Shamir Mehta, MD, MSc, FRCPC Director Interventional Cardiology Associate Professor of Medicine...
44
Shamir Mehta, MD, MSc, FRCPC Shamir Mehta, MD, MSc, FRCPC Director Interventional Cardiology Associate Professor of Medicine McMaster University Hamilton, Ontario, Canada Continues – But with Better Outcomes? A Critical Appraisal of Recent Clinical Data
-
Upload
nathaniel-nicholson -
Category
Documents
-
view
218 -
download
0
Transcript of Shamir Mehta, MD, MSc, FRCPC Director Interventional Cardiology Associate Professor of Medicine...

Shamir Mehta, MD, MSc, FRCPCShamir Mehta, MD, MSc, FRCPCDirector Interventional Cardiology
Associate Professor of Medicine
McMaster University
Hamilton, Ontario, Canada
The Balancing Act in ACS Continues – But with BetterOutcomes? A Critical Appraisal of Recent Clinical Data
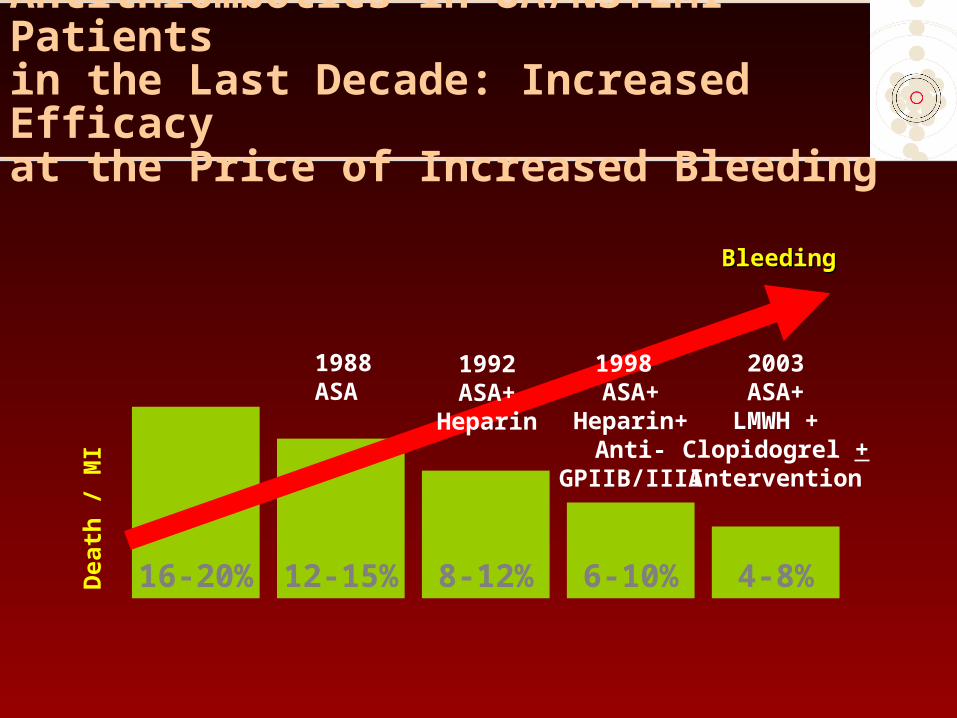
Antithrombotics in UA/NSTEMI Patients in the Last Decade: Increased Efficacy at the Price of Increased Bleeding
16-20% 12-15% 8-12% 6-10% 4-8%Dea
th /
MI
BleedingBleeding
1988ASA
1992ASA+
Heparin
1998 ASA+
Heparin+Anti-
GPIIB/IIIA
2003ASA+
LMWH +Clopidogrel +Intervention

Bleeding is Associated with an Increased 30-Day Mortality in NSTEMI Patients
Rao et al. Am J Cardiol 2005;96:1200-1206
N = 26,452 ACS patients from GUSTO IIb, PURSUIT and PARAGON A&B
Log-rank p values are 0.0001 for all 4 categories, 0.20 for no bleeding vs. mild bleeding, 0.0001 for mild vs. moderate bleeding, and 0.001 for moderate vs. severe bleeding.
Adjusted HR (95% CI)
% Death
2.9% 1.03.5% 1.6 (1.3-1.9)5.9% 2.7 (2.3-3.4)
25.7% 10.6 (8.3-13.6)
GUSTO bleeding None Mild Moderate Severe
0 5 10 15 20 25 30
0.70
0.75
0.80
0.85
0.90
0.95
1.00
Days to Death
Cu
mu
lati
ve s
urv
ival

Procedure-Related and Non-Procedure-Related Bleeds are Associated with an Increased 30-Day Mortality in NSTEMI Patients
Rao et al. Am J Cardiol 2005;96:1200-1206
Procedure-related GUSTO bleeds
Non-procedure-related GUSTO bleeds
Ris
k o
f d
eath
(H
azar
d R
atio
)
None
1.0
Mild
1.3
Severe
16.5
0
5
20
10
15
None
1.0
Mild
2.1
Moderate
2.5
Severe
10.9
Moderate
3.7
N = 26,452 ACS patients from GUSTO IIb, PURSUIT and PARAGON A & B

OASIS Registry, OASIS-2, CUREStrong, Independent Association
OutcomeMajorBleed
No MajorBleed
Hazard (Adjusted)
P-Value
Death 60/470(12.8%)
833/33676(2.5%)
5.37(3.97-7.26)
<0.0001
MI46/436(10.6%)
1375/33710(4.1%)
4.44(3.16-6.24)
<0.0001
Stroke12/469
(2.6%)
187/33677
(0.6%)
6.46
(3.54-11.79)<0.0001
Eikelboom JW et al. Circulation. 2006;114(8):774-82.
N = 34,126

Increased Mortality at Days 30/180 in Patients with Major Bleeds by Day 9 (All Patients)
Budaj et al. JACC. 2006;abstract 972-224
Adjusted HR (95% CI) at day 30: 5.06 (4.59-5.62); at day 180: 3.16 (2.92-3.44)
0.00
0.05
0.10
0.15
0.20
0 30 60 90 120 150 180
Major Bleed 9 days
No Major Bleed 9 days
Cu
mu
lati
ve
Ha
zard
Days

Increased Risk of MI at Days 30/180 in Patients with Major Bleeds by Day 9 (All Patients)
Adjusted HR (95% CI) at day 30: 5.01 (4.56-5.57); at day 180: 2.99 (2.75-3.28)
Budaj et al. JACC. 2006;abstract 972-224
0 30 60 90 120 150 180
Days
0.00
Cu
mu
lati
ve
Ha
zard
0.05
0.10
0.15
Major Bleed 9 days
No Major Bleed 9 days

