (SPECT) and SPECT/low-dose computerized tomography did not increase sensitivity or specificity compared to planar bone scintigraphy for detection of bone metastases in advanced breast cancer Ate Haraldsen, Henrik Bluhme, Lisbeth Røhl, Erik Morre Pedersen, Anders Bonde Jensen, Eva Boysen Hansen, Hanne Nellemann, Finn Rasmussen and Anni Morsing Nuclear medicine Department & PET Center, Department of Radiology, Department of Oncology, Aarhus University Hospital, Aarhus C, Denmark Summary Correspondence Ate Haraldsen, Nuclear medicine Department & PET Center, Norrebrogade 44, 8000 Aarhus C, Denmark E-mail: [email protected] Accepted for publication Received 25 February 2014; accepted 15 August 2014 Key words bone metastases; bone scintigraphy; breast cancer; magnetic resonance imaging; SPECT/CT Purpose To evaluate and compare the diagnostic performance of whole-body planar bone scintigraphy (WBS), single photon emission computed tomography (SPECT), SPECT/low-dose computerized tomography (SPECT/ldCT) and SPECT/ contrast enhanced diagnostic CT (SPECT/cdCT) in the staging of patients with advanced breast cancer. Methods Seventy-eight patients with recurrence of biopsy-proven breast cancer and suspicion of disseminated disease were investigated with WBS, SPECT, SPECT/ ldCT, SPECT/cdCT and MRI performed on the same day in this prospective study. Images were separately analysed in a blinded fashion by radiologists and nuclear medicine physicians regarding the presence of pathological findings. MRI served as reference standard. Results According to reference standard, 38 of 73 patients had bone metastases. The sensitivity was 87%, 87%, 79%, and 84% and specificity 63%, 71%, 63% and 83% for WBS, SPECT, SPECT/ldCT and SPECT/cdCT. A significantly increased specificity of SPECT/cdCT compared to WBS and SPECT/ldCT was found, and other parameters did not differ significantly between modalities. Additional two patients had bone metastases solely located outside the MRI scan field and seven patients had soft tissue metastases, but no skeletal changes on MRI. Conclusion WBS, SPECT and SPECT/ldCT were less sensitive than MRI and equally specific for the detection of bone metastases in patients with advanced breast can- cer. Based on our findings, we suggest that initial staging include WBS, MRI of the spine and CT for soft tissue evaluation. Further studies may clarify the poten- tial benefits of whole-body MRI and 18F-NaF PET/CT or 18F-FDG PET/CT. Introduction Breast cancer is the most common cancer in women with an annual incidence rate in Denmark of 144/100000 (The Dan- ish Cancer Registry 2011). Each year, around 1250 Danish women will die from advanced breast cancer (The Danish Register of Causes of Death 2011). It is therefore important that timely and individually tailored treatment is launched to optimize prognosis and increase survival. Morbidity and survival of breast cancer are highly dependent on whether the disease is localized or has disseminated. Bone is the most frequent site of distant metastases and cause significant morbidity. However, treatment with specific osteoclast inhibit- ing drugs reduces the number of skeletal-related events, reduce pain and improve quality of life. On that basis, precise and accu- rate evaluation of skeletal involvement is important in the initial work-up for the treatment planning.(Solomayer et al., 2000; Hamaoka et al., 2004; Lluch et al., 2014) . However, due to lack of evidence based on data from ran- domized prospective studies, clear recommendations of algo- rithms and use of imaging modalities for staging are not available. Clin Physiol Funct Imaging (2014) doi: 10.1111/cpf.12191 1 © 2014 Scandinavian Society of Clinical Physiology and Nuclear Medicine. Published by John Wiley & Sons Ltd
Transcript of Single photon emission computed tomography (SPECT) and SPECT/low-dose computerized tomography did...

