
Sexual Safety of Mental Health Consumers Guidelines · Sexual Safety of Mental Health Consumers...
86
Sexual Safety of Mental Health Consumers Guidelines Summary The purpose of these guidelines is to - Support mental health services to meet their responsibilities in relation to the sexual safety of mental health consumers through the provision of practical advice and strategies; - Promote sexual safety to key stakeholders – health staff and managers, consumers and their families and carers; - Clearly outline the information consumers and their families and carers should receive about their rights and obligations in relation to the sexual safety of consumers; and- Improve collaboration and strengthen relationships between mental health services and Sexual Assault Services. Document type Guideline Document number GL2013_012 Publication date 12 November 2013 Author branch Mental Health Branch contact 02 9391 9306 Review date 30 May 2020 Policy manual Patient Matters File number H13/72517 Previous reference N/A Status Review Functional group Clinical/Patient Services - Mental Health Applies to Local Health Districts, Board Governed Statutory Health Corporations, Chief Executive Governed Statutory Health Corporations, Specialty Network Governed Statutory Health Corporations, Community Health Centres, NSW Ambulance Service, Ministry of Health, Public Hospitals Distributed to Public Health System, Ministry of Health Audience All Staff;Clinical;Allied Health;Nursing;Emergency Departments Guideline Secretary, NSW Health
Transcript of Sexual Safety of Mental Health Consumers Guidelines · Sexual Safety of Mental Health Consumers...

Sexual Safety of Mental Health Consumers Guidelines
Summary The purpose of these guidelines is to - Support mental health services to meet their responsibilities in relation to the sexual safety of mental health consumers through theprovision of practical advice and strategies; - Promote sexual safety to key stakeholders – health staff and managers, consumers and their families and carers; - Clearly outline the information consumers and their families and carers should receive about their rights and obligations in relation to the sexual safety of consumers;and- Improve collaboration and strengthen relationships between mental health services and Sexual Assault Services.
Document type Guideline
Document number GL2013_012
Publication date 12 November 2013
Author branch Mental Health
Branch contact 02 9391 9306
Review date 30 May 2020
Policy manual Patient Matters
File number H13/72517
Previous reference N/A
Status Review
Functional group Clinical/Patient Services - Mental Health
Applies to Local Health Districts, Board Governed Statutory Health Corporations, Chief Executive Governed Statutory Health Corporations, Specialty Network Governed Statutory Health Corporations, Community Health Centres, NSW Ambulance Service, Ministry of Health, Public Hospitals
Distributed to Public Health System, Ministry of Health
Audience All Staff;Clinical;Allied Health;Nursing;Emergency Departments
Guideline
Secretary, NSW Health

GUIDELINE SUMMARY
GL2013_012 Issue date: November-2013 Page 1 of 2
SEXUAL SAFETY OF MENTAL HEALTH CONSUMERS GUIDELINES
PURPOSE The Sexual Safety of Mental Health Consumers Guidelines provide practical information, advice and strategies to help mental health services maintain the sexual safety of mental health consumers and respond appropriately to incidents that breach or compromise this safety. Sexual safety refers to the recognition, maintenance and mutual respect of the physical (including sexual), psychological, emotional and spiritual boundaries between people.
These Guidelines should be read in conjunction with Policy Directive PD 2013_038, which mandates the minimum requirements that must be met in this regard.
KEY PRINCIPLES The key principles in these Guidelines, and the associated Policy Directive, are listed below.
1. All mental health consumers are entitled to be sexually safe.
2. Mental health services take appropriate action to prevent and appropriately respond to sexual safety incidents.
3. Mental health services support mental health consumers to adopt practices and behaviours that contribute to their sexual safety, both within the mental health service environment and within the community.
4. Mental health services develop individual sexual safety standards appropriate for their particular setting, in collaboration with all members of the service including staff, consumers, carers, clinicians, advocates etc.
5. The physical environment of the mental health service takes account of the need to support the sexual safety of mental health consumers in its layout and use, particularly in regard to gender sensitivity.
6. Mental health consumers, and their families, carers and advocates, are given access to clear information regarding the consumer’s rights, advocacy services, and appropriate mechanisms for complaints and redress regarding sexual safety issues.
7. Mental health service staff and clinicians foster a compassionate and open culture that encourages reporting of incidents relating to the sexual safety of mental health consumers.
8. Disclosures from mental health consumers about incidents that compromise or breach their sexual safety are taken seriously and addressed promptly and empathetically, regardless of the identity or affiliation of the alleged perpetrator, and with the utmost regard for the complainant’s privacy and dignity, past trauma, cultural background, gender, religion, sexual identity, age and the nature of their illness.
9. Mental health service staff are provided with training and education to enable them to:
a. Effectively promote strategies to support sexual safety and prevent sexual assault and harassment
b. Respond appropriately and sensitively to sexual safety issues involving mental health consumers, both within the service environment and within the community
c. Integrate trauma-informed care principles into all aspects of treatment.

GUIDELINE SUMMARY
GL2013_012 Issue date: November-2013 Page 2 of 2
10. Mental health consumers are supported to access education to enable them to:
a. Effectively recognise and respond to behaviours, both their own and other people’s, that may compromise or breach their own or another person’s sexual safety
b. Develop self-protective behaviours
c. Establish and maintain good sexual health.
USE OF THE GUIDELINE These Guidelines apply to NSW Health services providing specialist mental health care in all settings including acute inpatient, non-acute inpatient, rehabilitation and community,and staff working for such services.
Where a service has a mix of acute and non-acute consumers in the one unit or facility, it is the responsibility of the service to ensure they implement these Guidelines and the associated Policy Directive in a way that addresses this mix.
The scope of the Guidelines does not extend to providing practical and detailed guidance about how services can best manage issues relating to sexual activity involving consumers. Services are encouraged to develop their own local policies and protocols in relation to this area, being mindful of the policy approach advocated within these Guidelines regarding the right of consumers to express their sexuality safely and respectfully in the appropriate settings.
The Policy Directive outlines a number of Responsibilities and Minimum Requirements for:
• all Mental Health Services, (pg 11)
with additional Responsibilities and Minimum Requirements specific to:
• acute inpatient mental health settings (pg 13)
• non-acute and residential mental health settings (pg 14)
• community mental health settings (pg 15).
Implementation will be staged over a two year period, and must be completed by June of 2014.
Implementation by individual services should be monitored by each Local Health District via the Individual Service Implementation Monitoring Form at Appendix IV of the associated Policy Directive.
REVISION HISTORY Version Approved
by Amendment notes
November 2013 (GL2013_012)
Director General
Inclusion of all mental settings, education, prior history, gender sensitive practices, safe sex practices, respected disclosure, trauma informed care approach and identification of specific incident types.
January 2005 (GL2005_049)
Director General
New policy.
ATTACHMENTS 1. Sexual Safety of Mental Health Consumers: Guidelines
Sexual Safety of Mental Health Consumers
GuidelinesPractical information, advice and strategies to help mental health
services maintain the sexual safety of mental health consumers
NSW MINISTRY OF HEALTH
73 Miller Street
NORTH SYDNEY NSW 2060
Tel. (02) 9391 9000
Fax. (02) 9391 9101
TTY. (02) 9391 9900
www.health.nsw.gov.au
This work is copyright. It may be reproduced in whole or in part for study
training purposes subject to the inclusion of an acknowledgement of the source.
It may not be reproduced for commercial usage or sale. Reproduction for
purposes other than those indicated above requires written permission from the
NSW Ministry of Health.
© NSW Ministry of Health 2013
GL2013_012
SHPN: (MHDAO) 120421
ISBN: 978-1-74187-865-3
For further copies of this document please contact:
Better Health Centre – Publications Warehouse
PO Box 672
North Ryde BC, NSW 2113
Tel. (02) 9887 5450
Fax. (02) 9887 5452
Further copies of this document can be downloaded from the
NSW Ministry of Health website www.health.nsw.gov.au
November 2013

Sexual Safety of Mental Health Consumers Guidelines NSW HealtH PaGe 1
Contents
1. Introduction ........................................... 31.1 Definitions ............................................... 3
1.2 Principles of care ..................................... 5
1.3 Scope ..................................................... 5
1.3.1 Settings ................................................ 5
1.3.2 Focus .................................................... 6
1.3.3 Population groups ................................ 6
1.4 Purpose and intended outcomes .............. 6
1.5 Background ............................................. 7
1.6 Development process ............................. 7
1.6.1 Expert practitioners .............................. 7
1.6.2 Literature review ................................... 7
1.6.3 Consultation ......................................... 7
2. Sexual safety and mental health ............ 92.1 Defining sexual safety .............................. 9
2.2 The importance of sexual safety for
people with a mental illness ..................... 9
2.3 Sexual safety incident types ................... 10
2.3.1 Sexual assault and harassment ........... 10
2.3.2 Consensual sexual activity in an
inappropriate context or setting ..........11
2.3.3 Sexually disinhibited behaviour ............12
2.4 Rights and responsibilities regarding
sexual safety ...........................................12
2.4.1 Mental health consumers in all
settings have the right to: ....................12
2.4.2 All members of a mental health
service have the right to: .....................13
2.4.3 Mental health services in all settings
have a responsibility to: .......................13
2.4.4 All members of a mental health
service have a responsibility to: ............13
2.5 Relevant legislation, standards/rights
and policies ............................................13
2.5.1 Legislation ...........................................13
2.5.2 Standards and rights ........................... 14
2.5.3 Associated NSW Health policies ......... 14
3. Fostering a culture that supports sexual safety .......................................... 163.1 Training and education .......................... 16
3.1.1 Supporting mental health staff .......... 16
3.1.2 Empowering consumers .....................17
3.1.3 Recognising families, friends
and carers .......................................... 18
3.2 Promoting sexual safety .........................19
3.3 The importance of collaboration ............19
3.3.1 Consumers ......................................... 19
3.3.2 Families and carers ............................. 20
3.3.3 General practitioners (GPs) ................. 20
3.3.4 NSW Health Sexual Assault Services ... 20
3.3.5 NSW Police Force................................ 21
3.3.6 Other agencies ................................... 21
3.3.7 Partner programs/Community
managed organisations (CMOs) .......... 22
4. Preventing a Sexual Safety Incident ... 244.1 Sexual assault and harassment ............... 24
4.1.1 Assessing vulnerability ....................... 24
4.1.2 Taking an appropriate sexual assault
and harassment history ...................... 24
4.1.3 Recognising offender tactics ............... 26
4.1.4 The role of gender sensitivity .............. 26
4.1.5 Practical security measures ................. 27
4.1.6 Maintaining professional boundaries . 28
4.2 Consensual sexual activity in an
inappropriate context or setting ............. 30
4.2.1 Sexual safety standards ...................... 30
4.2.2 Addressing sexuality needs ................ 30
4.3 Sexually disinhibited behaviour ............. 31

PaGe 2 NSW HealtH Sexual Safety of Mental Health Consumers Guidelines
5. Responding to a Sexual Safety Incident .................................................. 35
5.1.1 When there is disclosure or
acknowledgement of sexual assault
or harassment .................................... 35
5.1.2 When sexual assault or harassment
is suspected but not disclosed .............41
5.2 Consensual sexual activity in an
inappropriate context or setting ............. 43
5.2.1 Understanding consent and
capacity .............................................. 43
5.2.2 Staff attitudes .................................... 44
5.3 Sexually disinhibited behaviour .............. 44
6. Reporting and Recording .................... 476.1.1 Reporting ............................................. 47
6.1.2 Recording .......................................... 49
6.2 Consensual sexual activity in an
inappropriate context or setting ............. 50
6.2.1 Reporting .......................................... 50
6.2.2 Recording ........................................... 50
6.3 Sexually disinhibited behaviour ..............51
6.3.1 Reporting ...........................................51
6.3.2 Recording ............................................51
7. Highly vulnerable groups ..................... 527.1 Consumers who are Aboriginal and
Torres Strait Islander ............................. 52
7.2 Consumers who are children or
young people ........................................ 53
7.3 Consumers from a culturally and
linguistically diverse background ............ 54
7.4 Consumers with Intellectual
Disability ................................................ 54
7.5 Gay, Bisexual, Lesbian and
Transgender Consumers ........................ 55
7.6 Older consumers .................................. 56
Appendices .................................................. 57Appendix A – Example Sexual Safety Standards
of Behaviour ...................................... 58
Appendix B – Charter of Victims Rights .................... 59
Appendix C – Relevant standards and the
legislative framework ..........................61
Appendix D – Information about support options
for consumers who have experienced
sexual assault .................................... 64
Appendix E – Information about reporting to
Police for consumers who have
experienced sexual assault .................. 65
Appendix F – Example posters on accessing
support............................................... 66
Appendix G – Sexual Assault Screening Tool ........... 68
Appendix H – Examples of sexualised behaviour
by healthcare professionals towards
consumers or their carers ................... 70
Appendix I – Responding to a disclosure of sexual
assault – key actions ........................... 71
Appendix J – Responding to a disclosure of recent
sexual assault – quick checklist ............ 73
Appendix K – Follow up medical exams required
when a person has been sexually
assaulted .............................................74
Appendix L – Reporting process for an incident
of sexual assault ............................... 75
Appendix M – Information about Managing
Disinhibited Behaviour ....................... 76
References .................................................... 77

Sexual Safety of Mental Health Consumers Guidelines NSW HealtH PaGe 3
SECTION 1
Introduction
1.1 Definitions
For the purpose of this resource, the following definitions apply.
Term Meaning
Consensual sexual activity
Sexual activity that occurs after mutual sexual consent has been provided by those involved. Also see ‘sexual consent’.
Consumer Someone with a mental illness or disorder that uses a mental health service.
Continuum of sexual violence
A range or succession of related sexual behaviours involving intrusion and violation, extending from unwanted sexual comments to unwanted touching of a sexual nature and rape.
Gender sensitive practices
The different needs of men and women are considered in all aspects of service planning and service delivery.
Intra-familial sexual assault
Any sexual activity between closely related persons, normally within the immediate family, which is either illegal or socially forbidden. Immediate family can include a parent, son, daughter, sibling (including a half-brother or half-sister), grandparent or grandchild, being such a family member from birth.
Informed decision A decision made by a consumer who understands the nature, extent, or probable consequences of the decision, and can make a rational evaluation of the risks and benefits of alternatives. The decision cannot be considered informed unless the consumer is mentally competent and the decision made voluntarily.
Masturbation The stimulation of one’s own genital organs, usually to orgasm, by manual contact or means other than sexual intercourse.
Mental health service Any establishment or any unit of an establishment that has the primary function of providing mental health care.
Mental health workers/staff
Any person working in a permanent, temporary, casual, term appointment or honorary capacity within a NSW Health mental health organisation. This includes volunteers, consumer advocates, contractors, visiting practitioners, students, consultants and researchers performing work within NSW Health facilities.
Mentally competent The capacity to understand information, make decisions, and act reasonably.
Perpetrator/offender Someone who has breached the sexual safety of a consumer.
Sexual abuse See ‘sexual assault’.
Sexual activity Activity of a sexual nature with oneself (masturbation) or another (sexual touching, sexual intercourse, oral sex).
Sexual assault Sexual assault occurs when:
■ a person is forced, coerced or tricked into sexual acts against their will or without their consent, or
■ a child or young person under 16 years of age is exposed to sexual activities, or
■ a young person over 16 and under 18 years of age is exposed to sexual activities by a person with whom they have a relationship of ‘special care’ e.g. step-parent, guardian, foster parent, health practitioner, employer, teacher, coach, priest, etc.
Sexual coercion The practice of gaining involuntary permission to gain access to a person for the purposes of sexual gratification. Methods used include psychological inducements and physical force e.g. trickery, bribes, inducements (money, food, drugs, etc), offers of care, love, protection, meeting emotional needs, threats, making captive. Coercion is intrinsic in child sexual assault and to the exploitation of other vulnerable persons.

PaGe 4 NSW HealtH Sexual Safety of Mental Health Consumers Guidelines
Term Meaning
Sexual consent To give permission for something of a sexual nature to happen, agree to do something of a sexual nature, or accept something of a sexual nature proposed or desired by another. Consent can only be considered valid if:
■ the consumer is an adult (16 years of age and over) that is mentally competent to consent, and
■ where the consumer is between 16 and 18 years of age, there is no ‘special care’ relationship with the person to whom they have consented e.g. step-parent, guardian, foster parent, health practitioner, employer, teacher, coach, priest, etc, and
■ the consent is given voluntarily and without coercion.
Consent must be provided each time and not be based on prior behaviour.
Sexually disinhibited behaviour
Poorly controlled behaviour of a sexual nature, where sexual thoughts, impulses or needs are expressed in a direct or disinhibited way, such as in inappropriate situations; at the wrong time; or with the wrong person.
Sexual harassment Unwelcome conduct of a sexual nature which makes a person feel offended, humiliated and/or intimidated where that reaction is reasonable in the circumstances. Can involve physical, visual, verbal or non-verbal conduct.
Sexual health A state of physical, emotional, mental and social well-being related to sexuality, including the absence of disease, dysfunction or infirmity; a positive and respectful approach to sexuality and sexual relationships; the possibility of having pleasurable and safe sexual experiences, free from coercion, discrimination and violence, and; respect for the sexual rights of all persons. (World Health Organisation)
Sexual safety The recognition, maintenance and mutual respect of the physical, psychological, emotional and spiritual boundaries between people.
Sexual safety incident The term used to refer to an incident that breaches or compromises the sexual safety of a consumer, and which is recognised as either sexual assault or harassment, consensual sexual activity in an inappropriate setting or sexually disinhibited behaviour.
Sexual violence See ‘sexual assault’.
‘Special care’ relationship
A relationship that exists between a young person 16–18 years of age and a person in a position of influence or authority over that young person. This group could include:
■ step-parents
■ guardians
■ foster parents
■ health practitioners
■ employers
■ teachers
■ sporting coaches
■ priests
Survivor A person who has been sexually assaulted or has experienced sexual harassment. Also see ‘victim’.
Trauma informed care Mental health treatment that is directed by:
■ a thorough understanding of the profound neurological, biological, psychological and social effects of trauma and violence on the individual; and
■ an appreciation for the high prevalence of traumatic experiences in persons who receive mental health services. (Jennings, 2004)
Victim A person who has been sexually assaulted or has experienced sexual harassment. Also see ‘survivor’.

Sexual Safety of Mental Health Consumers Guidelines NSW HealtH PaGe 5
1.2 Principles of care
The following principles have been developed to provide
a clear foundation for the establishment and maintenance
of the sexual safety of consumers in all mental health
service settings.
1. All mental health consumers are entitled to be
sexually safe.
2. Mental health services take appropriate action to
prevent and appropriately respond to sexual safety
incidents.
3. Mental health services support mental health
consumers to adopt practices and behaviours that
contribute to their sexual safety, both within the
mental health service environment and within the
community.
4. Mental health services develop individual sexual safety
standards appropriate for their particular setting, in
collaboration with all members of the service – staff,
consumers, carers, clinicians, advocates etc.
5. The physical environment of the mental health service
takes account of the need to support the sexual
safety of mental health consumers in its layout and
use, particularly in regard to gender sensitivity.
6. Mental health consumers, and their families, carers
and advocates, are given access to clear information
regarding the consumer’s rights, advocacy services,
and appropriate mechanisms for complaints and
redress regarding sexual safety issues.
7. Mental health service staff and clinicians foster a
compassionate and open culture that encourages
reporting of incidents relating to the sexual safety of
mental health consumers.
8. Disclosures from mental health consumers about
incidents that compromise or breach their sexual
safety are taken seriously and addressed promptly and
empathetically, regardless of the identity or affiliation
of the alleged perpetrator, and with the utmost
regard for the complainant’s privacy and dignity, past
trauma, cultural background, gender, religion, sexual
identity, age and the nature of their illness.
9. Mental health service staff are provided with training
and education to enable them to:
a. Effectively promote strategies to support sexual
safety and prevent sexual assault and harassment;
and
b. Respond appropriately and sensitively to sexual
safety issues involving mental health consumers,
both within the service environment and within
the community; and
c. Integrate trauma-informed care principles into all
aspects of treatment.
10. Mental health consumers are supported to access
education to enable them to:
a. Effectively recognise and respond to behaviours,
both their own and other people’s, that may
compromise or breach their own or another
person’s sexual safety;
b. Develop self-protective behaviours; and
c. Establish and maintain good sexual health.
1.3 Scope
1.3.1 SettingsThese guidelines apply to NSW Health services providing
specialist mental health care in all settings – acute
inpatient, non-acute inpatient, rehabilitation and
community – and staff working for such services.
The guidelines outline the recommended policy approach
to maintaining the sexual safety of consumers and
responding appropriately to incidents that breach or
compromise this safety. They should be read in
conjunction with Policy Directive PD 2013_038, which
mandates the minimum requirements that must be met in
this regard.
It should be noted that where a service has a mix of acute
and non-acute consumers in the one unit or facility, it is
the responsibility of the service to ensure they implement
these guidelines and the associated Policy Directive in a
way that addresses this mix.

PaGe 6 NSW HealtH Sexual Safety of Mental Health Consumers Guidelines
1.3.2 FocusThe focus of these guidelines is sexual safety for
consumers. Sexual safety refers to the recognition,
maintenance and mutual respect of the physical (including
sexual), psychological, emotional and spiritual boundaries
between people. Advice regarding how to manage
incidents of sexual assault or harassment that do not
involve consumers of the service can be accessed from a
range of NSW Health policies, including Complaints
Management Policy PD2006_073 and Criminal
allegations, charges and convictions against employees
PD2006_026. See Section 2.5.3 Associated NSW Health
Policies for further information.
The scope of these guidelines does not extend to
providing practical and detailed guidance about how
services can best manage issues relating to sexual activity
involving consumers. Services are encouraged to develop
their own local policies and protocols in relation to this
area, being mindful of the policy approach advocated
within these guidelines regarding the right of consumers
to express their sexuality safely and respectfully in the
appropriate settings.
However, NSW Health recognises that good sexual health
and healthy and respectful sexual relationships are important
and intrinsically linked to sexual safety. For this reason,
information about sexual health issues is included where
appropriate, and sexuality and sexual health education for
consumers and training for staff is acknowledged as an
important component of an overall sexual safety strategy.
1.3.3 Population groupsInformation specific to the needs of consumers who are
particularly vulnerable, including children and young
people, is provided in Section 7.
At relevant points throughout the document advice is
also provided around the responsibilities of service
providers in relation to the safety, welfare and wellbeing
of the children and young people who may be in contact
with or in the care of consumers using an adult mental
health care service.
The reforms to the NSW child protection system under
Keep Them Safe: A Shared Approach to Child Wellbeing
2009–2014 mandates that every health worker that
comes into contact with a child or young person has
a responsibility to protect their health, safety, welfare
and wellbeing.
The NSW Health Frontline Policies and Procedures for
Child Protection and Wellbeing (revised procedures being
finalised at the time of printing) operationalise the
responsibilities of NSW Health under the Children and
Young Persons (Care and Protection) Act 1998 and are
relevant to all health workers and services, including
those providing services to adult clients who may be
parents or carers.
1.4 Purpose and intended outcomes
The purpose of these guidelines is to:
■ Support mental health services to meet their
responsibilities in relation to the sexual safety of
mental health consumers through the provision of
practical advice and strategies.
■ Promote sexual safety to key stakeholders – health
staff and managers, consumers and their families
and carers.
■ Increase the awareness of all stakeholders regarding
the importance of:
– Training for staff to enable them to prevent and
respond to sexual safety incidents; and
– Access to education for consumers to enable them
to recognise behaviours that could compromise or
breach their sexual safety, develop self-protective
behaviours and attain good sexual health.
■ Clearly outline the information consumers and their
families and carers should receive about their rights
and obligations in relation to the sexual safety of
consumers.
■ Improve collaboration and strengthen relationships
between mental health services and Sexual Assault
Services.
The intended outcomes of the guidelines are:
■ Prioritisation of the sexual safety of mental health
consumers by mental health services.
■ An increase in the number of mental health staff
who are appropriately trained to manage sexual
safety issues.
■ Reduction of the number of sexual safety incidents in
inpatient and rehabilitation units.
■ Greater promotion of the responsibilities of mental
health services in relation to sexual safety, including their
role in supporting consumers within the community.
■ Awareness by mental health staff of the benefits of

Sexual Safety of Mental Health Consumers Guidelines NSW HealtH PaGe 7
helping consumers to access education on sexuality
and sexual health issues.
■ Awareness by consumers and their families and carers
of the rights and responsibilities of consumers
regarding their sexual safety.
■ A greater sense of confidence within the community
regarding the sexual safety of mental health consumers.
■ Stronger collaboration between Sexual Assault
Services and mental health services.
■ Consideration of prior sexual trauma of consumers
within the treatment context.
1.5 Background
These guidelines supersede the Guidelines for the
Promotion of Sexual Safety in NSW Mental Health
Services, which were first released in 1999 and revised
and re-released in 2005.
Since that time, feedback to the Mental Health and Drug
and Alcohol Office (MHDAO) and the Clinical Advisory
Council (CAC) has indicated that the guidelines in their
current format may not have been providing the
appropriate level of support to mental health service staff
regarding how to respond to sexual safety issues.
Points raised in relation to the guidelines included:
■ Insufficient information provided regarding how staff
should respond to particular sexual safety issues (e.g.
prior sexual assault trauma; consensual sex;
identifying offender tactics etc)
■ Limited scope – only applicable to inpatient units
■ Did not take account of the differing needs of
particular groups, such as children and adolescents,
older people, Gay, Lesbian, Bisexual and Transgender
(GLBT) people, Aboriginal people, culturally and
linguistically diverse people etc.
■ Out of date information regarding reporting
procedures, including the use of mental health clinical
documentation (formerly MH-OAT)
In response to this, CAC agreed to review of the
guidelines with a view to improving their effectiveness,
and this action was endorsed by the Mental Health
Program Council (MHPC). This also provided an
opportunity to develop a Policy Directive to improve
consistency across services and clarity around
responsibilities as well as to review and revise the current
format and content of the sexual safety training provided
to mental health services.
As the new guidelines are about promoting sexual safety,
and preventing and appropriately responding to sexual
safety incidents in all settings, the title has been changed
to Sexual Safety of Mental Health Consumers to
reflect this.
1.6 Development process
1.6.1 Expert practitionersA range of expert practitioners provided input and
guidance throughout the development process, including
individuals from the following sectors:
■ Sexual assault prevention and response education
■ Sexual Assault Services
■ Community mental health
■ Inpatient mental health
■ Mental health rehabilitation
■ Violence prevention
Consumer representatives from the NSW Consumer
Advisory Group – Mental Health (Inc) also contributed to
the development of the framework and content of this
document.
1.6.2 Literature reviewA literature review was undertaken, primarily utilising
electronic research methods, regarding sexual safety
issues within a mental health service context that
encompassed national and international literature.
The review also identified strategies and recommendations
for improving sexual safety in mental health services and
examples of tools, guidelines and policies that would
support better management of sexual safety issues
for consumers.
This information, along with additional research
undertaken around the importance of sexual ethics and
sexual health information for consumers in preventing
sexual assault and harassment, provided a framework for
development of the guidelines.
1.6.3 ConsultationConsultation was considered a critical component in the
development of the guidelines.

