SHIP Priorities Committee...disease. ED affects up to 80% of all patients who have undergone pelvic...
23
SCWCSU/Clinical Effectiveness 02/2020 for SHIP consideration Page 1 of 23 SHIP Priorities Committee Policy update: Evaluation of treatments for erectile dysfunction (96a) 1. Introduction and overview of existing policy The SHIP Priorities Committee requested an update of policy recommendation 96a, Evaluation of treatments for erectile dysfunction (ED), which dates from July 2011 (Appendix 2). This review seeks to update the guidance and evidence for the clinical and cost effectiveness of vacuum erection devices (VEDs), penile implants and psychosexual interventions for the treatment of ED. The existing policy recommendation states that: Treatment with vacuum erection devices is LOW PRIORITY in view of limited evidence for effectiveness and cost effectiveness Treatment with penile implants is LOW PRIORITY in view of limited evidence for effectiveness and cost effectiveness and the high complication rate. Treatment with psychosexual interventions is LOW PRIORITY in view of limited evidence for effectiveness and cost effectiveness. An update on the regulations underpinning the medicines elements of the current policy, including provision of phosphodiesterase type 5 inhibitors and intracavernous/intraurethral injections has been completed by Medicines Optimisation and is included in Section 6. Penile implants are now commissioned by NHS England (see Section 3.1) Use of VEDs in the post-prostatectomy setting is excluded from this review; this indication is included in the separate SHIP penile rehabilitation policy (Appendix 3). 2. Background 2.1 Erectile dysfunction (ED) 1,2,3 ED is the inability to attain and maintain an erection that is sufficient for satisfactory sexual intercourse; this can affect physical and psychosocial health and have a significant impact on the quality of life of men and their partners. ED is a very common condition; the prevalence is estimated at 40% of the population of males over the age of 40. Causes include psychological, pharmaceutical (there is a wide range of medications which may cause ED) or physical; for example due to treatments for pelvic cancers (including urological and colorectal cancers), diabetes, or Peyronie's disease. ED affects up to 80% of all patients who have undergone pelvic cancer surgery. 2.2 Treatment of ED 4 The primary goal in the management of ED is to enable an individual or couple to enjoy a satisfactory sexual experience. Treatment of ED varies depending on the cause, and can include lifestyle changes 1 https://www.england.nhs.uk/commissioning/wp-content/uploads/sites/12/2016/08/clinical-com-pol-16059p.pdf 2 https://prostatecanceruk.org/media/2477451/treating-ed-after-surgery-for-pelvic-cancers.pdf 3 http://www.bssm.org.uk/wp-content/uploads/2018/09/BSSM-ED-guidelines-2018-1.pdf 4 http://www.bssm.org.uk/wp-content/uploads/2018/09/BSSM-ED-guidelines-2018-1.pdf
Transcript of SHIP Priorities Committee...disease. ED affects up to 80% of all patients who have undergone pelvic...
SCWCSU/Clinical Effectiveness 02/2020 for SHIP consideration Page 1 of 23
SHIP Priorities Committee
Policy update: Evaluation of treatments for erectile dysfunction (96a)
1. Introduction and overview of existing policy
The SHIP Priorities Committee requested an update of policy recommendation 96a, Evaluation of treatments for erectile dysfunction (ED), which dates from July 2011 (Appendix 2). This review seeks to update the guidance and evidence for the clinical and cost effectiveness of vacuum erection devices (VEDs), penile implants and psychosexual interventions for the treatment of ED. The existing policy recommendation states that:
Treatment with vacuum erection devices is LOW PRIORITY in view of limited evidence for effectiveness and cost effectiveness
Treatment with penile implants is LOW PRIORITY in view of limited evidence for effectiveness and cost effectiveness and the high complication rate.
Treatment with psychosexual interventions is LOW PRIORITY in view of limited evidence for effectiveness and cost effectiveness.
An update on the regulations underpinning the medicines elements of the current policy, including provision of phosphodiesterase type 5 inhibitors and intracavernous/intraurethral injections has been completed by Medicines Optimisation and is included in Section 6. Penile implants are now commissioned by NHS England (see Section 3.1) Use of VEDs in the post-prostatectomy setting is excluded from this review; this indication is included in the separate SHIP penile rehabilitation policy (Appendix 3).
2. Background
2.1 Erectile dysfunction (ED)1,2,3
ED is the inability to attain and maintain an erection that is sufficient for satisfactory sexual intercourse; this can affect physical and psychosocial health and have a significant impact on the quality of life of men and their partners. ED is a very common condition; the prevalence is estimated at 40% of the population of males over the age of 40. Causes include psychological, pharmaceutical (there is a wide range of medications which may cause ED) or physical; for example due to treatments for pelvic cancers (including urological and colorectal cancers), diabetes, or Peyronie's disease. ED affects up to 80% of all patients who have undergone pelvic cancer surgery. 2.2 Treatment of ED4 The primary goal in the management of ED is to enable an individual or couple to enjoy a satisfactory sexual experience. Treatment of ED varies depending on the cause, and can include lifestyle changes
1 https://www.england.nhs.uk/commissioning/wp-content/uploads/sites/12/2016/08/clinical-com-pol-16059p.pdf
2 https://prostatecanceruk.org/media/2477451/treating-ed-after-surgery-for-pelvic-cancers.pdf
3 http://www.bssm.org.uk/wp-content/uploads/2018/09/BSSM-ED-guidelines-2018-1.pdf
4 http://www.bssm.org.uk/wp-content/uploads/2018/09/BSSM-ED-guidelines-2018-1.pdf