Single photon emission computed tomography (SPECT) andSPECT/low-dose computerized tomography did not increasesensitivity or specificity compared to planar bonescintigraphy for detection of bone metastases in advancedbreast cancerAte Haraldsen, Henrik Bluhme, Lisbeth Røhl, Erik Morre Pedersen, Anders Bonde Jensen, Eva Boysen Hansen,Hanne Nellemann, Finn Rasmussen and Anni Morsing
Nuclear medicine Department & PET Center, Department of Radiology, Department of Oncology, Aarhus University Hospital, Aarhus C, Denmark
Summary
CorrespondenceAte Haraldsen, Nuclear medicine Department &
PET Center, Norrebrogade 44, 8000 Aarhus C,
Denmark
E-mail: [email protected]
Accepted for publicationReceived 25 February 2014;
accepted 15 August 2014
Key wordsbone metastases; bone scintigraphy; breast cancer;
magnetic resonance imaging; SPECT/CT
Purpose To evaluate and compare the diagnostic performance of whole-body planarbone scintigraphy (WBS), single photon emission computed tomography(SPECT), SPECT/low-dose computerized tomography (SPECT/ldCT) and SPECT/contrast enhanced diagnostic CT (SPECT/cdCT) in the staging of patients withadvanced breast cancer.Methods Seventy-eight patients with recurrence of biopsy-proven breast cancer andsuspicion of disseminated disease were investigated with WBS, SPECT, SPECT/ldCT, SPECT/cdCT and MRI performed on the same day in this prospective study.Images were separately analysed in a blinded fashion by radiologists and nuclearmedicine physicians regarding the presence of pathological findings. MRI servedas reference standard.Results According to reference standard, 38 of 73 patients had bone metastases.The sensitivity was 87%, 87%, 79%, and 84% and specificity 63%, 71%, 63%and 83% for WBS, SPECT, SPECT/ldCT and SPECT/cdCT. A significantly increasedspecificity of SPECT/cdCT compared to WBS and SPECT/ldCT was found, andother parameters did not differ significantly between modalities. Additional twopatients had bone metastases solely located outside the MRI scan field and sevenpatients had soft tissue metastases, but no skeletal changes on MRI.Conclusion WBS, SPECT and SPECT/ldCT were less sensitive than MRI and equallyspecific for the detection of bone metastases in patients with advanced breast can-cer. Based on our findings, we suggest that initial staging include WBS, MRI ofthe spine and CT for soft tissue evaluation. Further studies may clarify the poten-tial benefits of whole-body MRI and 18F-NaF PET/CT or 18F-FDG PET/CT.
Introduction
Breast cancer is the most common cancer in women with an
annual incidence rate in Denmark of 144/100�000 (The Dan-
ish Cancer Registry 2011). Each year, around 1250 Danish
women will die from advanced breast cancer (The Danish
Register of Causes of Death 2011). It is therefore important
that timely and individually tailored treatment is launched to
optimize prognosis and increase survival.
Morbidity and survival of breast cancer are highly dependent
on whether the disease is localized or has disseminated. Bone is
the most frequent site of distant metastases and cause significant
morbidity. However, treatment with specific osteoclast inhibit-
ing drugs reduces the number of skeletal-related events, reduce
pain and improve quality of life. On that basis, precise and accu-
rate evaluation of skeletal involvement is important in the initial
work-up for the treatment planning.(Solomayer et al., 2000;
Hamaoka et al., 2004; Lluch et al., 2014) .
However, due to lack of evidence based on data from ran-
domized prospective studies, clear recommendations of algo-
rithms and use of imaging modalities for staging are not
available.
Clin Physiol Funct Imaging (2014) doi: 10.1111/cpf.12191
1© 2014 Scandinavian Society of Clinical Physiology and Nuclear Medicine. Published by John Wiley & Sons Ltd

Due to its ability to evaluate the entire skeleton at a relatively
low-cost conventional 2-dimensional whole-body scintigraphy
(WBS) has been widely used for the detection of bone metasta-
ses in breast cancer. However, WBS relies on the osteoblastic
response to bone destruction and may be positive in increased
bone turnover of any aetiology such as malignancy, osteoar-
thritis, fractures or infection (Gates, 1998; Solomayer et al.,
2000). Specificity is therefore low and a positive finding often
necessitates further evaluation with computerized tomography
(CT), magnetic resonance imaging (MRI) or biopsy.
The use of new hybrid imaging technology supplementing
SPECT (3D examination) with CT has gained popularity
hypothesizing increased specificity as areas of stimulated bone
turnover may be correlated with anatomical changes such as
sclerosis, osteophytes, arthritis-related changes. Furthermore,
studies on mixed populations have indicated that sensitivity of
3D SPECT is superior to 2D WBS (Gates, 1998; Solomayer
et al., 2000; Savelli et al., 2001). However, prospective studies
in patients with advanced breast cancer comparing WBS and
SPECT/CT to a gold standard technique have to our knowl-
edge not been published.
MRI is considered an accurate and reliable method for addi-
tional evaluation of bone changes judged as possibly malig-
nant on bone scan (Kosuda et al., 1996). Furthermore, MRI
characterizes bone metastases as primarily lytic, sclerotic or
mixed and additionally visualize lesions in the bone marrow
(Even-Sapir, 2005; Vassiliou et al., 2007). As histological veri-
fication of each positive finding on WBS or SPECT/CT was
impossible for ethical and practical reasons, we chose to use
MRI as relative gold standard in the present prospective study.