PaGe 8 NSW HealtH Sexual Safety of Mental Health Consumers Guidelines
A reference group, comprised of key stakeholder groups
and individuals, provided regular feedback to the project
throughout the development process. Sectors represented
included:
■ Forensic mental health
■ Children and adolescent mental health
■ Older people’s mental health
■ Carers and families
■ Multicultural mental health
■ Aboriginal mental health
■ Mental health consumers
■ Patient safety
Further consultation was also undertaken with the
following stakeholder groups at fundamental stages:
■ ACON
■ Aboriginal Health and Medical Research Council
■ Adults Surviving Child Abuse
■ Ministry of Health Mental Health Clinical Advisory
Council
■ Ministry of Health Mental Health Program Consumer
Sub-committee
■ NSW Police Force
■ NSW Rape Crisis Centre
Academics that reviewed and endorsed the guidelines
include:
■ Professor Moira Carmody, University of Western
Sydney’s Centre for Educational Research, former
member of the National Council to Reduce Violence
against Women and their Children, national expert on
sexual assault prevention education
■ Dr Lesley Laing, Senior Lecturer, Undergraduate and
Pre-service Programs, Program Co-director, Faculty of
Education and Social Work, University of Sydney,
former Director of the Education Centre Against
Violence (ECAV)

Sexual Safety of Mental Health Consumers Guidelines NSW HealtH PaGe 9
SECTION 2
Sexual Safety and Mental Health
SECTION 2
Sexual Safety and Mental Health
2.1 Defining sexual safety
Sexual safety refers to the respect and maintenance of an
individual’s physical (including sexual) and psychological
boundaries.
Core elements of sexual safety in a mental health service
include:
■ A safe physical environment
■ Recognition of the rights of consumers to physical
and psychological safety
■ Assessment of the consumer’s vulnerability or
potential to harm others
■ Identification of the consumer’s past experience of
sexual assault
■ Consideration of how the service environment could
be improved, including adoption of gender-sensitive
practices
■ Monitoring of professional boundaries
■ Management of sexually disinhibited behaviour and
prevention of sexual activity in an inappropriate
context or setting
■ Provision of professional development for staff
■ Appropriately responding to sexual assault and
harassment
■ Proper reporting and recording of sexual safety
incidents, and feeding back outcomes of cause
analysis into safety improvement processes at the
service level.
2.2 The importance of sexual safety for people with a mental illness
Mental health consumers are exposed to a number of
potential risks, particularly when they are acutely unwell.
Often these risks are related to their own behaviour or to
the behaviour of other consumers, or are a direct result
of their mental illness. Others relate to safety risks from
their care or treatment. This makes mental health
consumers a particularly vulnerable group within the
health sector.
Mental health consumers can be more vulnerable to
sexual assault in particular for a number of reasons,
such as:
■ Low self esteem and confidence
■ Social isolation and loneliness
■ Poor social and communication skills
■ Impaired judgement, due to their mental illness,
medication(s) prescribed for their illness or drug and
alcohol abuse, or a combination of these
■ Interruption of usual developmental stages due to
onset of mental illness combined with limited
education regarding relationships, appropriate sexual
behaviour and sexual safety.
In the community, this complex mix can also include an
increased likelihood of living in poverty with fewer
resources and options to change their living circumstance
and lack of access to outside assistance. In an inpatient or
residential rehabilitation setting, the power imbalance
between staff and consumers, either real or perceived,
can lead to a fear of retribution if the disclosure involves
a staff member.
According to research, the prevalence of people with a
mental illness who have been exposed to or have
experienced personal trauma, including sexual abuse and
violence, is high. There is also evidence to suggest that:
■ The influence of violence can persist long after the
abuse has stopped.
■ The more serious the abuse, the greater its impact on
physical and mental health.
■ The impact over time of different types and multiple
episodes of abuse appear to be cumulative (Evans
2007; Golding 1999; Taft 2003; WHO 2000).
■ Suicidal ideation is more common among victims/
survivors of sexual assault than the general population
(Stepakoff, 1998) and younger victims/survivors may
be at particular risk of actually attempting suicide
following rape (Petrak, 2002).

PaGe 10 NSW HealtH Sexual Safety of Mental Health Consumers Guidelines
This highlights the need for greater awareness of the
sexual vulnerability of people with a mental illness, and
the link between mental health issues and prior sexual
assault and violence.
It also confirms the important responsibility mental health
services have to ensure that policies and procedures are in
place to support consumers to be sexually safe, and that
care and treatment plans take account of sexual safety
issues and adopt a trauma-informed care approach.
2.3 Sexual safety incident types
For the purposes of these guidelines, the types of
behaviour that can breach and/or compromise the sexual
safety of a mental health consumer have been split into
the following three incident types:
■ Sexual assault and harassment
■ Consensual sexual activity in an inappropriate context
or setting
■ Sexually disinhibited behaviour
Within the context of these guidelines, each of these
behaviours is referred to as a ‘sexual safety incident’.
2.3.1 Sexual assault and harassment
Definitions
Sexual assault is a broad term used to describe a range
of sexual acts committed against a person without their
consent. It occurs when:
■ a person is forced, coerced or tricked into sexual acts
against their will or without their consent, or
■ a child or young person under 16 years of age is
exposed to sexual activities, or
■ a young person between 16 and 18 years of age is
exposed to sexual activities by a person with whom
they have a relationship of ‘special care’ e.g.. step-
parent, guardian, foster parent, health practitioner,
employer, teacher, coach, priest, etc.
Sexual assault is a crime of violence with serious
consequences. Conviction for sexual assault is punishable
by law and depending on the category of assault, can
carry a gaol term. The Crimes Act 1900 sets out offences
of a sexual nature at Part 3, Division 10. See Appendix C
– Relevant standards and the legislative framework for
further information about what this Act says.
Sexual harassment can occur between any combinations
of individuals and is defined by the Australian Human
Rights Commission as ‘unwelcome conduct of a sexual
nature which makes a person feel offended, humiliated
and/or intimidated where that reaction is reasonable in
the circumstances.’
Sexual harassment can involve conduct such as:
■ unwelcome touching, hugging or kissing
■ staring or leering
■ suggestive or offensive comments or jokes
■ unwanted invitations to go out on dates or requests
for sex
■ intrusive questions about an individual’s private life
or body
■ unnecessary familiarity, such as deliberately brushing
up against someone
■ insults or taunts of a sexual nature
■ sexually explicit emails or SMS messages
■ behaviour which would also be an offence under the
criminal law, such as physical assault, indecent
exposure, sexual assault, stalking or obscene
communications.
Sexual harassment is not sexual interaction, flirtation,
attraction or friendship which is invited, mutual,
consensual or reciprocated.
Sexual assault and sexual harassment potentially affect all
members of the community. However, there are certain
groups that are more likely to be targeted than others,
and this includes men and women with a mental
impairment (Cook, 2001).
Beyond Belief, Beyond Justice (Goodfellow and Camilleri,
2003) notes that women with cognitive impairment
(including women with cognitive impairment from mental
illness) are especially vulnerable to abuse, particularly
those who are homeless or living in boarding houses or
institutional settings.
Impact
Sexual assault and sexual harassment for those who
experience it can affect their short and long-term physical
and mental health, their economic wellbeing, and their
feelings of safety.
Of all the traumatic stressors researched, trauma of sexual
assault is the strongest predictor of Post Traumatic Stress

Sexual Safety of Mental Health Consumers Guidelines NSW HealtH PaGe 11
Disorder and is associated with increased rates of other
mental disorders including depression, anxiety, anti-social
personality disorder, substance dependence, suicidal
ideation and suicide attempts.
The immediate emotional consequences of sexual assault
might include terror, anguish, disgust, personal vulnerability,
shock, numbness and denial. The long-term emotional
impact can be experienced in many ways including:
■ Disturbed sleep
■ Frequent nightmares
■ Flashbacks to the assault
■ Embarrassment, shame, eroded self-esteem
■ Poor body image, weight gain used as a protective
mechanism
■ Depression and anxiety
■ Hostility, anger, and behavioural problems
■ Self-harming and compulsive behaviours (including
self-mutilation, reckless behaviour, drug and/or
alcohol abuse)
■ Relationship difficulties and loss of sexual confidence
■ Feelings of isolation, guilt or self-blame, suicidal
thoughts and suicide attempts
Overall, the reactions to sexual assault of both women
and men tend to be similar (Crome, 2006), but research
addressing the impact on men has been limited.
Some impacts of particular relevance to males include
sexual orientation conflict, homophobia, male specific
sexual dysfunction and compulsions, and masculine
identity confusion.
Sexual harassment is a type of sexual assault, and victims/
survivors of severe or chronic sexual harassment can
suffer the same psychological effects as victims/survivors
of sexual assault.
2.3.2 Consensual sexual activity in an inappropriate context or setting
Definitions
For the purposes of the guidelines, consensual sexual
activity is any activity of a sexual nature (sexual touching,
sexual intercourse, oral sex) that occurs between people
over the age of 16 years after mutual sexual consent has
been provided by those involved, who have been
assessed as having the capacity to consent.1 The term
inappropriate context or setting refers to consensual
sexual activity taking place in an environment or
associated with a set of circumstances that is not
considered to be suitable, such as:
■ An acute inpatient setting
■ A public area of a non acute, residential or
rehabilitation unit
■ When a health worker suspects that a consumer has
been coerced into engaging in sexual activity or was
unwell at the time that the activity occurred.
Impact
The impact for consumers of consensual sexual activity in
an inappropriate context or setting will vary based on the
individual circumstances involved, but could involve:
■ sexual exploitation
■ damage to self esteem and other relationships
■ sexually transmitted infections or pregnancy
Witnessing sexual activity, even if it is consensual, can
also be traumatic for others within the service setting,
particularly those that have previously experienced sexual
assault or harassment.
When a mental health worker or clinician is involved, the
consequences could include:
■ significant and enduring harm to the consumer
■ damage to the trust that should exist between
consumer and mental health worker or clinician
■ the mental health worker or clinicians decisions about
care and treatment may be influenced to the
consumer’s detriment
■ a breach of the NSW Health Code of Conduct
(PD2012_018) resulting in disciplinary action against
the mental health worker or clinician
■ criminal charges being laid against the mental health
worker or clinician.
1 Note: It is a crime to have sexual intercourse with a young person between the ages of 16 and 18 if you are in a relationship of ‘special care’ with that young person, regardless of whether they consent to this. ‘Special care’ relationships include step-parent, guardian, foster parent, health practitioner, employer, teacher, coach, priest, etc.

PaGe 12 NSW HealtH Sexual Safety of Mental Health Consumers Guidelines
2.3.3 Sexually disinhibited behaviour
Definitions
Sexual disinhibition is an inability to restrain sexual
impulses and involves behaviour or talk which is
considered inappropriate for a particular environment.
This behaviour arises for a variety of reasons that can
include a mental illness or disorder, dementia or
Alzheimers, or the side effects of medication.
Behaviours can exist on a continuum and can escalate in
severity, from an increase in sexual thoughts through to
indiscriminate sexual activity.
Impact
Sexually disinhibited behaviour can be embarrassing,
distressing and potentially dangerous for the person
exhibiting the behaviour as well as for those that may be
exposed to it. It can also negatively impact on existing
relationships and for those that have experienced a prior
incident of sexual assault or harassment, being exposed to
this behaviour can trigger strong feelings of fear and anxiety.
Sexually disinhibited behaviour also has the potential to
make consumers exhibiting this behaviour vulnerable to
sexual assault or harassment.
2.4 Rights and responsibilities regarding sexual safety
In protecting the sexual safety of consumers, mental
health services must ensure that the consumers’ rights
are respected. Services will also need to understand and
promote the responsibilities all members of the service
have while in the care of or involved with the service.
2.4.1 Mental health consumers in all settings have the right to:
■ Receive clear information and advice that takes
account of their cultural background, gender, sexual
orientation, age and personal experiences regarding:
– their rights and responsibilities in relation to sexual
safety;
– the standards of appropriate behaviour that exist in
the service setting;
– the process for addressing a sexual safety incident;
– the support services available should they
experience sexual assault or harassment; and
– how to manage sexual health issues, such as
contraception, sexually transmitted diseases (STDs)
and pregnancy.
■ Be heard and believed regarding their experience
of sexual assault and harassment.
■ Be treated with compassion and understanding
when they disclose incidents that have compromised
their sexual safety.
■ Be supported by the person of their choice after a
sexual safety incident has occurred, whether this is a
family member, friend, preferred staff member or
other advocate.
■ Receive prompt treatment once their experience of
sexual assault and harassment is disclosed, whether
this experience occurred prior to or after their
admission to a mental health service.
■ Be informed about their options after experiencing
a sexual assault or sexual harassment, and have their
wishes respected, particularly regarding whether to:
– Remain within the service environment in which the
assault occurred, or be moved to another environment;
– Disclose their experience of sexual assault,
including to their carer and/or family;
– Make a formal complaint to the NSW Police Force,2
Talk to a Sexual Assault Service; and
– Undergo a medical or forensic examination.
■ Be protected from further contact with the alleged
perpetrator of a sexual assault or sexual harassment
when in the care environment, regardless of whether
this is a staff member, a consumer, the consumer’s
family member, carer or friend or a casual visitor.
2 An allegation of sexual assault must be reported to NSW Police Force if it involves an employee of NSW Health – PD2006_026
SEXUALLY DISINHIBITED BEHAVIOUR
Increase in sexual
thoughts
Engaging in indiscriminate sexual activity
Being hypersexual
eg masturbating in public
Sexualised demeanour and general disinhibition
Being overly familiar or
touching others
Wearing overly revealing
clothing
Removing clothes when not required
Sexual Safety of Mental Health Consumers Guidelines NSW HealtH PaGe 13
■ Receive support to access sexuality and sexual
health education, if they wish to be involved in such
education, and contribute to determining the topics
that such education will cover.
2.4.2 All members of a mental health service have the right to:
■ Feel safe from acts that compromise or breach their
sexual safety while in a mental health service environment.
■ Be consulted about and provide input to the
sexual safety standards developed to govern
appropriate behaviour within the service they are
involved with.
2.4.3 Mental health services in all settings have a responsibility to:
■ Implement and monitor compliance with these
Guidelines to establish and maintain the sexual
safety of the consumers who use their service.
■ Develop sexual safety standards that define
appropriate behaviour for the service setting in
consultation with all members of the service,
including consumers and their families and carers –
see Appendix A for example standards.
■ Provide clear information and advice to
consumers that takes account of their cultural
background, gender, sexual orientation, and personal
experiences regarding:
– their rights and responsibilities in relation to sexual
safety;
– the sexual safety standards that exist in the service
setting;
– the process for addressing a sexual safety incident;
– the support services available should they
experience sexual assault or harassment; and
– how to manage sexual health issues, such as
contraception, sexually transmitted diseases (STDs)
and pregnancy.
■ Ensure consumers are supported to access
condoms in service settings where sexual activity is
recognised as appropriate e.g. non-acute inpatient/
rehabilitation and community.
■ Be non-judgemental, compassionate and
understanding when a consumer discloses their
experience of sexual assault or harassment.
■ Organise prompt treatment for a consumer once
their experience of sexual assault and harassment is
disclosed, whether this experience occurred prior to
or after their admission to a mental health service.
■ Explain the available options the consumer should
consider if they have experienced sexual assault or
harassment, and ensure the consumer’s wishes
are respected unless legislatively prohibited.
■ Protect the consumer from further contact with
the accused perpetrator, regardless of whether this
is a staff member, another consumer, the consumer’s
family member, carer or friend or a casual visitor.
■ Support the consumer to be free from pressure
to engage in sexual activity with another person,
including the consumer’s partner or spouse.
■ Help the consumer to access sexuality and
sexual health education that is appropriate to
their cultural background, gender, sexual
orientation, age and personal experiences, and
ensure that consumers are able to contribute to
determining the topics such education should involve.
2.4.4 All members of a mental health service have a responsibility to:
■ Respect the rights of others to feel safe from acts
that compromise or breach their sexual safety,
regardless of their cultural background, gender and
sexual orientation.
■ Read the information provided to them about
sexual safety within the service environ and ask
questions as required to support their understanding.
■ Adhere to the sexual safety standards that
define appropriate behaviour for the service
setting.
2.5 Relevant legislation, standards/rights and policies
2.5.1 Legislation■ Anti Discrimination Act 1977
■ Child Protection (Offenders Registration) Amendment
Act 2000
■ Children and Young Person’s (Care and Protection)
Act 1998
■ Crimes (Sentencing Procedure) Act 1999
■ Crimes Act 1900
■ Criminal Procedure Act 1986
■ Evidence Act 1995
■ Health Administration Act 1982
■ Health Records and Information Privacy Act 2002
■ Victims Rights Act 1996
■ Ombudsman Act 1974
■ Commission for Children and Young People Act 1998

PaGe 14 NSW HealtH Sexual Safety of Mental Health Consumers Guidelines
■ Child Protection (Working with Children) Act 2012 –
not yet in force.
■ Health Services Act 1997
Links to some of these documents online, along with
extracts that pertain specifically to these guidelines, are
provided at Appendix B and C.
2.5.2 Standards and rights■ Charter of Victims Rights (Extract from the Victims
Rights Act 1996 – Part 2, Section 6)
■ National Statement of Rights and Responsibilities of
Consumers of Mental Health Services
■ NSW Ministry of Health Charter for Mental Health
Care in NSW
■ NSW Police Force, Health and Office of the Director
of Public Prosecutions: Guidelines for Responding to
Adult Victims of Sexual Assault 2006
■ UN Declaration – Rights of Disabled Persons
■ UN Principles for the Protection of Persons with
Mental Illness and for the Improvement of Mental
Health Care
2.5.3 Associated NSW Health policies■ Child Protection and Wellbeing – Information
Exchange PD2011_057
■ Child Protection Issues for Mental Health Services –
Risk of Harm Assessment Checklist PD2006_003
■ Child Protection Roles and Responsibilities –
Interagency PD2006_104
■ Child related allegations, charges and convictions
against employees PD2006_025
■ Complaint Management Guidelines GL2006_023
■ Complaint or Concern about a Clinician –
Management Guidelines GL2006_002
■ Complaint or Concern about a Clinician – Principles
for Action PD2006_007
■ Complaints Management Policy PD2006_073
■ Coroners’ Cases and Amendments to Coroners Act
1980 PD2005_352
■ Criminal allegations, charges and convictions against
employees PD2006_02
■ Disciplinary Process in NSW Health – A Framework for
Managing the Disciplinary Process in NSW Health
PD2005_225
■ Domestic Violence – Identifying and Responding
PD2006_084
■ Employment Screening PD2008_029
■ Improper Conduct – Procedures for Recruitment/
Employment of Staff and Other Persons PD2005_109
■ Incident Management Policy PD2006_030
■ Interpreters – Standard Procedures for Working with
Health Care Interpreters PD2006_053
■ Keep Them Safe – Making a Child Protection Report
IB 2010_005
■ Legal Matters of Significance to Government
PD2006_009
■ Lookback Policy PD2007_075
■ NSW Health Code of Conduct PD2012_018
■ NSW Health Frontline Policies and Procedures for
Child Protection and Wellbeing (update being finalised
at time of printing)
■ NSW Health Subpoenas PD2010_065Open Disclosure
PD2007_037
■ Privacy Manual (Version 2) – NSW Health
PD2005_593
■ Protecting Children and Young People PD2005_299
■ Reportable Incident definition under section 20L of
the Health Administration Act PD2005_634
■ Reportable Misconduct under the Medical Practice
Act – Guidelines for practitioners, August 2008
IB2008_062
■ Sexual Assault Services Policy and Procedure Manual
(Adult) PD2005_607
■ Statutory Guidelines under the Health Records and
Information Privacy Act 2002
■ Violence Prevention & Management Training
Framework for the NSW Public Health System
PD2012_008
Sexual Safety of Mental Health Consumers Guidelines NSW HealtH PaGe 15Sexual Safety of Mental Health Consumers Guidelines NSW HealtH PaGe 15
KEY POINTS – SEXUAL SAFETY AND MENTAL HEALTH
■ Sexual safety refers to the respect and maintenance
of an individual’s physical (including sexual) and
psychological boundaries.
■ Mental health consumers are exposed to a number of
potential risks, especially when they are acutely
unwell, and are more vulnerable to sexual assault in
particular.
■ The prevalence of people with a mental illness who
have been exposed to or have experienced personal
trauma, including sexual abuse and violence, is high.
■ The types of behaviour that can breach and/or
compromise the sexual safety of a mental health
consumer are:
– Sexual assault and harassment
– Consensual sexual activity in an inappropriate
context or setting
– Sexually disinhibited behaviour
■ Sexual assault is when:
– a person is forced, coerced or tricked into sexual
acts against their will or without their consent;
– a child or young person under 16 years of age is
exposed to sexual activities, or
– a young person over the age of 16 but under the
age of 18 years of age is exposed to sexual
activities by someone with whom they have a
‘special care’ relationship e.g. step-parent,
guardian, foster parent, health practitioner,
employer, teacher, coach, priest, etc.
■ Sexual assault is a crime.
■ Sexual harassment is unwelcome conduct of a sexual
nature which makes a person feel offended,
humiliated and/or intimidated where that reaction is
reasonable in the circumstances.
■ Consensual sexual activity is any activity of a sexual
nature that occurs:
– between people over the age of 16 years, or over
the age of 18 years if there is a ‘special care’
relationship between those involved; and
– after mutual sexual consent has been provided by
those involved; and
– when those involved have been assessed as having
the capacity to consent .
■ Sexually disinhibited behaviour involves actions or talk
of a sexual nature that is considered inappropriate for
a particular environment.
■ In protecting the sexual safety of consumers, mental
health services must ensure that the consumer’s rights
are respected and the responsibilities of all members
of the service are promoted and upheld. See Section
2.4 for further information.
■ Services will need to familiarise themselves with the
range of relevant legislation, standards and NSW
Health policies. See Section 2.5 for further
information.

PaGe 16 NSW HealtH Sexual Safety of Mental Health Consumers GuidelinesSexual Safety of Mental Health Consumers Guidelines NSW HealtH PaGe 16
Fostering a culture that supports sexual safety
SECTION 3
For consumers to feel sexually safe, services will need to
foster a culture that encourages and supports consumers
to report a sexual safety incident. This will involve strong
leadership that inspires transparency and trust.
Transparency means the degree to which information
flows freely within the service, among managers and
staff, and outward to consumers, their families and
carers, and other key stakeholders. Trust means members
of the service can communicate upward and honestly,
teams can challenge their own assumptions freely, and
managers and clinicians can successfully communicate
important messages to staff.
Training and education, promotion and collaboration will
all play a critical role in supporting services in this regard.
3.1 Training and education
3.1.1 Supporting mental health staff
Service staff
Training is essential for all frontline staff and managers
around sexual safety and sexual assault and harassment.
Awareness and knowledge of the impact of sexual
assault and harassment, and the implications of sexual
offender tactics, informs clinical practice and can
significantly improve treatment outcomes for consumers.
This in turn can reduce the possibility of consumers being
re-traumatised, both while in the care of a mental health
service and when they move into the community.
Training also provides staff with the opportunity to reflect
on many of the common myths held within society about
sexual assault. This reflection in conjunction with
evidence-based facts can have a positive impact on
attitudes around sexual assault and drive cultural change
where required.
KEY ACTIONS/POINTS FOR ALL SETTINGS
■ All staff need to be aware of and cognisant with their
Local Health District policy and procedures that
outline their responsibilities in relation to preventing
potential sexual assault and harassment and
responding appropriately if an assault or harassment
occurs.
■ Staff in all settings should be provided with optimal
opportunity to attend training on managing sexual
safety and this should be provided within an
orientation period where possible.
■ Such training must include advice about how to
appropriately take a consumer’s sexual assault history.
Other areas or topics for training include:
– The increased vulnerability of people with a mental
illness to sexual assault and harassment
– Management of sexuality in different health care
settings
– Recognition of signs of sexual assault in different
consumer groups
– What behaviour constitutes sexual harassment
– Management of disinhibitive behaviour
– Processes for reporting a sexual assault to Police
and requirements for preserving a potential crime
scene
– An understanding of different religious and cultural
mores
– Management and support of the consumer who
has experienced previous sexual assault or
harassment
– The sexual rights of people with a mental illness
– Child protection issues in relation to children and
young people living with or related to a consumer
■ Education may also be required around how to
discuss sexual safety issues with consumers and
their families and carers in a sensitive and non-
sexualised way.
■ Any training and education should include gender-
sensitive and trauma informed care practice principles.
Having clinical supervision systems in place will also
support staff in developing their understanding of
gender sensitive practice, trauma informed care, and
professional boundaries.
■ Refresher training should be considered for all staff
annually.

