Share01.pdf

of 12
-
Upload
sanjay-nayak -
Category
Documents
-
view
215 -
download
0
Transcript of Share01.pdf
-
7/28/2019 Share01.pdf
1/12
585
Review
www.expert-reviews.com ISSN 1478-7210 2012 Expert Reviews Ltd10.1586/ERI.12.36
Despite enormous advances in techniques orthe management o mechanically ventilatedpatients, ventilator-associated pneumonia(VAP) remains the most requent inectionamong patients hospitalized in intensive careunits (ICUs) [1]. It represents a nosocomialinection that develops in ICU patients atleast 48 h ater mechanical ventilation (MV)is established and is caused by pathogens thatwere incubating or not present at the time MVwas started [1,2].
VAP has a greater impact on morbidity, occur-ring at an estimated rate o 13% per day oMV, with a 927% incidence among all intu-bated patients [35]. Based on the timing oonset, VAP can be divided into early-onset VAP(approximately a third o cases), occurring within45 days ater intubation and mainly caused bycommunity pathogens with a avorable pattern oantibiotic sensitivity (Streptococcus pneumoniae,Haemophilus inuenzae and anaerobes o theoral cavity), and late-onset VAP (approximatelytwo-thirds o cases), oten caused by multidrug-
resistant (MDR) pathogens (e.g., Staphylococcus
aureus, Pseudomonas aeruginosa, Enterobacteriaceaeand Acinetobacter baumannii) selected byexposure to broad-spectrum antibiotics andresponsible or greater morbidity, prolongedICU stay and longer duration o ventilation,with estimated costs exceeding US$15,000 peroccurrence [6,7].
In addition to morbidity and economiccosts associated with VAP, the burden o dis-ease is heightened by the still high mortality.In particular, the mortality rate or late-onset
VAP ranges rom 24 to 50% and can reach76% in some specic settings or when lunginection is caused by high-risk pathogens [2].Notwithstanding, mortality is heavily infu-enced by the disease severity at VAP onset anddierent values are reported in dierent studies,ranging between 0 and 50% [8,9]. A recent meta-analysis demonstrated that although presence,compared with absence, o VAP seems to beassociated with higher mortality in critically i llpatients, appropriateness o initial antimicrobialtreatment in such patients may moderate this
association [10].
Matteo Bassetti*1,2,
Lucia Taramasso3
,Daniele RobertoGiacobbe3 andPaolo Pelosi4
1Inectious Diseases Division, Santa
Maria Misericordia University Hospital,
Udine, Italy2Clinica Malattie Inettive, Azienda
Ospedaliera Universitaria Santa Maria
della Misericordia, Piazzale Santa
Maria della Misericordia 15,
33100 Udine, Italy3Division o Inectious Diseases,
San Martino Hospital and University
o Genoa, Genoa, Italy4Department o Surgical Sciences andIntegrated Diagnostics, University o
Genoa, Genoa, Italy
*Author or correspondence:
Tel.: +39 432 559355
Fax: +39 432 559360
Ventilator-associated pneumonia (VAP) is the most requent inection among patientshospitalized in intensive care units, maintaining a high morbidity and mortality. The globalincidence o VAP ranges rom 8 to 28%. Early-onset VAP is mainly caused by communitypathogens with a avorable pattern o antibiotic sensitivity, whereas late-onset VAP is otencaused by multidrug-resistant pathogens, mainly methicillin-resistant Staphylococcus aureus,Pseudomonas aeruginosa and Acinetobacter spp. and enteric Gram-negative bacilli. Thediagnosis o VAP remains dicult to conrm, lacking both microbiological analysis andradiological signs o high specicity. The Clinical Inection Pulmonary Score has been proposedto overcome the diculties related to the diagnosis, but is not applicable to all patientcategories. A continuous evaluation o the antimicrobial therapeutic options, along with theirpharmacodynamic and pharmacokinetic proles, is mandatory to create therapeutic protocolsand reduce VAP-related mortality.
Management o ventilator-
associated pneumonia:epidemiology, diagnosisand antimicrobial therapyExpert Rev. Anti Inect. Ther. 10(5), 585596 (2012)
Keywords:Acinetobacter baumannii Clinical Infection Pulmonary Score Enterobacteriaceae intensive care unit
multidrug-resistant pathogens Staphylococcus aureus ventilator-associated pneumonia
-
7/28/2019 Share01.pdf
2/12
Expert Rev. Anti Inect. Ther. 10(5), (2012)586
Review
Moreover, among 215 ICU patients with microbiologicallyconrmed VAP, the presence o chronic obstructive pulmo-nary disease (COPD), increased Simplied Acute PhysiologyScore II (SAPS II) and shock at the day o VAP diagnosis wereound as independent risk actor or mortality[11]. Conversely,
mortality in trauma patients seems to be lower than in otherpatients, according to the data o a prospective observationalstudy conducted in 27 ICUs in Europe, probably because odierent demographic characteristics and etiology [12]. Owingto concerns regarding the high morbidity and mortality, andthe spread o MDR, current knowledge and recent advances inthe eld o epidemiology, pathogenesis and management o VAPwill be discussed, along with a description o epidemiologic andetiologic patterns.
Epidemiology
The incidence o VAP has ranged rom 8 to 28% in dierent
retrospective and prospective analyses[13]
. Regarding early-onsetVAP, ew data are available. A perspective surveillance study hasbeen perormed over a period o 9 years (20012009) among11 French hospitals to estimate the incidence o VAP within 48 ho ICU admission. It ound an incidence o early-onset VAP o8.3 per 1000 invasive MV days (95% CI: 6.111.1), while theglobal incidence o VAP was 20.6 per 1000 invasive MV days(95% CI: 18.622.8) [14].
The International Nosocomial Inection Control Consortium(INICC) involved 422 ICUs and reported a pooled rate o VAPo 15.8 cases per 1000 ventilator days, with the highest ratesreported in trauma ICUs (40 cases per 1000 ventilator days) [15].
On the other hand, among 1500 US hospitals, the NationalHealthcare Saety Network (NHSN) reported minor rates oVAP (three cases per 1000 ventilator days), with highest ratesin trauma (eight cases per 1000 ventilator days) and burn(10.7 cases per 1000 ventilator days) ICUs [4].
However, a comparison o INICC and NHSN is dicult tomake. Refecting the lack o a denitive diagnostic approach,the INICC adopts a denition o VAP based on clinical andradiological ndings, without requiring microbiologic evidenceo inection, whereas microbiologic evidence o a pathogen wasrequired in the NHSN report, leading to a decrease in rates acrossthe dierent US ICUs [16]. Moreover, VAP prevalence seems tobe higher across Europe compared with in the USA (23.5 cases
per 1000 ventilator days), both among mixed populations andspecic ICU subtypes [17]. This variability in prevalence and inci-dence rates underscored the need or uniorm diagnostic criteriaor VAP to correctly interpret the dierent local epidemiologicalreports in a global perspective [16].