To evaluate the hypothesized incremental effect on sensitiv-
ity, specificity and diagnostic accuracy of SPECT and SPECT/
CT compared to conventional WBS, we designed a prospective
study including women with recurrence of histopathological
proven breast cancer suspected of disseminated disease. A sec-
ondary aim was to suggest an algorithm suitable for reliable
and adequate staging for metastatic disease based on the prev-
alence of metastatic changes in this population.
Material and methods
Patients
Seventy-eight women (mean age 61�7, range 29–89) with
recurrence of histopathological proven breast cancer referred
to the Department of Oncology at Aarhus University Hospital
between May 2008 and June 2011 were consecutively
included in this prospective study. The study was approved by
the regional ethical committee, and oral and written consent
was obtained. The following imaging studies were performed
in 1 day: WBS, SPECT, SPECT/ldCT, SPECT/cdCT and MRI.
Five patients were excluded from the study; three because of
incomplete imaging sets, one because of concurrent multiple
myeloma and one because of lesions classified as equivocal on
MRI.
Clinical informations about the 73 patients included are
listed in Table 1.
Image acquisition
Bone scintigraphy
WBS was performed 3 h after injection of 750 MBq 99mTc-
dicarboxypropane diphosphonate according to a clinical rou-
tine protocol (scan time 20 min, LEUHR or LEHR collimator,
1024 9 256 or 1024 9 512 matrix) on a dual-head camera
(Picker Axis or Philips Precedence 16-slice SPECT/CT scanner;
Table 1 Clinical informations about the 73 patients included.
n Fraction (%)
Patient age (years)<40 1 140–49 7 1050–59 17 2360–69 34 47≥70 14 19Total 73
Tumour characteristicsSize (mm)<10 6 811–20 26 3621–30 21 2931–50 10 14≥50 8 11Unknown 2 3
Nodes0 20 271–5 31 42>5 18 25Unknown 4 5
ERPositive 56 77Negative 16 22Unknown 1 1
HER2Positive 23 32Negative 42 58Unknown 8 11
Previous treatmentNo prev. treatment 10 14Operation 50 68ChemotherapyCEF 22 30CMF 4 5Taxotere 6 8E/C 6 8
Herceptin 6 8Irradiation 44 60Endocrine therapyTamoxifen 38 52AI 21 29
ER, Estrogene receptor; HER2, Human Epidermal Growth FactorReceptor 2; CEF, Cyclophosphamide, Epirubicin, Fluorouracil; CMF,Cyclophosphamide, Methotrexate, Fluorouracil; E/C, Epirubicin/Cyclo-phosphamide; AI, Aromatase Inhibitor.
© 2014 Scandinavian Society of Clinical Physiology and Nuclear Medicine. Published by John Wiley & Sons Ltd
Comparison of WB, SPECT and SPECT/ldCT in patients with breast cancer, A. Haraldsen et al.2

Philips Healthcare, Eindhoven, Holland) followed by SPECT
on the Philips Precedence camera (LEHR collimator, 128
views, 20 s/view, 128 9 128 matrix, zoom 1�46). SPECT
was reconstructed on a Philips Extended Brilliance Workspace
NM (Philips Healthcare), using Auto SPECT Pro (ASTONISH
iterative reconstruction, 4 iterations, 8 subsets including scat-
ter and ldCT attenuation correction and no filtering) and knit-
ted into a total body SPECT.
CT
CT from the base of the skull to the upper femoral region was
performed on the Philips Precedence scanner in immediate
sequence with the SPECT; ldCT (120 kV, 60 mAs/slice,
600 mm FOV, 512 9 512 matrix, 5 mm/slice, pitch 0�875,collimation 8 9 3) and cdCT (120 kV, 200 mAs/slice,
300 mm FOV, 512 9 512 matrix, 2 mm/slice, pitch 0�938,collimation 16 9 1�5). cdCT was performed as two-phase
spiral CT with arterial phase of the thorax and upper abdomen
and portovenous phase of the abdomen and pelvis using bolus
tracking technique after intravenous injection of Iodixanol
270 mgl ml-1 (Visipaque, GE Health Care, Oslo, Norway)
adjusted to body weight (2 ml kg bw-1). Additional recon-
struction was made of the arterial phase, with enhanced win-
dowing for bone (centre 650 HU, width 2600 HU) and
zoom to encompass the spine.
