
Side effects of new and old HCV...
59
Massimo Puoti Dept. of Infectious Diseases AO Ospedale Niguarda Cà Granda Milan, Italy Side effects of new and old HCV medications
Transcript of Side effects of new and old HCV...

Massimo Puoti
Dept. of Infectious Diseases
AO Ospedale Niguarda Cà Granda
Milan, Italy
Side effects of new and old HCV medications
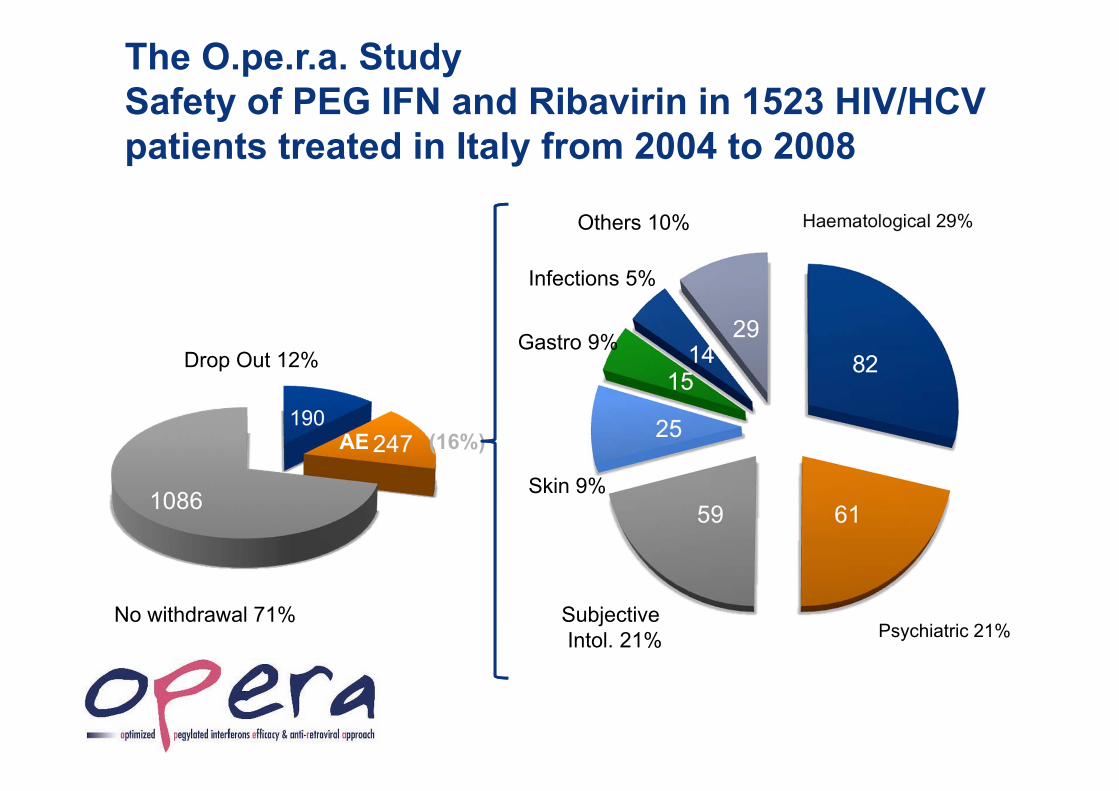
The O.pe.r.a. StudySafety of PEG IFN and Ribavirin in 1523 HIV/HCV patients treated in Italy from 2004 to 2008
Psychiatric 21%SubjectiveIntol. 21%
Skin 9%
Gastro 9%
Infections 5%
Others 10%
No withdrawal 71%
Drop Out 12%
AE (16%)

• 750 mg (two 375-mg tablets) q8hr with food (not low fat; standard fat meal is 21 g)
No eRVR or cirrhosis; PR
Telaprevir in Genotype 1 Patients
TVR + PReRVR non cirrhosis; stop at Wk 24: 63%
PR
Telaprevir [package insert]. May 2011. EMA. Telaprevir [package insert] 2011.
Time Point Criterion Stopping RuleWk 4 or 12 HCV RNA > 1000 IU/mL Discontinue all therapyWk 24 Detectable HCV RNA Discontinue PRAny Discontinuation of PR for any reason Discontinue TVR
Treatment Naive and Previous Relapsers
Previous Partial or Null Responders
TVR + PR
480 24124
PR
eRVR: HCVRNA undetectable at 4 & 12 weeks
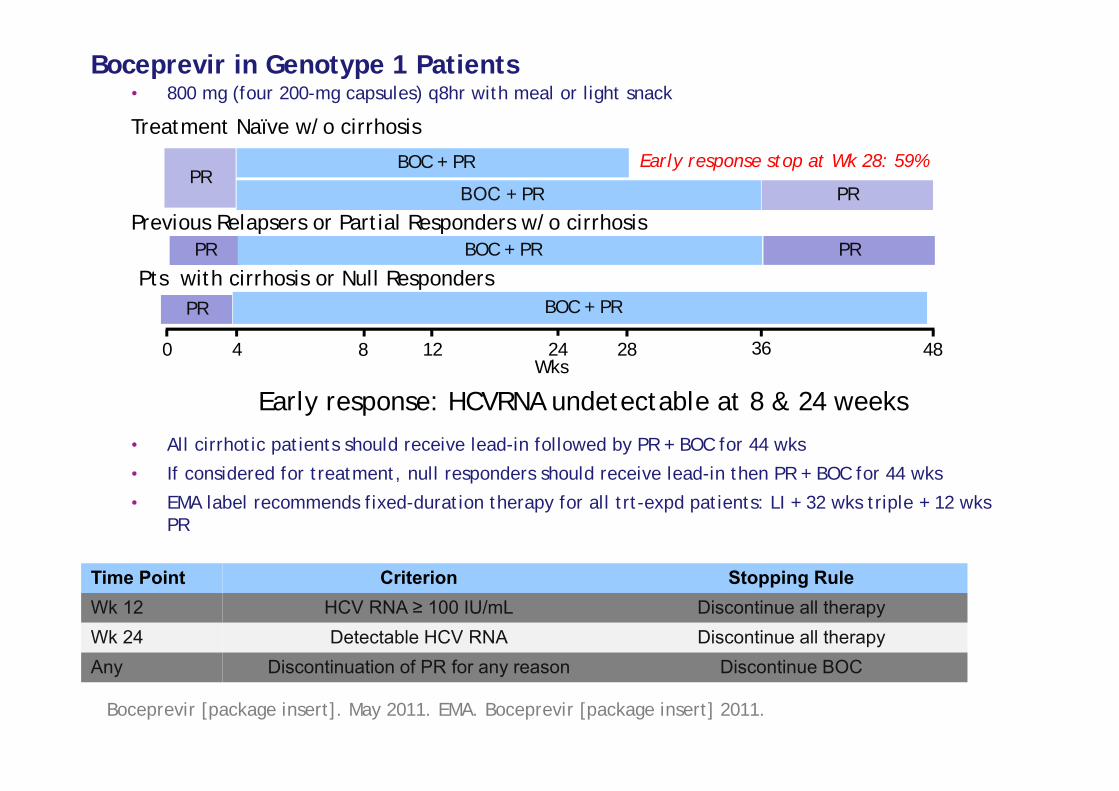
Boceprevir in Genotype 1 Patients• 800 mg (four 200-mg capsules) q8hr with meal or light snack
• All cirrhotic patients should receive lead-in followed by PR + BOC for 44 wks
• If considered for treatment, null responders should receive lead-in then PR + BOC for 44 wks
• EMA label recommends fixed-duration therapy for all trt-expd patients: LI + 32 wks triple + 12 wks PR
BOC + PR
PRPR
BOC + PR
Boceprevir [package insert]. May 2011. EMA. Boceprevir [package insert] 2011.
Treatment Naïve w/o cirrhosis
Previous Relapsers or Partial Responders w/o cirrhosis
Wks480 28124
PRPR
8 36
BOC + PR
24
Time Point Criterion Stopping RuleWk 12 HCV RNA ≥ 100 IU/mL Discontinue all therapyWk 24 Detectable HCV RNA Discontinue all therapyAny Discontinuation of PR for any reason Discontinue BOC
Early response stop at Wk 28: 59%
Early response: HCVRNA undetectable at 8 & 24 weeks
PR BOC + PRPts with cirrhosis or Null Responders
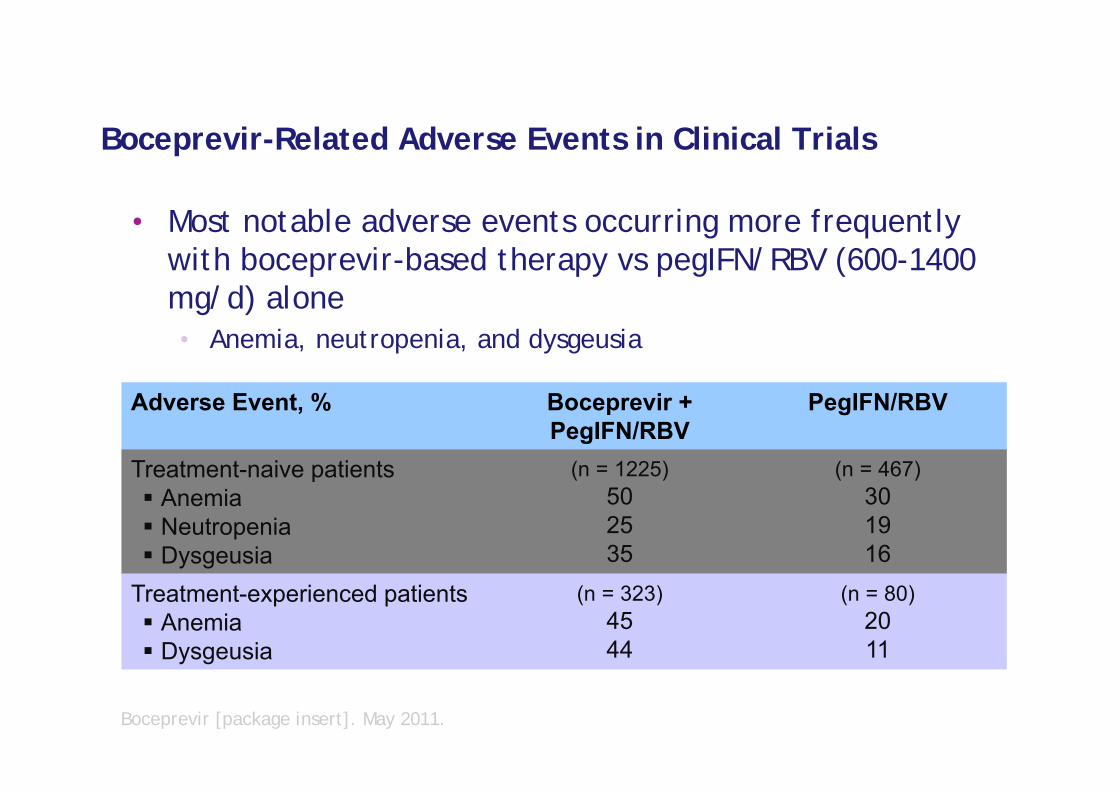
Boceprevir-Related Adverse Events in Clinical Trials
• Most notable adverse events occurring more frequently with boceprevir-based therapy vs pegIFN/RBV (600-1400 mg/d) alone• Anemia, neutropenia, and dysgeusia
Adverse Event, % Boceprevir + PegIFN/RBV
PegIFN/RBV
Treatment-naive patients Anemia Neutropenia Dysgeusia
(n = 1225)502535
(n = 467)301916
Treatment-experienced patients Anemia Dysgeusia
(n = 323)4544
(n = 80)2011
Boceprevir [package insert]. May 2011.
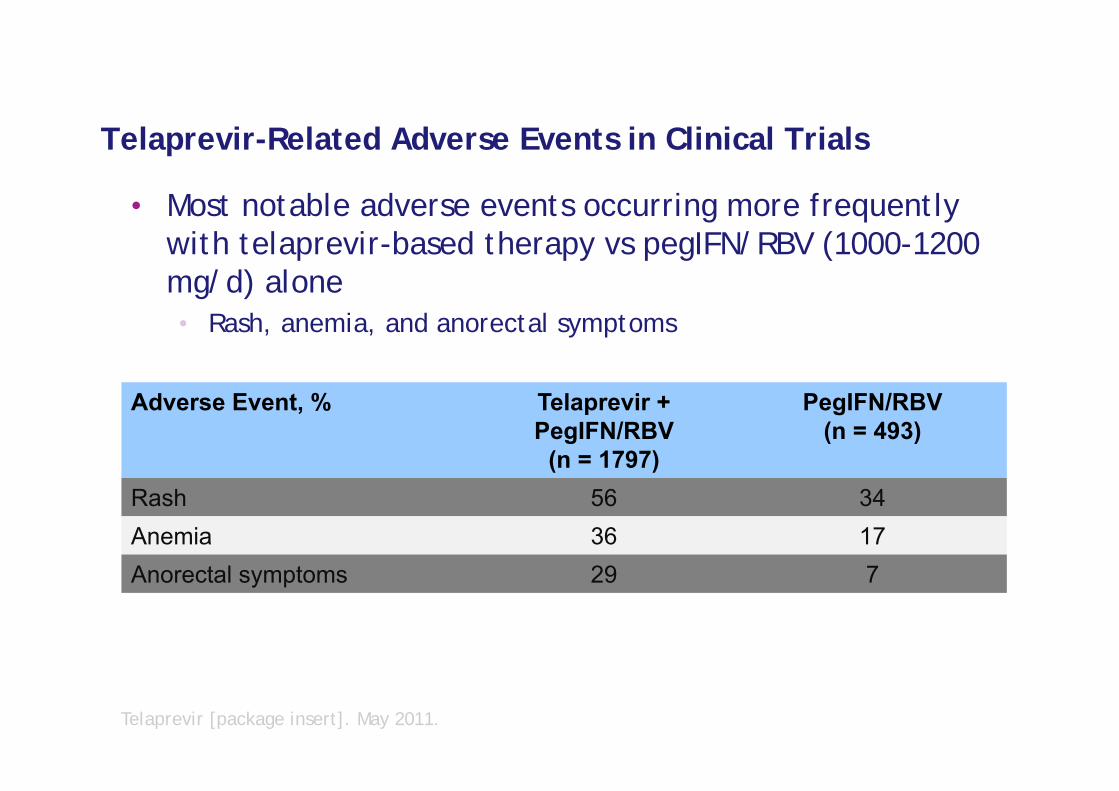
Telaprevir-Related Adverse Events in Clinical Trials
• Most notable adverse events occurring more frequently with telaprevir-based therapy vs pegIFN/RBV (1000-1200 mg/d) alone• Rash, anemia, and anorectal symptoms
Adverse Event, % Telaprevir + PegIFN/RBV
(n = 1797)
PegIFN/RBV(n = 493)
Rash 56 34Anemia 36 17Anorectal symptoms 29 7
Telaprevir [package insert]. May 2011.