Increased Risk of Stroke at Days 30/180 in Patients with Major Bleeds by Day 9 (All Patients)
Adjusted HR (95% CI) at day 30: 4.77 (3.95-6.00); at day 180: 3.30 (2.82-3.97)
Budaj et al. JACC. 2006;abstract 972-224.
0 30 60 90 120 150 180
0.00
0.01
0.02
0.03
0.04
0.05
0.06
Cu
mu
lati
ve
Ha
zard
Days
Major Bleed 9 days
No Major Bleed 9 days

Potential Mechanisms for the Higher Morbidity/Mortality Associated with Bleeding
1. Activation of clotting cascade as a response to bleeding--may lead to recurrent events in at the site of plaque rupture
2. Cessation of antithrombotic therapies (eg. ASA, clopidogrel, heparin) after a bleeding event
3. Adverse effects of hypotension due to the bleed
4. Adverse effects of transfusion
5. Common risk factors for bleeding and adverse outcome

Coagulation Cascade and New Anticoagulants
Rosenberg & Aird. N Engl J Med. 1999;340:1555–64.Wessler & Yin. Thromb Diath Haemorrh. 1974;32:71–8.
Inhibition of one molecule of factor Xa can inhibit the generation of 50 molecules of thrombin
Intrinsic pathway Extrinsic pathway
1
50
Xa X
II
FibrinFibrinogen
Clot
XaVa
PLCa2+
IIa
VIIIa
Ca2+
PL
IXa
Bivalirudin
Fondaparinux

Herbert JM et al. Cardiovasc Drug Rev. 1997;15:1. van Boeckel CAA et al. Angew Chem, Int Ed Engl. 1993;32:1671.
Once daily administration Rapid onset (Cmax/2=25 min) Effects reversible with
administration of activated Factor VII (Novoseven®)
No liver metabolism No protein binding (other than AT) No risk of pathogen contamination No reported cases of HIT No dose adjustment necessary in
elderly
Fondaparinux: A Synthetic Inhibitor of Factor Xa

IIa IIa IIII
FibrinogenFibrinogen Fibrin clotFibrin clot
Extrinsic Extrinsic pathwaypathway
IntrinsicIntrinsicpathwaypathway
AT XaXaAT AT
Fondaparinux Fondaparinux
XaXa
Antithrombin
Fondaparinux Mechanism of Action
Olson et al. J Biol Chem. 1992;267:12528-38.Turpie et al. N Engl J Med. 2001;344:619-25.
THROMBIN
Recycled

EphesusN = 1817
Pentathlon 2000N = 1584
PenthifraN = 1250
PentamaksN = 724
Overall Odds Reduction
% odds reduction
Fondaparinux better Enoxaparin better
-100 -80 -60 -40 -20 200 40 60 80 100
58.5%
28.1%
61.6%
63.1%
55.3%P = 0.000000000000000001
Overall odds reduction for proximal DVT = 57.4% [CI: 72.3 - 35.6]; p = 10-6
Overall Efficacy of Fondaparinux vs Enoxaparin in VTE Prevention: Meta-analysis
Turpie et al. Arch Intern Med. 2002;162:1833-40.
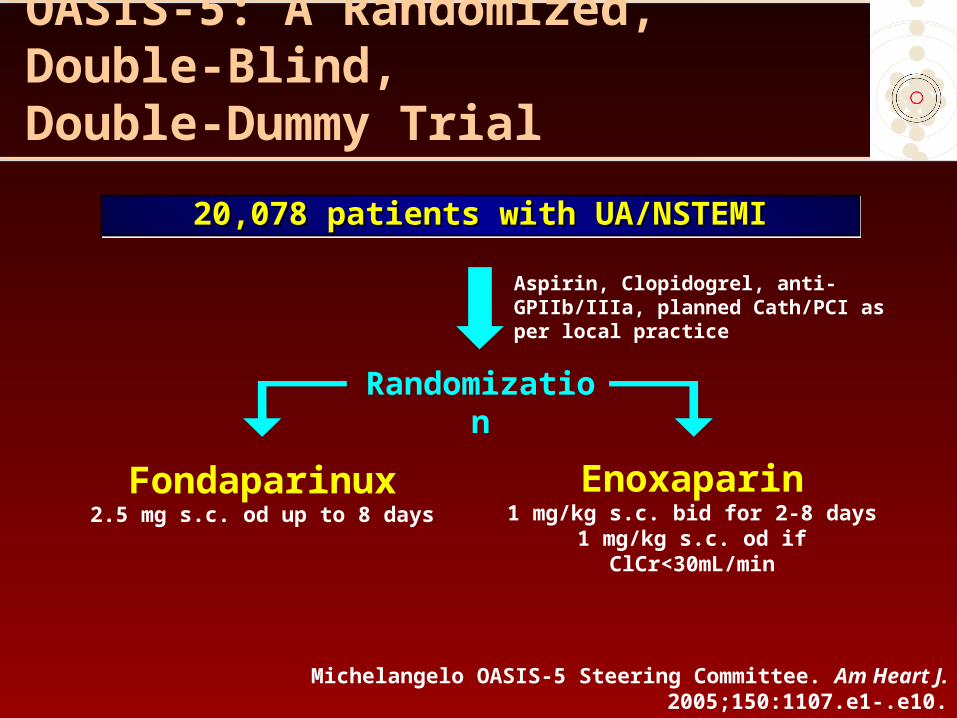
OASIS-5: A Randomized, Double-Blind, Double-Dummy Trial
20,078 patients with UA/NSTEMI20,078 patients with UA/NSTEMI20,078 patients with UA/NSTEMI20,078 patients with UA/NSTEMI
Fondaparinux2.5 mg s.c. od up to 8 days
Aspirin, Clopidogrel, anti-GPIIb/IIIa, planned Cath/PCI as per local practice
Randomization
Enoxaparin1 mg/kg s.c. bid for 2-8 days
1 mg/kg s.c. od if ClCr<30mL/min
Michelangelo OASIS-5 Steering Committee. Am Heart J. 2005;150:1107.e1-.e10.OASIS 5 Investigators. I. 1464-76.
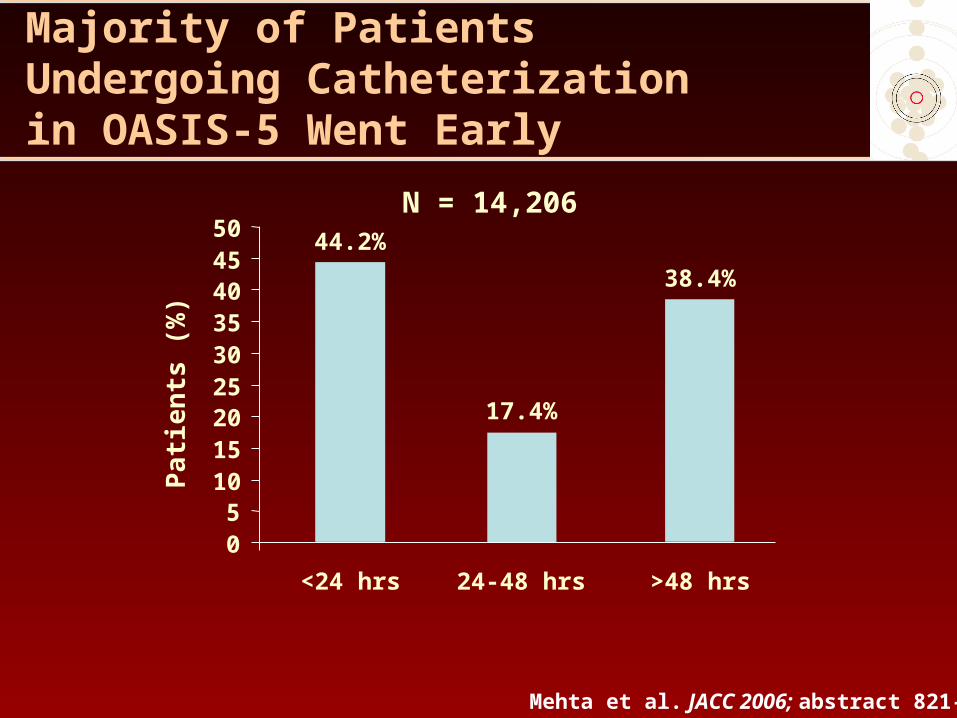
Majority of Patients Undergoing Catheterization in OASIS-5 Went Early
Mehta et al. JACC 2006; abstract 821-5
44.2%
17.4%
38.4%
05
101520253035404550
<24 hrs 24-48 hrs >48 hrs
Pa
tie
nts
(%
)N = 14,206

