
Sharing and Caring: Modern Milk Banking - hacked by Hmei7
48
Mercy Health Sharing and Caring: Modern Milk Banking Dr Gillian Opie MBBS FRACP IBCLC Kerri McEgan RN,RM,Masters of Midwifery,IBCLC
Transcript of Sharing and Caring: Modern Milk Banking - hacked by Hmei7

Mercy Health
Sharing and Caring:
Modern Milk Banking
Dr Gillian Opie MBBS FRACP IBCLC
Kerri McEgan RN,RM,Masters of Midwifery,IBCLC

Mercy HealthNot so new and not so old
• Milk banking is not a new concept
• Operating in various capacities since time immemorial
• What is new, is the level of rigor required by both government and
insurance bodies to establish a milk bank
• < 5 years in Australia
• 20 years ago Switzerland formalised operating guidelines
• 70 years ago in Stockholm, Sweden
•100 years ago opened in Europe and USA

Mercy Health
Is there a need ?
2004 audit
NICU breastfeeding initiation 98%
1:6 infants in MHW nursery required formula
supplementation in first 2 weeks of life due to
insufficient supply
250 litres per year

Mercy HealthEvidence
Lucas 1990:
Better weight gain
Better bone density
Lower BP
McGuire 2003:
•Systematic review of Donor Milk vs Formula for prevention of NEC found
significant protective effect
Schanler 2005:
•RCT of DM vs Formula as supplement to MOM ? Beneficial
•Significant decrease in Chronic Lung Disease in MOM and DM
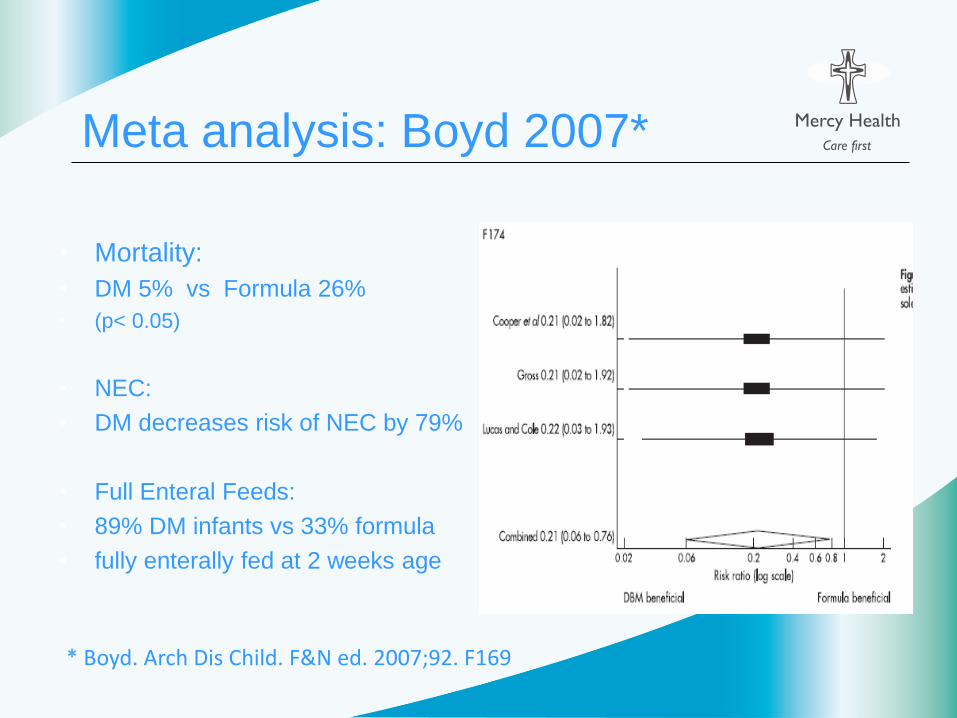
Mercy HealthMeta analysis: Boyd 2007*
• Mortality:
• DM 5% vs Formula 26%
• (p< 0.05)
• NEC:
• DM decreases risk of NEC by 79%
• Full Enteral Feeds:
• 89% DM infants vs 33% formula
• fully enterally fed at 2 weeks age
* Boyd. Arch Dis Child. F&N ed. 2007;92. F169

