
Shoulder disorders. Shoulder disorders symptoms: Pain; in tip of the shoulder from rotator cuff or...
38
Shoulder disorders Shoulder disorders
-
Upload
angelica-whitehead -
Category
Documents
-
view
225 -
download
4
Transcript of Shoulder disorders. Shoulder disorders symptoms: Pain; in tip of the shoulder from rotator cuff or...

Shoulder disordersShoulder disorders


Shoulder disordersShoulder disorderssymptoms:symptoms:
Pain; in tip of the shoulder from rotator Pain; in tip of the shoulder from rotator cuff or acromioclavicular (AC) joint cuff or acromioclavicular (AC) joint disorders. disorders.
Referred pain; from neck (eg. Cervical Referred pain; from neck (eg. Cervical spondylosis), mediastinum (eg. IHD).spondylosis), mediastinum (eg. IHD).
Stiffness (eg frozen shoulder).Stiffness (eg frozen shoulder). Swelling.Swelling. Instability.Instability. Weakness; as in neurological disorders Weakness; as in neurological disorders
or tendon rupture.or tendon rupture.

SignsSigns Expose both upper limbs, neck and Expose both upper limbs, neck and
chest.chest. Exam from front, behind and axilla.Exam from front, behind and axilla. Look:Look:
Skin; scar or sinus.Skin; scar or sinus. Shape; swelling,Shape; swelling,
wasting or deformity.wasting or deformity. Position; Position;

EchymosisEchymosis

Swelling over Swelling over acromioclvicular jointacromioclvicular joint

Wasting of the deltoid Wasting of the deltoid musclemuscle
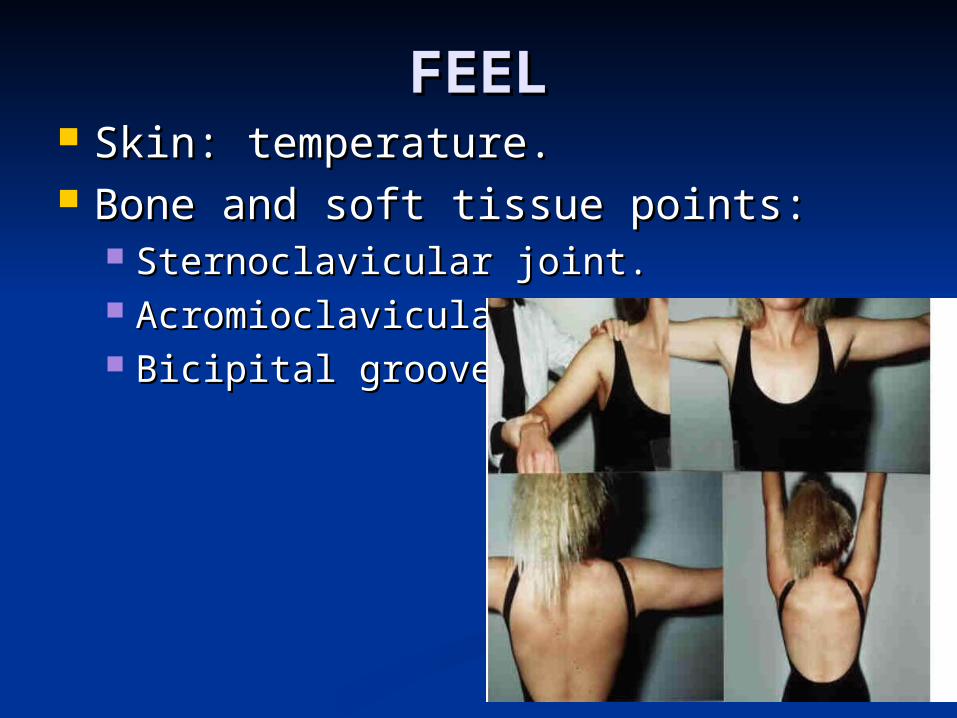
FEELFEEL Skin: temperature.Skin: temperature. Bone and soft tissue points:Bone and soft tissue points:
Sternoclavicular joint.Sternoclavicular joint. Acromioclavicular joint.Acromioclavicular joint. Bicipital groove.Bicipital groove.
Move Move
Active movements:Active movements: Abduction: 0-90 degrees glenohumeral Abduction: 0-90 degrees glenohumeral
movement. Last 60 degrees is movement. Last 60 degrees is scapulothoracic movement.scapulothoracic movement.

