Shoulder and Pectoral

of 95
Transcript of Shoulder and Pectoral
-
8/8/2019 Shoulder and Pectoral
1/95
www.Examville.com
Online practice tests, live classes, tutoring, study guidesQ&A, premium content and more .
-
8/8/2019 Shoulder and Pectoral
2/95
Shoulder and PectoralShoulder and Pectoral
regionregion
-
8/8/2019 Shoulder and Pectoral
3/95
THE SCAPULATHE SCAPULA
Supraspinatus Fossa:Supraspinatus Fossa: Depression in theDepression in thescapula, above the scapular spine.scapula, above the scapular spine.
I nfraspinatus Fossa:I nfraspinatus Fossa: Depression in the scapula,Depression in the scapula,below the scapular spine.below the scapular spine.TR APEZI US MUSCLE: I t is innervated by the spinalTR APEZI US MUSCLE: I t is innervated by the spinalaccessory nerve. H ence with a cervical neckaccessory nerve. H ence with a cervical neckfracture, some people can still shrug theirfracture, some people can still shrug theirshoulders, even though they've lost uppershoulders, even though they've lost upper- -limblimbinnervation, due to residual innervation from thisinnervation, due to residual innervation from thisnerve.nerve.
-
8/8/2019 Shoulder and Pectoral
4/95
TRI ANGLE OF AU SC ULT ATI ONTRI ANGLE OF AU SC ULT ATI ON
On the medial back, it is an area of littleOn the medial back, it is an area of littlemuscle and hence a good place to listen tomuscle and hence a good place to listen to
the lungs.the lungs.Medial Border : T rapezius muscleMedial Border : T rapezius muscleLateral Border : T eres Major, laterally andLateral Border : T eres Major, laterally anddeep.deep.I nferior Border (base) : Latissimus DorsiI nferior Border (base) : Latissimus Dorsi
-
8/8/2019 Shoulder and Pectoral
5/95
TRI ANGLE OF AU SC ULT ATI ONTRI ANGLE OF AU SC ULT ATI ON
On the medial back, it is an area of littleOn the medial back, it is an area of littlemuscle and hence a good place to listen tomuscle and hence a good place to listen to
the lungs.the lungs.Medial Border : T rapezius muscleMedial Border : T rapezius muscleLateral Border : T eres Major, laterally andLateral Border : T eres Major, laterally anddeep.deep.I nferior Border (base) : Latissimus DorsiI nferior Border (base) : Latissimus Dorsi
-
8/8/2019 Shoulder and Pectoral
6/95
QUAD R ANGULA R SP ACEQUAD R ANGULA R SP ACE
Just medial to the surgical neck of the humerus onJust medial to the surgical neck of the humerus onthe posterior side.the posterior side.Superior border : T eres Minor (posteriorly)Superior border : T eres Minor (posteriorly)I nferior border : T eres Major (anteriorly)I nferior border : T eres Major (anteriorly)Lateral border : Lateral head of the T ricepsLateral border : Lateral head of the T ricepsMedial border : Long head of the T ricepsMedial border : Long head of the T ricepsCONTE NT S: T hese guys can be damaged with aCONTE NT S: T hese guys can be damaged with afracture of the neck of the humerus.fracture of the neck of the humerus.
Axillary Nerve Axillary NerveP osterior Circumflex Humeral ArteryP osterior Circumflex Humeral Artery
-
8/8/2019 Shoulder and Pectoral
7/95
-
8/8/2019 Shoulder and Pectoral
8/95
TRI ANGULAR I NTERV ALTRI ANGULAR I NTERV AL
Between the two heads of the tricepsBetween the two heads of the tricepsmuscle, inferior to the teres major.muscle, inferior to the teres major.
CONTE NT S: CONTE NT S: Deep Brachial ArteryDeep Brachial Artery andandRadial NerveRadial Nerve , both of which continue, both of which continuealong the radial groove of the humerus.along the radial groove of the humerus.
-
8/8/2019 Shoulder and Pectoral
9/95
-
8/8/2019 Shoulder and Pectoral
10/95
Deltoid MuscleDeltoid Muscle
I t inserts on the Deltoid T uberosity of theI t inserts on the Deltoid T uberosity of thehumerus and has multiple actionshumerus and has multiple actions
Anterior part flexes and medially rotates the Anterior part flexes and medially rotates thearm.arm.Posterior part extends and laterally rotatesPosterior part extends and laterally rotatesthe arm.the arm.Lateral fibers abduct the arm.Lateral fibers abduct the arm.
-
8/8/2019 Shoulder and Pectoral
11/95
Abduction of the Arm Abduction of the Arm
STE P I: Movement of supraspinatus andSTE P I: Movement of supraspinatus anddeltoid muscles, until the angle is about 80deltoid muscles, until the angle is about 80at which point the acromion and greaterat which point the acromion and greatertubercle hit each other.tubercle hit each other.STE P II: STE P II: Rotation of the ScapulaRotation of the Scapula, to get the, to get theacromion process out of the way. T heacromion process out of the way. T heSerratus Anterior and T rapezius move theSerratus Anterior and T rapezius move theinferior border of the scapula laterally.inferior border of the scapula laterally.
-
8/8/2019 Shoulder and Pectoral
12/95
PE CT OR ALI S MAJORPE CT OR ALI S MAJOR
Aids in both flexing and extending the arm, Aids in both flexing and extending the arm,depending on part of muscle.depending on part of muscle.
Clavicular HeadClavicular Head : I t flexes the arm.: I t flexes the arm.S ternocostal Head:S ternocostal Head: I t extends the arm.I t extends the arm.
-
8/8/2019 Shoulder and Pectoral
13/95
CLAVIP ECTOR AL FA SCI ACLAVIP ECTOR AL FA SCI AFascia separating the pectoralis major from pectoralisFascia separating the pectoralis major from pectoralisminor, and overlying the pecs, the serratus anterior, andminor, and overlying the pecs, the serratus anterior, andlatissimus dorsi muscles. I t goes from the peclatissimus dorsi muscles. I t goes from the pec- -minor to theminor to theclavicle.clavicle.
Perforations : Perforations : T heT he Cephalic VeinCephalic Vein goes through the membrane to become thegoes through the membrane to become theaxillary vein.axillary vein.T heT he Thoracoacromial ArteryThoracoacromial Artery comes from axillary artery andcomes from axillary artery andperfuses the deltoid and pecperfuses the deltoid and pec- -minor muscles.minor muscles.
T he subclavius muscle is completely invested by the fascia,T he subclavius muscle is completely invested by the fascia,both anteriorly and posteriorly.both anteriorly and posteriorly.Costocoracoid LigamentCostocoracoid Ligament is the strongest part of theis the strongest part of thefascia, going from the 1st rib to the coracoid process. I t fascia, going from the 1st rib to the coracoid process. I t travels along the lower border of the subclavius.travels along the lower border of the subclavius.
-
8/8/2019 Shoulder and Pectoral
14/95
CEP HALIC VEI N (CEP HALIC VEI N ( CLI NI CAL)CLI NI CAL)
A surgeon may pass a fine tube through the A surgeon may pass a fine tube through theCephalic VeinCephalic Vein ------------> Axillary Vein> Axillary Vein ------------>>SubclavvianSubclavvian ------------> S VC> S VC ------------> H eart to> H eart towithdraw blood.withdraw blood.
-
8/8/2019 Shoulder and Pectoral
15/95
THE AXI LLATHE AXI LLA
Borders of the Axilla : Borders of the Axilla : Anterior Border : T he pectoralis major and minor, and Anterior Border : T he pectoralis major and minor, andthe subclavius, plus investing fascia (Clavipectoralthe subclavius, plus investing fascia (Clavipectoralfascia).fascia).Base of the Axilla : T he skin of the armpit, superficialBase of the Axilla : T he skin of the armpit, superficialfascia.fascia.
Apex of the Axilla : T he root of the neck, through which Apex of the Axilla : T he root of the neck, through whichthe brachial plexus of nerves and vessels travels.the brachial plexus of nerves and vessels travels.
Medial Border : Serratus Anterior and intercostalMedial Border : Serratus Anterior and intercostalmuscles.muscles.Posterior Border : Subscapularis, Latissimus Dorsi, andPosterior Border : Subscapularis, Latissimus Dorsi, andT eres Minor.T eres Minor.
-
8/8/2019 Shoulder and Pectoral
16/95
THE AXI LLATHE AXI LLA
CONTE NT S: CONTE NT S: T he axillary arteryT he axillary arteryT
he axillary veinT
he axillary veinT he Brachial PlexusT he Brachial PlexusT he Axillary group of lymph nodesT he Axillary group of lymph nodes
-
8/8/2019 Shoulder and Pectoral
17/95
AXI LLARY ART ERY AXI LLARY ART ERY
Branches of the Axillary Artery.Branches of the Axillary Artery.1st Part of Axillary Artery:1st Part of Axillary Artery: Above the pectoralis Above the pectoralisminor. H as 1 branch.minor. H as 1 branch.
Superior
Thoracic Artery
Superior
Thoracic Artery2nd Part of Axillary Artery:2nd Part of Axillary Artery: Dir ectly d eep to theDir ectly d eep to the
Pecto rali s Mi no r . H a s 2 bra n ches.Pect o rali s Mi no r . H a s 2 bra n ches.Thoracoacromial ArteryThoracoacromial Artery (pierces clavipectoral fascia)(pierces clavipectoral fascia)
Deltoid Branch of ThoracoacromialDeltoid Branch of Thoracoacromial
P ectoralis Branch of ThoracoacromialP ectoralis Branch of Thoracoacromial ..Lateral Thoracic ArteryLateral Thoracic Artery (aka E xternal Mammary(aka E xternal Mammary Artery) Artery) ---- important source of blood for mammaryimportant source of blood for mammaryglands.glands.
-
8/8/2019 Shoulder and Pectoral
18/95
AXI LLARY ART ERY AXI LLARY ART ERY3 r d Part of Axillary Art ery :3 r d Part of Axillary Art ery : Be l o w t he pec t o rali s m i no r . H a sBel o w t he pec t o rali s m i no r . H a s3 bra nches.3 bra nches.
Anterior Circumflex Humeral Artery Anterior Circumflex Humeral ArteryP osterior Circumflex Humeral ArteryP osterior Circumflex Humeral Artery ---- passes throughpasses throughQuadrangular space along with the axillary nerve.Quadrangular space along with the axillary nerve.
And anterior and posterior circumflex humerals anastomose with each And anterior and posterior circumflex humerals anastomose with eachother around the lateral neck of the humerus.other around the lateral neck of the humerus.T he posterior circumflex also anastomoses with the deep brachialT he posterior circumflex also anastomoses with the deep brachialartery.artery.
Subscapular ArterySubscapular Artery ---- largest branch which supplies muscles of largest branch which supplies muscles of posterior wall (scapula)posterior wall (scapula)
Circumflex Scapular ArteryCircumflex Scapular Artery branches off and proceeds posteriorlybranches off and proceeds posteriorlythrough thethrough the triangular spacetriangular space. .Thoracodorsal ArteryThoracodorsal Artery travels along with thoracodorsal nerve.travels along with thoracodorsal nerve.
-
8/8/2019 Shoulder and Pectoral
19/95
-
8/8/2019 Shoulder and Pectoral
20/95
TH YROCER VIC AL TRUNKTH YROCER VIC AL TRUNK
An arterial branch that comes off the subclavian artery, An arterial branch that comes off the subclavian artery,before it turns into the Axillary Artery. I t has the followingbefore it turns into the Axillary Artery. I t has the followingbranches : branches : Transverse Cervical Artery:Transverse Cervical Artery: T urns into the DorsalT urns into the DorsalScapular Artery.Scapular Artery.