Similar Efficacy Outcome Rates in Both Groups at Day 9
OASIS-5 Investigators. N Engl J Med. 2006;354:1464-76.
5.8%5.7%Death/MI/RI
1.9%1.9%Refractory Ischemia
2.6%2.7%MI
1.8%1.9%Death
4.1%4.1%Death/MI
FondaparinuxEnoxaparin
0.8 1.0 1.2
Non-inferiorityMargin = 1.185
Hazard Ratio
Fondaparinux better Enoxaparin better
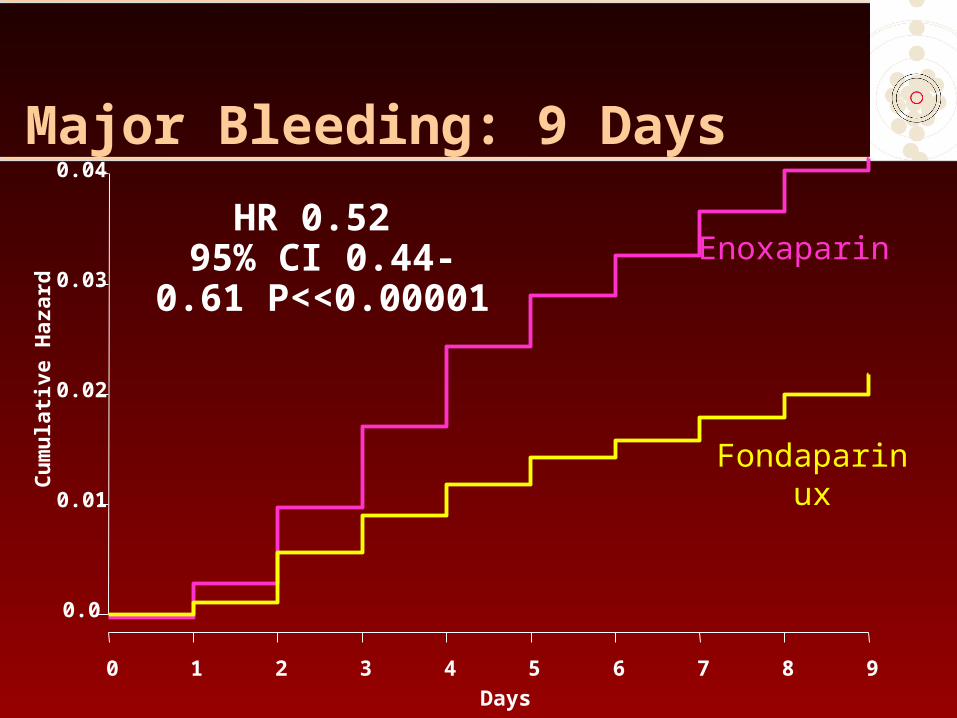
Major Bleeding: 9 Days
Days
Cu
mu
lati
ve H
azar
d
0.0
0.01
0.02
0.03
0.04
0 1 2 3 4 5 6 7 8 9
HR 0.52 95% CI 0.44-0.61
P<<0.00001Enoxaparin
Fondaparinux

Mortality: Day 30
Days
Cu
mu
lati
ve H
azar
d0.
00.
010.
020.
03
0 3 6 9 12 15 18 21 24 27 30
HR 0.83 95% CI 0.71-0.97
P=0.02
Enoxaparin
Fondaparinux

Efficacy at 6 Months
OASIS 5 Investigators. N Engl J Med. 2006;354:1464-76.
0.8 1 1.2
11.3%12.5%Death/MI/Stroke
12.3%13.2%Death/MI/RI
1.3%1.7%Stroke
6.3%6.6%MI
5.8%6.5%Death
10.5%11.4%Death/MI
0.06
0.05
0.05
NS
0.04
0.007
P value
Fondaparinux better Enoxaparin better
Enoxaparin Fondaparinux Hazard Ratio
Hazard Ratio