Etiology & MDR
As previously reported, early-onset VAP is mainly caused bycommunity pathogens with a avorable pattern o antibiotic sensi-tivity (S. pneumoniae, H. inuenzaeand anaerobes o the oral cav-ity), whereas late-onset VAP is oten caused by MDR pathogens,mainly methicillin-resistant S. aureus(MRSA), P. aeruginosaand
Acinetobacterspp. and enteric extended-spectrum b-lactamase
(ESBL)-producing Gram-negative bacilli [18,19]. Coagulase-negative staphylococci and various other organisms includinganaerobic bacteria, ungi, Corynebacterium species, Moraxellaspecies and enterococci represent rare pathogens. Overall, datarom the NHSN reported that the most common pathogens iso-
lated rom patients with VAP were S. aureus(24%), P. aeruginosa(16%), Enterobacterspp. and A. baumannii (8%) [20]. Among356 ICU patients with microbiologically documented VAP inEurope, Enterobacteriaceae, S. aureusand P. aeruginosa rep-resented the most requent isolated pathogens (43, 33 and23%, respectively) [21]. All o these pathogens refected thephenomenon o growing resistance resumed with the wordESCAPE, containing the initials o the most requent MDRmicroorganisms (Enterococcus aecium, S. aureus, Clostridiumdifcile, A. baumanniiand Enterobacteriaceae) [22]. O note,prior use o antimicrobials and hospitalization within the past90 days are risk actors particularly associated with the develop-
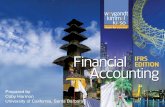
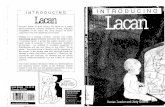
ment o MDR organisms and MDR has a signicant impact onmortality, length o and costs related to hospitalization [23,24].Growing rates o resistance o MDR Gram-negative bacteriahave been reported in the USA (Figure 1) [25]. The last annualreport o the European Antimicrobial Resistance SurveillanceNetwork (EARS-Net) showed a signicant increase in preva-lence o resistance strains among Enterobacteriaceae [26]. Forexample, among 10,952 Klebsiella pneumoniaeisolates tested orthird-generation cephalosporins, fuoroquinolones and amino-glycosides, 35% o isolates were resistant to one or more o thethree considered antibiotic classes [26]. Among nonermentingGram-negative bacteria in Europe, MDR is also a concern.Among 8376 P. aeruginosa isolates tested or at least threeantibiotic classes among piperacillin/tazobactam, cetazidime,fuoroquinolones, aminoglycosides and carbapenems, 33% wereresistant to one or more o the ve considered antibiotic classes,while 16% were resistant to three or more [26]. EARS-Net alsoreported S. aureusresistance rates to methicillin and riampin,as outlined in Figure 2[26].
MDR Gram-negative bacteria
MDR Gram-negative bacteria are especially common andproblematic in some ICUs and they have developed numerousmechanisms o drug resistance against available antimicrobials,includingb-lactamases, efux pumps, porin mutations and bind-
ing site mutations [27]. In particular, b-lactamase-mediated resis-tance is a concern. The appearance o ESBLs and the diusiono AmpC cephalosporinases now compromise the use o third-generation cephalosporins [28]. Moreover, b-lactamases suchIMP, VIM, K. pneumoniaecarbapenemases (KPC) and OXA areincreasingly seen in Gram-negative isolates, and are capable oconerring resistance to carbapenems and lead to the insurgenceo VAP caused by MDR pathogens susceptible only to colistin[29]. Nevertheless, Gram-negative bacteria, especially noner-menters, may even lose their susceptibility to colistin as a result othe combination o di erent resistance mechanisms, such as theouter membrane porin OprD, the AmpC cephalosporinase and a
multitude o efux pumps [30]. For example, the MYSTIC study
Bassetti, Taramasso, Giacobbe & Pelosi
-
7/28/2019 Share01.pdf
3/12
www.expert-reviews.com 587
Review
reported that 12% oP. aeruginosastrains isolated in ICUs areMDR, dened as resistance to at least ciprofoxacin, cetazidimeand gentamicin [31]. Moreover, P. aeruginosatrends toward piper-acillin/tazobactam resistance were noted between 19971999and 20002007 worldwide, with only polymyxins capable o
providing an overall coverage 90% [32].
MRSA
Inections due to Gram-positive bacteria are one o the leadingcauses o morbidity and mortality in ICUs, and MRSA repre-sents a major problem [33]. Resistance is conerred by an addi-tional penicillin-binding protein (PBP2a), encoded by mecA,leading to an intrinsic resistance to all b-lactams and theirderivatives [34]. Although methicillin resistance is associatedwith mortality among patients with VAP caused byS. aureus,this association might not be causal, but is probably due toconounders, such as the adequacy o empirical treatment and
severity o illness[35]
.Moreover, among 30 MRSA isolates, vancomycin ecacy wasdecreased when the isolates MICs were >1 g/ml, compared withthe ecacy in isolates with MICs to vancomycin 32 g/ml denes vancomycin-resistant S. aureus(VRSA) [37]. However, when MRSA MICs to vancomycin are atthe high end o the susceptibility range, vancomycin is alreadyless eective and patients may have a higher likelihood orecurrence and a longer length o stay in hospital [38,39] .
There are some reports o S. aureus and Staphylococcusepidermidiswith documented genetic resistance to linezolid,which is a synthetic oxazolidinone that shows excellent penetra-tion into the epithelial lining fuid [40,41]. The potential clinicalsuperiority o linezolid compared with vancomycin in MRSApneumonia will be discussed later.
The clinical impact o resistance to the lipopeptide dapto-mycin is not o particular concern. However, daptomycin isnot suitable or the treatment o VAP because o suractantinactivation [42].
Diagnosis o VAP in mechanically ventilated critically ill
patientsThe diagnosis o VAP is generally based on clinical maniesta-
tions and symptoms; inltrates at chest radiograph; laboratoryinvestigations; and microbiological ndings. However, it is alsoimportant to identiy methods to identiy VAP early, and toguide clinical management and treatment.
Individual clinical variables approach
The clinical maniestations and symptoms o VAP (i.e., ever,shortness o breath, chest pain, cough, sputum production,hypoxia and leukocytosis) are nonspecic with no pathogno-monic signs. A chest radiograph to conrm the presence o apulmonary inltrate may not provide denitive conrmation oVAP. Additionally, there is no specic pulmonary radiographic
pattern that is unique to a particular microorganism. Laboratory
investigations are not predictive o specic symptoms associ-ated with VAP. The presence o microorganisms in a respira-tory sample with or without a pulmonary inltrate on a chestradiograph has low specicity or the diagnosis o VAP. In act,it might merely represent colonization or tracheobronchitis andnot pulmonary inection. Furthermore, the timing o the clinicalpresentation is also important, varying rom an illness o abruptto gradual onset, associated with less or more severe sepsis andseptic shock. Thus, clinical maniestations, chest radiographicpattern and laboratory investigations can be mimicked in otherpathologies such as congestive heart ailure, pulmonary emboli,pulmonary hemorrhage and acute lung injury/acute respiratorydistress syndrome. Presentation may be dierent in time andseverity. The early recognition o VAP, timing and severity isessential to ensure the initiation o an appropriate diagnosticand therapeutic approach.
In conclusion, the evaluation o individual clinical variables,such as ever, shortness o breath, chest pain, cough, sputumproduction, hypoxia and leukocytosis, or chest radiograph is nothelpul in the diagnosis o VAP.
Figure 1. Proportion o multidrug-resistant pathogensamong Gram-negative bacteria in the USA. Multidrugresistance was dened as resistance to one or more testedantimicrobials in three or more antimicrobial classes [25].
0
Acinetobacter baumannii
Proportion resistant (%)
2008
2004
2000
Pseudomonas aeruginosa
Escherichia coli/Klebsiella pneumoniae
20 40 60 80
Figure 2. Staphylococcus aureus resistance rates in Europein 2010.Data taken rom [26].
0
UK
Germany
France
Italy
10 20 30 40
Methicillin
Rifampin
Proportion resistant (%)
Ventilator-associated pneumonia: epidemiology, diagnosis & antimicrobial therapy
-
7/28/2019 Share01.pdf
4/12
Expert Rev. Anti Inect. Ther. 10(5), (2012)588
Review
Combined clinical variables approachAnother approach is to consider and evaluate clinical maniesta-tions, chest radiographic patterns and laboratory investigationsin combination. The conventional diagnosis o VAP is classical lycharacterized by the presence o[43,44]:
Clinical criteria: one, two or three o the ollowing: core tem-perature >38.3 or 10,000 mm-3) orleukopenia (24 h) or progressiveinltrate at chest radiograph;
Microbiologic criteria: positive quantitative culture o a sampleobtained by bronchoalveolar lavage (BAL; 104 cu/ml) orprotected-specimen brush (PSB; 103 cu/ml); positive bloodculture unrelated to another source and obtained 48 h beoreand ater respiratory sampling; and positive pleural fuidculture in absence o previous pleural instrumentation.
More recently, another denition has been proposed to deter-mine the clinical screening o hospital acquired pneumonia andVAP [45]: the presence o new chest x-ray inltrates plus one o thethree clinical variables: ever 38C, leukocytosis or leukopenia,and purulent secretions. In acute lung injury/acute respiratorydistress syndrome and or those who it is dicult to demonstratea deterioration o radiological images, at least one o ever38C,leukocytosis or leukopenia, and purulent secretions may suceto warrant initial screening. The presence o new chest x-rayinltrates plus at least two o the three clinical variables (ever38C, leukocytosis or leukopenia, and purulent secretions) isaccurate enough to start antimicrobial treatment and cultures.However, both individually considered or combined with theclinical and laboratory variables, chest radiograph does not seemsto reach an acceptable sensitivity and specicity, when comparedwith post-mortem lung biopsies [46].