Dorsal Scapular Artery:Dorsal Scapular Artery: Branch on the posterior side, where it Branch on the posterior side, where it supplies the Levator Scapulae and R homboids, along with thesupplies the Levator Scapulae and R homboids, along with theDorsal Scapular N.Dorsal Scapular N.
The Suprascapular Artery:The Suprascapular Artery: H eads around the scapularH eads around the scapularnotch and anastomoses with thenotch and anastomoses with the circum f lex arter y circum f lex arter y to f ormto f ormone o f the main collateral channels around the scapula.one o f the main collateral channels around the scapula.
Suprascapular N. follows the suprascapular artery to supply to theSuprascapular N. follows the suprascapular artery to supply to thesupraspinatus and infraspinatus.supraspinatus and infraspinatus.
-
8/8/2019 Shoulder and Pectoral
21/95
AX I LLARY L Y MPH NODE S AX I LLARY L Y MPH NODE ST he apical group is the most crucial for spreadingT he apical group is the most crucial for spreadingof breast cancer. I f it has gotten to the axillaryof breast cancer. I f it has gotten to the axillarygroup, you is in trouble.group, you is in trouble.
Lateral Group:Lateral Group: Drains the upper limb. LocatedDrains the upper limb. Locatednear brachial artery.near brachial artery.Subscapular Group:Subscapular Group: Drains the scapular regionDrains the scapular regionand posterior thoracic wall.and posterior thoracic wall.
P ectoral Group:P ectoral Group: Drains the anterior thorax andDrains the anterior thorax andsome of mammary glands. Assoc. with lateralsome of mammary glands. Assoc. with lateralthoracic artery.thoracic artery.
-
8/8/2019 Shoulder and Pectoral
22/95
AX I LLARY L Y MPH NODE S . AX I LLARY L Y MPH NODE S .
CENTR AL G ROUP :CENTR AL G ROUP : I t receives the lymphI t receives the lymphfrom the previous three groups. I t forms thefrom the previous three groups. I t forms thelargest group and is often palpable uponlargest group and is often palpable uponexamination.examination.
APIC AL G ROUP : APIC AL G ROUP : T he only one above theT he only one above thepectoralis minor. I t receives lymph from thepectoralis minor. I t receives lymph from thecentral group as well as other locales, andcentral group as well as other locales, anddumps into the subclavian trunk.dumps into the subclavian trunk.
-
8/8/2019 Shoulder and Pectoral
23/95
THE BR ACHI AL PLE XUS OF NERVE STHE BR ACHI AL PLE XUS OF NERVE S
CERVI CALR OOT S of the Plexus : CERVI CALR OOT S of the Plexus : Dorsal Scapular ( C5)Dorsal Scapular ( C5)Long Thoracic Nerve ( C5 ,C6 ,C7)Long Thoracic Nerve ( C5 ,C6 ,C7) ..
R uns along the Serratus Anterior superficially. Y ouR uns along the Serratus Anterior superficially. Y ougotta watch it during a mastectomygotta watch it during a mastectomy -- -- it could be cut it could be cut accidentally.accidentally.
CLI NI CALCLI NI CAL ---- if the Long T horacic is accidentally cut,if the Long T horacic is accidentally cut, Y ou will get Y ou will get W inged ScapulaW inged Scapula . T he long T horacic. T he long T horacicwill no longer hold the Scapula in place, viawill no longer hold the Scapula in place, viaR homboids and Serratus Anterior.R homboids and Serratus Anterior.
-
8/8/2019 Shoulder and Pectoral
24/95
THE BR ACHI AL PLE XUS OF NERVE STHE BR ACHI AL PLE XUS OF NERVE S
SUPERI OR TR UNK SUPERI OR TR UNK ---- C5, C6, part of C4C5, C6, part of C4Direct BranchesDirect Branches
Suprascapular Nerve ( C5 ,C6)Suprascapular Nerve ( C5 ,C6)Subclavius Nerve ( C5 ,C6)Subclavius Nerve ( C5 ,C6)
ANTERI OR DIVI SI ON ANTERI OR DIVI SI ON ------------> LA TER AL COR D > LATER AL COR D POSTERI OR DIVI SI ON POSTERI OR DIVI SI ON ------------> P OSTERI OR > P OSTERI OR
COR D COR D
-
8/8/2019 Shoulder and Pectoral
25/95
THE BR ACHI AL PLE XUS OF NERVE STHE BR ACHI AL PLE XUS OF NERVE S
MI DDLE TR UNK MI DDLE TR UNK ---- C7C7 ANTERI OR DIVI SI ON ANTERI OR DIVI SI ON ------------> LA TER AL COR D > LATER AL COR D
POSTERI
OR
DIVI
SION POS
TERIO
R D
IVIS
ION ------------> P OS
TERIO
R > P OS
TERIO
R COR D COR D
-
8/8/2019 Shoulder and Pectoral
26/95
THE BR ACHI AL PLE XUS OF NERVE STHE BR ACHI AL PLE XUS OF NERVE S
I NFERI OR TR UNK I NFERI OR TR UNK ---- C8, L1C8, L1 ANTERI OR DIVI SI ON ANTERI OR DIVI SI ON ------------> M E DI AL COR D > M E DI AL COR D
POSTERI
OR
DIVI
SION POS
TERIO
R D
IVIS
ION ------------> P OS
TERIO
R > P OS
TERIO
R COR D COR D
-
8/8/2019 Shoulder and Pectoral
27/95
THE BR ACHI AL PLE XUS OF NERVE STHE BR ACHI AL PLE XUS OF NERVE S
LATER AL COR D LATER AL COR D Gives off theGives off the Lateral P ectoral Nerve.Lateral P ectoral Nerve.(mammary glands)(mammary glands)Becomes theBecomes the MUSC ULOCUT ANEOU S NER VEMUSC ULOCUT ANEOU S NER VE( C5 ,C6 ,C7) .( C5 ,C6 ,C7) .Forms a branch with the medial cord, to formForms a branch with the medial cord, to form
the Median Nerve.the Median Nerve.
-
8/8/2019 Shoulder and Pectoral
28/95
THE BR ACHI AL PLE XUS OF NERVE STHE BR ACHI AL PLE XUS OF NERVE S
ME DI AL COR D ME DI AL COR D Gives off the Medial Pectoral,Gives off the Medial Pectoral, MedialMedialBrachiocutaneousBrachiocutaneous , and, and MedialMedial
Antebrachial Cutaneous Antebrachial Cutaneous Nerves. (medialNerves. (medialaspect of arm)aspect of arm)Forms a branch with the Lateral Cord, to formForms a branch with the Lateral Cord, to form
the Median Nerve.the Median Nerve.Becomes theBecomes the ULNAR NER VE ( C8 ,T1 , someULNAR NER VE ( C8 ,T1 , someC7) .C7) .
-
8/8/2019 Shoulder and Pectoral
29/95
THE BR ACHI AL PLE XUS OF NERVE STHE BR ACHI AL PLE XUS OF NERVE S
POSTERI OR COR D POSTERI OR COR D Gives off the Upper and Lower SubscapularGives off the Upper and Lower SubscapularNerves, and theNerves, and the Thoracodorsal NerveThoracodorsal Nerve ..Forms theForms the AXI LLARY NER VE ( C5 ,C6) AXI LLARY NER VE ( C5 ,C6) ..Becomes theBecomes the R AD I AL NE R VE ( C5 ,C6 ,C7 ,C8)R AD I AL NE R VE ( C5 ,C6 ,C7 ,C8)
-
8/8/2019 Shoulder and Pectoral
30/95
THE BR ACHI AL PLE XUS OF NERVE STHE BR ACHI AL PLE XUS OF NERVE S
MEDI AN NE R VE:MEDI AN NE R VE: Formed by the union of Formed by the union of the anterior divisions of the lateral andthe anterior divisions of the lateral andmedial cords. I t is the bottommedial cords. I t is the bottom- -middle part of middle part of the "M"the "M"
-
8/8/2019 Shoulder and Pectoral
31/95
THE BR ACHI AL PLE XUS OF NERVE STHE BR ACHI AL PLE XUS OF NERVE S(clinical)(clinical)
DUCHENNEDUCHENNE--ERB P AR AL YSIS :ERB P AR AL YSIS : Damage to the UpperDamage to the UpperT runk of the Brachial PlexusT runk of the Brachial PlexusE xcessive downward traction of the arm during birth,E xcessive downward traction of the arm during birth,which can tear the upper trunk at its root.which can tear the upper trunk at its root.
T his cuts off the suprascapular and subclavius completely,T his cuts off the suprascapular and subclavius completely,as well as most of axillary nerve. Y ou lose shoulderas well as most of axillary nerve. Y ou lose shouldermovement.movement.Symptom : T he arm just droops there, medially rotated,Symptom : T he arm just droops there, medially rotated,elbow extended, shoulder adducted, forearm pronated.elbow extended, shoulder adducted, forearm pronated.Waiter's Tip Position.Waiter's Tip Position.Erb's Point:Erb's Point: T he location of the superior trunk, where C5T he location of the superior trunk, where C5and C6 unite, and where the Suprascapular and Subclaviusand C6 unite, and where the Suprascapular and Subclaviusare given off.are given off.
-
8/8/2019 Shoulder and Pectoral
32/95
THE BR ACHI AL PLE XUS OF NERVE STHE BR ACHI AL PLE XUS OF NERVE S(clinical)(clinical)
KLUMPKE'S P AR AL YSIS :KLUMPKE'S P AR AL YSIS : Damage to the lower trunkDamage to the lower trunk(C8(C8--T 1).T 1).Loss of most of median and especiallyLoss of most of median and especially ulna r ulna r ne r ves.ne r ves.Symptoms : Symptoms :
Clawed hands due to loss of innervation of intrinsic muscles ( T 1) of Clawed hands due to loss of innervation of intrinsic muscles ( T 1) of the hand.the hand.Loss of sensation on medial aspect of arm, forearm, and hand (dueLoss of sensation on medial aspect of arm, forearm, and hand (dueto loss of ulnar nerve).to loss of ulnar nerve).
Horner's Syndrome:Horner's Syndrome: Associated problem; cervical Associated problem; cervicalsympathetic paralysis, resulting in : sympathetic paralysis, resulting in :
Constriction of pupils.Constriction of pupils.E nophthalmosE nophthalmos ---- apparent recession of eyeballs.apparent recession of eyeballs.
-
8/8/2019 Shoulder and Pectoral
33/95
THE ARMTHE ARMTHE HUME RUS THE HUME RUS Radial Groove:Radial Groove: T he region of the humerus along which the radial nerveT he region of the humerus along which the radial nervetravels, just posteroinferior to the Deltoid T uberosity.travels, just posteroinferior to the Deltoid T uberosity.
CLI NI CAL: T hus a fracture in the middle of the radius could easily damage the radialCLI NI CAL: T hus a fracture in the middle of the radius could easily damage the radialnerve.nerve.CONTE NT S of R adial Groove : CONTE NT S of R adial Groove :
Radial NerveRadial NerveDeep Brachial ArteryDeep Brachial Artery
Surgical Neck of the Humerus:Surgical Neck of the Humerus: T heT he Axillary Nerve Axillary Nerve wraps around thewraps around thesurgical neck of the humerus. T hus injuries to the neck can damage that surgical neck of the humerus. T hus injuries to the neck can damage that nerve.nerve.Cutaneous I nnervation of the ArmCutaneous I nnervation of the Arm
Axillary Nerve: Axillary Nerve: Supplies the skin over the deltoid muscle.Supplies the skin over the deltoid muscle.Radial Nerve:Radial Nerve: Posterior of arm and forearm.Posterior of arm and forearm.
