Simbarashe Takuva, AIDS 2010. Durability of first line antiretroviral therapy in Swaziland
25
Durability of First Line Antiretroviral Therapy : Reasons and Predictive Factors for Treatment Modifications in a Swaziland Cohort Simbarashe Takuva 1, 2 , Goedele Louwagie 1 , Khangelani Zuma 1, 3 , Velephi Okello 2 1 School of Health Systems & Public Health, Faculty of Health Sciences , University of Pretoria 2 Ministry of Health and Social Welfare, Mbabane, Swaziland 3 Human Sciences Research Council , Pretoria, South Africa
-
Upload
simbarashe-takuva -
Category
Health & Medicine
-
view
472 -
download
0
Transcript of Simbarashe Takuva, AIDS 2010. Durability of first line antiretroviral therapy in Swaziland

Durability of First Line Antiretroviral Therapy : Reasons and
Predictive Factors for Treatment Modifications in a Swaziland
Cohort
Simbarashe Takuva 1, 2 , Goedele Louwagie 1 , Khangelani Zuma 1, 3 , Velephi Okello 2
1 School of Health Systems & Public Health, Faculty of Health Sciences , University of Pretoria2 Ministry of Health and Social Welfare, Mbabane, Swaziland3 Human Sciences Research Council , Pretoria, South Africa

BACKGROUND
High burden of HIV / AIDS in sub-Saharan Africa
Swaziland has highest prevalence in the world
ART has reduced morbidity and mortality
W.H.O 3 x 5 initiative resulted in rapid scale up
At least 35 000 on treatment by beginning of 2009
No data available for drug tolerability and durability

BACKGROUND : Rationale
Optimizing initial ART regimens in terms of durability and
efficacy is paramount for the prognosis of patients initiating
treatment
Where drug options are limited, it is important to understand
the reasons and risk factors that may lead to poor tolerability
of ART
This will help to individualize drug regimens among patients
Most studies done in resourceful settings. Generalizability
difficult

BACKGROUND : SOPs
Initiation of ART based on CD4 counts and WHO staging
FBC, AST/ALT and CD4 count done at baseline
First line options:
NVP-3TC-d4T
NVP-3TC-AZT
Visits – 2weeks,1, 2, 3 months and then 6 monthly
Patients screened by nurses at all visits

BACKGROUND : Aim of the study
To identify reasons for first line antiretroviral
modifications
• To examine risk factors for first line antiretroviral
modifications

METHODS : Study setting
The Mbabane Government Hospital ART Unit is the largest HIV
outpatient clinic in Swaziland.
Currently 15 800 patients, of which 7 000 are presently on ART [2009]
Standard WHO adapted treatment and care guidelines are followed
Clinic records are kept both in a paper-based form and in an electronic
database
A home-based follow-up system is currently undergoing finalization

METHODS : Study design and population
• We conducted a retrospective cohort study
• We included patients who met the following criteria :
1. HIV-infected adults older than 18 years
2. Initiated 1st line ART between 1 March 2006 and 31 May 2008
3. ART naive
4. The end-date for the follow-up was 31 December 2008
5. At least 2 recorded visits
6. Available essential patient information
METHODS : Data issues
Three main data sources
1. Database (an excel database structure recently introduced)
2. Patient clinical notes
3. Patient handheld booklet (used for pharmacy refills)
Data entered into Epi-Data (with double data entry)
Missing values – patients with missing values listed and files
excluded
Data Epi-Data exported from Epi-Data TM to STATA version 10 for
analysis
METHODS : Statistical analysis
Categorical data – proportions and continuous data – medians and
means for non-normally distributed data
Study time – date of ART initiation to the date of ART modification or
censorship
Patients were censored at the date of lost to follow up, last visit date ,
death or date of transfer out
Log – rank test and Kaplan-Meier plots were used to compare survival
time between any 2 compared groups
• Piecewise Cox proportional hazards regression model used for the multivariate analysis (proportionality violation)
METHODS : Ethical considerations
Ethics approval from the Ministry of Health and Social Welfare
Ethics Committee, Swaziland and also from the Ethics Committee
of the University of Pretoria’s Faculty of Health Sciences

