Short- and long-term outcome of balloon angioplasty for compromised side branches after...
4
Short- and Long-Term Outcome of Balloon Angioplasty for Compromised Side Branches After Intracoronary Stent Deployment Neeraj Prasad, MD, Humara Ali, MD, and Leonard Schwartz,*MD During coronary stent deployment there is a risk of compromising side branches, which can result in chest pain. Compromised side branches can be reopened by balloon angioplasty through the side of the stent. In a consecutive series of 10 patients with side-branch compromise and chest pain, balloon angioplasty through the side of the stent resolved the ischemia in all cases. The stented segment showed no deterioration following side-branch angioplasty. Six-month follow-up angiography showed a resteno- sis in the branch vessel of eight patients. The stented parent vessel restenosed in four patients. Therefore, side-branch balloon angioplasty after coronary stenting for ongoing ischemia is technically feasible and immediately effective. Restenosis of the branch occurs in most cases. Cathet. Cardiovasc. Intervent. 46:421–424, 1999. r 1999 Wiley-Liss, Inc. Key words: side-branch compromise; coronary stent INTRODUCTION Side branches are present in over 50% of coronary segments undergoing angioplasty and the majority of branches are medium sized [1]. During coronary stent deployment there is a risk of compromising such branches within the vicinity of the target lesion. Various definitions of branch compromise have been stated, i.e., occlusion of branch [2,3], progression in branch disease [4], TIMI flow deterioration [5], or a minimum change of 20% [6], but none includes the symptoms that may result within the definition. Chest pain can occur in 15% of medium- sized side-branch compromise patients [2–14]. Compro- mised side branches can be reopened by balloon angio- plasty through the side of the stent. This study describes the immediate and long-term results of this approach in a case series of 10 patients who were acutely ischemic following the initial stent deployment and side-branch compromise. MATERIALS AND METHODS This study was carried out at The Toronto Hospital (General Division), Toronto, Canada. All the angioplasty procedures and follow-up angiograms were performed by one staff operator. Each patient gave written informed consent for the initial procedure and the repeat follow-up angiogram. The study population consisted of 10 consecutive patients in whom side-branch occlusion or aggravation occurred immediately after stent deployment and was associated with ischemia. Prior to the angioplasty six patients had CCS class 4 angina, two had class 3, and two had class 2 symptoms. In eight of the cases the branch angioplasty was performed using an ACE balloon (Scimed, MN), which is a fixed wire catheter with a 1- or 2-cm steerable wire tip. In the other two cases, a monorail balloon system was used. The balloon was passed through the side of the stent into the branch ostia and inflated to reopen the compromised branch. The original angioplasty wire used for stent deployment of the main artery was left in place during the side-branch angioplasty for potential access but on no occasion did the side-branch treatment aggravate the main vessel, so no subsequent redilatation of the stent was performed. Repeat coronary angiography was carried out 6 months after the procedure to assess the angiographic results. The angiographic results were mea- sured by quantitative coronary angiographic (QCA) analy- sis (Cardiac Measurement System, Medical Imaging Systems, Nuenen, the Netherlands) for the vessel size of the parent vessel and the side branch as well as the percentage stenosis in the parent vessel. QCA analysis was difficult to perform at the ostia in the branch vessel due to the takeoff angulation of the branch. This segment Division Of Cardiology, The Toronto Hospital, Toronto, Canada *Correspondence to: Dr. Leonard Schwartz, 200 Elizabeth St, 13 en-204, Toronto M5G 2C4, Canada. Received 19 June 1998; Revision accepted 15 October 1998 Catheterization and Cardiovascular Interventions 46:421–424 (1999) r 1999 Wiley-Liss, Inc.
-
Upload
neeraj-prasad -
Category
Documents
-
view
213 -
download
1
Transcript of Short- and long-term outcome of balloon angioplasty for compromised side branches after...
Short- and Long-Term Outcome of Balloon Angioplastyfor Compromised Side Branches After Intracoronary
Stent Deployment
Neeraj Prasad, MD, Humara Ali, MD, and Leonard Schwartz, *MD
During coronary stent deployment there is a risk of compromising side branches, whichcan result in chest pain. Compromised side branches can be reopened by balloonangioplasty through the side of the stent. In a consecutive series of 10 patients withside-branch compromise and chest pain, balloon angioplasty through the side of the stentresolved the ischemia in all cases. The stented segment showed no deteriorationfollowing side-branch angioplasty. Six-month follow-up angiography showed a resteno-sis in the branch vessel of eight patients. The stented parent vessel restenosed in fourpatients. Therefore, side-branch balloon angioplasty after coronary stenting for ongoingischemia is technically feasible and immediately effective. Restenosis of the branchoccurs in most cases. Cathet. Cardiovasc. Intervent. 46:421–424, 1999.r 1999 Wiley-Liss, Inc.