Sexual Safety of Mental Health Consumers Guidelines NSW HealtH PaGe 17
KEY ACTIONS/POINTS FOR ACUTE INPATIENT
■ Training for staff working in an acute inpatient setting
must include risk assessment of consumers for
victimisation or offending and management of
disinhibitive behaviours.
■ Support to appropriately utilise tools such as
environmental audits will also be required.
KEY ACTIONS/POINTS FOR NON-ACUTE/
RESIDENTIAL AND COMMUNITY
■ Promoting safety within settings where a consumer’s
right to consensual sexual activity is respected can be
supported through education on topics such as
assessing a consumer’s capacity to provide sexual
consent and understanding the tactics of coercion.
■ Staff in community based and residential services who
are involved in case management will also need
information and advice regarding how to manage the
particular issues that exist when home visiting.
Consumer workers and representatives
Consumers often feel a particular level of trust in confiding
in and disclosing to consumer workers. This makes consumer
workers vital members of the service environment.
KEY ACTIONS/POINTS FOR ALL SETTINGS
■ Consumer workers must be provided with education
and training that mirrors the training provided to
service staff.
■ This will support them to play a pivotal role in
providing advocacy in the event of sexual harassment
or assault within services and to gain information
from a trauma focused perspective.
■ Consumer workers and representatives also need to
be able to access training in terms of reflective
practice around appropriate boundaries and ethical
practice within the context of their workplace roles.
Clinicians already receive this training as part of their
health qualifications.
Volunteers
Anyone who carries out volunteer work within a mental
health service does so to enhance services for consumers.
Accordingly, they should be provided with adequate
support to help them to be aware of and understand
sexual safety issues for consumers.
KEY ACTIONS/POINTS FOR ALL SETTINGS
Volunteers will need education and training regarding:
■ The rights and responsibilities of the consumers who
use the service;
■ Their own responsibilities and the NSW Health Code of
Conduct that applies to all health positions or roles;
■ How to respond if they receive a disclosure of sexual
assault, suspect someone has been sexually assaulted
or witness a sexual assault; and
■ How to respond if they become aware in the course
of their duties that a child or young person may be at
risk of significant harm.
3.1.2 Empowering consumers Empowerment in the context of a mental health service is
the meaningful participation of people with mental illness
in decision making and activities that give them increased
power, control, or influence over important areas of their
lives. Any process that prepares people to participate
more effectively in an activity that increases their power,
control, or influence can be considered empowering.
Consumers can participate more effectively in the
establishment and maintenance of their sexual safety
through the provision of information and opportunities
to be involved in education programs.
It is also important that consumers understand the link
between sexual safety and sexual health. The World
Health Organisation (WHO) defines sexual health
as follows.
Sexual health
A state of physical, emotional, mental and social well-being related to sexuality, including the absence of disease, dysfunction or infirmity; a positive and respectful approach to sexuality and sexual relationships; the possibility of having pleasurable and safe sexual experiences, free from coercion, discrimination and violence, and; respect for the sexual rights of all persons.
World Health Organisation

PaGe 18 NSW HealtH Sexual Safety of Mental Health Consumers Guidelines
Good sexual health can facilitate the development of
respectful, healthy and equitable relationships and
improve attitudes toward gender equity, gender roles,
and violence, particularly violence against women.
KEY ACTIONS/POINTS FOR ALL SETTINGS
■ Information for consumers should include advice
about their rights and responsibilities as they pertain
to the service they are involved with as well as the
sexual safety standards of the service. Staff can provide
this information to consumers in a written format on
admission and assist them with understanding the
implications at daily unit meetings, within case
management relationships and within the context
of daily care.
■ Consumers should also be advised of the complaints
process, including how to access the Official Visitors.
■ Information and resources need to be made available
in community languages as well as English and access
to interpreters and Aboriginal liaison staff made
available.
■ Consumers in all settings should be provided with
opportunities to participate in sexuality education
programs as part of a wider preventative approach.
■ Such sexuality education must include more than just
the biological details of reproductive sex and sexual
health, but also engagement with the meaning and
negotiation of sexual consent (Carmody, 2003, 2005;
Carmody and Willis, 2006; Powell, 2007).
KEY ACTIONS/POINTS FOR ACUTE INPATIENT
■ While consumers in an inpatient setting are not
encouraged or supported to engage in sexual activity,
education and training around ethical behaviour and
developing respectful relationships can be beneficial.
Such education could include information about:
– Building self-esteem and resilience
– Developing the social skills to cultivate and
maintain relationships
– Different types of relationships
– Coping with relationship difficulties or rejection
■ Helping consumers to develop respectful relationships,
and promoting alternative ways of relating that are
non-violent and non-sexual, can provide an important
contribution to the establishment and maintenance of
a sexually safe environment. This can also help to
prepare consumers to enjoy a healthy and safe sex life
once they are well enough to leave the inpatient setting.
■ Communicating with consumers verbally about how
some of their behaviour can impact on consumers
who may have experienced past trauma can also be
an effective education strategy.
KEY ACTIONS/POINTS FOR NON-ACUTE/
RESIDENTIAL AND COMMUNITY
■ In non-acute/residential and community settings, a
significant proportion of consumers are sexually active
and may participate in high-risk behaviours, placing
them at an increased risk of sexually transmitted
infections (STIs), including gonorrhoea, chlamydia,
syphilis and HIV, as well as unwanted pregnancy.
■ Mental health staff in these settings have an important
role to play in providing educative information that
promotes sexual health as part of routine care.
■ Sexuality education and training should also be
offered to consumers in a non-acute/residential
setting. In a community setting, information about
how to access this education can be provided. Such
education can help consumers to recognise and
identify inappropriate sexual behaviours, their own
and others, develop strong self-protective knowledge
and skills3 (e.g. how to assert their right to say ‘no’) as
well as develop a positive and respectful approach to
their sexuality and to sexual relationships.
■ This education and training could include information
about:
– Sex and relationships, including marriage, same sex
attraction and parenting
– The physical mechanics of sex, including
reproduction and masturbation
– Appropriate and inappropriate expressions of
sexuality
– Sexually transmissible infections
– Safer sex and contraception
– Sexuality in older age
3.1.3 Recognising families, friends and carers
A consumer’s family and/or carer are an integral part of
the care team. Accordingly, they will require information
to enable them to understand the importance of sexual
safety for the consumer they support and how they can
help to ensure it is maintained.
3 Beyond Belief, Beyond Justice – Disability Discrimination Legal Service Inc, Victoria – November 2003

Sexual Safety of Mental Health Consumers Guidelines NSW HealtH PaGe 19
KEY ACTIONS/POINTS FOR ALL SETTINGS
■ Families and carers should be provided with advice
about the consumer’s rights within the service setting
and pathways for complaint if these rights are
not upheld.
■ Additionally, they will need information that indicates
what will happen if the consumer they support is
sexually assaulted or harassed, or sexually assaults or
harasses someone else, and the referral services that
are available to help with understanding issues
around sexual assault. This information could include
advice about disinhibited behaviour, where relevant,
to ensure the consumer’s partner or family is aware
of the connection between this type of conduct and
the consumer’s illness, and to help them to help the
consumer manage their behaviour when in a
manic phase.
■ Families and carers will also require information
regarding the consumer’s responsibilities while
involved with the service and the sexual safety
standards that define appropriate behaviour for the
consumers involved with the service.
3.2 Promoting sexual safety
Promoting sexual safety is an important component of
any strategy to prevent sexual assault and harassment.
The most effective way to promote sexual safety is through
the adoption of an ethos that promotes, encourages and
models mutual respect in its relationships between staff,
between staff and consumers, and between consumers.
Information regarding sexual assault, and about support
services for people who have been assaulted in particular,
should also be readily accessible. The World Health
Organisation recommends that health services consider:
■ Compiling a list of local services and telephone
numbers that can be kept in a place that is easily
accessible.
■ Displaying posters about sexual assault and where to
go for help on the walls of the facility (having
information prominently displayed may make people
who have been assaulted feel more comfortable in
disclosing and talking about the sexual violence in
their lives). See Appendix D, E and F for examples of
information and posters that could be utilised for this
purpose.
■ Placing pamphlets and brochures regarding sexual
assault in designated areas, such as toilets and
gender-specific areas, so that consumers can take them
away with them or read the information in private.
Other practical promotion strategies include:
■ Developing sexual safety standards of appropriate
behaviour in consultation with consumers and their
carers and families.
■ Regularly communicating and promoting these
standards to all members of the service, including
casual visitors, such as tradespeople or couriers, via
posters or written materials.
■ Conducting periodic surveys or forums involving
consumers, carers and families on the quality of the
service, including matters relating to sexual safety.
■ Prominently displaying the service’s position on sexual
safety in the adult acute inpatient unit.
■ Discussing behavioural expectations and sexual safety
in consumer unit meetings and programs.
■ Providing gender specific programs, groups and
activities.
■ Changing practices to consider sexual safety issues,
and communicating these changes to all staff.
■ Conducting a clinical review of every sexual safety
incident as a matter of urgency.
■ Reporting every sexual safety incident through the
mental health service incident reporting system. (See
Reporting and Recording for further information.)
3.3 The importance of collaboration
Maintaining a sexually safe environment within the
service, supporting consumers receiving treatment within
the community to maintain their own sexual safety, and
responding appropriately when a sexual safety incident
occurs, will require collaboration with a range of key
stakeholders.
3.3.1 ConsumersConsumers have a critical role to play in contributing to
the sexual safety of the service environment, and to their
own sexual safety, and the safety of others, if they are
receiving treatment within the community. Accordingly,
they need to be actively involved in developing sexual
safety standards of appropriate behaviour for the service
they are involved with.
Working collaboratively with consumers in relation to
managing sexual safety can also help to empower them,
which is an important component of the recovery process
in relation to their mental illness.

PaGe 20 NSW HealtH Sexual Safety of Mental Health Consumers Guidelines
3.3.2 Families and carersA consumer’s family and/or carer are an integral part of
the care team. They can offer critical emotional support
to a consumer who has experienced sexual harassment,
assault or violence, as well as support to liaise with health
care and other professionals, such as Sexual Assault
Services and Police. They can also help the consumer to
understand and adhere to the sexual safety standards of
the service.
However, staff must ensure that the consumer’s carer,
family or friends are only advised of any sexual safety
incident with the express consent of the consumer.
Additionally, staff should be mindful of the high
prevalence of intra-familial sexual assault for consumers.
Family members may have been or may continue to be
perpetrators of abuse, and this must be considered when
organising family visits or conferencing.
Staff should also familiarise themselves with the NSW
Health Frontline Procedures for the Protection and
Wellbeing of Children and Young People (revised
procedures being finalised at the time of printing) and
assess the safety risk to children and young people under
18 who may be living with or have access to an adult
consumer exhibiting behaviours that may place a child or
young person at risk of harm.
3.3.3 General practitioners (GPs)GPs are uniquely placed to provide information and
support to consumers, as well as their family and carers,
in relation to sexual safety and sexual health matters and
can provide long-term continuity of care that will support
consumers to build a trusting relationship with them.
For those consumers being treated within the community
or in a residential setting, the role of the GP in relation to
sexual safety can include:
■ Providing information about treatment options
regarding sexual assault or harassment
■ Referring the consumer to local support services, such
as a counsellor or the local Sexual Assault Service or
rape crisis centre
■ Discussing contraception, STIs and other sexual health
issues
■ Organising a forensic examination if an assault has
occurred recently, or conducting this exam if they
have been trained in this field and have the necessary
equipment
■ Providing follow-up care
All consumers being treated outside of a hospital setting
should have a regular GP.
Developing shared care arrangements with a consumer’s
GP, or linking consumers with a GP in the area, should be
a priority for mental health services and all services should
have a strategy in place, at either a local or Local Health
District level, to strengthen relationships with local GPs.
3.3.4 NSW Health Sexual Assault Services
NSW Health Sexual Assault Services are based in hospitals
or community health centres across NSW. They are
staffed by specially trained counsellors and are accessible
24 hours a day. Their role is to provide specialist guidance
to health staff in responding to incidents as well as
counselling and relevant medical assessment and
treatment for people who have experienced sexual
assault and their family/significant others. This includes:
■ crisis and ongoing counselling
■ specialist medical and forensic services
■ court preparation and support
■ community education and prevention
■ professional training and consultation
■ advocacy
Differing perspectives, along with language differences
across service models and frameworks, can be barriers to
developing good collaborative relationships between
mental health and Sexual Assault Services. However,
collaboration between these services offers invaluable
support for staff, as well as better outcomes for the
consumer who has experienced the assault, through:
■ access to other knowledge and information
■ consultancy on issues of sexual assault and mental
health
■ supportive debriefing where appropriate
■ breaking down staff isolation
■ introduction of new ideas and strategies from people
who are outside the sector
■ support and advocacy for services in addressing the
needs of consumers

Sexual Safety of Mental Health Consumers Guidelines NSW HealtH PaGe 21
Mental health services should look to develop a close
partnership with their local Sexual Assault Service, with
consideration given to inviting key members of the Sexual
Assault Service to visit the service on a regular basis so
that consumers are familiar with them. The Sexual Assault
Service may also be able to provide recurrent education
sessions with consumers around relevant topics, or visit to
talk about what they do and how they can help
consumers when required. See the NSW Health Sexual
Assault Webpage (http://www.health.nsw.gov.au/
publichealth/sexualassault/index.asp ) for further
information.
3.3.5 NSW Police ForceThe role of the NSW Police Force is to:
■ ensure that the Charter of Victims’ Rights is observed
at all times
■ provide protection to victims/survivors of sexual
assault who are at immediate or continuing risk, using
relevant powers
■ investigate reports of sexual assault
■ assess the case and decide if there is adequate
evidence to proceed with an investigation or to
charge an assailant
■ apprehend and charge an alleged perpetrator with
sexual assault.
Every Local Area Command in NSW has a designated
Mental Health Contact Officer (MHCO) at Inspector Rank.
One of the responsibilities of the MHCO is interagency
liaison with local NSW Mental Health Services. Mental
health services can obtain their local MHCOs contact
details via their Emergency Mental Health Local Protocol
Committee member or by making a request through their
Local Area Command. The MHCO can be engaged for
any interagency issue or for facilitating training for staff
involving Police.
Many NSW Police Officers have also received Mental
Health Intervention Team (MHIT) training and some Police
Officers have specific training in taking sexual assault
statements in a sensitive and respectful way from people
who have been assaulted. Mental health services can ask
at their Local Area Command for the support of a MHIT
trained Officer, and can request a female Police Officer, if
one is available.
Mental health services should ensure that they establish
and maintain a good working relationship with the local
Police service, which should include the development of
local protocols to manage reporting of sexual assault or
harassment.
3.3.6 Other agenciesThere are a range of other agencies that can support
both staff and consumers when there is an allegation of
sexual assault or harassment. These include what is in the
table below.
Services should familiarise themselves with these agencies
and the type of support they offer so that they are able
to provide relevant options to consumers as required
should they experience a sexual safety incident. A handout
for consumers may be useful that provides the contact
information for these and other local agencies and
support groups.
Adults Surviving Child Abuse (ASCA) www.asca.org.au
Child and Adolescent Sexual Assault Counsellors Inc www.casac.org.au
The Gender Centre www.gendercentre.org.au
Intellectual Disability Rights Service www.idrs.org.au
NSW Department of Community Services www.community.nsw.gov.au
NSW Rape Crisis Centre www.nswrapecrisis.com.au
NSW Service for the Treatment and Rehabilitation of Torture and Trauma Survivors(STARTTS):
www.startts.org.au
Transcultural Mental Health Centre www.dhi.health.nsw.gov.au/tmhc
Women’s Legal Services NSW www.womenslegalnsw.asn.au

PaGe 22 NSW HealtH Sexual Safety of Mental Health Consumers Guidelines
3.3.7 Partner programs/Community managed organisations (CMOs)
Mental health CMOs provide a range of interventions for
mental health consumers, including:
■ Promotion and prevention to early intervention
■ Family and peer support
■ Mentoring and counselling
■ Community awareness activities and
■ Education and training.
In many cases, a CMO can be a consumer’s primary
non-clinical service provider. This makes CMOs important
stakeholders whose capacity to support and encourage
consumers to consider their sexual safety and sexual
health should not be undervalued. CMOs can also
provide advice to mental health services in terms of
appropriate approaches to effectively engage consumers.
Working collaboratively with CMOs at local level can help
to ensure a complementary approach is taken to raising
awareness about sexual safety issues for consumers, which
avoids duplications, provides continuity of care and more
efficient use of limited resources.

Sexual Safety of Mental Health Consumers Guidelines NSW HealtH PaGe 23
KEY POINTS – FOSTERING A CULTURE THAT SUPPORTS SEXUAL SAFETY
Training and education
■ Training and education, promotion and collaboration
will all play a critical role in supporting services to
foster a culture that encourages and supports
consumers to report a sexual safety incident.
■ Training is essential for all frontline staff and managers
around managing sexual safety, inclusive of taking a
consumer’s sexual assault history. Such training must
include gender sensitive and trauma informed care
principles. Consumer workers and volunteers will also
need training. See Section 3.1 for further information.
■ Education should also be offered to mental health
consumers on topics relevant to the setting in which
they are receiving care e.g. building the social skills to
develop and maintain relationships for consumers in
an acute setting; sexuality and sexual health
education, including cultivating and maintaining
ethical relationships, for consumers in a non-acute/
residential setting.
■ For consumers in a community setting, help to access
such education should be offered if relevant.
Promotion
■ The most effective way to promote sexual safety is
through the adoption of an ethos that promotes,
encourages and models mutual respect in its
relationships between staff and consumers, between
staff, and between consumers.
■ Information regarding sexual assault, and about
support services for people who have been assaulted
in particular, should be readily accessible. See Section
3.2 for further information.
Collaboration
■ Maintaining a sexually safe environment within the
service, supporting consumers receiving treatment
within the community to maintain their own sexual
safety, and responding appropriately when a sexual
safety incident occurs, will require collaboration with
a range of key stakeholders, including:
– Consumers
– Families and carers
– GPs
– NSW Health Sexual Assault Services
– NSW Police Force
– Other agencies
– Partner programs/community managed or
non-government organisations
■ See Section 3.3 for further information.
Sexual Safety of Mental Health Consumers Guidelines NSW HealtH PaGe 23

PaGe 24 NSW HealtH Sexual Safety of Mental Health Consumers Guidelines
SECTION 4
Preventing a Sexual Safety Incident
4.1 Sexual assault and harassment
4.1.1 Assessing vulnerability All consumers are vulnerable by the nature of their illness
and/or the experience of being hospitalised. Being female
in particular increases the consumer’s vulnerability to
being sexually assaulted or harassed, as is being under
the age of 18 years. Other factors that increase the risk
for a consumer of being sexually assaulted include:
■ Having a past history of being sexually assaulted
■ Being a young female experiencing their first admission
■ Being heavily medicated
■ Being intoxicated and/or having a comorbid drug and
alcohol condition
■ Having an intellectual disability
■ Being Aboriginal or Torres Strait Islander
■ Being a refugee/torture and trauma survivor
■ Experiencing a psychosis
■ Being a victim/survivor of domestic violence
■ Sexual disinhibition
■ Having a cognitive impairment e.g. delirium
■ Impaired communication skills e.g. English
competence, hearing speech or visual impairment
KEY ACTIONS/POINTS FOR ALL SETTINGS
■ Assessing the vulnerability of a consumer to being
sexually assaulted and harassed can support staff to
better manage any risk to their sexual safety and
should be undertaken on the consumer’s admission.
■ Any existing screening process (e.g. for domestic
violence and/or elder abuse) should be broadened to
take account of any history the consumer may have
of experiencing or perpetrating sexual assault and
harassment (see below).
■ If a consumer is assessed as being vulnerable to sexual
assault, this assessment must be:
– Documented within the admission clinical
documentation, progress notes and management/
care plans, along with what steps will be taken to
address this vulnerability; and
– Communicated to all staff.
4.1.2 Taking an appropriate sexual assault and harassment history
Knowledge about a consumer’s previous history of being
subjected to sexual assault or harassment can inform staff
of the consumer’s particular needs and what may or may
not be problematic or ‘triggering’ situations for them.
Feeling safe within services is essential for healing and for
decreasing vulnerability to further victimisation.
Research indicates that people who have experienced
sexual abuse that occurs within an institutional
environment are unlikely to disclose the abuse unless they
are asked directly.
This reluctance is due to a range of factors, including:
■ denial
■ fear of stigmatisation
■ inability to trust
■ loyalty to the perpetrator
■ feelings of shame
■ inability to identify the experience as abuse or realise
that they have a right to safety
■ fear of retaliation by the perpetrator or others
■ fear of being labelled as a liar, attention-seeking or
out of touch with reality
Accordingly, taking a consumer’s sexual assault history
when they are admitted to a mental health service is
critical to enable staff to adequately support the consumer,
both in terms of their illness and their sexual safety while
involved with the service.
It is important, however, to ensure that this process is
carried out when the consumer is comfortable to do so.
For acute admissions, taking such a history should be
delayed until the consumer is stable.
Taking a consumer’s history of perpetrating sexual assault
is also vitally important to assess the risk that they may
continue to offend while involved with the mental health
service, separate them from consumers that have been
identified as vulnerable and to ensure they receive

Sexual Safety of Mental Health Consumers Guidelines NSW HealtH PaGe 25
appropriate support to recognise their behaviour as
inappropriate.
Risk factors for offending include:
■ Having a history of sexually offending behaviour
■ Having a history of domestic violence offending
■ Violent and threatening behaviours
■ Intimidating behaviours including sexual harassment
■ Sexually disinhibitive behaviours
■ Acute drug intoxication e.g. methamphetamines
KEY ACTIONS/POINTS FOR ALL SETTINGS
■ The process for admitting a consumer to any mental
health service should include taking a sexual assault
history. A screening tool to help with this process is
available at Appendix G.
■ It is critical that only staff who have undertaken
training on how to appropriately take such a
history, and respond to disclosures, are
nominated to conduct the associated
assessment. Alternatively, services may wish to
contact their local Sexual Assault Service or another
sexual assault counselling service for support or advice
for the clinician undertaking this assessment.
■ Taking a sexual assault history can be traumatic for
the consumer, so those undertaking the assessment
must be sensitive to the consumer’s feelings and needs
and ensure:
– The assessment is undertaken only when the
consumer is in a stable condition – in acute
admissions, a delay may be required prior to
undertaking the assessment;
– Adequate time is set aside for the assessment – the
consumer should be allowed to proceed at their
own pace; and
– An appropriately private space is allocated to
support the assessment to be undertaken – privacy
and confidentiality are key concerns.
■ Taking a sexual assault history may also be traumatic
for a staff member that has experienced sexual assault
or violence themselves. Staff should be cognisant of
their own feelings about sexual assault and seek
management support to ensure they do not experience
re-traumatisation themselves as a result of their
involvement in the sexual assault history assessment.
■ When possible, family members, carers or friends
should not be present during the assessment so that
influences and distractions are kept to a minimum.
However, the wishes of the consumer must be
respected in this regard – if the consumer feels more
comfortable having a support person attend the
assessment with them, this should not be discouraged.
■ Mental health staff should commence by explaining
to the consumer what will happen with the
information to be collected, how it will be stored and
who will have access to it, which must include the
consumer’s rights under State and Commonwealth
privacy legislation (see Appendix C for further
information).
■ An explanation should be provided to the consumer
regarding why what may be perceived as personal
questions are being asked:
‘So that I can work out the right way to support you
while you are with our service, I need to know a bit
more detail about your life before you came here,
including any experiences you may have had that
made you uncomfortable.’
■ The consumer should also be advised that they have
the right not to answer at the present time but that
the staff member would be available at a future time
should the consumer wish to speak with them.
■ If the consumer identifies a history of sexual assault/
abuse, their experience should be validated:
‘Thank you for telling me about such a difficult
experience.’
‘I’m sure that was hard for you to talk about, but it’s
good that you did.’
■ The consumer’s response should be documented in
their file using the consumer’s own words.
■ An evaluation should immediately be carried out
regarding the present-day level of danger – refer to
Section 5 Responding to a sexual safety incident for
further advice on actions to take when a sexual
assault has been disclosed.
■ If there is no immediate danger, the consumer
should be:
– asked if they have previously disclosed the assault
or abuse and received any support or treatment:
‘Have you had the opportunity to talk to anyone
about this before?’
‘Have you had any support or help to deal with
your feelings about what happened?’
– offered appropriate follow-up and counselling:
‘Sexual assault is devastating in many ways. Let’s
talk about some things we could do to support you.’
■ If support is initially refused, staff should ask the
consumer if they are comfortable to talk again about
their disclosure and support options and set a time
for this.

PaGe 26 NSW HealtH Sexual Safety of Mental Health Consumers Guidelines
■ Consideration should also be given to how
re-traumatisation could be prevented. If the past
assault occurred in the current or another mental
health facility, every effort must be made to not place
the consumer back in the same environment and/or
to discuss what might be helpful for the consumer in
decreasing the risk of re-traumatisation.
■ Where there is no disclosed history of previous sexual
assault, clinical practice can still operate from the
premise that this history is a possibility. The consumer
should also be advised that support is available in the
future if they wish to re-visit this topic at a later date:
‘That’s fine – the reason we ask is that we like to
offer people the opportunity to get some support if
they want it.’
■ The admission process will also need to take account
of any history the consumer may have of violent
offending, as this can alert staff to potential problems
and inform care plans to maximise monitoring of
those deemed at risk for violence.
■ Disclosure of alleged sexual assault by a person who
may be working with or who has access to children or
young people requires a report to the Child Protection
Helpline.
4.1.3 Recognising offender tacticsSexual assault can involve a one-off opportunistic event
or a series of ongoing aggressive attacks, but they can be
planned attempts designed by those who perpetrate
sexual assault to coerce another person to provide
sexual favours.
In this situation, deliberate tactics are used to select and
abuse vulnerable or desirable individuals. These tactics
could include:
■ Recruiting these individuals by means of bribes
(money, cigarettes, food, other items) or offering
perceptions of care, love and intimacy
■ Utilising power/positions of power to gain confidence
and trust for the purposes of gaining sexual favours
■ Maintaining this accessibility by using threats to
discourage the individual from disclosing the assault
■ Grooming staff by ingratiating themselves as helpful
and suggesting to staff that the individual they
assaulted is lying
Conditions such as organic brain syndromes may include
sexually aggressive behaviours and require appropriate
supervision where this occurs.
4.1.4 The role of gender sensitivity4
Health policies that are gender neutral assume that men
and women are affected equally or in a similar manner by
ill health. However, because of social and biological
differences, women and men face different health risks,
experience different responses from health systems, and
their health-seeking behaviour and health outcomes
differ (WHO, 2006).
For example, throughout their lifetime, women are more
likely to be affected by physical and sexual abuse
(WHO, 2006)., and have a higher degree of lifetime
exposure to sexual abuse and violence (McGee, 2002).
Nonetheless, there should be no bias or any assumptions
made by services when a sexual assault is reported or
disclosed by a consumer who is a man.
A significant proportion of adults who were sexually
abused as children are male, and male consumers who
are Gay, Bisexual or Transgender (refer to Section 7.4, p. 63)
may have increased vulnerability to sexual victimisation.
Men who are heavily sedated are also more vulnerable to
sexual assault. When consumers who are sedated
experience a sexual assault, the powerlessness they feel
will often be magnified due to their loss of control and
choice in such a situation.
The impact of such an experience for a man will not in
any way be more significant than for a woman, but may
give rise to additional issues because of cultural/social
expectations of men. Evidence suggests that services who
recognise these gender differences within their care
provision, that is those who are ‘gender-sensitive’, achieve
better health outcomes for consumers.
4 Information in this section is drawn from the Women’s Centre for Health Matters paper entitled ‘Gender Sensitive Mental Health Service Delivery’, April 2009.