Flexion and extension: Flexion and extension: raise the arm raise the arm forwards and backwards.forwards and backwards.

Rotation; external (ask the patient to Rotation; external (ask the patient to clasp fingers behind the neck), internal clasp fingers behind the neck), internal (reach up the back with fingers).(reach up the back with fingers).

Disorders of the Disorders of the rotator cuffrotator cuff
The commonest cause of The commonest cause of pain around the shoulder.pain around the shoulder.

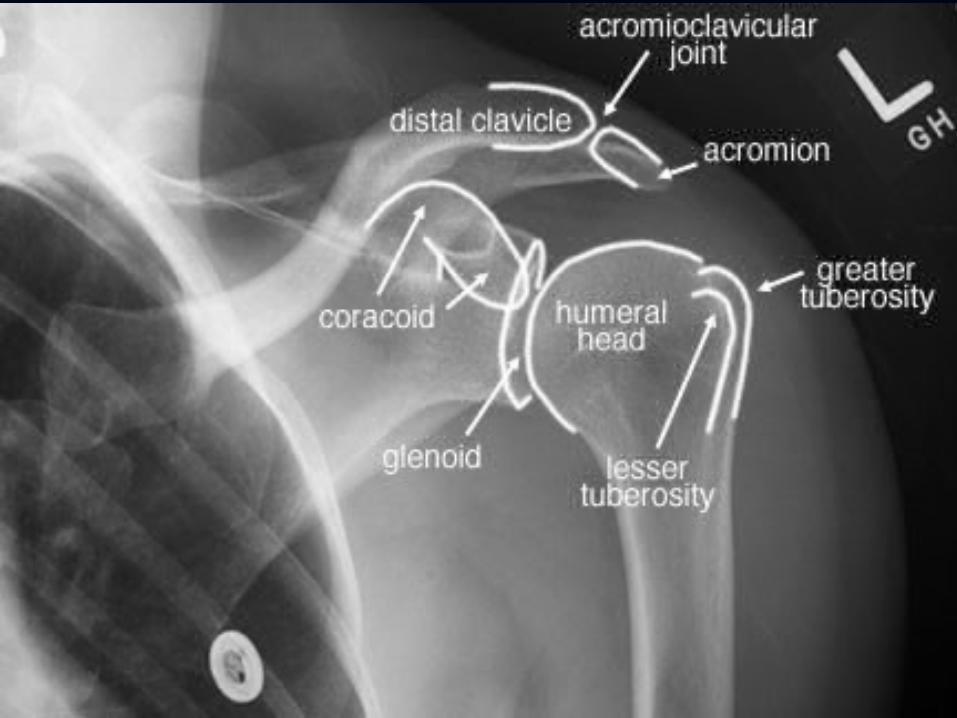
Rotator cuff anatomyRotator cuff anatomy
Consist of tendons of:Consist of tendons of: Supraspinatus.Supraspinatus. Infraspinatus.Infraspinatus. Subscapularis.Subscapularis. Teres minor.Teres minor.
Fused to the capsule of shoulder joint Fused to the capsule of shoulder joint and insert around the greater and insert around the greater tuberosity.tuberosity.
Function: Abduction and stabilize the Function: Abduction and stabilize the shoulder during movement.shoulder during movement.

