Shifting the Balance of Care Models, Pathways and People stories Stuart Cumming Bette Locke Kathy...
74
Shifting the Balance of Care Models, Pathways and People stories Stuart Cumming Bette Locke Kathy O’Neil January 2014
-
Upload
emil-harvey -
Category
Documents
-
view
212 -
download
0
Transcript of Shifting the Balance of Care Models, Pathways and People stories Stuart Cumming Bette Locke Kathy...

Shifting the Balance of Care
Models, Pathways and People stories Stuart CummingBette LockeKathy O’NeilJanuary 2014


The Kerr Report -2005Traditional model Aspirational model
Geared towards acute conditions
Geared towards long term conditions
Hospital centred Embedded in Communities
Doctor dependant Team driven
Episodic, disjointed and reactive care
Continuous, integrated and preventative care
Patient and carers as passive recipients
Patient and carers as partners. Self Care encouraged and facilitated
Low Tech High tech

2014 - How far have we shifted?• 2020 Vision “Everyone is able to live longer and healthier lives at home or
homely setting” (SGHD)
• NHS Forth Valley Integrated Healthcare Strategy“Our focus now is to fully embed the new and integrated models of care across the range of care settings from acute through to primary and community care facilities.”
• Primary Care Development Plan “Shifting the balance of care away from reactive episodic care in an acute setting to team based anticipatory care closer to people’s homes is a vital part of implementing our strategy”

Acut
e Fo
cus
TTG
RTT
HAI
HEAT
Front Door
Prim
ary C
are
Focu
s
SBC
Admission avoidance
Lifestyle
LTCs
ACPs
Getting the Balance Right – Embedding Care in Communities

The demographic challengePopulation Trends Forth Valley 2013 - 33
0
10,000
20,000
30,000
40,000
50,000
60,000
70,000
80,000
90,000
0-15 16-29 30-49 50-64 65-74 75+
2013 2018 2023 2028 2033
+73.7%+33.6%
Overall increase 10%

NHS Scotland - Whole system working -Secondary Care Impact
0
500
1000
1500
2000
2500
Glo
ba
l Su
m
Qo
F
Pre
mis
es
En
ha
nce
d
Se
rvic
es
Bo
ard
Ad
min
iste
red
Fu
nd
s
Em
erg
en
cy
ad
mis
sio
ns
Ele
ctiv
e IP
& D
C
Pre
scrib
ing
Ne
w O
utp
atie
nt
atte
nd
an
ce
s
Dire
ct a
cce
ss
A&
E
£'m
Direct Impact=£4.75bn (approx. 70% Board expenditure)
Contracted=£700m (approx. 10% Board expenditure)

Kerr Theme
Continuous, integrated and preventative care

Anticipatory Care“Doing the right thing for the right person at the right time with the right outcome – every time”
• Anticipatory rather than reactive approach• Co-ordinated and planned care • Improve communication and 24/7 partnership working with patient and family as partners in care
• Workforce – education, training, communication, capacity, planning• Share information appropriately (KIS) 6258 in Forth Valley
ACPTriggers
Situation• Long term housebound• Complex care package or in receipt of respite care• Entry to care home* or community hospital • After discharge from unplanned admission• Frequent OOH contacts• Carer stress
Condition• Deteriorating long term condition• Requiring specialist nurse• Placed on palliative care *, dementia, learning disability or mental health register
Clinical Assessment• SPARRA(?>40)• Polypharmacy • Falls assessment• Recognised as vulnerable

Anticipatory Care - Avoiding unnecessary hospital admission
Margaret’s story
• Margaret age 84, lives alone, diabetic, CHD and has been admitted twice in 12 months confused ?CVA. Diagnosis UTI /low sodium
• Discussion with Margaret and her daughter ACP developed• Key Information Summary (KIS) highlighting Margaret is prone
to UTIs cause delirium. KIS accessible to PHCT/OOH/NHS 24/SAS
• Polypharmacy review• PHCT meeting to raise awareness of management of delirium
• Power of attorney in place• MECS• Emergency antibiotics in house• Daughter’s contact details available

Anticipatory Care Planning Assessment
Change Fund Reshaping Care for Older PeopleIrene Warnock

What is Anticipatory Care Planning?
• Many interpretations.• Anticipatory Care Planning- allows people to
think about their future care needs at the same time allowing difficult conversations to be addressed if desired. Person centred goals are set and signposting to available identified needs.
• For us as a team we are looking at how an anticipatory assessment influences outcomes and how this process can be mainstreamed in future..

