
Shoulder impingement syndrome larissa 2016
45
Subacromial Impingement Syndrome Subacromial Decompression Aaron Venouziou Orthopaedic Surgeon St. Luke’s Hospital Thessaloniki
-
Upload
aaron-venouziou -
Category
Health & Medicine
-
view
103 -
download
0
Transcript of Shoulder impingement syndrome larissa 2016
Subacromial ImpingementSyndromeSubacromial Decompression
AaronVenouziouOrthopaedic SurgeonSt.Luke’sHospital
Thessaloniki
Introduction
ü Ill-definedtermforavarietyshoulderdisordersthatmanifestasantero-lateralshoulderpain
üNonspecificdiagnosis
üNumeroustypesofshoulderimpingement
üOnlyasmallproportionofthesenecessitatedecompression
Etiology
üExtrinsic– PrimaryImpingement• Oulet stenosis
– SecondaryImpingement• Instability
üIntrinsic– Degeneration• Aging• Avascularity
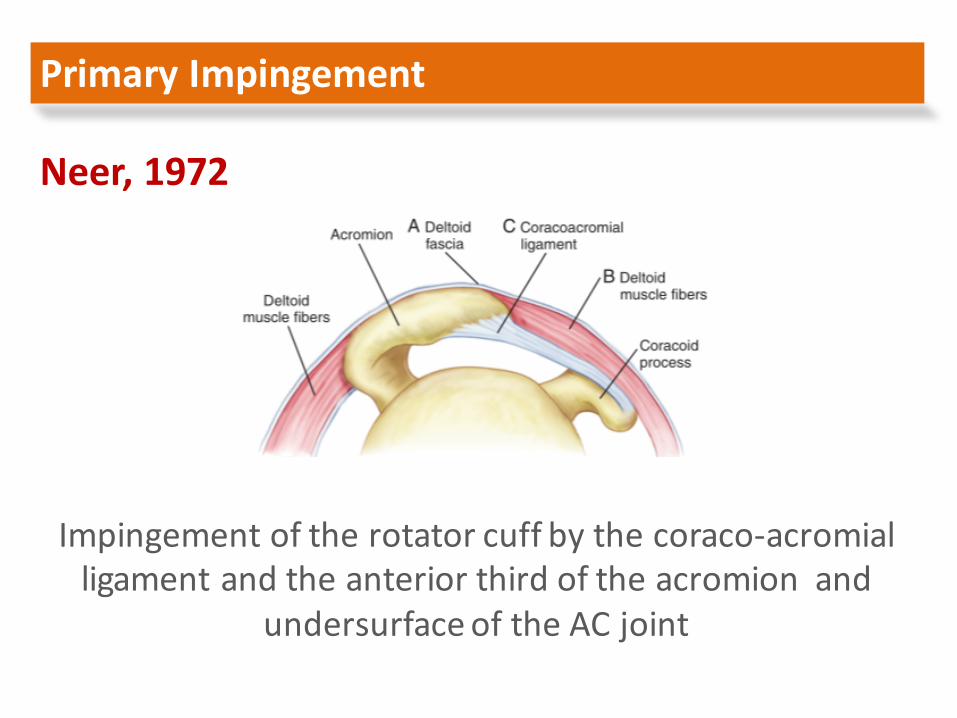
Neer,1972
Impingementoftherotatorcuffbythecoraco-acromialligamentandtheanteriorthirdoftheacromionand
undersurfaceoftheACjoint
PrimaryImpingement

ü Spursandbonychangesontheundersurfaceoftheanterior1/3oftheacromioncorrelatedwithrotatorcufftears
ü 90%ofptstreatedbyacromioplasty hadsignificantpainreduction,fulluseofshoulder,<20o ofoverheadlimitation,andatleast75%normalstrength
ü RCinjuryisaresultofprimaryimpingement
PrimaryImpingement
Neer,1972