SCWCSU/Clinical Effectiveness 02/2020 for SHIP consideration Page 2 of 23
to reduce the risk of cardiovascular disease, prescribing appropriate medication, treating an underlying health condition (such as heart disease or diabetes), psychological treatments such as cognitive behavioural therapy or sex therapy, or prescribing alternatives if a medication is causing ED. Addressing lifestyle and other possible causes of ED should precede or accompany any pharmacological treatment.
Psychosexual Intervention5: Psychosexual therapy may be indicated where the patient and or partner identify a significant psychological contribution to the problem or as perpetuating the problem. Psychotherapeutic methods may integrate cognitive, behavioural, systemic, psychodynamic, and interpersonal approaches.
Pharmaceutical Treatment: The currently available pharmaceutical therapies include: oral phosphodiesterase type 5 (PDE5) inhibitors, intra-urethral alprostadil (vasoactive agent) and intracavernous vasoactive drug injections.
Vacuum erection devices: VEDs are external, mechanical pumps which are used to help men with ED to get an erection. There are many types (both battery-operated and manually-operated). The erection is sustained with the placement of a constricting band across the base of the penis. The devices work by increasing arterial flow to the corpora cavernosa (erectile tissue) and by decreasing venous outflow once the constriction ring is applied. Once the band is removed, the penis can return to a flaccid state.
Patients may stop due to the inconvenience of using the device and a painful and cold-to-the-touch penis with use of the constriction ring.6 The device may also be challenging to use for patients with decreased dexterity or a large amount of lower abdominal fat and a buried penis7. The decrease in long term device use can lead to potential waste.
Vacuum devices are contraindicated in men with bleeding disorders or currently receiving anticoagulant therapy. Adverse events include pain, inability to ejaculate, petechiae (small circular patches of skin that look similar to a rash), bruising, coldness, and numbness8. Serious adverse events (skin necrosis) can be avoided if patients remove the constriction ring within 30 minutes.
NHS prescribing restrictions apply to vacuum pumps and constrictor rings for ED9. They can be prescribed on the NHS for treatment of ED only if the patient is a man who is suffering from any of the following: a) Diabetes, multiple sclerosis, Parkinson’s disease, poliomyelitis, prostate cancer, severe
pelvic injury, single gene neurological disease, spina bifida, spinal cord injury; or b) a man who is receiving treatment for renal failure by dialysis; or c) a man who has had the following surgery
prostatectomy radical pelvic surgery renal failure treated by transplant.
5 http://www.bssm.org.uk/wp-content/uploads/2018/09/BSSM-ED-guidelines-2018-1.pdf
6 Lee et al. (2018).Non-invasive management options for erectile dysfunction when a phosphodiesterase type 5 inhibitor
fails. https://link.springer.com/article/10.1007/s40266-018-0528-4 7 Krzastek et al. (2019) Recent advances in the understanding and management of erectile dysfunction.
https://doi.org/10.12688/f1000research.16576.1 8 http://www.bssm.org.uk/wp-content/uploads/2018/09/ED-Practical-Guide-v3-for-BSSM-review.pdf
9 http://www.drugtariff.nhsbsa.nhs.uk/#/00774110-DC/DC00773869#d2e92786/Part IXA-Appliances,
https://contactcentreservices.nhsbsa.nhs.uk/selfnhsukokb/AskUs_PS/en-gb/7834/sls/17254/information-on-the-selected-
list-scheme-sls

SCWCSU/Clinical Effectiveness 02/2020 for SHIP consideration Page 3 of 23
Penile Prosthesis10: Penile prosthesis implantation involves the surgical insertion of a rod or cylinder inside the penis. There are two types of penile prosthesis: malleable and inflatable. Inflatable prosthesis can also be antibiotic coated or non-antibiotic coated. Antibiotic coated implants can be pre-coated in antibiotic by the manufacturer or soaked in antibiotic intraoperatively, prior to implantation.
3. Relevant policies, guidance and audits
3.1 NHS England NHS England Clinical Commissioning Policy: Penile prosthesis surgery for end stage erectile dysfunction (2016) https://www.england.nhs.uk/commissioning/wp-content/uploads/sites/12/2016/08/clinical-com-pol-16059p.pdf