Achieving their “Good Life”.The Vision of Anticipatory Care Planning
Team is to:
Ensure the people of Stirling and Clackmannanshire lead as healthy a life as possible in a homely place of their choice within a culture of person centred, safe and effective care. Enabling them to plan for future care and ensuring they achieve their “Good Life”.

The interview is a conversation, not a tick box exercise
The team are• trained to manage difficult conversations and have a wide knowledge of local services • The interview is a conversation to allow flow from the
patient. Exchange Conversation where all partners are equal.
• If a follow-up meeting is required this can be arranged, or a phone call.
• If any tests eg blood, MSU or repeat B/P are required these are included in the visit.
• If an ongoing need requires to be met then these patients will be referred to the appropriate person.

“What makes your life good?”
• “What makes your life good?” The answer given sets the tone of the conversation and is reflected upon at the end of the assessment. This acts as an outcome measure to suit the patients needs. Goals that people aim for have been mostly easily met and ensures we are performing a person centred assessment with a positive outcome at each visit.
• Sams Story

Kerr Theme
Care geared towards managing long term conditions

Managing Long Term Conditions and Complex Care
• Condition Management • Complex Care and Co-morbidities• Self Management
• Education and Training• Multidisciplinary work and communication • Effective use of technology (communication and care) • Links with WSW, ACP and preventative approach
Tier 0Well
Tier 1Development of Symptoms
Tier 2Established Long Term Condition or Health Problem
Care managed in Community
Tier 3Enduring or complex problem.
Care mostly managed in community but requiring specialist input
Tier 4More serious exacerbations
or single episodesCare needs more complex
Tier 5End of
life care

Supporting long term condition managementand Shifting workload out across the interface
Increased range of community services• Near Patient Testing• Anticoagulant monitoring• Direct access to diagnostics• Pre-clinic, pre-diagnostic, pre- chemo tests
Improving access and care• Admission alternatives/ Early discharge• Primary Care LTC clinics and management plans• Physical Health checks for long term complex mental health needs• Minor Surgery, Joint Injections
Agreed processes• Shifts need to be communicated, planned and agreed (e.g. prostate
cancer)• Clear Guidelines- outline roles and responsibilities• Ensure safety and quality- infrastructure, capability and capacity• Support professional development

Laura age 41• Rapidly
progressive MS• Communication,
airway, mobility, care and nutritional issues
• Medication management and symptom control
• Childcare• Carer Support
• Home adaptations• Telehealth• 24/7 care package• PEG feeding• Respite care• Collaborative
Work with Primary Care, REACH, Complex Care and Local Authority
“I want to spend more quality time at home with family and friends” Laura 2006
Laura is still cared for 24/7 at home in 2014. She has had no unscheduled hospital stays in 7 years









Learning….?
• Need for consistency of service delivery and collaboration
• Increased awareness of anticipatory care
• Need to recognise the capability of community services
• Individuals and primary care manage risk in community at all times

Shifting the management of long term conditions
Diabetic care • In 1995 all diabetics attended hospital based diabetic clinics• Now all Type 2 diabetics primarily managed in the community• Community workforce (GPs, PNs, DNs) upskilling and training• Supported by GMS contract (2004) and LTCC (2006)
• Medication co-ordinated and complications managed by PHCTs• Focus on prevention and lifestyle interventions and self
management enabled
• Improved interface links with specialist nursing• Only most complex seen by diabetologist
NB. Workforce capacityPrevalence of diabetes in 2000 2.8% population, 2013 4.4%
population
Tier 0Well
Tier 1Development of Symptoms
Tier 2Established Long Term Condition or Health Problem
Care managed in Community
Tier 3Enduring or complex problem.
Care mostly managed in community but requiring specialist input
Tier 4More serious exacerbations
or single episodesCare needs more complex
Tier 5End of
life care

Kerr Theme
Care embedded and accessed in communities

RESHAPING CARE FOR OLDER PEOPLEIN
Forth Valley
THE RIGHT SERVICE - IN THE RIGHT PLACE - AT THE RIGHT TIME

Our Mission…
“to enable older people in Forth Valley to live full and positive lives in their own homes or when this is not possible within homely settings within supportive communities.”