Clinical Inection Pulmonary ScoreTo improve the sensitivity and specicity o VAP diagnosis, ithas been proposed to combine and score the individual values,generating the Clinical Inection Pulmonary Score (CPIS) [47].The CPIS is obtained rom: clinical maniestations and symp-toms; inltrates at chest radiograph; laboratory investigations;
and microbiological ndings (Table 1). Dierent modications oCPIS have been suggested. In the original and modied CPIS,in addition to the variables reported above, the level o oxygen-ation has been included, while the semiquantitative culture otracheal aspirate is not considered mandatory[48]. In the original
paper rom Pugin et al. it was reported that in a limited numbero mechanically ventilated patients with dierent diseases, aCPIS equal to or higher than 6 out o a maximum o 12 wascorrelated with high bacterial counts isolated rom the lowerrespiratory tract and able to predict pulmonary inection with ahigh specicity and sensitivity o 93 and 100%, respectively[47].
Successively, Fartoukh et al. ound that clinical predictionalone was inaccurate, but a modied CPIS, incorporating aGram stain o respiratory tract secretions, improved diagnosticaccuracy[49]. The diagnostic accuracy was enhanced and thelikelihood ratio or pneumonia based on a score greater than 6increased rom a baseline o 1.46 (using the CPIS) to 1.67 i a
Gram stain o blind protected samples was obtained and to 1.77i a Gram sta in o a directed sample was obtained. Nonetheless,the authors cautioned that urther renement o the clinicalscoring approach was necessary to improve the diagnosticaccuracy in patients suspected o having VAP. In a large rangeo studies, including a dishomogeneous population o patientsmechanically ventilated and recovered in an ICU, CPIS doesnot appear to be suciently accurate compared with a BALfuid-established diagnosis with a sensitivity between 30 and89% and specicity between 17 and 80% [4956].
The major limitations about the appropriate evaluation oCPIS in the diagnosis o VAP are related to: the dishomogeneouspopulation o patients investigated; the limitation o BAL todiagnose VAP with high sensitivity and specicity; the dier-ent threshold o CPIS to diagnose VAP; and the interobservervariability to calculate CPIS.
We believe that to improve and optimize the ecacy o CPISto diagnose VAP it is important to take into account the clinicalcondition o the patient, the underlying disease and the alterationat chest radiograph. It is evident that in a previous disease condi-tion markedly aecting the temperature, leukocytes, trachealsecretions and oxygenation, as well as chest radiograph, the roleo CPIS to diagnose VAP is markedly aected. Thus, we believethat CPIS might have a more relevant role in clinical conditions
Table 1. Clinical Pulmonary Inection Score chart.
Diagnostic eature 0 1 2
Tracheal secretions Rare Abundant Abundant and purulent
Chest x-ray inltrate None Diuse Localized
Temperature (C) 36.5 and 38.4 38.5 and 38.9 39.0 or 36.5
White blood cells (109/l) 4.0 and 11.0 11.0 11.0 plus band orms 0.5
PaO2/FiO
2mmHg >240 or ARDS
-
7/28/2019 Share01.pdf
5/12
www.expert-reviews.com 589
Review
in which these parameters are minimallyaected at ICU entry. A specic popula-tion o patients could show these charac-teristics, such as brain trauma or braininjury patients. In act, Pelosi et al. demon-
strated that CPIS could predict VAP withhigh sensitivity and specicity early on ina selected population o patients sueringrom brain injury[57]. Nonetheless, thesending cannot be directly transerred to amore dishomogeneous group o patients.
The most common method to diagnoseVAP is the quantitative analysis o theBAL, as discussed below. However, it hasbeen clearly demonstrated that BAL is notalways so specic and sensitive when com-pared with immediate postmortem pul-
monary biopsy. The consequence o thisis the overall uncertainty o both BAL andCPIS to diagnose VAP [45,56].
Finally, some parameters included inCPIS are subjective and depend on theexperience o the observer [53]. The quan-tication and evaluation o the quality osecretions is not easily perormed at thebedside, and the chest radiograph inter-pretation might show a high intraobservervariability. The level o oxygenation depends on the ventilationsetting used, which is not included in the CPIS. We believe thatto improve the specicity and sensitivity o CPIS to diagnoseVAP in the ICU, a selected population o patients with no majoralteration o parameters included in CPIS at ICU entry shouldbe considered. O course, this dramatically reduces the num-ber o patients in whom CPIS might be relevant. Evaluation osecretions, interpretation o chest radiographs and oxygenationshould be considered in patients with brain injury.
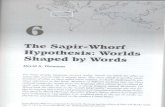
However, although the CPIS seems to play a minor role in thediagnosis o VAP, it should be considered to identiy patients atrisk o VAP and to monitor the adequacy o the antibiotic treat-ment and clinical management. It is our opinion that when theCPIS is higher than or equal to 6, microbiological analysis as wellas appropriate empirical antibiotic treatment should be considered
(Figure 3). Furthermore, it has been clearly demonstrated that theCPIS might have a relevant role in monitoring the evolution oVAP, to predict the outcome early, as well as to guide the durationo the antibiotic treatment [58]. It has been ound that oxygen-ation and temperature are the rst parameters to improve whenadequate treatment has been given to patients aected by VAP [59].In a prospective randomized controlled study it has been shownthat the use o CPIS could be associated with an early withdrawalo the antibiotic treatment, with a marked reduction in associatedcosts [60]. However, these positive ndings were not conrmed inother nonrandomized observational studies [61].
In conclusion, clinical maniestations are usual ly considered to
conrm or diagnose VAP. Chest radiograph may be sensitive but
is oten not specic. CPIS may be helpul tool to conrm VAPand or monitoring antibiotic treatment and clinical evolution.It appears to only be helpul to diagnose VAP in standardizedpopulations o patients, such as those aected by brain traumaand injury. Further studies are required to better identiy the at-bedside role o the CPIS in the clinical management o criticallyill mechanical ly ventilated patients.
Role o bacteriological analysis to diagnose VAPMany studies have evaluated the value o bacteriological data inestablishing the diagnosis o VAP compared with pathological,clinical or other bacteriological criteria. The quantitative analy-sis o the bacteriological data are usually considered the goldstandard in the diagnosis o VAP.
Quantitative cultures might be obtained by dierent methods,
including BAL, protective BAL (pBAL), PSB or tracheal aspirate(TA), which overall appear to be equivalent or the diagnosiso VAP. In general, compared with a pathologically conrmeddiagnosis o VAP, BAL shows a sensitivity between 19 and 83%and specicity between 45 and 100%; PSB shows a sensitivitybetween 36 and 83% and specicity between 50 and 95%; pBALshows a sensitivity between 39 and 80% and specicity between66 and 100%; and TA shows a sensitivity between 44 and 87%and specicity between 31 and 92% [62].
Several actors might aect the sensitivity and specicity oBAL in the diagnosis o VAP: prior antibiotic treatment thatmight considerably decrease the sensitivity o cultures o BAL
samples; the inconsistency o tracheal and alveoli microbiological
Figure 3. Flowchart or using the Clinical Pulmonary Inection Score.CPIS: Clinical Pulmonary Inection Score.
Calculate patients CPIS
Does the CPIS= 6?
Is the CPIS 6 on day 3
Initiate
therapy
No
No
No
Yes
Yes
Yes
Yes
Yes
Recalculate
CPIS daily
Are tracheobronchial
secretions availablefor Gram stain?
Are pus cells and
organisms present?
Ventilator-associated pneumonia: epidemiology, diagnosis & antimicrobial therapy
-
7/28/2019 Share01.pdf
6/12
Expert Rev. Anti Inect. Ther. 10(5), (2012)590
Review
cultures when compared with the pathological samples; and thevariability in di erent sites o sampling o culture in the lung.