RESULTS :Baseline Characteristics
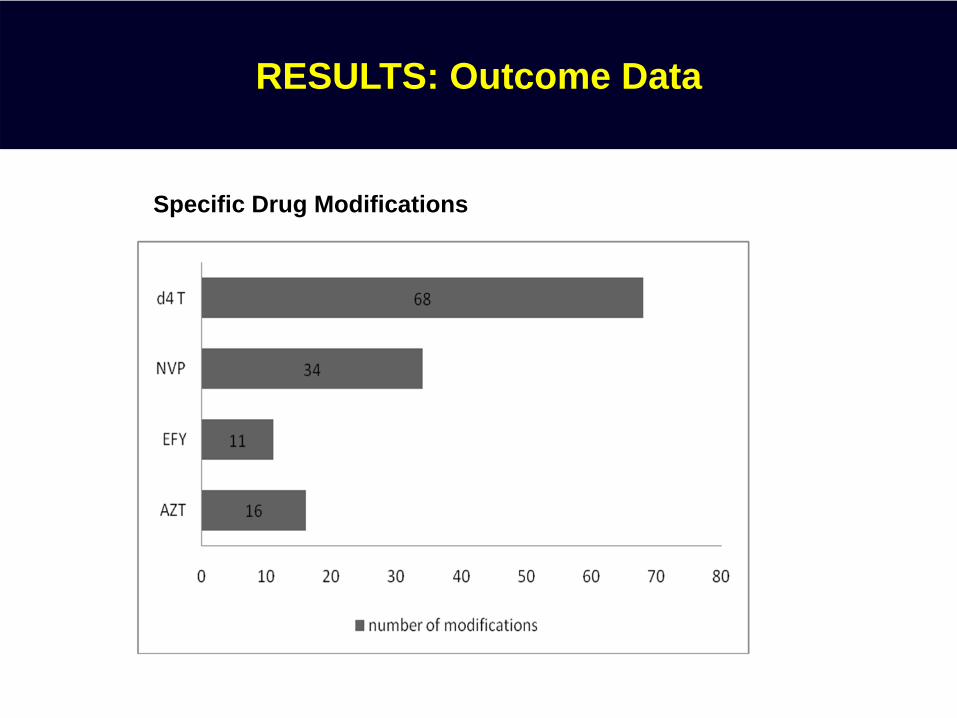
RESULTS: Outcome Data
Specific Drug Modifications
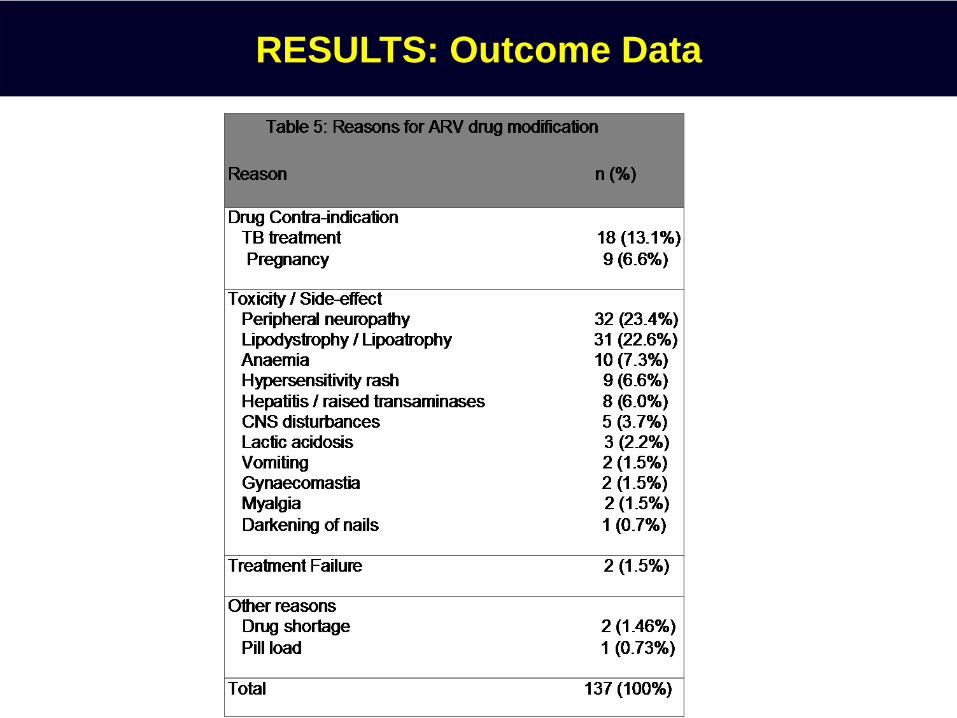
RESULTS: Outcome Data