All Types of Bleeding were Reduced in the Fondaparinux Group at Day 9
Outcome Enoxaparin(%)
Fondaparinux(%)
p value
No. Randomized 10,021 10,057
Total bleeds 7.3 3.3 <0.001*
Major bleeds 4.1 2.1 <0.001
TIMI major + fatal bleeds
1.3 0.7 <0.001**
Fatal bleeds 0.2 0.1 0.005
Minor bleeds 3.2 1.1 <0.001
* HR (95% CI): 0.44 (0.39-0.50);**HR (95% CI): 0.55 (0.41-0.74)
OASIS-5 Investigators. N Engl J Med. 2006;354:1464-76.
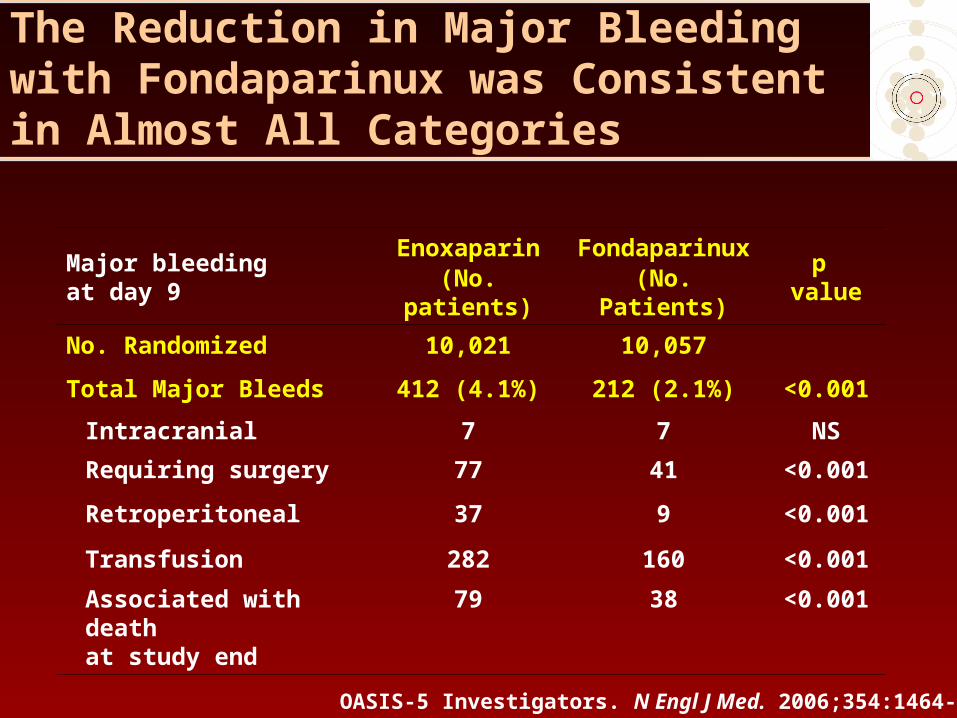
The Reduction in Major Bleeding with Fondaparinux was Consistent in Almost All Categories
Major bleeding at day 9
Enoxaparin(No. patients)
Fondaparinux(No. Patients)
p value
No. Randomized 10,021 10,057
Total Major Bleeds 412 (4.1%) 212 (2.1%) <0.001
Intracranial 7 7 NS
Requiring surgery 77 41 <0.001
Retroperitoneal 37 9 <0.001
Transfusion 282 160 <0.001
Associated with death at study end
79 38 <0.001
OASIS-5 Investigators. N Engl J Med. 2006;354:1464-76.

OASIS-5 – The Reduction in Major Bleeding at Day 9 Was Independent of Renal Function
OASIS-5 Investigators. N Engl J Med. 2006;354:1464-76.
*88 µmol/L
Creatinine
1.9%3.4%<1.04 mg/dL* (n = 8871)
2.4%4.7%>1.04 mg/dL* (n = 11,124)
FondaparinuxEnoxaparin
0.6 1.0 1.2
Interaction p value = 0.71
Hazard Ratio
Fondaparinux better Enoxaparin better
0.80.4

Major Bleeding was Reduced with Fondaparinux Irrespective of Creatinine Clearance
CrCl(mL/min)
Enoxaparin*(%)
Fondaparinux(%)
P value
< 30 (n = 535) 9.9 2.4 0.001
> 30 (n = 19442) 4.0 2.2 <0.001
OASIS 5 Investigators. N Engl J Med. 2006;354:1464-76.
*Enoxaparin dose reduced to 1 mg/kg od according to label if clearance of creatinine was below 30 mL/min

The Reduction in Major Bleeding at Day 9 with Fondaparinux was Consistent in All Subgroups
OASIS-5 Investigators. N Engl J Med 2006;354:1464-76
Characteristics N Enoxaparin Fondaparinux
% %
Age≥ 65 yr 12,261 5.5 2.7< 65 yr 7814 2.1 1.4 0.11
SexMale 12,379 3.3 2.0Female 7699 5.5 2.5 0.07
CreatinineAt or above median* 11,124 4.7 2.4Less than median* 8871 3.4 1.9 0.71
Heparin at randomizationYes 3566 5.0 3.0No 16,512 4.0 2.0 0.35
Revascularization in 9 daysYes 7372 6.0 4.2No 12,706 3.0 1.0 < 0.001
Catheterization laboratory in centerYes 14,028 5.0 2.6No 6050 2.3 1.2 0.88
1.0 1.40.2
Fondaparinux better Enoxaparin better
0.4 0.6 0.8 1.2* The median value for creatinine was 88 µmol/L (1.04 mg/dL)
Interaction p value
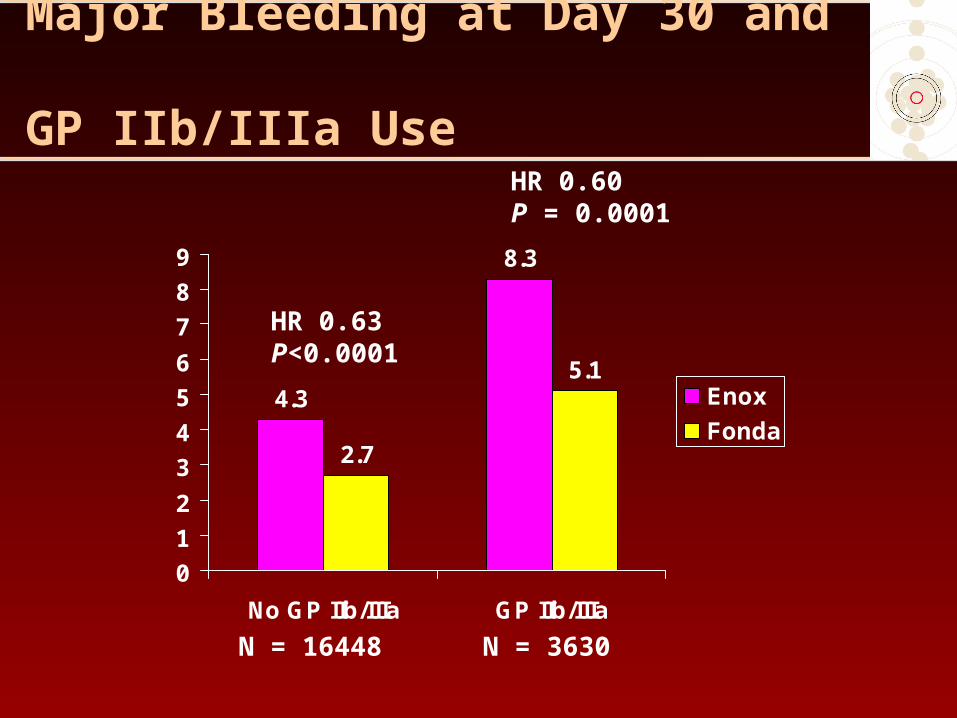
Major Bleeding at Day 30 and GP IIb/IIIa Use
4.3
8.3
2.7
5.1
0
1
2
3
4
5
6
7
8
9
No GP IIb/IIIa GP IIb/IIIa
Enox
Fonda
HR 0.63P<0.0001
HR 0.60P = 0.0001
N = 16448 N = 3630