Rotator cuff syndrome is Rotator cuff syndrome is caused by 5 conditions:caused by 5 conditions:
Supraspinatus tendinitis Supraspinatus tendinitis (impingement syndrome).(impingement syndrome).
Rupture of the rotator cuff.Rupture of the rotator cuff. Acute calcific tendinitis.Acute calcific tendinitis. Biceps tendinitis and /or rupture.Biceps tendinitis and /or rupture. Adhesive capsulitis (frozen Adhesive capsulitis (frozen
shoulder).shoulder).

Impingement syndromeImpingement syndrome(supraspinatus tendinitis)(supraspinatus tendinitis)
Cause: Repetitive compression or Cause: Repetitive compression or rubbing of the supraspinatus tendon rubbing of the supraspinatus tendon under the coracoacromial arch during under the coracoacromial arch during abduction of the arm; abduction of the arm;
As in painting a wall or cleaning a As in painting a wall or cleaning a window.window.
Other predisposing factors:Other predisposing factors: Acromiocalvicular joint OA,Acromiocalvicular joint OA, Gout and rheumatoid arthritis.Gout and rheumatoid arthritis.
Pathogenisis of Pathogenisis of supraspinatus tendinitis: supraspinatus tendinitis: ((wear, tear and repair)wear, tear and repair)
1.1. Edema and swelling,Edema and swelling,
2.2. Minute tears develop.Minute tears develop.
3.3. Scarring, fibrocartilagenous Scarring, fibrocartilagenous metaplasia or calcification in the metaplasia or calcification in the tendon.tendon.
4.4. Healing or partial or complete tears.Healing or partial or complete tears.
5.5. The adjacent tendon of the long head The adjacent tendon of the long head of biceps often involved by tendinitis of biceps often involved by tendinitis or tear.or tear.


Clinical featuresClinical features3 clinical patterns:3 clinical patterns:
1.1. Subacute tendinitis (painful arc Subacute tendinitis (painful arc syndrome):syndrome):
Age <40 years.Age <40 years. Anterior shoulder pain after vigorous or Anterior shoulder pain after vigorous or
unaccustomed activity.unaccustomed activity. Tenderness over the anterior edge of Tenderness over the anterior edge of
the acromion.the acromion. The painful arc: The painful arc: pain on active pain on active
abduction of the shoulder between 60 abduction of the shoulder between 60 and 120 degrees.and 120 degrees.