T he lateral dorsal aspect of the hand (posterior of thumb and index finger up to theT he lateral dorsal aspect of the hand (posterior of thumb and index finger up to theDI P joint).DI P joint).
Medial Antebrachial Cutaneous Nerve:Medial Antebrachial Cutaneous Nerve: Supplies much of the anterior skinSupplies much of the anterior skinof arm.of arm.
-
8/8/2019 Shoulder and Pectoral
34/95
THE ARMTHE ARM
BR ACHI AL ART ERY :BR ACHI AL ART ERY : Supplies the arm.Supplies the arm.T heT he Deep Brachial ArteryDeep Brachial Artery comes off the brachialcomes off the brachialartery to curl around the back of the humerus,artery to curl around the back of the humerus,along the radial groove, to supply to the T riceps.along the radial groove, to supply to the T riceps.
P osterior Circumflex Humeral:P osterior Circumflex Humeral: Deep Brachial givesDeep Brachial givesoff this branch, which goes back up arm to theoff this branch, which goes back up arm to theQuadrangular space.Quadrangular space.
Radial CollateralRadial Collateral andand Middle Collateral ArteriesMiddle Collateral Arterieswhich join up with R adial R ecurrent to form elbowwhich join up with R adial R ecurrent to form elbowanastomoses.anastomoses.
-
8/8/2019 Shoulder and Pectoral
35/95
THE ARMTHE ARM
MUSC ULOCUT ANEOU S NER VEMUSC ULOCUT ANEOU S NER VE: T he: T hemajor innervator of the arm.major innervator of the arm.I t goes straight through the coracobrachialisI t goes straight through the coracobrachialismuscle to innervate the anterior aspect of muscle to innervate the anterior aspect of the brachialis.the brachialis.Lateral Antebrachial Cutaneous Nerve:Lateral Antebrachial Cutaneous Nerve:
After innervating the brachialis, it goes to After innervating the brachialis, it goes tothe anterior arm to innervate the skin of thethe anterior arm to innervate the skin of theanterior arm.anterior arm.
-
8/8/2019 Shoulder and Pectoral
36/95
I ntermuscular SeptaI ntermuscular Septa
F ibrous sheath that separates the anteriorF ibrous sheath that separates the anteriorand posterior compartments of the forearm.and posterior compartments of the forearm.
CONTE
NT
S OF
IN
TERMUSCULA
RS
EP
TUM
: CON
TEN
TS O
F IN
TERMUSCULA
RS
EP
TUM
: Deep Brachial ArteryDeep Brachial Artery
R adial NerveR adial NerveBasilic VeinBasilic VeinUlnar NerveUlnar NerveMedian NerveMedian Nerve
-
8/8/2019 Shoulder and Pectoral
37/95
ARTERI AL AN AST OMOSE S AR OUND ARTERI AL AN AST OMOSE S AR OUND E LBOW E LBOW
Collateral Branches off the Ulnar ArteryCollateral Branches off the Ulnar ArteryP osterior Ulnar Recurrent Artery:P osterior Ulnar Recurrent Artery: Medial anastomoses with I nferiorMedial anastomoses with I nferiorUlnar Collateral.Ulnar Collateral.
Anterior Ulnar Recurrent Artery: Anterior Ulnar Recurrent Artery: Medial anastomoses with SuperiorMedial anastomoses with SuperiorUlnar Collateral.Ulnar Collateral.
Collateral Branches off theR
adial ArteryCollateral Branches off theR
adial ArteryRadial Recurrent Artery:Radial Recurrent Artery: Lateral anastomoses with R adial CollateralLateral anastomoses with R adial CollateralCollateral Branches off the Brachial Artery : Collateral Branches off the Brachial Artery :
I nferior Ulnar Collateral:I nferior Ulnar Collateral: (Ulnar R ecurrent)(Ulnar R ecurrent)Superior Ulnar Collateral:Superior Ulnar Collateral: (Ulnar R ecurrent)(Ulnar R ecurrent)
Collateral Branches off the Deep Brachial Artery : Collateral Branches off the Deep Brachial Artery :
Radial Collateral Artery:Radial Collateral Artery: (R
adialR
ecurrent)(R
adialR
ecurrent)Middle Collateral Artery:Middle Collateral Artery: Anastomoses with I nterosseus R ecurrent, but Anastomoses with I nterosseus R ecurrent, but there is variety.there is variety.
-
8/8/2019 Shoulder and Pectoral
38/95
ULN AR ARTERY ULN AR ARTERY
One of the terminal branches of the BrachialOne of the terminal branches of the Brachial Artery. Artery.Gives off theGives off the Common I nterosseusCommon I nterosseus
Artery Artery , a short stub which divides into two, a short stub which divides into twoparts : parts :
Anterior I nterosseus Artery: Anterior I nterosseus Artery: Supplies theSupplies thedeep muscles of the flexor forearm.deep muscles of the flexor forearm.P osterior I nterosseus Artery:P osterior I nterosseus Artery: Supplies theSupplies theentire extensor forearm.entire extensor forearm.
-
8/8/2019 Shoulder and Pectoral
39/95
BREAK TI MEBREAK TI ME
-
8/8/2019 Shoulder and Pectoral
40/95
THE EX TENSOR FOREARMTHE EX TENSOR FOREARMBR ACHI OR ADI ALI S: CLI NI CALBR ACHI OR ADI ALI S: CLI NI CAL ---- it may become damagedit may become damagedduring a distal radial fracture, because it inserts on theduring a distal radial fracture, because it inserts on thestyloid process of the radius.styloid process of the radius.COMMON EX TENSOR TENDON:COMMON EX TENSOR TENDON: T he origin of theT he origin of the
superfici al superfici al extensor fore a rm musc l es.It hooks onto theextensor fore a rm musc l es.
It hooks onto thela ter al epicon d yl ela ter al epicon d yl e a nd a nd supr ac on d yla r rid gesupr ac on d yla r rid ge of the humerus.of the humerus.
POST ERI OR I NTEROSS EUS NER VE:POST ERI OR I NTEROSS EUS NER VE: T he Deep BranchT he Deep Branchof the R adial Nerve. I t innervates most muscles of theof the R adial Nerve. I t innervates most muscles of theextensor forearm.extensor forearm.I t pierces the supinator muscle to come into the posteriorI t pierces the supinator muscle to come into the posteriorforearm.forearm.I t travels between the superficial and deep groups of I t travels between the superficial and deep groups of muscles in the posterior forearm.muscles in the posterior forearm.
-
8/8/2019 Shoulder and Pectoral
41/95
THE EX TENSOR FOREARMTHE EX TENSOR FOREARM
P OST ERI OR I NTEROSS EUS ART ERY :P OST ERI OR I NTEROSS EUS ART ERY :Supplies the extensor forearm muscles andSupplies the extensor forearm muscles andtravels with the Posterior I nterosseus Nerve.travels with the Posterior I nterosseus Nerve.I t is a branch of the Common I nterosseusI t is a branch of the Common I nterosseus
Artery, which comes from the Ulnar Artery. Artery, which comes from the Ulnar Artery.
-
8/8/2019 Shoulder and Pectoral
42/95
EXTENSOR RETI NACULUMEXTENSOR RETI NACULUMT he sheath that covers all of the extensor tendonsT he sheath that covers all of the extensor tendonsgoing into the wrist.going into the wrist.OR DER OF E X TE NSOR TE NDONS GOI NG I NT O OR DER OF E X TE NSOR TE NDONS GOI NG I NT O THE WRI ST THE WRI ST
E xtensor Pollicis BrevisE xtensor Pollicis BrevisE xtensor Pollicis LongusE xtensor Pollicis LongusE xtensor Carpi R adialis LongusE xtensor Carpi R adialis LongusE xtensor Carpi R adialis BrevisE xtensor Carpi R adialis Brevis
(E xtensor I ndices, concurrent with and deep to E xtensor(E xtensor I ndices, concurrent with and deep to E xtensorDigitorum)Digitorum)E xtensor DigitorumE xtensor Digitorum
E xtensor Digiti MinimiE xtensor Digiti Minimi
-
8/8/2019 Shoulder and Pectoral
43/95
ANATOMIC AL SNUFFBOX ANATOMIC AL SNUFFBOX : :
I n between theI n between the Extens o r Po llicis Lo ngu s Exten s o r Po llicis Lo ngu s andandExten s o r Po llicis Br ev is Exten s o r Po llicis Br ev is . T he. T he Abdu c t o r Po llicis Abdu c t o r Po llicis Lo ngu s L o ngu s is dir ec t l y l ate r a l t o i t.is dir ec t l y l ate r a l t o i t.T heT he Radial NerveRadial Nerve runs over the superficial part runs over the superficial part of the anatomical snuffbox, to innervate the lateralof the anatomical snuffbox, to innervate the lateralcutaneous hand.cutaneous hand.T heT he Radial ArteryRadial Artery is the "floor" of the snuffbox,is the "floor" of the snuffbox,snugged right on top of the Scaphoid bone.snugged right on top of the Scaphoid bone.
Y ou can take a pulse in anatomical snuffbox, by Y ou can take a pulse in anatomical snuffbox, bypalpating the radial artery against the Scaphoid bone.palpating the radial artery against the Scaphoid bone.
-
8/8/2019 Shoulder and Pectoral
44/95
THE FLEXO R FOREARMTHE FLEXO R FOREARM
THE FLEXO R FOREARMTHE FLEXO R FOREARMMED I AN NE R VE:MED I AN NE R VE: Lies in between theLies in between the f l exo r d igit o rum sup er f ic ial isf l exo r d igit o rum sup er f ic ial is a nd a nd f l exo r d igit o rum pr of u nd u sf l exo r d igit o rum pr of u nd u s in the fo r earm .in the fo r earm .T ra ve l s int o the h a nd d ee p t o theT ra ve l s int o the h a nd d ee p t o the palmar is l o ng u spalmar is l o ng u s ( r ight in the m idd l e,(r ight in the m idd l e,a nte r io r sur f ac e), t ra ve l ing th r o ug h the carpal t u nne l .a nte r io r sur f ac e), t ra ve l ing th r o ug h the carpal t u nne l .Suppl ies all of f l exo r fo r earm E XCE PT theSuppl ies all of f l exo r fo r earm E XCE PT the F l exo r Carp i Ul nar isF l exo r Carp i Ul nar is a nd thea nd them ed ial hal f of them ed ial hal f of the F l exo r Dig it o rum Pr of u nd u sF l exo r Dig it o rum Pr of u nd u s..I NJU RY: Ca n be inj ur ed in w r ist s la shin g a nd carpal t u nne l syn d r o m e.I NJU RY: Ca n be inj ur ed in w r ist s la shin g a nd carpal t u nne l syn d r o m e.
Lost sensation to area supplied by median nerve in hand.Lost sensation to area supplied by median nerve in hand.Paralysis of long flexors of wrist (except the two ulnar flexors)Paralysis of long flexors of wrist (except the two ulnar flexors)T henar muscles atrophy, with the result that opposition of thumb is lost.T henar muscles atrophy, with the result that opposition of thumb is lost.Loss of pronation, depending on where the severance occurs (wrist or elbow)Loss of pronation, depending on where the severance occurs (wrist or elbow)
SUMMARY
OF
INJU
RY: V
ery crippling:
loss of action of thumb andSUMMARY
OF
INJU
RY: V
ery crippling:
loss of action of thumb andcutaneous sensation on palm of hand.cutaneous sensation on palm of hand.