Routinely Commissioned - NHS England will routinely commission this specialised treatment in accordance with the criteria described in this policy. First line therapy: Some GPs will commence first-line oral medicinal therapies such as a PDE5 inhibitor (beyond scope of this review). Patients will be referred to a specialist urological team if lifestyle modifications and initial treatments are ineffective and at this stage be introduced to second-line therapies. If a hormonal condition is causing ED, patients are referred for hormonal treatment and investigation. Psychosexual counselling including sensate focus and cognitive behavioural therapy (CBT) will also be offered to patients with psychogenic causes of erectile dysfunction Second line therapy: Second line therapies include intracavernous and intraurethral vasoactive agents or external vacuum devices, which are contraindicated in men at risk of priapism (e.g. those with sickle cell anaemia) and those taking anticoagulant medication. End stage erectile dysfunction: If none of these treatments are effective at allowing penetrative intercourse, patients are considered to have end stage ED and will be referred for consideration of penile prosthesis in a tertiary urology centre. Primary penile prosthesis will be routinely commissioned for patients who have been assessed by the specialist andrology multi-disciplinary team (MDT) and fulfil all of the following criteria:
1. Males with end stage* ED of all aetiologies including; vasculogenic (including priapism), neurogenic, hormonal, anatomical (e.g. secondary to pelvic surgery, radiotherapy for cancer, or cases of buried penis), drug-induced, psychogenic or traumatic (e.g. Peyronie's disease and pelvic or spinal cord trauma).
2. Any males who fulfil criterion (1) and for whom lifestyle modifications, medicinal management, psychosexual counselling, intraurethral or intracavernous vasoactive agents (e.g. alprostadil), and external devices such as a vacuum pump have been ineffective.
3. Males who fulfil criteria (1) and (2) who have been appropriately risk-assessed by the specialist MDT with attention to diabetes, BMI and steroid use.
Exclusions:
1. Males with contraindications to penile prosthesis (including allergy to device components, or untreated lower urinary tract symptoms)
2. Males with risk of anaesthesia deemed too high. *End stage ED in the context of this guidance refers to ED that has not responded to treatment with pharmacotherapies including oral medications, intracavernous injections, intraurethral vasoactive agents as well as external vacuum devices. First and second line treatments for erectile dysfunction
10
https://www.england.nhs.uk/commissioning/wp-content/uploads/sites/12/2016/08/clinical-com-pol-16059p.pdf
SCWCSU/Clinical Effectiveness 02/2020 for SHIP consideration Page 4 of 23
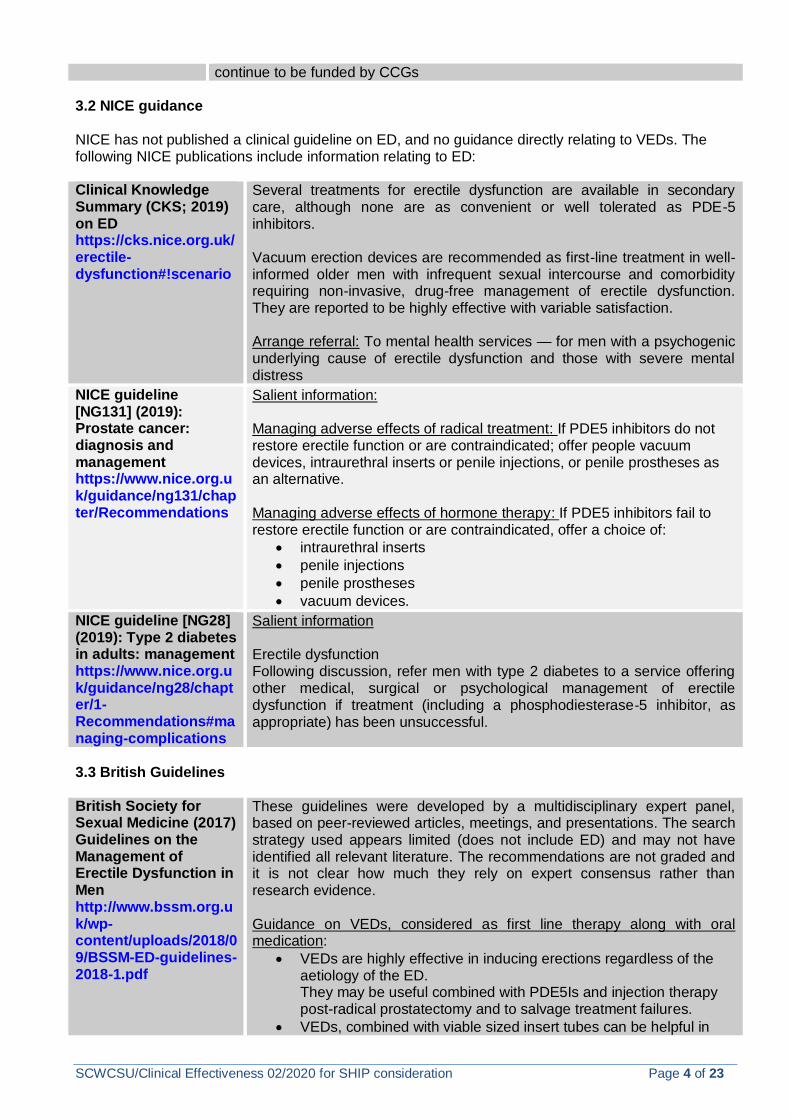
continue to be funded by CCGs 3.2 NICE guidance NICE has not published a clinical guideline on ED, and no guidance directly relating to VEDs. The following NICE publications include information relating to ED: Clinical Knowledge Summary (CKS; 2019) on ED https://cks.nice.org.uk/erectile-dysfunction#!scenario
Several treatments for erectile dysfunction are available in secondary care, although none are as convenient or well tolerated as PDE-5 inhibitors. Vacuum erection devices are recommended as first-line treatment in well-informed older men with infrequent sexual intercourse and comorbidity requiring non-invasive, drug-free management of erectile dysfunction. They are reported to be highly effective with variable satisfaction. Arrange referral: To mental health services — for men with a psychogenic underlying cause of erectile dysfunction and those with severe mental distress
NICE guideline [NG131] (2019): Prostate cancer: diagnosis and management https://www.nice.org.uk/guidance/ng131/chapter/Recommendations
Salient information: Managing adverse effects of radical treatment: If PDE5 inhibitors do not restore erectile function or are contraindicated; offer people vacuum devices, intraurethral inserts or penile injections, or penile prostheses as an alternative. Managing adverse effects of hormone therapy: If PDE5 inhibitors fail to restore erectile function or are contraindicated, offer a choice of:
intraurethral inserts
penile injections
penile prostheses
vacuum devices.
NICE guideline [NG28] (2019): Type 2 diabetes in adults: management https://www.nice.org.uk/guidance/ng28/chapter/1-Recommendations#managing-complications
Salient information Erectile dysfunction Following discussion, refer men with type 2 diabetes to a service offering other medical, surgical or psychological management of erectile dysfunction if treatment (including a phosphodiesterase‑5 inhibitor, as appropriate) has been unsuccessful.
3.3 British Guidelines British Society for Sexual Medicine (2017) Guidelines on the Management of Erectile Dysfunction in Men http://www.bssm.org.uk/wp-content/uploads/2018/09/BSSM-ED-guidelines-2018-1.pdf
These guidelines were developed by a multidisciplinary expert panel, based on peer-reviewed articles, meetings, and presentations. The search strategy used appears limited (does not include ED) and may not have identified all relevant literature. The recommendations are not graded and it is not clear how much they rely on expert consensus rather than research evidence. Guidance on VEDs, considered as first line therapy along with oral medication:
VEDs are highly effective in inducing erections regardless of the aetiology of the ED. They may be useful combined with PDE5Is and injection therapy post-radical prostatectomy and to salvage treatment failures.
VEDs, combined with viable sized insert tubes can be helpful in

