Shoulder ppt
79
CME on Approach to Shoulder Pain Assessment&Evaluation Presenter: Dr. Fahad Islam Honorary Medical Officer, CMCH Physical Medicine &Rehabilitation Department
-
Upload
fahad-islam -
Category
Health & Medicine
-
view
315 -
download
4
Transcript of Shoulder ppt

CME on Approach to Shoulder Pain Assessment&Evaluation
Presenter:
Dr. Fahad IslamHonorary Medical Officer, CMCH
Physical Medicine &Rehabilitation Department

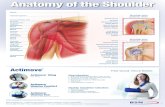
SHOULDER JOINT
Patient Evaluation

SHOULDER JOINT
*Multiaxial Ball& Socket type of synovial joint
*Most flexible joint in the entire human body due to limited interface
*Formed by the articulation between the glenoid fossa of scapula& Head of Humerus

ANATOMY..
• Shoulder Girdle: humerus, clavicle, scapula & sternum
• Physiologic area: subacromial space• Muscles• Non-contractile structures (ligament,
capsule, bursa, labrum, nerves & blood vessels)

Bursa around Shoulder
1.Subdeltoid Bursa
2.Subcoracoid Bursa
3.Coracobrachial Bursa
4.Subacromial Bursa
5.Subscapular Bursa

Ligaments
1.Superior, middle and inferior glenohumeral Ligaments
2.Coracohumeral Ligaments
3.Transeverse humeral ligaments
4.Coraco-acromial Ligaments

Nerve Supply
1.Suprascapular N
2.Axillary N
3.Lateral Pectoral N

Blood Supply
The glenohumeral joint is supplied with blood by branches of the-
1.Anterior and Posterior circumflex humeral,
2.Suprascapular arteries and
3.The scapular circumflex arteries.

PURPOSE OF SHOULDER ASSESSMENT
• Verify the nature and extent of impairments (e.g. pain, movement restriction, impaired proprioception etc.)

• Ascertain the degree of the resulting disability (e.g. difficulty throwing, inability to perform freestyle stroke etc.)
• Gather significant information about the patient (e.g. level of motivation, expectations, occupation, sport activities etc.)

SUBJECTIVE EXAMINATION
• Patient’s profile– Age– Occupation– Hand dominance– Recreational pursuits– Work requirements– ADL

Continue..
• Comfortable/ Preferred limb position
• Mechanism of Injury– Overhead exertion involving
repetitive motion – Fall or blow to tip of shoulder or
land on elbow– Shoulder feels unstable or “coming
out”

• Body Chart– Symptomatic representation of pt’s
complaints– Most important element of subj
examination• Movements that cause pain or
problems? – Lateral rotation- ant. Dislocation– Dead Arm Syndrome – ant. instability– Night & Resting pain- rotator cuff tear– Activity related pain- tendinitis– Pain greater than 90 degrees of ABD-
AC joint

• Extent & behavior of patient’s pain (e.g. deep, boring, toothache-like pain – TOS)
• Activities that causes or aggravates pain (e.g. overhead elevation – impingement)
• Pain relieving positions (e.g. overhead – nerve root pain)
• Functional capabilities of the patient
• Onset and duration of sx? (e.g. frozen shoulder – 3 stages)

• Any indication of muscle spasm, deformity, wasting, bruising, paresthesia or numbness?
• Any feeling of heaviness and weakness of the limb after activity? (e.g. TOS – coolness & pallor)
• Any indication of nerve injury? (paresthesia, numbness, weakness)

Chief Complaints
1.Pain-True/referred
*AC joint/Referred pain=Top of the Shoulder *Glenohumeral Joint/rotatory cuff= Front& outer aspect of joint as far as the middle of the arm. *Rotatory cuff impingment=pain in Window cleaning position *Shoulder instability=Sudden pain in over headed position

Continue..
2.Weakness
*True Loss of power=Neurological disorder *Sudden& Surprising inability to abduct=Rotatory cuff Tear

Continue..
3.Instability-Feeling of shoulder jumps out of its socket when raising arm, Click/Jerk when arm is held over headed. 4.Stiffness-May be Severe/progressive---Frozen Shoulder 5.Swelling-may be Joint/Muscle/Bone

Continue..
6.Deformity-May be either Muscle wasting,AC jt prominence,Winging of scapula,or an abnormal position of the arm 7.Loss of Function-Expressed as difficulty with dressing &grooming or inability to lift objects or work with the arm above shoulder height.