Sexual Safety of Mental Health Consumers Guidelines NSW HealtH PaGe 27
Gender sensitive practices
In the context of a mental health service, gender-sensitive
practices include:
■ Offering choices about the type of support consumers
receive, and who provides it to them (e.g. a choice
between a male or female doctor, care coordinator
and advocate).
■ Providing opportunities for consumers, but women in
particular, to be involved in their own care and
treatment, including service planning and delivery.
■ Having staff that treat both women and men with
respect, give them time to talk and listen to what
they have to say.
■ Having ‘women only’ spaces within their buildings
(see 4.1.5 Improving the physical environment).
■ Seeing mental health from a holistic perspective, that
is, they consider mental health in the context of the
consumer’s life experiences and personal situations.
■ Taking into account the ‘social determinants of
health’, that is, they acknowledge the way that
women’s and men’s personal circumstances and
socioeconomic status affects their mental health.
■ Recognising a consumer’s strengths and empowering
them to take control of their own lives.
■ Operating in a way that is culturally sensitive to
women from outside the dominant culture.
Gender sensitive seclusion and restraint practices
Where seclusion or restraint is used, there needs to be
additional sensitivity. Re-experiencing trauma or abuse
may trigger the ‘fight, flight or freeze’ response, which
will produce a catecholamine (adrenal) flood. Every effort
should be made to avoid retraumatising or triggering
events in individuals with trauma histories. Where this is
unavoidable, same gender staff should be allocated and
consumers should be adequately clothed.
An audit to assess the current level of gender sensitivity
within the service should be undertaken to determine
priorities for action to increase safety and gender sensitivity.
This audit should be carried out every two years.
4.1.5 Practical security measures
Improving the physical environment
Making improvements to the physical environment of a
facility can have a real and positive impact on addressing
sexual safety issues for consumers. The suggestions
provided here regarding changes to the physical
environment are supported by the Australasian Health
Facility Guidelines.
However, it is recognised that implementing these
changes in some facilities may be difficult. Services should
work towards introducing similar changes to their
facility’s physical environment where the layout of the
existing facility allows this, and taking account of these
suggestions when planning any new facilities.
The NSW Policy Directive Protecting People/Property:
NSW Health Policy/Guidelines for Security Risk
Management in Health Facilities (PD 2005_339) provide
advice for Health Services on maintaining an effective
security program that is based on a structured, ongoing
risk management process, consultation, appropriate
documentation and record keeping and regular
monitoring and evaluation.
Single gender corridors/accommodation and bathrooms
Establishing corridors/accommodation and bathroom
facilities that are specifically for each gender can greatly
improve the feeling of safety for women. Where the
design of the unit features a number of corridors
radiating out from the nurse station, particular corridors
can be designated as either female or male, dependent
upon the needs of the service.
Alternatively, where the unit has a long, circular corridor
with limited visibility, a lockable door could be
constructed at the halfway point of the horseshoe with
one half designed as female and the other male.
Women’s lounges
Women’s lounges can play an important part in helping
women to feel safe and more relaxed as well as providing
a space where supportive contact between other female
consumers and therapeutic relationships with staff can
be promoted.

PaGe 28 NSW HealtH Sexual Safety of Mental Health Consumers Guidelines
Existing lounge areas located in women’s corridors could
be designated as women specific or areas which had
previously been used as interview rooms could be used
for this purpose. These lounges could be established as a
sensory /therapeutic room for women with sensory
equipment and a massage chair, or used as a venue for
women specific group activities.
Family visiting areas
The establishment of gender specific areas where
consumers with children and families can visit can
enhance the safety and amenity of inpatient
environments for these groups.
Family visiting areas need to be located near the entrance
to the ward as it is not desirable for children to go through
the main part of the psychiatric unit to visit their parent.
Nurse call buttons
The provision of nurse call buttons enables consumers to
call for staff assistance in case of emergency. Nurse call
buttons could be located in both bedrooms and
bathrooms and promoted to consumers within their
orientation so that they are aware of their existence.
Lockable bedroom doors
Being able to lock themselves in their bedrooms can
greatly contribute to a consumer’s feeling of security at
night. Consumers could either ask to have their bedrooms
locked from the outside, or a mechanism could be utilised
that allows staff to override the locks and gain access
if required.
Sensory motion detectors
Sensory motion detectors installed in all bedrooms can be
activated at night and alert staff if consumers leave their
rooms. These detectors can support staff to monitor
consumer movement and to prevent inappropriate access
to other consumer’s rooms, promoting safety and privacy.
Signage
Clear signage in inpatient units can help to stop
inadvertent accessing of male/female areas. When the
consumer is acutely unwell their usual cognitive abilities
may be impaired, so signage and clear labelling can
support consumers to read environmental cues.
Labels should be easily understood, with accepted symbols
given preference over written language where possible.
Increased vigilance
Increasing vigilance and observation at particular times
when staff are less available is a simple yet effective way
to increase the safety and security of the service
environment. This could include night time, when handover
occurs and during ward rounds, when consumers are
more vulnerable. A constant staff presence is required in
acute inpatient units, including overnight.
Screening of staff
The screening of staff (including volunteers) who apply
for roles within a mental health service must be managed
in accordance with NSW Health’s policies on recruitment
and employment screening.
The introduction of increased screening of staff who
apply for roles within a mental health service, similar to
the working with children check undertaken for those
who work with children, should also be considered as
part of an overall sexual assault prevention strategy.
4.1.6 Maintaining professional boundaries Staff in mental health services, like other public sector
employees, must conduct themselves in a way that promotes
public confidence and trust in their organisation. They
have a duty of care to the consumers utilising the service
in which they work as well as to other staff.
For the purposes of this policy, the definition of staff
includes the following individuals that perform work
within NSW Health facilities:
■ Volunteers
■ Consumer advocates
■ Contractors
■ Visiting practitioners or Medical Officers
■ Students; and
■ Consultants and researchers.
NSW Health Code of Conduct
The NSW Health Code of Conduct (PD2012_018) sets out
the conduct expected of health staff and applies to staff
working in any permanent, temporary, casual, termed
appointment or honorary capacity within any NSW Health
facility, which includes mental health service environments.
The Code of Conduct makes it clear that sexual
involvement with a consumer is a breach of professional
and ethical boundaries:

Sexual Safety of Mental Health Consumers Guidelines NSW HealtH PaGe 29
NSW Health Code of Conduct
Sexual relationships with patients or clients – Section 1.5 I will not exploit my relationship of trust with patients or clients in any way because I recognise that such behaviour is a breach of professional and ethical boundaries and amounts to serious misconduct. I will not have a sexual relationship with a patient or client during the professional relationship.
Relevant legislation
Sexual activity between a NSW Health staff member and
a consumer may constitute a sexual offence under various
sections of the Crimes Act 1900 (NSW) even if the
consumer has not alleged to have been sexually assaulted
and/or appears to have consented to the sexual activity.
Under Section 61 of the Crimes Act, a person is not
considered to have consented to sexual intercourse if:
■ they do not have the capacity to consent, including
because of age or cognitive impairment;
■ they have the mistaken belief that the sexual
intercourse is for medical or hygienic purposes;
■ they are substantially intoxicated by alcohol or any
drug;
■ there has been an abuse of a position of authority
or trust.
Under Section 66F (2) of the Crimes Act, a person who
has sexual intercourse with a person who has a cognitive
impairment, such as a mental illness, and who was
responsible for the care of that person, whether generally
or at the time of the sexual intercourse, is guilty of an
offence. Further information about this Act is provided at
Appendix C.
Under Section 66 of the Crimes Act, any person that has,
or tries to have sexual intercourse with an under 16 year
old, or engages in the ‘grooming’ of children (as defined
in the Act) is guilty of an offence.
Under Section 73 of the Crimes Act, a person who has
sexual intercourse with a child aged between the age of
16 and under 18 when they are in a special care
relationship is guilty of an offence punishable by up to
eight years prison.
Under section 25A of the NSW Ombudsman Act,
allegations against NSW Health staff of sexual assault or
sexual misconduct involving anyone under the age of 18
years are required to be notified by the Chief Executive to
the NSW Ombudsman and investigated by the employer.
Notifications are also required to the Commission for
Children and Young People where there is evidence that
the conduct has occurred. Refer to the NSW policy
directive (PD2006_025) Child Related Allegations,
Charges and Convictions against Employees.
Although the Anti-Discrimination Act 1977 (NSW)
makes sexual harassment a civil not criminal offence,
some types of harassment may also be offences under
the criminal law. These include:
■ physical molestation or assault
■ indecent exposure
■ sexual assault
■ stalking
■ obscene communications such as telephone calls
and letters.
The Medical Practice Act 1992 also places an obligation
on all registered medical practitioners in NSW to report
certain types of misconduct by other registered medical
practitioners to the Medical Council of New South Wales.
This includes sexual misconduct in the practice of
medicine. Further advice about this Act is provided within
Appendix C.
KEY ACTIONS/POINTS FOR ALL SETTINGS
■ A breach of professional boundaries can occur if a
mental health worker displays sexualised behaviour
towards a consumer. This is not limited to criminal
acts such sexual assault but could also include
behaviour such as conducting clinically unjustified
physical examinations.
■ Appendix H expands on the types of sexualised
behaviour that may constitute a breach of professional
boundaries.
■ If a mental health worker becomes sexually attracted
to a consumer and has concerns that this may affect
their professional judgement, they should seek
guidance from their manager or discuss the matter
with a colleague. The development of a culture within
mental health facilities which supports staff to discuss

PaGe 30 NSW HealtH Sexual Safety of Mental Health Consumers Guidelines
ethical conduct regularly and to report or raise
concerns/observations is important.
■ If the mental health worker’s manager, or the worker
themselves, believes that their professional judgement
is impaired, they should:
– Find alternative care for the consumer
– Ensure a proper handover of care, where
necessary
– Ensure the consumer does not feel that they are in
the wrong as a result of the handover of care to
another clinician or worker
KEY ACTIONS/POINTS FOR ACUTE INPATIENT
■ In an inpatient setting, consumers are extremely
vulnerable.
■ Maintenance of professional boundaries in this setting
can be supported by strategies such as using a
chaperone when conducting any examinations of a
physical or intimate nature and organising for female
staff, wherever possible, to treat consumers,
particularly at night.
KEY ACTIONS/POINTS NON-ACUTE/RESIDENTIAL
AND COMMUNITY
■ In a situation where a mental health worker is
attracted to a consumer they must be careful not to
display any sexualised or inappropriate behaviour
towards them. Outside of the inpatient setting,
sexualised behaviour can include:
– Revealing intimate details to a consumer during a
professional consultation
– Giving or accepting social invitations where this is
sexually motivated
– Visiting a consumer’s home unannounced and
without a prior appointment
– Seeing consumers outside of normal practice
– Clinically unnecessary communications
4.2 Consensual sexual activity in an inappropriate context or setting
Sexual activity is a natural and healthy part of life, and for
mental health consumers, reaching out to someone
sexually can be a way to attain reassurance through
affection and touch. However, when it occurs in an
inappropriate context or setting it can be detrimental to
those consumers involved as well as to any consumers
that may witness the activity.
4.2.1 Sexual safety standardsHaving a set of standards that clearly defines appropriate
behaviour for consumers in relation to sexual safety will
help such behaviour to be adopted. An example set of
standards for an acute inpatient and a non-acute/residential
and community setting is provided at Appendix A.
However, services should use these examples as a guide
only – standards should be developed collaboratively with
staff and clinicians, consumers, families and carers,
advocates etc so that they are meaningful and
representative of the service’s own individual ethos.
An annual review of these standards should be
undertaken to maintain their relevance, which should
involve consultation with and input from all of the
above stakeholders.
4.2.2 Addressing sexuality needs Staff should remember that sexuality is a normal part of
life and just because the consumer has a mental illness
does not mean they do not have normal sexual needs. A consumer may need others to give them space and
privacy to express or meet their sexual needs e.g. privacy
to masturbate, watch videos or, in a non-acute inpatient,
rehabilitation or community setting, to have a sexual
relationship.
Masturbation can be a safe alternative to sexual activity
with another person and is appropriate for consumers
receiving treatment in any setting. It carries no risk of
sexually transmissible infection or unwanted pregnancy
and can also be beneficial from a health perspective,
as it promotes the release of the brain’s opiod-like
neurotransmitters (endorphins), which cause feelings of
physical and mental wellbeing.
‘The greatest and most healing service that can be offered to people with psychiatric disabilities is to treat them with respect and honour them as human beings. This means honouring us in our full humanity, including our sexuality and our desire to love and be loved.’
(Deegan, 2001)

Sexual Safety of Mental Health Consumers Guidelines NSW HealtH PaGe 31
KEY ACTIONS/POINTS FOR ALL SETTINGS
■ All mental health services have a responsibility to
develop individual sexual safety standards appropriate
for their particular setting. These must be developed in
consultation with all members of the service e.g. staff
and clinicians, consumers, families and carers etc.
■ These standards should be explained and also
promoted regularly to both consumers and staff so
that they become embedded in service practice.
■ Staff may benefit from training on how to talk about
sexual safety and sexual health issues with consumers
(see Section 3.1 Training and Education for more
information).
■ Education on sexuality and managing sexual
relationships appropriately should also be offered to
consumers so that they understand the positive
expression of sexuality and can distinguish it from
sexual assault.
■ Clear advice must be provided to consumers and their
families and carers regarding the need for expressions
of sexuality, such as masturbation, to be conducted in
a place and at a time that will ensure it remains
private. It will also be important to ensure that the
sexual safety standards for the service include this
stipulation, and that consumers are aware of the need
to adhere to these standards at all times.
■ If masturbation seems to be taking place excessively,
for example if it is interfering with day to day living,
or taking place in inappropriate situations, it may
indicate other issues which need to be addressed.
KEY ACTIONS/POINTS FOR ACUTE INPATIENT
■ Consensual sexual activity is not supported in an acute
inpatient setting due to the extreme vulnerability of
the consumer/s involved, as well as the vulnerability
of the consumers that may witness any such activity.
Consumers in this setting are generally very unwell,
which makes the consensual, voluntary and mutual
nature of any sexual activity difficult to confirm.
■ Information about this restriction will need to be
included within the information provided to the
consumer and explained, along with the rationale for
its existence, to the consumer and their partner and
family or carer. This should be undertaken with extreme
sensitivity so that the restriction is recognised as being
beneficial for the consumer’s safety and care, which is
paramount, rather than misinterpreted as an action
that is meant to further disempower them.
KEY ACTIONS/POINTS FOR NON-ACUTE/
RESIDENTIAL AND COMMUNITY
■ While consensual sexual activity for consumers who
receive treatment in these settings is recognised as a
normal and healthy part of life, consumers can still be
vulnerable to sexual assault and harassment and/or
sexually abusive relationships.
■ Consumers in these settings should be offered
information and access to education that will support
them to understand how to manage sexual
relationships safely or to recognise and appropriately
respond to unwanted sexual advances (see Education
and Training for more information).
■ Consumers should also be provided with clear advice
regarding how to report an incident of sexual assault
or sexual harassment, and encouraged through
education around resilience and building self-esteem
to speak up when they or someone else is being
mistreated.
■ Additionally, consumers in a non-acute/residential
setting must be provided with a copy of the sexual
safety standards for the service, which should be
explained and discussed as required.
4.3 Sexually disinhibited behaviour
Prevention of sexually disinhibited behaviour, whether it is
associated with the consumer’s mental illness or with a
physical condition or disease, such as dementia, will
require correct assessment, vigilance and a high level of
support for the consumer so that the risk of them being
sexually assaulted or assaulting others, being exploited or
exploiting others, and retraumatisation of consumers
witnessing the behaviour, is minimised.
While the behaviour is generally best managed through
the consistent use of simple behavioural techniques, this
approach is less likely to be successful with consumers
who have dementia due to the way in which the disease
impairs new learning. Sexually disinhibited behaviour
occurs at some point in most people with dementia,
particularly those that are men, and is more common
when the disease is mild rather than severe.

PaGe 32 NSW HealtH Sexual Safety of Mental Health Consumers Guidelines
KEY ACTIONS/POINTS FOR ALL SETTINGS
■ Consumers will need to be assessed by the senior
clinician at the time of admission regarding both their
vulnerability to sexual assault and exploitation and
their potential to assault or exploit others (see 4.1.1
Assessing vulnerability pg 36). This assessment will
need to consider the likelihood of the consumer
exhibiting sexually disinhibited behaviour, any previous
occurrences and whether the behaviour is linked to
their mental illness or is a result of a physical condition
or disease (e.g. dementia) or substance misuse.
■ Other key factors to consider within this assessment
include:
– The form the behaviour takes and the context in
which it occurs
– The frequency of the behaviour
– Contributing factors or triggers
– Whether the behaviour is problematic and if so
to whom
– The risks associated with the behaviour
■ This assessment will support development of an
appropriate, agreed and comprehensive management
plan. In developing the management plan, services
should take account of:
– The need for a higher level of supervision and
monitoring, and the capacity of the service to
provide this
– How to reinforce appropriate behaviour and
clothing
– Any medication that should be prescribed in the
treatment of the sexual disinhibition
– How to minimise retraumatisation for those who
have experienced a previous sexual assault
– Strategies to distract the consumer should their
behaviour be associated with dementia
– Any changes required to the service setting to
provide safety for other consumers and staff and
privacy for the consumer who may exhibit the
behaviour
– How and what to communicate to the consumer
and their family and carer/s about the behaviour
and how it can be managed
■ Appendix L – Information about managing disinhibited
behaviour provides further advice regarding factors to
consider in the management plan.

Sexual Safety of Mental Health Consumers Guidelines NSW HealtH PaGe 33
KEY POINTS – PREVENTING A SEXUAL SAFETY INCIDENT
Sexual assault and harassment
Assessing the mental health consumer for vulnerability and prior assault
■ The vulnerability of a consumer should be assessed at
the time of admission in all settings. This includes
taking a sexual assault and harassment history.
■ Taking a consumer’s sexual assault history on their
admission to a mental health service is critical to
enable staff to adequately support the consumer,
both in terms of their illness and their sexual safety
while involved with the service. A screening tool to
help with this process is available at Appendix G and
further information is provided in section 4.1.2
■ Only those staff who have received appropriate
training in taking a sexual assault history should
manage this process, or support should be
sought from the local Sexual Assault Service.
■ Where there is no disclosed history of previous sexual
assault, clinical practice can still operate from the
premise that this history is a possibility.
■ Taking a consumer’s history of perpetrating sexual
assault is also vitally important.
Gender sensitivity
■ Throughout their lifetime, women are more likely to
be affected by physical and sexual abuse (Astbury,
2001), and have a higher degree of lifetime exposure
to sexual abuse and violence (McGee et al., 2002).
■ However, a significant proportion of adults who were
sexually abused as children are male, and male
consumers who are Gay, Bisexual or Transgender
(refer to Section 7.4) may have increased vulnerability
to sexual victimisation.
■ Evidence suggests that services who recognise gender
differences within their care provision, that is those
who are ‘gender-sensitive’, achieve better health
outcomes for consumers.
■ An audit to assess the current level of gender
sensitivity within the service should be undertaken to
determine priorities for action to increase safety and
gender sensitivity. This audit should be carried out
every two years.
■ A key strategy to consider in addressing gender-
sensitivity and improving security for consumers is to
establish gender specific accommodation. Other
practical examples of how the physical environment
could be improved to take account of gender-sensitive
practices are provided in section 4.1.4.
Practical security measures
■ Practical security measures have an important part to
play in improving the sexual safety of mental health
consumers in an inpatient or long term residential or
rehabilitation setting and can include:
– Increased vigilance
– Nurse call buttons
– Lockable bedroom and bathroom doors
– Sensory motion detectors
– Clear signage
Staff conduct
■ The NSW Health Code of Conduct (PD2012_018),
which sets out the conduct expected of health staff,
makes it clear that sexual involvement with a
consumer is a breach of professional and ethical
boundaries.
■ Sexual activity between a NSW Health staff member
and a consumer may also constitute a sexual offence
under various sections of the Crimes Act 1900 (NSW).
See section 4.1.6 and Appendix C for further
information.
Consensual sexual activity in an inappropriate context or setting
■ All mental health services have a responsibility to
develop individual sexual safety standards appropriate
for their particular setting. These must be developed
in consultation with all members of the service and
provided to consumers and their families and carers
on admission.
■ Consensual sexual activity is not supported in an acute
inpatient setting due to the extreme vulnerability of
the consumer/s involved, as well as the vulnerability of
the consumers that may witness any such activity.
■ Consensual sexual activity for consumers who receive
treatment outside of the acute setting is recognised
as a normal and healthy part of life. However, any
such activity must adhere to the sexual safety
standards for the service.
Sexually disinhibited behaviour
■ An assessment will need to be carried out by the
senior clinician at the time of a consumer’s admission
regarding the likelihood of the consumer exhibiting
Sexual Safety of Mental Health Consumers Guidelines NSW HealtH PaGe 33

PaGe 34 NSW HealtH Sexual Safety of Mental Health Consumers Guidelines
sexually disinhibited behaviour and any previous
occurrences.
■ This assessment will support development of an
appropriate, agreed and comprehensive management
plan for the consumer, which should consider factors
such as additional supervision, behavioural strategies,
medication etc. See section 4.3 and Appendix L for
further information.
PaGe 34 NSW HealtH Sexual Safety of Mental Health Consumers Guidelines

Sexual Safety of Mental Health Consumers Guidelines NSW HealtH PaGe 35
5.1 Sexual assault and harassment
There are four main ways that sexual assault involving a
consumer may come to the attention of another person:
■ the consumer tells someone they have been sexually
assaulted;
■ the sexual assault or exploitative behaviour is
observed by a third party;
■ the behaviour of the consumer changes significantly; or
■ the consumer complains of physical symptoms or they
are observed by another person.
5.1.1 When there is disclosure or acknowledgement of sexual assault or harassment
Disclosure means telling another person about an incident
of sexual abuse, sexual assault, or sexual harassment, or
acknowledging to another person that this has occurred,
whether the incident is recent, past or ongoing.
Disclosure or acknowledgement is distinct from making a
report or allegation (even if sometimes they are one and
the same event). Disclosure is about support-seeking,
while reporting to Police and making allegations are
formal mechanisms to bring an incident to the attention
of law enforcement and other agencies. The following
information provides guidance about the key actions to
take when a disclosure of sexual assault is made. These
actions are summarised in Appendix I and a quick
checklist provided at Appendix J.
Acknowledging and affirming the disclosure
KEY ACTIONS/POINTS FOR ALL SETTINGS
■ Disclosing an incident of sexual assault or harassment
can be traumatic.
■ The fear of not being believed, an issue for many who
are assaulted, may be heightened for people with a
mental health problem or mental illness. The stigma
that surrounds mental health problems or mental
illness can result in a consumer feeling their
experiences are not legitimate.
■ When a consumer discloses past, recent or ongoing
sexual assault or harassment it is essential that staff
believe and validate the consumer’s experiences rather
than make assumptions about what has happened, or
how the consumer feels about the incident
■ Staff have a responsibility to initiate and adhere to the
formal process outlined within these guidelines to
respond to disclosures of sexual assault or harassment
until assessment of the consumer’s clinical mental
state determines otherwise (see advice under
Exploring the Disclosure).
■ Implicit in the provision of a caring and effective
response is the understanding that no-one ever
deserves to be sexually assaulted or harassed. A
judgmental or indifferent response to a disclosure can
negatively impact the recovery process.
Exploring the disclosure
KEY ACTIONS/POINTS FOR ALL SETTINGS
■ The consumer who has disclosed the sexual assault
should immediately be provided a safe, quiet and
private space.
■ Staff should let the consumer tell them in their own
words and at their own pace about their experience
and concerns, and unnecessary or repeated
questioning should be avoided as this may cause
distress.
■ Once they feel able, the consumer should be gently
encouraged to provide staff with brief details about:
– the name of the alleged perpetrator
– where and when the alleged assault or harassment
took place
– any injuries or other concerns that may require
medical attention
■ Any questioning that is required should be ‘open not
closed’ questioning to prevent any risk of contamination
of evidence if a matter proceeds to court. Examples of
open-ended questions are, ‘Can you tell me more?
What happened next? Did anything else happen?
When did this happen?’ and so on. These are
clarifying questions.
SECTION 5
Responding to a Sexual Safety Incident

PaGe 36 NSW HealtH Sexual Safety of Mental Health Consumers Guidelines
■ Consumers may at times retract a disclosure. This may
be due to a failure of staff to believe them, and/or
because of undue pressure, with negative outcomes
for a consumer who persists with a disclosure.
■ In the case of individuals who have a refugee
background, mistrust of authorities such as health
services due to previous political persecutions or
torture may result in a retraction.
■ A retraction does not mean that an incident of sexual
assault or harassment did not occur and that no
assessment should take place.
■ Pursuing the issue may be difficult without clear
support. However should a consumer retract a
disclosure, the incident should still be reported and
recorded (see Reporting and Recording). Should the
disclosure involve a NSW Health staff member, the
reasons for the disclosure may need to be considered
and an internal investigation still completed with a
recorded outcome.
■ Disclosures, where the alleged perpetrator is a NSW
Health employee, must be notified to the relevant
manager and managed in accordance with NSW
Health policies for managing child related and criminal
allegations against employees.
■ Where the disclosure relates to a risk of significant
harm to a child or group of children, the Child
Protection Helpline must be notified.5
KEY ACTIONS/POINTS FOR ACUTE INPATIENT
■ An assessment of the consumer’s clinical mental state
must be carried out by the senior clinician (where not
involved in the allegation) within 24 hours.
KEY ACTIONS/POINTS FOR NON-ACUTE/
RESIDENTIAL AND COMMUNITY
■ An assessment of the consumer’s clinical mental state
must be carried out by the senior clinician (where not
involved in the allegation) within 48 hours.
5 The NSW Government Mandatory Reporter Guide (including a decision tree for sexual assault) can be found at: http://dr.sdm.community.nsw.gov.au/mrg/app/summary.page;jsessionid=B13F2B7E7C8AFBC0DE2854A2F1E2F6AC
Establishing and maintaining safety
KEY ACTIONS/POINTS FOR ALL SETTINGS
When the alleged perpetrator is a consumer
■ If the consumer who has disclosed the sexual assault
wishes to be moved to another room or unit/facility/
service, this request should be accommodated where
possible.
■ The consumer who has disclosed the sexual assault
and the person who has been named as the perpetrator
should be separated. The alleged perpetrator should
be moved to another facility, unless the consumer
who has disclosed the assault specifically requests
otherwise or there are other extenuating circumstances.
This helps to address the feelings of self-blame that
victims/survivors of sexual assault often experience.
■ If staff have reason to believe the alleged perpetrator
poses some ongoing risks to the consumer who has
disclosed the assault or other consumers, all
reasonable steps should be taken to minimise risk,
including a comprehensive ongoing risk management
strategy to prevent any harm.
■ Where the alleged perpetrator is a consumer and the
person who has disclosed the assault is a child, for
example a visiting family member, a report to the
Child Protection Helpline (phone 13 36 27) should be
made, in addition to taking steps to minimise further
risk to the child, or other consumers or staff in the
service. Where the consumer who has disclosed the
assault is a young person, a report may be made to
the Child Protection Helpline. Reports should be made
in accordance with the NSW Health Frontline Policies
and Procedures for Child Protection and Wellbeing
(revised procedures being finalised at the time of
printing).
When the alleged perpetrator is a NSW Health
employee
■ Allegations or disclosures of sexual assault against
NSW Health staff members must be reported to a
relevant line manager and to the NSW Police Force or
to the Child Protection Helpline depending on the
current age of the victim.
■ Allegations of sexual misconduct or sexual assault
against NSW Health staff members involving under 18
year olds must be reported to a relevant line manager
and will require a notification to the NSW Ombudsman.