RESULTS: Outcome Data
Regimen Incidence rate
d4T-based regimen 11.3 per 1 000 person-years of follow-up
AZT-based regimen 6.1 per 1 000 person-years of follow-up
NVP-based regimen 9.5 per 1 000 person-years of follow-up
EFV-based regimen 6.0 per 1 000 person-years of follow-up
Time on treatment Probability modifying treatment (95% CI)
6 months 0.04 (0.03-0.06)
12 months 0.08 (0.06-0.10)
18 months 0.12 (0.10-0.15)
24 months 0.18 (0.15-0.22)
36 months 0.33 (0.27-0.40)
Incidence rates for treatment change by regimen
Probability of modification according to time on treatment

RESULTS : Cumulative hazard estimates for modification
Fig 2: Cumulative proportion modifying ART regimen by baseline CD4 category statusFig 1: Cumulative proportion modifying ART regimen
Fig 3: Cumulative proportion modifying ART regimen by baseline weight category status
Fig 4: Cumulative proportion modifying ART regimen by baseline NTRI regimen status
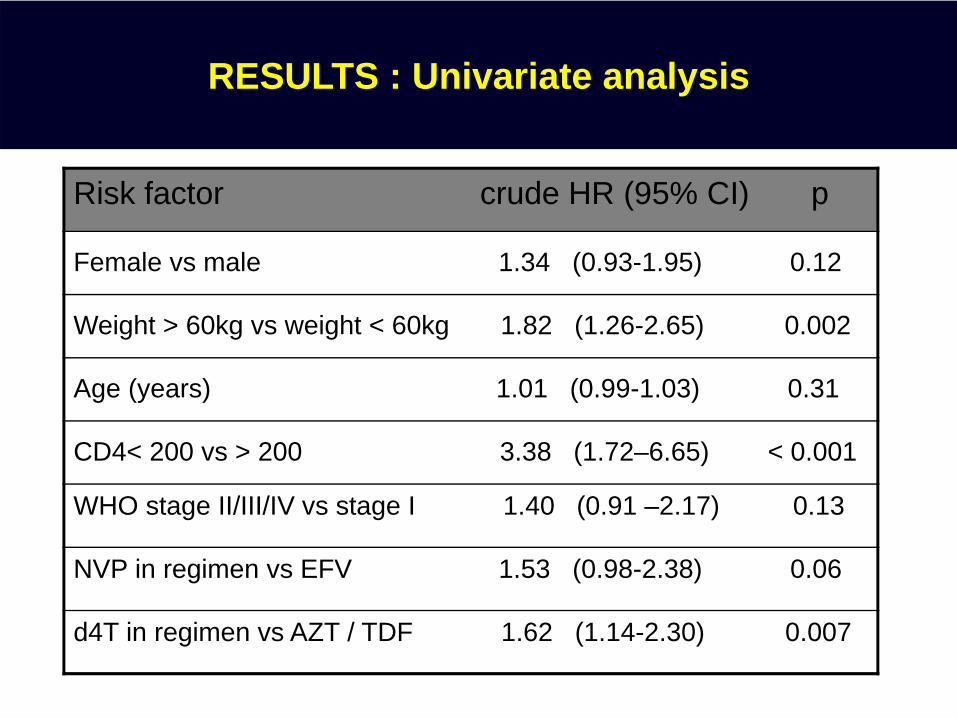
RESULTS : Univariate analysis
Risk factor crude HR (95% CI) p
Female vs male 1.34 (0.93-1.95) 0.12
Weight > 60kg vs weight < 60kg 1.82 (1.26-2.65) 0.002
Age (years) 1.01 (0.99-1.03) 0.31
CD4< 200 vs > 200 3.38 (1.72–6.65) < 0.001
WHO stage II/III/IV vs stage I 1.40 (0.91 –2.17) 0.13
NVP in regimen vs EFV 1.53 (0.98-2.38) 0.06
d4T in regimen vs AZT / TDF 1.62 (1.14-2.30) 0.007