Safety and tolerability with DAAs
Common AEs with PR include:1–3
– Fatigue, headache, nausea, pyrexia and myalgia– Anemia and neutropenia– Depression, irritability and insomnia– Rash
Additional management considerations with DAAs– Telaprevir:4–6 Rash, Anorectal symptoms, Anemia– Boceprevir:7,8 Anemia and Dysgeusia
1. Pegintron EMA Summary of Product Characteristics; 2. Pegasys EMA Summary of Product Characteristics3. Rebetol EMA Summary of Product Characteristics; 4. Jacobson IM, et al. Hepatology 2010;52(Suppl.):427A
5. Sherman KE, et al. Hepatology 2010;52(Suppl.):401A; 6. Foster GR, et al. Hepatol Int 2011;5(Suppl. 1):147. Poordad F, et al. NEJM 2011;364:1195–206; 8. Bacon BR, et al. N Engl J Med 2011;364:1207–17AE: adverse event
Side Effects of new and old HCV medications
Rash Anorectal disorders Anemia Side effects in cirrhotics Side effects in HIV DDI in the management of AE
8

Side Effects of new and old HCV medications
Rash Anorectal disorders Anemia Side effects in cirrhotics Side effects in HIV DDI in the management of AE
9

Summary of rash data from placebo-controlled Phase II and III trials: telaprevir treatment phase
>90% of all rash = mild/moderate
Inci
denc
e of
rash
(%)
Features: Typically pruritic and eczematous, and involving <30% BSA Progression was infrequent (<8% of cases)
Time to onset: Approximately 50% of rashes started during the first 4 weeks But rash can occur at any time during telaprevir treatment
Inci
denc
e of
rash
(%)
http://www.fda.gov/downloads/AdvisoryCommittees/CommitteesMeetingMaterials/Drugs/AntiviralDrugsAdvisoryCommittee/UCM252562.pdf;
Data on file: TVR/DoF/January2011/EMEA01
(N=1346) (N=764)
Reported within a special search category

Summary of rash data from Phase II and III placebo-controlled trials:* discontinuations
*During telaprevir treatment phase; analyzed within SSC
Improvement of rash occurs after telaprevir discontinuation Rashes may take weeks for complete resolution
Dis
cont
inua
tions
(%)
Dis
cont
inua
tions
(%)Telaprevir alone All treatment at the
same time
INCIVO (telaprevir) draft EU SmPC [TBC]

Grading of skin eruption severity
Mild: localized skin eruption and/or a skin eruption with limited distribution (up to several isolated sites on the body)
Moderate: diffuse rash involving ≤50% of body surface area
Severe: extent of rash >50% of body surface area or associated with significant systemic symptoms, mucous membrane ulceration, target lesions, epidermal detachment
SCAR: generalized bullous eruption, drug rash with eosinophilia and systemic symptoms (DRESS), Stevens-Johnson Syndrome (SJS)/toxic epidermal necrolysis (TEN), acute generalized exanthematous pustulosis (AGEP), erythema multiforme (EM)
INCIVO (telaprevir) draft EU SmPC [TBC]

Mild rash Moderaterash
Severerash

Estimating body surface area (BSA)
9%
9%
Front18%
Back18% 9%
18% 18%
Hettiaratchy S, et al. BMJ 2004;329:101–3
Adult body BSA
Perineum 1%
Arm 9%
Head (front and back) 9%
Leg 18%
Chest 18%
Back 18%
Roujeau JC, Stern RS. N Eng J Med 1994;331:1272–85Roujeau JC, et al. Dermatol Sinica 2009;27:203–9; Mockenhaupt M. J Dtsch Dermatol Ges 2009;7:142–160
http://www.fda.gov/downloads/AdvisoryCommittees/CommitteesMeetingMaterials/Drugs/AntiviralDrugsAdvisoryCommittee/UCM252562.pdf
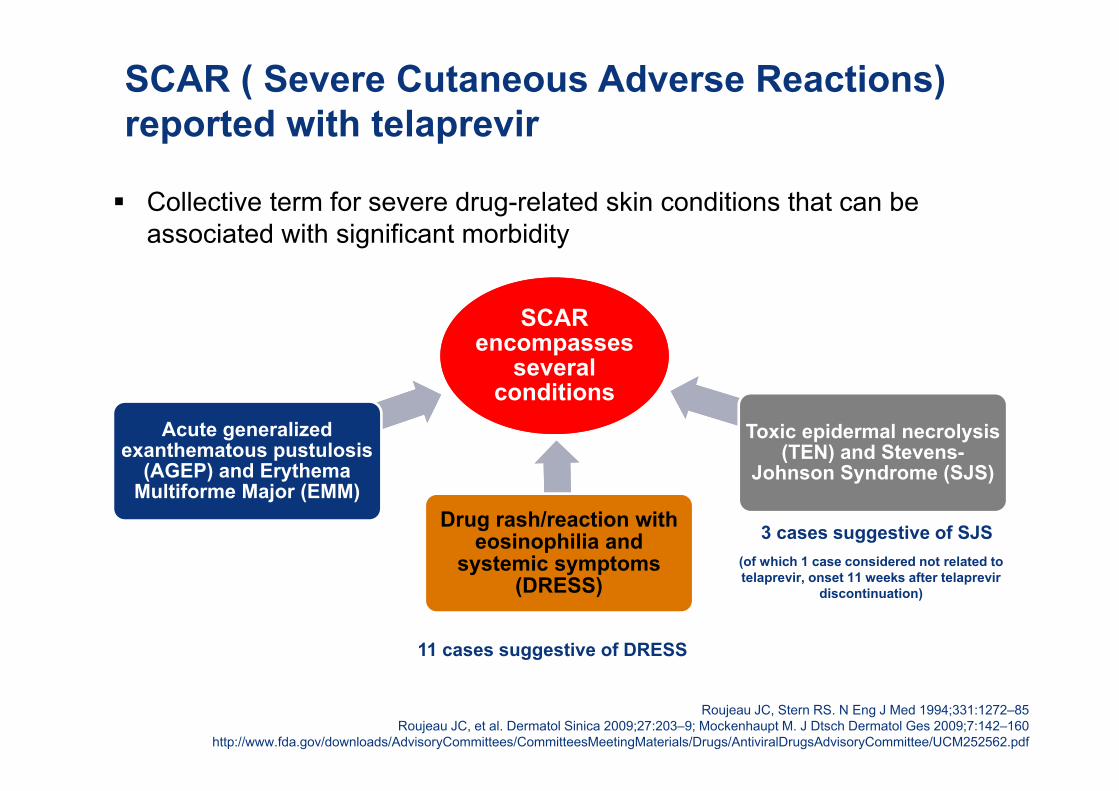
Collective term for severe drug-related skin conditions that can be associated with significant morbidity
SCAR ( Severe Cutaneous Adverse Reactions) reported with telaprevir
3 cases suggestive of SJS
11 cases suggestive of DRESS
(of which 1 case considered not related to telaprevir, onset 11 weeks after telaprevir
discontinuation)
SCAR encompasses
several conditions
Acute generalizedexanthematous pustulosis
(AGEP) and Erythema Multiforme Major (EMM)
Drug rash/reaction with eosinophilia and
systemic symptoms (DRESS)
Toxic epidermal necrolysis (TEN) and Stevens-
Johnson Syndrome (SJS)