Some studies clearly question the reliability o microbiologicalcultures obtained rom the tracheobronchial tree or alveolar sideor the diagnosis o VAP [45,46,49]. In these studies quantitativecultures were obtained through conventional techniques (BAL,pBAL, PSB or TA) and were compared with histological andmicrobiological reerences. Sensitivities or diagnosis o VAPwere extremely low, ranging rom 36 to 91%, with specicitiesranging rom 45 to 92%.
It is common experience that bacteriological cultures requiresome days or the results to be available. For these reasons, alterna-tive methods to better identiy patients at risk o VAP earlier havebeen developed and investigated. One such approach is the analysiso the number o infammatory cells and Gram stains. The pres-ence o over 2% infammatory cells had a sensitivity o 7586%
and a specicity o 7898% in diagnosing VAP. Furthermore,the presence o bacteria in Gram stains o BAL specimens had asensitivity o 4490% and specicity o 49100% in identiyingpatients with VAP. However, it should be remembered that theaccuracy o Gram stains is slightly better or Gram-positive thanGram-negative microorganisms.
In conclusion, bacteriologic data do not increase the accu-racy o diagnosis when compared with clinical diagnosis.Quantitative cultures obtained by dierent methods, includ-ing BAL, pBAL, PSB or TA seem to be roughly equivalentin diagnosing VAP. The rapid availability o cytological data,including infammatory cells and Gram stains, might be helpul
in initial therapeutic decisions in patients with suspected VAP,
but may clearly be infuenced by antibiotic treatment and inect-ing microorganisms.
Biomarkers & VAP diagnosis
In order to improve the sensitivity and specicity o clinicaland microbiological diagnosis o VAP, the laboratory analysis ospecic biomarkers has been proposed and investigated. Severalbiomarkers have been proposed or diagnosing VAP, but ew othem have been ound to be reliable [62].
Among them, the most important are procalcitonin (PCT) andC-reactive protein (CRP). Serum PCT levels had better peror-mance than alveolar PCT concentrations, with a sensitivity anda specicity varying according to the etiology and the severity othe disease. On the other hand, a CRP higher than 10 mg/dl hasbeen reported to be associated with VAP. The major limitationso these parameters is that several actors might increase both
PCT and CRP, minimizing its eciency to detect VAP early[63].Furthermore, they need continuous daily monitoring, which hasa major impact on economic resources, especially in ICUs witha large number o patients.
In conclusion, several biomarkers have been evaluated toimprove the diagnosis o VAP. Among them PCT and CRPappear to be the most promising but with major intrinsic limita-tions. Further studies are warranted to better dene their role inclinical practice taking into account the costs.
Furthermore, another important biomarker is represented bythe detection oAspergillus galactomannan (GM; a cell wallconstituent released during tissue invasion) in BAL luid
(BAL-GM) or diagnosing VAP caused byAspergil lus spp.
Table 2. Pharmacokinetic/pharmacodynamic parameters and usual clinical dosage or agents commonlyused or Gram-negative coverage in ventilator-associated pneumonia.
Drug Usual clinical dosage or VAP PK/PD parameter predictive o breakpointefcacy
b-lactamsPiperacillin/tazobactam 4.5 g q.i.d. or in prolonged (4 h) or continous
inusion
Time > MIC
Cetazidime 2 g t.i.d. or in continous inusion
Ceepime 2 g t.i.d.
Meropenem 12 g t.i.d./q.i.d. in prolonged (3 h) or continuous
inusion
Imipenem 1 g t.i.d.
Doripenem 0.5 g t.i.d.
Aminoglycosides
Gentamycin 7 mg/kg q.d. Cmax
/MIC
Amikacin 15 mg/kg q.d.
Fluoroquinolones
Ciprofoxacin 400 mg t.i.d. AUC/MIC
Levofoxacin 500 mg b.i.d. or 750 mg q.d.
AUC: Area under the curve; b.i.d.: Two times a day; PD: Pharmacodynamic; PK: Pharmacokinetic ; q.d.: Once a day; q.i.d.: Four times a day; t.i.d.: Three times a day;VAP: Ventilator-associated pneumonia.
Bassetti, Taramasso, Giacobbe & Pelosi
-
7/28/2019 Share01.pdf
7/12
www.expert-reviews.com 591
Review
The new ndings that BAL-GM is a valuable test or diagnos-ing invasive pulmonary aspergillosis in apparently immunocom-petent ICU patients set a new and practice-changing standardand one that comes without the requirement or additionalprocedures or novel technologies. All that is needed is to sub-
mit a sample or GM testing rom fuid obtained during BAL,a commonly perormed diagnostic procedure or VAP [64].
Antimicrobial treatment o VAP
The treatment o VAP remains a dicult and complex chal-lenge infuenced by various actors, or example the requentabsence o denitive diagnosis o VAP and the presence o MDRpathogens [2,65].
Two principles guide the strategy o antibiotic therapy orVAP. The rst is the initial administration o appropriate anti-biotics potentially active on causative pathogens, whereas thesecond is the shortening o inappropriate therapy. The strategy
o de-escalation attempts to uniy these two principles withina single strategy, optimizing patient outcome and minimiz-ing the emergence o antibiotic resistance at the same time. Inaddition to these principles it is necessary to ensure that theadministration o antibiotics satises certain requirements, suchas the appropriate dose and dosing intervals, the optimal dura-tion o treatment and the monitoring o drug levels and druginteractions. The lack o adherence tothese minimal requirements can result inreduced or excessive tissue concentrationo the drugs and lead, respectively, to theoccurrence o antibiotic resistance and lacko therapeutic ecacy or to toxicity despitea qualitatively correct treatment.
When VAP is suspected, the initial treat-ment regimen is oten chosen without theidentication o the responsible pathogen.However, the epidemiology may changein dierent hospitals and even in ICUswithin the same hospital. Knowledge othe bacteria primarily associated with VAPin the dierent local realities can helpin the selection o the correct empiricaltreatment regimen [66,67].
A guideline-based approach based on
local antibiotic susceptibility patterns canreduce the overall use o antibiotics, theselective pressure or MDR bacteria andthe outcome o VAP [68,69]. The treatmentmust be initiated as soon as possible, beingthe outcome strictly related to the delayo administration o active antimicrobialdrugs. Thereore, an empirical treatment isrecommended when VAP is clinically sus-pected and the de-escalation o the chosenregimen has to be made when microbiologi-cal data become available [70,71]. However,
although de-escalation therapy appears to
correlate with lower mortality, it is not applicable to the casesin which the etiological diagnosis o pneumonia is not reachedbecause o dierent actors, such as inadequate sampling, cortico-steroid therapy, initiation o antimicrobial drugs beore samplingor the presence o dicult-to-isolate strains [7274].
Except or the treatment o nonermenting Gram-negativebacteria such as P. aeruginosaand A. baumannii, the durationo the empiric therapy may be shortened in patients with a goodclinical response, rom the traditional 1421 days to 8 days odrug administration [75,76] . In order to shorter the duration oantibiotic treatment, PCT-guided antibiotic therapy in patientswith respiratory tract inections appea rs to reduce antibioticuse without aecting overall mortality or length o stay in thehospital [77]. Moreover, a short, as opposed to long, course oantibiotics did not adversely aect mortality, length o ICU stayor recurrence rates o patients with VAP [78]. A correct antibioticadministration must take account o drug pharmacokinetic
prole. A single daily dose regimen is appropriate or amino-glycosides and fuoriquinolones (concentration dependent),while more requent administrations o lower doses are appro-priate or b-lactams and other time-dependent antimicrobial,in order to obtain adequate values o the area under the curveabove the MIC or the dierent antibiotics (Table 2) . The lungpenetration o the dierent drugs is another pharmacokinetic
Box 1. American Thoracic Society initial empiric therapy orhospital-acquired pneumonia, ventilator-associated pneumonia andhealthcare-associated pneumonia in patients with late-onset diseaseor risk actors or multidrug-resistant pathogens and all disease
severity.