Partnership Approach
Reshaping Care for Older People is being delivered through a partnership approach between Local Authority, NHS, Third and Independent Sectors in Forth Valley.
Joint Strategic Comissioning Plans were developed and consulted upon early 2013
People said….

More joined up services, not just joined up structures
•Improved ability to co-ordinate care and support around individual needs•Shared roles and responsibilities•All services working to common outcomes•Streamlined systems and Shared information•Less duplication, less hurdles to jump between agencies•Better care for individuals, particularly those with complex needs.

People don’t want health care or social
care, they just want the best care.
•Less complexity•Easier points of access•Easier to navigate•Co-ordinated care from joined up services•Services “planned around me” and working to common outcomes • integrated services which do feel truly seamless

Impact on ServicesCare Provision Projections (Scenario 1)
0
1000
2000
3000
4000
5000
6000
2000 2005 2010 2015 2020 2025 2030 2035
Year
Co
un
t o
f C
lie
nts
Non-Intensive Home Care
Intensive Home Care
Residential Care
Geriatric Care
Actual
Forecast

Priority Areas for Change
• Preventative and Proactive Care in the Community and Support at Home
• Anticipating and Preventing Unnecessary Hospital Admission
• Effective Care at Times of Transition (including effective flow through hospital)
• Reshaping Hospital and Care Homes

Preventative and Proactive Care in the Community and Support at
Home – Keeping Well
– Early Preventative approaches– Early Intervention – Choice & Control (including SDS)
• Community Based Supports• Development of Third and Independent Sector Capacity &Co-Production
approaches to community support services • Increased Community Capacity and Increased Co production
Also includes. • Significant Growth in Telehealthcare• Responsive Adaptations and Equipment Services
• Support for Carers• Proactive and responsive support for carers• Effective Respite and support models in place

PARTNERSHIP INNOVATION FUND: Reshaping Care for Older People
Royal Voluntary Services Community Transport and Good Neighbours service aims to reduce social isolation in people of 65yrs+ by helping them to stay independent at home. They provide a volunteer based transport service to those unable to access public transport. Volunteer drivers are available daytime, evenings and at weekends. Good neighbour support can include grocery shopping, going for a walk, completing forms, small household tasks or just sitting with a cuppa for a chat.
Royal Voluntary Services Community Transport and Good Neighbours service aims to reduce social isolation in people of 65yrs+ by helping them to stay independent at home. They provide a volunteer based transport service to those unable to access public transport. Volunteer drivers are available daytime, evenings and at weekends. Good neighbour support can include grocery shopping, going for a walk, completing forms, small household tasks or just sitting with a cuppa for a chat.
Community Transport Service:
volunteer assistance with transport to appointments / shopping / social activities etc.
Good Neighbours: help with a range of practical tasks around the home & garden / someone to chat to.
Telephone Support Service:
Regular telephone contact with a volunteer.
Service Users – 254
34% aged 60-75yrs
66% aged over 75yrs
Volunteers – 66
25% males, 75% females
Service User Quotes: “Thank you for restoring my ability to remain independent”
“I look forward to someone coming to have a talk to for company.”Case Study:
Mr and Mrs White were referred when Mr White was in latter stages of dementia and had been admitted to a Care Home. Mrs White, with no family supports, required support and transport to visit. Once matched with an RVS Volunteer who also provided support to couple with facilitating some reminiscence support. Mr. White’s condition deteriorated and was transferred to Hospital. RVS Volunteer supported Mrs A to visit husband with a flexible short notice service to meet Mrs White needs. Sadly Mr White passed away, RVS continued to provide emotional support to Mrs White through her bereavement.

Supporting Carers
Princes Royal Trust for Carers ProjectsACP, Discharge support workers. Carers Training programme and Development mgr Post
6 month snapshot 2013
232 new carers 1:1 supported
22 care with confidence sessions completed
952 carer interfaces (enquiries, contacts, supports etc)
109 carers trained through care with confidence programme
351 professional based enquiries69 meetings with professionals37 Trainer and awareness sessions
2 carers awareness sessions with student nurses
347 additional proactive approaches to professionalsCarers Forum actively meeting and engaging
Carers Forum developed in both Stirling and Clacks, actively meeting, engaging and involving carers

Anticipating and Preventing Unnecessary Hospital Admission
• Personal Planning with individuals who have significant health and care needs.
• Remodel pathway of acute care for frailer older people
• Clear pathways and interventions for individuals who Fall or are at risk of falling
• Rural models of care and support will be extended• Support for Carers- Effective Respite and support
models in place.• Third and Independent Sector Capacity & Co-
Production approaches will be developed to support anticipatory models.