Telaprevir interruption guidance
Rash
Mild
Moderate
Severe
TELAPREVIR must not be restarted if discontinued
SCAR
Permanently discontinue telaprevir immediatelyMonitor for progression or systemic symptoms until the rash is resolved. If no improvement within 7 days of stopping telaprevir (or earlier if rash worsens), sequential or simultaneous interruption or discontinuation of ribavirin and/or peginterferon should be considered
Permanent and immediate discontinuation of telaprevir, peginterferon and ribavirin is required
Monitor for progression or systemic symptoms until the rash is resolved
INCIVO (telaprevir) draft EU SmPC [TBC]
Monitor for progression or systemic symptoms until the rash is resolved For moderate rash that progresses, permanent discontinuation of telaprevir should be considered. For moderate rash that progresses to severe (≥50% body surface area), permanently discontinue telaprevir

Drug considerations: mild and moderate rash
Treating patients with mild or moderate rash Use topical corticosteroids Permitted topical antihistaminic drugs may be tried Limit exposure to sun/heat Suggest baking soda or oatmeal baths, and loose-fitting clothes Treatment of rash with systemic corticosteroids is not recommended*
Rash
Mild
Moderate
Monitor for progression or systemic symptoms until the rash is resolved
For moderate rash that progresses, permanent discontinuation of telaprevir should be considered
If the rash does not improve within 7 days following telaprevir discontinuation, ribavirin should be interrupted. Interruption of ribavirin may be required sooner if the rash worsens despite discontinuation of telaprevir
Peginterferon alfa may be continued unless interruption is medically indicated
For moderate rash that progresses to severe (≥50% body surface area), permanently discontinue telaprevir
*Concomitant telaprevir and systemic dexamethasone should be used with caution or alternatives should be considered. Co-administration with fluticasone or budesonide is not recommended unless the potential benefit outweighs the risk of corticoseroid side effects INCIVO (telaprevir) draft EU SmPC [TBC]

When to suspect DRESS
Roujeau JC, et al. Dermatol Sinica 2009; 27:203–209Walsh SA, et al. Clin Exp Dermatol 2011;36:6–11
Jeung Y-J, et al. Allergy Asthma Immunol Res 2010;2:123–126Wolf R, et al. Clin Dermatol 2005;23:171–181
Alarm signs: – Relatively late eruption (2–6 weeks
after treatment initiation)– Prolonged fever >38.5°C– Facial oedema– Lymphadenopathy (at least 2 sites)
What to do? Check for biological alterations
– Eosinophilia (absolute count and/or %)– Atypical lymphocytes– Leucocytosis– Lymphocytosis– Involvement of at least one internal
organ (liver, kidney, lungs); raised alanine aminotransferase, creatinine
– Platelet levels below normal
If DRESS is suspected– Stop all drugs– Hospitalize the patient

When to suspect SJS/TEN
Roujeau JC, et al. Dermatol Sinica 2009; 27:203–209; French LE, et al. Allergol Int 2006;55:9–16 Jeung Y-J, et al. Allergy Asthma Immunol Res 2010;2:123–126; Mockenhaupt M, et al. J Invest Dermatol 2008;128:35–44
Acute onset and rapid progression of skin and mucous lesions– Small blisters arising on purple macules, widespread and
usually predominantly on the trunk– Severe and painful erosions of mucous membranes
(buccal, ocular, genital) Epidermal detachment led by confluence of blisters
– Stevens-Johnson Syndrome: 1–10% of body surface area– Toxic epidermal necrolysis: >30% of body surface area)
Positive Nikolsky sign (epidermis detaches easily under lateral pressure with thumb)
High fever Erythema
What to do? Stop all drugs
Hospitalize the patient
Get dermatological advice

Side Effects of new and old HCV medications –Key messages
Rash frequent with TPV close monitoring, management plan and identification of SCAR might reduce its impact on Treatment safety and efficacy
20

Side Effects of new and old HCV medications
Rash Anorectal disorders Anemia Side effects in cirrhotics Side effects in HIV DDI in the management of AE
21
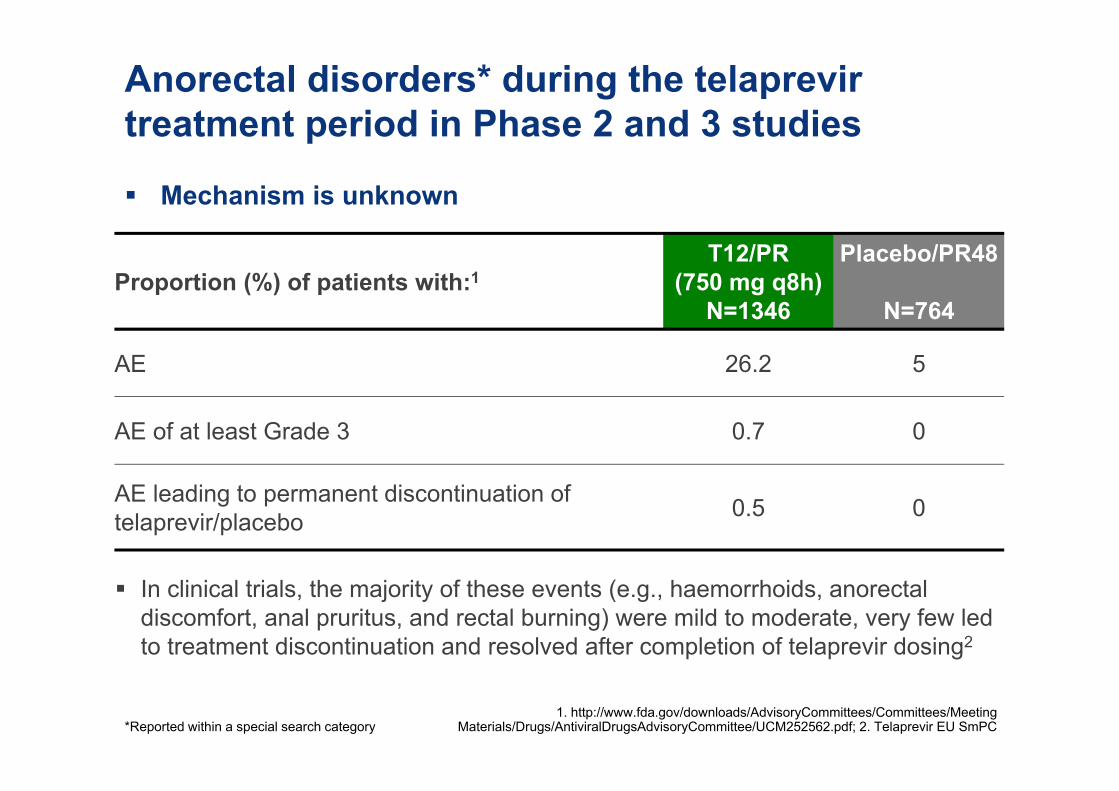
Anorectal disorders* during the telaprevir treatment period in Phase 2 and 3 studies
Mechanism is unknown
*Reported within a special search category1. http://www.fda.gov/downloads/AdvisoryCommittees/Committees/Meeting
Materials/Drugs/AntiviralDrugsAdvisoryCommittee/UCM252562.pdf; 2. Telaprevir EU SmPC
Proportion (%) of patients with:1T12/PR
(750 mg q8h)N=1346
Placebo/PR48
N=764
AE 26.2 5
AE of at least Grade 3 0.7 0
AE leading to permanent discontinuation of telaprevir/placebo 0.5 0
In clinical trials, the majority of these events (e.g., haemorrhoids, anorectal discomfort, anal pruritus, and rectal burning) were mild to moderate, very few led to treatment discontinuation and resolved after completion of telaprevir dosing2

Anorectal signs and symptoms: management
Standard, short-term symptomatic care may be warranted
Consider proprietary combination hemorrhoid preparations according to the nature of the event
Hézode C. Liver International 2012;32 Suppl 1:32-8
Topical local anaesthetics
(e.g. lidocaine2% cream)
Topical local anaesthetics
(e.g. lidocaine2% cream)
Topical cortico-steroids
Topical cortico-steroids
Anti-histamines
Anti-histamines

Side Effects of new and old HCV medications –Key messages
Rash frequent with TPV close monitoring, management plan and identification of SCAR might reduce its impact on Treatment safety and efficacy
Anorectal discomfort is frequent but manegeable with prompt symptomatic treatment
24
Side Effects of new and old HCV medications
Rash Anorectal disorders Anemia Side effects in cirrhotics Side effects in HIV DDI in the management of AE
25

Summary of anemia data from Phase II and III placebo-controlled studies
Incidence and severity of anemia increased with telaprevir combination treatment compared with PR alone
T12/PR Control T12/PR Control
Hemoglobin <10 g/dL Hemoglobin <8.5 g/dL
Pat
ient
s (%
)
INCIVO (telaprevir) draft EU SmPC [TBC]

Summary of anemia data from the boceprevir SPRINT-2 study over course of therapy
Incidence and severity of anemia increased with boceprevir combination treatment compared with PR alone
BOC RGT
Control
Hemoglobin <10 to 8.5 g/dL Hemoglobin <8.5 g/dL
Pat
ient
s (%
)
BOC44/PR48
BOC RGT
ControlBOC44/PR48
Poordad F, et al. N Engl J Med 2011;364:1195–206