Potential pathogens
Streptococcus pneumonia, Haemophilus infuenzae, methicillin-sensitiveStaphylococcus aureus, antibiotic-sensitive enteric Gram-negative bacilli (Escherichiacoli, Klebsiella pneumoniae, Enterobaterspp., Proteus spp., Serratia Marcescens),MDR pathogens (Pseudomonas aeruginosa, K. pneumoniae ESBL+,Acinetobacterspp.), Legionella pneumophila and methicillin-resistant S. aureus
Combination antibiotic therapy
Antipseudomonal cephalosporin (ceepime, cetazidime)
or
Antipseudomonal carbapenem (imipenem, meropenem)
or
b-lactam/b-lactamase inhibitor (piperacillintazobactam)plus
Antipseudomonal fuoroquinolone (ciprofoxacin, levofoxacin)
or
Aminoglycoside (amikacin, gentamicin, tobramycin)
plus
Linezolid or vancomycinI an ESBL- strain, such as Klebsiella pneumoniae, or anAcinetobacterspecies is suspected a carbapenem isa reliable choice.I Legionella pneumophila is suspected, the combination antibiotic regimen should include a macrolide(e.g., azithromycin) or a fuoroquinolone (e.g., ciprofoxacin or levofoxacin) should be used rather than anaminoglycoside.I methicillin-resistant Staphylococcus aureus risk actors are present or there is a high incidence locally.ESBL: Extended-spectrum b-lactamase; MDR: Multidrug resistant.
Data taken rom [81].
Ventilator-associated pneumonia: epidemiology, diagnosis & antimicrobial therapy
-
7/28/2019 Share01.pdf
8/12
Expert Rev. Anti Inect. Ther. 10(5), (2012)592
Review
actor to consider. For example, higher vancomycin serumconcentrations may be necessary to achieve appropriate lungconcentrations to optimize treatment outcomes in VAP causedby MRSA, whereas linezolid demonstrates adequate penetra-tion into lung and other sot tissues with sustained concentra-
tions above the MIC or MRSA, or the majority o the dosinginterval [79]. Moreover, pharmacokinetics are infuenced by thealtered physiology (presence o multiple organ impairment) andassociated pharmacology in the critically ill patient undergoingMV. With some limitations, the application o sotware suchas Monte Carlo simulation may provide the doses and inu-sion duration that should be used to treat critically ill patients[80]. The initial empiric therapy recommended by the AmericanThoracic Society or the treatment o VAP should be based onthe presence or absence o risk actors or MDR pathogens, suchas prolonged hospitalization (5 days or more), admission rom ahealthcare-related acility and recent antibiotic therapy[81]. The
ATS principles or healthcare-associated pneumonia and VAPare outlined in box 1. A recent published paper that aimed toimprove compliance with these guidelines and assess outcomeshas demonstrated that the adherence to empirical recommendedtreatment was associated with increased mortality[82].
However, as discussed earlier, MDR may lead to a reduction insusceptibility and also to a guideline-based therapy, so cliniciansare orced to use new drugs that have been recently marketedor a combination o already known antimicrobial agents, try-ing to overcome resistance especially among Gram-negativebacteria, where colistin oten remains the only therapeuticoption available with one study showing a synergistic activ-ity with riampin [83]. The use o tigecycline, although activeagainst MDRAcinetobacter spp., is questioned because o itsbacteriostatic mechanism and low concentrations in serum and
epithelial lining fuid, with high mortality reported amongtigecycline-treated patients with VAP and bacteremia[84].
Regarding hospital-acquired pneumonia caused byGram-positive pathogens such as MRSA, both telavancin andlinezolid result in signicantly greater clinical cure rates com-
pared with vancomycin [8588]. In the Phase III noninerioritystudy, a subgroup analysis revealed that patients with VAP exhib-ited a trend toward higher clinical cure rates with telavancin rela-tive to vancomycin [85]. The European Medical Agency (EMA)has recently approved telavancin or the treatment o adults withhospital-acquired pneumonia, including VAP, known or sus-pected to be caused by MRSA, but only when other treatments(e.g., other antibiotics) are not suitable because o the increasedrisk o renal toxicity o telavancin compared with vancomycin.Also, the data o the recently completed and published Zephyrtrial suggested a clinical superiority o linezolid compared withvancomycin, with higher rates o successul clinical response,
acceptable saety and tolerability prole or the treatment oproven MRSA nosocomial pneumonia. Microbiologic responsesparalleled clinical outcomes, and MRSA clearance was 30%greater with linezolid than with vancomycin. A di erence o atleast 20% persisted until late ollow-up, suggesting that linezolidtreatment may result in more complete bacterial eradication [89].The higher rate o nephrotoxicity with vancomycin may par-tially refect the use o adjusted vancomycin doses in this trial,as recommended by current clinical guidelines [90]. A higherincidence o renal injury was seen in patients with vancomycintrough levels >20 g/ml on day 3, as previously reported [91].
Conclusion
In conclusion, an eective antimicrobial therapy and the appro-priate use o supportive measures remain essential in the treat-
ment o VAP (Figure 4). However, because othe progressive reduction o bacterial sus-ceptibility to currently used antimicrobialsin ICUs and the high mortality related toVAP caused by MDR strains, a continu-ous evaluation o the therapeutic options,along with their pharmacodynamic andpharmacokinetic proles, is mandatoryto create better therapeutic protocols andreduce VAP-related mortality.
Expert commentary & fve-yearview
VAP still remains the most requent inec-tion among patients hospitalized in ICUsand is associated with high economiccosts and mortality, especially when lunginection is caused by high-risk pathogens,such as MRSA, ESBL-producing Gram-negative bacteria, and MDRP. aeruginosaand A. baumannii . The paucity o cur-rently used agents active against these
MDR strains underlines the importance
Figure 4. Empiric antibiotic therapy in patients with ventilator-associatedpneumonia and the risk actors indicated in the box.
Late onset (>5 days)Antibiotics in preceding 90 days
>5 days of hospitalizationImmunosuppressed
Long-term care facility residentChronic hemodialysis
Amikacin or
levofloxacin orciprofloxacin(if resistance rate inPseudomonas
aeruginosa isolateswithin the hospital
-
7/28/2019 Share01.pdf
9/12
www.expert-reviews.com 593
Review
o antimicrobial development. However, ew new antibioticshave been advanced into clinical practice or the treatment omost o the MDR pathogens, especially Gram-negative bacteria.Thereore, containing the spread o these resistant pathogensremains crucial and an optimized prescription o suitable anti-
biotics is mandatory. Moreover, the diagnosis o VAP in theseverely ill patients remains a clinical d ilemma. In the presenceo a previous disease condition markedly aecting the tempera-ture, leukocytes, tracheal secretions and oxygenation, as wellas chest radiograph, the role o CPIS to diagnose VAP remainsuncertain. CPIS might be useul when these parameters areminimally aected at ICU entry, such as in trauma or braininjury patients, but not in a more dishomogeneus population.CPIS might be an important tool to predict outcomes earlier aswell as to guide the duration o antibiotic treatment, but urtherstudies are required to better identiy the role o CPIS in theclinical management o critically ill mechanically ventilated
patients. Furthermore, regarding diagnosis diculties, bacterio-logical data do not increase the accuracy o diagnosis when com-pared with clinical diagnosis. Quantitative cultures obtained bydierent methods, including BAL, pBAL, PSB or TBA seemto be roughly equivalent or the diagnosis o VAP. The rapidavailability o cytological data, including infammatory cellsand Gram stains, might be helpul in initial therapeutic deci-sions in patients with suspected VAP, although they are clearlyinfuenced by antibiotic treatment and inecting microorgan-ism. Several biomarkers have also been evaluated to improve thediagnosis o VAP. Among them, PCT and CRP appear to bethe most promising but with major intrinsic limitations, suchas the presence o several actors that might increase both PCTand CRP, minimizing their eciency or the early detection o
VAP. Further studies are warranted to better dene the role oPCT and CRP in clinical practice taking into account the costs.The antimicrobial treatment o VAP remains a dicult andcomplex challenge infuenced by various actors, or examplethe requent absence o denitive diagnosis o VAP and the pres-
ence o MDR pathogens. When VAP is suspected, the initialtreatment regimen is oten chosen without the identicationo the responsible pathogen. However, the epidemiology maychange in dierent hospitals and even in ICUs within the samehospital. Knowledge o the bacteria primarily associated withVAP in the dierent local realities can help in the selection othe correct empirical treatment regimen.
In conclusion, because o the progressive reduction obacterial susceptibility to currently used antimicrobials andthe high mortality related to VAP caused by MDR strains, acontinuous evaluation o the therapeutic options, along withtheir pharmacodynamic and pharmacokinetic proiles, is
mandatory.