ü Popularizedthetheoryof“extrinsic”impingement,statingthatacromialchangeswereprimaryasopposedtosecondarychanges—causingimpingement
ü 70%offull-thicknessRCtearsintypeIIIacromion
üNeverbeenprovenorpeerreviewed
PrimaryImpingement
Bigliani,1986
üGlenohumeral Instability– Commonintheoverheadthrowingathlete– Cocking=>strainonthestaticstabilizersoccur• Earlyphase(45ºabd,ER)- MGHL• Latephase(90ºabd,ER)– IGHL
ü Anteriorsofttissuedeficiency
ü Anteriortranslationofhumeralhead
SecondaryImpingement
Jobe andKvitne,1989
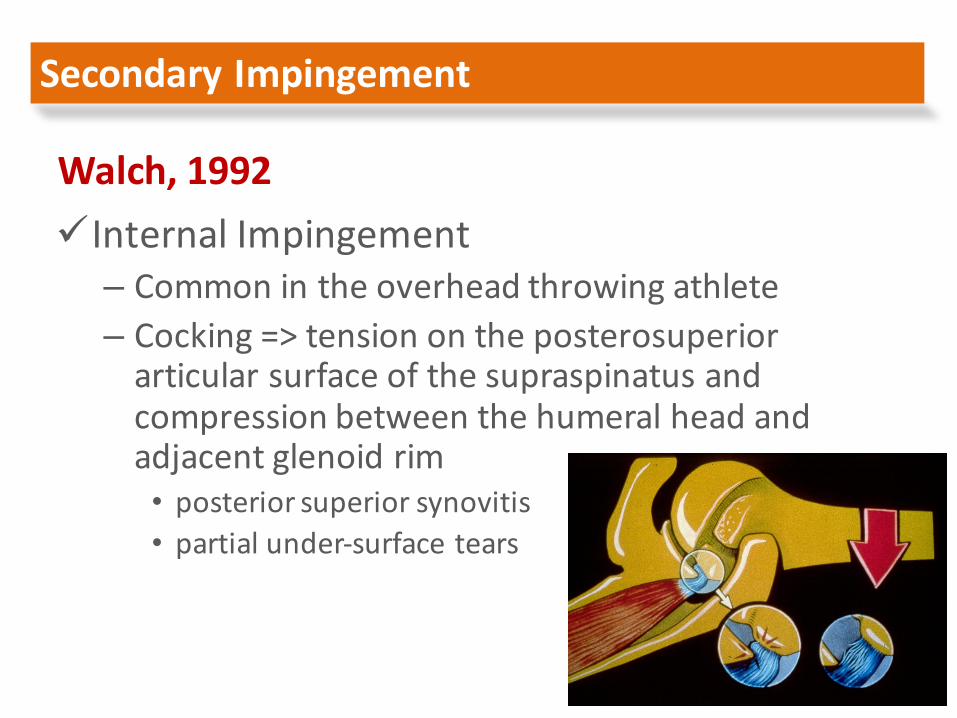
üInternalImpingement– Commonintheoverheadthrowingathlete– Cocking=>tensionontheposterosuperiorarticularsurfaceofthesupraspinatusandcompressionbetweenthehumeralheadandadjacentglenoidrim• posteriorsuperiorsynovitis• partialunder-surfacetears
SecondaryImpingement
Walch,1992
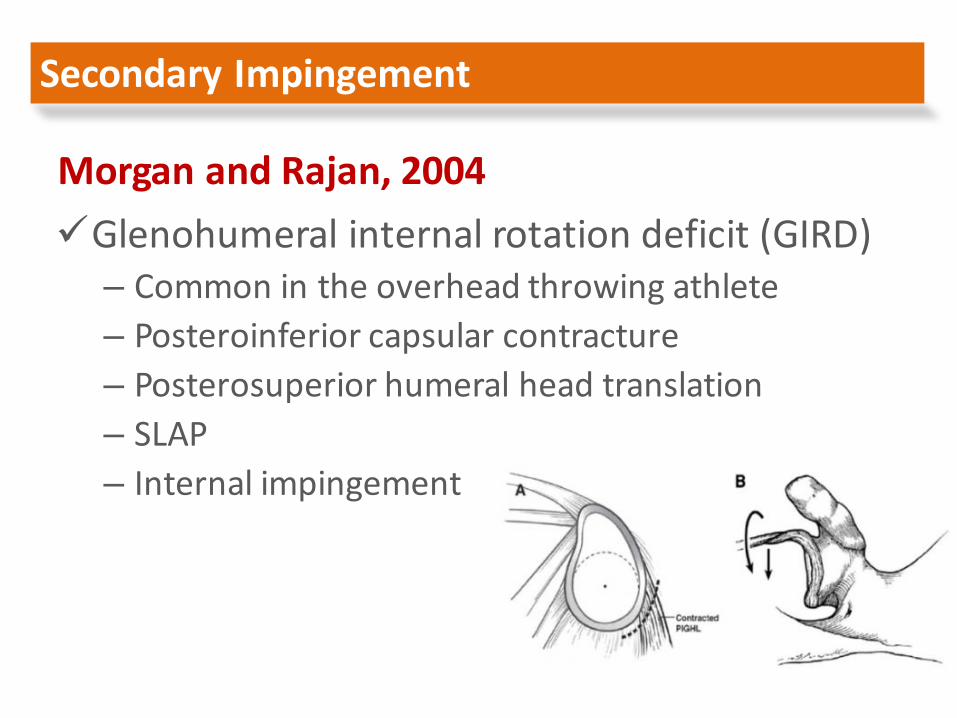
üGlenohumeral internalrotationdeficit(GIRD)– Commonintheoverheadthrowingathlete– Posteroinferior capsularcontracture– Posterosuperior humeralheadtranslation– SLAP– Internalimpingement
SecondaryImpingement
MorganandRajan,2004