Continue..
Examined from front, side, behind & above, both upper limb, Neck ,upper chest& outline of Scapula must be visible

OBSERVATION• Observe shoulder,
head, cervical spine, thorax (anterior & posterior
aspects) & entire UE

ANTERIOR VIEW• Step Deformity
– Distal end of clavicle lying superior over the Acromion Process (AC dislocation)
• Sulcus Sign– Sulcus below Acromion (GH
subluxation)• Flattening of deltoid muscle:
ant dislocation of GH jt or deltoid paralysis

STEP DEFORMITY

SULCUS SIGN

POSTERIOR VIEW• Examine for bony contours &
alignment• Atrophy: Upper trapz,
supra/infraspinatus• Winging of the scapula: medial
border moves away from posterior chest wall
• ROTARY WINGING- inf angle is rotated farther from the spine

• DYNAMIC WINGING- with mov’t caused by lesion in long thoracic nerve & spinal accessory nerve
• STATIC WINGING- at rest due to structural deformity
• SCAPULAR TILT- superior/ inferior border tilt away from the chest
• SPRENGEL’s DEFORMITY- congenitally high or undescended scapula

WINGING of the SCAPULALong ThoracicNerve Lesion

SPRENGEL’S DEFORMITY

FEEL
1.Skin-Temparature 2.Bony points &Soft tissues *6 Points= SC jt,trace clavicle, AC jt, Ant. Edge of Acromion& Around acromion, Ant.& Post.margin of glenoid, Bicipital groove *Supraspinatus Tendon =Palpated just under the Ant. edge of Acromion(Crepitus+=Tendinitis/Tear) Below this Tendon bony prominences bounding the Bicipital groove easily felt if the gently Rotated.

EXAMINATION

Range of Motion 3 CLASSIC SHOULDER
CASES–JOINT PATHOLOGY–MUSCLE/ TENDON PATHOLOGY
–NERVE COMPRESSION INJURIES

MOVEMENTS
Observed from Front, then behind, Pt either standing/sitting
1.AROM
a. Abduction(0-170)&Adduction(0-50) b.Flexion(0-165)& Extension(0-60) c.Horizontal Flexion &Adduction=0-140 degree d.Internal rotation in abduction=0-70 degree

AROM..continue
e. External rotation in abduction=0-100 degree f.External rotation in extension=0-70 degree
g.Internal rotation in extension 0-70 degree h.Shoulder Elevation=37 degree i.Shoulder depression=8 degree

CONTINUE..
2.PROM-Examiner press Firmly down on the Top of the shoulder with one hand while the other hand moves the Pts arm
3.Power

COMMON CAUSES OF SHOULDER PAIN
A. Joint patholgy- GH arthritis,AC arthritisB. Rotatory cuff patholgy-Impingement,
Tendinitis, Tear, Frozen shoulderC. Bone pathology-Infection,TumorD. Nerve patholgy-Suprascapular N
entrapmentE. Referred Pain-
C/Spondylosis,Mediastinal &Cardiac Ischemia

Disorder of Rotatory Cuff (Rotatory Cuff Syndrome)
Comprises at least 4 condition with distinct clinical features& conditions:
1.Supraspinatus impingement syndrome& Tendinitis
2.Rotatory cuff tear
3.Acute calcific Tendinitis
4.Biceps Tendinitis and,or/ Rupture

Impingement site
pics-1.lnk

Impingement Syndrome
Pathology:
1.Repetitive compression or rubbing of the tendons under coracoacromial arch specially in Impingement position
2.Osteoarthritic Thickening of AC joint

Impingement Syndrome- pathology. continue
3.Osteophyte on the ant. Edge of acromion
4.Inflammatory swelling of rotatory cuff or subacromial bursa.eg: Gout,RA
5.Acromial Morphology.

Pathology..continue
6.Friction in Old age may leads to minute tear of cuff
7.Sudden strain-partial/full thickness tear, associated with Biceps tendon tear.
8.Secondary arthropathy

Clinical features of Rotatory Cuff Syndrome
3 Pattern are encountered:
1.Subacute tendinitis-Painful arc syndrome
2.Chronic tendinitis
3.Cuff disruption

Impingement Test
1.The Painful arc-on active abduction (60-120 degree)
2.Neer’s Impingement sign: 80 percent sensitive. also (+)ve in Rotatory cuff tear, AC joint OA, Glenohumeral instability& SLAP lesions.

1.PAINFUL ARC

2.NEER IMPINGEMENT TEST

3.HAWKINS-KENNEDY IMPINGEMENT TEST

continue..
TEST FOR ISOLATED MUSCLE WEAKNESS

1.Supraspinatus-EMPTY CAN TEST

2.INFRASPINATUS TEST- resisted external rotation

3.DROP ARM TEST-found in Infraspinatus &Post. cuff tear

4.LIFT-OFF SIGN / TEST subscapularis pathology

Investigations
1.X-ray examination- early stages found normal, but in
*Ch. tendinitis= erosion, sclerosis& Cyst formation at the site of cuff insertion
*In Ch. Case caudal tilt view show roughening or overgrowth of ant. Edge of acromion& upward displacement of humeral head

Investigations..
2.MRI-gives valuable information about structures like lesion of glenoid labrum, joint capsule or surrounding muscle, bone.
3.USG-identifying and measuring the size of full thickness or partial thickness tear.