MRI
MRI of the total spine, sternum and pelvic bones was performed
on a 3T Philips Achieva scanner. For the spine standard, short
tau inversion recovery (STIR, TE=80 ms, TR=3300 ms. Inplane
resolution 1�0 9 1�3 mm) and T1 turbo spin echo (TSE,
TE=8 ms, TR=400 ms. Inplane resolution 1�0 mm 9 1�2 mm)
were acquired for the total spine in the sagittal plane acquiring
15 slices (slice thickness=4 mm). For the pelvic bones, a coro-
nal STIR (TE=57 ms, TR=7200 ms (inplane resolution 1�19 1�7 mm) and an axial T1 TSE (TE=18 ms, TR=594 ms.
Inplane resolution 1�1 9 1�3 mm) were performed.
Image analysis
All image data were stored on a HERMES server (Hermes
Medical Solutions, Sweden) and systematically blinded, so that
no cross reference could be made between modalities. The
blinded data were then redistributed to the physician’s respec-
tive workstations for later analysis. Each scan was analysed by
two experienced consultants in nuclear medicine (WBS,
SPECT, SPECT/ldCT), or in radiology (MRI), and consensus
was obtained without access to clinical data or findings on the
other imaging modalities. SPECT/cdCT was analysed side-by-
side by two nuclear medicine consultants and one radiology
consultant, and consensus was obtained. Data were entered
into separate case report forms for each reading. Any focus of
tracer accumulation or pathological appearance was classified
according to a three-point scale: (i) malignant, (ii) equivocal
or (iii) benign according to the following criteria:
On WBS and SPECT, focal tracer uptake was categorized as
malignant if not located adjacent to joints or representing
well-known normal variants in the sternum (Syed et al., 2005;
Kakhki & Zakavi, 2006) .
On SPECT/ldCT and SPECT/cdCT, focal tracer uptake was
characterized as malignant if not located adjacent to joints or
if corresponding to osteolytic, osteosclerotic mixed changes in
bone structure. Lesions were characterized as benign if local-
ized adjacent to joints or corresponding to benign degenera-
tive changes on CT such as osteophytes, spondylophytes,
subcondral sclerosis and narrowing of joint space. Lesions that
could not be identified as malignant or benign according to
the chosen criteria were categorized as equivocal.
On MRI, findings were characterized as (i) malignant, (ii)
equivocal or (iii) benign based on signal intensities, position
and composition on STIR and T1-weighted images and in
cases of equivocal findings on the course seen in consecutive
scans. Example is presented in Figure 1. On CT, malignant
lesions were suggested by the presence of lytic and/or scle-
rotic changes or as disruption of cortical bone. Furthermore,
enlarged lymph nodes and visceral metastases were described
and registered.
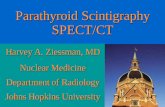
(a) (b) (c)
Figure 1 Horizontal view through pelvis in one patient on (a) SPECT/ldCT, (b) cdCT and (c) T1-weighted MRI showing metastases on SPECT/ldCT and MRI.
© 2014 Scandinavian Society of Clinical Physiology and Nuclear Medicine. Published by John Wiley & Sons Ltd
Comparison of WB, SPECT and SPECT/ldCT in patients with breast cancer, A. Haraldsen et al. 3

MRI was used as reference standard. To improve our refer-
ence standard, radiologists evaluated consecutive MRI scans
for patients with equivocal findings.
All data were stored in a database for subsequent analyses.
Statistical analysis
Data were analysed on patient level and region based. Sensitiv-
ity, specificity, accuracy, and positive and negative predictive
values (PPV and NPV) were calculated and compared with the
MRI using Fisher’s exact test and between modalities with
McNemar’s test. Lesions characterized as equivocal were
encountered in the group of malignant lesions.
On patient level, the patients were categorized as malignant
if the patient had at least one malignant lesion, equivocal if
no malignant lesions and at least one equivocal lesion and last
benign if no malignant or equivocal findings were seen.
Results
Patient characteristics are summarized in Table 1.
Of the 73 included patients, 38 had bone metastases based
on the reference standard including MRI of the spine, sternum
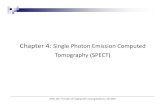
and pelvic bones. Two additional patients had bone metastases
exclusively located outside the MRI scan field of view identi-
fied on WBS or SPECT and confirmed by subsequent diagnos-
tic CT or MRI during follow-up (Fig. 2).
Diagnostic contrast enhanced CT identified soft tissue
metastases in 40 patients of whom seven did not have
bone metastases in the spine, sternum or pelvic bone on
MRI. In total, 45 patients of 73 had bone and/or soft tissue
metastases.