SCWCSU/Clinical Effectiveness 02/2020 for SHIP consideration Page 5 of 23
correcting penile curvature.
Reported satisfaction rates vary considerably Long-term usage of VEDs also varies but is considerably higher than for self-injection therapy.
Most men who are satisfied with VEDs continue to use them long term.
Adverse effects include bruising, local pain, and failure to ejaculate. Partners sometimes report the penis feels cold.
Serious adverse events are very rare, but skin necrosis has been reported.
VEDs are contraindicated in men with bleeding disorders or those taking anti-coagulant therapy. They work best if the man and his partner have a positive attitude to them and sufficient time has been spent demonstrating their use. They can be prescribed under schedule 2 and represent a very cost-effective way of treating ED, even though initial costs are high. Psychosexual/Relationship Therapy Psychosexual therapy either alone or alongside the couple’s relationship therapy is indicated particularly where the patient and or partner identify significant psychological contribution to the problem or as perpetuating the problem. Psychotherapeutic methods integrating cognitive, behavioural, systemic, psychodynamic, and interpersonal approaches still lack adequate evidence based outcome studies, but literature suggests positive outcomes from a synthesis of these approaches.
3.4 International Guidelines European Association of Urology (2018) Male Sexual Dysfunction EAU guidelines https://uroweb.org/guideline/male-sexual-dysfunction/
The suggested management algorithm accompanying the guidance is included in Appendix 4. The guidelines appear to be in part based on a systematic but potentially limited search of the literature. They include chapters on ED, premature ejaculation, penile curvature, and peyonies disease. Only recommendations related to ED are reported here. For each recommendation within the guidelines there is an accompanying online strength rating form which addresses:
1. Overall quality of the evidence which exists for the recommendation (graded according to the Oxford Centre for Evidence-Based Medicine Levels of Evidence)
2. The magnitude of the effect (individual or combined effects) 3. The certainty of the results (precision, consistency, heterogeneity
and other statistical or study related factors) 4. The balance between desirable and undesirable outcomes. 5. The impact of patient values and preferences on the intervention. 6. The certainty of those patient values and preferences.
Guidance on VEDs: If drug treatment fails, then patients should be offered an alternative therapy such as intracavernous injection therapy or use of a VED. Vacuum erection devices VEDs provide passive engorgement of the corpora cavernosa, together with a constrictor ring placed at the base of the penis to retain blood within the corpora. Published data report that efficacy, in terms of erections satisfactory for intercourse, is as high as 90%, regardless of the cause of ED and satisfaction rates range between 27% and 94%.Most men who
SCWCSU/Clinical Effectiveness 02/2020 for SHIP consideration Page 6 of 23
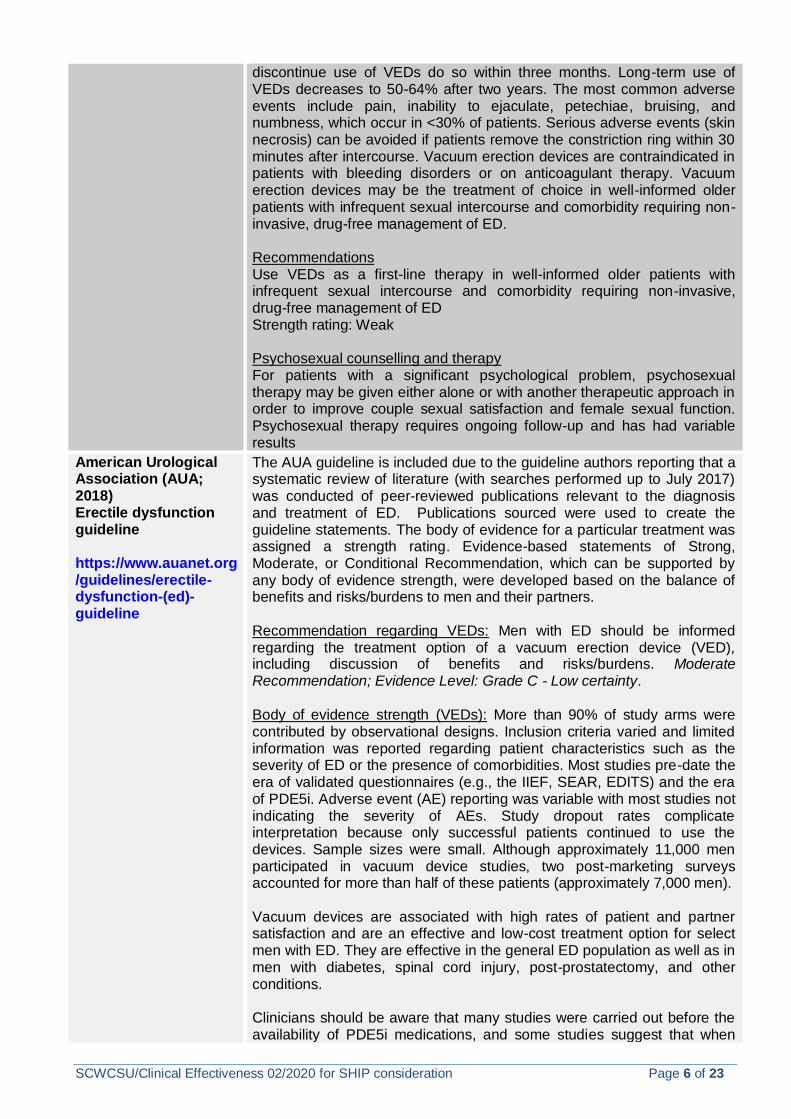
discontinue use of VEDs do so within three months. Long-term use of VEDs decreases to 50-64% after two years. The most common adverse events include pain, inability to ejaculate, petechiae, bruising, and numbness, which occur in <30% of patients. Serious adverse events (skin necrosis) can be avoided if patients remove the constriction ring within 30 minutes after intercourse. Vacuum erection devices are contraindicated in patients with bleeding disorders or on anticoagulant therapy. Vacuum erection devices may be the treatment of choice in well-informed older patients with infrequent sexual intercourse and comorbidity requiring non-invasive, drug-free management of ED. Recommendations Use VEDs as a first-line therapy in well-informed older patients with infrequent sexual intercourse and comorbidity requiring non-invasive, drug-free management of ED Strength rating: Weak Psychosexual counselling and therapy For patients with a significant psychological problem, psychosexual therapy may be given either alone or with another therapeutic approach in order to improve couple sexual satisfaction and female sexual function. Psychosexual therapy requires ongoing follow-up and has had variable results
American Urological Association (AUA; 2018) Erectile dysfunction guideline https://www.auanet.org/guidelines/erectile-dysfunction-(ed)-guideline
The AUA guideline is included due to the guideline authors reporting that a systematic review of literature (with searches performed up to July 2017) was conducted of peer-reviewed publications relevant to the diagnosis and treatment of ED. Publications sourced were used to create the guideline statements. The body of evidence for a particular treatment was assigned a strength rating. Evidence-based statements of Strong, Moderate, or Conditional Recommendation, which can be supported by any body of evidence strength, were developed based on the balance of benefits and risks/burdens to men and their partners. Recommendation regarding VEDs: Men with ED should be informed regarding the treatment option of a vacuum erection device (VED), including discussion of benefits and risks/burdens. Moderate Recommendation; Evidence Level: Grade C - Low certainty. Body of evidence strength (VEDs): More than 90% of study arms were contributed by observational designs. Inclusion criteria varied and limited information was reported regarding patient characteristics such as the severity of ED or the presence of comorbidities. Most studies pre-date the era of validated questionnaires (e.g., the IIEF, SEAR, EDITS) and the era of PDE5i. Adverse event (AE) reporting was variable with most studies not indicating the severity of AEs. Study dropout rates complicate interpretation because only successful patients continued to use the devices. Sample sizes were small. Although approximately 11,000 men participated in vacuum device studies, two post-marketing surveys accounted for more than half of these patients (approximately 7,000 men). Vacuum devices are associated with high rates of patient and partner satisfaction and are an effective and low-cost treatment option for select men with ED. They are effective in the general ED population as well as in men with diabetes, spinal cord injury, post-prostatectomy, and other conditions. Clinicians should be aware that many studies were carried out before the availability of PDE5i medications, and some studies suggest that when