Treatment of Cuff disorders
Conservative:
1.ADLs modification
2.Physiotherapy=UST
3.AROMs
4.NSAIDs,I/A depot corticosteroids

CONTINUE
Surgical management:
*When conservative treatment fails after 3 months
*Symptoms persist or worse after adequate treatment

CONTINUE
1.Decompress rotatory cuff by excising coracoacromial ligament,undercutting the ant. Part of acromion
2.Open/Arthroscopic acromioplasty
3.Open/Arthroscopic repair of the rotatory cuff

Calcification of the Rotatory cuff
Acute calcific tendinitis:*deposition of CPPD crystal in critical zone, also occurs in
ankle, knee, hip, elbow
*Cause is unknown, supposed that ischemia leads to fibrocartilaginous metaplasia& crystal deposition by chondrocytes.
*Florid vascular reaction produces tension& swelling of the tendons causes pain
*Resorbtion of calcific materials is rapid with in few weeks.

C/F of Acute calcific tendinitis
1.30-50 yrs age
2.Aching pain develops with in hours after overuse, raising to an agonizing
3.After few days pain subside

X-ray findings
1.Calcification just above greater tuberosity
2.Well demarcated deposit becomes more woolly and then dissappears.

Treatment of Acute calcific tendinitis
Conservative Mx:
1.NSAIDs
2.Subacromial I/A steroids
3.Physiotherpay
4.Extra corporeal shock wave therapy
5.Needle aspiration& Irrigation

Management continue
Surgical Mx: after 6months of conservative treatment
*Arthroscopic incision from bursal side with fibre orientation of the tendon,then curette to milk out the tooth paste deposit.Sub-acromial decompression may also done.

Lesions of the Biceps Tendon
1.Tendinitis
2.Rupture:Pop-Eye Bulge
3.Hypertrophy & Intra-articular entrapment (The Hour glass Biceps)
4.Instability*Subluxation-Partial&/transient loss of contact between the
tendons& its groove
*Dislocation-complete& permanent loss of contact between the tendons& its groove

TEST FOR BICEPS TENDON
1.Speed’s Test
2.Yergason’s Test

1.Speed’S Test

2.Yergason’s Test

SLAP Lesions
Compressive loading of the shoulder in the flexed abducted position like fall on the out-stretched hand.4 main types:
1.Non-traumatic(degenerative) sup. labral tear
2.Avulsion of the sup.part of labrum(commonest)
3.A Bucket handle tear of Sup.labrum
4.Bucket handle tear with its extension into long head of biceps

Special Test:O’Brien Test

SHOULDER INSTABILITY
1.Type I: Traumatic structural(Ant.) Instability
2.Type II: Atraumatic /minimally traumatic structural instability, multidirectional instability eg:repetitive microtrauma/overall laxity like during swimmers, athelets, throwers
3.Type III: Atraumatic non-structural instability(muscular dyskinesia)

Shoulder Instabilities
• Instability Anterior– Crank (apprehension) test– Anterior Drawer Test
• Instability Posterior– Posterior Drawer Test– Posterior Apprehension Test
• Instability Inferior– Sulcus Sign

APPREHENSION TEST FOR ANTERIOR SHOULDER
DISLOCATION

POSTERIOR APPREHENSION TEST

DRAWER TEST

SULCUS SIGN

LOAD AND SHIFT TEST

FROZEN SHOULDER

Frozen Shoulder
* Progessive pain and stiffness of the shoulder joint which spontaneously resolve after 18 months.
*Restricted both active &passive ROMs in all planes.
*commonly associated with DM, Hyperlipidaemia, Hyperthyroidism, Dupuytren’s disease, IHD, Inflammatory arthritis & C/Spondylosis

Continue..
Passes in 3 stages:
1.1st stage/Freezing phase: 3-6months
2. 2nd stage/Frozen phase/Progessive stiffness: 3-18 months
3.Final stage/Resolution/Thawing phase: 3-6 months

Test for Frozen shoulder

Treatment
Diagnosis is clinical. Rx combining:
1.ADLs modification
2.NSAIDs
3.I/A Steroid,or 50-200 sterile saline under pressure
4.Codman pendulum ex is very effective
5.Physical agent: UST

Thank you ..