Fondaparinux Superior to Enoxaparin for Bleeding Irrespective of Rx Duration
6.8
5.2
3
4.8
2.9
2
0
1
2
3
4
5
6
7
8
0-4 Days 5-6 Days 7-8 Days
Maj
or
Ble
eds
at D
ay30
Enox
Fonda
HR 0.69P = 0.001
HR 0.55P <0.0001
HR 0.67P = 0.018
N = 5581 N = 8712 N = 5785

Incidence of Major Bleeds with Enoxaparin in OASIS-5 is Consistent with Previous Trials
Enoxaparin Enox Fonda Enox Fonda
SYNERGY1
In-hospital
ESSENCE2
Day 30
A to Z3
Day 6
Meta-analysis4
Day 7
OASIS 5
Day 9
OASIS 5
Day 9
OASIS 5
Day 30
OASIS 5
Day 30
TIMI major+fatal bleeds
9.1% - 0.9% - 1.3% 0.7% 1.5% 1.0%
Major bleeds - 6.5% - 4.7% 4.1% 2.2% 5.0% 3.1%
1. SYNERGY Investigators. JAMA. 2004;292:45-54. 2. Cohen et al. N Engl J Med. 337:447-52.
3. Blazing et al. JAMA 2004;292:55-64 • 4. Petersen et al. JAMA. 2004;292:89-96.

Fondaparinux-Associated Reduction of Bleeding Translated into Long-Term Mortality Benefit
Patients with Enoxaparin Fondaparinux Difference
No Bleed 526 523 -3
Minor Bleeds 33 13 -20
Major Bleeds 79 38 -41
Total 638 574 -64
No. of deaths at 180 days
OASIS-5 Investigators. N Engl J Med. 2006;354:1464-76.
Days
Cu
mu
lati
ve H
azar
d0.
00.
050.
100.
15
0 20 40 60 80 100 120 140 160 180
Enoxaparin
Fondaparinux
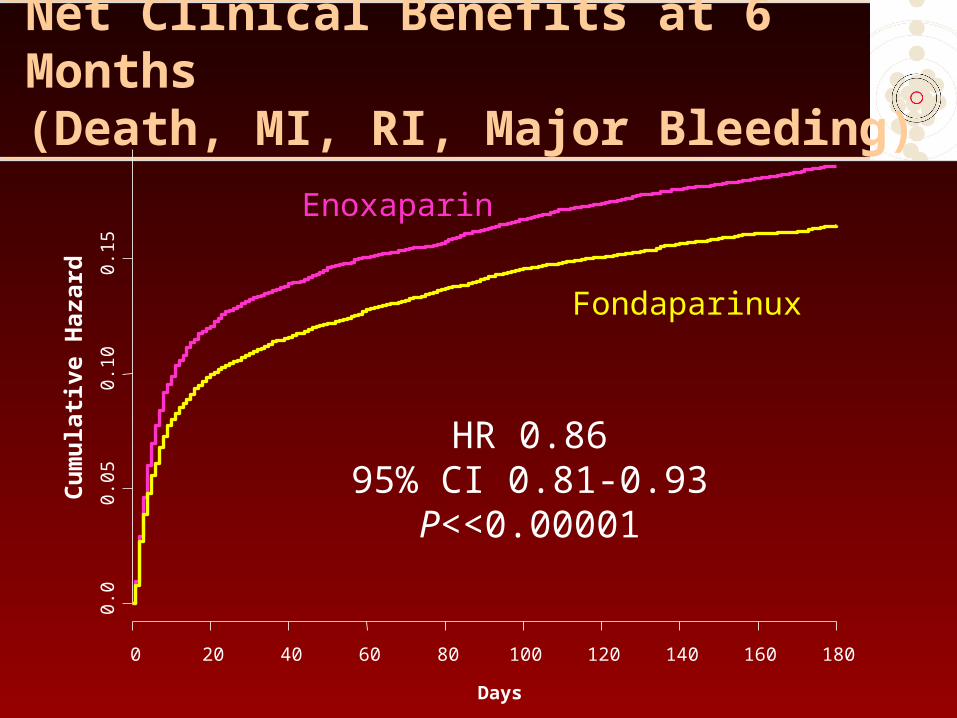
HR 0.8695% CI 0.81-0.93P<<0.00001
Net Clinical Benefits at 6 Months(Death, MI, RI, Major Bleeding)

Efficacy and Safety in PCI PatientsOutcome Day 9 Enox
N = 3072Fonda
N = 3105HR (95% CI) P value
Death, MI or Stroke 190 (6.2) 197 (6.3) 1.03 (0.84-1.25)
0.79
Death 38 (1.2) 37 (1.2) 0.96 (0.61-1.52)
0.87
MI 154 (5.0) 160 (5.2) 1.03 (0.82-1.28)
0.80
Stroke 13 (0.4) 12 (0.4) 0.91 (0.42-2.00)
0.82
Major Bleeding 155 (5.1) 73 (2.4) 0.46 (0.35-0.61)
<0.00001
Death, MI, stroke, major bleeding
318 (10.4) 255 (8.2) 0.78 (0.67-0.93)
0.004
Mehta et al. JACC. 2006;abstract 821-5.

PCI < 24 Hours of RandomizationOutcomeDay 9
EnoxN = 1420
FondaN = 1414
HR (95% CI) P value
Death, MI or Stroke 77 (5.4) 75 (5.3) 0.98 (0.71-1.34)
0.89
Death 19 (1.3) 19 (1.3) 1.01 (0.53-1.90)
0.98
MI 55 (3.9) 53 (3.8) 0.97 (0.66-1.41)
0.86
Stroke 8 (0.6) 6 (0.4) 0.76 (0.23-2.18)
0.60
Major Bleeding 69 (4.9) 33 (2.3) 0.48 (0.31-0.72)
0.0005
Death, MI, stroke, major bleeding
135 (9.5) 103 (7.3) 0.76 (0.59-0.98)
0.035
Mehta et al. JACC. 2006;abstract 821-5

RR 0.4295% CI 0.26-0.65
P <0.0001
RR 0.9695% CI 0.73-1.26
P = 0.78
RR 0.3995% CI 0.22-0.67
P <0.0001
RR 1.4095% CI 1.00-1.97
P = 0.048
Major Bleeding 48 hours after PCI Abrupt/threatened abrupt closure
N = 1277 N = 1275 N =
1633
N = 1648
N = 1275
RR 0.94 95% CI 0.63-1.33
P=0.62
RR 0.70 95% CI 0.51-0.96
P=0.026
OASIS 5: Fonda vs Enox alone and vs UFH + Enox
Mehta et al. Presented at WCC/ESC Hotline Session, Barcelona, 2006
3.83.4
6.2
4.3
1.3
5.9 6
0
2
4
5
6
7
% E
ven
ts
FondaFonda
Enox alone
UFH+
EnoxFonda
Fonda
Enoxalone UFH
+Enox
1
N = 1633
N = 1648
1.6
3 N = 1277
N = 1633
N = 1648
N = 1277
N = 1275