Sexual Safety of Mental Health Consumers Guidelines NSW HealtH PaGe 37
■ An immediate risk assessment must be conducted to
determine whether there is any risk to consumers or
employees and whether the staff member subject to
the allegation requires relocation, supervision or
suspension. Once an initial risk assessment is
completed, the service must liase with NSW Police or
Community Services regarding the commencement of
an internal investigation.
■ Any allegations that involve NSW Health staff members
must be managed in accordance with the relevant
policies for managing child related or criminal allegations
against staff. And for managing the disciplinary process.
■ A decision regarding whether an entry is required on
the NSW Health Service Check Register must also be
considered.
■ Where an allegation involves the conduct of a health
practitioner or health service provider that is not a
criminal offence, and does not involve a consumer
under 18 years of age, the NSW Health Policy
Directive concerning the management of a complaint
or concern about a clinician (Complaint or concern
about a clinician – principles for action PD2005_007)
should be consulted and appropriate action should be
taken to inform registration authorities and other
bodies, as relevant.
When the alleged perpetrator is a family member
or person in a position of continuing power or
authority over the consumer
■ Staff should consult with their supervisor or appropriate
senior manager to explore how to establish and
maintain the safety of the consumer in these particular
circumstances. This may include approaching the
Guardianship Tribunal about the concerns or seeking
advice from the Police about obtaining an
Apprehended Violence Order (AVO) for the consumer.
Securing any evidence
KEY ACTIONS/POINTS FOR ALL SETTINGS
■ If the sexual assault has occurred within the last seven
days, staff should immediately secure any evidence
related to the sexual assault pending Police
involvement, or until the consumer disclosing the
sexual assault has made a definite decision not to
involve the Police. At the first opportunity, the senior
manager or supervisor should also consult with the
local Sexual Assault Service, being mindful to
maintain the privacy of the consumer.
■ Securing the evidence will involve:
– Keeping any clothing that the consumer who
has experienced the sexual assault was wearing at
the time of the assault – these should only be
handled by the consumer to minimise DNA
contamination and kept in a safe place in a paper,
not plastic, bag and not washed. Appropriate bags
can be obtained from the local Sexual Assault
Service.
– Securing the location of the assault if possible to
prevent any evidence being disturbed.
– Securing any CCTV footage of the incident area
– this footage will be required by investigators.
Offering support and options
It is not uncommon for someone who has experienced a
sexual assault to minimise their feelings about an assault
or to feel that they do not deserve any assistance.
However, reassurance that there are services and
professionals able to provide assistance and advocacy is
important. Support can help to validate the consumer’s
experience, and assist them to take appropriate steps to
deal with a sexual assault.
A sexual safety incident, particularly an assault, can also
be stressful for staff. Support and an opportunity to
debrief should be offered to the staff member to whom
the disclosure was made, particularly when this is a
consumer advocate or worker, and to all staff connected
with the incident. The local Sexual Assault Service may be
able to help with this.
KEY ACTIONS/POINTS FOR ALL SETTINGS
■ Staff should calmly outline the available options so
that the consumer who has experienced the sexual
assault can make an informed decision about how
they want to proceed. It is important that they do not
feel pressured to take a particular course of action.
Information about available options is provided at
Appendix D.
■ The consumer who has experienced the sexual assault
should be informed that they can choose a support
person, such as a consumer worker, family member,
friend or a staff member that they know and are
comfortable with.
■ If the consumer does not wish to inform their carer or
family, their wishes must be respected, within the
limits of legislation. If the consumer’s carer and family
are informed, they can be referred independently to

PaGe 38 NSW HealtH Sexual Safety of Mental Health Consumers Guidelines
the local Sexual Assault Service to learn how they can
best support the consumer.
■ An interpreter should be made available for the
consumer who has experienced a sexual assault who
has communication difficulties, for example a
consumer with limited English language proficiency or
those who are deaf or have a hearing impairment.
■ Staff are not required to report a sexual assault to
Police if this is against the wishes of the consumer
who has experienced a sexual assault, except where:
– the alleged perpetrator is identified as a NSW
Health staff member, or
– the consumer is a child under the age of sixteen,
or
– the consumer does not have the capacity to make
an informed decision and the senior clinician has a
duty of care to act in the consumer’s best interests.
■ All allegations that involve possible criminal conduct
involving a staff member must be reported to the
NSW Police Force. Where the NSW Police Force
undertakes or is undertaking an investigation, an
ongoing liaison should be maintained to ensure that
investigations are coordinated and re-interviewing is
minimised or prevented.
■ If the consumer decides to report the assault, staff
should offer to immediately refer the consumer to
their local Sexual Assault Service and/or arrange for
the consumer to talk to the on-call sexual assault
counsellor about their options and what services the
Sexual Assault Service can provide – including a
medical and/or forensic examination, crisis and
ongoing counselling and support, and assistance
reporting to the Police.
■ If a referral is made to a Sexual Assault Service, staff
should inform the on-call counsellor about the
consumer’s capacity to consent, any guardianship
arrangements that are in place, whether an
interpreter or other support services are required, and
whether the consumer has any injuries or medical
issues that require immediate treatment.
■ At all times, however, staff should be guided by the
wishes of the consumer who has disclosed the sexual
assault, where possible. It is important that the
consumer retains control over decisions, including the
decision to report the crime to the NSW Police Force
or to contact the Sexual Assault Service.
■ This does not prevent the service from consulting with
the NSW Police Force and the Sexual Assault Service
as long as the consumer is de-identified.
The consumer who has experienced a sexual assault should be informed that:
■ They can have the support of a consumer worker, family member, friend, staff member, care coordinator, advocate or other significant person in any interviews.
■ They can have access to the local Sexual Assault Service (SAS) for counselling, help in completing a Police report and legal representation, or to simply assist them to make informed choices and decisions.
■ Their right to privacy and confidentiality, within the limits of legislation, will be respected at all times.
■ Their informed decisions will be respected at every stage of the process.
■ It is their decision whether or not to involve the Police and participate in a Police investigation, except in certain circumstances (e.g. where the alleged perpetrator is an employee of the service – reporting is mandatory in these circumstances).
Adapted from the VIC Chief Psychiatrists Guidelines –
Promoting sexual safety, responding to sexual activity
and managing allegations of sexual assault in adult
acute inpatient units
Organising medical care
It is important that consumers who disclose sexual assault
are offered medical assistance to treat any physical or
psychological injuries, regardless of whether the assault
or harassment was recent or occurred some time ago.
Medical care can involve managing physical injuries
(including concerns about pregnancy or sexually
transmitted diseases), psychological impacts, and possible
forensic examinations (to collect any physical evidence
that may be used if criminal charges are laid).

Sexual Safety of Mental Health Consumers Guidelines NSW HealtH PaGe 39
Assessment and treatment of physical injuries
KEY ACTIONS/POINTS FOR ALL SETTINGS
■ The consumer who has disclosed a recent sexual
assault should be encouraged to seek immediate
medical assistance to identify and treat any physical
injuries they may have sustained as a result of the
assault.
■ Provided the consumer has given permission for the
service to contact them, the local Sexual Assault
Service can organise this. If permission has not been
given for Sexual Assault Service involvement, the
Sexual Assault Service can still be consulted regarding
current clinical practice to ensure the most effective
treatment is provided.
■ Where appropriate, the risk of infection or pregnancy
should be discussed with the consumer, and testing
recommended. (It should be noted that morning after
pills are most effective taken within 72 hours of
the assault.)
■ Follow-up medical assessments for the consumer are
recommended at two weeks, three months and six
months post assault and services should liaise with
the local Sexual Assault Service involved, or the
consumer’s GP if relevant, regarding appointments for
these assessments to occur. Further information about
the medical assessments required when a person has
been sexually assaulted is provided at Appendix K.
KEY ACTIONS/POINTS FOR ACUTE INPATIENT
■ If the consumer who has disclosed the sexual assault
decides not to involve the local Sexual Assault Service,
the service itself will need to consider the medical
needs of the consumer and organise a medical
assessment, with the consumer’s consent.
■ Staff must ensure that any assessment of or medical
treatment for the consumer in the acute inpatient
setting is carried out with the consent of the
consumer, where they have the capacity to provide
this (see Assessing Capacity for further information).
KEY ACTIONS/POINTS FOR NON-ACUTE/
RESIDENTIAL AND COMMUNITY
■ In this setting, the consumer who has disclosed the
sexual assault should be supported to see their local
GP, Sexual Assault Service or other support group if
they choose to do so.
■ If the consumer is not in urgent need of medical
treatment, but is assessed as at risk of significant
harm to themselves (i.e. due to suicide or dangerous
self-neglect) they may require involuntary admission
to hospital under the Mental Health Act.
■ In any such situation, extreme sensitivity must be
applied, with careful consideration of the importance
of minimising any risk of re-traumatisation.
Counselling for psychological injuries
KEY ACTIONS/POINTS FOR ALL SETTINGS
■ A consumer who has disclosed a sexual assault can
access specialised counselling through their local Sexual
Assault Service or may address their experiences of
sexual assault or harassment through counselling with
a range of different health providers such as mental
health staff, counsellors with the Approved Counselling
Scheme (Victims Services, Justice and Attorney-General),
and counsellors in private practice.
■ Counselling can take a variety of forms, and consumers
interested in counselling can choose between options
such as individual, group therapies, family therapy
and/or opt for formal or more informal support.
■ Staff should explore with, and support, the consumer
to access the types of counselling and social support,
if any, that the consumer thinks will be useful and
beneficial to help them to deal with their experience
of sexual assault or harassment.
■ Social support in a group setting is often valuable for
people who have experienced sexual assault or
harassment especially when they have little or no
existing social support as usually:
– it helps to decrease the isolation that someone
who has experienced a sexual assault often feels;
– it provides a supportive atmosphere;
– attendees are encouraged to share their experiences;
– it helps those who have experienced a sexual
assault to establish their own support network.
■ Staff may wish to establish a sexual assault support
group in their facility and/or contact their local Sexual
Assault Service to collaborate in establishing and
co-facilitating a group for consumers who have
experienced sexual assault.
■ Mental health services should be familiar with the full
range of formal and informal resources that are
available locally for victims/survivors of sexual assault
and harassment. It is the role of the mental health
worker to help consumers identify and choose the
most suitable option(s) for their particular requirements.

PaGe 40 NSW HealtH Sexual Safety of Mental Health Consumers Guidelines
Organising a forensic examination
KEY ACTIONS/POINTS FOR ALL SETTINGS
■ A forensic examination is a medical examination that
can only be conducted by specially trained doctors
and nurses. The purpose of the examination is to
collect any physical evidence that may be used as
evidence against the alleged perpetrator if criminal
charges are laid after a sexual assault has occurred.
■ Specially trained doctors and nurses are available at all
Sexual Assault Services to provide medical and
forensic examinations for victims of sexual assault.
■ The consumer who has disclosed the sexual assault
should be able to consent to a forensic examination
and make decisions about whether or not to proceed
with making a report to the Police (assuming the
consumer has been provided with the relevant
information).
■ However, the consumer may not have the capacity to
make informed decisions at this time and a medical or
forensic examination, although agreed to by the
consumer, may not be in the consumer’s best interest.
In such instances a medical or forensic examination, if
there are no obvious injuries, can wait until the
person is able to give consent.
■ The local Sexual Assault Service counsellor can advise
on consent issues in this context and forensic
examination timeframes.
■ If the consumer decides to undertake a forensic
examination, they can request that a person of their
choice – such as a friend or social worker – supports
them during the examination.
■ It is important to remember that accessing medical
care and undergoing a forensic examination does not
mean that the consumer has to report the assault to
Police or request further action.
KEY ACTIONS/POINTS FOR ACUTE INPATIENT
■ Where the senior clinician is satisfied that a forensic
examination can be performed as an addition to
appropriate medical treatment, the procedure is a
minor medical treatment to which a ‘person
responsible’ can provide a valid substitute consent,
provided there are no objections from the consumer.
■ If the senior clinician considers there is no medical
reason why an examination should be undertaken
and the only reason for such an examination is the
collection of forensic evidence, the procedure is not
medical treatment and the ‘person responsible’ has
no authority to consent to such an examination.
■ In such circumstances, an application should be made
to the Guardianship Tribunal for the appointment of a
Guardian who is authorised to give (or withhold)
consent to a forensic examination (see Assessing
Capacity for further information).
■ However, a sexual assault forensic examination will
never be performed on a person who is unwilling to
proceed with the examination, even if the necessary
consent is obtained.
■ Additionally, the consent for a sexual assault forensic
examination does not include consent to release the
Sexual Assault Investigation Kit (SAIK) to Police. It is
preferable, where possible, to wait until the consumer
can make their own decision about releasing the
forensic protocol and proceeding with the report to
Police.
■ A decision about whether the consumer has
recovered the capacity to make informed consent in
relation to the release of the kit will be determined by
the treating mental health practitioner and the
consumer. The process and basis of this decision will
be documented in the consumer’s file.
■ If the consumer does not recover the capacity to give
informed consent, only a guardian appointed by the
Guardianship Tribunal will have the authority to
determine whether to release the SAIK or not.
■ Due to the issue of re-traumatisation and the capacity
for consent around complex issues it is recommended
that consent not be given for the taking of
photographs for forensic or educational purposes.
KEY ACTIONS/POINTS FOR NON-ACUTE/
RESIDENTIAL AND COMMUNITY
■ Outside of the acute setting, consumers who have
disclosed a sexual assault should be encouraged and
supported to contact the local Sexual Assault Service
or the local hospital, or to provide staff with
permission to do so, regarding a forensic examination.
Assessing capacity to make informed decisions
Whether the consumer has the capacity to make
informed decisions in relation to an incident of sexual
assault or harassment, including reporting to Police, is an
important consideration. The capacity to make informed
decisions requires not only cognitive function, but also
the ability to process information in a meaningful way.

Sexual Safety of Mental Health Consumers Guidelines NSW HealtH PaGe 41
KEY ACTIONS/POINTS FOR ALL SETTINGS6
■ The treating team will need to evaluate:
– The consumer’s capacity to understand the process
of reporting an allegation to the Police, and what
it might mean for them.
– The consumer’s capacity to process and
communicate information and effectively exercise
their rights.
– The consumer’s suitability to attend for Police
interview and any likely detrimental effects on their
mental health.
– The consumer’s capacity to collaborate with an
investigation.
■ This will assist the senior clinician to form an opinion
about the consumer’s wellness, the likely impact of
Police interview on their mental state, and any other
clinical considerations.
■ However, individual values and beliefs can vary
considerably from person to person and one
individual’s decisions may not always appear rational
to others. It is important that mental health staff do
not judge a consumer as not competent to make their
own decisions simply because they do not agree with
their views or decisions.
■ Basic principles to be used in assessing a person’s
capacity include:
– Always presume a person has capacity
– Capacity is decision specific
– Don’t assume a person lacks capacity on
appearances
– Assess the person decision making ability not the
decision they make
– Respect a person’s privacy
– Substitute decision-making is a last resort
(New South Wales Attorney General’s Department
Capacity Toolkit May 2008 p. 27)
■ It should also be noted that a consumer’s capacity
may fluctuate, so decisions regarding what action to
take in response to an incident of sexual assault or
harassment should be delayed if possible until the
consumer’s capacity is restored.
■ If there are doubts about the consumer’s capacity to
make an informed decision, a formal mental health
assessment may be required.
■ While a consumer may permanently lack the capacity
to make medical decisions, they may still be able to
6 Information adapted from the Victorian Government Department of Health Promoting sexual safety, responding to sexual activity, and managing allegations of sexual assault in adult acute inpatient units
contribute meaningfully to a discussion about what
actions they wish to take in response to an incident of
sexual assault or harassment. The consumer’s
nominated primary carer, if they have one and they
are not the alleged perpetrator, can also support
them with decision making.
■ Special attention is required in the case of involuntary
consumers under the Mental Health Act 2007.
■ Involuntary status refers to the consumer’s capacity
to consent to psychiatric treatment and does not
automatically extend to a consumer’s capacity to
make decisions about non-psychiatric medical
treatment or other wellbeing or lifestyle matters.
■ Where it is determined that an involuntary consumer
does not have capacity to make an informed decision,
urgent application can be made for a Guardian to
make some decisions in the consumer’s best interests
or the consumer’s ‘person responsible’ can be
contacted.
5.1.2 When sexual assault or harassment is suspected but not disclosed
Sometimes staff may have a suspicion that sexual assault
or harassment has occurred even when there has not
been a disclosure by the consumer. While staff should be
cognisant of the signs that could indicate this, it should
be stressed that it is extremely difficult to tell, by
observation alone, if someone has been the victim/
survivor of sexual assault or harassment.
If a staff member suspects that a consumer has been
sexually assaulted or harassed, it is important to ask the
consumer directly (refer to Section 4).
Indication of possible recent sexual assault
Psycho-social
Psycho-social behavioural responses may occur
immediately or within a few weeks of the sexual assault
and may vary in their intensity, receding and intensifying
at different times. Any individual might experience some,
all or none of these responses and these will be expressed
differently from one person to another. These responses
could include:
■ Significant changes in the consumer’s usual behaviour
or affective state
■ Acute stress response
■ Avoidance of specific settings or individuals
■ Withdrawal
■ Sleep disturbances
■ Changes to eating habits (e.g. refusing to eat)
PaGe 42 NSW HealtH Sexual Safety of Mental Health Consumers Guidelines
■ Regression
■ Excessive crying
■ Non-compliance or over-compliance
Physical
The incidence of physical injury related to sexual assault is
low and the extent does not equate with the extent of
psychological trauma. However, physical signs that may
indicate a recent sexual assault include:
■ Bruises, bleeding or other signs of physical trauma
■ Foreign objects in genital, rectal or urethral openings
■ Genital, urethral, or anal discomfort (e.g. itching,
inflammation, infection)
■ Sexually transmitted infection
■ Torn or missing clothing
■ Pregnancy
■ Semen stains on clothing, particularly on women’s
clothing
Indication of possible prior sexual assault
For some people, their psycho-social reactions persist or
worsen over time, or may appear some time after the
assault or abuse has occurred. Some reactions that could
indicate prior sexual assault include:
■ Depression
■ Flattened or hyper-aroused affect
■ Flashbacks and/or nightmares
■ Response to ‘triggers’ (i.e. any sensory stimulus that
evokes a fear response related to a sexual assault)
■ Substance misuse
■ Atypical attachment
■ Poor self-esteem, including body image issues
■ Eating disorders
■ Fear of a medical or dental examination
■ Self-harming behaviour e.g. cutting, burning, head-
banging, severe scratching
■ Suicidality
■ Sexually inappropriate behaviour
■ Somatic health responses e.g. gynaecological
problems, gastro-intestinal problems
Consumers who were sexually abused as children, or in
other settings, may be retraumatised when they enter a
new facility, or by events at a facility. Mental health staff
should note the following ‘triggers’ that may suggest
earlier sexual abuse, and may cause retraumatisation:
■ Being out of control in a situation
■ Derogatory or insensitive comments about people
who have experienced a sexual assault
■ Television and movie violence
■ Seeing someone who looks like assailant
■ People touching or standing close without permission
■ Being hugged or touched by any adult
■ Being in a vulnerable position or situation
■ Sexual advances
■ Reading or hearing about other sexual assaults
■ Feeling that people are staring
■ Action, smell, sound, that reminds the consumer of
the assailant or the place where assaulted
Reasons for non-disclosure
Consumers may not disclose sexual assault or sexual
violence for a number of reasons, including:
■ Fear of disbelief, or blame
■ Past negative experience of disclosure
■ Impact on family and significant others
The relationship between the consumer who has
experienced a sexual assault and the perpetrator can also
influence disclosure as the consumer may have a sense of
responsibility to protect the perpetrator.
KEY ACTIONS/POINTS FOR ALL SETTINGS
■ If a staff member suspects that a consumer has been
sexually assaulted they should gently ask the person
and offer help.
■ However, in some cases, the consumer may not wish
to confirm they have been sexually assaulted, even if
the staff member has reasonable evidence to suggest
that such an event has occurred.
■ The staff member should discuss what they have
observed with the consumer and explain why they
continue to be concerned about the consumer’s
health and safety. The consumer should also be
advised that they have the right not to discuss the
issue at the present time but that the staff member
would be available at a future time should the
consumer wish to speak with them.

Sexual Safety of Mental Health Consumers Guidelines NSW HealtH PaGe 43
■ Educative information about sexual assault and
harassment should be offered along with advice
about the role of the local Sexual Assault Service and
how to contact them.
■ Support to contact the local Sexual Assault Service or
another specialist support organisation should also be
offered.
■ Even if the consumer does not confirm that a sexual
assault has taken place, the suspicion of sexual assault
should be reported internally via the available
mechanisms (see Reporting and recording
requirements – page 66).
KEY ACTIONS/POINTS FOR ACUTE INPATIENT
■ In an inpatient setting, the senior clinician has a duty
of care to consider and act in the consumer’s best
interests. Staff should refer to the information within
Assessing capacity to decide whether a consumer is
able to make informed decisions about their options
regarding a sexual assault.
■ Where an involuntary consumer has been assessed by
the senior clinician and the consumer does not have
the capacity to make informed decisions in relation to
a disclosure of sexual assault, the senior clinician has a
duty of care to report the allegation to Police.
■ Where an involuntary consumer has been assessed
and does have capacity, their wishes must be
respected, unless legislatively prohibited e.g. when
the alleged perpetrator is a member of staff.
KEY ACTIONS/POINTS FOR NON-ACUTE/
RESIDENTIAL AND COMMUNITY
■ Outside of the acute setting, the consumer’s wishes
must be respected. The senior clinician should however
take the necessary steps to protect the consumer’s
interests should they change their mind over time.
■ This may involve the senior clinician ensuring the
incident is well documented and any objective
evidence is collected and preserved should the person
wish to proceed at a later date. The consumer should
be fully informed about the actions that will be taken
and the reasons behind them.
■ Follow-up care should also be provided including
ongoing counselling about the event to understand
their wish not to report, and help them exercise their
rights, which may still include a choice not to proceed
with any further action.
5.2 Consensual sexual activity in an inappropriate context or setting
5.2.1 Understanding consent and capacity
When sexual activity occurs, in all cases it must be easily
recognised as consensual, voluntary and mutual in nature
and the persons involved must have given informed
consent.
Consent exists only when a person freely and voluntarily
agrees to engage in sexual intercourse and can only be
said to be valid if the person knows what they are
consenting to, and has a real option of saying yes or no.
Additionally, most jurisdictions in Australia recognise that
there is no consent where the person who has agreed or
submitted to the sexual act does not have the capacity to
understand the sexual nature of the act.
Other factors which might make a person’s consent to
sex invalid include:
■ If a person does not really understand what is being
asked
■ If a person does not know they have the right to
refuse sex
■ If a person does not know how to refuse sex
■ If a person is afraid to refuse sex
■ If a person does not know that sex is not meant to be
painful or uncomfortable
■ If a person does not know that he or she is being
exploited when a reward/incentive or payment for sex
is used
■ If a person does not know that some relationships are
illegal, such as those within families, or between
health staff and consumers.
It is important, therefore, for mental health staff to have
an understanding of the capacity of the consumers under
their care to consent to sexual activity. When this capacity
is in doubt, an assessment should be undertaken of the
consumer’s clinical mental health status, communication
skills and current level of knowledge and understanding
regarding sexual and personal relationships.
Specific questions to be considered within such an
assessment include:

PaGe 44 NSW HealtH Sexual Safety of Mental Health Consumers Guidelines
■ Is the consumer aware of the relationship?
Is the consumer aware of who is initiating the sexual
contact? Does the consumer believe that the other
person is a spouse, or do they know the other
person’s identity and intent? Can the consumer state
what level of sexual intimacy with which they would
be comfortable?
■ What is the consumer’s ability to avoid
exploitation? Is the behaviour consistent with
formerly held beliefs or values? Moreover, does the
consumer have the capacity to say no to uninvited
sexual contact?
■ What is the consumer’s understanding of the
parameters and impact of the relationship? If the
consumer realised that the relationship may be time
limited, can they describe how they will act if the
relationship ends?
Further information regarding what the law in NSW says
about consent is provided at Appendix C – Crimes Act
2000.
5.2.2 Staff attitudesThere are situations where consumers may be engaging
in activities which other people view as morally wrong or
not in the best interests of the individual.
Mental health staff are not expected to judge the
rightness of any sexual activity that has taken place.
However, they are expected to be sensitive to the
possibility of assault and abuse, and to raise any concerns
with their line manager or the senior clinician if they
believe a consumer’s behaviour is putting them at risk.
KEY ACTIONS/POINTS FOR ALL SETTINGS
■ It can be difficult for staff to decide whether sexual
activity involving a consumer is consensual or should
be recognised as an assault. An assessment that is
specifically about the consumer’s abilities to
understand sexual and personal relationships, and
therefore provide informed consent, will support staff
in this regard. This assessment must be recorded in
the consumer’s collaborative care plan and reviewed
on a regular basis.
■ When assessing whether consent has been provided,
evidence of mutuality should also be considered to
rule out coercion. Factors to consider could include:
– both parties seeking each other out
– spending spare time together
– shared resources
– shared leisure activities
– restriction of activities with other potential
partners
■ If the sexual activity is deemed to be assault or
harassment, the guidelines for responding to sexual
assault or harassment will need to be followed.
■ Even where the sexual activity is deemed consensual,
staff should be cognisant of the need to provide
counselling or other additional care or treatment, for
either the participants or those who have witnessed
the activity, to avoid retraumatisation for those who
have experienced prior sexual assault or harassment.
■ Staff will also need to ensure that the sexual safety
standards for the service are reiterated to the
consumer and their families and carers as well as the
requirement to adhere to these.
KEY ACTIONS/POINTS FOR ACUTE INPATIENT
■ In this setting, care should be taken to ensure that the
consumer or consumers involved understand that
sexual activity is not supported due to the
vulnerability of those in care.
KEY ACTIONS/POINTS FOR NON-ACUTE/
RESIDENTIAL AND COMMUNITY
■ Consumers in non-acute/residential and community
settings have the same rights as the rest of the
community to engage in sexual activity so long as
both parties consent, demonstrate capacity to make
decisions and any activity takes place privately.
■ In a non-acute/residential setting, where one or both
individuals lack the capacity to consent, mental health
staff should work with these individuals to explore
solutions. Where a sexual relationship is established,
staff should monitor the general wellbeing of the
consumers involved and attempt to obtain an
understanding of how this relationship may be
impacting upon their wellbeing.
5.3 Sexually disinhibited behaviour
When a consumer exhibits sexually disinhibited behaviour,
it can be confronting and embarrassing for those who
witness the behaviour, or for those to whom the
behaviour may be directed. Reassurance should be
provided to both the consumer who is exhibiting the
behaviour as well as to the person or persons who may
have been offended by this behaviour.