Key words: side-branch compromise; coronary stent
INTRODUCTION
Side branches are present in over 50% of coronarysegments undergoing angioplasty and the majority ofbranches are medium sized [1]. During coronary stentdeployment there is a risk of compromising such brancheswithin the vicinity of the target lesion. Various definitionsof branch compromise have been stated, i.e., occlusion ofbranch [2,3], progression in branch disease [4], TIMIflow deterioration [5], or a minimum change of 20% [6],but none includes the symptoms that may result withinthe definition. Chest pain can occur in 15% of medium-sized side-branch compromise patients [2–14]. Compro-mised side branches can be reopened by balloon angio-plasty through the side of the stent. This study describesthe immediate and long-term results of this approach in acase series of 10 patients who were acutely ischemicfollowing the initial stent deployment and side-branchcompromise.
MATERIALS AND METHODS
This study was carried out at The Toronto Hospital(General Division), Toronto, Canada. All the angioplastyprocedures and follow-up angiograms were performed byone staff operator. Each patient gave written informedconsent for the initial procedure and the repeat follow-upangiogram.
The study population consisted of 10 consecutivepatients in whom side-branch occlusion or aggravationoccurred immediately after stent deployment and was
associated with ischemia. Prior to the angioplasty sixpatients had CCS class 4 angina, two had class 3, and twohad class 2 symptoms. In eight of the cases the branchangioplasty was performed using anACE balloon (Scimed,MN), which is a fixed wire catheter with a 1- or 2-cmsteerable wire tip. In the other two cases, a monorailballoon system was used. The balloon was passed throughthe side of the stent into the branch ostia and inflated toreopen the compromised branch. The original angioplastywire used for stent deployment of the main artery was leftin place during the side-branch angioplasty for potentialaccess but on no occasion did the side-branch treatmentaggravate the main vessel, so no subsequent redilatationof the stent was performed. Repeat coronary angiographywas carried out 6 months after the procedure to assess theangiographic results. The angiographic results were mea-sured by quantitative coronary angiographic (QCA) analy-sis (Cardiac Measurement System, Medical ImagingSystems, Nuenen, the Netherlands) for the vessel size ofthe parent vessel and the side branch as well as thepercentage stenosis in the parent vessel. QCA analysiswas difficult to perform at the ostia in the branch vesseldue to the takeoff angulation of the branch. This segment
Division Of Cardiology, The Toronto Hospital, Toronto, Canada
*Correspondence to: Dr. Leonard Schwartz, 200 Elizabeth St, 13en-204, Toronto M5G 2C4, Canada.
Received 19 June 1998; Revision accepted 15 October 1998
Catheterization and Cardiovascular Interventions 46:421–424 (1999)
r 1999 Wiley-Liss, Inc.