üScapulothoracic Dyskinesis– Functionalscapularinstability– Increaseddistancefromspinousprocesstomedialborderofthescapula
– Lossofacromialelevation
SecondaryImpingement
ü Tendondegeneration(andfibersfailure)isthemostimportantetiologicfactorofsymptoms(andcufftears)inthesubacromial spaceandnottheimpingementsyndrome
ü Partial thicknesstearsaremostoftenonthearticularside
ü Articularsideofcuffishypovascularized
IntrinsicFactors
Ozaky 1988,Ogata&Uhthoff 1990

üThemainproblemistendondegenerationandweakness
IntrinsicFactors
Burkhart,1995

Neer impingementtest
ClinicalAssessmentLO
WSPE
CIFICITY
Hawkin’s impingementtest
Lidocaineinjectiontest
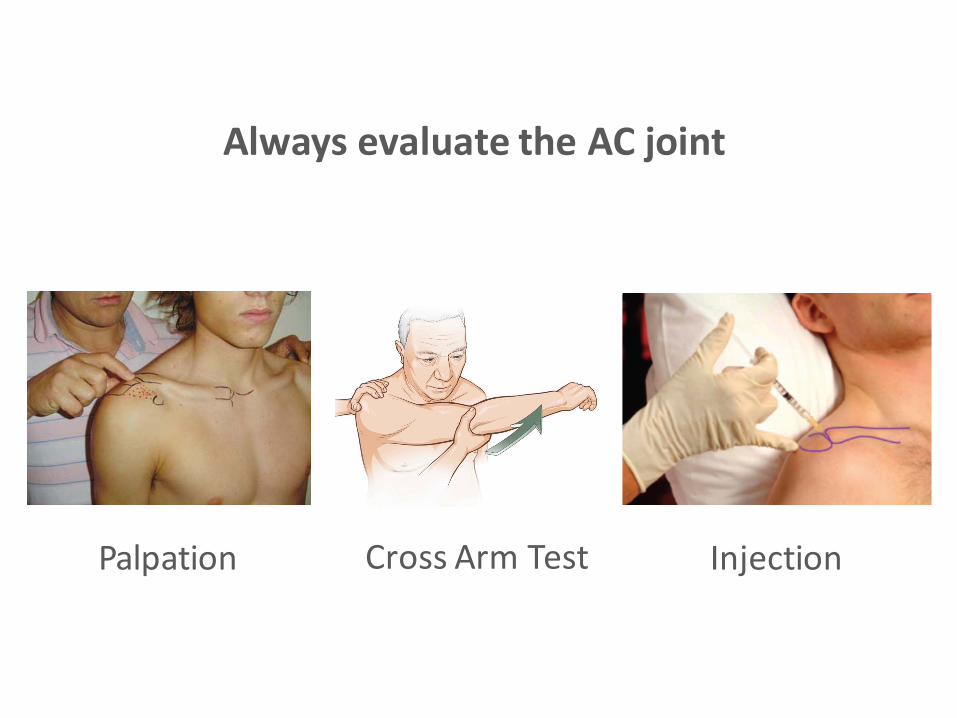
AlwaysevaluatetheACjoint
Palpation CrossArmTest Injection
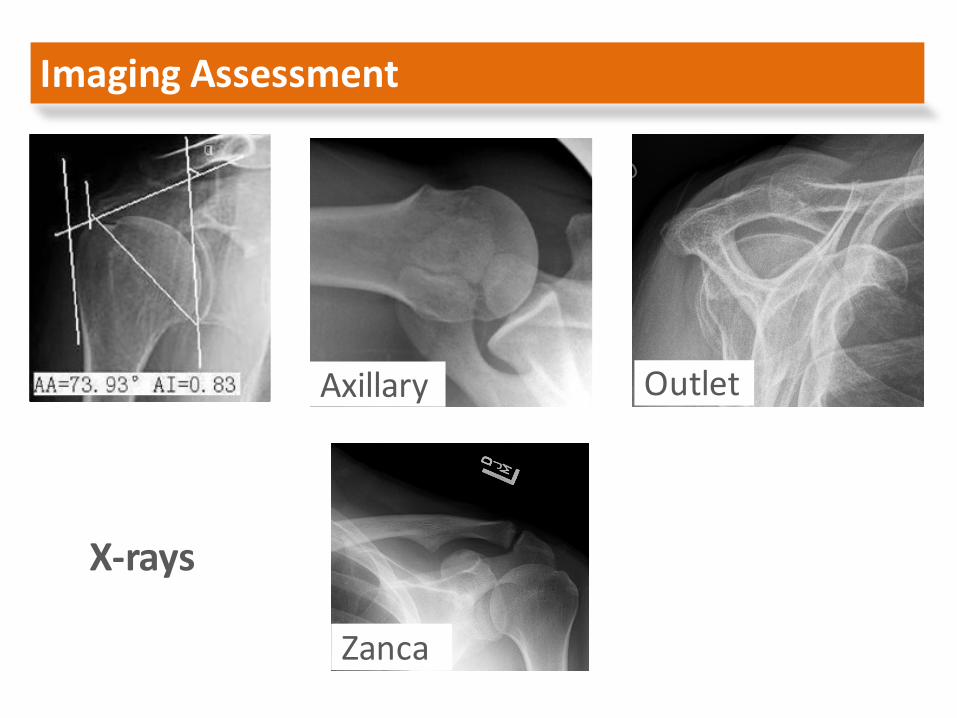
ImagingAssessment
X-rays
Axillary Outlet
Zanca
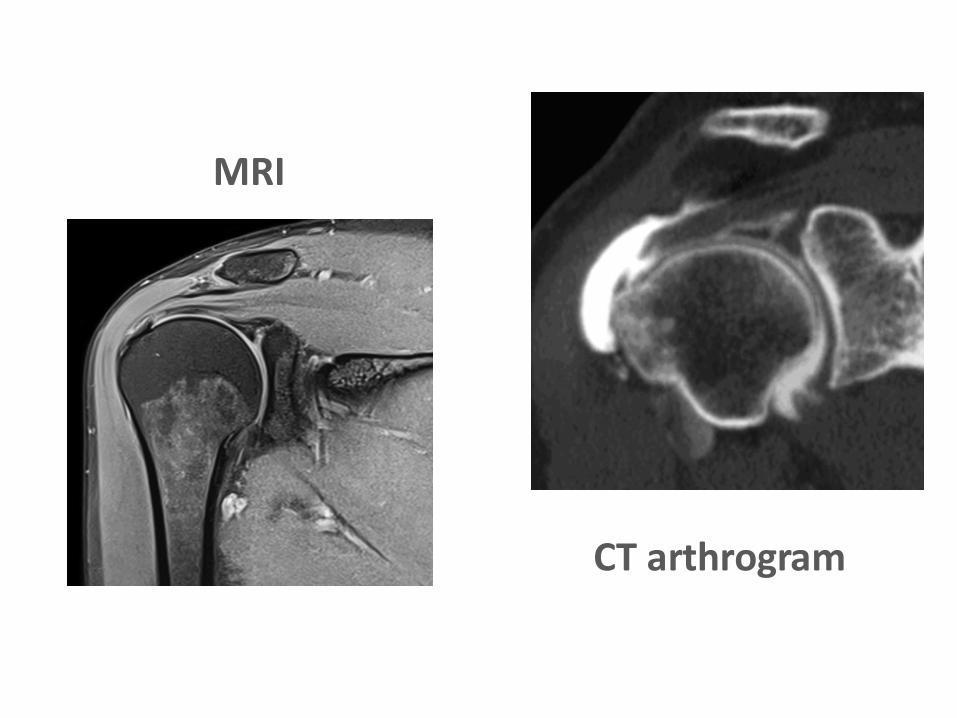
MRI
CTarthrogram