On each modality, the patients were classified as having a
malignant, benign or equivocal scan based on the findings
within the MRI scan field of view (Table 2). The scan were
categorized as malignant if the patient had at least one malig-
nant lesion, equivocal if no malignant lesions and at least one
equivocal lesion were present and last benign if no malignant
or equivocal findings were seen.
Table 2 show a significant decrease in the number of equiv-
ocal scans when performing SPECT and SPECT/ldCT compared
to WBS. On MRI, we have no equivocal scans because consec-
utive MRI scans were evaluated to improve our reference stan-
dard and 1 patient was excluded from the study because of
persisting equivocal scan on MRI.
Patient-based values of sensitivity, specificity, PPV, NPV and
diagnostic accuracy are given in Table 3 according to the MRI
scan field of view. SPECT/cdCT showed significant higher
specificity compared to WBS and SPECT/ldCT based on McNe-
mar0s test with a P-value of 0�046. Furthermore, the overlap-
ping 95% confidence intervals between WBS, SPECT and
SPECT/ldCT demonstrate that no difference was found
between any of these modalities. In particular did SPECT not
increase sensitivity compared to WBS and SPECT/ldCT did not
increase specificity compared to neither WBS nor SPECT.
Figure 3 shows the distribution of patients with bone
metastases in the different skeletal regions limited to areas
covered by all modalities. The shaded areas represent the
number of patients with false positive (red) or false negative
findings (blue) compared to MRI. In none of the regions did
SPECT prove superior sensitivity or SPECT/ldCT superior
specificity than WBS when compared to MRI. Figure 2 also
shows that half of the patients included in the study had bone
(a) (b)
Figure 2 (a) Anterior view of WBS from a patient with a single cos-tal bone metastasis. (b) Posterior view of WBS form another patientwith a solitary bone metastasis in the scull.
Table 2 Number of patients classified as malignant, equivocal orwithout findings suspicious of bone metastases on WB, SPECT,SPECT/ldCT, SPECTcdCT and MRI according to the MRI scan field ofview.
Patients
N = 73 WBS SPECT SPECT/ldCT SPECT/cdCT MRI
Malignant 31 38 35 28 38Equivocal 15 5 8 10 0Benign/Normal 27 30 30 35 35
WBS, whole-body planar bone scintigraphy; SPECT, single-photonemission computed tomography; CT, computerized tomography;SPECT/ldCT, SPECT/low-dose computerized tomography; SPECT/cdCT, SPECT/contrast enhanced diagnostic CT.
© 2014 Scandinavian Society of Clinical Physiology and Nuclear Medicine. Published by John Wiley & Sons Ltd
Comparison of WB, SPECT and SPECT/ldCT in patients with breast cancer, A. Haraldsen et al.4

metastases in the thoracic spine making this location the pre-
dominating skeletal metastatic site in this population (Fig. 4).
Discussion
The present study is one of the first prospective study systemati-
cally comparing conventional WBS, SPECT and new hybrid
technology SPECT/CT for evaluation of bone metastases regard-
less of findings in each modality in women with advanced
breast cancer. All imaging studies including MRI were per-
formed on the same day allowing for direct comparison.
We have evaluated the performance of WB, SPECT, SPECT/
ldCT and SPECT/cdCT separately and not the added value of
modalities.
The present study confirms the high prevalence of metastatic
spread to the bone in patients with advanced breast cancer pre-
viously shown in retrospective studies (Hamaoka et al., 2004;
Manders et al., 2006). In the present study, half of the included
patients had skeletal metastases primarily located to the spine
and pelvis emphasizing the need for high accuracy in evaluation
of these regions. However, two patients had findings highly
suspicious of malignancy exclusively in areas such as skull and
costae, which were not covered by MRI, demonstrating the
need for whole-body evaluation. From the higher sensitivity of
MRI for detecting bone metastases in the present study, a
rational approach would be to extend the MRI coverage to the
entire skeletal system. A recent metaanalysis found PET and MRI
to be superior to both CT and WBS for detecting metastatic dis-
ease in bone (Yang et al., 2011), and a single study indicates
that previous shortcomings of MRI with respect to costal metas-
tases may have been overcome (Chen et al., 2012)
The skeleton is the predominating metastatic site in breast
cancer (Hamaoka et al., 2004). However, in the present study,
seven out of 73 patients had metastases in soft tissue but not
in bone demonstrating that complete staging of these patients
should include evaluation of both skeletal and soft tissue. Fur-
thermore, we found that the NPVs of WBS and SPECT were
only 81% and 83%, respectively, demonstrating that a nega-
tive bone scintigraphy (WBS or SPECT) cannot rule out skele-
tal metastases in these patients. This is in accordance with data
from a recent meta-analysis comparing bone scintigraphy and
PET/CT (Rong et al., 2013).