Management of anemia observed with telaprevir and boceprevir in clinical trials
Telaprevir Phase II/III placebo-
controlled trials1
Boceprevir Phase III trials2,3
Ribavirin dose reductions due to anemia
21.6% (telaprevir arms) vs 9.4% (control)
21% (boceprevir arms) vs 13% (control)*
EPO use Not permitted (1% use) 41–46% (boceprevir arms) vs 21–24% (control)
Transfusions
Telaprevir/placebo dosing phase: 2.5% (telaprevir arms) vs 0.7% (control) Overall study period:4.6% (telaprevir arms) vs 1.6% (control)
2–9% (boceprevir arms) vs 0–1% (control)
Discontinuation
Telaprevir alone: 1.9%All treatment at the same time: 0.9% (telaprevir arm) vs 0.5% (control)
0–3% (boceprevir arms) vs 0–1% (control)
1. INCIVO (telaprevir) draft EU SmPC [TBC] 2. Poordad F, et al. N Engl J Med 2011;364:1195–206
3. Bacon BR, et al. N Engl J Med 2011;364:1207–17 *SPRINT-2 data only2

SVR by minimum RBV dose/day during telaprevir/Pbo treatment phase (1 of 2)
Patie
nts
with
SVR
(%)
n/N=
Never reduced
800–1000 mg
346/439
291/395
≤ 600 mg
38/51
Treatment-naïve patients
133/292
13/24
16/38
Never reduced
800–1000 mg
73/89
27/29
≤ 600 mg
20/24
Prior relapsers
11/55
2/7
2/6
PRT12/PR or T12/PR48
Pbo: placebo Sulkowski MS, et al. J Hepatol 2012;56 (Suppl 2):S459–S460
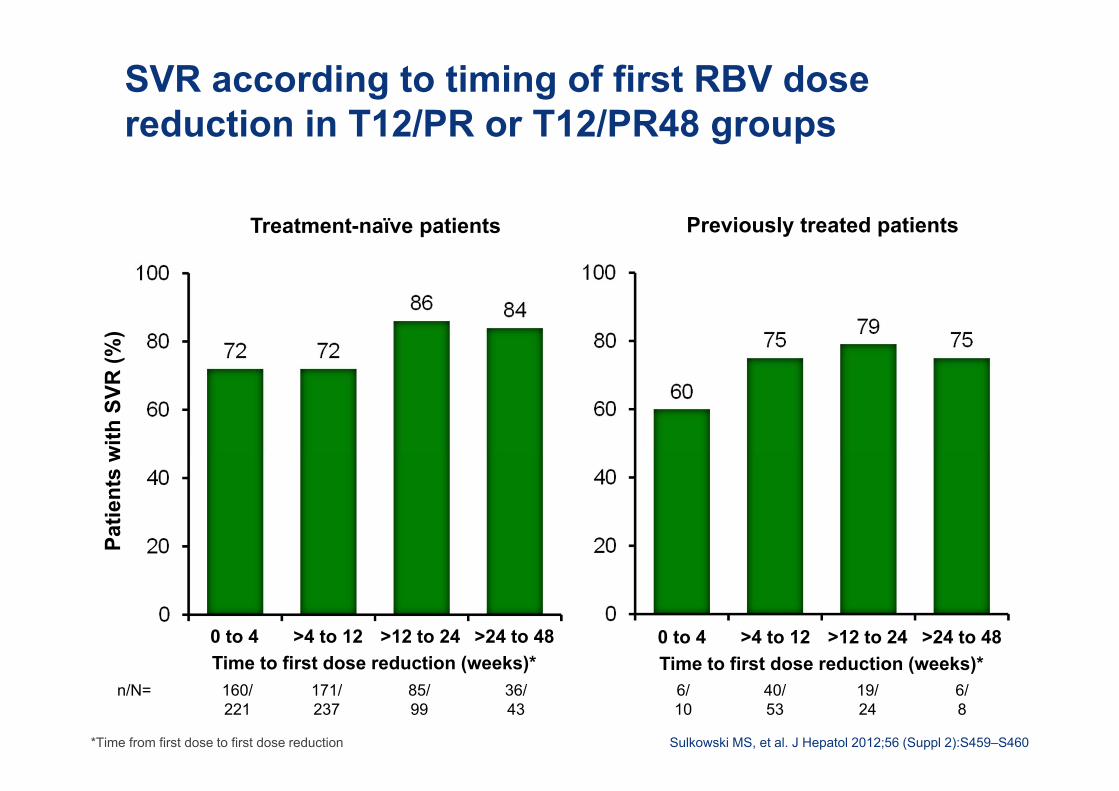
SVR according to timing of first RBV dose reduction in T12/PR or T12/PR48 groups
Patie
nts
with
SVR
(%)
n/N=
0 to 4 >4 to 12
160/221
85/99
>12 to 24
171/237
Treatment-naïve patients Previously treated patients
Time to first dose reduction (weeks)*>24 to 48
36/43
6/10
19/24
40/53
6/8
0 to 4 >4 to 12 >12 to 24Time to first dose reduction (weeks)*
>24 to 48
*Time from first dose to first dose reduction Sulkowski MS, et al. J Hepatol 2012;56 (Suppl 2):S459–S460
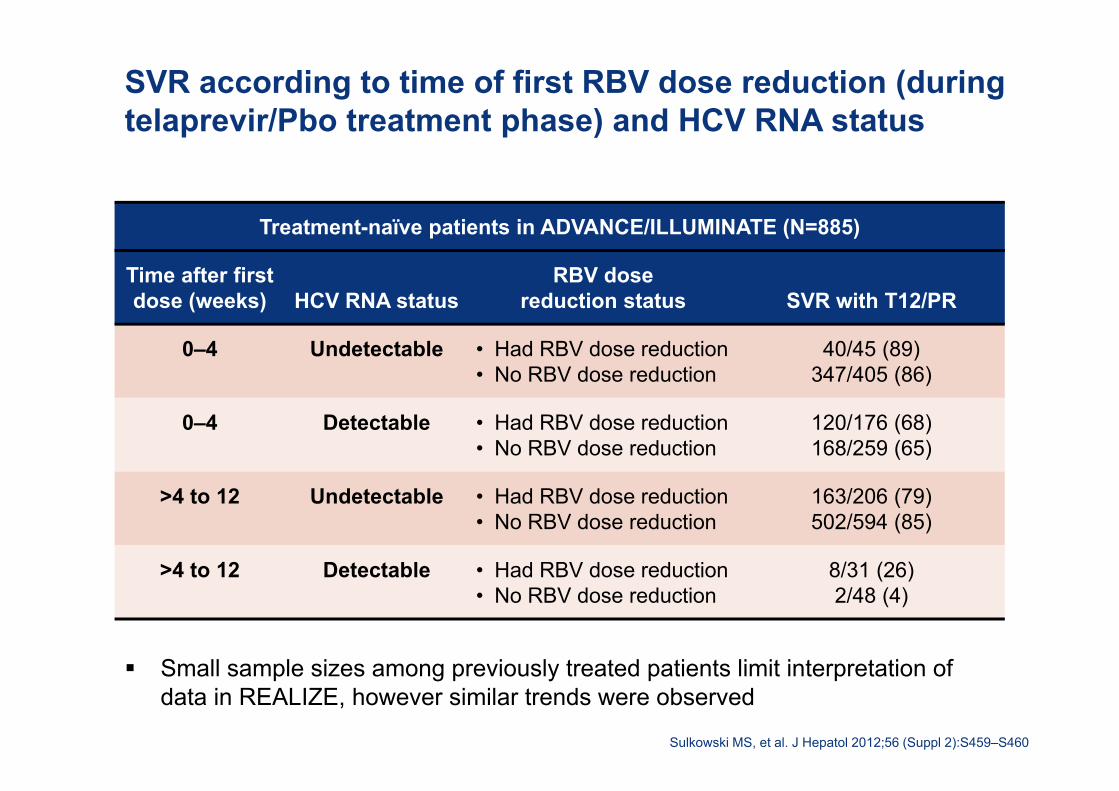
SVR according to time of first RBV dose reduction (during telaprevir/Pbo treatment phase) and HCV RNA status
Treatment-naïve patients in ADVANCE/ILLUMINATE (N=885)
Time after first dose (weeks) HCV RNA status
RBV dose reduction status SVR with T12/PR
0–4 Undetectable • Had RBV dose reduction• No RBV dose reduction
40/45 (89)347/405 (86)
0–4 Detectable • Had RBV dose reduction• No RBV dose reduction
120/176 (68)168/259 (65)
>4 to 12 Undetectable • Had RBV dose reduction• No RBV dose reduction
163/206 (79)502/594 (85)
>4 to 12 Detectable • Had RBV dose reduction• No RBV dose reduction
8/31 (26)2/48 (4)
Small sample sizes among previously treated patients limit interpretation of data in REALIZE, however similar trends were observed
Sulkowski MS, et al. J Hepatol 2012;56 (Suppl 2):S459–S460

SVR according to permanent RBV discontinuation during overall treatment phase and HCV RNA status (TVR)
Treatment-naïve patients in ADVANCE/ILLUMINATE (N=885)
HCV RNA status RBV discontinuation status SVR with T12/PR
Undetectable • Did not discontinue• Discontinued RBV
591/659 (90)84/171 (49)
Detectable • Did not discontinue• Discontinued RBV
0/8 (0)0/47 (0)
Small sample sizes among previously treated patients limit interpretation of data in REALIZE, however similar trends were observed
Sulkowski MS, et al. J Hepatol 2012;56 (Suppl 2):S459–S460
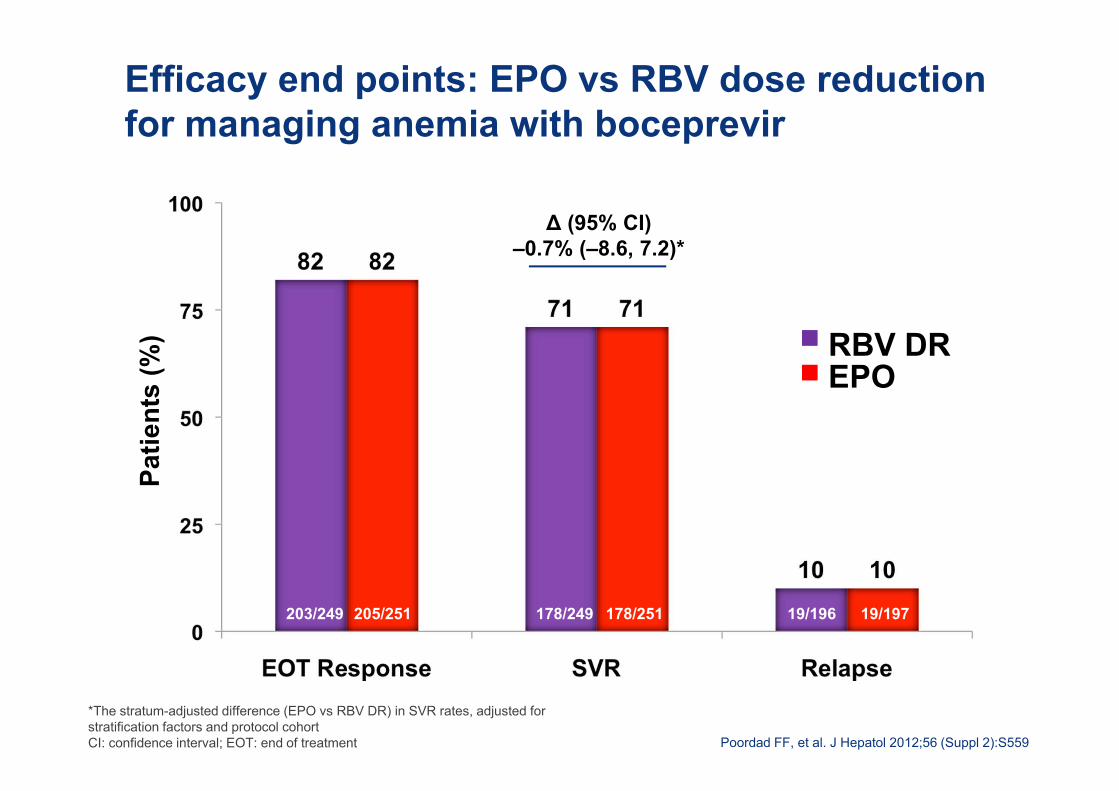
Efficacy end points: EPO vs RBV dose reduction for managing anemia with boceprevir
*The stratum-adjusted difference (EPO vs RBV DR) in SVR rates, adjusted for stratification factors and protocol cohortCI: confidence interval; EOT: end of treatment
Patie
nts
(%)
∆ (95% CI)–0.7% (–8.6, 7.2)*
203/249 205/251 178/249 178/251 19/196 19/197
Poordad FF, et al. J Hepatol 2012;56 (Suppl 2):S559
RBV DREPO