Mercy HealthA Brief History
• Minimum 2 years formal planning within MHW
• Further18 months negotiating with regulatory bodies
• – Department of Health (DoH)
• - Victorian Managed Insurance Authority (VMIA)
• - Risk mitigation paramount
• Ministerial approval in relation to specific Acts
• - Food Act, Therapeutic Goods Act, Human Tissue Act
• DoH considered the UK NICE Guidelines as the benchmark
• Additional legal consultation (total 62.3 hours)
• Pathology service accreditation with NATA to test milk
Mercy HealthInternational Guidelines
• Clinical Guideline 93: Donor breast milk banks: the operation of donor
breast milk bank services. Issued February 2010 www.nice.org.uk
• Guidelines for the Establishment and Operation of a Donor Human Milk
Bank. Human Milk Banking Association of North America,Inc. 2008
www.hmbana.org

Mercy HealthIt’s more than the milk……
• Obtain and refurbish a suitable area
• Equipment procurement and testing (3 pasteurisers)
• Development of risk management plan and corporate governance
- policy and procedure development
- thorough process for extensive donor screening
- staff recruitment and training
• Registration and monitoring for Food Safety requirements
- regular auditing storage conditions
- annual inspection + independent audit
• Equipment repair and maintenance
• Nursery staff education
• Accreditation for pathology services

Mercy HealthDecisions
• Pasteurise
• No mixing of donors ( ie no pooling)
• Benchmark with UK guidelines
• Heat seal bottles pre-pasteurisation
• No post pasteurisation aliquotting
• Re-use BPA free bottles

Mercy Health Funding-Mercy Health Foundation
• No government funding currently available
• Corporate approach to develop an endowment fund
• Developed a marketing strategy for the milk bank
• Sought philanthropic donors
• Foundation provided the expertise for this important
component of the project development

Mercy Health

Mercy HealthSurvey prior to opening
Nursery families and staff
• Understanding of donor milk
• Donor milk safety
• Feelings about donor milk
• Willingness to donate
• Return rate of survey • 45 /100 nursery families
• 75/110 nursery staff

Mercy HealthFamilies’ response (n = 45)
• 30/45 providing breastmilk (BM) only
• 11/45 mostly BM
• 4/45 mostly formula
• 0/45 formula only
• Benefits of BF - majority aware
- 37/45 natural,43/45 benefits baby, 27/45 benefits mother
15/45 convenience
• Benefits of BF
- 23/45 immunity, 14/45 bonding, 12/45 nutrients
• Importance of BF
- 44/45 extremely or very important, 11/45 very important
• Most wanted to BF / provide BM for as long as they could

Mercy HealthUnderstanding of donor milk
• Understanding of the term “donor milk” very good
- only 5/45 had never heard of / didn’t know
• Breastmilk which has been given freely under carefully controlled &
medically supervised conditions
• Someone else giving their milk to your baby
• Providing breastmilk for every single mother even if they can’t generate
enough themselves
• Excess milk donated by a lactating mother to be made available to
mothers with not enough or no breastmilk
Mercy Health Survey: Donor milk safety
Donor screening 19/45 not aware *
Donated milk is pasteurised 30/45 didn’t know,
Pasteurisation destroys infectious diseases 32/45 didn’t know,
Pasteurisation preserves healthy properties 31/45 didn’t know
Donor milk is safe & effective
- 20/45 well aware, 20/45 somewhat, 5/45 didn’t know

Mercy HealthFeelings about using donor milk
• 16/45 very willing to accept donor milk
• 17/45 somewhat willing
• 6/45 somewhat uncomfortable
• 0/45 very uncomfortable
• 4/45 prefer baby to receive formula
• 7/45 would need more information before making a decision
Partners input
• 29/45 extremely important to ask partner
• 10/45 very important
• 3/45 somewhat important
• 3/45 not all important
Mercy Health
Willingness to Donate
• 23/45 very willing to donate
• 13/45 somewhat willing
• 7/45 only consider is a strong need
• 2/45 not willing
Age:
• 43 females & 4 males answered the questions
• 16/45 are 20 -29 years
• 25/45 are 30 – 39 years
• 3/45 are 40 – 49 years
Education:
10/45 completed year 11or12
16/45 Certificate or Diploma
18/45 Bachelor Degree or higher