Financial & competing interests disclosure
M Basset ti serves on scientifc advisory boards or Pfzer, Inc., Merck
Serono, Novartis, Shionogi and Co., Ltd, and Astella s Pharma, Inc.; and
has received unding or travel or speaker honoraria rom Pfzer, Inc.,
Merck Serono, Novartis , GlaxoSmithKline, Gil ead Sciences , Inc., Sanof-
Aventis, Cephalon , Inc., Bayer Schering Pharma, Janssen and Astellas
Pharma, Inc. The authors have no other relevant afliations or fnancial
involvement with any organization or entity with a fnancial interest in
or fnancial conict with the subject matter or materials discussed in the
manuscript apart rom those disclosed.
No writing assistance was utilized in the production o this
manuscript.
Key issues
Ventilator-associated pneumonia (VAP) has a great impact on morbidity, occurring at an estimated rate o 13% per day o mechanical
ventilation, with a 927% incidence among all intubated patients.
VAP can be divided in early-onset VAP occurring within 45 days ater intubation and mainly caused by community pathogens
with a avorable pattern o antibiotic sensitivity, and late-onset VAP, oten caused by multidrug-resistant (MDR) pathogens
(e.g., Staphylococcus aureus, Pseudomonas aeruginosa, Enterobacterobacteriaceae andAcinetobacter baumannii).
Although methicillin resistance is associated with mortality among patients with VAP due to S. aureus, this association might not becausal, but probably due to conounders, such as the adequacy o empirical treatment and severity o illness.
The clinical maniestations and symptoms o VAP are nonspecic and no pathognomonic signs are present.
To improve the sensitivity and specicity o VAP diagnosis, it has been proposed to combine and score the individual values, generatingthe Clinical Inection Pulmonary Score (CPIS).
It is our opinion that when the CPIS is greater than or equal to 6, microbiological analysis as well as appropriate empiric antibiotic
treatment should be considered.
The quantitative analysis o the bacteriological data are usually considered the gold standard in the diagnosis o VAP.
Several biomarkers have been evaluated to improve the diagnosis o VAP, among them procalcitonin and C-reactive protein appear to
be the most promising but with major intrinsic limitations.
Two principles guide the strategy o antibiotic therapy or VAP. The rst is the initial administration o appropriate antibiotics, potentially
active on causative pathogens, whereas the second is the shortening o inappropriate therapy.
A guideline-based approach based on local antibiotic susceptibility patterns can reduce the overall use o antibiotics, the selective
pressure or MDR bacteria and the outcome o VAP.
Regarding VAP caused by Gram-positive pathogens such as methicillin-resistant S. aureus, both telavancin and linezolid result insignicantly greater clinical cure rates compared with vancomycin.
Ventilator-associated pneumonia: epidemiology, diagnosis & antimicrobial therapy
-
7/28/2019 Share01.pdf
10/12
Expert Rev. Anti Inect. Ther. 10(5), (2012)594
Review
ReerencesPapers o special note have been highlighted as:ofinterest
1 Davis KA. Ventilator-associatedpneumonia: a review.J. Intensive Care Med.21(4), 211226 (2006).
2 Chastre J, Fagon JY. Ventilator-associatedpneumonia.Am. J. Respir. Crit. Care Med.165(7), 867903 (2002).
3 Lisboa T, Rello J. Diagnosis o ventilator-associated pneumonia: is there a goldstandard and a simple approach?Curr. Opin. Inect. Dis. 21(2), 174178(2008).
4 Dudeck MA, Horan TC, Peterson KD et al.National Healthcare Saety Network(NHSN) Report, data summary or 2010,device-associated module.Am. J. Inect.Control. 39, 798816 (2011).
5 Rello J, Ollendor DA, Oster G et al.Epidemiology and outcomes o ventilator-associated pneumonia in a large USdatabase. Chest122(6), 21152121 (2002).
Largeretrospectivematchedcohortstudy,
demonstratingthatventilator-associated
pneumoniaisacommonnosocomial
infectionassociatedwithpoorclinicaland
economicoutcomes.
6 Giard M, Lepape A, Allaouchiche B et al.Early- and late-onset ventilator-associatedpneumonia acquired in the intensive careunit: comparison o risk actors.J. Crit.Care. 23(1), 2733 (2008).
7 Shorr AF, Zilberberg MD, Kolle M.Costeectiveness analysis o a silver-coatedendotracheal tube to reduce the incidence oventilator-associated pneumonia. Inect.Control. Hosp. Epidemiol. 30(8), 759763(2009).
8 Melsen WG, Rovers MM, BontenMJ. Ventilator-associated pneumonia andmortality: a systematic review oobservational studies. Crit. Care Med.37(10), 27092718 (2009).
9 Bekaert M, Timsit JF, Vansteelandt S et al.
Attributable mortal ity o ventilatorassociated pneumonia: a reappraisal usingcausal analysis.Am. J. Respir. Crit. CareMed. 184(10), 11331139 (2011).
10 Agraotis M, Siempos II, Ntaidou TK,Falagas ME. Attributable mortality oventilator-associated pneumonia: ameta-analysis. Int. J. Tuberc. Lung Dis.15(9), 11541163 (2011).
11 Makris D, Desrousseaux B, Zakynthinos E,Durocher A, Nseir S. The impact o COPDon ICU mortality in patients withventilator-associated pneumonia. Respir.
Med. 105(7), 10221029 (2011).
12 Magret M, Amaya-Villar R, Garnacho Jet al. Ventilator-associated pneumonia intrauma patients is associated with lowermortality: results rom EU-VAP study.J. Trauma69(4), 849854 (2010).
13 Klompas M, Platt R. Ventilator-associated
pneumonia the wrong quality measureor benchmarking.Ann. Intern . Med. 147(11), 803 805 (2007).
14 Vanhems P, Benet T, Voirin N et al.Early-onset ventilator-associatedpneumonia incidence in intensive careunits: a surveillance-based study. BMCInect. Dis. 11(1), 236 (2011).
15 Rosenthal VD, Bijie H, Maki DG et al.International Nosocomial InectionControl Consortium (INICC) Report,data summary o 36 countries, or20042009.Am. J. Inect. Control .
doi:10.1016/j.ajic.2009.12.004 (2011)(Epub ahead o print).
16 Shorr AF, Chan CM, Zilberberg MD.Diagnostic and epidemiology inventilator-associated pneumonia. Ther.Adv. Respir. Dis. 5(2), 121130 (2011).
17 Bouadma L, Mourvillier B, Deiler et al. Amultiaceted program to preventventilator-associated pneumoniae. Crit.Care Med. 38(3), 789796 (2010).
18 Giard M, Lepape A, Allaouchiche B et al.Early- and late-onset ventilator-associatepneumonia acquired in the intensive care
unit: comparison o risk actors.J. Crit.Care. 23(1), 2733 (2008).
19 Joseph NM, Sistl a S, Dutta TK, BadheAS, Parija SC. Ventilator-associatedpneumonia: a review. Eur. J. Intern. Med.21(5), 360368 (2010).
Reviewsvariousaspectsofventilator-
associatedpneumonia,withemphasison
therecentadvances.
20 Hidron AI, Edwards JR, Patel J et al.NHSN annual update: antimicrobial-resistant pathogens associated withhealthcare-associated inections: annual
summary o data reported to the NationalHealthcare Saety Network at the Centersor Disease Control and Prevention,20062007. Inect. Control. Hosp.Epidemiol. 29(11), 9961011 (2008).
21 Koulenti D, Lisboa T, Brun-Buisson Cet al. Spectrum o practice in thediagnosis o nosocomial pneumonia inpatients requiring mechanical ventilation inEuropean intensive care units. Crit. CareMed. 37(8), 23602368 (2009).
22 Peterson LR. Bad bugs, no drugs: noESCAPE revisited. Clin. Inect. Dis. 49(6),992993 (2009).
23 Giske CG, Monnet DL, Cars O, CarmeliY. Clinical and economic impact ocommon multidrug-resistant Gram-negative bacilli.Antimicrob. AgentsChemother. 52(3), 813821 (2008).