2- Chronic tendinitis2- Chronic tendinitis
Age 40-50 years.Age 40-50 years. History of recurrent attacks of History of recurrent attacks of
subacute tendinitis.subacute tendinitis. Pain worse at night and on lying on Pain worse at night and on lying on
affected side.affected side. Slight stiffness.Slight stiffness. Tenderness over the bicipital groove Tenderness over the bicipital groove
(biceps tendinitis).(biceps tendinitis).
3- Cuff disruption3- Cuff disruption(partial or full thickness (partial or full thickness
tear)tear) Age >45.Age >45. History of refractory shoulder pain History of refractory shoulder pain
with increasing stiffness and with increasing stiffness and weakness.weakness.
Partial tears; Partial tears; abduction is possible abduction is possible but weak.but weak.
Full-thickness tear; Full-thickness tear; abduction of the abduction of the arm is not possible.arm is not possible.
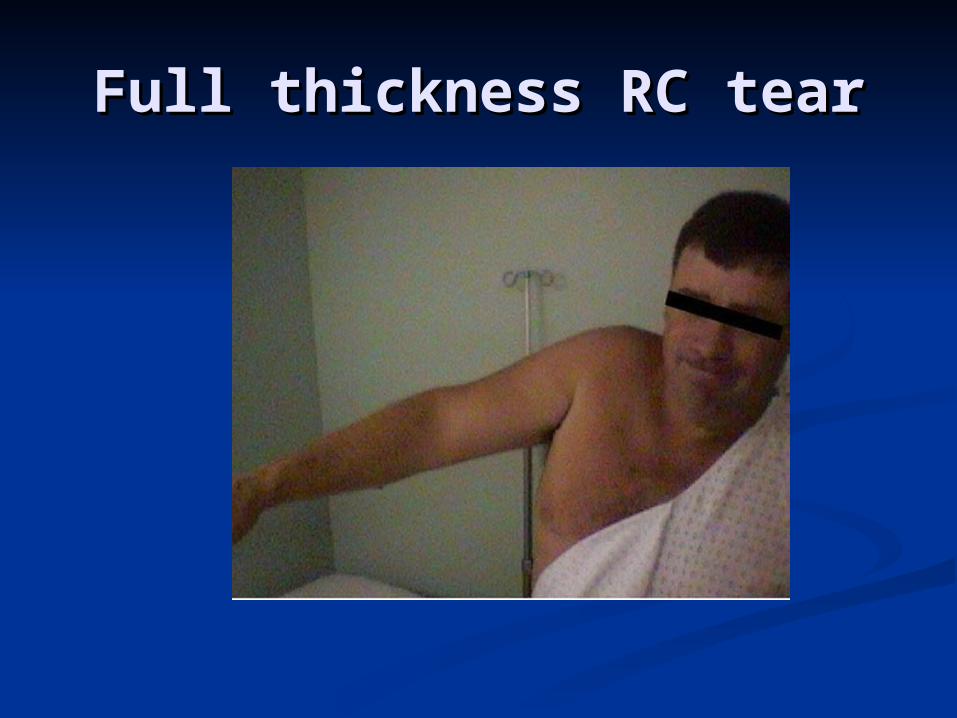
Full thickness RC tearFull thickness RC tear

Treatment Treatment Conservative treatmentConservative treatment
Uncomplicated impingement syndrome is Uncomplicated impingement syndrome is often self-limiting by eliminating the often self-limiting by eliminating the aggravating activity.aggravating activity.
Avoid impingement position (abduction, Avoid impingement position (abduction, slight flexion and internal rotation).slight flexion and internal rotation).
Physiotherapy; ultrasound and active Physiotherapy; ultrasound and active exercise.exercise.
NSAID. If fails,NSAID. If fails, Local injection of corticosteroid in the Local injection of corticosteroid in the
subacromial space.subacromial space.

Surgical treatmentSurgical treatment
Indications:Indications: Persistent symptoms >3months despite Persistent symptoms >3months despite
conservative treatment.conservative treatment. Younger patients with full thickness Younger patients with full thickness
tear.tear. Open or arthroscopic acromioplasty.Open or arthroscopic acromioplasty. Repair of rotator cuff tear.Repair of rotator cuff tear.