Mercy Health Staff Prior Knowledge (n = 75)
• When a mother is unable to provide sufficient breastmilk to her infant, it is
acceptable to provide the infant with donor breastmilk
59 agree, 5 disagree, 9 +/-, 3 not sure
• Donor milk banks play an important role in promoting breastfeeding
53 agree, 15 +/-, 6 disagree, 3/75 not sure
• Donor milk banking is a safe practice
52 agree, 11 +/-, 4 disagree, 8 not sure
• Donor milk is superior to infant formula
65 agree, 6 +/-, 3 disagree, 1 not sure
• Infant formula carries risks to infant health
47agree, 15 +/-, 10 disagree, 3 not sure

Mercy HealthStaff Education
• 49/75 attended education sessions & 29/75 did not
• Those that had attended were more knowledgeable
• 40/75 were more supportive of milk banks after education
• 33/75 just as supportive
• 33/75 more confident discussing use of pasteurised donor milk (PDM)
with mothers/families
• 18/75 somewhat confident
• 21/75 not confident
Mercy HealthSummary of Staff Comments
Staff want more education in general re milk banks
• more on safety & handling issues- concerns parents might have re
receiving donated breastmilk
• a guideline -flow chart to discuss donor milk with parents or donors
• development of a protocol & pamphlet for parents
• procedure of how mothers can donate
• regular in services & easily accessible info to rely on particularly on N/D
when we don't have access to an LC
• Pasteurisation. MHW procedures & policies/guidelines. Legal
ramifications

Mercy HealthDonor Eligibility
• Own baby < 6 months age
• Baby and mother healthy
• Lactation well established – own baby fully breastmilk fed, either
at breast or expressed breastmilk
• Serological screening- similar to Blood Bank
• Donation is voluntary: no payment
• Milk is gifted to MHW
• Donors must drop off milk in person & sign a Declaration form
Dept of Health Victoria requests donors are known to Mercy
Hospital for Women (MHW) and have birthed at MHW or baby
cared for in MHW nursery

Mercy HealthDonors
• Volunteers must meet initial donor criteria
• Screening includes lifestyle and viral blood testing
• Donor accepted → signs consent form
• Donors must bring milk to the milk bank frozen
• Pasteurisation (Holder method)
• Bacterial testing pre + post pasteurisation
• Frozen for storage (up to 3 months)
• Donors not identified to recipients
• Individual donor pooling only
Mercy HealthTransmission of Infection
• Mothers own milk has small number of non-pathogenic bacteria
• Easily removed by pasteurisation
• Viruses: screening serology
• HIV 1&2
• Hepatitis B and C
• HTLV I & II
• Syphilis
• Any bacterial growth post pasteurisation means donor milk is unacceptable for distribution to babies

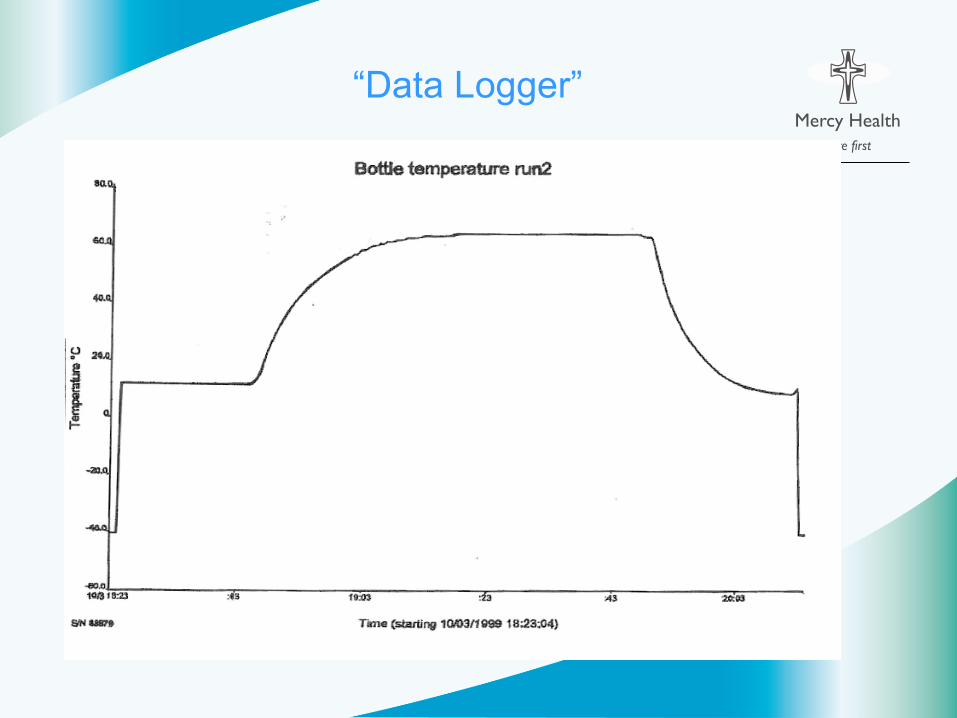
Mercy HealthHolder Pasteurisation
Boiling sterilises milk but removes many desirable factors
“Holder” pasteurisers developed in early 1980s
Baum et al (Oxford)
62.5OC for 30 minutes, then rapid cooling < 10OC
(not slower than 3.75O /minute)