Treatment
GoaltorestorethehealthofRotatorCuff
Restorationofneuromuscularbalanceoftheshouldergirdleandthesynchronousmotionofthe3jointsabouttheshouldertopreventsubluxation
Treatment
üModificationofactivitywithcessationofoverheadactivity
üNSAIDSorsubacromial injection
üPhysicaltherapy:stretching/strengthening
üAcuteinjurywithprofoundstrengthloss:MRIofrotatorcuff
Non-operativeTreatment

üFailedconservativetreatment>6months
üAcromialprominence/spurs/sclerosis,+impingementsign,arcofpain,relieffromsubacromial injection
üNoevidenceofRCT(+/- MRI)
üArthroscopicsubacromial decompression
SurgicalTreatment
Historical background Ellman,1987
ü Technicallydemandingprocedure
ü Ifacufftearispresentyoucannotrepairit

SurgicalTechnique
PatientSetup
Beachchairposition
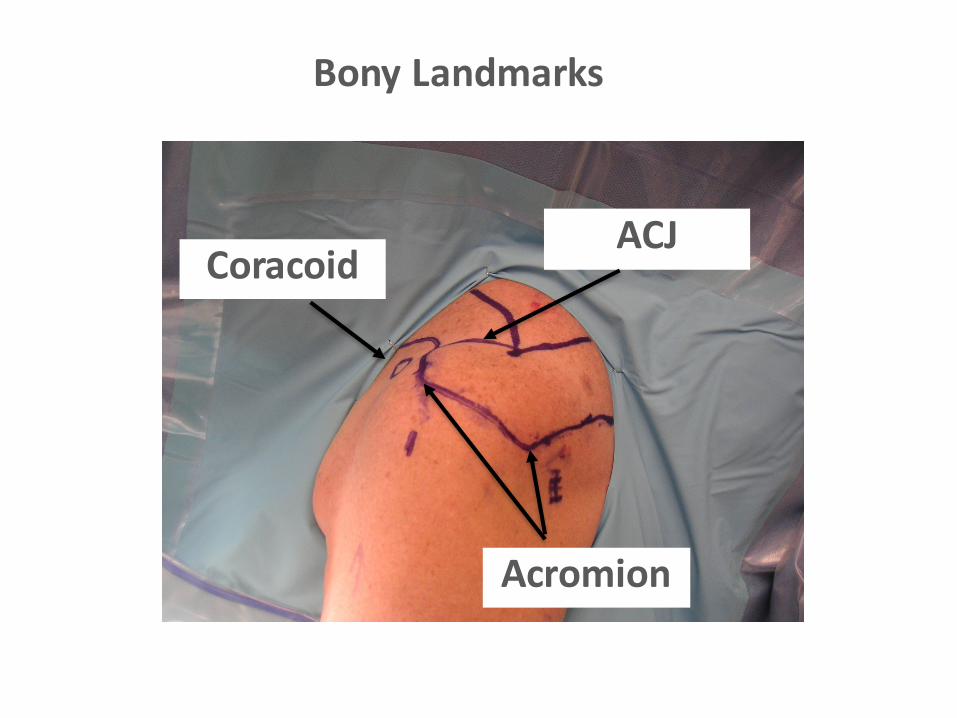
BonyLandmarks
Acromion
ACJCoracoid
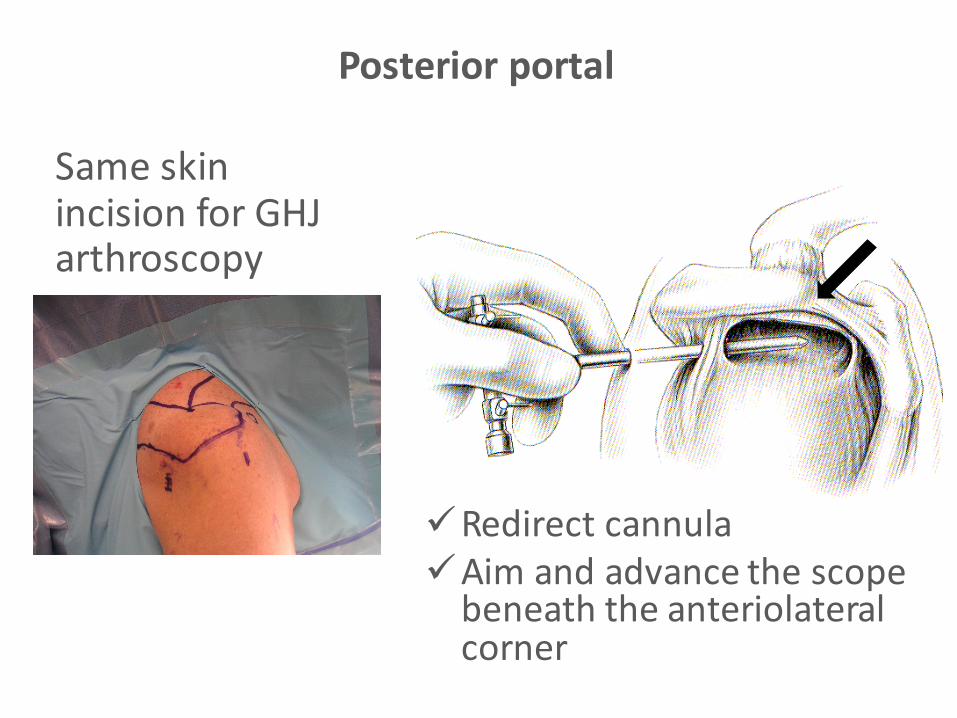
Posteriorportal
SameskinincisionforGHJarthroscopy
üRedirectcannulaüAimandadvancethescopebeneaththeanteriolateralcorner