SCWCSU/Clinical Effectiveness 02/2020 for SHIP consideration Page 7 of 23
men have a choice, more men prefer PDE5i. Of the 12 studies that reported patient satisfaction rates, six rates were 80% or higher and 11 studies reported rates of 60% or higher. Of the seven studies that reported partner satisfaction rates, all rates were above 70% except for one. In men who are PDE5i non-responders, VED may have a role as a “rescue” device. A study of 69 men who had failed PDE5i therapy and were subsequently treated with a combination of PDE5i and VED for 4 weeks demonstrated that this regimen may be effective in at least a subset of this cohort. For men being treated for ED, referral to a mental health professional should be considered to promote treatment adherence, reduce performance anxiety, and integrate treatments into a sexual relationship Moderate Recommendation; Evidence Level: Grade C

SCWCSU/Clinical Effectiveness 02/2020 for SHIP consideration Page 8 of 23
4. Evidence review Outcome measures in the literature include validated psychometric questionnaires, such as the International Index for Erectile Function (IIEF) or its short version the Sexual Health Inventory for Men (SHIM). These assess the different sexual function domains (i.e. sexual desire, erectile function, intercourse, and overall satisfaction), as well as the potential impact of a specific treatment modality11. 4.1 Vacuum Devices 4.1.1 Search Strategy A literature search was conducted to identify research on VEDs for ED from the past 10 years (2010 onwards). Databases searched included EMBASE, Medline, PubMed, Cochrane Library, and TRIP. Terms used for VEDs included: vacuum device, vacuum constriction device, VCD, vacuum erection assistance device, VED, penis pump, vacuum pump. As ED is linked to numerous comorbidities, searches were not limited in terms of population. However, studies related to the post-prostatectomy setting were screened out as this population was excluded from the review. Most literature published in the past decade related to the excluded post-prostatectomy setting. Very little robust research (such as systematic reviews [SRs] or randomised controlled trials [RCTs]) appears to have been published relating to VED use for ED as a result of other causes. 4.1.2 Systematic reviews
The search identified 2 SRs. Khera et al. (2011)12 considered evidence published up to 2009 which predates the current policy and is therefore not included here in depth. The authors concluded that devices are of unknown effectiveness for ED of any cause and the evidence was insufficient to judge the effects of this intervention. They did not identify any RCTs assessing the effectiveness of VEDs versus placebo. Vacuum devices were found to be associated with haematoma and blocked ejaculations. A more recent SR by Russo et al. (2018) considered all therapies for Peyronie’s disease, including VEDs. The SR authors only identified one uncontrolled case series study relating to VED’s; due to this and the patient cohort, this SR has not been critically appraised. The authors suggested that it is not possible to draw conclusions due to a lack of comparative randomised studies. Several other narrative reviews were identified but were not included due to the methodology being non-systematic. The VED studies discussed in these narrative reviews13,14,15were mostly conducted in the 1980s and 1990s; the authors noted that VEDs, unlike PDE5i medications, have not had to undergo
11
https://uroweb.org/guideline/male-sexual-dysfunction/#3_1 12
Khera and Goldstein (2011) Erectile dysfunction. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC3217797/ 13
Yuan et al. (2010) Vacuum therapy in erectile dysfunction—science and clinical evidence. https://www.ncbi.nlm.nih.gov/pubmed/20410903 14
Porst et al. (2013) SOP conservative (medical and mechanical) treatment of erectile dysfunction. https://onlinelibrary.wiley.com/doi/abs/10.1111/jsm.12023. 15
Brison et al. (2013) The resurgence of the vacuum erection device (VED) for treatment of erectile dysfunction. https://onlinelibrary.wiley.com/doi/abs/10.1111/jsm.12046
SCWCSU/Clinical Effectiveness 02/2020 for SHIP consideration Page 9 of 23
strict clinical trials to show their safety and efficacy before their widespread usage meaning that evidence consists largely of single-centre observational case series13. 4.1.3 Randomised controlled trials No RCTs comparing VEDs to an alternative intervention could be identified. One RCT involving two VED arms in a population with Type 2 diabetes was identified. This RCT (below) is also included in the AUA guideline authors’ SR.
Study
reference/aim,
objective of the
study and study
setting
Sun et al (2014) Combined sildenafil with vacuum erection device therapy in the management of diabetic men with erectile
dysfunction after failure of first-line sildenafil monotherapy https://onlinelibrary.wiley.com/doi/epdf/10.1111/iju.12564
To evaluate the efficacy and safety of combination therapy of sildenafil plus vacuum erection devices in men with type 2 diabetes
mellitus (DM) with moderate to severe erectile dysfunction who are dissatisfied with the results of using sildenafil alone
Study Design RCT of 66 men with type 2 DM comparing VED (n=30) with sildenafil plus VED (n=30)
Population
characteristics
Inclusions:
Clinically diagnosed with type 2 DM together with ED
Diagnosis of ED using a standardized questionnaire (IIEF- 5)
Moderate (score 11–16) to severe ED (score 10 points or less)
Acceptable metabolic control, glycosylated haemoglobin levels ranged
between 6∼8%
Non-responders after 4-6 unsuccessful attempts using a maximum dose of 100 mg sildenafil citrate over at least a 3-month
period.
Exclusions:
Peyronie’s disease, penile curvature
History of penile surgery
Radical prostatectomy
Severe renal or hepatic abnormalities
Congestive heart failure
Low testosterone levels
Alcohol/drugs abuse
Receiving nitrates, anti-androgens, α-blockers
Major psychiatric disorders

SCWCSU/Clinical Effectiveness 02/2020 for SHIP consideration Page 10 of 23
Haematological disorders
Intervention and
comparison
Intervention: VED device with constrictor ring. Instructed by personal tutoring and watching an instructional video. [Once the desired
state of erection was achieved, the erect state was maintained for 1–2 min, released and then pumped again; this was practiced for
at least 30 min every day, and the patients used a constriction ring during coitus].
Comparison (Combined Therapy): VED combined with sildenafil therapy (100 mg daily 1 h before sexual activity or 2 h after a meal).
Same course of VED as intervention group.
Outcome/Outco
me measures
IIEF-5 questionnaire
SEP questionnaire
Data were collected at visit 1 (baseline; study entry), visit 2 (4 weeks after baseline) and visit 3 (12 weeks after baseline; study end),
during each follow-up visit at the urological office.
Results / clinical
significance
Scores were significantly higher for the sildenafil plus VED group than for the VED group alone (14.86 ± 2.17 vs 12.41 ± 2.63;
P < 0.0001) and (17.53 ± 2.95 vs 14.29 ± 2.81; P < 0.0001).
Men in the combined group had better successful penetration (43.7% vs 30% and 73.3% vs 46.6%) successful intercourse
(43.3% vs 26.6% and 70% vs 46.6%) at the 1-month and 3-months visits compared with the VED group.
Combination therapy significantly improved erectile function compared with the VED group, as assessed by each of the three
primary efficacy variables (mean IIEF-5 score, SEP-2 successful penetration, SEP-3 successful intercourse)
Adverse side-effects of sildenafil; flushing (n=6) nausea (n=5) and headache (n=5).
Adverse side-effects of VED; penile bruising (n=6) and numbness (n=5). No adverse events associated with the use of
tension rings during the trial.
Adverse events were mostly mild, and did not affect the patients’ daily life; none of the patients withdrew from the study as a
result of side-effects
Author’s conclusions: The study authors suggested that combination therapy could be effectively used for some sildenafil non-
responders, and could be considered before initiating more invasive alternatives. The authors highlight severe, inconvertible
neuropathy, endothelial dysfunction and progression of penile atherosclerosis as a possible explanation as to why some patients
responded poorly to combination therapy.
Critical
Appraisal
Summary
Method: Reasonably well reported RCT in relation to CONSORT. No sample size calculation. Risk of bias:
Unable to blind participants due to nature of device.
Block randomisation (computer generated)
Equal LTFU from both groups (3).
Blinding of assessor is unclear Limitations
Authors highlight the inability to establish actual frequency of VED use or dose of sildenafil. Generalisability / applicability:
SCWCSU/Clinical Effectiveness 02/2020 for SHIP consideration Page 11 of 23
4.2 Psychosexual Interventions The following terms were used to search Medline and PsychInfo for SRs and RCTs relating to psychological interventions and published subsequent to the SHIP policy: Psychosexual OR Psycho* OR CBT OR cognitive OR counsel*. One SR was found relating to of psychosocial interventions for male sexual dysfunction:
This study was concerned only with men with type 2 DM who had experienced PDE5i monotherapy failure.
This study only included men with a ‘steady female partner’. This was for consistency with completing efficacy questionnaires. Sponsorship: None declared.
Study reference /
objective
Berner et al (2012) Efficacy of psychosocial interventions in men and women with sexual dysfunctions--a systematic
review of controlled clinical trials: part 1-the efficacy of psychosocial interventions for male sexual dysfunction
https://onlinelibrary.wiley.com/doi/pdf/10.1111/j.1743-6109.2012.02970.x
To review the efficacy of psychosocial interventions in all male sexual dysfunctions
Study Design SR of 19 RCTs and 1 controlled clinical trial (CCT)
In relation to ED: 13 studies (12 RCTs and 1 CCT). Results for premature ejaculation not reported here.
Population
characteristics
Formal diagnosis of a sexual dysfunction (International Statistical Classification of Diseases and Related Health Problems,
Diagnostic and Statistical Manual of Mental Disorders). Trails with concomitant somatic or mental disease were included if the
disorder did not cause sexual dysfunction.
Intervention and
comparison
Intervention: Psychosocial or psychotherapeutic:
Psychoeducational
Individual psychotherapy
Couple therapy
Group therapy with different approaches (cognitive behavioural, systemic, dynamic)
Biofeedback
Hypnosis
Comparison: Other treatment, placebo or a waiting‑list control group