Sexual Safety of Mental Health Consumers Guidelines NSW HealtH PaGe 45
Sexual disinhibition can also impact on the consumer’s
existing intimate relationships, their self-esteem and their
reputation – the consumer may take actions that they would
not ordinarily take while in a well state, such as engaging
or offering to engage in sexual activity with someone.
Staff should try not to overreact to the behaviour – a
gentle and patient approach should be adopted,
particularly where the consumer has dementia, as they
will often be anxious and need additional reassurance.
If there is any real threat to the safety of other consumers
or staff from the consumer exhibiting the behaviour, the
emphasis must be on protecting others.
KEY ACTIONS/POINTS FOR ALL SETTINGS
■ When sexually disinhibited behaviour occurs, it is
important to give clear, simple and unambiguous
feedback. Staff cannot assume that a consumer will
recognise hints that their behaviour is not appreciated.
■ Staff should take the consumer who has exhibited the
behaviour aside and gently yet firmly provide this
feedback, which may need to include matter-of-fact
advice regarding unspoken rules about appropriate
social behaviour.
■ The consumer’s understanding of what has been said
should be checked by asking them to repeat the
information. Staff should use this approach with care
and sensitivity to avoid being interpreted as patronising.
■ If the consumer does not already have a plan in place
to manage their disinhibited behaviour, this will need
to be developed (see section 4.3 and Appendix L for
further information). After an incident of sexual
disinhibition, any existing management plan for the
consumer/s involved should be reviewed and updated
to take account of the need for further actions or
strategies.
■ Staff will also need to ensure this updated plan is
agreed with and communicated to all mental health
staff involved in the consumer’s care as well as to the
consumer’s family and carer so that the consumer is
receiving a consistent message about their behaviour.
■ Where a consumer has engaged in sexual activity
with someone other than their regular partner as a
part of their sexual disinhibition, they may require
counselling along with their family, carer or friends.
They may also require sexual health advice or treatment.
■ If a consumer has sexually assaulted another
consumer, or been assaulted themselves, as a result
of their sexual disinhibition, the protocols for
responding to this type of sexual safety incident
should be followed.

PaGe 46 NSW HealtH Sexual Safety of Mental Health Consumers Guidelines
KEY POINTS – RESPONDING TO A SEXUAL SAFETY INCIDENT
Sexual assault and harassment
When there is disclosure or acknowledgement of sexual assault or harassment
■ Key actions to take when a disclosure of sexual
assault is made:
– Acknowledge and affirm the disclosure
– Explore the disclosure
– Establish and maintain safety
– Secure any evidence
– Offer support and options
– Assess capacity to make informed decisions
– Organise medical care
■ See Section 5.1 for further information, as well as
Appendix I and J.
■ In relation to reporting to the NSW Police Force,
contacting the local Sexual Assault Service or
informing the consumer’s family or carer, the wishes
of the consumer who has disclosed the sexual assault
must be respected at all times, except where:
– the alleged perpetrator is a NSW Health staff
member; or
– the consumer does not have the capacity to make
an informed decision.
■ The Child Protection helpline must be notified when
there is risk of significant harm to a child or group of
children.
■ Relevant line managers must be informed of
allegations involving NSW Health staff members.
When sexual assault or harassment is suspected but not disclosed
■ Staff should be cognisant of the signs that could
indicate that sexual assault or harassment has
occurred. See Section 5.1.2 for further information.
■ If a mental health worker suspects that a consumer
has been sexually assaulted or harassed, it is
important to ask the consumer directly. See Section 4
for further information.
Consensual sexual activity in an inappropriate context or setting
Understanding consent
■ When sexual activity occurs, in all cases it must be
easily recognised as consensual, voluntary and mutual
in nature and the persons involved must have given
informed consent.
■ Further information regarding what the law says
about consent is provided at Appendix C.
Staff attitudes
■ Mental health staff are not expected to judge the
rightness of any sexual activity that has taken place.
However, they are expected to be sensitive to the
possibility of assault and harassment.
■ An assessment that is specifically about the
consumer’s abilities to understand sexual and
personal relationships will support staff in this regard.
See 5.2.2 for further information.
Sexually disinhibited behaviour
■ When a consumer exhibits sexually disinhibited
behaviour, staff should provide clear and
unambiguous feedback about the inappropriateness
of the consumer’s actions in a gentle yet firm manner.
■ A management plan will need to be developed to
manage any further behaviour of this nature, which
should be communicated to all staff as well as the
consumer’s family and carer – see section 4.3 and
Appendix L for further information.
■ If a consumer has sexually assaulted another
consumer, or been assaulted themselves, as a result of
their sexual disinhibition, the protocols for responding
to this type of sexual safety incident should be
followed.
PaGe 46 NSW HealtH Sexual Safety of Mental Health Consumers Guidelines
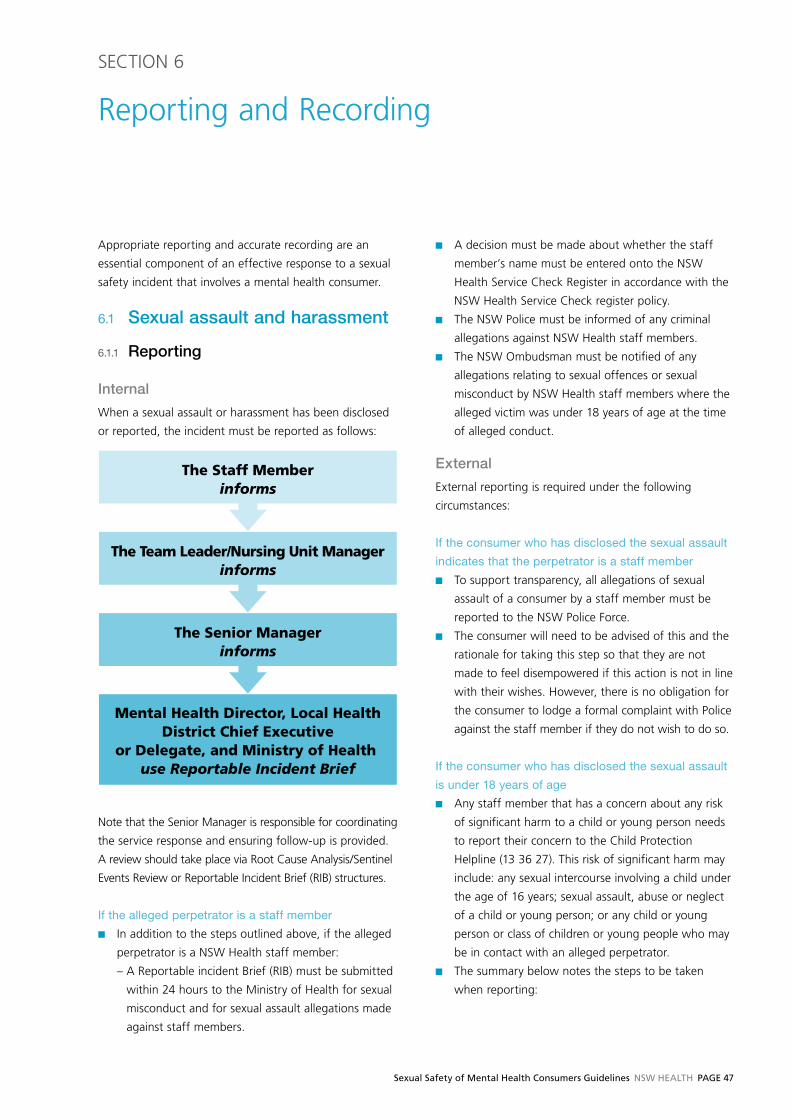
Sexual Safety of Mental Health Consumers Guidelines NSW HealtH PaGe 47
SECTION 6
Reporting and Recording
Appropriate reporting and accurate recording are an
essential component of an effective response to a sexual
safety incident that involves a mental health consumer.
6.1 Sexual assault and harassment
6.1.1 Reporting
Internal
When a sexual assault or harassment has been disclosed
or reported, the incident must be reported as follows:
The Staff Memberinforms
The Team Leader/Nursing Unit Managerinforms
The Senior Managerinforms
Mental Health Director, Local HealthDistrict Chief Executive
or Delegate, and Ministry of Health use Reportable Incident Brief
Note that the Senior Manager is responsible for coordinating
the service response and ensuring follow-up is provided.
A review should take place via Root Cause Analysis/Sentinel
Events Review or Reportable Incident Brief (RIB) structures.
If the alleged perpetrator is a staff member
■ In addition to the steps outlined above, if the alleged
perpetrator is a NSW Health staff member:
– A Reportable incident Brief (RIB) must be submitted
within 24 hours to the Ministry of Health for sexual
misconduct and for sexual assault allegations made
against staff members.
■ A decision must be made about whether the staff
member’s name must be entered onto the NSW
Health Service Check Register in accordance with the
NSW Health Service Check register policy.
■ The NSW Police must be informed of any criminal
allegations against NSW Health staff members.
■ The NSW Ombudsman must be notified of any
allegations relating to sexual offences or sexual
misconduct by NSW Health staff members where the
alleged victim was under 18 years of age at the time
of alleged conduct.
External
External reporting is required under the following
circumstances:
If the consumer who has disclosed the sexual assault
indicates that the perpetrator is a staff member
■ To support transparency, all allegations of sexual
assault of a consumer by a staff member must be
reported to the NSW Police Force.
■ The consumer will need to be advised of this and the
rationale for taking this step so that they are not
made to feel disempowered if this action is not in line
with their wishes. However, there is no obligation for
the consumer to lodge a formal complaint with Police
against the staff member if they do not wish to do so.
If the consumer who has disclosed the sexual assault
is under 18 years of age
■ Any staff member that has a concern about any risk
of significant harm to a child or young person needs
to report their concern to the Child Protection
Helpline (13 36 27). This risk of significant harm may
include: any sexual intercourse involving a child under
the age of 16 years; sexual assault, abuse or neglect
of a child or young person; or any child or young
person or class of children or young people who may
be in contact with an alleged perpetrator.
■ The summary below notes the steps to be taken
when reporting:

PaGe 48 NSW HealtH Sexual Safety of Mental Health Consumers Guidelines
about their capacity to make an informed decision
(see Assessing capacity to make informed decisions
for further advice).
■ Information should be provided to the consumer
regarding reporting to Police to help them to decide
whether or not this is how they want to proceed, and
whether they wish to make a formal complaint or
simply notify the Police that the incident has occurred.
Appendix E provides relevant information for this
purpose. ■ In all circumstances, the wishes of the consumer in
relation to making a Police report must be respected,
unless the consumer indicates that the perpetrator is
a staff member. In this circumstance, Police must be
notified of the alleged incident to ensure transparency
regardless of whether the consumer wishes to take
this step, but a formal complaint does not have to
be made by the consumer if they do not wish to
make one.
If the consumer who has disclosed the sexual assault
requests support from the local Sexual Assault Service
■ All requests by the consumer to report the assault to
the local Sexual Assault Service should be actioned.
■ Information should be provided to the consumer
regarding how the Sexual Assault Service can help them,
including reporting to Police to help them to decide
whether or not this is how they want to proceed.
■ The local Sexual Assault Service can also provide
information regarding legal and complaint options
and help the consumer to explore these in relation
to their own needs and circumstances and to move
towards a decision that is best for them. Involvement
of or consultation with the Sexual Assault Service is
important as legislation and witness support
þComplete the Mandatory Reporter Guide (MRG) tool to help you identify if there is risk of significant harm.
You can access the MRG at http://www.keepthemsafe.nsw.gov.au/home. Hard copies of the MRG are also available
at health workplaces.
þIf you identify risk of significant harm, call the Child Protection Helpline on 13 36 27 (for mandatory reporters) or
in an emergency, call 000.
þHealth Child Wellbeing Units (CWU) provide advice to NSW Health workers on what action to take and who to
talk to about concerns for children at risk.
þContact child protection professionals at the CWU on 1300 480 420:
– if you are uncertain about what action to take
– if you need help on how to use the Mandatory Reporter Guide (MRG)
– to inform the CWU of concerns for a child or young person below the threshold for risk of significant harm
– where the Mandatory Reporter Guide advises you to do so.
■ If the report concerns a young person aged over 16
but under 18 years, the young person should be
involved in the decision to report to the Child
Protection Helpline and the process of reporting,
unless there are exceptional reasons for excluding
them. Staff should note that a young person may
perceive sexual activity as consensual because of the
way the other person involved has promoted it, even
though the situation may be one of sexual abuse and
exploitation. If the young person does not agree to
the report being made, staff may still make a report
and this information must be conveyed to Community
Services, as they must consider the young person’s
wishes in any investigations and assessments.
■ All concerns that a child or young person may be at
risk of significant harm and action taken are to be
documented in the consumer’s health record.
■ For any allegations of sexual assault by a NSW Health
staff member against a person who was under 18
years of age at the time of the alleged assault (even if
they are an adult now), the NSW Police must be notified.
■ The NSW Ombudsman must also be notified of any
allegations of sexual assault or sexual misconduct
against current staff members where the alleged victim
is under 18 years of age at the time of the alleged
assault, regardless of where or when the alleged assault
is said to have occurred, and the health service must
complete an investigation in accordance with the NSW
Ombudsman’s requirements, and notify the Commission
for Children and Young People as required.
If the consumer who has disclosed the sexual assault
requests that the assault is reported to the Police
■ All requests by the consumer to report the assault to
the Police should be actioned, unless there is doubt

Sexual Safety of Mental Health Consumers Guidelines NSW HealtH PaGe 49
provisions may change; it is the role of the Sexual
Assault Service to maintain up to date knowledge.
If the consumer who has disclosed the sexual assault
requests support from the service to notify their family
or carer
■ The service can help the consumer talk to their family
or carer about the assault, if they request this.
■ However, consent is required for staff to take this
action, regardless of whether the consumer is
voluntary or involuntary, and must be clearly
documented in the consumer’s file.
■ The Sexual Assault Service can also provide counselling
to family and significant others – this may be a counsellor
separate to the counsellor who sees the consumer if
indicated. This intervention is concerned with ensuring
that family is able to appropriately respond to the
consumer and to provide trauma informed support.
6.1.2 Recording The sexual assault incident needs to be clearly and
accurately recorded in the file of the consumer who has
disclosed the sexual assault and the alleged perpetrator’s
file. Documentation should comprise actual accounts of
events using the consumer’s own words and clear
descriptions of behaviours wherever possible.
Terminology or language which can be interpreted in
different ways should not be used (e.g. terms such as
‘inappropriate’ or ‘suspicious’).
File of the consumer who has disclosed the sexual assault
The consumer’s file should record:
■ Specific details including the nature, time and location
of the allegation, any witnesses, the consumer’s account.
■ The consumer’s clinical state including mental status,
the effects of the assault, and any coping strategies
used.
■ That the consumer has been provided with
information regarding their rights, action which may
be taken and support available.
■ Any management strategies implemented and their
outcome (i.e. helpful or not).
■ To whom the incident has been reported, the actions
taken thus far and the wishes of the consumer in
relation to reporting the incident to external agencies,
such as Police or the local Sexual Assault Service.
■ The Incident Information Management System (IIMS)
notification number.
■ A review of the consumer’s current status using the
MH-OAT Standard Measure 1B (SM1B) needs to be
completed. (MH-OAT protocols require the
completion of a SM1B in response to a critical
incident.)
■ Where the allegation relates to a NSW Health staff
member, the consumer’s file should not contain all
the details but should provide a reference to the
location of the information.
Subpoenaed Files
■ Medical records staff need to be provided with clear
information about the information to be provided if a
consumer’s file is subpoenaed for legal proceedings in
response to a sexual assault investigation. In particular,
Sexual Assault Communications Privilege must be
considered. (People who have experienced a sexual
assault have certain protection against discussions
with counsellors being obtained under subpoena by
Defendants in criminal proceedings. The aim is to
protect the confidentiality of sexual assault counselling,
so as to encourage people who have experienced
sexual assault to seek counselling, and to make them
feel more confident about actually reporting sexual
assaults – see Subpoenas PD2010_065)
■ Further, if the consumer’s file is subpoenaed for some
other reason, it should be noted that the consumer’s
file contains information of a sensitive nature that must
not be provided except where the legal proceedings
are relevant to the specific sexual assault and Sexual
Assault Communications Privilege does not apply.
■ Under Section 29 of the Children and Young Persons
(Care and Protection) Act 1998 the protection of the
reporter’s identity must be considered by services
when executing exchange of information requests,
providing a response to court subpoena or responding
to requests for public access to government information.
■ Section 29 protects the identity of people who report
concerns about children and young people to the
Child Protection Helpline or to a Child Wellbeing Unit
which sends the report on to the Child Protection
Helpline. It also protects the identity of persons
concerned in making the report or causing the report to
be made. It is prohibited under this section to disclose
the reporter’s identity as well as any information from
which the reporter’s identity might be deduced.

PaGe 50 NSW HealtH Sexual Safety of Mental Health Consumers Guidelines
■ A local protocol for Medical Records staff must be
developed to ensure there is a clear process for
identifying issues associated with the use of medical
files as evidence in legal proceedings.
File of the person who has been identified as the perpetrator of the sexual assault
Where the alleged perpetrator is a consumer, the
following information is to be recorded in their file:
■ Specific details including the time and location of the
incident and any witnesses.
■ Whether the alleged perpetrator has been informed
of the allegation of sexual assault. (The alleged
perpetrator should not be informed of the allegation
immediately where this may compromise the
investigation or the safety of the consumer who has
experienced the sexual assault.)
■ That the alleged perpetrator has been provided
information regarding their legal rights including
access to legal services.
■ To whom the incident has been reported and actions
taken thus far. This includes any medical response,
who has been notified, Police involvement and what
consent has been given.
■ IIMS notification number.
Where the alleged perpetrator is a staff member, the
following information is to be recorded by the Senior
Manager and kept separately from the staff member’s
HR file:
■ Specific details including the nature, time and location
of the alleged incident and any witnesses, and when
and how reported.
■ Details of any action taken in response to the
allegation, such as counselling to any of the parties,
notifications to external bodies such as he NSW
Police, Child Protection Helpline etc.
■ Any advice or information from NSW Police or
Community Services, including advice that the NSW
Health investigation may commence.
■ Details of any investigation, including any
investigation plan, details of interviews with relevant
parties, details of any risk assessments and related risk
management decision, including decisions around the
NSW Health Service Check Register.
■ The investigation report and all other documentation
created in relation to the investigation.
■ Any submissions from the staff member.
■ Signed and dated File Notes must be kept of each
telephone conversation, interview, notification sent
and advice received during an internal investigation
■ All e-mail correspondence.
■ IIMS notification number.
6.2 Consensual sexual activity in an inappropriate context or setting
6.2.1 Reporting Internal
When consensual sexual activity in an inappropriate
context or setting has been disclosed or reported, the
incident must be reported as follows:
The Staff Memberinforms
The Team Leader/Nursing Unit Manager
External
External reporting of this type of sexual safety incident is
not required.
6.2.2 RecordingIf the consumers involved in this type of sexual safety
incident are both in an inpatient or residential setting,
files for both consumers must have the incident
documented in their files. Any action taken must be
documented as well, including any increase in levels of
observation, assessment of the consensual, voluntary and
mutual nature of the sexual activity, counselling or
education for consumer/s involved or debriefing with
consumers who may have witnessed the incident.
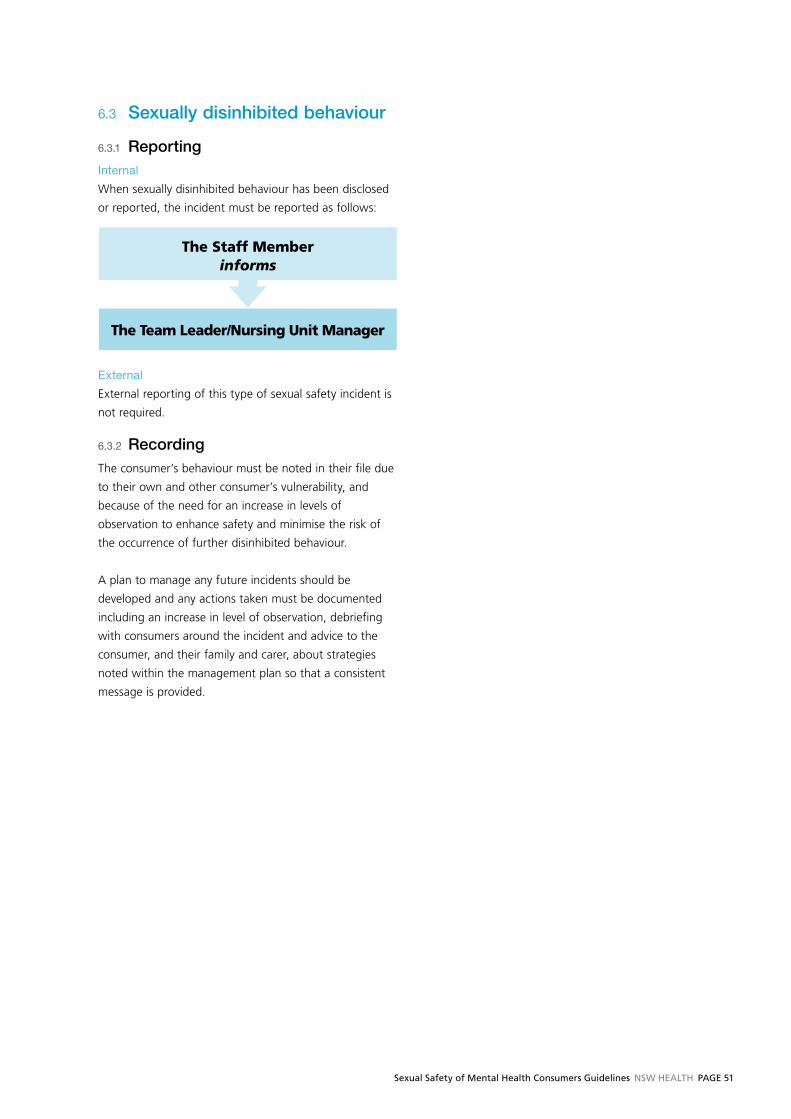
Sexual Safety of Mental Health Consumers Guidelines NSW HealtH PaGe 51
6.3 Sexually disinhibited behaviour
6.3.1 Reporting Internal
When sexually disinhibited behaviour has been disclosed
or reported, the incident must be reported as follows:
The Staff Memberinforms
The Team Leader/Nursing Unit Manager
External
External reporting of this type of sexual safety incident is
not required.
6.3.2 RecordingThe consumer’s behaviour must be noted in their file due
to their own and other consumer’s vulnerability, and
because of the need for an increase in levels of
observation to enhance safety and minimise the risk of
the occurrence of further disinhibited behaviour.
A plan to manage any future incidents should be
developed and any actions taken must be documented
including an increase in level of observation, debriefing
with consumers around the incident and advice to the
consumer, and their family and carer, about strategies
noted within the management plan so that a consistent
message is provided.
PaGe 52 NSW HealtH Sexual Safety of Mental Health Consumers Guidelines
7.1 Consumers who are Aboriginal and Torres Strait Islander
The prevalence of trauma such as sexual assault within
the Aboriginal and Torres Strait Islander communities
across Australia is relatively high. Yet non-Aboriginal staff
often feel challenged and uncertain about the most
culturally respectful and competent approach to
effectively supporting Aboriginal consumers who have
experienced sexual assault and violence.
Although it relates specifically to family violence in
Aboriginal communities, the Aboriginal Family Health
Strategy (http://www.health.nsw.gov.au/pubs/2011/
aboriginal_family_health_.html )provides an example of
the approach and specific considerations that would
enhance service provision to Aboriginal consumers in
relation to sexual safety. In particular, the Principles of
Aboriginal Health, the Model of Care and the healing
approach promoted by the Strategy, should be considered
where appropriate.
One of the key tactics highlighted within the Strategy is
the provision of clear, effective and culturally appropriate
information for Aboriginal people. Mental health staff
should consider sourcing culturally appropriate and
sensitive material that supports advice to the consumer
and family about responding to sexual assault and
violence. Alternatively, services may wish to develop their
own resources for the specific Aboriginal communities in
their locality. The following NSW Health resources may
provide advice and support in relation to this.
Communicating Positively
http://www.health.nsw.gov.au/pubs/2004/aboriginal_
terms.html
Working with Aboriginal Communities
http://www.community.nsw.gov.au/docswr/_assets/
main/documents/working_with_aboriginal.pdf
Relevant training for mental health staff will also be
critical to enhancing cultural competence in responding
to sexual safety incidents involving Aboriginal mental
health consumers. The Education Centre Against Violence
(ECAV) provides a number of relevant courses including:
Defining healthy boundaries when working in
Aboriginal communities
(http://www.ecav.health.nsw.gov.au/ecav/index.
asp?pg=2&s=C&cNo=175)
This training is for Aboriginal staff who engage in
supportive and healing relationships with Aboriginal
clients and communities that have experienced family
violence, child abuse, adult or child sexual assault.
NSW Health specialist Sexual Assault Services training
http://www.ecav.health.nsw.gov.au/ecav/index.
asp?pg=2&s=C&cNo=200
Defines culturally competent responses to diverse
population groups including Aboriginal or Torres
Strait Island people and people of Culturally and
Linguistically Diverse backgrounds.
Where possible, appropriately qualified Aboriginal
Workers or Aboriginal Liaison Officers (within agencies
e.g. hospitals, Police) should be engaged to work with
consumers around appropriately preventing and
responding to sexual safety incidents.
It is also vital that the Aboriginal status of clients is
recorded accurately and consistently in order to develop
and improve, monitor and evaluate services providing
care and protection for Aboriginal children and families.
In general, Aboriginal status is poorly recorded in health
related data and consequently the utilisation of services
by Aboriginal clients is under represented. This in turn
contributes to insufficient culturally appropriate and
accessible service provision. See principles for recording
Aboriginal and Torres Strait Islander origin information of
consumers and clients
http://www.health.nsw.gov.au/policies/
pd/2012PD2012_042.html.
SECTION 7
Highly vulnerable groups