Supporting Acute Flow – Allied Health Professions (AHP) 7 Day Model of Working
Since April 2013 the following services have been provided within FVRH:-
Sunday AHP Fastrack service in the; Emergency Department, Clinical Assessment and Acute Assessment Units at FVRH (enabling a 7 day service).•Provides urgent triage to identify frail older people•Assess, treat, provide equipment and establish care packages to prevent admission•Early assessment and rehab
Sunday Fastrack:- 100% of patients seen in the Emergency Dept on a Sunday have been discharged following assessment/treatment by Fastrack. An average of 5.5 people/Sunday are seen.
7 day Occupational Therapy and Physiotherapy service to downstream wards to provide:•continued rehabilitation•assessment and treatment for timely discharge.•Since August 2013 - Support the Frail Elderly Assessment Unit in comprehensive geriatric assessment and treatment.
Support discharge at weekends – particularly Orthopaedic patients
Weekend Physiotherapy:-

Developing Enabling Services Delivery of an INTEGRATED Intermediate Care service, with single
access points for assessment and review including the following:
• A responsive 7 day model• An effective Intermediate Care Bed Model• Reshaped Home care with Re-ablement Pathway as the
norm for individual identified with new or increasing “needs”• Reshaped internal Day Care services• Reshaped Dementia Pathway which facilitates early
diagnosis, post diagnostic support and personal planning.• Moving away from statutory provision to that of alternative
supports through community, third and independent sector supports.

Re-design of Homecare Services
Project description Development of Reablement based home care
Integration of Rehabilitation and Reablement services
•Rural Northwest
•Clackmannanshire Reablement
•Falkirk home care redesign
•Stirling Intermediate care model

Reshaping Hospital and Care Homes
Models of care which use hospital and care home resources most effectively
•Embedded Intermediate Care Bed Model •Remodel Community Hospital Beds
• Ultimate integration between health and social care models
• Business Case for Stirling Care village•Reduced average length of stay long term care•Reduce rate of care home place per head of population.•Reduced Acute Hospital Bed Days >75yrs•Alternatives to admission including Hospital @ Home

Supporting Care HomesPreventing Admission
Care Home Liaison Psychiatry
The Care Home Liaison Psychiatry Service has been piloted in Clacks & Stirling during the period Oct '12 to Oct '13 using Change Funding
Since the establishment of the service in October 2012, admissions to the acute psychiatric inpatient wards from the care homes covered by the Care Home Liaison Nurse have reduced from 17 patients up to and including September 2012; to 3 patients up to and including September 2013.
In the same period the total amount of referrals to the service was 211 (Stirling area 131, Clacks 80).
A service evaluation was produced in Dec'13

Supporting People to Remain at Home Stirling Intermediate Care; 25 Short
Stay Assessment Beds in Beech Gardens and Allan Lodge Residential Care Homes
.
25 bed model achieved in November 2013 across two local authority care homes88 Discharges between April and November 201348% being discharged Home (sustained at 3 months post discharge)50-60% of admissions are from hospital and 40-50% direct from communityLength of stay in this period was 7 weeks in Allan Lodge and 9 weeks in Beech Gardens. This has reduced from an overall average of 9 weeks in previous reporting period.
See also Personal Outcomes section
Mrs B was admitted for a short stay assessment placement following a fall while on holiday. She was in severe pain upon admission, requiring high levels of pain medication and with subsequently, severely limited mobility. She required the support of stand-aid equipment to rise and the support of 2 staff for all transfers. Mrs B’s main outcome was to improve her independence to allow her to go home with minimal supports. She met this outcome, returning home, walking with the assistance of a walking stick, with the support of Reablement services. She was visited 3 months following her period of rehabilitation, and was found to have returned to activities such as going to the shops and to local groups in her town. She had accepted a small package of support from a framework provider to assist her with her personal care each day, but was otherwise largely independent.