SCWCSU/Clinical Effectiveness 02/2020 for SHIP consideration Page 12 of 23
Outcome/Outcome
measures
Frequency of and satisfaction with sexual activity, sexual functioning (e.g. Sexual desire, erectile functioning, ejaculation
latency)
Self-assessment of efficacy of treatment
Satisfaction with treatment
Aspects correlating with sexual dysfunction (QoL and partnership, depressiveness).
Measures depended on study and included:
Psychometrically validated scales
Diary notes to interviewers
Clinical assessments by and independent rater
Adverse events / dropout rates
Results / clinical
significance
Due to heterogeneity, pooling of the results was not possible. LTFU = loss to follow up. 13 studies investigated psychosocial
interventions in men with ED. Duration varied between one time psychoeducational workshop and 6 month Psychotherapy.
2 RCTs compared 3 groups; sildenafil, psychosocial intervention and a combination of both. 1 (n=117) study found that 3
months combined treatment or sildenafil was more effective than counselling alone in men with psychogenic or mixed ED
(measures included the sexual health inventory for men and the male sexual quotient); 1 study (n=30 LTFU = 8) concluded
that ED improved significantly at 6 months after psychosocial treatment or combined treatment but not after sildenafil alone
for men with psychogenic ED.
1 RCT (n=57, 11 LTFU) compared a stepped treatment programme (sildenafil followed by CBT after failure of sildenafil
alone) with combined treatment at the start of the study for men with predominantly psychogenic ED. Both conditions were
similarly effective.
1 RCT (83 couples, 28 LTFU) compared sildenafil alone with sildenafil and a psychoeducational workshop; the addition of
the workshop did not substantially improve ED compared to sildenafil alone (although treatment satisfaction was higher).
1 RCT (n=44 couples, 13 LTFU) compared a 10 week internet CBT with wait list control and found that the internet group
was superior in relation to ED.
2 RCTs combined psychosocial intervention with injection therapy. 1 study (n=50, LTFU =21) found that after 3 months of
sex therapy, 82% of men reported they were able to achieve an erection in sexual situations compared to 63% with
injection alone however p>0.05. 1 study (n=70, LTFU = 13) of men who received injection therapy alone vs. injection
therapy and sexual counselling found no significant differences.
1 RCT (n=69 LTFU = 9) compared 3 groups; psychosocial intervention, 30mg yohimbine, placebo. There was a significant
difference between psychosocial (40% - 35% improved ED), yohimbine (20% - 45%) and placebo (15%-30%) using the
cologne questionnaire of erectile dysfunction.
1 RCT compared 6 months hypnosis with testosterone or trazadone for men with no organic cause of ED. At 4 weeks,
60% of men considered themselves cured (hypnosis) compared to 40% in the pharmacology groups.

SCWCSU/Clinical Effectiveness 02/2020 for SHIP consideration Page 13 of 23
4.3 Evidence/evaluation of cost effectiveness
No robust cost effectiveness research focusing on VEDs was identified. An abstract (full text not available) of a 2019 review of economic evaluation of ED therapies suggested that minimal research has been conducted to assess the cost-effectiveness of VEDs in men with ED, and that substantial research is needed to evaluate the cost-effectiveness of ED treatments across different patient populations, countries, and reimbursement systems.16
16
Rezaee et al. (2019) Review of Economic Evaluations of Erectile Dysfunction Therapies. https://www.sciencedirect.com/science/article/abs/pii/S2050052119300587?via%3Dihub
1 RCT (n=60, LTFU = 0) found no significant differences between 6 month hypnosis, acupuncture, and controls (oral
placebo, placebo needle puncture) for men with no organic cause of ED.
1 RCT (n=45) compared relationship/ sex therapy and VED with relationship/ sex therapy alone. Both treatments led to
improvements.
1 CCT (n=70, LTFU =13) compared a 6 month psychodynamic therapy with psychodynamic therapy and virtual reality. Half
of men reported improvement in ED in the combined group compared to quarter in the psychodynamic only group.
1 RCT (21 couples, LTFU =1) reviewed three treatments (communication training for couples, sex therapy [Masters and
Johnson] or combined. The controls were attention placebo or wait list control. No significant differences were found in
between the treatment groups or attention placebo.
Author’s conclusions: Overall psychosexual interventions in men with ED are successful. Whether they are more successful than
pharmacology is still unclear.
Critical Appraisal
Summary
Method: Well reported SR in relation to PRISMA. Risk of bias: General quality score used (it is unclear if this is the authors own scale). Sequence generation, allocation concealment, implementation of allocation sequence, blinding of assessors, incomplete outcome data, selective reporting and allegiance were assessed as +ve (2 points) or –ve (0 points). 1 point was assigned if information was missing; the authors note that this was a liberal approach. Maximum points =16, good methodology =12. 18/20 studies scored <12. 2/20 studies scored 12. Wait list controls may be subject to bias. Limitations:
High LTFU in several studies
Low methodological quality of studies
Small sample sizes in the majority of the studies
The authors highlight that ½ of included trials only included men and not partners.
Psychosexual interventions are not well described Sponsorship None stated.

SCWCSU/Clinical Effectiveness 02/2020 for SHIP consideration Page 14 of 23
5. Local data and financial impact
Prescribing data for all SHIP CCGs for vacuum pumps and constrictor rings was obtained for the one year period between December 2018 and November 2019. Note that this data includes all indications, and therefore it is unclear which costs are associated with the ED indications covered within this review. Spend across all CCGs was:
Pump costs: £63,785.18 (382 patients / note that overlap is possible)
Ring costs: £9,328.27 (172 patients / note that overlap is possible)
Total annual costs: £73,113.45 Total costs per CCGs are noted below (includes both pumps and rings):
CCG Cost
Fareham and Gosport £9,102
Isle of Wight £1,331
North East Hampshire and Farnham £3,021
North Hampshire £6,910
Portsmouth £8,597
South Eastern Hampshire £9,222
Southampton £8,813
West Hampshire £26,112
Total £73,113
Spend and patient numbers per pump device type for each CCG is available in Appendix 5. Device prices are also reported in the NHS Drug Tariff17.
6. Medicines (Completed by Interface Pharmacist – see Appendix 1) 6.1 Background
Much of the evidence around the use of medicines for ED has been considered nationally and has been pivotal to any changes in the regulations for prescribing. The information below has been updated with any changes to regulations on the assumption that the evidence for efficacy and safety has already been addressed. Prescribing is governed by the information in Health Service Circulars 1999/14818 and 1999/177. 6.2 Oral treatment
Oral treatment with Phosphodiesterase type-5 inhibitors is recommended in the following situations: First line Sildenafil in a single dose of 25mg to 100mg.
Prescribing is no longer restricted to the patient groups identified in HSC 1999/148 and can be prescribed for any patient where a clinical need is identified.19 Second line Tadalafil in a single dose of 10mg or 20mg for men in patient groups identified by HSC 1999/148.
Daily doses of tadalafil (2.5mg or 5mg) are not recommended for prescribing in primary care20. Vardenafil and avanafil are both high cost options and are not recommended for first or second line treatment.
17
http://www.drugtariff.nhsbsa.nhs.uk 18
Health Service Circular SC 1999/148 (June 1999) 19
Statutory Instrument 2014, No:1625 20
Items which should not routinely be prescribed in primary care: Guidance for CCGs Version 2, June 2019