Open Label UFH Prior to PCI Data After Protocol Amendment
No UFH Prior to PCI UFH Prior to PCI
Enox(%)
Fonda(%)
HR (95% CI)
Enox(%)
Fonda(%)
HR(95% CI)
Number randomized 810 793 80 75
Death/MI/Stroke/Major Bleed
90 (11.1) 80 (10.1) 0.90(0.67-1.22)
9 (11.2) 4 (5.3) 0.45(0.14-1.47)
Death/MI/Stroke 60 (7.4) 57 (7.2) 0.97(0.68-1.40)
5 (6.3) 3 (4.0) 0.62(0.15-2.61)
Major Bleed 35 (4.3) 26 (3.3) 0.75(0.45-1.25)
5 (6.2) 1 (1.3) 0.21(0.02-1.79)
Abrupt Closure 13 (1.6) 15 (1.9) 1.18(0.56-2.5)
0 1 (1.3) --
Threatened abrupt closure
38 (4.7) 31 (3.9) 0.83 (0.52-1.32)
2 (2.5) 4 (5.3) 2.13(0.40-11.3)
Catheter Thrombus 4 (0.5) 9 (1.1) 2.30(0.71-7.4)
0 1 (1.3)* --
Vascular Access Site complication
56 (6.9) 22 (2.8) 0.40(0.25-0.65)
5 (6.3) 1 (1.3) 0.21(0.03-1.8)
Final 1758 patients randomized*represents 1 patient with low dose of UFH 5 IU/kg vs mean dose of 47 IU/kg
Mehta et al. JACC. 2006;abstract 821-5
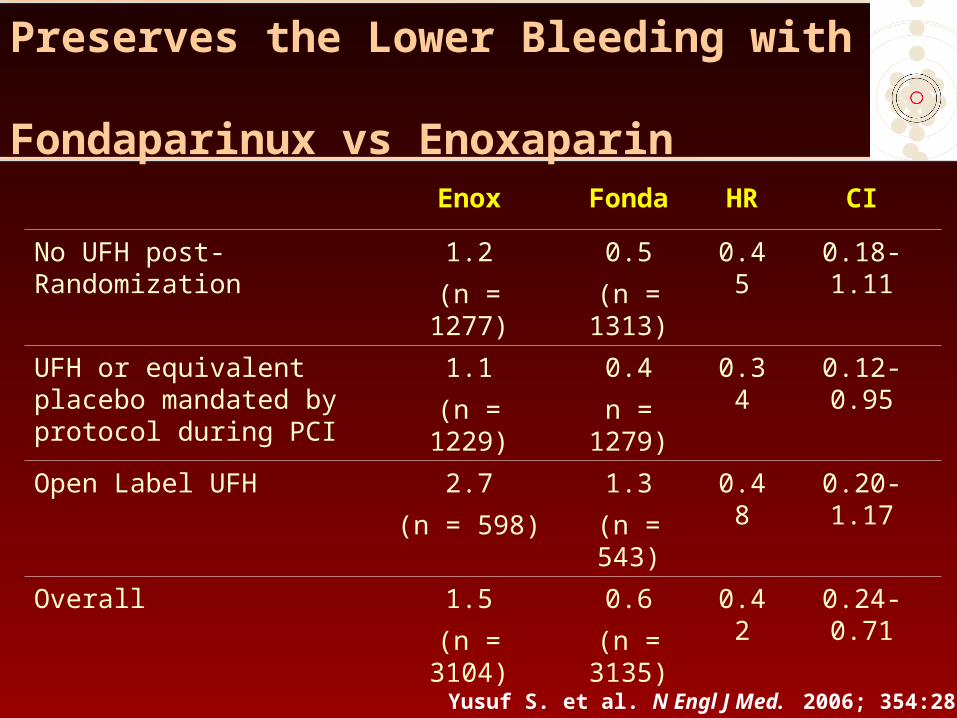
Adding UFH to Fondaparinux is Safe and Preserves the Lower Bleeding with Fondaparinux vs Enoxaparin
Enox Fonda HR CI
No UFH post-Randomization
1.2
(n = 1277)
0.5
(n = 1313)
0.45 0.18-1.11
UFH or equivalent placebo mandated by protocol during PCI
1.1
(n = 1229)
0.4
n = 1279)
0.34 0.12-0.95
Open Label UFH 2.7
(n = 598)
1.3
(n = 543)
0.48 0.20-1.17
Overall 1.5
(n = 3104)
0.6
(n = 3135)
0.42 0.24-0.71
Yusuf S. et al. N Engl J Med. 2006; 354:2829.
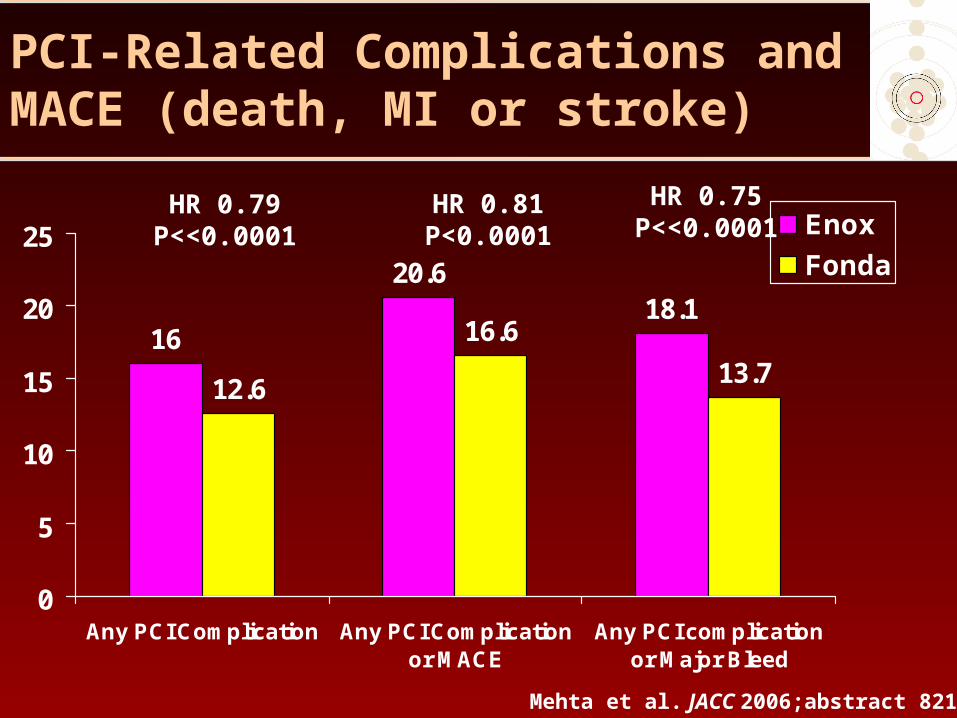
PCI-Related Complications and MACE (death, MI or stroke)
16
20.618.1
12.6
16.6
13.7
0
5
10
15
20
25
Any PCI Complication Any PCI Complicationor MACE
Any PCI complicationor Major Bleed
Enox
Fonda
HR 0.79P<<0.0001
HR 0.81P<0.0001
HR 0.75P<<0.0001
Mehta et al. JACC 2006;abstract 821-5

Advantage of a Single Dose with Fondaparinux
The advantage of a single dose for all patients is clear; in this era of recognition of the common
occurrence of medical errors that lead to harm, a single dose would result in fewer medical errors
because complex calculations of the type identified in the CRUSADE registry would not be needed
Califf. JAMA. 2006;295:1579-80.