In accordance with previous findings in patients with pros-
tate and breast cancer, we found that WBS had a sensitivity of
87% for detection of bone metastases compared to MRI
(Even-Sapir, 2005; Shie et al., 2008; Rong et al., 2013) .
WBS detects areas in the bone where an osteoblastic response
is evoked by increased bone turnover. Malignant skeletal
involvement in advanced breast cancer may be lytic, blastic or
mixed suggesting that full evaluation cannot be based on imag-
ing modalities relying on osteoblastic response only. However,
Table 3 According to MRI scan field of view following table showper patient-based sensitivity, specificity, positive predictive value, neg-ative predictive value, and diagnostic accuracy of WB, SPECT, SPECT/ldCT and SPECT/cdCT compared to MRI in diagnosing bone metasta-ses (value with a 95% confidence interval).
WBS SPECT
SPECT/
ldCT
SPECT/
cdCT
Sensitivity(%)
87 (72–96) 87 (72–96) 79 (63–90) 84 (69–94)
Specificity(%)
63 (45–79) 71 (54–85) 63 (45–79) 83 (66–93)*
PPV (%) 72 (57–84) 77 (61–88) 70 (54–83) 84 (69–94)NPV (%) 81 (62–94) 83 (65–94) 73 (54–88) 83 (66–93)Diag.accuracy(%)
75 (64–100) 79 (68–100) 71 (59–100) 84 (73–100)
*McNemar0s test shows significant difference between WB andSPECT/ldCT compared to SPECT/cdCT; P = 0.046.WBS, whole-body planar bone scintigraphy; SPECT, single-photonemission computed tomography; CT, computerized tomography;SPECT/ldCT, SPECT/low-dose computerized tomography; SPECT/cdCT, SPECT/contrast enhanced diagnostic CT; PPV, positive predictivevalues; NPV, negative predictive values.
Figure 3 Distribution of true positive (red),true negative (blue), false positive (shadedred) and false negative findings (shaded blue)for all 5 modalities, separated in 5 anatomicalregions according to the MRI scan field ofview.
© 2014 Scandinavian Society of Clinical Physiology and Nuclear Medicine. Published by John Wiley & Sons Ltd
Comparison of WB, SPECT and SPECT/ldCT in patients with breast cancer, A. Haraldsen et al. 5

we found a sensitivity of 87% of SPECT compared to MRI
within identical field of view. As MRI identifies both blastic and
lytic metastases this suggest that the majority of bone metastases
in these patients lead to an osteoblastic response. This is sup-
ported by data from a study by Hahn et al. showing that the
majority of bone metastases in breast cancer appear to be mixed
osteblastic/osteolytic (Hahn et al., 2011).
Because of its two-dimensional structure, visualization of
increased uptake on WBS may be limited by the superimposi-
tion of structures. Even-Sapir and others showed that the
cross-sectional acquisition planes in SPECT increased sensitivity
compared to WBS in patients with high-risk prostate cancer
(Even-Sapir, 2005).
No significant difference in sensitivity for detecting bone
metastases between attenuation corrected SPECT and WBS was
demonstrated in the present study.
With specificities of 63% and 71% of WBS and SPECT,
respectively, our data confirm the limitation of WBS and
SPECT in discriminating between benign and malignant patho-
logical processes in the cortex.
Fusing SPECT images with simultaneous obtained low-dose
CT (SPECT/ldCT) enable anatomical localization of focal
increased bone turnover thereby potentially improving the dif-
ferentiation of benign versus malignant findings. However, in
the present study, SPECT/ld CT did not increase specificity
demonstrating that improving the anatomical localization of
scintigraphic findings was insufficient to distinguish benign
from malignant bone changes in this population. Our findings
are in accordance with results from a prospective study
including 100 oncologic and non-oncologic patients where
SPECT/ldCT did not increase specificity compared to SPECT
alone (Franc et al., 2012), but contrary to studies on mixed
populations (Gates, 1998; Costelloe et al., 2009; Palmedo et al.,
2014). The discrepancy between our data and the other stud-
ies may be explained by significant differences in study
design. We systematically imaged all patients regardless of
findings on either modality and without first identifying non-
specific and inconclusive findings on SPECT.
As reference standard we used MRI performed on the same
day as the other modalities evaluated in contrast to clinical
follow-up, which is temporally separated from the modalities
to be evaluated. MRI may have both false positives and false
negatives but has been proven more accurate in diagnosing
bone metastases compared to bone scintigraphy and CT (Yang
et al., 2011).