SCWCSU/Clinical Effectiveness 02/2020 for SHIP consideration Page 15 of 23
The Department of Health advises doctors that one treatment a week will be appropriate for most patients treated for erectile dysfunction. If the GP in exercising his or her clinical judgement considers that more than one treatment a week is appropriate he or she should prescribe that amount on the NHS.1 6.3 Intracavernosal injections and intraurethral instillations
Intracavernosal injections and intraurethral instillations are recommended where oral phosphodiesterase type-5 inhibitors are contraindicated or ineffective.1 Treatment should be initiated in secondary care. First line Alprostadil in a single injection of 10 to 40 microgram for men in patient groups identified by HSC 1999/148
Second line Phentolamine plus aviptadil in a single injection of 2mg plus 25microgram may be an option for
some patients where treatment with intracavernosal alprostadil is not tolerated. Prescribing is not restricted to the patient groups identified in HSC 1999/148 The Department of Health advises doctors that one treatment a week will be appropriate for most patients treated for erectile dysfunction. If the GP in exercising his or her clinical judgement considers that more than one treatment a week is appropriate he or she should prescribe that amount on the NHS.1
7. Public Sector Equality Duty and equity issues
ED is more prevalent among older men
Men undergoing treatment for pelvic cancers and those with certain conditions such as MS or cardiovascular diseases (see background section) are considered more likely to have ED.
8. Summary
This review examined the evidence for VEDs and psychosexual interventions in order to update the current SHIP policy recommendation dating from 2011. Penile implants for end stage ED are now commissioned by NHS England. NHS prescribing restrictions apply to both vacuum pumps and constrictor rings for ED; they can only be prescribed for men with the listed health conditions. Data:
Within the SHIP CCGs, vacuum pump prescribing costs over one year (up to November 2019) amounted to £63,785, and associated constrictor ring prescribing costs totalled £9,328. This data includes all indications; it is unclear what costs are related solely to the causes of ED covered within this review. Guidance:
VEDs: There is no specific NICE Guidance for ED; however NICE Clinical Knowledge Summary for ED (2019) and NICE Clinical Guideline for Prostate Cancer (2019) reference the use of VEDs as an option. The British Society for Sexual Medicine [BSSM] (2017), European Association of Urology (2018) and American Urological Association (AUA) (2018) guidelines support the use of VEDs as a suitable option for some men despite weak evidence. The American guideline authors noted that most VED studies were conducted prior to the availability of oral medication.
4 Notes from Portsmouth Area Prescribing Committee, the Isle of Wight Primary Care Prescribing Committee and
Basingstoke, Southampton and Winchester District Prescribing Committee

SCWCSU/Clinical Effectiveness 02/2020 for SHIP consideration Page 16 of 23
Psychosexual Interventions: The BBSM guidance recommends that psychosexual therapy either alone or alongside the couple’s relationship therapy is indicated particularly where the patient and/or partner identify a significant psychological contribution to the problem. NHS England (2016) commissioning guide states that within first line treatment, psychosexual counselling including sensate focus and CBT will also be offered to patients with psychogenic causes of ED. Medicines: An update of the prescribing regulations has been undertaken; no evidence review has been undertaken for the medicines elements of the current policy (See Section 6). Evidence:
This review found no robust (high quality) evidence for the use of VEDs in ED for indications within the review scope. No recent SRs or RCTs comparing the effectiveness of VEDs to other interventions could be identified. One RCT with 2 VED arms (VED vs VED + sildenafil) suggests that combination therapy is more effective than VED alone in men with type 2 DM. Overall, there is weak evidence suggesting that VED devices may be useful for some patients with ED. One SR relating to psychosocial therapies was found which concluded that these interventions can be effective (and that the nature of the psychosexual intervention did not appear to alter findings) in men with psychogenic ED. Included studies were generally of low methodological quality and often compared psychosexual interventions in combination with pharmacology vs psychosexual interventions alone. Cost-effectiveness:
Rezaee et al. (2019) review found that economic evaluations of ED therapies (including VEDs) are dated, do not reflect present-day physician, pharmaceutical, and device costs, fail to account for patient comorbidities, and may not be generalisable to today’s ED patients. The full text of this article was not available and therefore no critical analysis has been undertaken. Some literature suggests that a high number of patients stop using VEDs after a short time.
9. Options for consideration
The following options might be considered for recommendation: Option 1: Update existing policy as follows:
Maintain ‘not normally funded’ position for VED in light of paucity of evidence for clinical and cost effectiveness OR consider funding VEDs within NHS prescription recommendations AND
Amalgamate statement for VED with updated medicines information.
Remove outdated ’not normally funded’ statement from policy for penile implants and consider including a statement that NHS England commissions these for end stage ED
Maintain ‘not normally funded’ position for psychosexual interventions in light of limited evidence for clinical and cost effectiveness
Option 2: Consider discontinuation of VED / penile implant elements of policy in light of NHS prescribing guidance and NHSE commissioning statement.
For further discussion at the Committee re. medicines elements of policy.

SCWCSU/Clinical Effectiveness 02/2020 for SHIP consideration Page 17 of 23
Appendix 1: Feedback from consultees
Catherine McLean, Interface Pharmacist, NHS West Hampshire Clinical Commissioning Group.
Much of the evidence around the use of medicines for erectile dysfunction has been considered nationally and has been pivotal to any changes in the regulations for prescribing. Therefore I have updated the policy from the South Central Priorities Committee with any changes to these regulations on the assumption that the evidence for efficacy and safety has already been addressed. There are some minor differences in the products that are recommended by different organisations, but colleagues in Portsmouth and the Isle of Wight have been consulted and are happy with the content. West Hampshire, North Hampshire and Southampton already make joint formulary decisions. Something that is outside this remit but that came up in conversation with colleagues is the use of vacuum pumps. They are available on prescription but, as devices, do not qualify for review through the usual medicines evaluation processes. There is a lot of confusion in primary care about whether they should or should not be prescribed, so it will be good to have this clarified by
the evidence review. Carlton Symonds; Clinical Effectiveness Lead Isle of Wight NHS Trust Evaluation of Treatments for erectile dysfunction • Many patients that attend the urology ED service have been helped with many of these strategies • There is a danger that there is an assumption that a lack of high quality evidence means that a treatment shouldn’t be offered or doesn’t work. • Decisions to take into account the difficulty of proving the efficacy of some treatments, especially where placebo comparisons are difficult or where there is little commercial drive to provide trial data and for a holistic view of the unmeasured costs of not providing treatments that may impact significantly on quality of life and holistic wellbeing. • To increase offers of interventions to aid sexual functions • Application of holistic need assessment as per Cancer Recovery package. • Patients are seen as individuals with differing needs. • Prescriptions for the VED is now only available privately. Routine prescribing of a VED was not always necessary as a PDE5 once or twice a week would be as effective. While there is little evidence, the majority of those that have used it after privately buying it have found it very beneficial. These patients would be those that have failed or cannot have PDE5’s or injection therapy. • There is evidence that these men are willing to try anything that would help a deb ilitating problem. • All options should be available, but with algorithms and not a ‘one for all’ approach.
Declarations of Interest for incorporating to SHIP evidence reviews
Members and standing invitees are strongly reminded to identify and declare at this point, of feeding back on the supplied draft evidence review on behalf of the Southampton, Hampshire, Isle of Wight and Portsmouth (SHIP) Committee, any direct or indirect conflicts of interest in relation to the clinical topics under review for the consideration of the SHIP meeting. Declarations are to be made regardless of whether they are already standing declarations already published on registers of interest. These may relate to themselves or others (close family members, business partners, close friend or associate) with regard to:
Directorships, including non-executive directorships, held in private companies or PLCs.
Ownership or part-ownership of private companies, businesses or consultancies likely or
possibly seeking to do business with the NHS.
Shareholdings and ownership interests in any publicly listed, private or not for profit company,
business, partnership or consultancy, which are doing, or might reasonably be expected to do,