-
8/8/2019 Shoulder and Pectoral
45/95
ULNAR NER VEULNAR NER VEI n the forearm, it supplies theI n the forearm, it supplies the Flexor Carpi U lnarisFlexor Carpi U lnarisand the medial half of theand the medial half of the Flexor Di g itorumFlexor Di g itorumProfundusProfundus. .I t passesI t passes superfi c ialsuperfi c ial to the flexor retina c ulum.to the flexor retina c ulum.I NJU RY: Commonly injured around the posteriorI NJU RY: Commonly injured around the posteriorof the medial epi c ondyleof the medial epi c ondyle ---- rig ht where the funnyrig ht where the funnybone is.bone is.
ClawClaw--Hand:Hand: Paralysis of small muscles of handParalysis of small muscles of hand
supplied by Ulnar Nerve.T
his is the result of loss of supplied by Ulnar Nerve.T
his is the result of loss of control over intrinsic hand muscles, which supply thecontrol over intrinsic hand muscles, which supply the"balance" between the long flexor and extensor"balance" between the long flexor and extensortendons. R esult is overtendons. R esult is over- -flexion of distal phalanges andflexion of distal phalanges andextension of proximal phalanges.extension of proximal phalanges.
-
8/8/2019 Shoulder and Pectoral
46/95
R AD I AL NE R VER AD I AL NE R VEE nters the forearm by traveling over the lateral epicondyle.E nters the forearm by traveling over the lateral epicondyle.Splits into two branches.Splits into two branches.Superficial Branch of the Radial Nerve:Superficial Branch of the Radial Nerve: T ravelsT ravels d ee p d ee p t o th e bra chi o ra d i ali st o th e bra chi o ra d i ali s t o go t o th e h an d .t o go t o th e h an d .
Deep Branch of the Radial NerveDeep Branch of the Radial Nerve -- -- Goes deep back toGoes deep back toposterior compartment, where it isposterior compartment, where it is P osteriorP osteriorI nterosseus Nerve.I nterosseus Nerve. thetheI NJURY: I NJURY: W ristW rist- -DropDrop is the sign of radial nerve injury.is the sign of radial nerve injury.
I t is the most frequently injured, due to breaks in the middle of theI t is the most frequently injured, due to breaks in the middle of thehumerus.humerus.Paralysis of the long extensors of the fingers.Paralysis of the long extensors of the fingers.Lateral (radial deviation) of hand is difficult.Lateral (radial deviation) of hand is difficult.Movement (extension and abduction) of thumb is difficult.Movement (extension and abduction) of thumb is difficult.
-
8/8/2019 Shoulder and Pectoral
47/95
I ntrinsic hand musclesI ntrinsic hand muscles
T1 : I NTRI NSIC MUSC LEST1 : I NTRI NSIC MUSC LES ---- All intrinsic muscles All intrinsic musclesof the hand are supplied by T 1 fibers, whetherof the hand are supplied by T 1 fibers, whetherfrom the Ulnar or R adial nerves.from the Ulnar or R adial nerves.
LATER AL AN TEBR ACHI AL CUT ANEOU S LATER AL AN TEBR ACHI AL CUT ANEOU S NER VE:NER VE: From the Musculocutaneous Nerve, it From the Musculocutaneous Nerve, it innervates the lateral part of the anterior forearm.innervates the lateral part of the anterior forearm.MEDI AL AN TEBR ACHI AL CUT ANEOU S MEDI AL AN TEBR ACHI AL CUT ANEOU S
NER VE:NER VE:F
rom the medial cord of the brachialF
rom the medial cord of the brachialplexus, it innervates the medial part of theplexus, it innervates the medial part of thecutaneous flexor forearm.cutaneous flexor forearm.
-
8/8/2019 Shoulder and Pectoral
48/95
Arterial supply Arterial supplyR AD I AL ART ERY :R AD I AL ART ERY : One of the terminal branches of theOne of the terminal branches of theBrachial Artery.Brachial Artery.Gives off the Deep Palmar Arch.Gives off the Deep Palmar Arch.Gives off the Dorsalis Pollicis and Dorsalis I ndices Arteries.Gives off the Dorsalis Pollicis and Dorsalis I ndices Arteries.CLI NI CALCLI NI CAL ---- R AD I AL P ULSER AD I AL P ULSE: On the palmar lateral wrist,: On the palmar lateral wrist,at the location of theat the location of the Radial TrioRadial Trio , you can feel the pulse., you can feel the pulse.
T he R adial Artery is found lateral to theT he R adial Artery is found lateral to the Flexor Carpi RadialisFlexor Carpi Radialisandand Flexor P ollicis LongusFlexor P ollicis Longus tendons at this location in the wrist.tendons at this location in the wrist.T hose are the components of the radial trio.T hose are the components of the radial trio.
PATH: T hen the radial artery goes to the floor of thePATH: T hen the radial artery goes to the floor of theanatomical snuffboxanatomical snuffbox ------------> through the adductor pollicis> through the adductor pollicisand dorsal interosseus musclesand dorsal interosseus muscles ------------> deep palmar arch.> deep palmar arch.
-
8/8/2019 Shoulder and Pectoral
49/95
Arterial supply Arterial supply
ULNAR ART ERY :ULNAR ART ERY : One of the terminalOne of the terminalbranches of the Brachial Artery.branches of the Brachial Artery.
D o
es no
t D o
es no
t pa ss t hro
ugh t heF
lexo
rpa ss t hro
ugh t heF
lexo
rR e t in aculum.R e t in aculum.Gives o ff t he Superficial Palmar Arch.Gives o ff t he Superficial Palmar Arch.
-
8/8/2019 Shoulder and Pectoral
50/95
FLEXOR RETI NACULUMFLEXOR RETI NACULUMT he sheath that contains the flexor tendons on theT he sheath that contains the flexor tendons on theanterior wrist.anterior wrist.Goes from the T rapezium to the Scaphoid.Goes from the T rapezium to the Scaphoid.
C ARP AL TUNNEL SYNDROME:C ARP AL TUNNEL SYNDROME: T heT he Me d ia n Med ia n Nerv eNerv e p a sses d eep to the flexo r r et i n a culum. I f i t pa sses d eep to the flexo r r et i n a culum. I f i t i s e n t ra ppe d , c ar pa l tu nn el sy nd r ome r esults.i s e n t ra ppe d , c ar pa l tu nn el sy nd r ome r esults.
Causes numbness and tingling in the lateral part of theCauses numbness and tingling in the lateral part of thehand supplied by the median nerve, and some motorhand supplied by the median nerve, and some motordysfunction.dysfunction.T reatment : Cut the flexor retinaculum and relieve theT reatment : Cut the flexor retinaculum and relieve thepressure.pressure.
-
8/8/2019 Shoulder and Pectoral
51/95
F lexor ..F lexor ..
MOB I LE W AD:MOB I LE W AD: T he lateral compartment of theT he lateral compartment of theflexor forearm, which is more loosely connectedflexor forearm, which is more loosely connectedthan the other compartments. I t contains twothan the other compartments. I t contains two
muscles : muscles : BrachioradialisBrachioradialisExtensor Carpi Radialis LongusExtensor Carpi Radialis Longus
PALMARI
S LONGUS MUSCLE:
Absent in about PALMARI
S LONGUS MUSCLE:
Absent in about 30% of people, and a good candidate for surgical30% of people, and a good candidate for surgicaltendon transferstendon transfers when it is present.when it is present.
-
8/8/2019 Shoulder and Pectoral
52/95
F lexors F lexors FLEXOR DI GIT ORUM:FLEXOR DI GIT ORUM: Acts differently than the extensor digitorum. Acts differently than the extensor digitorum.Superficial Flexor Digitorum:Superficial Flexor Digitorum: I nserts on the distal phalanx andI nserts on the distal phalanx andcrosses over the DI P joint.crosses over the DI P joint.P rofunda Flexor Digitorum:P rofunda Flexor Digitorum: I nserts on the proximal phalanx andI nserts on the proximal phalanx andcrosses over the P I P joint.crosses over the P I P joint.
SP ACE OF P ARONA:SP ACE OF P ARONA: T he potential space between the superficial andT he potential space between the superficial anddeep groups of anterior musclesdeep groups of anterior muscles -- -- essentially between the F lexoressentially between the F lexorDigitorum Superficialis and F lexor Digitorum Profundus.Digitorum Superficialis and F lexor Digitorum Profundus.FASCI A AN TEBR ACHI ALIS :FASCI A AN TEBR ACHI ALIS : T hick fascial plane over the anteriorT hick fascial plane over the anteriorforearm.forearm.I NTEROSS EUS MEMBR ANE:I NTEROSS EUS MEMBR ANE: Between the radius and ulna, theBetween the radius and ulna, theposterior limit to the anterior compartment. T he Anterior I nterosseusposterior limit to the anterior compartment. T he Anterior I nterosseusNerve and Artery, and the Flexor Digitorum Profundus, are directlyNerve and Artery, and the Flexor Digitorum Profundus, are directlysuperficial to it.superficial to it.
-
8/8/2019 Shoulder and Pectoral
53/95
J OI NTS OF THE U PP ER J OI NTS OF THE U PP ER EXTREMITYEXTREMITY
T ypes of Joints : Joints are structures that connects bones together.T ypes of Joints : Joints are structures that connects bones together.Fibrous Joints:Fibrous Joints: Collagen joints.Collagen joints.
Suture of the skull.Suture of the skull.T heT he i n terosseus m em bra n ei n terosseus m em bra n e betwee n the r a di us a n d ul n a . T hi s i s a type of betwee n the r a di us a n d ul n a . T hi s i s a type of syndesmosissyndesmosis ---- i.e. a sheet of fibrous tissue.i.e. a sheet of fibrous tissue.
Cartilaginous Joints:Cartilaginous Joints:E xamples : E xamples : Epiphyseal PlatesEpiphyseal PlatesCostochondral JointsCostochondral JointsI ntervertebral DiscI ntervertebral DiscPubic SymphysisPubic Symphysis
P rimary Cartilagi no us J o i n ts :P rimary Cartilagi no us J o i n ts : SynchondrosesSynchondroses ---- hyaline cartilage.hyaline cartilage.S ec ond ary Cartilagi no us J o i n ts :S ec ond ary Cartilagi no us J o i n ts : SymphysisSymphysis ---- hyaline cartilage along withhyaline cartilage along withfibrous tissue or fibrous cartilage.fibrous tissue or fibrous cartilage.
-
8/8/2019 Shoulder and Pectoral
54/95
Joints of Upper extremityJoints of Upper extremityT ypes of Joints : Joints are structures that connects bones together.T ypes of Joints : Joints are structures that connects bones together.Fibrous Joints:Fibrous Joints: Collagen joints.Collagen joints.
Suture of the skull.Suture of the skull.T heT he i n terosseus m em bra n ei n terosseus m em bra n e betwee n the r a di us a n d ul n a . T hi s i s a type of betwee n the r a di us a n d ul n a . T hi s i s a type of syndesmosissyndesmosis ---- i.e. a sheet of fibrous tissue.i.e. a sheet of fibrous tissue.