Roomwithaview
ü4Walls,floor,ceiling
üCAligamentislandmark
Clearvisualization

Lateralportal
ü 3cmlateraltoacromionü Spinalneedleü TriangulationüUnderneaththeanteriorhalfoftheacromion
ü Parallel toit
SkinmarkingbisectsmidAC
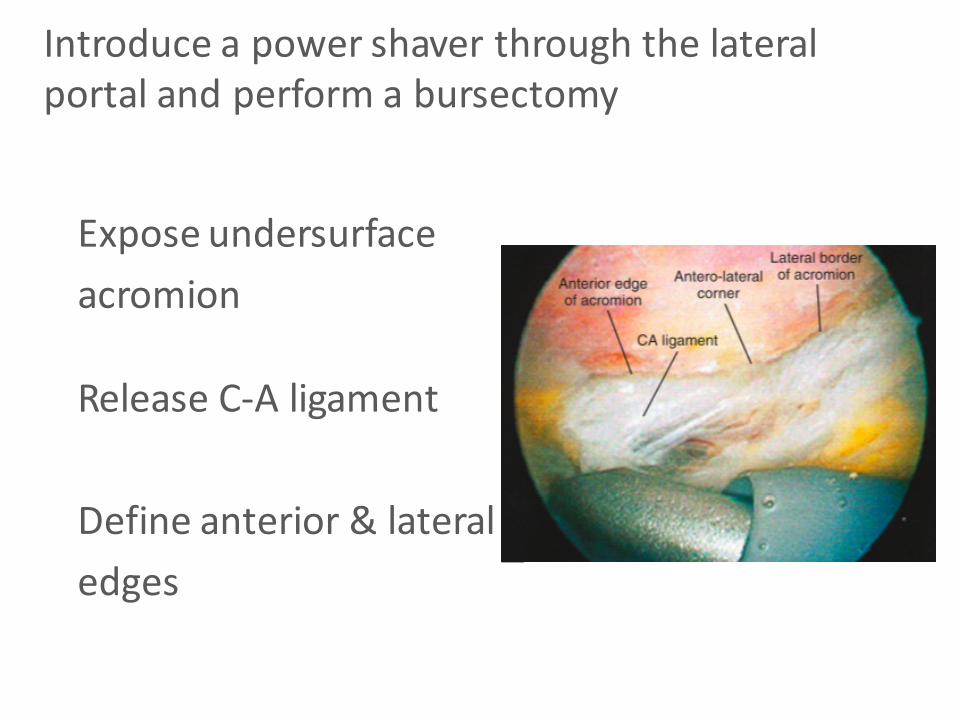
Introduceapowershaverthroughthelateralportalandperformabursectomy
Exposeundersurfaceacromion
ReleaseC-Aligament
Defineanterior&lateraledges
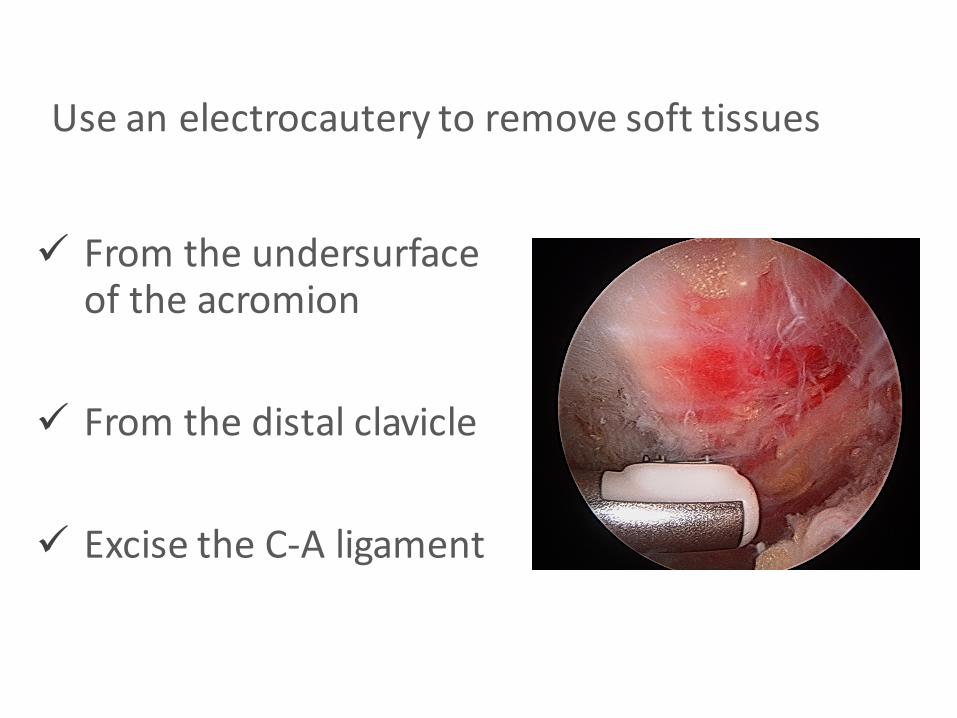
ü Fromtheundersurfaceoftheacromion
ü Fromthedistalclavicle
ü ExcisetheC-Aligament
Useanelectrocautery toremovesofttissues