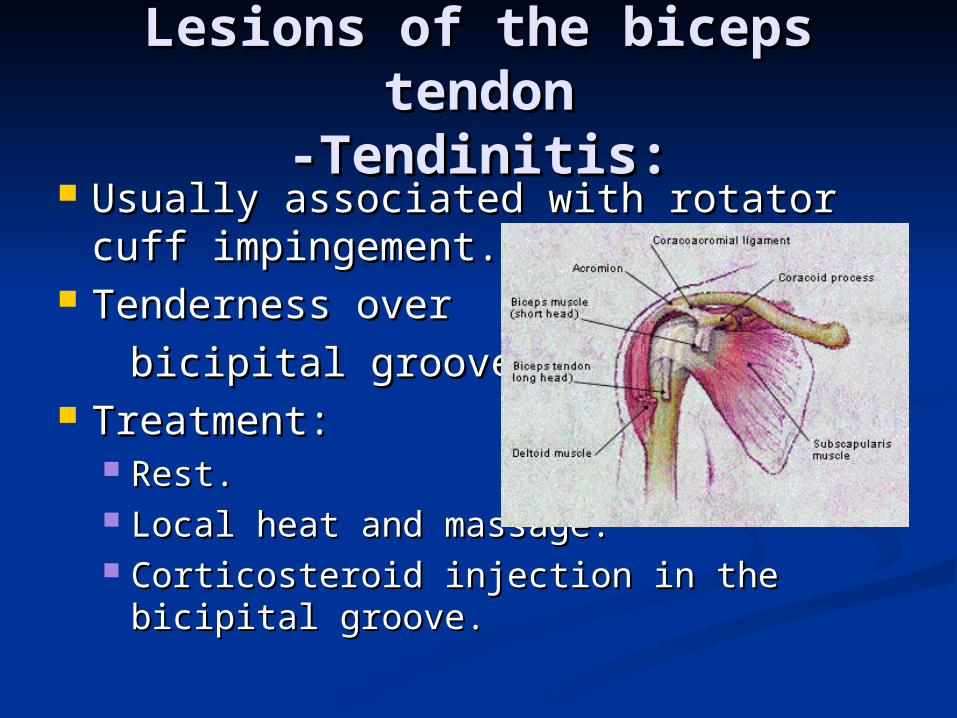
Lesions of the biceps Lesions of the biceps tendontendon
-Tendinitis:-Tendinitis: Usually associated with rotator cuff Usually associated with rotator cuff
impingement.impingement. Tenderness over Tenderness over
bicipital groove.bicipital groove. Treatment: Treatment:
Rest.Rest. Local heat and massage.Local heat and massage. Corticosteroid injection in the bicipital Corticosteroid injection in the bicipital
groove.groove.

Rupture of long head of Rupture of long head of bicepsbiceps
Usually accompany rotator cuff Usually accompany rotator cuff disruption.disruption.
Age >50.Age >50. Snap in the shoulder after lifting an Snap in the shoulder after lifting an
object.object. Lump in the lower arm on flexing the Lump in the lower arm on flexing the
elbow.elbow. Treatment; conservative.Treatment; conservative.

Adhesive capsulitisAdhesive capsulitis(Frozen shoulder)(Frozen shoulder)
Progressive pain and stiffness of the Progressive pain and stiffness of the shoulder which usually resolves shoulder which usually resolves spontaneously after about 18 spontaneously after about 18 months.months.
Cause; unknown.Cause; unknown. Pathology: fibroblast proliferation in Pathology: fibroblast proliferation in
the joint capsule.the joint capsule.

Frozen shoulderFrozen shoulder
Associated with:Associated with: Diabetes mellitus.Diabetes mellitus. DupuytrenDupuytren’’s disease.s disease. Hyperlipidemia.Hyperlipidemia. Hyperthyroidism.Hyperthyroidism. Cardiac disease.Cardiac disease. Hemiplegia.Hemiplegia.

Frozen shoulderFrozen shoulderClinical featuresClinical features
Age: 40-60.Age: 40-60. Pain; gradually increasing, Pain; gradually increasing,
disappear within 6 months.disappear within 6 months. Stiffness; gradually appears as the Stiffness; gradually appears as the
pain subside, persist for 6-12 months pain subside, persist for 6-12 months then start thawing.then start thawing.
Passive and active movement is Passive and active movement is restricted in all directions.restricted in all directions.

Frozen shoulderFrozen shoulderTreatmentTreatment
Conservaive: Conservaive: during the painful stage:during the painful stage: Reassurance.Reassurance. Analgesics and antiinflammatory.Analgesics and antiinflammatory. Exersice (pendulum).Exersice (pendulum).
After pain subside:After pain subside: Manipulation under anesthesia with Manipulation under anesthesia with
Steroid injection of methyleprednisolone Steroid injection of methyleprednisolone and lignocaine (risk of fracture neck of and lignocaine (risk of fracture neck of humerus in porotic patients).humerus in porotic patients).

Surgical treatmentSurgical treatment
Surgical release is Indicated for Surgical release is Indicated for persistent and disabling cases. persistent and disabling cases.


