Pause for thought..
• Supporting People at Home– Intermediate Care Services…..
– Next slide Stirling Care Village

A Care Village in StirlingA Health & Social Care Partnership Venture

Stirling Care Village Scope• 116 bed integrated care hub,• 5 GP Practices, • Urgent Care, GP OOH, • Diagnostic X Ray & U/S, • Ambulance Station, • FV College partnership.
Out with Project Scope• Housing• Retained Stirling Community Hospital

The Care Village: Care Hub
One Key Component of the Wider Pathway of Care for Older People

Review of other Care Village models

Case for Change• Demographics, complexity, co-morbidity.
• Transformational change required around long term care and acute care pathways
• Stirling bed based care model is across 5 different sites, all of poor condition & inefficient size.
– Interface between hospital and community admission/ discharge care paths are “Clunky”
– Limited ability to integrate further
– Limited ability to develop models of scale in current state
– Unnecessary delays and inefficient use of resources
• Evidence of growing impact of intermediate and short term models

•Home•Community Services•Primary Care Services•Limited Capacity•Transforming from Reactive Care
Acute Hospital Sandwich
Acute Hospital: 3500 >65 Stirling Res admissions Place of SafetyRising DemandRising AdmissionsRising Bed Days
SCH : c400 annual
admissions Rehabilitation –
Home 50%
Unsustainable
Delays
Delays
Care Homes: 20% of CH Discharges Plus Community Admissions

Care Hub Model• An Integrated Care Model which transforms the “step up and step down” element of a single care
pathway
• Providing Integrated care in the Right environment for a short period of Time– Rehabilitation – Assessment for long term care– Step up admission from community or urgent care– Discharge processing– Step down hospital care (medical, palliative, specialist..)– Psychiatry intermediate care
• A facility that should not be seen in isolation nor as the whole solution– Independent sector, community provision

Care Homes:Avoiding / Delaying admission.Reducing average LoSINTEGRATE CAPACITY - Utilise for short stay respite / Int Care assessment / Palliative Care
HospitalAvoiding Admission, expediting discharge.Effective Frailty Model
Community Focus•Person Centred•Family and Community supports•Homecare Transformation: Reablement•Anticipatory Care•Preventative Planning Approaches•Carers supported
Community Focus•Person Centred•Family and Community supports•Homecare Transformation: Reablement•Anticipatory Care•Preventative Planning Approaches•Carers supported
Care Hub – a key part of a much wider pathway
Care HuB: Integrated
Intermediate Care: Short Term Assessment
Step Up & Step Down
Social Care Based Model – optimising home based care

Masterplan July 2013

Kerr Theme
Self care encouraged and facilitated.
Patients and carers seen as partners

Supporting Self Care• Person Centred Care- “Nothing about me, without me” (SGHD, 2013)
• Development of a wide range of early interventions across lifecourse (including Early Years and Ageing Well)
• Greater focus and collaboration on lifestyle interventions ObesitySmoking cessationAlcohol and drugs (ABIs, methadone)
• Physical Activity - Pathways to Health - OTAGO
- LTC rehabilitation
• Mental Wellbeing - “See Me”, Keep Well-Stress Control, Moodjuice, Beating the Blues
• Community Planning initiatives - Hawkhill - Clacks Healthy Lives

Kerr Theme
Healthcare embedded in communities

Healthcare Embedded in CommunitiesPrimary care - Delivering for the future
Health and Social Care Integration and 2020- Opportunities, catalysts and challenges- Recognise and join up ongoing work -RCOP, Change
Fund, Early Years, ACP, Care Village…and plan to deal with gaps
- Integrated workforce modelling inclusive of independent contractorsLocality Planning Group – Early visioning and engagement
- Purpose, priorities, plans and outcomes- Develop community infrastructure- Benefit of collaborative working ( Rural Stirling and
Bo’ness)- Need for autonomy, action plans and priorities - Person centred model

Self Directed Support
Supported Self Mix
Family &
Community
Anticipatory Care
Planning
CORE LOCALITY NETWORKEnabling Integrated Team Development
OOH (24/7Health & Social Care)
Patient
Older Peoples Services & Children's Services
Hospital & Home
including:AHP weekend
support, Overnight
Care, Rehab at Home
Community Hospital &
Intermediate Beds Model
Telecare
Responsive Social Care Services
Employability
Rehabilitation / Early Intervention
REACH
• General Practice and Nursing Teams
• Community Pharmacy
Mental Health & Learning Disability Support
Third Sector
Other Community Services: Police, Education / Care Homes
EXTENDED LOCALITY NETWORK
Specialist Mental Health
Services
Specialist Learning Disability Service
Complex Care Services
Specialist Rehab
Specialist Nursing
Workforce
Secondary Care
Tertiary Care
Reshaping Care for Older People
Integrated Care Pathways
Daycare Redesign
e.g. Acute, Hospital Liaison
Ambulatory Care including:AAU, CAU, ED
Review
Enhanced Carer
Support
SAS – See & Treat
Enhanced Discharge & Discharge Planning
Management Plans, LOS, Ward Reconfiguration
Carer Support & Training
Diagnostic Services
ACUTE SERVICES NETWORK
2020 Person-centred caremodel