Side Effects of new and old HCV medications –Key messages
Rash frequent with TPV close monitoring, management plan and identification of SCAR might reduce its impact on Treatment safety and efficacy
Anorectal discomfort is frequent but manegeable with prompt symptomatic treatment
Anemia could be managed with ribavirin dose reduction without reducing treatment efficacy ( ribavirin overdosed?). Ribavirin withdrawal should be avoided
34
Side Effects of new and old HCV medications
Rash Anorectal disorders Anemia Side effects in cirrhotics Side effects in HIV DDI in the management of AE
35
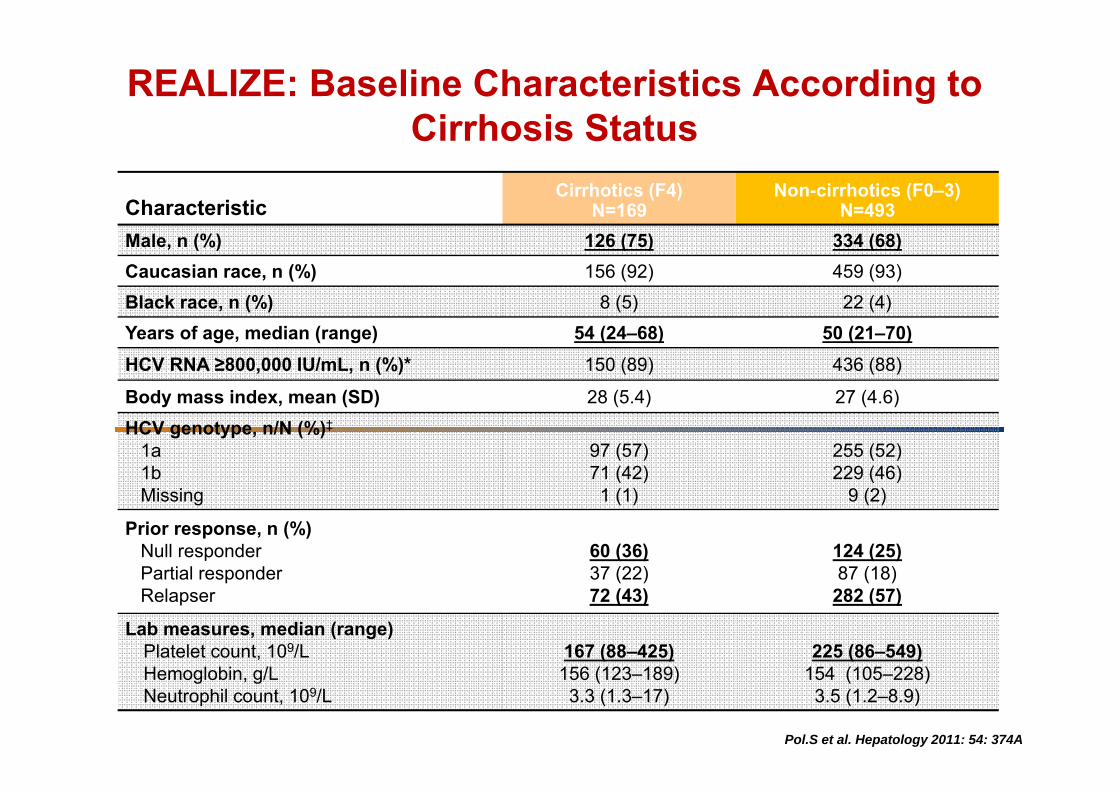
CharacteristicCirrhotics (F4)
N=169Non-cirrhotics (F0–3)
N=493Male, n (%) 126 (75) 334 (68)Caucasian race, n (%) 156 (92) 459 (93)Black race, n (%) 8 (5) 22 (4)Years of age, median (range) 54 (24–68) 50 (21–70)HCV RNA ≥800,000 IU/mL, n (%)* 150 (89) 436 (88)
Body mass index, mean (SD) 28 (5.4) 27 (4.6)
HCV genotype, n/N (%)‡
1a1bMissing
97 (57)71 (42)1 (1)
255 (52)229 (46)
9 (2)
Prior response, n (%)Null responderPartial responderRelapser
60 (36)37 (22)72 (43)
124 (25)87 (18)
282 (57)
Lab measures, median (range)Platelet count, 109/LHemoglobin, g/LNeutrophil count, 109/L
167 (88–425)156 (123–189) 3.3 (1.3–17)
225 (86–549)154 (105–228) 3.5 (1.2–8.9)
REALIZE: Baseline Characteristics According to Cirrhosis Status
Pol.S et al. Hepatology 2011: 54: 374A