Administering medical oncology treatment may effectively
influence bone metastases and their appearance on imaging
modalities. Development of metastases is a dynamic process
and bone metastases can develop within a short time, making
follow-up as reference standard difficult.
SPECT/ldCT was examined as consensus reading by two
nuclear medicine consultants in contradiction to SPECT/cdCT,
which was consensus reading between two nuclear medicine
consultants and one radiology consultant.
SPECT/cdCT showed significantly higher specificity com-
pared to WBS and SPECT/ldCT based on McNemar0s test witha P-value of 0�046. If consensus reading of SPECT/ldCT was
made in association of nuclear medicine consultant and radiol-
ogy consultant, specificity might potentially be higher. How-
ever we find no significant change in accuracy, NPV, PPV and
sensitivity between SPECT/ldCT and SPECT/cdCT indicating
that only minor additional information may be overlooked on
the ldCT when solely viewed by nuclear medicine consultants.
Furthermore, we would expect a difference between perfor-
mance of ldCT and cdCT in favour of the latter.
Nevertheless, we found that SPECT and SPECT/ldCT reduced
the number of reader defined inconclusive studies compared to
WBS. This is in line with results from previous retrospective and
prospective studies in mixed patient populations suggesting that
the improved focal visualization and anatomical localization in
SPECT and SPECT/ldCT leads to a greater level of observer confi-
dence (Romer et al., 2006; Franc et al., 2012) .
(a) (b)
Figure 4 Sagittal view of one patient with a bone metastasis in sternum visualized on T2- and T1-weighted MRI, but not visual on SPECT/ldCT.
© 2014 Scandinavian Society of Clinical Physiology and Nuclear Medicine. Published by John Wiley & Sons Ltd
Comparison of WB, SPECT and SPECT/ldCT in patients with breast cancer, A. Haraldsen et al.6

In the present study, five different modalities were used for
the evaluation of metastases in advanced breast cancer, a dis-
ease entity and population with a high pretest probability of
having disseminated disease. No single modality proved suffi-
cient for complete staging. In the cervical spine lesions may
be overlooked or not visualized by WBS and SPECT, SPECT/
ldCT could not exclude non-metastatic lesions, the skull and
costae were not included in the MRI field of view. It is there-
fore necessary to include more than one imaging modality in
the initial staging of these patients if relying on the modalities
used in the present study. The perspective is shared by Costel-
lo et al. but in contrast to their recommendation of using WBS
as gatekeeper for further imaging evaluation (Costelloe et al.,
2009). Because of the high pretest probability of benign as
well as malignant pathological skeletal findings and a relatively
large number of patients having soft tissue metastases exclu-
sively, we suggest that initial staging should include WBS,
MRI of the spine and CT for soft tissue evaluation. Future
studies may prove the role of whole-body MRI or PET/CT in
such one-stop-shop evaluation.
Conclusion
WBS, SPECT and SPECT/ldCT were less sensitive than MRI and
equally specific for the detection of bone metastases in
patients with advanced breast cancer. Based on our findings,
we suggest that initial staging include WBS, MRI of the spine
and CT for soft tissue evaluation. Further studies may clarify
the potential benefit of whole-body MRI and 18F-FDG PET/
CT.
Conflict of interest
The authors declare that they have no conflict of interest.
References
Chen YQ, Yang Y, Xing YF, Jiang S, Sun XW.Detection of rib metastases in patients with
lung cancer: a comparative study of MRI.CT and bone scintigraphy. PLoS ONE
(2012); 7: e52213.Costelloe CM, Rohren EM, Madewell JE, Hama-
oka T, Theriault RL, Yu TK, Lewis VO, Ma J,Stafford RJ, Tari AM, Hortobagyi GN, Ueno
NT. Imaging bone metastases in breast
cancer: techniques and recommendationsfor diagnosis. Lancet Oncol (2009); 10: 606–
614.Even-Sapir E. Imaging of malignant bone
involvement by morphologic, scintigraphic,and hybrid modalities. J Nucl Med (2005);
46: 1356–1367.Franc BL, Myers R, Pounds TR, Bolton G, Conte
F, Bartheld M, Da Silva AJ. Clinical utility ofSPECT-(low-dose) CT versus SPECT alone in
patients presenting for bone scintigraphy.Clin Nucl Med (2012); 37: 26–34.
Gates GF. SPECT bone scanning of the spine.Semin Nucl Med (1998); 28: 78–94.