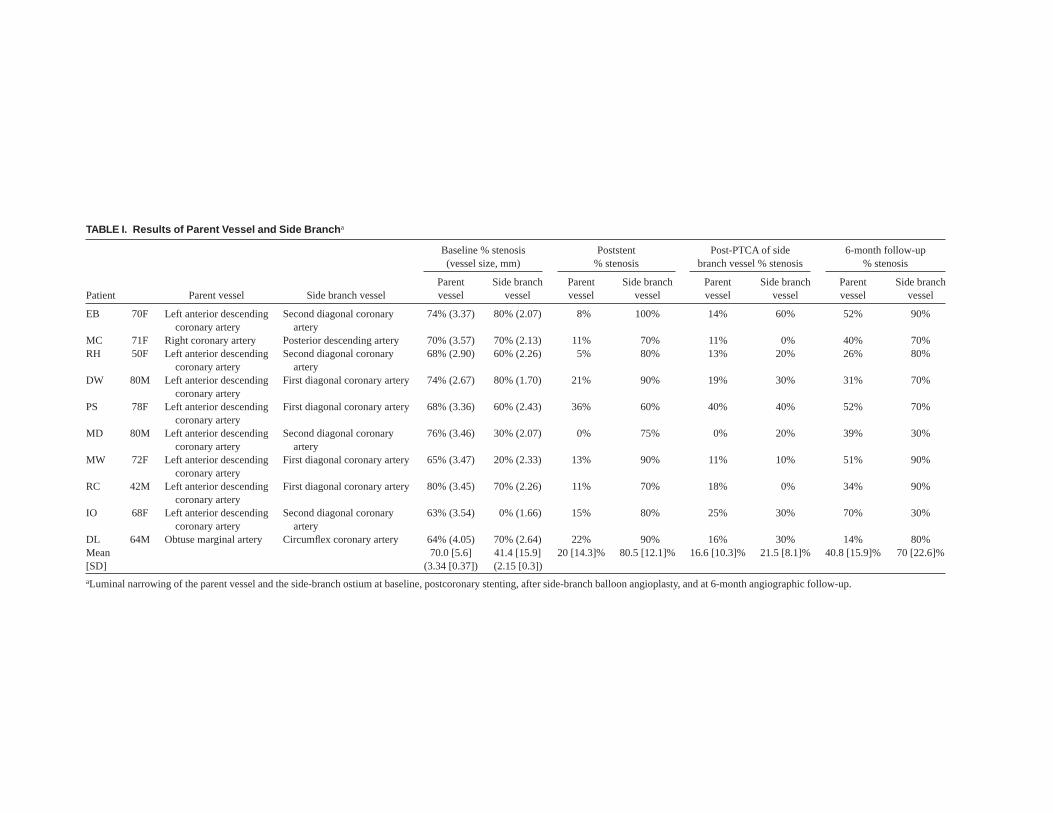
TABLE I. Results of Parent Vessel and Side Branch a
Patient Parent vessel Side branch vessel
Baseline % stenosis(vessel size, mm)
Poststent% stenosis
Post-PTCA of sidebranch vessel % stenosis
6-month follow-up% stenosis
Parentvessel
Side branchvessel
Parentvessel
Side branchvessel
Parentvessel
Side branchvessel
Parentvessel
Side branchvessel
EB 70F Left anterior descendingcoronary artery
Second diagonal coronaryartery
74% (3.37) 80% (2.07) 8% 100% 14% 60% 52% 90%
MC 71F Right coronary artery Posterior descending artery 70% (3.57) 70% (2.13) 11% 70% 11% 0% 40% 70%RH 50F Left anterior descending
coronary arterySecond diagonal coronary
artery68% (2.90) 60% (2.26) 5% 80% 13% 20% 26% 80%
DW 80M Left anterior descendingcoronary artery
First diagonal coronary artery 74% (2.67) 80% (1.70) 21% 90% 19% 30% 31% 70%
PS 78F Left anterior descendingcoronary artery
First diagonal coronary artery 68% (3.36) 60% (2.43) 36% 60% 40% 40% 52% 70%
MD 80M Left anterior descendingcoronary artery
Second diagonal coronaryartery
76% (3.46) 30% (2.07) 0% 75% 0% 20% 39% 30%
MW 72F Left anterior descendingcoronary artery
First diagonal coronary artery 65% (3.47) 20% (2.33) 13% 90% 11% 10% 51% 90%
RC 42M Left anterior descendingcoronary artery
First diagonal coronary artery 80% (3.45) 70% (2.26) 11% 70% 18% 0% 34% 90%
IO 68F Left anterior descendingcoronary artery
Second diagonal coronaryartery
63% (3.54) 0% (1.66) 15% 80% 25% 30% 70% 30%
DL 64M Obtuse marginal artery Circumflex coronary artery 64% (4.05) 70% (2.64) 22% 90% 16% 30% 14% 80%Mean 70.0 [5.6] 41.4 [15.9] 20 [14.3]% 80.5 [12.1]% 16.6 [10.3]% 21.5 [8.1]% 40.8 [15.9]% 70 [22.6]%[SD] (3.34 [0.37]) (2.15 [0.3])aLuminal narrowing of the parent vessel and the side-branch ostium at baseline, postcoronary stenting, after side-branch balloon angioplasty, and at 6-month angiographic follow-up.

was therefore assessed independently by two experiencedangiographers. Restenosis was categorized as luminalnarrowing of greater than 50%. Cardiac enzyme (creati-nine kinase) measurements were evaluated at baselineand 16 hr postprocedure.