Mercy Health

Mercy Health
Mercy Health
Mercy Health

Mercy Health
Electronic log of all pasteurisation runs

Mercy Health
Mercy Health
“Data Logger”
Mercy Health
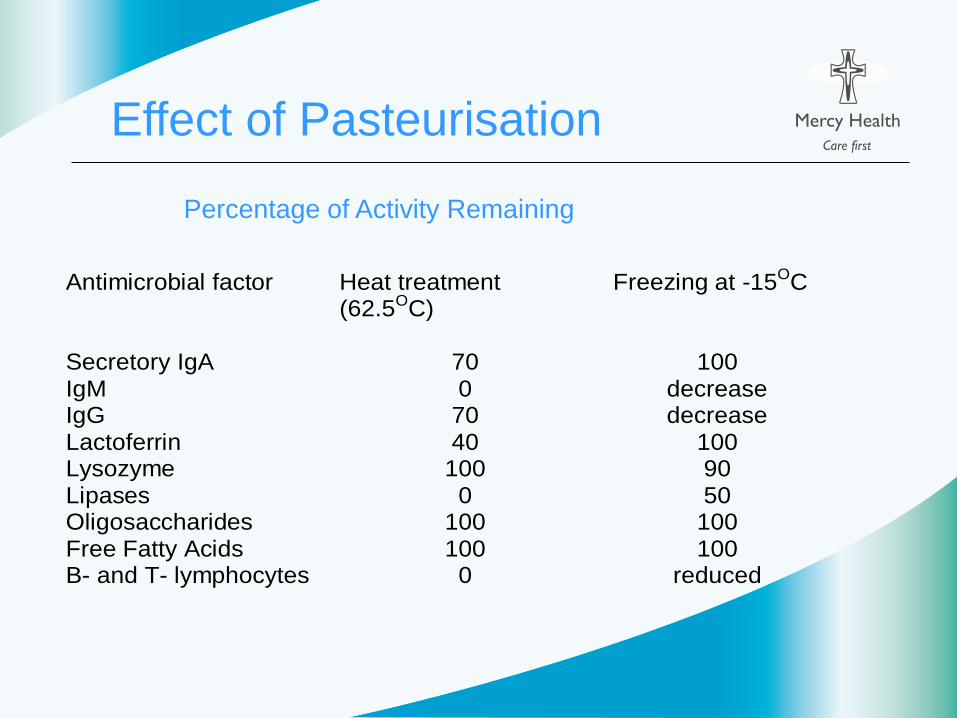
Effect of Pasteurisation
Percentage of Activity Remaining
Antimicrobial factor Heat treatment (62.5OC)
Freezing at -15OC
Secretory IgA 70 100 IgM 0 decrease IgG 70 decrease Lactoferrin 40 100 Lysozyme 100 90 Lipases 0 50 Oligosaccharides 100 100 Free Fatty Acids 100 100 B- and T- lymphocytes 0 reduced

Mercy Health
Standards pre-pasteurisation
Bacteria in milk North
America
UK
Commensals < 104 cfu/ml < 105 cfu/ml
Eg CONS, Strep
viridans
Staph Aureus Unsuitable Unsuitable
Enterobacteria Unsuitable Unsuitable

Mercy HealthStandards post pasteurisation
Any bacterial growth post
pasteurisation is unacceptable for
distribution to babies