Hahn S, Heusner T, Kummel S, Koninger A,Nagarajah J, Muller S, Boy C, Forsting M,
Bockisch A, Antoch G, Stahl A. Comparisonof FDG-PET/CT and bone scintigraphy for
detection of bone metastases in breast can-cer. Acta Radiol (2011); 52: 1009–1014.
Hamaoka T, Madewell JE, Podoloff DA, Hort-obagyi GN, Ueno NT. Bone imaging in
metastatic breast cancer. J Clin Oncol (2004);22: 2942–2953.
Kakhki VD, Zakavi SR. Age-related normalvariants of sternal uptake on bone scintigra-
phy. Clin Nucl Med (2006); 31: 63–67.
Kosuda S, Kaji T, Yokoyama H, Yokokawa T,Katayama M, Iriye T, Uematsu M, Kusano
S. Does bone SPECT actually have lowersensitivity for detecting vertebral metastasis
than MRI? J Nucl Med (1996); 37: 975–978.Lluch A, Cueva J, Ruiz-Borrego M, Ponce J,
Perez-Fidalgo JA. Zoledronic acid in thetreatment of metastatic breast cancer. Anti-
cancer Drugs (2014); 25: 1–7.
Manders K, van de Poll-Franse LV, Creemers GJ,Vreugdenhil G, van der Sangen MJ, Nie-
uwenhuijzen GA, Roumen RM, Voogd AC.Clinical management of women with metastatic
breast cancer: a descriptive study accordingto age group. BMC Cancer (2006); 6: 179.
Palmedo H, Ebert A, Kreft B, Ko Y, T€urler A,Vorrenther R, G€ohring U, Schild HH, Ger-
hardt T, P€oge U, Ezziddin S, Bier Sack HJ,Ahmadzadehfar H. Whole-body SPECT/CT
for bone scintigraphy: diagnostic value andeffect on patient management in oncologi-
cal patients. Eur J Nucl Med Mol Imaging(2014); 41(1): 59–67.
Romer W, Nomayr A, Uder M, Bautz W,Kuwert T. SPECT-guided CT for evaluating
foci of increased bone metabolism classifiedas indeterminate on SPECT in cancer
patients. J Nucl Med (2006); 47: 1102–1106.Rong J, Wang S, Ding Q, Yun M, Zheng Z,
Ye S. Comparison of 18 FDG PET-CT andbone scintigraphy for detection of bone
metastases in breast cancer patients. A meta-analysis. Surg Oncol (2013); 22: 86–91.
Savelli G, Maffioli L, Maccauro M, De DeckereE, Bombardieri E. Bone scintigraphy and the
added value of SPECT (single photon emis-
sion tomography) in detecting skeletallesions. Q J Nucl Med (2001); 45: 27–37.
Shie P, Cardarelli R, Brandon D, Erdman W,Abdulrahim N. Meta-analysis: comparison
of F-18 Fluorodeoxyglucose-positron emis-sion tomography and bone scintigraphy in
the detection of bone metastases in patientswith breast cancer. Clin Nucl Med (2008);
33: 97–101.
Solomayer EF, Diel IJ, Meyberg GC, Gollan C,Bastert G. Metastatic breast cancer: clinical
course, prognosis and therapy related to thefirst site of metastasis. Breast Cancer Res Treat
(2000); 59: 271–278.Syed GM, Fielding HW, Collier BD. Sternal
uptake on bone scintigraphy: age-relatedvariants. Nucl Med Commun (2005); 26: 253–
257.The Danish Cancer Registry. (ed.) (2011) Sta-
tens Serum Institut, Denmark. www.ssi.dkThe Danish Register of Causes of Death.
(2011) Statens Serum Institut, KøbenhavnS, Denmark. www.ssi.dk
Vassiliou V, Kalogeropoulou C, Giannopou-lou E, Leotsinidis M, Tsota I, Kardamakis
D. A novel study investigating the thera-peutic outcome of patients with lytic,
mixed and sclerotic bone metastases treatedwith combined radiotherapy and ibandro-
nate. Clin Exp Metastasis (2007); 24:169–178.
Yang HL, Liu T, Wang XM, Xu Y, Deng SM.Diagnosis of bone metastases: a meta-analy-
sis comparing (1)(8)FDG PET, CT. MRI andbone scintigraphy. Eur Radiol (2011); 21:
2604–2617.
© 2014 Scandinavian Society of Clinical Physiology and Nuclear Medicine. Published by John Wiley & Sons Ltd
Comparison of WB, SPECT and SPECT/ldCT in patients with breast cancer, A. Haraldsen et al. 7