Simultaneous bilateral third to fifth carpometacarpal joint dislocations; a boxing first?
3
CASE REPORT Simultaneous bilateral third to fifth carpometacarpal joint dislocations; a boxing first? Marcus Davis & Ertan Erel & Jill Webb Received: 24 February 2010 / Accepted: 8 March 2010 / Published online: 8 April 2010 # Springer-Verlag 2010 Abstract Carpometacarpal joint dislocations (isolated and multiple) are uncommon hand injuries occurring in less than 1% of osseous hand injuries. Despite this, unilateral dislocations, with and without associated injuries, have been well-documented in the medical literature. We report the first case of bilateral third to fifth CMC joint dislocations occurring simultaneously in a 20-year-old boxer during a training session. Keywords CMCJ . Dislocation . Carpometacarpal . Bilateral Introduction Carpometacarpal joint (CMCJ) dislocations, isolated and multiple, with and without associated injuries have been well-documented in the medical literature [1–9]. These reports however, have all been of unilateral injuries. We report the case of bilateral third to fifth CMC joint dislocations occurring simultaneously, a previously unre- ported phenomenon. Case report Whilst performing a sequence of punches during a training session, a 20-year-old male boxer described feeling an almost instantaneous pain in both hands, resulting in his having to stop practice. He presented to the emergency department (ED) the same day complaining of pain and swelling over the dorsum of both hands. On examination, both hands were neurovascularly intact, but palpable steps were present on the dorsum of both hands. Plain radio- graphs confirmed dislocation of the third, fourth and fifth metacarpals at the CMC joints bilaterally (Figs. 1 and 2). No fractures were sustained. Closed reduction of all six metacarpals was achieved under Entonox in the ED with subsequent percutaneous K-wire stabilisation performed under general anaesthesia (Figs. 3, 4, 5). Cast immobilisation was used and maintained for 6 weeks. Plain radiographs were taken at first follow-up 1 week post-operation to check that the correct position was maintained. Cast and K-wires were removed in clinic after 6 weeks. Subsequent hand therapy to aid rehabilitation was undertaken resulting in a successful return to work as a plumber 6 months post- injury, confirmed by follow up 1 year post injury. Despite reporting occasional use of the punch bag, the patient has not returned to boxing due to fear of pain. Other late sequela included palpable bony prominences over the k-wire sites and cold intolerance. Discussion CMC joint dislocations are uncommon hand injuries, occurring in less than 1% of osseous hand injuries [10]; M. Davis (*) Queen Victoria Hospital, West Sussex, UK e-mail: [email protected] E. Erel : J. Webb Selly Oak Hospital, Birmingham, UK Eur J Plast Surg (2011) 34:57–59 DOI 10.1007/s00238-010-0424-6
-
Upload
marcus-davis -
Category
Documents
-
view
213 -
download
1
Transcript of Simultaneous bilateral third to fifth carpometacarpal joint dislocations; a boxing first?

CASE REPORT
Simultaneous bilateral third to fifth carpometacarpal jointdislocations; a boxing first?
Marcus Davis & Ertan Erel & Jill Webb
Received: 24 February 2010 /Accepted: 8 March 2010 /Published online: 8 April 2010# Springer-Verlag 2010
Abstract Carpometacarpal joint dislocations (isolated andmultiple) are uncommon hand injuries occurring in lessthan 1% of osseous hand injuries. Despite this, unilateraldislocations, with and without associated injuries, havebeen well-documented in the medical literature. We reportthe first case of bilateral third to fifth CMC jointdislocations occurring simultaneously in a 20-year-oldboxer during a training session.
Keywords CMCJ . Dislocation . Carpometacarpal .
Bilateral
Introduction
Carpometacarpal joint (CMCJ) dislocations, isolated andmultiple, with and without associated injuries have beenwell-documented in the medical literature [1–9]. Thesereports however, have all been of unilateral injuries. Wereport the case of bilateral third to fifth CMC jointdislocations occurring simultaneously, a previously unre-ported phenomenon.
Case report
Whilst performing a sequence of punches during a trainingsession, a 20-year-old male boxer described feeling analmost instantaneous pain in both hands, resulting in hishaving to stop practice. He presented to the emergencydepartment (ED) the same day complaining of pain andswelling over the dorsum of both hands. On examination,both hands were neurovascularly intact, but palpable stepswere present on the dorsum of both hands. Plain radio-graphs confirmed dislocation of the third, fourth and fifthmetacarpals at the CMC joints bilaterally (Figs. 1 and 2).No fractures were sustained.
Closed reduction of all six metacarpals was achievedunder Entonox in the ED with subsequent percutaneousK-wire stabilisation performed under general anaesthesia(Figs. 3, 4, 5). Cast immobilisation was used andmaintained for 6 weeks. Plain radiographs were takenat first follow-up 1 week post-operation to check that thecorrect position was maintained. Cast and K-wires wereremoved in clinic after 6 weeks. Subsequent handtherapy to aid rehabilitation was undertaken resulting ina successful return to work as a plumber 6 months post-injury, confirmed by follow up 1 year post injury. Despitereporting occasional use of the punch bag, the patient hasnot returned to boxing due to fear of pain. Other late sequelaincluded palpable bony prominences over the k-wire sitesand cold intolerance.
Discussion
CMC joint dislocations are uncommon hand injuries,occurring in less than 1% of osseous hand injuries [10];
M. Davis (*)Queen Victoria Hospital,West Sussex, UKe-mail: [email protected]
E. Erel : J. WebbSelly Oak Hospital,Birmingham, UK
Eur J Plast Surg (2011) 34:57–59DOI 10.1007/s00238-010-0424-6