Mercy HealthDonors to date…
• Number of donors screened - 40
• Reasons donors unable to donate
- not a MHW patient
- medication( prescription and herbal)
- lived in UK during exclusion time
- partner smokes inside
- only wanted to donate previously expressed milk
- distance
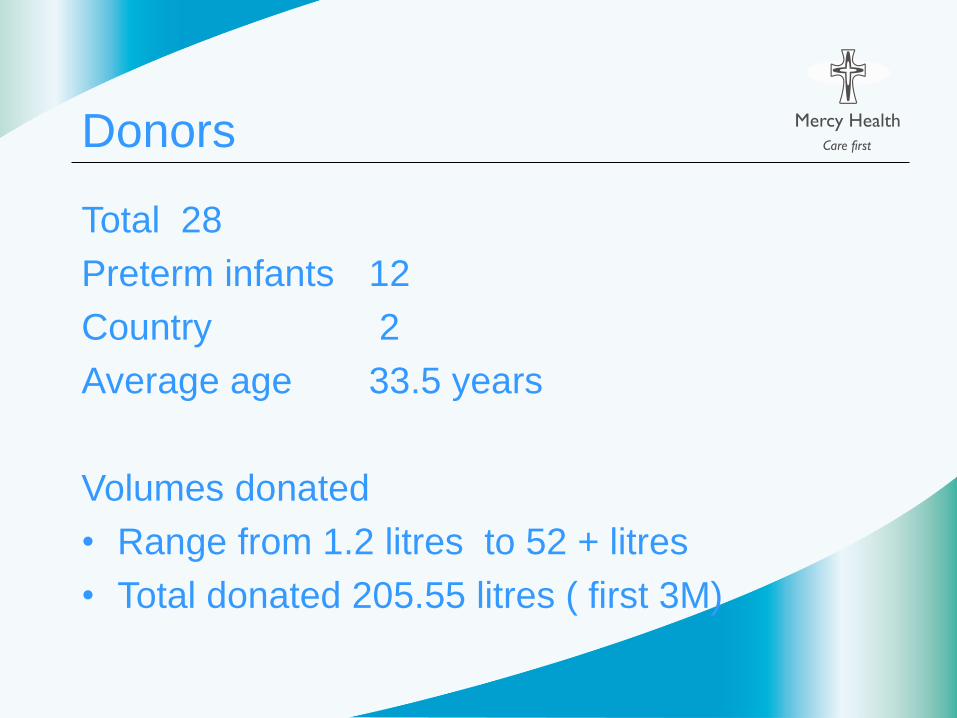
Mercy HealthDonors
Total 28
Preterm infants 12
Country 2
Average age 33.5 years
Volumes donated
• Range from 1.2 litres to 52 + litres
• Total donated 205.55 litres ( first 3M)

Mercy HealthVolumes Donated first 3 M

Mercy HealthBacteria: what has grown
Pre-pasteurisation: 85 isolates
49% CONS coagulase negative staphylococcus
13% Acetinobacter species
7 % Enterobacter cloacae
5% Gram negative bacilli ( not otherwise identified)
4% Streptococcus Salivarius
3 % Staph aureus
27% mixed isolates
13% unacceptable – milk discarded ( 72.7 litres in first 3 months)
37% acceptable – usually low growth of CONS

Mercy HealthDonors-how much time does it take?
• Telephone/face to face conversations re screening criteria(5-30 minutes)
• Allow 1 hour for face to face donor screening
• An additional 30 minutes to discuss decontamination of pump parts,
expressing, storing & transportation
• Blood testing
• Ongoing telephone/face to face conversations (5-30 minutes)
• Administrative tasks to record donor details
• Allow 1 week for all serological results to be reported
• May take up to 2-3 weeks before sufficient donor milk available to be
pasteurised
• Meet donors weekly for milk drop off and sign donor declaration form
• Scan milk into milk bank via LacTrack®

Mercy HealthRecipients
• Potential recipient families given written information
regarding PDM
• Written consent from family required before distribution
of PDM
• Lactation consultant referral for milk supply issues
• Daily collection of PDM orders, allocation & distribution
of milk
• Allocate weekend & after hours supply
• Separate PDM freezer in SCN to distinguish form
mothers’ own

Mercy HealthEligibility to Receive Donor Milk
• Inpatient in tertiary NICU/SCN
• Pre terms <32 weeks
• VLBW <1500 grams
• Post Necrotising Enterocolitis
• Post-operative short gut syndromes
• Malabsorportion syndromes
• Identified by clinical staff
• Written parental consent to accept PDM
• Medical order