RESULTS
In these 10 patients (6 female, 4 male), the parentvessel lesion was successfully stented (Johnson & JohnsonPalmatz-Schatz stents in 5 patients, Cook Gianturco-Rubin stents in 4 patients, and ACS Multilink stent in 1patient). The mean deployment pressure was 15.5 atm(range, 12–18 atm). Chest pain occurred in each patientafter stent deployment, which was ischemic in nature. Allpatients subsequently had successful side-branch balloonangioplasty. The mean balloon pressure of the side branchwas 8.1 atm (range, 6–10 atm), the diameter of theballoons used were 2 mm in four patients and 2.5 mm inthe remainder. The results of the procedure for both theparent vessel and the side branch are shown in Table I.The stented segment showed no deterioration followingside-branch angioplasty (parent vessel minimum luminaldiameter after stent deployment 2.91 mm, parent vesselminimum luminal diameter after side-branch angioplasty2.84 mm, P 5 NS). In eight patients there were noobserved cardiac enzyme elevation (for these patients,CK at baseline5 77.4 IU/L; range, 1–214; CK postproce-dure 5 88.8 IU/L; range, 34–192). One patient had amoderate CK rise from 190 to 521 IU/L. This patient hadhad successful opening of the LAD and first diagonalbranch. However, the second diagonal branch occludedduring the procedure but this branch was not reopened;thus, this may have contributed to the cardiac enzymeelevation. The other patient had a rise in CK from 120 to281 IU/L postprocedure.
All 10 patients had repeat coronary angiography andthese results are shown in Table I. Parent vessel restenosisoccurred in 4 out of 10 patients and side-branch restenosisoccurred in 8 out of 10 patients. Two patients had earlyrepeat angiography at 3 months for severe angina andboth were referred for coronary bypass surgery. Theothers were all symptomatically improved at 6-monthfollow-up with six class 1, one class 2, and one class 3;none of these patients required repeat intervention.
DISCUSSION
This case series shows that if side-branch compromiseoccurs immediately following stent deployment and isassociated with chest pain, it is possible to reopen thebranch by balloon angioplasty without compromising thestent result and with effective resolution of the ischemicsyndrome. Furthermore, this approach is associated with
a low incidence of cardiac enzyme elevation. However,the long-term angiographic results are poor, with almostinvariable branch restenosis. This may not be surprisingas ostial and small vessel balloon angioplasty are bothassociated with higher restenosis rate (ostial restenosis68%, small vessel restenosis 40% to 55%) [15–18].Recently, there has been some concern about ballooningthrough the side of a stent as this has been associated withdistal stent distortion [19]. We did not notice this; byQCA there was no change in parent vessel diameter afterside-branch angioplasty. Four of the 10 patients didrestenose the stent site in the parent vessel and this mayreflect an early structural change induced by the side-branch angioplasty, but in three of these four patients thestents were only minimally restenosed. A larger studywould be necessary to evaluate this issue.
In summary, side-branch balloon angioplasty aftercoronary stenting for ongoing ischemia is technicallyfeasible and immediately effective; it is also associatedwith a low incidence of cardiac enzyme elevation. From along-term standpoint, restenosis of the side-branch os-tium is almost invariable, suggesting that alternativeapproaches such as kissing balloon or ostial branchstenting before stenting the main artery should be ex-plored for this clinical situation.
ACKNOWLEDGMENTS
We thank Sanh Bui for his help with the QCA analysis.
REFERENCES
1. Lewis BE, Leya FS, Johnson SA, Grassman ED, Hwang M, LoebHS, Scanlon PJ, Euler D, Keeler G, McKiernan TL for theCAVEAT Investigator Group. Assessment of outcome of bifurca-tion lesions and non-bifurcation lesions treated in the CAVEATtrial. J Invas Cardiol 1995;7:251–258.
2. Meier B, Gruentzig AR, King SB, Douglas JS, Hollman J,Ischinger T, Aueron F, Galan K. Risk of side branch occlusionduring coronary angioplasty. Am J Cardiol 1984;53:10–14.
3. Aliabadi D, Tilli FV, Bowers TR, Benzuly KH, Safian RD,Goldstein JA, Grines CL, O’Neill WW. Incidence and angio-graphic predictors of side branch occlusion following high-pressure intracoronary stenting. Am J Cardiol 1997;80:994–997.