REALIZE: AEs in ≥25% of TVR-treated Patients during Any Treatment Phase
AE, n (%)Cirrhotics (F4)
N=139Non-cirrhotics (F0–3)
N=391
Rash SSC 93 (67) 206 (53)
Pruritus SSC 82 (59) 205 (52)
Fatigue 62 (45) 214 (55)
Headache 54 (39) 167 (43)
Anemia SSC 59 (42) 134 (34)
Nausea 52 (37) 129 (33)
Influenza-like illness 55 (40) 124 (32)
Insomnia 39 (28) 113 (29)
Anorectal symptoms 33 (24) 101 (26)
Diarrhea 33 (24) 102 (26)
Pyrexia 34 (25) 97 (25)
Pol.S et al. Hepatology 2011: 54: 374A
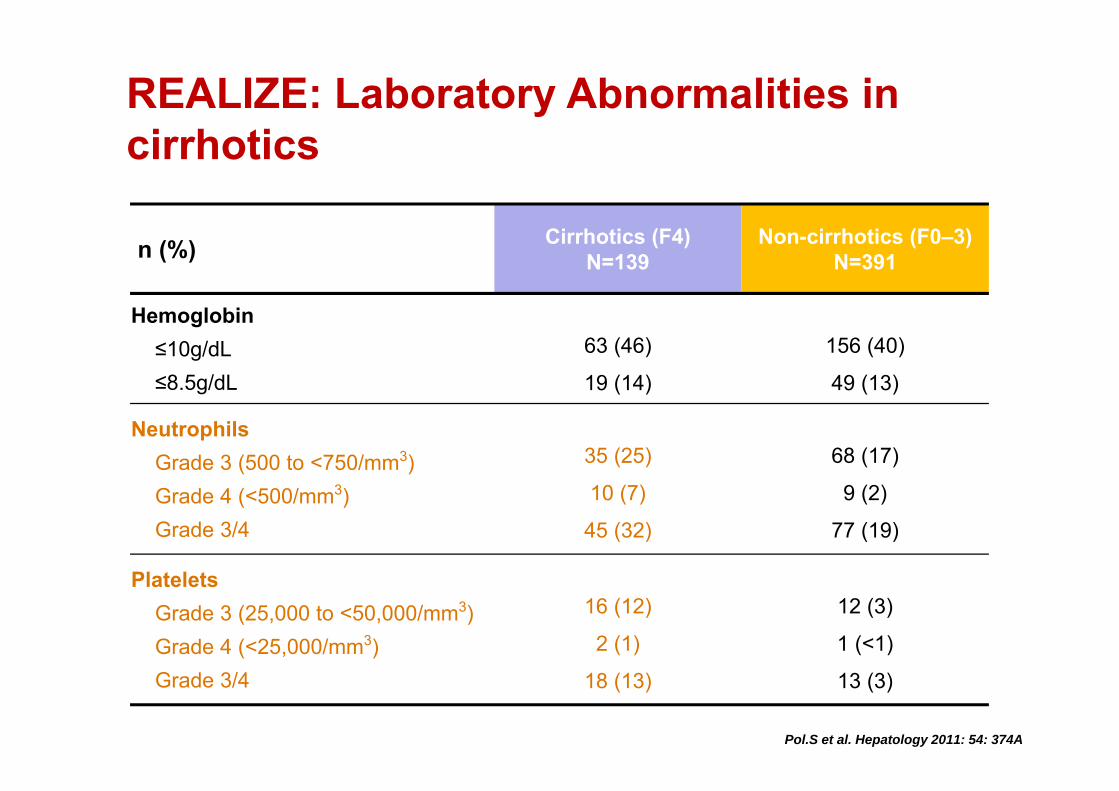
REALIZE: Laboratory Abnormalities in cirrhotics
n (%) Cirrhotics (F4) N=139
Non-cirrhotics (F0–3) N=391
Hemoglobin≤10g/dL≤8.5g/dL
63 (46)
19 (14)
156 (40)
49 (13)
NeutrophilsGrade 3 (500 to <750/mm3)Grade 4 (<500/mm3)Grade 3/4
35 (25)
10 (7)
45 (32)
68 (17)
9 (2)
77 (19)
PlateletsGrade 3 (25,000 to <50,000/mm3)Grade 4 (<25,000/mm3)Grade 3/4
16 (12)
2 (1)
18 (13)
12 (3)
1 (<1)
13 (3)
Pol.S et al. Hepatology 2011: 54: 374A
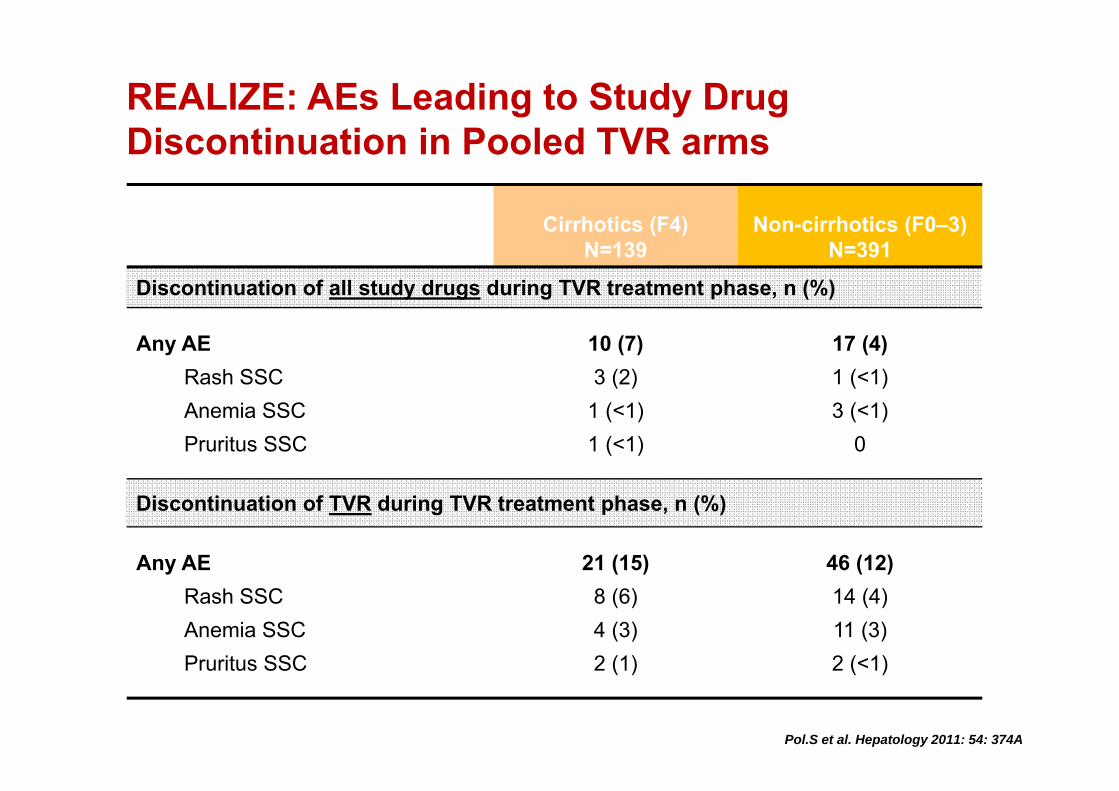
REALIZE: AEs Leading to Study Drug Discontinuation in Pooled TVR arms
Cirrhotics (F4) N=139
Non-cirrhotics (F0–3) N=391
Discontinuation of all study drugs during TVR treatment phase, n (%)
Any AERash SSCAnemia SSCPruritus SSC
10 (7)3 (2)
1 (<1)1 (<1)
17 (4)1 (<1)3 (<1)
0
Discontinuation of TVR during TVR treatment phase, n (%)
Any AERash SSCAnemia SSCPruritus SSC
21 (15)8 (6)4 (3)2 (1)
46 (12)14 (4)11 (3)2 (<1)
Pol.S et al. Hepatology 2011: 54: 374A
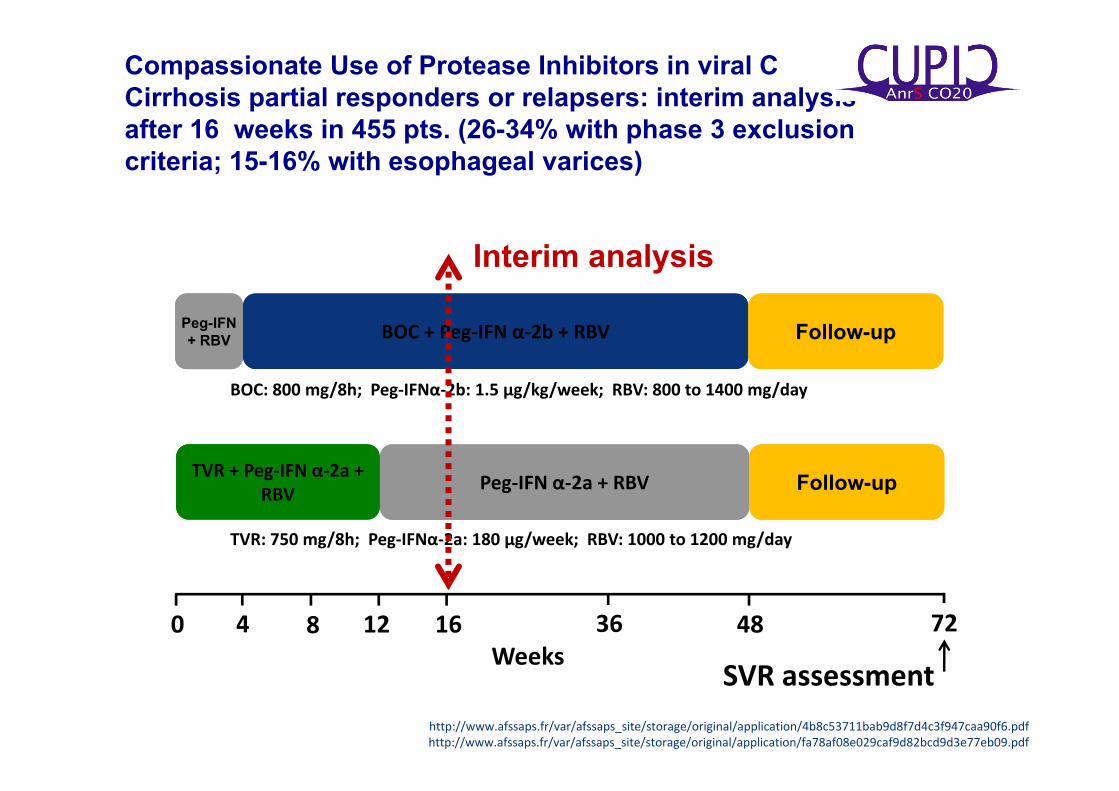
Compassionate Use of Protease Inhibitors in viral C Cirrhosis partial responders or relapsers: interim analysis after 16 weeks in 455 pts. (26-34% with phase 3 exclusion criteria; 15-16% with esophageal varices)
Peg‐IFN α‐2a + RBVTVR + Peg‐IFN α‐2a + RBV Follow-up
484 160 128Weeks