RESULTS: Multivariate analysis
Multivariate piecewise Cox proportional hazards model
Risk factor Adjusted Hazard Ratios (95% CI)
duration < 11 months duration > 11 months
d4T in regimen vs AZT / TDF in regimen 1.41 (0.82 – 2.44) 2.64 (1.56 – 4.46)
Weight > 60kg vs weight < 60kg 1.22 (0.71 – 2.11) 2.40 (1.43 – 4.04)
CD4< 200 cells/mm3 vs > 200 cells/mm3 1.14 (0.45 – 2.90) 4.42 (1.62 – 12.1)
Gender 1.26 (0.59 – 2.70) 1.56 (0.86 – 2.85)
Age 0.98 (0.95 – 1.02) 1.03 (1.00 – 1.05)
DISCUSSION
overall, a high proportion of patients are able to tolerate their initial
antiretroviral regimen
lack of alternative treatment options in a RLS
current guidelines are rigid 1
less informed patients
1. World Health Organization , 2006.
DISCUSSION
Toxicity related reasons resulted in most modifications
gastrointestinal toxicities – the most commonly reported toxicities
resulting in treatment modification, especially in resource-rich
cohorts 1-4
burden of peripheral neuropathy and lipodystrophy related to
d4T use was of major concern. Similar findings in Cape Town 5
1. Youle M, et al. AIDS 1998. 2. Hansel A,et al. J Acquir Immune Defic Syndr. 2001. 3.Mocroft A, et al. AIDS 2001. 4. Jeanne P, et al. AIDS 2002. 5. Coetzee D, et al. AIDS 2004.

DISCUSSION
modification due to anaemia related to AZT toxicity were
significant (7.3 % of the modifications). DART trial similar 1
NVP in a treatment regimen was well tolerated, accounting for
less than 10% of the reasons for modification.
The latter is in contrast to resource-rich settings (NVP) 2,3
1. Ssali F, et al. Antiviral Ther 11:741-749. 2. MMWR Morb Mortal Wkly Rep 2001. 3. Wit FWNM, et al. J Infect Dis 2002.

DISCUSSION
Another concern : significant number of modifications due to starting
TB therapy (13%) and incident pregnancy (6.6% of reasons)
clearly emphasizes the burden of TB in this setting and brings
out the need for more aggressive TB screening in patients
initiating ART
family planning programmes also need to be routinely integrated
into routine HIV care, to prevent unplanned and unwanted
pregnancies. Patients most likely to become pregnant need to be
identified early on during their treatment

DISCUSSION
Patients initiating ART with lower CD4 cell counts had poor regimen
durability (almost 4 X likely to modify) 1,2
Weight at initiating ART was also a very strong risk factor for
modification (weight over 60 kg: almost 3 x the hazards).
may have been on the d4T 40mg regimen.
heavier patients have also been shown by some studies to be
more susceptible to mitochondrial-related toxicities 3,4
1. IAS , 2008. 2.Ssali F, et al. Antiviral Ther 2009. 3. Moh R ,et al. Antivir Ther 2005. 4.Youle M,et al. AIDS 1998.
DISCUSSION : Limitations
Lots of data with missing values – don’t know if this was influential
on our outcome or was data MCAR
Misclassification bias – information not recorded accurately during
clinic visits
The analysis of a single treatment site may just reflect practices at
this particular site
Informative censoring bias – underestimates outcome

DISCUSSION : Recommendations
1. Early initiation of ART , at higher CD4 cell counts
2. Avoiding drugs with poor toxicity profiles especially Stavudine
(d4T)
3. Before ART initiation, those individuals who may require therapy
for TB or who may become pregnant must be identified promptly
and the appropriate regimen started
4. Develop simple evidence-based algorithms to individualize patient
ART regimens

Acknowledgements
• This study is dedicated to the patients of the Mbabane
Government Hospital Antiretroviral Therapy Unit
• Dr Marian Calnan for conceptual discussions
• Data collection team : Sicelo Zondo, Delisile Mavimbela,
Muzomuhle Stewart and Sicelo Dlamini
• The School of Health Systems and Public Health, Faculty of
Health Sciences , University of Pretoria
• Clinical staff of the study site and the Ministry of Health and Social
Welfare, Swaziland