ACUITY Study Design – Patient Flow
UFH/Enox+ GP IIb/IIIa(N = 4,603)
Bivalirudin+ GP IIb/IIIa(N = 4,604)
BivalirudinAlone
(N = 4,612)
R*
Moderate-high risk unstable angina or NSTEMI undergoing an invasive strategyModerate-high risk unstable angina or NSTEMI undergoing an invasive strategy
GPI upstream (N = 2294)
GPI CCL for PCI (N = 2309)
GPI upstream (N = 2311)
GPI CCL for PCI (N = 2293)
Aspirin in allClopidogrel
dosing and timingper local practice
Aspirin in allClopidogrel
dosing and timingper local practice
*Stratified by pre-angiography thienopyridine use or administration*Stratified by pre-angiography thienopyridine use or administration
Moderate-high risk
ACS
Stone GW, et al. N Engl J Med. 2006 Nov 23;355(21):2203-16.

ACUITY Primary Outcome: No Difference in Ischemic Outcomes or Major Bleeding with Bivalirudin vs Heparin in Presence of GPI
11.7%
7.3%5.7% 5.3%
11.8%
7.7%
Net clinicaloutcome
Ischemiccomposite
Major bleeding
30
da
y e
ve
nts
(%
)
UFH/Enoxaparin+GPI (N=4603) Bivalirudin+GPI (N=4604)
PSup = 0.93 PSup = 0.39 PSup = 0.38
Stone GW, et al. N Engl J Med. 2006 Nov 23;355(21):2203-16.
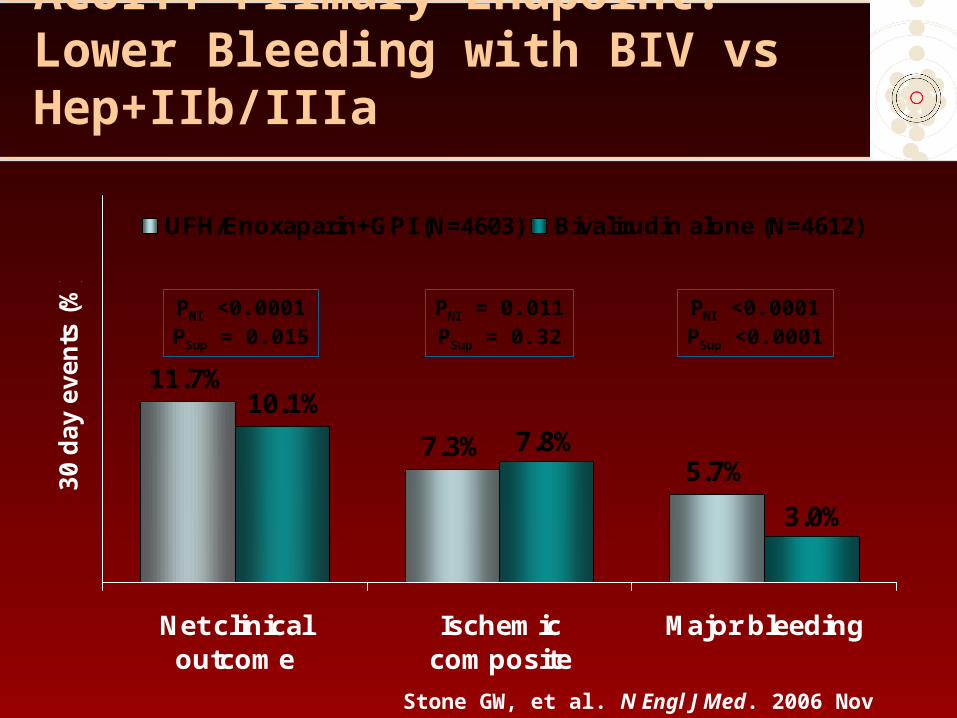
ACUITY Primary Endpoint: Lower Bleeding with BIV vs Hep+IIb/IIIa
11.7%
7.3%5.7%
3.0%
10.1%
7.8%
Net clinicaloutcome
Ischemiccomposite
Major bleeding
30
da
y e
ve
nts
(%
)
UFH/Enoxaparin+GPI (N=4603) Bivalirudin alone (N=4612)
PNI <0.0001PSup = 0.015
PNI = 0.011PSup = 0.32
PNI <0.0001PSup <0.0001
Stone GW, et al. N Engl J Med. 2006 Nov 23;355(21):2203-16.