Cartilaginous Joints:Cartilaginous Joints:E xamples : E xamples : Epiphyseal PlatesEpiphyseal PlatesCostochondral JointsCostochondral JointsI ntervertebral DiscI ntervertebral DiscPubic SymphysisPubic Symphysis
P rimary Cartilagi no us J o i n ts :P rimary Cartilagi no us J o i n ts : SynchondrosesSynchondroses ---- hyaline cartilage.hyaline cartilage.S ec ond ary Cartilagi no us J o i n ts :S ec ond ary Cartilagi no us J o i n ts : SymphysisSymphysis ---- hyaline cartilage along withhyaline cartilage along withfibrous tissue or fibrous cartilage.fibrous tissue or fibrous cartilage.
-
8/8/2019 Shoulder and Pectoral
55/95
Joints of upper extremityJoints of upper extremitySynovial J oints:Synovial J oints:
Characterized by four things.Characterized by four things. A A joint ca v ity joint ca v ity, filled with a v iscous lubricant substance, filled with a v iscous lubricant substance -- -- syno v ial fluid.syno v ial fluid. A A syno v ial m em branesyno v ial m em brane, which produces the syno v ial fluid to fill the joint , which produces the syno v ial fluid to fill the joint cav ity.cav ity.
Articular cartilage Articular cartilage\\Fibrous CapsuleFibrous CapsuleT ypes of Synovial JointsT ypes of Synovial Joints
P la n e J o i n t P la n e J o i n t ---- m o vea bl e on l y i n on e a xi s, i n on e p la n e.mo vea bl e on l y i n on e a xi s, i n on e p la n e.H i n g e J o i n t H i n g e J o i n t ---- m o vea bl e on l y i n on e a xi smo vea bl e on l y i n on e a xi s ---- i .e. f l ex i on a n d ex t en si on .i .e. f l ex i on a n d ex t en si on .P i vo t J o i n t P i vo t J o i n t ---- m o vea bl e on l y i n on e a xi smo vea bl e on l y i n on e a xi s ---- i .e. r o tati on .i .e. r o tati on .
Con dyl o i d J o i n t C on dyl o i d J o i n t ---- m o vea bl e i n t wo a xesmo vea bl e i n t wo a xes ---- i .e. f l ex i on i .e. f l ex i on --ex t en si on , o rex t en si on , o ra bduc ti on a bduc ti on --a dduc ti on .a dduc ti on .I t is usually ellipsoid in shape.I t is usually ellipsoid in shape.
S a dd l e J o i n t S a dd l e J o i n t ---- t wo a xes.t wo a xes.Ball a nd S o ck e t J o i n t Ball a nd S o ck e t J o i n t ---- Multi Multi --a xi s m o veme n t .a xi s m o veme n t .
-
8/8/2019 Shoulder and Pectoral
56/95
Movements of jointsMovements of jointsSynovial J oints:Synovial J oints:
Characterized by four things.Characterized by four things. A A joint ca v ity joint ca v ity, filled with a v iscous lubricant substance, filled with a v iscous lubricant substance -- -- syno v ial fluid.syno v ial fluid. A A syno v ial m em branesyno v ial m em brane, which produces the syno v ial fluid to fill the joint , which produces the syno v ial fluid to fill the joint cav ity.cav ity.
Articular cartilage Articular cartilage\\Fibrous CapsuleFibrous CapsuleT ypes of Synovial JointsT ypes of Synovial Joints
P la n e J o i n t P la n e J o i n t ---- m o vea bl e on l y i n on e a xi s, i n on e p la n e.mo vea bl e on l y i n on e a xi s, i n on e p la n e.H i n g e J o i n t H i n g e J o i n t ---- m o vea bl e on l y i n on e a xi smo vea bl e on l y i n on e a xi s ---- i .e. f l ex i on a n d ex t en si on .i .e. f l ex i on a n d ex t en si on .P i vo t J o i n t P i vo t J o i n t ---- m o vea bl e on l y i n on e a xi smo vea bl e on l y i n on e a xi s ---- i .e. r o tati on .i .e. r o tati on .
C on dyl o i d J o i n t C on dyl o i d J o i n t ---- m o vea bl e i n t wo a xesmo vea bl e i n t wo a xes ---- i .e. f l ex i on i .e. f l ex i on --ex t en si on , o rex t en si on , o ra bduc ti on a bduc ti on --a dduc ti on .a dduc ti on .I t is usually ellipsoid in shape.I t is usually ellipsoid in shape.
S a dd l e J o i n t S a dd l e J o i n t ---- t wo a xes.t wo a xes.Ball a nd S o ck e t J o i n t Ball a nd S o ck e t J o i n t ---- Multi Multi --a xi s m o veme n t .a xi s m o veme n t .
-
8/8/2019 Shoulder and Pectoral
57/95
Clinical .Clinical .CLI NI CALCLI NI CAL ---- I njuries / Diseases of the Joints : I njuries / Diseases of the Joints : Dislocation:Dislocation: Complete loss of apposition between twoComplete loss of apposition between twoarticular surfaces.articular surfaces.Subluxation:Subluxation: Partial dislocation; partial loss of appositionPartial dislocation; partial loss of apposition
between two articular surfaces.between two articular surfaces.Osteoarthritis:Osteoarthritis: Degeneration of articular cartilage and/orDegeneration of articular cartilage and/orsurfaces in weight surfaces in weight- -bearing joints, resulting from age and/orbearing joints, resulting from age and/ortrauma.trauma.Rheumatoid Arthritis:Rheumatoid Arthritis: Connective tissue disorderConnective tissue disorderaffecting the whole body, mainly affecting the small jointsaffecting the whole body, mainly affecting the small jointsin terms of joints.in terms of joints.Gout:Gout: Painful inflammation of the joint from excess uricPainful inflammation of the joint from excess uricacid, resulting sodium biurate deposits in joints.acid, resulting sodium biurate deposits in joints.
-
8/8/2019 Shoulder and Pectoral
58/95
Movements of joints .Movements of joints .
CONJUNCT R OT ATI ON: I nstinctive or automaticCONJUNCT R OT ATI ON: I nstinctive or automaticrotation of the forearm, as demonstrated byrotation of the forearm, as demonstrated byCodman's paradox, where you hold your palm toCodman's paradox, where you hold your palm to
your side, abduct it, rotate it anteriorly, and bringyour side, abduct it, rotate it anteriorly, and bringit back to your body, to discover that it is nowit back to your body, to discover that it is nowfacing the other way.facing the other way.
ADJUNCT R OT ATI ON: Deliberate rotation of the ADJUNCT R OT ATI ON: Deliberate rotation of the joint, such as when you point your hands laterally joint, such as when you point your hands laterallyand then try to abduct your arm.and then try to abduct your arm.
-
8/8/2019 Shoulder and Pectoral
59/95
GLENOHUME R AL JOI NT:GLENOHUME R AL JOI NT:ROT ATOR CUFFROT ATOR CUFF : T he tendons of the muscles surrounding the shoulder joint.: T he tendons of the muscles surrounding the shoulder joint.T hey rotate the shoulder.T hey rotate the shoulder.
Anterior Border : Subscapularis Anterior Border : SubscapularisSuperolateral Border : H ead of the bicepsSuperolateral Border : H ead of the bicepsPosterior Border : I nfraspinatus and T eres MinorPosterior Border : I nfraspinatus and T eres MinorSuperior Border : SupraspinatusSuperior Border : Supraspinatus
CLI NI CAL: T he joint is covered on all sides except inferiorly. H ence shoulderCLI NI CAL: T he joint is covered on all sides except inferiorly. H ence shoulderdislocations tend to occur inferiorly.dislocations tend to occur inferiorly.I n this case you have to watch for damage to theI n this case you have to watch for damage to the a xill ary ne rv ea xill ary ne rv e andand P oste ri o r P oste ri o r Cir cumflex Hume ral Ar te ry Cir cumf l ex Hume ral Ar te ry , both of which are directly inferior, in the, both of which are directly inferior, in theQuadrangular Space, because this is straight below the shoulder joint.Quadrangular Space, because this is straight below the shoulder joint.TE ST for Axillary Nerve damage : Cutaneous sensation in the Deltoid regionTE ST for Axillary Nerve damage : Cutaneous sensation in the Deltoid region
THREE DE GREE S OF FREE DOM: Circumduction + R otation. H ence it is aTHREE DE GREE S OF FREE DOM: Circumduction + R otation. H ence it is a
mobile but unstable joint.mobile but unstable joint.T he glenohumeral joint is anT he glenohumeral joint is an in c ongruent inc ongruent joint joint ---- note that the head of the humerusnote that the head of the humerusdoes not fit in perfe c tly with the Glenoid Cavity of the S c apula.does not fit in perfe c tly with the Glenoid Cavity of the S c apula.
ST ABI LIZI NG MUSCLE S: T heST ABI LIZI NG MUSCLE S: T he d e lt o i d d e lt o i d an d an d bic eps bic eps he lp st ab ili ze t he s ho ul d er,he lp st ab ili ze t he s ho ul d er,d ue t o t he i nc o ngruen c e o f t he j o i nt .d ue t o t he i nc o ngruen c e o f t he j o i nt .
-
8/8/2019 Shoulder and Pectoral
60/95
ULNOHUME R AL J OI NT (ELBO W ) ULNOHUME R AL J OI NT (ELBO W )
H as higher stability and lower mobility : only one degree of H as higher stability and lower mobility : only one degree of freedom (flexion / extension).freedom (flexion / extension).The H u mer u s arti cu lates only with the U lnaThe H u mer u s arti cu lates only with the U lna ---- the radi u sthe radi u shas nothing to do with it! has nothing to do with it! Radial Collateral LigamentRadial Collateral Ligament ---- Lateral ligament support.Lateral ligament support.Ulnar Collateral LigamentUlnar Collateral Ligament ---- Medial ligament support.Medial ligament support.CONGR UE NCE: T he Olecranon of the Ulna fits much betterCONGR UE NCE: T he Olecranon of the Ulna fits much better
into the Olecranon Fossa of the H umerus, as compared tointo the Olecranon Fossa of the H umerus, as compared tothe shoulder joint.the shoulder joint.Posterior E lbow : T he joint capsule is lax on the posterior,Posterior E lbow : T he joint capsule is lax on the posterior,so that the elbow can flex and extend.so that the elbow can flex and extend.
-
8/8/2019 Shoulder and Pectoral
61/95
ULNO R AD I AL J OI NT (ELBO W ) ULNO R AD I AL J OI NT (ELBO W )
Proximal Ulnoradial Joint : Proximal Ulnoradial Joint : Annular AnnularLigamentLigament holds the R adial H ead in place inholds the R adial H ead in place inthe R adial Notch of the Ulna.the R adial Notch of the Ulna.I ntermediate Ulnoradial Joint : I ntermediate Ulnoradial Joint : I nterosseusI nterosseusMembraneMembrane holds them together along theholds them together along the
shafts of both bones.shafts of both bones.Distal Ulnoradial Joint : Distal Ulnoradial Joint : Anterior Anterior andandP osterior Ulnoradial LigamentsP osterior Ulnoradial Ligaments ..
-
8/8/2019 Shoulder and Pectoral
62/95
R AD I OC ARP AL J OI NT ( WRIST)R AD I OC ARP AL J OI NT ( WRIST)
T h e R a d ius articulat es with th e Carpal Bon es T h e R a d ius articulat es with th e Carpal Bon es ---- no t th e Ul n a at all ! no t th e Ul n a at all ! T WO DE GREE S OF FREE DOM: We can circumduct the wrist.T WO DE GREE S OF FREE DOM: We can circumduct the wrist.Much of flexion (especially) and extension actually occurs at theMuch of flexion (especially) and extension actually occurs at theI ntercarpal JointsI ntercarpal Joints between the two rows of Carpal Bones.between the two rows of Carpal Bones.Joint of K nuckles and F ingers : Joint of K nuckles and F ingers :
Carpometacarpal Joints:Carpometacarpal Joints: Joints between distal row of carpal bonesJoints between distal row of carpal bonesand metacarpals.and metacarpals.Metacarpophalangeal (M CP) Joints:Metacarpophalangeal (M CP) Joints: T he knuckles, between theT he knuckles, between themetacarpals and proximal phalanges.metacarpals and proximal phalanges.P roximal I nterphalangeal ( PIP) J oints:P roximal I nterphalangeal ( PIP) J oints: Between the proximal andBetween the proximal andmiddle phalanges.middle phalanges.