Mercy HealthRecipients
First baby fed 2st July 2011
Total to end December 2011 = 30
Average statistics
Gestation at birth = 29.6 weeks
Birthweight = 1329 g
Days of PDM = 20
Twins = 6 pairs
Volumes required 640mls to 10.64 litres
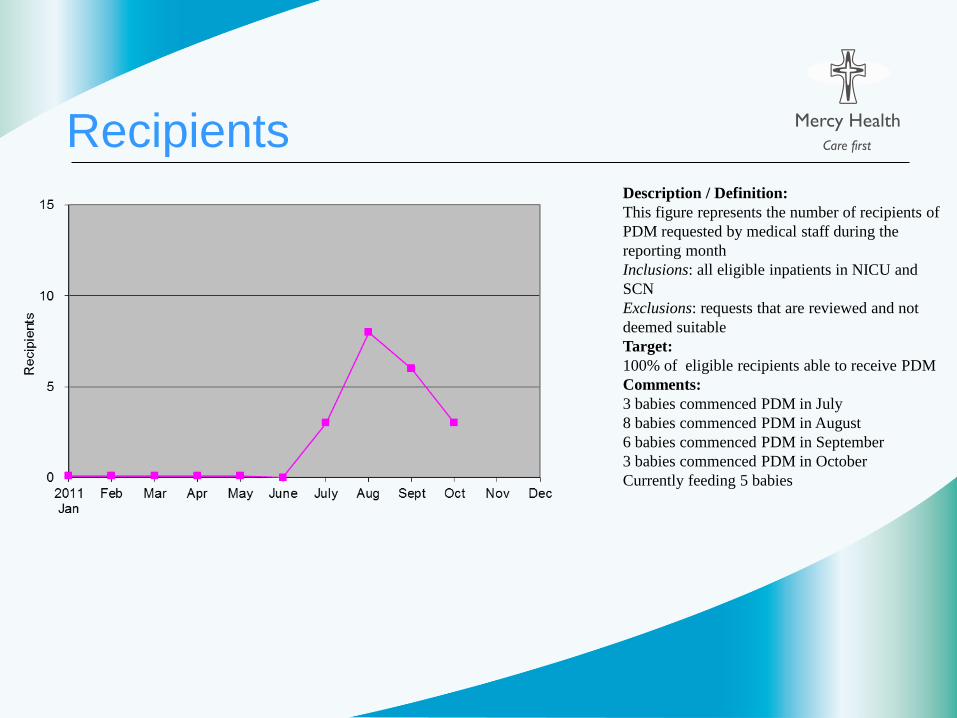
Mercy HealthRecipients Description / Definition:
This figure represents the number of recipients of
PDM requested by medical staff during the
reporting month
Inclusions: all eligible inpatients in NICU and
SCN
Exclusions: requests that are reviewed and not
deemed suitable
Target:
100% of eligible recipients able to receive PDM
Comments:
3 babies commenced PDM in July
8 babies commenced PDM in August
6 babies commenced PDM in September
3 babies commenced PDM in October
Currently feeding 5 babies
Mercy HealthRecipient reasons:
Reasons for use of pasteurised
donor
milk (PDM)
- <1500 grams
- < 34 weeks
- little or no supply available
(early)
- maternal medication
- maternal medical conditions
- diminishing maternal supply
(late)
Mercy HealthRecipients: Feeding at discharge
27 discharged or transferred
9 breastmilk
9 formula
8 transferred to level 2 SCN
3 inpatients
1death ( early sepsis )

Mercy HealthThe Next Phase….
• Consolidate practice at MHW
• Establish budgetary requirements
• Expand current Food Safety Plan to meet audit requirements
• Negotiate with regulatory bodies regarding current restrictions
• Develop business case for supply of PDM to other tertiary facilities
• Ongoing staff development and training
• Refine data collection
• Define research questions
• Develop National Standards for Milk Banks In Australia

Mercy HealthThe Necessities of Milk Banking
• Patience +++
• Tenacity in adversity
• Flexibility/lateral thinking
• Attention to detail/methodical approach
• Sense of humour
• Counselling skills
• A knowledge of lactation, expressing and breastfeeding
• Jack of all trades
Above all else - believe in the product!

Mercy Health
Start Small, Grow Slowly
Acknowledgments: Ms Kerri McEgan, Manager Milk Bank
Robyn Kilpatrick, Milk Bank assistant
Mercy Health Foundation


