24 Depuydt PO, Vandijck DM, Bekaert MA
et al. Determinants and impact omultidrug antibiotic resistance inpathogens causing ventilator-associated-pneumonia. Crit. Care12(6), R142 (2008).
25 Kallen AJ, Srinivasan A. Currentepidemiology o multidrug resistanGram-negative bacilli in the United States.Inect. Control. Hosp. Epidemiol.31(Suppl. 1), S51S54 (2010).
26 European Centre or Disease Preventionand Control. Antimicrobial resistancesurveillance in Europe 2009. AnnualReport o the European Antimicrobial
Resistance Surveillance Network(EARS-Net). European Centre or DiseasePrevention and Control, Stockholm,Sweden (2010).
27 Maragakis LL. Recognition and preventiono multidrug-resistant Gram-negativebacteria in the intensive care unit. Crit.Care Med. 38(Suppl. 8), S345S351(2010).
28 Peier Y, Cullik A, Witte W. Resistance tocephalosporins and carbapenems inGram-negative bacterial pathogen. Int.J. Med. Microbiol. 300(6), 371379 (2010).
29 Walsh TR. Emerging ca rbapenemases: aglobal perspective. Int. J.Antimicrob.Agents36(Suppl. 3), S8S14 (2010).
30 Lister PD, Wolter DJ, Hanson ND.Antibacteria l-resistant Pseudomonasaeruginosa: clinical impact and complexregulation o chromosomally encodedresistance mechanisms. Clin. Microbiol.Rev. 22(4), 582610 (2009).
31 Goossens H. Susceptibility omulti-drug-resistant Pseudomonasaeruginosain intensive care units: resultsrom the European MYSTIC study group.Clin. Microbiol. Inect. 9(9), 980983
(2003).
32 Jones RN, Stilwell MG, R homberg PR,Sader HS. Antipseudomonal activity opiperacillin/tazobactam: more than adecade o experience rom the SENTRYAntimicrobial Surveillance Program(19972007). Diagn. Microbiol. Inect. Dis.65(3), 331334 (2009).
33 Wisplingho H, Bischo T, Tallent SM,Seiert H, Wenzel RP, Edmond MB.Nosocomial bloodstream inections in UShospitals: ana lysis o 24,179 cases rom aprospective nationwide surveillance s tudy.
Clin. Inect. Dis. 39(3), 309317 (2004).
Bassetti, Taramasso, Giacobbe & Pelosi
-
7/28/2019 Share01.pdf
11/12
www.expert-reviews.com 595
Review
34 Berger-Bchi B, Rohrer S. Factorsinfuencing methicillin resistance instaphylococci.Arch. Microbiol. 178(3),165171 (2002).
35 Athanassa Z, Siempos II, Falagas ME.Impact o methicillin resistance on
mortality in Staphylococcus aureusVAP: asystematic review. Eur. Respir. J. 31(3),625632 (2008).
36 Sakoulas G, Moise-Broder PA, Schentag J,Forrest A, Moellering RC Jr, EliopoulusGM. Relationship o MIC andbactericidal activity to ecacy ovancomycin or treatment o methicillin-resistant Staphylococcus aureusbacteremia.J. Clin. Microbiol. 42(6), 23982402 (2004).
37 Soriano A, Marco F, Martinez JAet al.Infuence o vancomycin minimuminhibitory concentration on the treatment o
methicillin-resistant Staphylococcus aureusbacteremia. Clin. Inect. Dis. 46(2), 193200(2008).
38 Bassetti M, Ginocchio F, Giacobbe DR.New approaches or empiric theraphy inGram-positive sepsis.Minerva Anestesiol.77(8), 821827 (2011).
39 Annane D, Aegerter P, Jars-Guincestre MC,Guidet B. Current epidemiology o septicshock: the CUB-Rea Network.Am.J. Respir. Crit. Care Med. 168(2), 165172(2003).
40 Conte JE Jr, Golden JA, Kipps J, Zurlinden
E. Intrapulmonary pharmacokinetics olinezolid.Antimicrob. Agents Chemother.46(5), 14751480 (2002).
41 Wong A, Reddy SP, Smyth DSAquero-Roseneld ME, Sakoulas G,Robinson DA. Polyphyletic emergence olinezolid-resistant Staphylococciin theUnited States.Antimicrob. Agents Chemother.54(2), 742748 (2010).
42 Silverman JA, Mortin LI, Vanpraagh AD, LiT, Alder J. Inhibition o daptomycin bypulmonary suractant: in vitro modeling andclinical impact.J. Inect. Dis. 191(12),21492152 (2005).
43 Andrews CP, Coalson JJ, Smith JD,Johanson WG Jr. Diagnosis o nosocomialbacterial pneumonia in acute, diuse lunginjury. Chest80, 254258 (1981).
44 Johanson WG Jr, Pierce AK, Sanord JP,Thomas GD. Nosocomial respiratoryinections with Gram-negative bacilli. Thesignicance o colonization o therespiratory tract.Ann. Intern. Med. 77,701706 (1972).
45 Torres A, Ewig S, Lode H, Carlet J;European HAP working group. Dening,treating and preventing hospital acquired
pneumonia: European perspective. IntensiveCare Med. 35, 929 (2009).
46 Fbregas N, Ewig S, Torres Aet al. Clinicaldiagnosis o ventilator associated pneumoniarevisited: comparative validation usingimmediate post-mortem lung biopsies.
Thorax54, 867873 (1999).
47 Pugin J, Auckenthaler R, Mili N, JanssensJP, Lew PD, Suter PM. Diagnosis oventilator-associated pneumonia bybacteriologic analysis o bronchoscopic andnonbronchoscopic blind bronchoalveolarlavage fuid.Am. Rev. Respir. Dis. 143,11211129 (1991).
48 Zilberberg MD, Shorr AF. Ventilator-associated pneumonia: the ClinicalPulmonary Inection Score as a surrogate ordiagnostics and outcome. Clin. Inect. Dis.51(Suppl. 1), S131S135 (2010).
49 Fartoukh M, Maitre B, Honor S, Cer C,Zahar JR, Brun-Buisson C. Diagnosingpneumonia during mechanical ventilation:the Clinical Pulmonary Inection Scorerevisited. Am. J. Respir. Crit. Care Med. 168,173179 (2003).
InterestingrevisitationoftheClinical
PulmonaryInfectionScore,including
valutationofGramstrainresults.
50 Papazian L, Thomas P, Garbe L et al.Bronchoscopic or blind sampling techniquesor the diagnosis o ventilator-associatedpneumonia.Am. J. Respir. Crit. Care Med.
152, 19821991 (1995).51 Croce MA, Swanson JM, Magnotti LJ et al.
The utility o the Clinical PulmonaryInection Score in trauma patients.J. Trauma60, 523527 (2006).
52 Luyt CE, Chastre J, Fagon JY. Value o theClinical Pulmonary Inection Score or theidentication and management o ventilator-associated pneumonia. Intensive Care Med.30, 844852 (2004).
53 Schurink CA, Van Nieuwenhoven CA,Jacobs JAet al. Clinical PulmonaryInection Score or ventilator-associated
pneumonia: accuracy and inter-observervariability. Intensive Care Med. 30, 217224(2004).
54 Flanagan PG, Findlay GP, Magee JT,Ionescu A, Barnes RA, Smithies M. Thediagnosis o ventilator-associated pneumoniausing non-bronchoscopic, non-directed lunglavages. Intensive Care Med. 26, 2030(2000).
55 Pham TN, Ne MJ, Simmons JM, GibranNS, Heimbach DM, Kelin MB. TheClinical Pulmonary Inection Score poorlypredicts pneumonia in patients with burns.J. Burn Care Res. 28, 7679 (2007).
56 Torres A, el-Ebiary M, Padr L et al.Validation o dierent techniques or thediagnosis o ventilator-associatedpneumonia. Comparison with immediatepostmortem pulmonar y biopsy.Am.J. Respir. Crit . Care Med. 149, 324331
(1994).57 Pelosi P, Baras si A, Severgnini P et al.
Prognostic role o clinical and laboratorycriteria to identiy early ventilator-associated pneumonia in brain injur y.Chest134(1), 101108 (2008).