Distal I nterphalangeal (D IP) J oints:Distal I nterphalangeal (D IP) J oints: Between the middle andBetween the middle anddistal phalanges (not present in thumb).distal phalanges (not present in thumb).THUMBTHUMB ---- NOT A ST ABLE JOI NT compared to the other fingers. T heNOT A ST ABLE JOI NT compared to the other fingers. T hethumb has more mobility, too, to allow opposition.thumb has more mobility, too, to allow opposition.
-
8/8/2019 Shoulder and Pectoral
63/95
THE HANDTHE HAND
Movements of the F ingers : Movements of the F ingers : F lexion and E xtension of F ingers : Uses the fingernails as aF lexion and E xtension of F ingers : Uses the fingernails as afan.fan.
Abduction and Adduction of F ingers : Uses the fingernails to Abduction and Adduction of F ingers : Uses the fingernails toslice through the air, centered around the middle finger.slice through the air, centered around the middle finger.TH UMB: Same goes for thumbTH UMB: Same goes for thumb -- -- flexion, extension,flexion, extension,abduction, and adduction are based on the position of theabduction, and adduction are based on the position of thethumbthumb--nail.nail.C
ircumduction:C
ircumduction:T
he combination action of flexion,T
he combination action of flexion,extension, abduction, and adduction. Moving around in aextension, abduction, and adduction. Moving around in acircle, as you can do with your fingers, wrist, and shoulder.circle, as you can do with your fingers, wrist, and shoulder.
-
8/8/2019 Shoulder and Pectoral
64/95
Force T ransduction through theForce T ransduction through theH and and Arm : H and and Arm :
Weight Weight--bearing on the hand can be transmitted asbearing on the hand can be transmitted asfollows : follows :
SCAPH OI D SCAPH OI D ------------> R adioCarpal joints> R adioCarpal joints ------------> R ADI US> R ADI US ------------> I nterosseus Membrane> I nterosseus Membrane ------------> UL N A> ULN A ------------>>
OlecranonOlecranon ------------>H
UMER
US>H
UMER
US ------------> Glenohumeral Joint > Glenohumeral Joint ------------> SCAPULA> SCAPULA ------------> Coracoclavicular Ligaments> Coracoclavicular Ligaments ------------> CLA VI CLE > CLA VI CLE
Th e c lavicl e is t h e on ly bon y articulation Th e clavicl e is t h e only b ony articulation be tw ee n t h e upp e r lim b and trunk be tw ee n t h e upp e r lim b and trunk ..
Most common points of fracture in a fall : Most common points of fracture in a fall : T he surgical neck of the humerusT he surgical neck of the humerusT he middle of the clavicleT he middle of the clavicle
-
8/8/2019 Shoulder and Pectoral
65/95
Common Wrist Fractures : Common Wrist Fractures :
Colles Fracture:Colles Fracture: Fracture of the distalFracture of the distalradius.radius.Scaphoid FracturesScaphoid Fractures : Fracture of the: Fracture of thescaphoid bone.scaphoid bone.
-
8/8/2019 Shoulder and Pectoral
66/95
H and functionsH and functions
E xtrinsic Muscles of the H ands : MostlyE xtrinsic Muscles of the H ands : Mostlyconcerned with grip.concerned with grip.I ntrinsic Muscles of the H ands : ConcernedI ntrinsic Muscles of the H ands : Concernedwith manipulation of the digits. All of themwith manipulation of the digits. All of themare basically innervated by T 1.are basically innervated by T 1.P ALMAR AP ONEU ROSIS :P ALMAR AP ONEU ROSIS : Deep to theDeep to theskin and fascia. I t holds it down, so that theskin and fascia. I t holds it down, so that theskin on the palm is tight and hairless.skin on the palm is tight and hairless.
-
8/8/2019 Shoulder and Pectoral
67/95
-
8/8/2019 Shoulder and Pectoral
68/95
F I BR OUS FLE X OR SHE ATH SF I BR OUS FLE X OR SHE ATH S
Strong sheath covering the long tendonsStrong sheath covering the long tendonsgoing into the hand, distal to the flexorgoing into the hand, distal to the flexorretinaculum.retinaculum.T he fibrous sheaths of the fingers containT he fibrous sheaths of the fingers containtwo tendons : T he tendons of thetwo tendons : T he tendons of the F lexorF lexorDigitorum Su p erficialisDigitorum Su p erficialis and theand the F lexorF lexorDigitorum P rofundusDigitorum P rofundus. .T he fibrous sheath of the thumb containsT he fibrous sheath of the thumb containsone tendon : T heone tendon : T he F lexor P ollicis Longus.F lexor P ollicis Longus.
-
8/8/2019 Shoulder and Pectoral
69/95
S Y NO VI AL FLE X OR SHE ATH SS Y NO VI AL FLE X OR SHE ATH S
) : T he fibrous sheaths are enclosed in) : T he fibrous sheaths are enclosed insynovial sheaths in areas where there issynovial sheaths in areas where there isfriction. Primarily : friction. Primarily : Deep to the flexor retinaculum.Deep to the flexor retinaculum.Within the digits.Within the digits.T here are NO S Y NO VI AL SHE ATH S in theT here are NO S Y NO VI AL SHE ATH S in thecentral palm of the hand.central palm of the hand.
-
8/8/2019 Shoulder and Pectoral
70/95
BursaeBursae
R AD I AL BU RS A:R AD I AL BU RS A:Contains the Pollicis Longus tendon.Contains the Pollicis Longus tendon.Communicates with Ulnar Bursa in 50% of people.Communicates with Ulnar Bursa in 50% of people.ULNAR BURS A:ULNAR BURS A:Contains the F lexor Digitorum Superficialis andContains the F lexor Digitorum Superficialis andProfundus tendons.Profundus tendons.
Communicates with R adial Bursa in 50% of Communicates with R adial Bursa in 50% of people.people.
-
8/8/2019 Shoulder and Pectoral
71/95
CLI NIC ALCLI NIC AL
HO RS ESHOE I NFECTI ON:HO RS ESHOE I NFECTI ON: I nfection spreadingI nfection spreadingfrom little finger to thumb or vice versa, as afrom little finger to thumb or vice versa, as aconsequence of the communication between theconsequence of the communication between the
radial and ulnar bursae.radial and ulnar bursae.DOR SAL SUBCUT ANE OUS SPACE will receive lymphDOR SAL SUBCUT ANE OUS SPACE will receive lymph
from the palmar aspect of the hand. T hus a handfrom the palmar aspect of the hand. T hus a hand- -infection can easily result in swelling on posteriorinfection can easily result in swelling on posterioraspect of the hand, in which case it would beaspect of the hand, in which case it would belymphlymph ---- not pusnot pus ---- so don't incise it.so don't incise it.
-
8/8/2019 Shoulder and Pectoral
72/95
Arterial supply of hand Arterial supply of hand
SUP ERFICI AL P ALMAR ARCH:SUP ERFICI AL P ALMAR ARCH: MainMainarterial supply to the hand.arterial supply to the hand.Literally it is formed by a continuation of theLiterally it is formed by a continuation of theartery, and it anastomoses with theartery, and it anastomoses with theSuperficial Palmar Branch of the R adialSuperficial Palmar Branch of the R adial
Artery. Artery.I t gives off I t gives off Common P almar DigitalCommon P almar Digital
Arteries Arteries ------------> P roper P almar Digital> P roper P almar Digital Arteries Arteries
-
8/8/2019 Shoulder and Pectoral
73/95
Arterial supply of hand Arterial supply of hand
DEEP P ALMAR ARCH:DEEP P ALMAR ARCH: Lies deep to theLies deep to theflexor retinaculum.flexor retinaculum.T his is formed by the radial artery, and it T his is formed by the radial artery, and it anastomoses with the terminal ulnar artery.anastomoses with the terminal ulnar artery.I t gives off theI t gives off the P almar MetacarpalP almar Metacarpal
Arteries Arteries ------------> P roper P almar Digital> P roper P almar Digital Arteries Arteries
-
8/8/2019 Shoulder and Pectoral
74/95
Arterial supply of hand Arterial supply of hand
DORS AL C ARP AL ARCH:DORS AL C ARP AL ARCH: From the dorsalFrom the dorsalcarpal branches of the R adial and Ulnarcarpal branches of the R adial and Ulnararteries.arteries.I t gives off theI t gives off the Dorsal MetacarpalDorsal Metacarpal
Arteries Arteries ------------> Dorsal Digital Arteries> Dorsal Digital Arteries ..
-
8/8/2019 Shoulder and Pectoral
75/95
Other parts ..Other parts ..
THENA R SP ACE:THENA R SP ACE: T he area deep to the 1st T he area deep to the 1st lumbrical muscle and the 2st flexor tendon,lumbrical muscle and the 2st flexor tendon,in the palm of the hand.in the palm of the hand.
MI DP ALMAR SP ACE:MI DP ALMAR SP ACE: T he medial part of T he medial part of the deep palm of the hand, deep to the rest the deep palm of the hand, deep to the rest of the flexor tendons. I t is next to theof the flexor tendons. I t is next to theT henar Space.T henar Space.
A SE PT UM separates the T henar from A SE PT UM separates the T henar fromMidPalmar spaces.MidPalmar spaces.
CUTANE OUS I NNERV ATI ON OFCUTANE OUS I NNERV ATI ON OF
-
8/8/2019 Shoulder and Pectoral
76/95
CUT ANE OUS I NNERV ATI ON OF CUT ANE OUS I NNERV ATI ON OF H AND, FORE AR M, AR MH AND, FORE AR M, AR M
Axillary N: Axillary N: Shoulder and Deltoid regionsShoulder and Deltoid regions
Musculocutaneous N / Lateral Antebrachial Cutaneous N: Musculocutaneous N / Lateral Antebrachial Cutaneous N: Lateral forearm (both posterior and anterior)Lateral forearm (both posterior and anterior)
Medial Antebrachial Cutaneous N: Medial Antebrachial Cutaneous N: Medial Forearm (both posterior and anterior)Medial Forearm (both posterior and anterior)
R adial N: R adial N: Central posterior arm and forearmCentral posterior arm and forearmLateral 2/3 of posterior hand (up to middle of 4th digit or so)Lateral 2/3 of posterior hand (up to middle of 4th digit or so) -- -- E XCEPT the fingerE XCEPT the fingertips!! tips!! Lateral part of the thumbLateral part of the thumb
Median N: Median N: Lateral two thirds of anterior handLateral two thirds of anterior handF ingertips of lateral 2/3 of posterior handF ingertips of lateral 2/3 of posterior hand
Ulnar N: Ulnar N: Medial third of the hand, both anterior and posterior.Medial third of the hand, both anterior and posterior.
-
8/8/2019 Shoulder and Pectoral
77/95
LUMBRIC ALS :LUMBRIC ALS :T hey provide stability to the digits.T hey provide stability to the digits.T hey areT hey are a n terioran terior to the Metacarpophala n geal (MCP) joi n ts (k n uckles).to the Metacarpophala n geal (MCP) joi n ts (k n uckles).