72
SVR assessment
BOC + Peg‐IFN α‐2b + RBV Follow-upPeg-IFN + RBV
36
http://www.afssaps.fr/var/afssaps_site/storage/original/application/4b8c53711bab9d8f7d4c3f947caa90f6.pdfhttp://www.afssaps.fr/var/afssaps_site/storage/original/application/fa78af08e029caf9d82bcd9d3e77eb09.pdf
BOC: 800 mg/8h; Peg‐IFNα‐2b: 1.5 µg/kg/week; RBV: 800 to 1400 mg/day
TVR: 750 mg/8h; Peg‐IFNα‐2a: 180 µg/week; RBV: 1000 to 1200 mg/day
Interim analysis
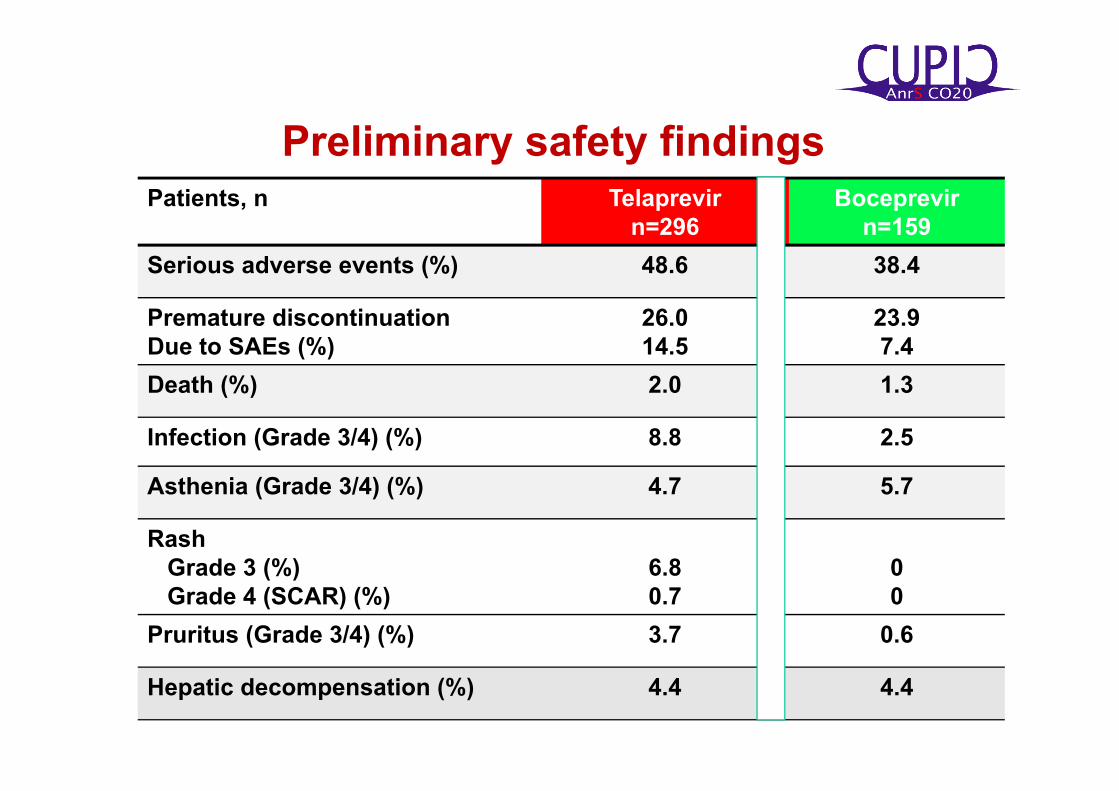
Patients, n Telaprevirn=296
Boceprevirn=159
Serious adverse events (%) 48.6 38.4
Premature discontinuationDue to SAEs (%)
26.014.5
23.97.4
Death (%) 2.0 1.3
Infection (Grade 3/4) (%) 8.8 2.5
Asthenia (Grade 3/4) (%) 4.7 5.7
RashGrade 3 (%)Grade 4 (SCAR) (%)
6.80.7
00
Pruritus (Grade 3/4) (%) 3.7 0.6
Hepatic decompensation (%) 4.4 4.4
Preliminary safety findings
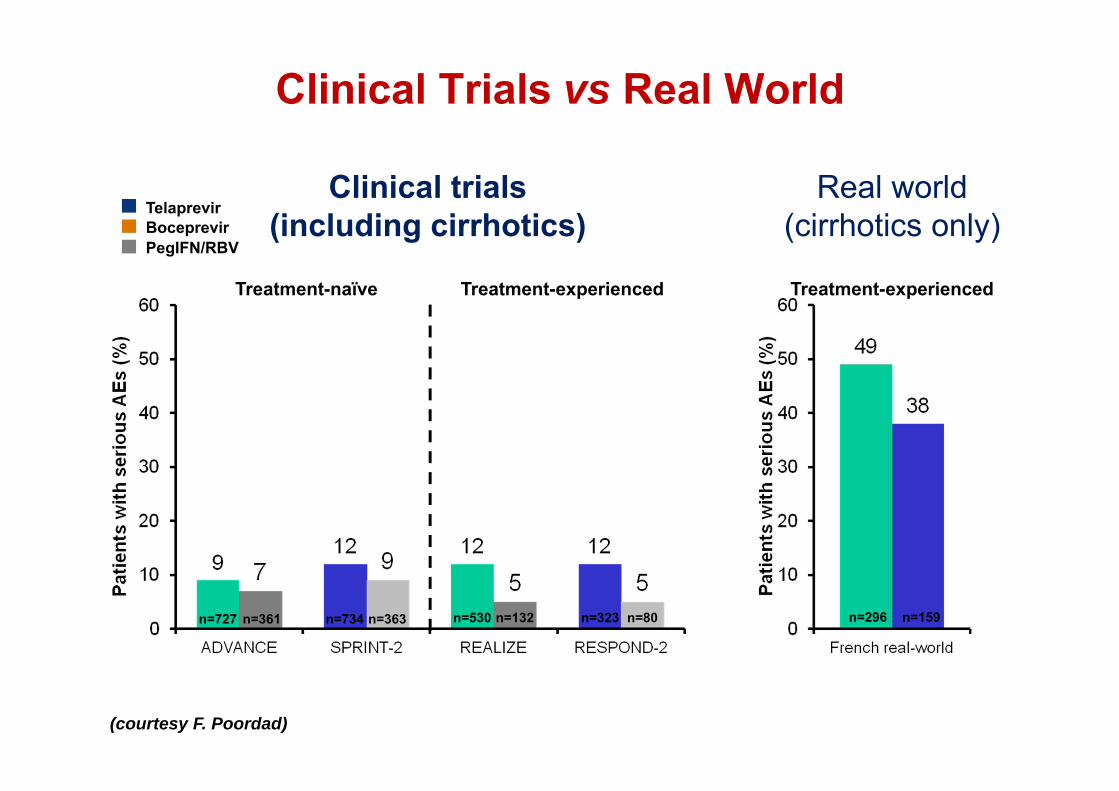
Clinical Trials vs Real World
n=530 n=323n=734n=727 n=159n=296
Clinical trials(including cirrhotics)
Real world(cirrhotics only)
Treatment-naïve Treatment-experienced Treatment-experienced
TelaprevirBoceprevir
n=132 n=80n=363n=361
PegIFN/RBV
(courtesy F. Poordad)
Causes of death
• Septicemia, • Septic shock, • Pneumopathy, • Oesophageal varices
bleeding, • Encephalopathy, • Lung carcinoma
• Bronchopulmonary infection,
• Sepsis
Telaprevir Boceprevir
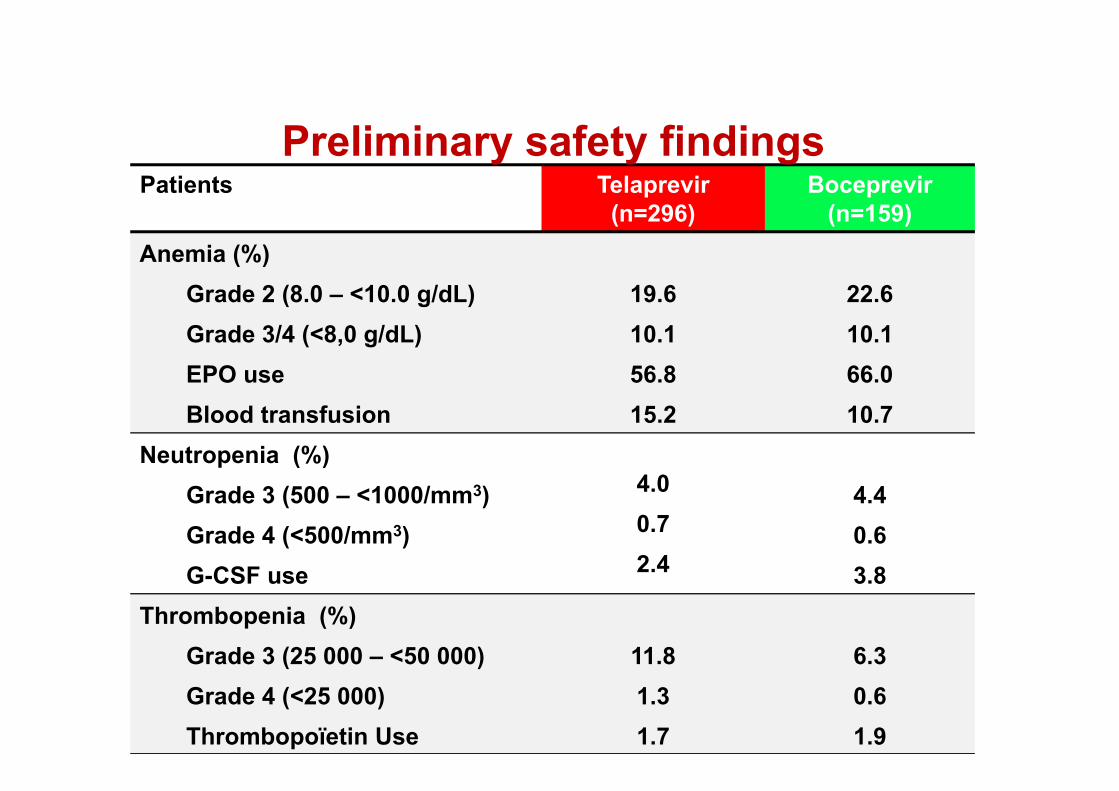
Patients Telaprevir (n=296)
Boceprevir (n=159)
Anemia (%)Grade 2 (8.0 – <10.0 g/dL)Grade 3/4 (<8,0 g/dL)EPO useBlood transfusion
19.610.156.815.2
22.610.166.010.7
Neutropenia (%) Grade 3 (500 – <1000/mm3)Grade 4 (<500/mm3)G-CSF use
4.00.72.4
4.40.63.8
Thrombopenia (%) Grade 3 (25 000 – <50 000)Grade 4 (<25 000)Thrombopoïetin Use
11.81.31.7
6.30.61.9
Preliminary safety findings