SCWCSU/Clinical Effectiveness 02/2020 for SHIP consideration Page 18 of 23
business with NHS England and/or NHS Improvement.
A position of authority in another NHS organisation, commercial, charity, voluntary,
professional, statutory or other body which could be seen to influence your role.
A position on an advisory group or other paid or unpaid decision-making forum that could
influence how NHS England and/or NHS Improvement spends taxpayers’ money.
Any connection with a private, public, voluntary or other organisation contracting for NHS
services.
Any other commercial interest relating to any relevant decision to be taken by the organisation;
such as financial benefit to primary care practice, private or secondary care provider and/or
other partner organisations in changes to formulary tariff / income / expenditure / costs through
prescribing of particular products resulting from adoption of TVPC commissioning policy
statements.
A judgement will be made by the Chair of the Committee as to materiality to decision making / recommendations in line with terms of reference.

SCWCSU/Clinical Effectiveness 02/2020 for SHIP consideration Page 19 of 23
Appendix 2: Current SHIP policy recommendation

SCWCSU/Clinical Effectiveness 02/2020 for SHIP consideration Page 20 of 23
Appendix 3: Current SHIP policy recommendation on penile rehabilitation following prostate surgery

SCWCSU/Clinical Effectiveness 02/2020 for SHIP consideration Page 21 of 23
Appendix 4: Management algorithm for erectile dysfunction: EAU guidelines

SCWCSU/Clinical Effectiveness 02/2020 for SHIP consideration Page 22 of 23
Appendix 5: Spend and patient numbers per pump device Osbon ErecAid Esteem Vacuum Pump
Commissioner / Provider Quantity X Items Actual Cost
FAREHAM AND GOSPORT CCG 9.0 1,666.71
NORTH HAMPSHIRE CCG <5 741.19
PORTSMOUTH CCG <5 185.70
PORTSMOUTH CCG 8.0 1,478.70
SOUTH EASTERN HAMPSHIRE CCG 10.0 1,850.83
WEST HAMPSHIRE CCG <5 183.98
Rapport Classic Vacuum Pump
FAREHAM AND GOSPORT CCG <5 220.04
PORTSMOUTH CCG 6.0 658.80
SOUTH EASTERN HAMPSHIRE CCG <5 329.92
WEST HAMPSHIRE CCG <5 328.87
VaxAid Hydropump V30 Vacuum Pump
NORTH HAMPSHIRE CCG <5 82.34
iMEDicare SomaCorrect Vacuum Pump
ISLE OF WIGHT CCG <5 148.77
NORTH EAST HAMPSHIRE AND FARNHAM CCG <5 445.06
NORTH HAMPSHIRE CCG <5 446.72
PORTSMOUTH CCG <5 149.01
SOUTH EASTERN HAMPSHIRE CCG <5 148.94
WEST HAMPSHIRE CCG 5.0 744.36
iMEDicare SomaCorrect Xtra Vacuum Pump
FAREHAM AND GOSPORT CCG 8.0 1,363.64
ISLE OF WIGHT CCG <5 171.10
NORTH EAST HAMPSHIRE AND FARNHAM CCG 8.0 1,365.92
NORTH HAMPSHIRE CCG 23.0 3,924.23
PORTSMOUTH CCG 6.0 1,025.03
SOUTH EASTERN HAMPSHIRE CCG 10.0 1,706.09
SOUTHAMPTON CCG <5 171.07
SOUTHAMPTON CCG 5.0 850.86
WEST HAMPSHIRE CCG <5 169.25
WEST HAMPSHIRE CCG 53.0 9,041.55
iMEDicare SomaErect Response II Vacuum Pump
FAREHAM AND GOSPORT CCG 33.0 5,068.42
ISLE OF WIGHT CCG <5 459.88
NORTH EAST HAMPSHIRE AND FARNHAM CCG 6.0 919.07
NORTH HAMPSHIRE CCG 8.0 1,230.24
PORTSMOUTH CCG <5 305.89
PORTSMOUTH CCG 29.0 4,451.43

SCWCSU/Clinical Effectiveness 02/2020 for SHIP consideration Page 23 of 23
SOUTH EASTERN HAMPSHIRE CCG <5 153.78
SOUTH EASTERN HAMPSHIRE CCG 32.0 4,903.70
SOUTHAMPTON CCG <5 459.93
SOUTHAMPTON CCG 35.0 5,364.81
WEST HAMPSHIRE CCG <5 152.05
WEST HAMPSHIRE CCG 64.0 9,796.76
iMEDicare SomaErect Response II XL Vacuum Pump
FAREHAM AND GOSPORT CCG <5 304.17
WEST HAMPSHIRE CCG <5 456.58
iMEDicare SomaErect Touch II Vacuum Pump
PORTSMOUTH CCG <5 159.80
Appendix 6: Review methodology checklist
Key resources searched and policy considerations National ‘best practice’ guidelines National evaluations and audits x Review of available evidence of clinical and cost effectiveness and best practice Local and other regional CCG funding polices x Local activity and audit data (eg, RightCare resources, HSCIC benchmarking, RCS quality dashboard)
Public Sector Equality Duty Patient / Public engagement x Clinical consultation Implementation and communication plan; primary and secondary care engagement x
The standard evidence review methodology for local funding policy updates includes the review of key national guidelines (NICE, Department of Health, Royal College of Physicians and other Royal Colleges, Scottish Intercollegiate Guideline Network, All Wales Medicines Strategy Group, Scottish Medicines Consortium, Clinical Knowledge Summaries and NHS Health Technology Assessment). If no national policy or guidance is available, then the international guideline resources (databases of international guidelines) are searched. Further evidence search will be carried out to include studies or reviews published since the publication of the most recent national guideline. Only in the absence of up-to-date evidence-based guidelines is a further full systematic literature search undertaken.