So theySo they f l exf l ex the knuck l es.the knuck l es.T hey areT hey are p o st er i o rp o st er i o r t o t he p ro xi mal and d ist al i nt er p halangeal (P I P andt o t he p ro xi mal and d ist al i nt er p halangeal (P I P andDI P) jo i nts .DI P) jo i nts .
So theySo they extend
extend
thed
istal phalan
ges.thed
istal phalan
ges.T hey originate from the tendon of the flexor digitorum Profundus.T hey originate from the tendon of the flexor digitorum Profundus.FUNCTI ON OF LUMBRI CALS: T hey are rich inFUNCTI ON OF LUMBRI CALS: T hey are rich in neuromuscularneuromuscularspindle organsspindle organs , and they are thought to give you, and they are thought to give you proprioceptionproprioception(spatial orientation) and(spatial orientation) and kinesthesiakinesthesia (sense of motion) of the digits,(sense of motion) of the digits,due to the tension placed on them by the digital tendons.due to the tension placed on them by the digital tendons.In other words, they allow you to know where your finger is and where
In other words, they allow you to know where your finger is and whereit is going.it is going.
CLI NICAL ST UFF: F RACTURES ANDCLI NICAL ST UFF: F RACTURES AND
-
8/8/2019 Shoulder and Pectoral
78/95
CLI NIC AL ST UFF: F R ACTURES ANDCLI NIC AL ST UFF: F R ACTURES ANDENTR AP MENT NEUROP ATHI ESENTR AP MENT NEUROP ATHI ES
SPACE OF PAR ON A COMPRE SSI ON: Veins areSPACE OF PAR ON A COMPRE SSI ON: Veins aresubject to compression when swelling or fluidsubject to compression when swelling or fluidbuildup occurs in any potential space. T his causesbuildup occurs in any potential space. T his causesblood to backflow, which causes the followingblood to backflow, which causes the followingcourse of events.course of events.I schemiaI schemia ------------> Necrosis> Necrosis ------------> Fibrosis> FibrosisFASCI OTOM Y:FASCI OTOM Y: Cutting through the fascia whichCutting through the fascia whichis causing the compartment syndrome, therebyis causing the compartment syndrome, therebyrelieving the pressure and hopefully therelieving the pressure and hopefully thecompartment syndrome.compartment syndrome.
CLI NICAL ST UFF F RACTURES ANDCLI NICAL ST UFF F RACTURES AND
-
8/8/2019 Shoulder and Pectoral
79/95
CLI NIC AL ST UFF: F R ACTURES ANDCLI NIC AL ST UFF: F R ACTURES ANDENTR AP MENT NEUROP ATHI ESENTR AP MENT NEUROP ATHI ES
S ATURDA Y NI GHT SYNDROME:S ATURDA Y NI GHT SYNDROME: Drunk person fallingDrunk person fallingasleep on elbow and hence on ulnar nerve. Wake up theasleep on elbow and hence on ulnar nerve. Wake up thenext morning and the ulnar nerve is dead.next morning and the ulnar nerve is dead.COR ACOBR ACHI ALIS SYNDROME (N44 7) :COR ACOBR ACHI ALIS SYNDROME (N44 7) : Loss of theLoss of theMusculocutaneous NerveMusculocutaneous Nerve where it runs through thewhere it runs through theCoracobrachialis MuscleCoracobrachialis Muscle . I f the muscle dies, then nerve. I f the muscle dies, then nervedies with it.dies with it.Y OU ALSO LOSE: Y OU ALSO LOSE: Bic eps, Brachialis, a nd Lat eral Bic eps, Brachialis, a nd Lat eral
An t eb rachial Cuta n eo us Nerv e An t eb rachial Cuta n eo us Nerv e..LOST FUN C TI ON : LOST FUN C TI ON :
Lost flexion at elbow.Lost flexion at elbow.Weak supination due to supinator muscle.Weak supination due to supinator muscle.
Lost sensation over lateral aspect of forearm (cutaneousLost sensation over lateral aspect of forearm (cutaneousinnervation of medial antebrachial cutaneous N.)innervation of medial antebrachial cutaneous N.)
CLI NICAL ST UFF F RACTURES ANDCLI NICAL ST UFF F RACTURES AND
-
8/8/2019 Shoulder and Pectoral
80/95
CLI NIC AL ST UFF: F R ACTURES ANDCLI NIC AL ST UFF: F R ACTURES ANDENTR AP MENT NEUROP ATHI ESENTR AP MENT NEUROP ATHI ES
SUPI NATOR CHANNEL SYNDROME:SUPI NATOR CHANNEL SYNDROME:Compression of theCompression of the Deep Branch of the RadialDeep Branch of the RadialNerveNerve between thebetween the S u perfi c ial a nd Deep He a d s of S u perfi c ial a nd Deep He a d s of the S u pina tor , a nd the La ter al Epic on d yl e.the S u pina tor , a nd the La ter al Epic on d yl e.T his occurs right at theT his occurs right at the lateral epicondylelateral epicondyle ,,where the R adial Nerve gives off two brancheswhere the R adial Nerve gives off two branches(Deep and Superficial) to innervate the forearm.(Deep and Superficial) to innervate the forearm.
Arcade of Frohn: Arcade of Frohn: Occurs in 20%Occurs in 20%- -30% of 30% of population, where one head of the Supinator ispopulation, where one head of the Supinator isactually a sharp tendon inserting on the lateralactually a sharp tendon inserting on the lateralepicondyle. T his can also lead to R adial N.epicondyle. T his can also lead to R adial N.damage.damage.
CLI NICAL ST UFF F RACTURES ANDCLI NICAL ST UFF F RACTURES AND
-
8/8/2019 Shoulder and Pectoral
81/95
CLI NIC AL ST UFF: F R ACTURES ANDCLI NIC AL ST UFF: F R ACTURES ANDENTR AP MENT NEUROP ATHI ESENTR AP MENT NEUROP ATHI ES
SUPR ACOND YLAR SYNDROME:SUPR ACOND YLAR SYNDROME: E ntrapment of E ntrapment of thethe Median N.Median N. beneath thebeneath the Ligament ofLigament ofS truthersS truthers , , which connects thewhich connects the S u pracon d yl arS u pracon d yl arP rocessP rocess to theto the Me d ial E picon d yl e.Med ial E picon d yl e.T he Supracondylar Process is a bit of bone stickingT he Supracondylar Process is a bit of bone stickingout the medial aspect of the humerus. I t is onlyout the medial aspect of the humerus. I t is onlypresent in a small fraction of population.present in a small fraction of population.LOSS OF FUNCTI ON AND SE NSATI ON: AnywhereLOSS OF FUNCTI ON AND SE NSATI ON: Anywherethe median N. innervates.the median N. innervates.
Lateral 2/3 of palm of hand, lost cutaneous sensation.Lateral 2/3 of palm of hand, lost cutaneous sensation.Lose motor to the palmar thenar muscles.Lose motor to the palmar thenar muscles.Lose motor to the first two lumbricals.Lose motor to the first two lumbricals.
CLI NICAL ST UFF F RACTURES ANDCLI NICAL ST UFF F RACTURES AND
-
8/8/2019 Shoulder and Pectoral
82/95
CLI NIC AL ST UFF: F R ACTURES ANDCLI NIC AL ST UFF: F R ACTURES ANDENTR AP MENT NEUROP ATHI ESENTR AP MENT NEUROP ATHI ES
PR ONATOR TERES SYNDROME:PR ONATOR TERES SYNDROME: E ntrapment of E ntrapment of Median N.Median N. passing between the Deep andpassing between the Deep andSuperficial H eads of the Pronator T eres.Superficial H eads of the Pronator T eres.T
he Median N. also passes deep to theF
lexorT
he Median N. also passes deep to theF
lexorDigitorum Superficialis tendon, right after it getsDigitorum Superficialis tendon, right after it getspast the Pronator T eres. T his can also causepast the Pronator T eres. T his can also causetrouble.trouble.LOSS OF FUNCTI ON and S E NSATI ON: Again,LOSS OF FUNCTI ON and S E NSATI ON: Again,whatever would happen if you lose the Median N.whatever would happen if you lose the Median N.See above.See above.
CLI NICAL ST UFF F RACTURES ANDCLI NICAL ST UFF F RACTURES AND
-
8/8/2019 Shoulder and Pectoral
83/95
CLI NIC AL ST UFF: F R ACTURES ANDCLI NIC AL ST UFF: F R ACTURES ANDENTR AP MENT NEUROP ATHI ESENTR AP MENT NEUROP ATHI ES
MARTI NMARTI N--G RUBER ANAST OMO SIS :GRUBER ANAST OMO SIS :Connection between the Median and UlnarConnection between the Median and Ulnarnerves in the palm of the hand, in about nerves in the palm of the hand, in about 30% of population. When the connection is30% of population. When the connection isthere, it is mainly a motor connection.there, it is mainly a motor connection.R esult = people with Ulnar N. damage mayR esult = people with Ulnar N. damage may
still have cutaneous anesthesia, but theystill have cutaneous anesthesia, but theymay keep some motor function in the hand.may keep some motor function in the hand.
CLI NICAL ST UFF F RACTURES ANDCLI NICAL ST UFF F RACTURES AND
-
8/8/2019 Shoulder and Pectoral
84/95
CLI NIC AL ST UFF: F R ACTURES ANDCLI NIC AL ST UFF: F R ACTURES ANDENTR AP MENT NEUROP ATHI ESENTR AP MENT NEUROP ATHI ES
C ARP AL TUNNEL SYNDROME:C ARP AL TUNNEL SYNDROME: T heT he Me d ia n Nerv eMed ia n Nerv epa sses d eep to the flexo r r et i n a culum. I f i t i s e n t ra ppe d ,pa sses d eep to the flexo r r et i n a culum. I f i t i s e n t ra ppe d ,car pa l tu nn el sy nd r ome r esults.car pa l tu nn el sy nd r ome r esults.Car pus i s a ctu a lly UCar pus i s a ctu a lly U--Sh a pe d .Sha pe d .LOSS OF FUNCTI ON : LOSS OF FUNCTI ON :
Causes numbness and tingling in the lateral part of the handCauses numbness and tingling in the lateral part of the handsupplied by the median nerve.supplied by the median nerve.Weakening and wasting of the T henar muscles.Weakening and wasting of the T henar muscles.
TRE AT ME NT: Cut the flexor retinaculum and relieve theTRE AT ME NT: Cut the flexor retinaculum and relieve thepressure.pressure.Superficial P almar Branch of Median NSuperficial P almar Branch of Median N do es no t g o do es no t g o thr o ugh th e Carpal T u nn e l thr o ugh th e Carpal T u nn e l . I t r esults in a n ar ea o f s kin in . I t r esults in a n ar ea o f s kin in th e mi dd l e o f th e pal m that is no t a ffec t ed by Carp e l th e mi dd l e o f th e pal m that is no t a ffec t ed by Carp e l T u nn e l Synd r o me.T u nn e l Synd r o me.
CLI NICAL ST UFF F RACTURES ANDCLI NICAL ST UFF F RACTURES AND
-
8/8/2019 Shoulder and Pectoral
85/95
CLI NIC AL ST UFF: F R ACTURES ANDCLI NIC AL ST UFF: F R ACTURES ANDENTR AP MENT NEUROP ATHI ESENTR AP MENT NEUROP ATHI ES
CUBIT AL TUNNEL SYNDROME:CUBIT AL TUNNEL SYNDROME: Compression of Compression of thethe Ulnar NerveUlnar Nerve between the two heads of originbetween the two heads of originof theof the F l exor Carpi Ul narisF l exor Carpi Ul naris..