ACUITY: Components of the Ischemic Composite
7.3%
1.3%
4.9%
2.3%2.7%2.4%
5.0%
7.7%
1.5% 1.6%
7.8%
5.4%
Ischemiccomposite
Death Myocardialinfarction
Unplannedrevasc forischemia
30
da
y e
ve
nts
(%
)
UFH/Enox+GPI (N=4603) Bivalirudin+GPI (N=4604) Bivalirudin alone (N=4612)
UFH/Enoxaparin + GPI vs. Bivalirudin + GPI vs. Bivalirudin AloneUFH/Enoxaparin + GPI vs. Bivalirudin + GPI vs. Bivalirudin Alone
PSup = 0.32 PSup = 0.34 PSup = 0.35 PSup = 0.78
Stone GW, et al. N Engl J Med. 2006 Nov 23;355(21):2203-16.
0 1 2
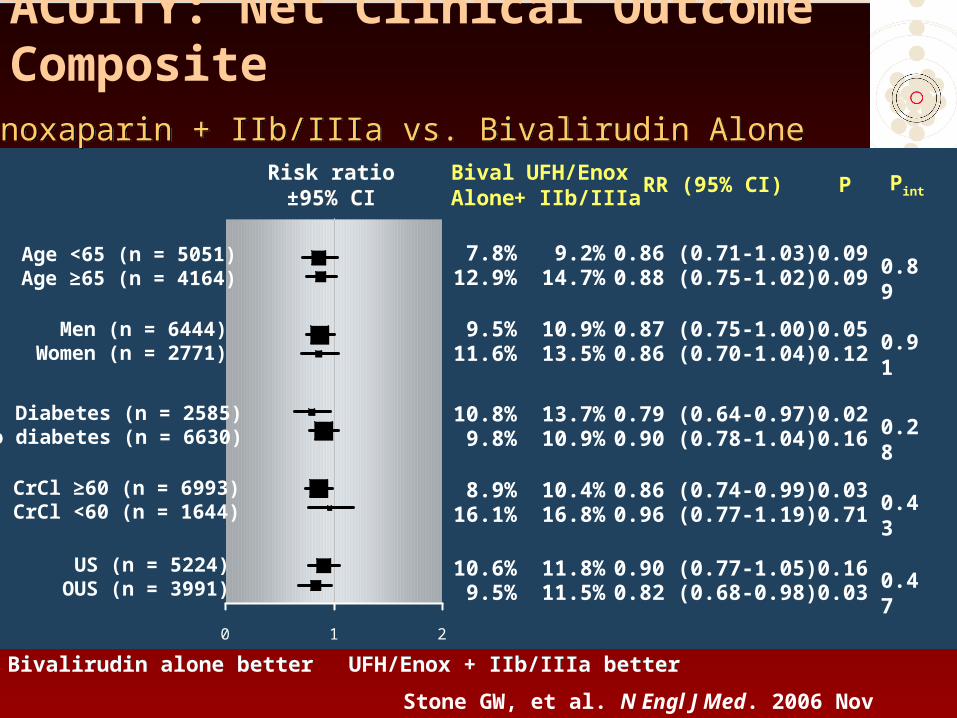
ACUITY: Net Clinical Outcome CompositeUFH/Enoxaparin + IIb/IIIa vs. Bivalirudin AloneUFH/Enoxaparin + IIb/IIIa vs. Bivalirudin Alone
Men (n = 6444)Women (n = 2771)
Diabetes (n = 2585)No diabetes (n = 6630)
CrCl ≥60 (n = 6993)CrCl <60 (n = 1644)
Age <65 (n = 5051)Age ≥65 (n = 4164)
Risk ratio±95% CI
Risk ratio±95% CI
BivalAlone
UFH/Enox+ IIb/IIIa
7.8%12.9%
US (n = 5224)OUS (n = 3991)
10.6%9.5%
8.9%16.1%
10.8%9.8%
9.5%11.6%
9.2%14.7%
11.8%11.5%
10.4%16.8%
13.7%10.9%
10.9%13.5%
P Pint
0.86 (0.71-1.03)0.88 (0.75-1.02)
0.90 (0.77-1.05)0.82 (0.68-0.98)
0.86 (0.74-0.99)0.96 (0.77-1.19)
0.79 (0.64-0.97)0.90 (0.78-1.04)
0.87 (0.75-1.00)0.86 (0.70-1.04)
0.090.09
0.160.03
0.030.71
0.020.16
0.050.12
0.89
0.47
0.43
0.28
0.91
RR (95% CI)
Bivalirudin alone betterBivalirudin alone better UFH/Enox + IIb/IIIa betterUFH/Enox + IIb/IIIa better
Stone GW, et al. N Engl J Med. 2006 Nov 23;355(21):2203-16.

0 1 2
ACUITY: Net Clinical Outcome CompositeUFH/Enoxaparin + IIb/IIIa vs. Bivalirudin AloneUFH/Enoxaparin + IIb/IIIa vs. Bivalirudin Alone
Yes (n = 3197)No (n = 6008)
Low (0-2) (n = 1291)Intermed (3-4) (n = 4407)
High (5-7) (n = 2449)
Elevated (n = 5368)Normal (n = 3841)
Risk ratio±95% CI
Risk ratio±95% CI
BivalAlone
UFH/Enox+ IIb/IIIa
9.2%11.3%
12.2%11.1%
P Pint
0.76 (0.65-0.89)1.02 (0.86-1.21)
12.2%7.1%
13.3%9.4%
0.92 (0.80-1.06)0.75 (0.61-0.93)
0.230.01
<0.0010.83
0.35
0.02
0.18
13.0%8.6%
13.7%10.6%
0.96 (0.80-1.14)0.81 (0.69-0.95)
0.610.01 0.42
Biomarkers (CK/Trop)
ST Deviation
TIMI Risk Score
Pre Thienopyridine
6.4% 10.2% 0.63 (0.43-0.91) 0.019.4% 10.2% 0.92 (0.77-1.10) 0.34
13.9% 15.2% 0.92 (0.76-1.11) 0.36
Yes (n = 5192)No (n = 4023)
RR (95% CI)
Bivalirudin alone betterBivalirudin alone better UFH/Enox + IIb/IIIa betterUFH/Enox + IIb/IIIa better
Stone GW, et al. N Engl J Med. 2006 Nov 23;355(21):2203-16.

0 1 2
ACUITY: Net Clinical Outcome CompositeUFH/Enoxaparin + IIb/IIIa vs. Bivalirudin AloneUFH/Enoxaparin + IIb/IIIa vs. Bivalirudin Alone
Bivalirudin alone betterBivalirudin alone better UFH/Enox + IIb/IIIa betterUFH/Enox + IIb/IIIa better
BivalAlone
UFH/Enox+ IIb/IIIa
P Pint
0.59
11.6% 13.3% 0.87 (0.75-1.00) 0.09
10.6% 18.2% 0.97 (0.75-1.26) 0.84
5.1% 6.5% 0.78 (0.58-1.04) 0.09
0.62
8.3% 9.8% 0.85 (0.67-1.06) 0.15
9.2% 9.4% 0.98 (0.78-1.23) 0.86
12.5% 14.4% 0.87 (0.73-1.05) 0.14
0.56
9.1% 10.0% 0.91 (0.73-1.12) 0.36
6.7% 7.1% 0.94 (0.80-1.10) 0.46
10.6% 12.6% 0.84 (0.65-1.10) 0.21
RR (95% CI)
PCI (n = 5170)
CABG (n = 1048)
Medical (n = 2989)
No prior AT (n = 3290)
Consistent Rx (n = 5519)
Crossover (n = 3211)
A-thrombin crossover
Early (<3.0 h)
Intermediate (3.0-19.7 h)
Late (≥19.7 h)
Risk ratio±95% CI
Risk ratio±95% CI
Actual treatment
Rand. to angio/interv.tertiles
Stone GW, et al. N Engl J Med. 2006 Nov 23;355(21):2203-16.

Summary
• Fondaparinux reduces bleeding and mortality in patients with NSTEACS compared with enoxaparin including those undergoing early intervention (<24 hours)
• Standard UFH +/- GPI is recommended in those receiving a PCI
• Bivalirudin is no different than UFH/enoxaparin in reducing ischemic outcomes or bleeding in presence of a GPI
• Bivalirudin reduces bleeding compared with UFH/enox + GPI but patients need to be pre-treated with a thienopyridine to maintain efficacy
• The two agents may be complementary—fondaparinux for initial upstream therapy and bivalirudin in those needing a PCI.