Sexual Safety of Mental Health Consumers Guidelines NSW HealtH PaGe 53
7.2 Consumers who are children or young people
The Children and Young Persons (Care and Protection)
Act 1998 defines a child as ‘a person under the age of
under 16 years’ and a young person as ‘a person who is
aged 16 years or above but who is under the age of 18
years’ (i.e. a person who is 16 or 17 years old). In addition,
the minimum age of consent for sexual activity in NSW is
16 years old. The NSW Ombudsman defines children as
being under the age of 18 years of age when dealing
with allegations of sexual assault by staff members.
While children and young people may be vulnerable to
sexual assault, they may also pose risks to other consumers,
especially when exploring their sexuality and experimenting
with sexual behaviour. Children and young people can
display a continuum of sexual behaviour, where at one
end they display healthy, age-appropriate sexual
behaviour and at the other may in some circumstances
engage in behaviours that are problematic or abusive.
Accordingly, mental health staff should not assume that
an age-specific service is automatically safe. Appropriate
risk assessment and mitigation will need to be
undertaken in all service settings that cater to the needs
of children and young people, including inpatient,
rehabilitation and community-based services.
Communication is also a key factor in the sexual safety of
consumers who are children and young people. Children
and young people may be reluctant to communicate their
experiences verbally, meaning mental health staff will need
to adopt communication styles that allow the child or
young person to feel safe to communicate in their own way.
Education about contraception and other aspects of
sexual health and safety may support young consumers
to better communicate about any sexual safety issue, and
consideration of the educative needs of this group should
be a routine part of comprehensive individually-tailored
care planning and service delivery.
Family and carers, who play an integral role in the
provision of care for this age group, can support children
and young people to understand the sexual safety
standards in place for the service and to speak up about
any incidents of sexual assault or harassment they are
subjected to or witness. However, staff must be cognisant
that the involvement of families and carers is subject to
child protection requirements where these are an issue.
Mental health staff must also be aware that if they
suspect, on reasonable grounds, that a child or young
person is at ‘risk of significant harm’ from abuse or
neglect, they must report these concerns to the
Community Services’ Child Protection Helpline. NSW
Ministry of Health Information Bulletin Keep Them Safe –
Making a Child Protection Report IB2010_005 (http://
www.health.nsw.gov.au/policies/ib/2010/IB2010_005.
html ) defines ‘significant harm’ as follows:
What is meant by ‘significant’ is that which is
sufficiently serious to warrant a response by a
statutory authority irrespective of a family’s consent.
What is significant is not minor or trivial and may
reasonably be expected to produce a substantial and
demonstrably adverse impact on the child or young
person’s safety, welfare or wellbeing.
Keep Them Safe – Making a Child Protection Report
IB2010_005 (http://www.health.nsw.gov.au/policies/
ib/2010/IB2010_005.html) outlines the legislative
requirements of NSW Health staff in protecting and
supporting the safety, welfare and wellbeing of children
and young people and reinforces the principle that care
and protection of children and young people is a shared
responsibility.
The NSW Mandatory Reporter Guide (MRG) assists NSW
Health staff in deciding whether concerns for the safety,
welfare and wellbeing of children and young people meet
the risk of significant harm threshold (NSW Mandatory
Reporter Guide - http://sdm.community.nsw.gov.au/mrg/
app/summary.page).
NSW Health Child Wellbeing Units (CWU) provide advice
to NSW Health staff on what action to take and who to
talk to about concerns for children at risk.
Mental health staff should contact child protection
professionals at the CWU on 1300 480 420:
■ if they are uncertain about what action to take
■ if they need help on how to use the Mandatory
Reporter Guide (MRG)

PaGe 54 NSW HealtH Sexual Safety of Mental Health Consumers Guidelines
■ to inform the CWU of concerns for a child or young
person below the threshold for risk of significant
harm
■ where the Mandatory Reporter Guide advises to do so.
Mental health staff should also familiarise themselves
with the following contact information:
■ Community Services’ Child Protection Helpline for
mandatory reporters – 13 36 27
■ NSW Health Child Wellbeing Units – 1300 480 420
■ NSW Health Keep Them Safe Website
http://www.health.nsw.gov.au/initiatives/kts/index.asp
■ Department of Premier and Cabinet Keep Them Safe
Website
http://www.keepthemsafe.nsw.gov.au/home
■ NSW Ombudsman Child Protection in the workplace –
responding to allegations against employees –
http://www.ombo.nsw.gov.au/news-and-publications/
publications/guidelines/child-protection
7.3 Consumers from a culturally and linguistically diverse background
Mental health consumers from culturally and linguistically
diverse (CALD) backgrounds who are sexually assaulted or
harassed can face multiple layers of disadvantage due to
a range of factors such as racism, the fear of bringing ‘shame’
to their family, and disconnection from their community.
Being able to effectively communicate about sexual safety
issues is the first step in ensuring that the special needs
of CALD consumers are taken into account. The NSW
Health Care Interpreter Service can assist persons from
CALD backgrounds who present with communication
difficulties – refer to NSW Ministry of Health Policy
Directive Standard Procedures for Working with Health
Care Interpreters PD2006_053. (http://www.health.nsw.
gov.au/policies/pd/2006/PD2006_053.html)
Should the NSW Heath Care Interpreter Service not be
able to assist in the provision of a language resource, the
Translating & Interpreting Service (http://www.immi.gov.
au/living-in-australia/help-with-english/help_with_
translating/ ) may be called upon for assistance.
While the Transcultural Mental Health Centre is not an
interpreting service, they may be engaged when specialist
cross cultural assessment or consultation is required.
The Centre also provides limited clinical care and
management and these services can be accessed through
Local Health Districts.
Family members, carers and friends may volunteer to
assist with interpreting during the reporting of an
incident, and this is acceptable at the first point of
contact and may be beneficial in establishing any
immediate concerns.
However family and friends of the consumer who has
experienced an assault are inappropriate substitutes for a
professional interpreter in the long term and their interests
may actually be different from or in conflict with those of
the consumer. Accordingly, an interpreter service should
be engaged as soon as practicable, and this advice should
be provided to the consumer’s family.
Culturally and linguistically appropriate information
regarding sexual violence and victims’ rights and services
are also critical. Services will need to consider the literacy
level of the consumer though and be prepared to explain
the written information in a clear and concise way,
highlighting relevant contact details and what support
can be accessed.
Documents that may provide further support for mental
health staff include:
■ Multicultural Mental Health Plan 2008-2012 –
PD2008_067 (http://www.health.nsw.gov.au/policies/
pd/2008/pdf/PD2008_067.pdf)
■ NSW Refugee Health Plan 2011-2016 – PD2011_014
(http://www.health.nsw.gov.au/policies/pd/2011/
PD2011_014.html)
7.4 Consumers with Intellectual Disability
People with intellectual disability (ID) often have key
deficits in adaptive behaviour such as social problem
solving and social judgement that can contribute to the
risk of sexual abuse or assault. When a person with ID
also has a mental illness or disorder, this risk can be
substantially increased. Social dislocation, fragmented
care and lack of education about sexuality and sexually
appropriate behaviour may also contribute to this
vulnerability.
Basic sex education, tailored to individually suit the

Sexual Safety of Mental Health Consumers Guidelines NSW HealtH PaGe 55
communication and comprehension level of the consumer
with ID, can help to combat this vulnerability by providing
the consumer with the knowledge to understand the
difference between normal sexual activity and sexual
assault. Armed with this knowledge, consumers with ID
can more effectively identify when they are being
victimised and develop self-protective behaviours.
Consumers with ID will also benefit from being provided
with clear advice about their rights in relation to sexual
safety, such as their right to say ‘no’ to sexual activity.
As people with ID can lack the confidence to assert their
rights even when they are aware of them, education will
also be required to help consumers with ID learn how to
ensure these rights are upheld. This in turn will support
them to speak up should they experience a sexual safety
incident.
While many adults with mild ID engage in fulfilling
consensual sexual relationships, some people with ID will
lack the capacity to make decisions in relation to this area
of their life.
Consumers with ID will benefit from an assessment of
their communication skills and current level of knowledge
and understanding regarding sexual and personal
relationships – see Section 5.2.1 Understanding consent
and capacity – to ensure they have the capacity to consent
to sexual activity. Further information regarding what the
law in NSW says about consent is provided at Appendix C.
The capacity of consumers with ID to make decisions if
they have been assaulted will also need to be considered
– further information regarding this is provided under the
heading Assessing capacity to make informed decisions,
page 41.
7.5 Gay, Bisexual, Lesbian and Transgender Consumers
The underlying issue in managing sexual safety for Gay,
Bisexual, Lesbian and Transgender (GLBT) mental health
consumers is the impact of real or perceived homophobia
and transphobia.
Homophobia is a term used to describe a range of
negative attitudes and feelings towards homosexuality
and people who are identified or perceived as being gay,
lesbian or bisexual.
Homophobia can occur in obvious and subtle ways and
can include:
■ Cultural stereotypes about acceptable forms of
conduct around GLB people that degrades their
sexual orientation;
■ Condoning homophobia by not addressing
inappropriate language/behaviour by others;
■ Discounting the severity and impact of a sexual
assault/harassment incident between people of the
same-sex, where a GLB person is involved, due to a
misconception that the behaviour is less traumatic
because of the gender of the perpetrator.
The impact of homophobic behaviours on GLB individuals
can be devastating, reducing their sense of personal
safety or increasing vulnerability to sexual incidents. For
GLB people who have experienced unwanted sexual
behaviours, fear or perceptions of homophobia may
affect their willingness to disclose the incident, due to
fears of receiving a lesser standard of support.
Transphobia refers to discrimination against transsexuality
and transsexual or transgender people because they do
not conform to or who transgress societal gender
expectations and norms.
While many of the ways in which homophobia manifests
itself can also impact on transgender consumers, there
are additional issues to consider in relation to the sexual
safety of this group, such as:
■ The assumption that gender identity is a disorder and
the individual’s presenting issue.
■ A misconception that gender identity and sexual
orientation are the same. Gender identity and sexual
orientation are two distinct issues. Transgender
people can be heterosexual, gay, lesbian or bisexual.
■ An inability to accept a transgender person’s chosen
gender. This can impact on transgender women’s
access to single sex spaces, thus increasing
vulnerability; and increase the vulnerability of
transgender men in male single sex settings.
Creating a culture of acceptance that normalises diverse
sexual orientations and gender identities will assist in
promoting sexual safety as well as encouraging openness
in reporting sexual safety incidents. Mental health
services can create safe and non-judgemental
environments for GLBT consumers through actively
PaGe 56 NSW HealtH Sexual Safety of Mental Health Consumers Guidelines
promoting the service’s acceptance of diverse sexual
orientations and gender identities, and having a clear
protocol or policy in place that dictates the
unacceptability of homophobic and transphobic
behaviour from either providers or consumers.
7.6 Older consumers
While the ageing process may impact on their sexual
health, older people continue to see sexual relationships
as an important aspect of their life.
However, older people are often viewed by society as
being physically unattractive, uninterested in sex and
incapable of achieving sexual arousal. Mental health staff
caring for older consumers need to challenge these
societal attitudes within their service to avoid the
inadvertent nurturing of professional responses and an
environment that could:
■ Discourage older mental health consumers from
reporting or freely discussing sexual safety incidents
■ Lead to an inappropriate categorisation and
intervention of sexual activity / expression from an
older mental health consumer; and
■ Overlook the needs of older mental health consumers
that are particularly vulnerable to sexual safety
incidences, including people that are cognitively
impaired, physically frail and/or with severe
depression.
The sexual safety of older mental health consumers can
also be impacted upon by dementia, which can be
complicated by behavioural and psychological symptoms
of dementia (BPSD). BPSD is an umbrella term for a
diverse group of non-cognitive symptoms such as
psychosis, depression, agitation, inappropriate sexual
behaviour, restlessness, intrusiveness and resistance
to care.
In aged residential care settings, it is common for older
mental health consumers with a diagnosis of BPSD, and
to a lesser extent with other diagnosis such as mania, to
be referred to Specialist Mental Health Services for Older
People (SMHSOP) when there has been a sexual safety
incident. These sexual safety incidents generally relate to
sexual activity such as masturbation in an inappropriate
setting, sexually disinhibited behaviour such as disrobing
and inappropriately touching nursing staff that are
providing care, and staff perceptions of older mental
health consumers and sexual safety.
Managing these referrals in an environment with other
older mental health consumers who are particularly
vulnerable to sexual safety requires specialised
intervention and an interagency approach.

Sexual Safety of Mental Health Consumers Guidelines NSW HealtH PaGe 57
Appendices
APPENDIX A Example Standards of Behaviour for an Acute Inpatient Mental Health Service setting and a Non-acute Inpatient or Rehabilitation Mental Health Service setting
APPENDIX B Charter of Victims Rights
APPENDIX C Relevant standards and legislation
APPENDIX D Information about support options for consumers who have experienced sexual assault
APPENDIX E Information about reporting to Police for consumers who have experienced sexual assault
APPENDIX F Example posters to promote Sexual Assault Services
APPENDIX G Sexual Assault Screening Tool
APPENDIX H Examples of sexualised behaviour by healthcare professionals towards consumers or their carers
APPENDIX I Responding to a disclosure of sexual assault – key actions
APPENDIX J Responding to a disclosure of recent sexual assault – quick checklist
APPENDIX K Follow up medical exams required when a person has been sexually assaulted
APPENDIX L Reporting process for an incident of sexual assault
APPENDIX M Information about managing Disinhibited Behaviour

PaGe 58 NSW HealtH Sexual Safety of Mental Health Consumers Guidelines
APPENDIX A
Example Sexual Safety Standards of Behaviour
Sexual Safety Standards of Behaviour for an Acute Inpatient Mental Health ServiceAll consumers involved with this mental health service are asked to adhere to the following standards of behaviour in
relation to sexual safety.
Standard 1 I respect myself.
Standard 2 I treat others with respect, dignity and courtesy.
Standard 3 I do not engage in any sexual activity with another person while on the grounds of the service.
Standard 4 I do not try to talk someone else into engaging in sexual activity, or harass another person sexually.
Standard 5 I try to be aware of how my behaviour makes others feel, and will change my behaviour if someone tells me it makes them uncomfortable, or I will ask for help with this if I need to.
Standard 6 I respect the rights of others to space and privacy to fulfil their sexual needs through masturbation.
Standard 7 I understand that fulfilling my own sexual needs through masturbation must be conducted privately and discreetly.
Standard 8 I speak up if I have been hurt, harassed or assaulted either physically or sexually.
Standard 9 I speak up if I see or hear about someone else being hurt, harassed or assaulted either physically or sexually.
Example Sexual Safety Standards of Behaviour for a Non-Acute Inpatient or Rehabilitation Mental Health ServiceAll consumers involved with this mental health service are asked to adhere to the following standards of behaviour in
relation to sexual safety.
Standard 1 I respect myself.
Standard 2 I treat others with respect, dignity and courtesy.
Standard 3 I only engage in sexual activity with another person when they have given their consent.
Standard 4 I do not try to talk someone else into engaging in sexual activity, or harass another person sexually.
Standard 5 I only engage in sexual activity with another person in the privacy of my own or the other person’s room, or a room that is provided by the service, while on the grounds of the service.
Standard 6 I understand that sexual activity with another person should be for mutual pleasure, and never used for punishment.
Standard 7 I never intentionally hurt anyone when engaging in sexual activity with them, and I understand that I must stop engaging in sexual activity when the person I am with says ‘stop’.
Standard 8 I always practice safe sex and use a condom when engaging in sexual activity with another person.
Standard 9 I try to be aware of how our behaviour makes others feel, and will change my behaviour if someone tells me it makes them uncomfortable, or I will ask for help with this if I need to.
Standard 10 I respect the rights of others to space and privacy to fulfil their sexual needs through masturbation.
Standard 11 I understand that fulfilling my own sexual needs through masturbation must be conducted privately and discreetly.
Standard 12 I speak up if I have been hurt, harassed or assaulted either physically or sexually.
Standard 13 I speak up if I see or hear about someone else being hurt, harassed or assaulted either physically or sexually
.

Sexual Safety of Mental Health Consumers Guidelines NSW HealtH PaGe 59
APPENDIX B
Charter of Victims Rights
Extract from the Victims Rights Act 1996 – Part 2, Section 6Courtesy, compassion and respect
A victim should be treated with courtesy, compassion, and respect for the victim’s rights and dignity.
Information about services and remedies
A victim should be informed at the earliest practical opportunity, by relevant agencies and officials, of the services and remedies available to the victim.
Access to services
A victim should have access where necessary to available welfare, health, counselling and legal assistance responsive to the victim’s needs.
Information about investigation of the crime
A victim should, on request, be informed of the progress of the investigation of the crime, unless the disclosure might jeopardise the investigation. In that case, the victim should be informed accordingly.
Information about prosecution of accused
A victim should, on request, be informed of the following:
(a) the charges laid against the accused or the reasons for not laying charges,
(b) any decision of the prosecution to modify or not to proceed with charges laid against the accused, including any decision for the accused to accept a plea of guilty to a less serious charge in return for a full discharge with respect to the other charges,
(c) the date and place of hearing of any charge laid against the accused,
(d) the outcome of the criminal proceedings against the accused (including proceedings on appeal) and the sentence (if any) imposed.
Information about trial process and role as witness
A victim who is a witness in the trial for the crime should be informed about the trial process and the role of the victim as a witness in the prosecution of the accused.
Protection from contact with accused
A victim should be protected from unnecessary contact with the accused and defence witnesses during the course of court proceedings.
Protection of identity of victim
A victim’s residential address and telephone number should not be disclosed unless a court otherwise directs.
Attendance at preliminary hearings
A victim should be relieved from appearing at preliminary hearings or committal hearings unless the court otherwise directs.
Return of property of victim held by State
If any property of a victim is held by the State for the purpose of investigation or evidence, the inconvenience to the victim should be minimised and the property returned promptly.
Protection from accused
A victim’s need or perceived need for protection should be put before a bail authority by the prosecutor in any bail application by the accused.
Information about special bail conditions
A victim should be informed about any special bail conditions imposed on the accused that are designed to protect the victim or the victim’s family.
Information about outcome of bail application
A victim should be informed of the outcome of a bail application if the accused has been charged with sexual assault or other serious personal violence.

PaGe 60 NSW HealtH Sexual Safety of Mental Health Consumers Guidelines
Victim impact statement
A relevant victim should have access to information and assistance for the preparation of any victim impact statement authorised by law to ensure that the full effect of the crime on the victim is placed before the court.
Information about impending release, escape or eligibility for absence from custody
A victim should, on request, be kept informed of the offender’s impending release or escape from custody, or of any change in security classification that results in the offender being eligible for unescorted absence from custody.
Submissions on parole and eligibility for absence from custody of serious offenders
A victim should, on request, be provided with the opportunity to make submissions concerning the granting of parole to a serious offender or any change in security classification that would result in a serious offender being eligible for unescorted absence from custody.
Compensation for victims of personal violence
A victim of a crime involving sexual or other serious personal violence should be entitled to make a claim under a statutory scheme for victims’ compensation.

Sexual Safety of Mental Health Consumers Guidelines NSW HealtH PaGe 61
APPENDIX C
Relevant standards and the legislative framework
Relevant standards
■ UN Declaration – Rights of Disabled Persons
http://www.un-documents.net/a30r3447.htm
■ UN Principles for the Protection of Persons with
Mental Illness and for the Improvement of Mental
Health Care
www.un.org/documents/ga/res/46/a46r119.htm
■ NSW Ministry of Health Charter for Mental Health
Care in NSW
www.health.nsw.gov.au/pubs/2000/mhcharter.html
■ National Statement of Rights and Responsibilities of
Consumers of Mental Health Services
http://www.health.gov.au/internetmhsc/publishing.
nsf/Content/pub-sqps-rights
The legislative framework
Medical Practice Act 1992
■ Section 71A of the Medical Practice Act introduces
‘reportable misconduct’, placing an obligation on
doctors to report certain types of misconduct to the
Medical Board. This requirement came into force on
1 October 2008.
■ The reporting obligations are not general, but focus
on three areas of serious misconduct, one of which is
sexual misconduct.
■ The misconduct to be reported is linked to the
practice of medicine. Under current Board policy,
it is an absolute rule that a medical practitioner who
engages in sexual activity with a current patient/
consumer is guilty of professional misconduct.
■ Engaging in sexual activity with a patient/consumer
following the termination of the doctor/patient
relationship may also amount to professional
misconduct, depending on the circumstances of each
case. For more information refer to the Board’s policy
on sexual misconduct.
www.mcnsw.org.au/resources/1034
Crimes Act 1900
http://www.legislation.nsw.gov.au/fullhtml/inforce/
act+40+1900+cd+0+N
■ The Crimes Act 1900 consolidates the Statutes
relating to Criminal Law and regulates criminal law in
NSW.
■ Part 3 Division 10 relates to sexual assault offences.
■ Section 66F refers specifically to people with a
‘cognitive impairment’, which is defined in the act
as follows:
…a person has a cognitive impairment if the
person has:
(a) an intellectual disability, or
(b) a developmental disorder (including an autistic
spectrum disorder), or
(c) a neurological disorder, or
(d) dementia, or
(e) a severe mental illness, or
(f) a brain injury,
that results in the person requiring supervision or
social habilitation in connection with daily life
activities. Section 61H, (1A)
■ Under Section 66F (2) the Act states that a person
who has sexual intercourse with a person who has a
cognitive impairment and who was responsible for
the care of that person, whether generally or at the
time of the sexual intercourse, is guilty of an offence.
The maximum penalty for this offence is
imprisonment for 10 years.