multiple dislocations even more uncommon [8]. CMC jointdislocations usually occur secondary to flexion or extensionforces acting directly over the CMCJs or indirect forcestransmitted along the metacarpal shaft [11]. The second andthird metacarpals require greater force than does the fifth
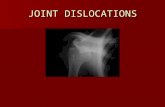
Fig. 2 Right hand lateral radiograph pre-reduction demonstratingmultiple CMCJ dislocations
Fig. 1 Left hand lateral radiograph pre-reduction demonstratingmultiple CMCJ dislocations
Fig. 3 Left hand lateral & oblique radiographs post- reduction andpercutaneous wire fixation
Fig. 4 Left hand AP radiograph post- reduction and percutaneouswire fixation
58 Eur J Plast Surg (2011) 34:57–59

metacarpal due to the former having both multiple articularfacets and thick, strong, ligamentous attachments. Thefourth and fifth metacarpals have fewer ligamentous attach-ments and are inherently more unstable.[7] CMC jointdislocations more commonly occur as a result of highenergy trauma (e.g., road traffic collision) [7–9], but havebeen reported to occur from relatively low energy traumaincluding fist fighting [8].
Management should include closed reduction and immo-bilisation for 4-6 weeks (the latter for multiple dislocations).Most cases of multiple dislocations require percutaneousfixation to maintain stability, as the significant hand oedemacan impede a good-fitting cast. Closed reduction is occa-sionally impossible due to soft tissue interposition, in whichcase, open reduction would be undertaken.
Subsequent presentation with weak grip and/or reducedfinger flexion (resulting from altered hand dynamics)
should alert clinicians to the possibility of incompletereduction [2, 6, 12]. Long-term, arthritic change can occur,although this is less likely to cause a functional problem in thesecond and third CMCJs due to their relative immobility.
Bilateral hand pain and/or swelling following relativelylow energy trauma should therefore cause clinicians to havea low index of suspicion, and thus seek to rule out CMCJdislocations, as prompt early treatment can result in fullrecovery of function; as we have demonstrated in this case.
References
1. Rivington S. Compound dislocation of all the metacarpal bones ofthe right hand: operation, recovery with a serviceable hand.Lancet 1873; 270–271
2. Waugh R, Yancey A (1948) Carpometacarpal dislocations: withparticular reference to simultaneous dislocation of the bases of thefourth and fifth metacarpals. J Bone Joint Surg Am 30:397–404
3. Hazlett J (1968) Carpometacarpal dislocations other than thethumb: a report of 11 cases. Can J Surg 11:315–323
4. Hartwig R, Louis D (1979) Multiple carpometacarpal dislocations:a review of four cases. J Bone joint Surg (Am) 61:906–908
5. Hsu J, Curtis R (1970) Carpometacarpal dislocations on the ulnarside of the hand. J Bone Joint Surg (Am) 52:927–930
6. Imbriglia J (1979) Chronic dorsal carpometacarpal dislocation ofthe index, middle, ring and little fingers: a case report. J HandSurg 4:343–345
7. Mueller JJ (1986) Carpometacarpal dislocations: report of fivecases and a review of the literature. J Hand Surg 11A(2):184–188
8. De Beer JdeV, Maloon S, Anderson P, Jones G, Singer M (1989)Multiple carpo-metacarpal dislocations. J Hand Surg (Br)14B:105–108
9. Edwards A, Pike J, Bird J (2000) Simultaneous carpometacarpaljoint dislocations of the thumb and all four fingers. Injury 31:116–118
10. Bohler L. The treatment of fractures, ed 5. New York, London,Grune and Stratton, pp 882-883
11. Oni OO, MacKenny RP (1986) Multiple dislocations of thecarpometacarpal joints. J Hand Surg Br 11(1):47–48
12. Green D (2005) Operative hand surgery, 5th ed. ChurchillLivingstone
Fig. 5 Right hand AP & oblique radiographs post- reduction andpercutaneous wire fixation
Eur J Plast Surg (2011) 34:57–59 59