T heT he P isiform boneP isiform bone , distally, acts as a lever in, distally, acts as a lever inallow the flexor carpi ulnaris to flex the fingersallow the flexor carpi ulnaris to flex the fingersmore strongly.more strongly.LOSS OF FUNCTI ON: Medial two heads of theLOSS OF FUNCTI ON: Medial two heads of theflexor digitorum profundus and most of theflexor digitorum profundus and most of theintrinsic muscles of the hand.intrinsic muscles of the hand.
CLI NICAL ST UFF F RACTURES ANDCLI NICAL ST UFF F RACTURES AND
-
8/8/2019 Shoulder and Pectoral
86/95
CLI NIC AL ST UFF: F R ACTURES ANDCLI NIC AL ST UFF: F R ACTURES ANDENTR AP MENT NEUROP ATHI ESENTR AP MENT NEUROP ATHI ES
GU YON' S C ANAL SYNDROME :GU YON' S C ANAL SYNDROME : Compression of Compression of thethe Ulnar NerveUlnar Nerve inin G uy on's C a nal G uy on's C a nal , between the, between theVola r Ca rpal L iga ment Vola r Ca rpal L iga ment a nd thea nd the F l exor Retin aculu mF l exor Retin aculu m..
Volar Carpal Ligament: Volar Carpal Ligament: I s superficial to theI s superficial to theflexor retinaculum. T he ulnar artery and nerveflexor retinaculum. T he ulnar artery and nervepass superficial to the flexor retinaculum but deeppass superficial to the flexor retinaculum but deepto the volar carpal ligament.to the volar carpal ligament.CUB ITA L T U NNE L CUB ITA L T U NNE L --V S V S- - G UYON'S C A N A L :G UYON'S C A N A L : I nI nGuyon's C anal, only the intrinsic muscles of theGuyon's C anal, only the intrinsic muscles of thehand are lost, whereas in C ubital T unnelhand are lost, whereas in C ubital T unnelS yndrome you also lose the innervation of theS yndrome you also lose the innervation of themedial half of the flexor digitorum profundus.medial half of the flexor digitorum profundus.
CLI NICAL ST UFF F RACTURES ANDCLI NICAL ST UFF F RACTURES AND
-
8/8/2019 Shoulder and Pectoral
87/95
CLI NIC AL ST UFF: F R ACTURES ANDCLI NIC AL ST UFF: F R ACTURES ANDENTR AP MENT NEUROP ATHI ESENTR AP MENT NEUROP ATHI ES
DUPU YTREN' S CON TR ACTURE:DUPU YTREN' S CON TR ACTURE: Progressive shorteningProgressive shorteningof the palmar aponeuroses, from hypertrophy andof the palmar aponeuroses, from hypertrophy andhyperplasia. Unknown cause.hyperplasia. Unknown cause.Found esp. in those who have done a lot of manual labor.Found esp. in those who have done a lot of manual labor.
S Y MPT OM: T ends to bring the medial two fingers in towardS Y MPT OM: T ends to bring the medial two fingers in towardthe palm and flex them downward a bit.the palm and flex them downward a bit.LOSS OF FUNCTI ON: Blood vessels that reach the skinLOSS OF FUNCTI ON: Blood vessels that reach the skinthrough the palmar aponeurosis are compromised!!! through the palmar aponeurosis are compromised!!! TRE AT ME NT: I f caught early enough, incise theTRE AT ME NT: I f caught early enough, incise theaponeurosis.aponeurosis.
CLI NICAL ST UFF: F RACTURES ANDCLI NICAL ST UFF: F RACTURES AND
-
8/8/2019 Shoulder and Pectoral
88/95
CLI NIC AL ST UFF: F R ACTURES ANDCLI NIC AL ST UFF: F R ACTURES ANDENTR AP MENT NEUROP ATHI ESENTR AP MENT NEUROP ATHI ES
TENO SYNOVITIS :TENO SYNOVITIS : Not to be messed with.Not to be messed with.I nflammation of the tendons in the synovial joints,I nflammation of the tendons in the synovial joints,which can spread proximally all the way to thewhich can spread proximally all the way to theelbow.elbow.I NFE CTI ON CAN SPRE AD from theI NFE CTI ON CAN SPRE AD from the Ulnar BursaUlnar Bursa - -----------> Carpal Tunnel> Carpal Tunnel (with secondary carpal(with secondary carpaltunnel syndrome)tunnel syndrome) ------------> Space of P arona> Space of P arona ------------> Cubital Fossa> Cubital Fossa ..T enosynovitis in the index finger flexor tendon canT enosynovitis in the index finger flexor tendon canrupture and get into therupture and get into the Thenar SpaceThenar Space , causing a, causing acompartment syndrome there as well.compartment syndrome there as well.
CLI NICAL ST UFF: F RACTURES ANDCLI NICAL ST UFF: F RACTURES AND
-
8/8/2019 Shoulder and Pectoral
89/95
CLI NIC AL ST UFF: F R ACTURES ANDCLI NIC AL ST UFF: F R ACTURES ANDENTR AP MENT NEUROP ATHI ESENTR AP MENT NEUROP ATHI ES
DEQUE R VA I N' S DIS EASE:DEQUE R VA I N' S DIS EASE: A specific A specifictenosynovitis of the first extensor compartment,tenosynovitis of the first extensor compartment,which transmits the E xtensor Pollicis Longus andwhich transmits the E xtensor Pollicis Longus andBrevis.Brevis.Found in people who use their thumb a lot and areFound in people who use their thumb a lot and arenot used to it.not used to it.S Y MPT OM: Dull pain around wrist and lack of S Y MPT OM: Dull pain around wrist and lack of desire to move the fingers.desire to move the fingers.
Dequervain's test:Dequervain's test: Make a fist like a child withMake a fist like a child withthe thumb inside, and then ulnar deviate (adduct)the thumb inside, and then ulnar deviate (adduct)the wrist. I t hurts even without the disease! the wrist. I t hurts even without the disease!
CLI NICAL ST UFF: F RACTURES ANDCLI NICAL ST UFF: F RACTURES AND
-
8/8/2019 Shoulder and Pectoral
90/95
CLI NIC AL ST UFF: F R ACTURES ANDCLI NIC AL ST UFF: F R ACTURES ANDENTR AP MENT NEUROP ATHI ESENTR AP MENT NEUROP ATHI ES
SC AP HO I D F R ACTURE:SC AP HO I D F R ACTURE: I f the scaphoid isI f the scaphoid isfractured, there is potential for avascular necrosisfractured, there is potential for avascular necrosisin 1/3 of all people, because blood comes fromin 1/3 of all people, because blood comes fromonly one placeonly one place -- -- the distal end.the distal end.T his will result in demineralization of the ScaphoidT his will result in demineralization of the Scaphoidfrom lack of use, and it will appear dark on the X from lack of use, and it will appear dark on the X- -R ay as a result.R ay as a result.When the fracture occurs in theWhen the fracture occurs in the neckneck of theof theScaphoid, blood supply is cut off to the proximalScaphoid, blood supply is cut off to the proximalpart.part.
CLI NICAL ST UFF: F RACTURES ANDCLI NICAL ST UFF: F RACTURES AND
-
8/8/2019 Shoulder and Pectoral
91/95
CLI NIC AL ST UFF: F R ACTURES ANDCLI NIC AL ST UFF: F R ACTURES ANDENTR AP MENT NEUROP ATHI ESENTR AP MENT NEUROP ATHI ES
TRI GGER FI NGER :TRI GGER FI NGER : Swelling of the fibrousSwelling of the fibroussheaths going around the tendons, suchsheaths going around the tendons, suchthat, when the tendon is on one side of thethat, when the tendon is on one side of theswelling, such that the finger is flexed, it willswelling, such that the finger is flexed, it willstay that way and you can't extend it. T henstay that way and you can't extend it. T henyou can pull real hard to get the tendonyou can pull real hard to get the tendon
past the "bottleneck" to the other side of past the "bottleneck" to the other side of the swelling, such that the finger extends,the swelling, such that the finger extends,and then you can't flex it again! and then you can't flex it again!
CLI NICAL ST UFF: F RACTURES ANDCLI NICAL ST UFF: F RACTURES AND
-
8/8/2019 Shoulder and Pectoral
92/95
CLI NIC AL ST UFF: F R ACTURES ANDCLI NIC AL ST UFF: F R ACTURES ANDENTR AP MENT NEUROP ATHI ESENTR AP MENT NEUROP ATHI ES
R A YNAUD' S DIS EASE:R A YNAUD' S DIS EASE: Vascular problem Vascular problemof too high of sympathetic tone, which canof too high of sympathetic tone, which cancause complications in the hand.cause complications in the hand.
Spasmodic vasoconstriction at the wrist willSpasmodic vasoconstriction at the wrist willcause one or two fingers to becomecause one or two fingers to becomecyanotic and ischemic.cyanotic and ischemic. Y ou could cut the sympathetic nerves at the Y ou could cut the sympathetic nerves at theneck to try and treat it.neck to try and treat it.I t is a very serious disease.I t is a very serious disease.
CLI NICAL ST UFF: F RACTURES ANDCLI NICAL ST UFF: F RACTURES AND
-
8/8/2019 Shoulder and Pectoral
93/95
CLI NIC AL ST UFF: F R ACTURES ANDCLI NIC AL ST UFF: F R ACTURES ANDENTR AP MENT NEUROP ATHI ESENTR AP MENT NEUROP ATHI ES
VA RUS : VA RUS : A bone A bone--fracture that createsfracture that createsangulationangulation towar d the m id line of the bo d y towar d the m id line of the bo d y ..
VALGU S : VALGU S : A bone A bone--fracture that createsfracture that createsangulationangulation awa y from the m id line of theawa y from the m id line of thebo d y bo d y ..
CLI NICAL ST UFF: F RACTURES ANDCLI NICAL ST UFF: F RACTURES AND
-
8/8/2019 Shoulder and Pectoral
94/95
CLI NIC AL ST UFF: F R ACTURES ANDCLI NIC AL ST UFF: F R ACTURES ANDENTR AP MENT NEUROP ATHI ESENTR AP MENT NEUROP ATHI ES
TY PE S OF FR ACT URE S: TY PE S OF FR ACT URE S: T ransverseT ransverseObliqueObliqueSpiralSpiralLongitudinalLongitudinalSegmental Fracture:Segmental Fracture: Broken bone in two or more places,Broken bone in two or more places,creating pieces of bone between the fractures.creating pieces of bone between the fractures.Open FractureOpen Fracture ---- fracture within an exposed wound andfracture within an exposed wound and
hence vulnerable to infection.hence vulnerable to infection.Close FractureClose Fracture ---- not exposed by a wound and hence not not exposed by a wound and hence not susceptible to infection.susceptible to infection.
-
8/8/2019 Shoulder and Pectoral
95/95
I t s FREE to join.
http : //www.examville.com

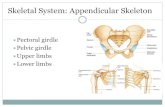

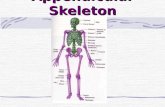

![[PPT]Appendicular Skeleton Pectoral Girdle and Upper … · Web viewAPPENDICULAR SKELETON PECTORAL GIRDLE AND UPPER LIMB PECTORAL GIRDLE scapula humerus clavicle CLAVICLE sternal](https://static.fdocuments.in/doc/165x107/5b1c49a87f8b9a2d258f98c3/pptappendicular-skeleton-pectoral-girdle-and-upper-web-viewappendicular-skeleton.jpg)