Performa“provisional”anterioracromioplasty
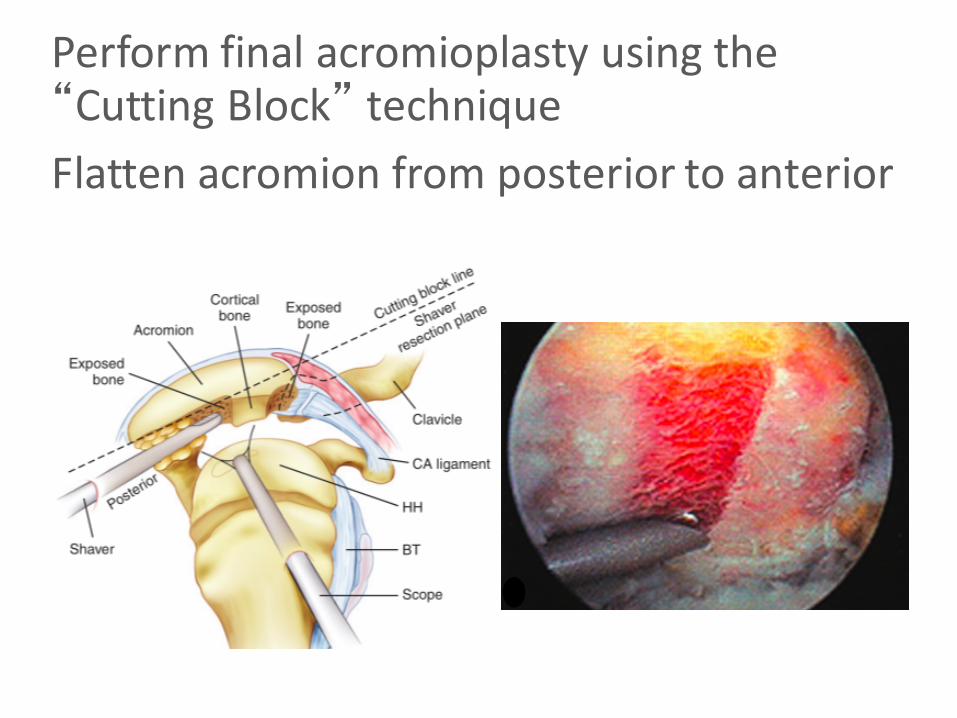
Performfinalacromioplasty usingthe“CuttingBlock” techniqueFlattenacromionfromposteriortoanterior

Watchtheangle!
ΟΚ ΟΚ

Checkacromioplasty inbothplanes
Post. Ant. Med. Lat.