58 Luna CM, Blanzaco D, Niederman MSet al. Resolution o ventilator-associatedpneumonia: prospective evaluation o theClinical Pulmonary Inection Score as anearly clinica l predictor o outcome. Crit.Care Med. 31, 676662 (2003).
59 Dennesen PJ, van der Ven AJ, Kessels AG,
Ramsay G, Bonten MJ. Resolution oinectious parameters ater antimicrobialtherapy in patients with ventil ator-associated pneumonia.Am. J. Respir. Crit.Care Med. 163, 13711375 (2001).
60 Singh N, Rogers P, Atwood CW, WagenerMM, Yu VL. Short-course empiricantibiotic therapy or patients withpulmonary inltrates in the intensive careunit. A proposed solution orindiscriminate antibiotic prescription.Am.J. Respir. Crit . Care Med. 162, 505511(2000).
61 Luyt CE, Chastre J, Fagon JY. Value o theClinical Pulmonary Inection Score or theidentication and management oventilator-associated pneumonia. IntensiveCare Med. 30, 844852 (2004).
62 Rea-Neto A, Yousse NC, Tuche F et al.Diagnosis o ventilator-associatedpneumonia: a systematic review o theliterature. Critical Care12, R56 (2008).
63 Palazzo SJ, Simpson T, Schnapp L.Biomarkers or ventilator-associatedpneumonia: review o the literature. HeartLung40, 293298 (2011).
64 Meersseman W, Lagrou K, Maertens J
et al. Galactomannan in bronchoalveolarlavage fuid: a tool or diagnosingaspergillosis in intensive care unit patients.Am. J. Respir. Crit. Care Med . 177, 2734(2008).
65 Jean SS, Hsueh PR. Current review oantimicrobial treatment o nosocomialpneumonia caused by multidrug-resistantpathogens. Expert Opin. Pharmacother.12(14), 21452148 (2011).
Overviewoftheuseofnewandold
antibioticsinmultidrug-resistant
pathogeninfections.
Ventilator-associated pneumonia: epidemiology, diagnosis & antimicrobial therapy
-
7/28/2019 Share01.pdf
12/12
Expert Rev. Anti Inect. Ther. 10(5), (2012)596
Review
66 Kolle MH. What is ventilator-associatedpneumonia and why is it important? Respir.Care. 50 (6), 714721 (2005).
67 Gupta A, Agrawal A, Mehrotra S, Singh A,Malik S, Khanna A. Incidence, riskstratication, antibiogram o pathogens
isolated and clinical outcome o ventilatorassociated pneumonia. Indian J. Crit. CareMed. 15(2), 96101 (2011).
68 Porzecanski I, Bowton DL. Diagnosis andtreatment o ventilator-associatedpneumonia. Chest130(2), 597604 (2006).
69 Wilke M, Grube RF, Bodmann KF.Guideline-adherent initial intravenousantibiotic therapy or hospital-acquired/ventilator-associated pneumonia isclinically superior, saves lives and ischeaper than non guideline adherenttherapy. Eur. J. Med. Res. 16(7), 315323
(2011).70 Rello J. Bench-to-bedside review:
therapeutic options and issues in themanagement o ventilator-associatedbacterial pneumonia. Crit. Care9(3),259265 (2004).
71 Niederman MS, Soulountsi V.De-escalation therapy: is it valuable or themanagement o ventilator-associatedpneumonia? Clin. Chest Med. 32(3),517534 (2011).
72 Kolle MH, Morrow LE, Niederman MS
et al. Clinical characteristics and treatment
patterns among patients with ventilator-associated pneumonia. Chest129(5),12101218 (2006).
73 Giantsou E, Liratzopoulos N, EraimidouE et al. De-escalation therapy rates aresignicantly higher by bronchoalveolarlavage than by tracheal aspirate. IntensiveCare Med. 33(9), 15331540 (2007).
74 Rello J, Vidaur L, Sandiumenge Aet al.De-escalation therapy in ventilator-associated pneumonia. Crit. Care Med.32(11), 21832190 (2004).
75 Niederman MS, Craven DE. Guidelines
or the management o adults withhospital-acquired, ventilator-associated,and healthcare-associated pneumonia.Am.J. Respir. Crit. Care Med. 171, 388 416(2005).
76 Chastre J, Wol M, Fagon JYet al.Comparison o 8 vs. 15 days o antibiotictherapy or ventilator-associatedpneumonia in adults: a randomized trial.JAMA 290(19), 25882598 (2003).
77 Li H, Luo YF, Blackwell TS, Xie CM.
Meta-analysis and systematic review oprocalcitonin-guided therapy in respiratorytract inections.Antimicrob. AgentsChemother. 55(12), 59005906 (2011).
78 Grammatikos AP, Siempos II,Michalopoulos A, Falagas ME. Optimalduration o the antimicrobial treatment oventilator-acquired pneumonia. ExpertRev. Anti Inect. Ther. 6(6), 861866(2008).
79 Stein GE, Wells EM. The importance otissue penetration in achieving successulantimicrobial treatment o nosocomial
pneumonia and complicated skin andsot-tissue inections caused bymethicillin-resistant Staphylococcus aureus:vancomycin and linezolid. Curr. Med. Res.Opin. 26(3), 571588 (2010).
80 Roberts JA, Kirkpatrick CM, LipmanJ. Monte Carlo simulations : maximizingantibiotic pharmacokinetic data tooptimize clinical practice or critically illpatients. J. Antimicrob. Chemother. 66(2),227231 (2011).
Focusesontheimportanceofcorrect
antibioticdosing,takingintoaccount
thepharmacokineticsandpharmacodynamicsofthedrugs.
81 American Thoracic Society. Guidelines orthe management o adults with hospital-acquired, ventilator-associated, andhealthcare-associated pneumonia.Am.J. Respir. Crit. Care Med. 171, 388416(2005).
82 Kett DH, Cano E, Quartin AAet al.;Improving Medicine through PathwayAssessment o Crit ical Therapy oHospital-Acquired Pneumonia (IMPACT-HAP) Investigators. Implementation oguidelines or management o possible
multidrug-resistant pneumonia inintensive care: an observational,multicentre cohort study. Lancet Inect.Dis. 11(3), 181189 (2011).
83 Bassetti M, Repetto E, Righi E et al.Colistin and riampicin in the treatment omultidrug-resistantAcinetobacterbaumanniiinections.J. Antimicrob.Chemother. 61(2), 417420 (2008).
84 Yahav D, Lador A, Paul M, Leibovici L.
Ecacy and saety o tigecycline: asystematic review and meta-analysis.
J. Antimicrob. Chemother. 66(9),19631971 (2011).
85 Rubinstein E, Lalani T, Corey GRet al.Telavancin versus vancomycin orhospital-acquired pneumonia due togram-positive pathogens. Clin. Inect. Dis.52(1), 3140 (2011).
86 van Hal SJ, Paterson DL.New Gram-positive antibiotics: better thanvancomycin? Curr. Opin. Inect. Dis. 24(6),515520 (2011).
87 Bouza E, Burillo A. Advances in theprevention and management o ventilator-associated pneumonia. Curr. Opin. Inect.Dis. 22(4), 345351 (2009).
88 Kolle MH, Rello J, Cammarata SK,Croos-Dabrera RV, Wunderink RG.Clinical cure and sur vival in Gram-positiveventilator-associated pneumonia:retrospective analysis o two double-blindstudies comparing linezolid withvancomycin. Intensive Care Med. 30(3),388394 (2004).
89 Wunderink RG, Niederman MS, Kolle
MH et al. Linezolid in methicillin-resistantStaphylococcus aureusnosocomialpneumonia: a randomized, controlledstudy. Clin. Inect. Dis. doi:10.1093/cid/cir895 (2012) (Epub ahead o print).
90 Liu C, Bayer A, Cosgrove SE et al. Clinicalpractice guidelines by the InectiousDiseases Society o America or thetreatment o methicillin-resistantStaphylococcus aureusinections in adultsand children: executive summary. Clin.Inect. Dis. 52, 285292 (2011).
91 Lodise TP, Patel N, Lomaestro BM,Rodvold KA, Drusano GL. Relationship
between initial vancomycin concentration-time prole and nephrotoxicity amonghospitalized patients. Clin. Inect. Dis. 49,507514 (2009).
Bassetti, Taramasso, Giacobbe & Pelosi