Kerr Theme
Developing high tech healthcare

Developing high tech healthcareCommunication• Emergency Care Summary and Key Information
summary• Electronic referral and discharge• Paperlight-ish• ? e-consultation /videoconferencingSafety• Telecare – MECS, fall sensors, tracking, personalised
patient IT systemsManagement• Telemedicine – ambulatory BP monitoring
- implantable defibrillators - condition monitoring and management
-Tele-Pulmonary Rehab

Kerr Theme
Using information effectively to drive change

Embedding quality care in community Using the GMS contract
Whole System Working Project
• Methodology to support quality improvement and anticipatory care across the system
• Comparative data, evidence, organisational support and protected learning time
• Allow reflection focussed on improving and developing services
• Improving consistent practise and reduce wasteful variability
• Effective and efficient use of resources
• Good engagement from practices

Whole System Working Project- Enhanced Services
– Anticipatory Care and Long Term Conditions
– Collaborative working- e.g. with Community Pharmacy/Diagnostics
– Health and Social Care Integration and Locality Planning
– Improving the Interfaces and developing pathways
– Improving long term condition management
– Patient Safety Programme
– Releasing Time to Care
– Prescribing Efficiency
– Shifting the Balance
– Introduce new ways of working e.g. SPSP (polypharmacy, falls) and Locality development

Whole System Working – appropriate information to promote consistent practise and reduce wasteful variation

Qualitative change- Dementia Pathway
• Need for better integration and consistency
• Develop patient pathway with referral criteria• Electronic referral pathway• Standardised use of assessment tools
• Effective signposting
• HEAT -post diagnostic support • Shared care protocols
• Increased awareness of legislation- Power of Attorney- Adults with Incapacity
• Consolidate changes- Dementia Steering Group

Ezetimibe GIC/1000 Patients - Mainland Health Boards and Scotland
Quantifiable changes
Benefit of Clinical Engagement

Quantifiable changes
•Lumbar Spine X Rays have reduced by 50% and a new access pathway proposed
•CT head has reduced by >50% with new guideline being implemented
•MSSU testing has reduced by 33%- SIGN 88
•B12 testing has reduced by 30% - Forth Valley guideline
•PSA testing to guideline and reduction of 16%
•6256 Key Info Summaries (2.25% population)

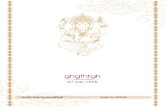
Prescribing efficiency
Health Boards GIC per patient
£140
£150
£160
£170
£180
£190
£200
£210
Sep
200
7
Nov
200
7
Jan
2008
Mar
200
8
May
200
8
Jul 2
008
Sep
200
8
Nov
200
8
Jan
2009
Mar
200
9
May
200
9
Jul 2
009
Sep
200
9
Nov
200
9
Jan
2010
Mar
201
0
May
201
0
Jul 2
010
Sep
201
0
Nov
201
0
Jan
2011
Mar
201
1
May
201
1
Jul 2
011
Sep
201
1
Nov
201
1
Jan
2012
Mar
201
2
May
201
2
Jul
y 20
12
Sep
201
2
Nov
201
2
Jan
201
3
Mar
201
3
May
201
3
An
nu
alis
ed T
ota
ls
NHS Ayrshire & Arran NHS Borders NHS Dumfries & Galloway NHS FifeNHS Forth Valley NHS Grampian NHS Greater Glasgow & Clyde NHS HighlandNHS Lanarkshire NHS Lothian NHS Tayside Scotland

Kerr aspirations have started to become a reality but there is a need to focus more on …
• workforce planning and skill development to meet the potential of shift to community based care
• aligning resources and positioning community services to deliver 2020
• mainstream existing quality initiatives and prioritise LTC, ACP and admission avoidance work
• managing interface between primary and secondary care and health and social care
• supporting the use of technology to improve patient care• provision of analytical and improvement support to assess
impact of revised models

A bit of a challenge …. but it can be done!