4. Vetrovec GW, Cowley MJ, Wolfgang TC, Ducey KC. Effects ofpercutaneous transluminal coronary angioplasty on lesion associ-ated branches. Am Heart J 1985;109:921–925.
5. Iniguez A, Macaya C, Alfonso F, Goicolea J, Hernandez R, ZarcoP. Early angiographic changes of side branches arising from aPalmaz-Schatz stented coronary segment: results and clinicalimplications. J Am Coll Cardiol 1994;23:911–915.6. AldermanEL, Stadius M. The angiographic definitions of the BypassAngioplasty Revascularisation Investigation. Coronary Artery Dis1992;3:1189–1207.
7. Boxt LM, Meyerovitz MF, Taus RH, Ganz P, Friedman PL, LevinDC. Side branch occlusion complicating percutaneous translumi-nal coronary angioplasty. Radiology 1986;161:681–683.
Side-Branch Angioplasty 423

8. Arora RR, Raymond RE, Dimas AP, Bhadwar K, Simpfendorfer C.Side branch occlusion during coronary angioplasty: incidence,angiographic characteristics, and outcome. Cathet CardiovascDiagn 1989;18:210–212.
9. Ciampricotti R, Gamal ME, vanGelder B, Bonnier J, Taverne R.Coronary angioplasty of bifurcational lesions without protection oflarge side branches. Cathet Cardiovasc Diagn 1992;27:191–196.
10. Zack PM, Ischinger T. Experience with a technique for coronaryangioplasty of bifuricational lesions. Cathet Cardiovasc Diagn1984;10:433–443.
11. Myler RK, Shaw RE, Stertzer SH, Hecht HS, Ryan C, RosenblumJ, Cumberland DC, Murphy MC, Hansell HN, Hidalgo B. Lesionmorphology and coronary angioplasty: current experience andanalysis. J Am Coll Cardiol 1992;19:1641–1652.
12. Fischman DL, Savage MP, Leon MB, Schatz RA, Ellis S, ClemanMW, Hirshfield JW, Teirstein P, Bailey S, Walker CM, Goldberg S.Fate of lesion related side branches after coronary artery stenting. JAm Coll Cardiol 1993;22:1641–1646.
13. Mazur W, Grinstead C, Hakim AH, Dabaghi SF, Abukhalil JM, AliNM, Joseph J, French BA, Raizner AE. Fate of side branches afterintra-coronary implantation of the Gianturco-Roubin flex-stent foracute or threatened closure after percutaneous transluminal coro-nary angioplasty. Am J Cardiol 1994;74:1207–1210.
14. Pan M, Medina A, Lezo JS, Romero M, Melian F, Pavlovic D,Hernandez E, Segura J, Marrero J, Torres F, Gimenez D, OrtegaJR. Follow-up patency of side branches covered by intracoronaryPalmaz-Schatz stent. Am Heart J 1995;129:436–440.
15. Savage MP, Fischman DL, Rake R, Leon MB, Schatz RA, Penn I,Nobuyoshi M, Moses J, Hirshfield J, Heuser R, Baim D, ClemanM, Brinker J, Gebhardt S, Goldberg S, for the STRESS Investiga-tors. Efficacy of coronary stenting versus balloon angioplasty incoronary arteries: results from STRESS. J Am Coll Cardiol1995;31:307–311.
16. Kawagishi N, Tsurumi Y, Ishii Y, Tanino S, Kawaguchi M,Magosaki N. Palmaz-Schatz stenting in ultra small coronaryarteries (,2.5). Circulation 1997;I274:1519.
17. Fernandez-Ortiz A, Vizcayno MP, Goicolea J, Alfonso F, BanuelosC, Hernandez R, Escaned J, Delgado A, Macaya C. Should westent small coronary vessels? comparison with balloon angio-plasty. Circulation 1997;I274:1521.
18. Mathias DW, Mooney JF, Lange HW, Goldenberg IF, Gobel FL,Mooney MR. Frequency of success and complications of coronaryangiography of a stenosis at the ostium of a branch vessel. Am JCardiol 1991;67:491–495.
19. Ormiston JA, Webster MWI, Ruygrok RN, Scott D, Stewart JT.Stent distortion during simulated side branch dilatation. J Am CollCardiol 1998;31:18A.
424 Prasad et al.