üCAligamentreleased?
üAcromionflatinA-Pplane?
üAcromionflatinM-Lplane?
üACjointinspected?
üRotatorcuffinspected?
End-pointAssessment

• Scopeposterior/instrumentslateral– Exposure
DistalClavicleResection

• Scopelateral/instrumentsanterior– Bestaccesstodistalclavicle
– 70° arthroscope– 8-10mmexcisionofthedistalclavicle
DistalClavicleResection
Whataboutefficacyofthetechnique?
Whataboutefficacyofthetechnique?
Odenbring etalArthroscopy2008
Long-termOutcomesofArthroscopicAcromioplasty forChronicShoulderImpingementSyndrome:AProspectiveCohortStudyWithaMinimumof12Years'Follow-up
31patients12-14yearsfollow-up29patients(openacromioplasty)asacontrolgroup
Nofullthicknesscufftears

Arth group:Revisionacromioplasty in6patientsOpengroup:Revisionacromioplasty in3patients
Goodexcellentresultsin77%Betterresultswitharthroscopicacromioplasty
OdenbringetalArthroscopy2008
Arthroscopicacromioplasty:a6- to10-yearfollow-up
83patients,meanfollow-up8.3years
Stephensetal.Arthroscopy1998
“Overall,81%ofpatientsinourserieshadgoodtoexcellentresultsafter6to10years”.
“Tooptimizetheindicationsfortheprocedure,othercausesofimpingement,suchasoccultinstabilityanddegenerativejointdisease,shouldberuledout”.
Long-termClinicalandUltrasoundEvaluationAfterArthroscopicAcromioplasty inPatientsWithPartialRotatorCuffTears
Minimum5yearfollow-up26patients10outof26patientsdevelopedfullthicknesstear
“Arthroscopicacromioplasty androtatorcuffdebridementinpatientswithpartialtearsdoesnotprotecttherotatorcufffromundergoingfurtherdegeneration.”
Kartus etal.Arthroscopy2007

TheRoleofSubacromial DecompressioninPatientsUndergoingArthroscopicRepairofFull-ThicknessTearsoftheRotatorCuff:ASystematicReviewandMeta-analysis
Chahal etal.Arthroscopy2012
“Onthebasisofthecurrentlyavailableliterature,thereisnostatisticallysignificantdifferenceinsubjectiveoutcomeafterarthroscopicrotatorcuffrepairwithorwithoutacromioplasty atintermediatefollow-up.”

Isacromioplasty necessaryinthesettingoffull-thicknessrotatorcufftears?Asystematicreview.
• 354patients:SADandScopeCuffRepair• 4Studies:2LevelIand2LevelII• Conlusions:
– “doesnotsupporttheroutineuseofpartialacromioplasty orCAligamentreleaseinthesurgicaltreatmentofrotatorcuffdisease”
– “insomeinstances,partialacromioplasty andreleaseoftheCAligamentcanresultinanteriorescapeandworseningsymptoms”
Familiari etal.JOrthop Traumatol 2012
“Functionaloutcomeofpatientswithcalcifictendonitisafterarthroscopicbursectomy anddebridementofthecalcificdepositisnotinfluencedifperformedincombinationwithorwithoutasubacromial decompression.”
Clementetal.Arthroscopy2015(September)
Short-TermOutcomeAfterArthroscopicBursectomyDebridementofRotatorCuffCalcificTendonopathyWithandWithoutSubacromial Decompression:A ProspectiveRandomizedControlledTrial
13MONTHSFOLLOW-UP
“Theemphasisoftreatmentisshiftingfromthatof
decompressiontorestoringthehealthoftherotatorcuff”
F.Fu,1991
üFailedconservativetreatment>6months
üAcromialprominence/spurs/sclerosis,+impingementsign,arcofpain,relieffromsubacromial injection
üNoevidenceofRCT(+/- MRI)
üArthroscopicsubacromial decompression
SurgicalTreatment


