Side Effects of new and old HCV medications –Key messages
Rash frequent with TPV close monitoring, management plan and identification of SCAR might reduce its impact on Treatment safety and efficacy
Anorectal discomfort is frequent but manegeable with prompt symptomatic treatment
Anemia could be managed with ribavirin dose reduction without reducing treatment efficacy ( ribavirin overdosed?). Ribavirin withdrawal should be avoided
Patients with cirrhosis should be treated with great caution and careful monitoring especially if advanced. Surveillance and prompt treatment of infections and decompensation play a key role
45

Side Effects of new and old HCV medications
Rash Anorectal disorders Anemia Side effects in cirrhotics Side effects in HIV DDI in the management of AE
46

Phase 2 studies with HCV PI in HIV/HCV
Naggie S et al. Submitted 2011

Proportion of patients with advanced fibrosis in HIV/HCV coinfected patients enrolled in previous studies with PR and in DAA Phase 2 studies
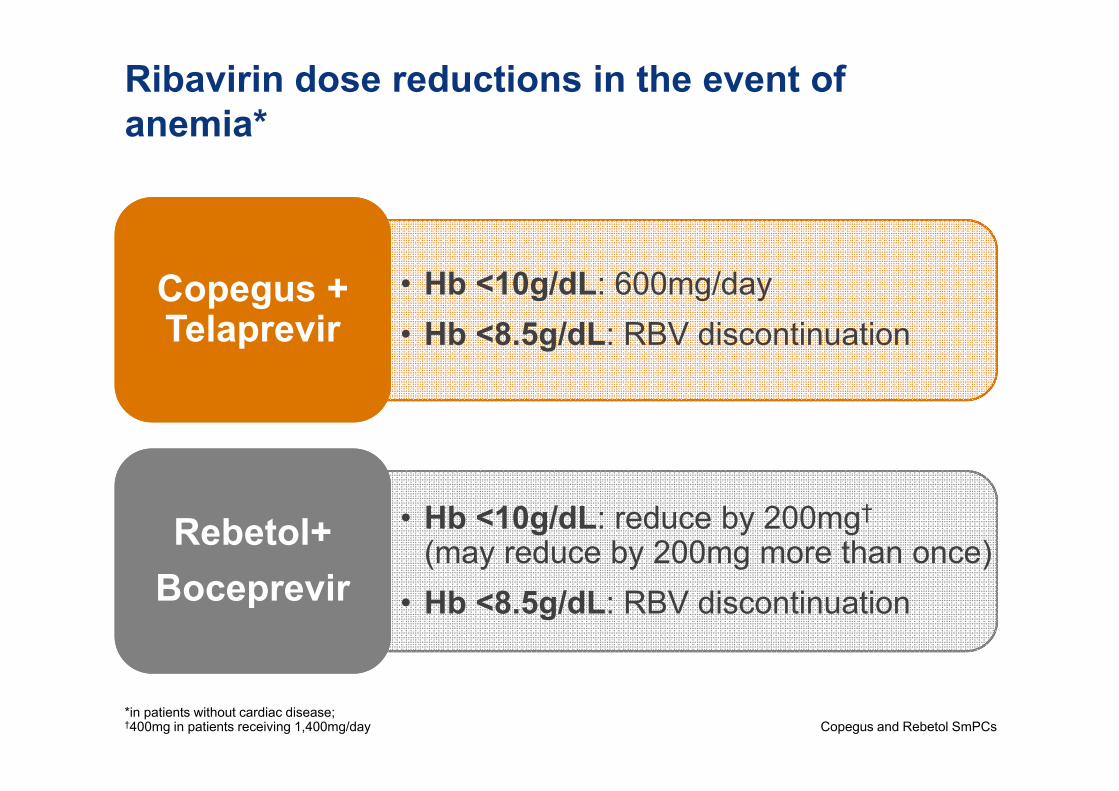
Ribavirin dose reductions in the event of anemia*
*in patients without cardiac disease; †400mg in patients receiving 1,400mg/day Copegus and Rebetol SmPCs
• Hb <10g/dL: 600mg/day• Hb <8.5g/dL: RBV discontinuation
Copegus + Telaprevir
• Hb <10g/dL: reduce by 200mg†
(may reduce by 200mg more than once)• Hb <8.5g/dL: RBV discontinuation
Rebetol+Boceprevir
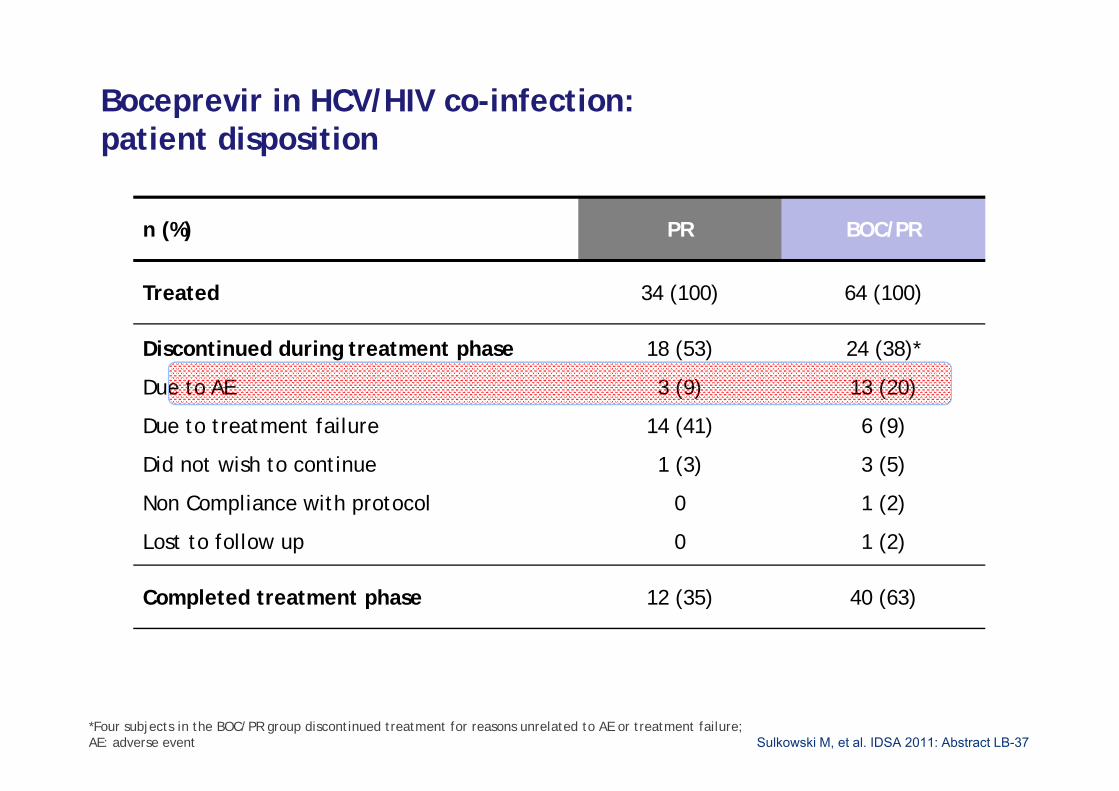
Boceprevir in HCV/HIV co-infection: patient disposition
Sulkowski M, et al. IDSA 2011: Abstract LB-37
n (%) PR BOC/PR
Treated 34 (100) 64 (100)
Discontinued during treatment phase
Due to AE
Due to treatment failure
Did not wish to continue
Non Compliance with protocol
Lost to follow up
18 (53)
3 (9)
14 (41)
1 (3)
0
0
24 (38)*
13 (20)
6 (9)
3 (5)
1 (2)
1 (2)
Completed treatment phase 12 (35) 40 (63)
*Four subjects in the BOC/PR group discontinued treatment for reasons unrelated to AE or treatment failure;AE: adverse event

Telaprevir in HIV/HCV Reasons for early discontinuation from study drugsReason T/PR (N=38) PR (N=22)Discontinued during treatment phase
16 (45) 9 (41)
Futility Rules 2 (5) 7 (32)Adverse events* 3 (8) 0 (0)Other** 11 (32) 2 (9)
*Adverse events were haemolytic anaemia, cholelitiasis , nausea and vomiting (n=3)** Other reasons include: lost to follow up (n=3), withdrawal of consent (n=1), noncompliance (n=4), lack of response (n=1), thought completed therapy (n=1), moved (n=1), patient decision (2).

Telaprevir in HCV/HIV co-infection: summary of rash and hematologic AEs
Sulkowski M, et al. IDSA 2011: Abstract LB-37
n (%) PR (n=22) TPV/PR (n=38)
Severe Rash
Mild and Moderate Rash
0
5 (23)
0
13 (34)
Anemia
AEs leading to discontinuation
Grade 3-4 (<8.0 g/dL)
Erythropoietin use
Transfusions
0
5 (23)
1 (5)
1 (5)
1 (2)
11 (29)
3 (8)
4 (11)
Neutropenia
Grade 1-4 (<1.55 x 109/L)
Grade 3-4 (<07.5 x 109/L)
?
?
?
?)

Boceprevir in HCV/HIV co-infection: summary of hematologic AEs
Sulkowski M, et al. IDSA 2011: Abstract LB-37
n (%) PR (n=34) BOC/PR (n=64)
Anemia
Serious AEs
AEs leading to discontinuation
Grade 1-4 (<11g/dL)
Grade 3-4 (<8.0 g/dL)
Erythropoietin use
Transfusions
2 (6)
1 (3)
18 (53)
1 (3)
7 (21)
2 (6)
1 (3)
1 (2)
40 (63)
3 (5)
24 (38)
4 (6)
Neutropenia
Grade 1-4 (<1.55 x 109/L)
Grade 3-4 (<07.5 x 109/L)
3 (74)
(12)
10 (86)
(27)

Side Effects of new and old HCV medications – Key messages
Rash frequent with TPV close monitoring, management plan and identification of SCAR might reduce its impact on Treatment safety and efficacy
Anorectal discomfort is frequent but manegeable with prompt symptomatic treatment
Anemia could be managed with ribavirin dose reduction without reducing treatment efficacy ( ribavirin overdosed?). Ribavirin withdrawal should be avoided
Patients with cirrhosis should be treated with great caution and careful monitoring especially if advanced. Surveillance and prompt treatment of infections and decompensation play a key role
Safety profile in persons living with HIV is similar to anti HIV –but data on cirrhotics are lacking
54

Side Effects of new and old HCV medications
• Rash• Anorectal disorders• Anemia• Side effects in cirrhotics• Side effects in HIV• DDI in the management of AE
55

Telaprevir and Antidepressants
DDI with escitalopram (major substrate of CYP3A4, mixed metabolism):
Co-administered drug Dosage
LSM ratio (90% CI), based on AUC
Co-administered drug Telaprevir
Escitalopram 10 mg 0.65 (0.60–0.70)
↔
Others not studied:Class Drug CYP3A4 substrate CYP3A4 inhibitor CYP3A4 inducer
SSRI Fluoxetine Minor Moderate (mixed metabolism)
SSRI Citalopram Major (mixed metabolism)
SSRI Paroxetine Minor (mixed metabolism)
SSRI Sertraline Minor (mixed metabolism)
SSRI Fluvoxamine Moderate (mixed metabolism)
Other Bupropion
Other Venlafaxine Minor (mixed metabolism)
TCA Trazodone Major (mixed metabolism)
TCA Mirtazapine Major (mixed metabolism)
Caution is warranted, and consider dose
reductionsof trazodone
SSRI: selective serotonin re-uptake inhibitors; TCA: tricyclic antidepressant; AUC: area under curve; LSM: least squares mean; CI: confidence interval
van Heeswijk R, et al. IWCPHT 2010. Abstract 12http://pharmacoclin.hug-ge.ch/actualites.html
Spina E, et al. Clinical Therapeutics 2008;30:1206-27

Contraindications with Telaprevir/Boceprevir
Telaprevir & Boceprevir EU SmPC
Class Agent Telaprevir1
Antihistamines Astemizole,† terfenadine†
Diphenhydramine hydroxyzine, levocetirizineand desloratadine can be used
CI
Benzodiazepines Oral midazolam, oral triazolam†
oxazepam can be usedCI
Digestive motility stimulants
Cisapride† DomperidoneMetoclopramide could be given
CI
Contraceptives (oral) Estroprogestatives Oral contraceptive
may not be reliable
PDE5 inhibitors* Sildenafil, tadalafilDose reduction maximum 25 mg SIL/24 hr;
10 mg TAD/72 hr; VAR 2.5 mg/24 H BOC or 2.5 mg per 72 h TPV
CI
*Pulmonary arterial hypertension; †removed/not available in all countriesBOLD: DDI study completed

Side Effects of new and old HCV medications – Key messages
Rash frequent with TPV close monitoring, management plan and identification of SCAR might reduce its impact on Treatment safety and efficacy
Anorectal discomfort is frequent but manegeable with prompt symptomatic treatment
Anemia could be managed with ribavirin dose reduction without reducing treatment efficacy ( ribavirin overdosed?). Ribavirin withdrawal should be avoided
Patients with cirrhosis should be treated with great caution and careful monitoring especially if advanced. Surveillance and prompt treatment of infections and decompensation play a key role
Safety profile in persons living with HIV is similar to anti HIV –but data on cirrhotics are lacking
Management of AE should take into consideration DDI58

Side Effects of new and old HCV medications – Key messages
Rash frequent with TPV close monitoring, management plan and identification of SCAR might reduce its impact on Treatment safety and efficacy
Anorectal discomfort is frequent but manageable with prompt symptomatic treatment
Anemia could be managed with ribavirin dose reduction without reducing treatment efficacy ( ribavirin overdosed?). Ribavirin withdrawal should be avoided.
Patients with cirrhosis should be treated with great caution and careful monitoring especially if advanced. Surveillance and prompt treatment of infections and decompensation play a key role
Safety profile in persons living with HIV is similar to anti HIV –but data on cirrhotics are lacking
Management of AE should take into consideration DDI59


