PaGe 62 NSW HealtH Sexual Safety of Mental Health Consumers Guidelines
■ The Act defines a ‘person responsible for care’ as
follows:
… a person is responsible for the care of a person
who has a cognitive impairment if the person
provides care to that person:
(a) at a facility at which persons with a cognitive
impairment are detained, reside or attend, or
(b) at the home of that person in the course of a
program under which any such facility or other
government or community organisation provides
care to persons with a cognitive impairment.
The care of a person with a cognitive impairment includes
voluntary care, health professional care, education, home
care and supervision.
Section 66F, (1)
■ Under Section 66F (3) a person who has sexual
intercourse with a person who has a cognitive
impairment, with the intention of taking advantage of
that person’s cognitive impairment, is guilty of an
offence. The maximum penalty for this offence is
imprisonment for eight years. Attempting sexual
intercourse attracts the same penalties.
■ Importantly, under Section 66F (5) consent is not a
defence for sexual intercourse on the basis that in
many of these cases it would be considered that the
victim is incapable of giving informed consent.
Victims Rights Act 1996
http://www.legislation.nsw.gov.au/sessionalview/
sessional/act/1996-114.pdf
■ The purpose of this Act is to recognise and promote
the rights of victims of crime. It establishes a Charter
of Victim’s Rights for the appropriate treatment of
victims of crime by government agencies and those
funded by government. This includes Police, health,
welfare, prosecution and correctional services.
■ This means that mental health staff have an
obligation to take account of the Charter in the
administration of their service when dealing with
a victim of crime.
■ The Charter is monitored by the Victim Services,
Department of Attorney General and Justice’ (http://
www.lawlink.nsw.gov.au/vs).
■ The rights outlined within the Charter have been
included at Appendix A.
Health Records and Information Privacy Act
www.legislation.nsw.gov.au/fullhtml/inforce/
act+71+2002+FIRST+O+N
■ The purpose of this Act is to promote fair and
responsible handling of health information by both
the private and public health sector.
■ Schedule 1 of this Act provides a set of Principles that
pertain specifically to public health organisations.
Health Privacy Principles (http://www.austlii.edu.au/
au/legis/nsw/consol_act/hraipa2002370/sch1.html)
Children and Young Persons (Care and Protection) Act 1998
http://www.legislation.nsw.gov.au/fullhtml/inforce/
act+157+1998+FIRST+0+N
■ Health care staff, including mental health, are
considered under this Act to be mandatory reporters.
■ A mandatory reporter is someone who is required
by law to make a report to the Department of
Community Services (DoCS) if they have current
concerns about the safety, welfare or wellbeing of a
child. This includes concerns about the child or young
person having been sexually abused or being at risk
of being abused. Mandatory reporters face penalties
for failing to make a report.
■ A child is a person under 16 years of age and a young
person is 16 or 17 years old. This is an important
distinction because the Act has different provisions
for children and young people.
■ Mandatory reporting requirements only apply to
children. Services can also report concerns they may
have about the safety, welfare or well-being of a
young person, but this is not a mandatory reporting
requirement (Refer to Section 3 of the Act for
definitions of children and young people.)
Crimes Act 2000
http://www.legislation.nsw.gov.au/viewtop/inforce/
act+66+2007+cd+0+Y/
■ Consent exists only when a person freely and
voluntarily agrees to engage in sexual intercourse.
The law states that a person is unable to give consent
when they were:
– asleep or unconscious
– significantly intoxicated or affected by drugs
– unable to understand what they are consenting to
Sexual Safety of Mental Health Consumers Guidelines NSW HealtH PaGe 63
– intimidated, coerced or threatened
– submitted to the abuse of authority of a
professional or any other trusted person
– unlawfully detained, or held against their will.
■ These laws do not generally apply to children and
vulnerable people who, under the law, cannot be
said to have consented because of their age and
vulnerability.
■ Vulnerable people include children less than 16 years
of age and people with a cognitive impairment.
A person has a cognitive impairment if they require
supervision or social habilitation in connection with
daily life activities, as a result of one or more of the
following:
(a) an intellectual disability
(b) a developmental disorder (including an autistic
spectrum disorder)
(c) a neurological disorder
(d) dementia
(e) a severe mental illness
(f) a brain injury.
Criminal Procedure Act 1986 No 2009 (Part 5 Division 2 – Sexual Assault Communications Privilege)
■ This Act provides specific protections where there are
criminal proceedings or in Apprehended Violence
Order (AVO) matters.
■ Health records are deemed to be privileged when
the consumer receives counselling or mental health
treatment in which confidential communications are
made by the consumer to health staff; this includes
health staff conversations about the consumer to
another person based upon the consumer’s
communications.
■ This legislation applies to any counselling or mental
health treatment received either before or after an
incident of sexual assault.
■ The privilege that may be claimed in district or local
court proceedings can at times be effectively used in
other court jurisdictions arguing that it is not in the
‘public interest’ for the health records to be accessed
by other parties or that it is not relevant to the current
proceedings.
■ Refer to NSW Health Policy on Subpoenas
(PD2010_065).

PaGe 64 NSW HealtH Sexual Safety of Mental Health Consumers Guidelines
APPENDIX D
Information about support options for consumers who have experienced sexual assault
If you experience sexual assault or harassment, you can: Report to Police and access medical care and support
You can choose to report right away. The Police will need to gather evidence of the assault, which will include a forensic medical examination. They can support you to access medical care (through the local Sexual Assault Service or your nearest hospital or emergency department) and counselling and can help with protection/ safety needs. They can also support you to make a statement but you don’t have to do this right away if you’re not feeling up to it.
Where possible a full forensic exam is most effective within 72 hours of the assault or within one week.
If you want to report to the Police, you can call 000 or contact your nearest Police station. You can ask to speak to a female officer.
Report to Police, access medical care and support, but request no further legal action
You can choose to report to Police and access medical care, counselling support, and undergo a forensic medical examination (through the local Sexual Assault Service or your nearest hospital or emergency department), but withdraw your complaint at a later time if you feel unable to proceed.
Where possible a full forensic exam is most effective within 72 hours of the assault or within one week.
If you want to report to the Police, you can call 000 or contact your nearest Police station. You can ask to speak to a female officer.
Police can also help with protection/safety needs.
Access medical care and forensic exam if undecided about whether to report
You can keep your options open by having a forensic medical examination and asking that the Sexual Assault Service store the evidence (for up to three months) while you decide if you want to proceed with legal action.
Where possible a full forensic exam is most effective within 72 hours of the assault or within one week.
You can contact your nearest Sexual Assault Service or go to your nearest hospital or emergency department – contact the Victims Access Line Line on 1800 633 063 or (02) 8688 5511 for referral to your nearest medical care facility where you can access a forensic medical examination.
Access medical care and support and not report assault to Police
You can choose not to report to Police but still get a medical check done and access counselling support from the local Sexual Assault Service.
Medical care can involve dealing with the physical and psychological impact of the assault, as well as any concerns about pregnancy or sexually transmitted infections. Please note that morning after pills are most effective taken within 72 hours of the assault.
You can contact your nearest Sexual Assault Service or go to your nearest hospital or emergency department.
You could also see a general practitioner/ doctor if you don’t want a full forensic exam. Women’s Health Centres, Sexual Health Centres and Family Planning Clinics can also offer medical support/ follow up.
No medical care or reporting, but still access support
You can choose not to report to Police or get a medical check done. This option does not include medical support or legal action.
For counselling support, you can still contact your nearest Sexual Assault Service or go to your nearest hospital or emergency department, the Victims Access Line on 1800 633 063 or (02) 8688 5511.

Sexual Safety of Mental Health Consumers Guidelines NSW HealtH PaGe 65
APPENDIX E
Information about reporting to Police for consumers who have experienced sexual assault
■ Sexual assault is a serious crime
■ A complaint can be made at any time. It does not have to be straight away.
■ You can have forensic evidence taken and decide about reporting later.
■ If the assault happened in the past, or when you were a child, a statement can still be made. Sometimes Detectives
have other information about the offender which may help build a case.
■ When making a complaint you can take a support person as long as that person will not be a witness – the Detectives
can assist in deciding this. You can ask to meet Detectives at another location initially although the statement will be
taken at the Police Station. If walking into the Police Station feels difficult, you can ring the Crime Manager, or ask your
mental health service to ring them, to arrange an easier way to make contact.
■ If an interpreter is needed the Police will arrange this.
■ You can ask to speak to a female Detective and if one is available that will be arranged.
■ If making a formal complaint is too difficult but you would like Police to have information about the crime, an informal
report can be made. This may help in other investigations.
■ You have the right to withdraw a complaint at any time.
■ The Police Duty Officer or Crime Manager will ask basic information and then call a Detective.
■ If the assault was recent Police will, with permission, take you to the nearest sexual assault unit where sexual assault
counselling, medical assistance and the collection of forensic evidence will, with your permission, be arranged.
■ Detectives will determine what investigations will take place after taking your statement. This may take some time and
the Detectives may ask for further information.
■ The investigating Detective will provide their contact details and the case number and keep you, or your nominated
representative, informed of progress. You can ring the Detective for updates, or ask your mental health service to do
this.
■ If the Detective can gather enough evidence, charges will be laid. Sometimes there is not enough evidence and there is
no further action. This does not mean the Police do not believe you – it only means that they cannot prove ‘beyond
reasonable doubt’ that a crime has occurred.
Source: NSW Rape Crisis Centre information sheet ‘Sexual Assault in NSW’
Things to consider when deciding whether to report an incident of sexual assault to police
What will happen when you do report sexual assault to police

PaGe 66 NSW HealtH Sexual Safety of Mental Health Consumers Guidelines
APPENDIX F
Example posters on accessing support
Appendix F – Example posters on accessing support
Are you someone with a mental illness that fits into one of the following groups? If you need help and advice about sexual assault or abuse, you can contact the Sexual Assault Service in your locality.
Are you from a Culturally and Linguistically Diverse background? If so, you can also contact:
Community Relations Commission
1300 651 500
Telephone Interpreter Services (24hrs)
13 14 50
Transcultural Mental Health
1800 648 911
Services for Treatment & Rehabilitation of Torture & Trauma Services (STARTTS)
02 9794 1900
<INSERT LOCAL SUBURB> SEXUAL ASSAULT SERVICE 02 <INSERT LOCAL SAS PHONE NUMBER>
An adult sexual assault victim
An adult who was sexually abused as a child
A child or young person under the age of 18 years who has been sexually assaulted or abused
A parent, carer, friend or family of a sexual assault victim

Sexual Safety of Mental Health Consumers Guidelines NSW HealtH PaGe 67
Are you a Koori person with a mental illness that needs information about sexual assault or abuse? If you are an Aboriginal person that needs help and advice about sexual assault or abuse, you can contact the following services.
•Indigenous Women's Legal Centre & Contact Line 1800 39 784•Wirringa Baiya Aboriginal women's Legal Centre, phone 1800 686 587•Aboriginal and Torres Strait Islander Legal Services: www.nwjc.org.au
Sexual Assault Services for Aboriginal & Torres Strait
Islander people
•If you wish to talk to the police about a sexual assault, you can ask to speak with an Aboriginal Community Liaison Officer, who may be located in the Local Area Command. •Police can also contact an Aboriginal Support Person if there is an Aboriginal Support Group or a list of Aboriginal Support persons located in that command.
Aboriginal Community Liaison Officer or
Aboriginal Support Person
•If you are an Aboriginal child or young person or are concerned that a child or young person has been sexually assaulted, you can make a report to the Department of Community Services by contacting the DoCS Helpline , phone 132 111. •If you would like to speak to someone in person, you can go your local Community Services Centre where arrangements can be made for you to talk to an Aboriginal Caseworker.
Department of Community Services or Community
Services Centre
•If you wish to speak to an Aboriginal counsellor in your area, you can contact the Centre for Aboriginal Health on (02) 9391 9502 about the availability of Aboriginal Family Health Workers, and/or Aboriginal sexual assault workers in your area. •NSW health has specially trained counsellors who receive training to respond to the needs of victims of sexual assault.
Centre for Aboriginal Health
•If you are an Aboriginal or Torres Strait Island person who is a victim of violent crime in NSW, like family violence or sexual assault you can call our confidential enquiry line on 188 019 123.• The Witness Assistance Service of the Office of the Director of Public Prosecutions, has some Aboriginal Witness Assistance Officers, who can assist you if you have to go to court. Contact (02) 9285 2502 or 1800 814 534.
Victims Services

PaGe 68 NSW HealtH Sexual Safety of Mental Health Consumers Guidelines
APPENDIX G
Sexual Assault Screening Tool
Assure the consumer of confidentiality:
■ Clearly state that any information shared will not be disclosed to the consumer’s carer or family.
■ Know your service’s responsibility regarding reporting sexual assault and take this into consideration when discussing the issue.
■ Assure the consumer that information provided will be kept confidential, except where the assault involves a child or young person, or where the alleged perpetrator is a health worker.
Frame the questions: ■ “So that I can work out the right way to support you while you are with our service, I need to know a bit more detail about your life before you came here, including any experiences you may have had that made you uncomfortable.”
■ “Because sexual assault is so common in many people’s lives, particularly people with mental health issues, we ask all our patients about it.”
■ “I don’t know if this is a problem for you, but many people we see are dealing with a past instance of sexual assault. Some people are reluctant to bring it up, so we always ask the question.”
Ask direct questions: ■ Are you in a relationship with someone who physically or emotionally hurts or threatens you?
■ Has your partner ever forced you to have sex when you didn’t want to or hurt you sexually?
■ Has a friend, a date, or an acquaintance ever pressured or forced you into sexual activities when you did not want them? Touched you in a way that made you uncomfortable? Anyone at home? Anyone at school? Anyone within this service? Any other adult?
Ask about injuries: ■ I notice you have a number of bruises (or other injury) - did someone do this to you?
■ Was it someone from home, like your partner or spouse? Was it someone from within this service?
In a private area
In all mental health settings
WH
ERE As part of routine
admission process or during initial visit
As part of a routine health assessment or taking a health history
During every encounter with a new consumer
Delay until the consumer is stable
WH
EN Combine with any existing violence screening processes
Assure the consumer of confidentiality
Frame the questions to be asked
Ask direct questions
Ask about injuries
Respond to disclosure OR respond to denials
HO
W

Sexual Safety of Mental Health Consumers Guidelines NSW HealtH PaGe 69
Respond to disclosure:
■ Allow the consumer to talk about it – listen non-judgmentally and validate the consumer’s experience by conveying affirming messages that demonstrate sensitivity and compassion.
■ Explore details of the assault (using open-ended questions only), if the consumer is comfortable to do this, and assess the consumer’s mental state.
■ Take steps to ensure the consumer’s safety and secure any evidence if the assault is recent.
■ Offer support and options for dealing with the assault, or set a time to discuss the assault further when the consumer is comfortable to do this.
■ Assess the consumer’s capacity to make decisions regarding reporting the assault or undertaking a forensic medical exam.
■ Organise for the consumer to receive medical care and counselling as required.
Respond to denials: ■ If the consumer denies any assault has taken place, but you still suspect it, let them know your concerns.
■ Make sure you provide the consumer with information about their options if they have been sexually assaulted.
■ Document your concerns in the consumer’s file.

PaGe 70 NSW HealtH Sexual Safety of Mental Health Consumers Guidelines
APPENDIX H
Examples of sexualised behaviour by healthcare professionals towards consumers or their carers
ý Asking for or accepting a date
ý Sexual humour during consultations or examinations
ý Inappropriate sexual or demeaning comments, or asking clinically irrelevant questions, for example about their body or
underwear, sexual performance or sexual orientation
ý Requesting details of sexual orientation, history or preferences that are not necessary or relevant
ý Internal examination without gloves
ý Asking for, or accepting an offer of, sex
ý Watching a consumer undress (unless a justified part of an examination)
ý Unnecessary exposure of the consumer’s body
ý Accessing a consumer’s or family member’s records to find out personal information not clinically required for their
treatment
ý Unplanned home visits with sexual intent
ý Taking or keeping photographs of the consumer or their family that are not clinically necessary
ý Telling consumers about their own sexual problems, preferences or fantasies, or disclosing other intimate
personal details
ý Clinically unjustified physical examinations
ý Intimate examinations carried out without the consumer’s explicit consent
ý Continuing with examination or treatment when consent has been refused or withdrawn
ý Any sexual act induced by the healthcare professional for their own sexual gratification
ý The exchange of drugs or services for sexual favours
ý Exposure of parts of the healthcare professional’s body to the consumer
ý Sexual assault
Source: Clear sexual boundaries between healthcare professionals and patients – Information for patients and carers Council for Healthcare Regulatory Excellence, April 2009

Sexual Safety of Mental Health Consumers Guidelines NSW HealtH PaGe 71
APPENDIX I
Responding to a disclosure of sexual assault – key actions
Key action When the assault occurred in the last 7 days
When the assault occurred in the last 6 months
When the assault occurred in the past
Acknowledge and affirm the disclosure
If it is the first disclosure or the consumer has had previous negative experiences of disclosure, regardless of when the assault occurred, this may be a time of crisis for the consumer and staff may need to respond particularly sensitively.
Explore the disclosure
Establish and maintain safety
Secure any evidence
Secure any evidence related to the sexual assault – keep any clothing removed by the victim/survivor that they were wearing at the time of the assault, and secure the location of the assault if possible to prevent any evidence being disturbed.
Offer support and options
A sexual assault can still be reported to the Police when it is not recent and the victim/survivor can still benefit from contact with the local Sexual Assault Service or other relevant counselling and support service.
Assess capacity to make informed decisions
Organise medical care
It is important that victims of sexual assault are offered medical assistance to treat any physical or psychological injuries, regardless of whether the assault was recent or occurred some time ago.
Consumers who were sexually abused as children, or in other settings, may be retraumatised when they enter a new facility, or by events at a facility. Mental health staff should note and be sensitive to ‘triggers’ in their work with consumers that may cause retraumatisation.

PaGe 72 NSW HealtH Sexual Safety of Mental Health Consumers Guidelines
Step Action Information
1 Acknowledge and affirm the disclosure
Be non-judgemental, compassionate and understanding when a consumer discloses their experience of sexual assault or harassment and respond promptly, in accordance with the Sexual Safety of Mental Health Consumers Guidelines, whether the assault occurred prior to or after the consumer’s admission.
2 Explore the disclosure Provide the consumer with a safe, quiet, private space and gently encourage them to provide information about the assault. Ensure an assessment of the consumer’s clinical mental state is undertaken within 24 hours in an acute inpatient setting and within 48 hours in all other settings before proceeding with next steps.
3 Establish and maintain safety Assess whether the consumer is in current danger and the need for special accommodations to make the consumer feel safe, being mindful that it is the alleged perpetrator and not the consumer who has been assaulted that should be moved from the facility if required, unless the consumer who has disclosed the assault specifically requests otherwise or there are other extenuating circumstances.
4 Secure any evidence Keep any clothing worn by the consumer at the time of the assault, ensure only the consumer handles these clothes, and secure the location of the assault if possible along with any CCTV footage of the area in which the incident occurred.
5 Offer support and options Provide the consumer with advice and information regarding their options (Appendix D of the Sexual Safety of Mental Health Consumers Guidelines) so they can decide how they want to proceed. The consumer’s wishes regarding how to proceed must be respected unless legislatively prohibited or they lack the capacity to make an informed decision (see Step 6).
6 Organise medical care Encourage the consumer to seek immediate medical care to identify and treat any physical injuries and to discuss issues such as the risk of infection or pregnancy. Offer counselling as required and ensure consent is obtained for any forensic exam.
7 Assess capacity to make informed decisions
This assessment will need to include an evaluation of the consumer’s capacity to understand their options, process and communicate information and effectively exercise their rights. If they are assessed as not having the capacity to make an informed decision regarding their options, any such decision should be delayed if possible until the consumer’s capacity is restored. Alternatively, urgent application can be made for a Guardian to make some decisions.

Sexual Safety of Mental Health Consumers Guidelines NSW HealtH PaGe 73
APPENDIX J
Responding to a disclosure of recent sexual assault – quick checklist
Issues to be considered Yes No Action required/taken Date action taken
Is the consumer in current danger?
Do special accommodations need to be made to make the consumer feel safe?
Has any evidence related to the assault been secured?
Does the consumer want a member of their family or their carer informed?
Does the consumer want to report the assault to the Police?
Does the consumer want to talk to a Sexual Assault Service or other counselling service?
Has the consumer been assessed regarding their capacity to make an informed decision in relation to their assault?
Does the consumer have acute injuries that need medical attention?
Does the consumer want or need a forensic exam to be performed?
If the assault happened within the past 120 hours, and the consumer is female, do they want or need emergency contraception?
Does the consumer want or need prophylaxes for HIV or other sexually transmitted infections?
Does the consumer want or need follow-up care, for either physical or psychological injuries?

PaGe 74 NSW HealtH Sexual Safety of Mental Health Consumers Guidelines
APPENDIX K
Follow up medical exams required when a person has been sexually assaulted
Follow-up medical exams are recommended at 2 weeks, 3 months and 6 months post assault. The local Sexual Assault
Service can organise this, but if the consumer does not wish to involve anyone outside of the mental health service, staff
will need to ensure these exams take place.
The 2-week follow-up exam – clinician will need to:
■ Examine any injuries for proper healing.
■ Photograph injuries if indicated (i.e. to document healing, comparisons in court). This should not include injuries to the
genital area.
■ Check that the consumer has completed the course of any medications given for STIs.
■ Obtain cultures and draw blood to assess STI status, especially if prophylactic antibiotics were not given at the
initial visit.
■ Discuss results of any tests performed.
■ Test for pregnancy if indicated. If pregnant, advise about options.
■ Remind consumers to return for their hepatitis B vaccinations in 1 month and 6 months, other immunisations as
indicated, and HIV testing at 3 and 6 months or to follow-up with their usual health care provider.
■ Make follow-up appointments.
■ Assess the consumer’s emotional state and mental status, and encourage the consumer to seek counselling if they have
not yet done so.
The 3-month follow-up exam – clinician will need to:
■ Test for HIV. Make sure that pre- and post-testing counselling is available or make the appropriate referral. Assess
pregnancy status and provide advice and support.
■ Discuss results.
■ Draw blood for syphilis testing if prophylactic antibiotics were not given previously.
■ Assess consumer’s emotional state and mental status and encourage the consumer to seek counselling if they have not
yet done so.
The 6-month follow-up exam – clinician will need to:
■ Test for HIV. Make sure that pre- and post-testing counselling is available or make an appropriate referral.
■ Discuss results.
■ Administer the third dose of the hepatitis B vaccine.
■ Assess the consumer’s emotional health and refer as necessary.
The above information is drawn from the World Health Organisation 2003 Guidelines for medico-legal care for victims of sexual violence, WHO, Geneva

Sexual Safety of Mental Health Consumers Guidelines NSW HealtH PaGe 75
APPENDIX L
Reporting process for an incident of sexual assault
Internally
■ To the Team Leader/Nursing Unit Manager, who must inform the Senior Manager.
■ Through the Reportable Incident Brief (RIB) system – RIB must be submitted within 24 hours when:– the alleged perpetrator is a staff member; or– the consumer who has been assaulted is under 16 years of age; or – the consumer who has been assaulted is over 16 but under 17 years of age and is in a care relationships with the
alleged perpetrator.
■ Through the Root Cause Analysis (RCA) investigation process.
Externally
To the NSW Police Force when:– the consumer requests this and an assessment of the consumer’s clinical mental state does not preclude this as a
relevant step;– the alleged perpetrator is a staff member; or– the consumer is under 16 years of age; or– the consumer is over 16 but under 18 years of age and in a care relationship with the alleged perpetrator; or the
consumer does not have the capacity to make an informed decision, and the senior clinician has a duty of care to formally report the assault.
To the Child Protection Helpline (13 36 27) when:– the consumer is a child under 16 years of age. The Helpline must also be contacted if the consumer is a child at risk
of significant harm (which includes when they have had consensual sexual intercourse); or– the consumer is over 16 but under 17 years of age and in a care relationship with the alleged perpetrator.

PaGe 76 NSW HealtH Sexual Safety of Mental Health Consumers Guidelines
APPENDIX M
Information about Managing Disinhibited Behaviour
Talk about behaviour Educate and inform family, friends, staff about the behaviour and strategies to manage it.
■ Talk to the person about their behaviour and what you expect.■ Let them know if behaviour is not appropriate – if they don’t know, they can’t change it.■ Let them know how the behaviour makes you feel e.g. ‘I feel uncomfortable when …’■ Let other people know what strategies to use.
Provide feedback about behaviour
Provide the person with frequent, direct and clear feedback. Feedback should:
■ Be immediate and early■ Be direct■ Be concrete and describe the behaviour■ Give direction■ Be consistent■ Not reinforce/encourage behaviour■ Help the person to learn■ Not be demeaning or humiliating■ Not impose your own values
Manage the environment ■ Try to predict situations where the behaviour is more likely to happen.■ Work out strategies ahead of time to cope with the behaviour.■ Restrict any opportunity to engage in inappropriate behaviour (planning, proximity,
opportunity, means)■ Limit any ‘at risk’ social activities e.g .crowded clubs or pubs or where alcohol is being
consumed.■ Provide cues re behaviour – what the person should/should not do – before, during, and
after social activities.■ Limit the amount of time a person spends in each situation.■ Provide alternative activities e.g. small groups verses large groups.■ Keep a comfortable distance so the person cannot touch, grab or get too close.
Provide supervision and structure
■ Provide one-to-one support and supervision in any ‘at risk’ situations.■ Provide cues and prompts about appropriate or inappropriate behaviour.■ Redirect, distract or divert the person e.g. more appropriate topics of conversation, or
change the activity or task.
Plan ahead If a person has a history of severe disinhibited sexual behaviour (exposure, masturbation in public, or sexual assault), it is essential that you plan ahead regarding personal safety.
Consider:
■ having two people provide care■ limiting home visits■ supervising children■ limiting access to certain environments
In the person’s home:
■ Always visit with another person or make sure someone knows you are there when you visit.■ Take a mobile phone with you, and carry it at all times.■ Have your car keys in your pocket.■ Get familiar with the home, so you know where the doors are located.■ Keep a comfortable distance. For example, sit across a table, sit close to the door.
Adapted from the State of Queensland (Queensland Health) 2007 Acquired Brain Injury Outreach Service

Sexual Safety of Mental Health Consumers Guidelines NSW HealtH PaGe 77
References
Abuse and Violence: Working with our patients in general
practice (3rd edition) (2008). South Melbourne: The
Royal Australian College of General Practitioners.
Acquired Brain Injury Outreach Service (2011). What is
disinhibited and inappropriate sexual behaviours?
Retrieved August 2011, from Queensland Health:
http://www.health.qld.gov.au/abios/
Agar, K, Read, J, Bush, J.M. (2002). ‘Identification of
abuse histories in a community mental health
centre: The need for policies and training’. Journal
of Mental Health, vol. 11, no. 5, pp. 533-543.
Burgess AW, Holmstrom LL. Rape trauma syndrome.
Am J Psychiatry 1974: 131:981–6.
Carmody, M. (2003). Sexual Ethics and Violence
Prevention. Social & Legal Studies, 199-216.
Carmody, M., Evans, S., Krogh, C., Flood, M., Heenan,
M., & Ovenden, G. (2009). Framing best practice:
National Standards for the primary prevention of
sexual assault through education, National Sexual
Assault Prevention Education Project for NASASV.
University of Western Sydney, Australia.
Carmody, M., & Willis, K. (2006). Developing Ethical
Sexual Lives: Young People, Sex and Sexual Assault
Prevention. Sydney: University of Western Sydney,
Social Justice Social Change Research Centre.
Cook, B., David, F., Grant, A. (2001). Sexual Violence in
Australia. Australian Institute of Criminology.
ISBN 0 642 24205 4.
Crome, S. (2006). Male survivors of sexual assault and
rape (ACSSA Wrap No. 2). Melbourne: Australian
Centre for the Study of Sexual Assault.
Deegan, P. E. (2001). Human Sexuality and Mental Illness:
Consumer Viewpoints and Recovery Principles. USA.
Department of Health. Women’s Mental Health: Into the
Mainstream, Strategic Development of Mental
Health Care for Women. (2002). Available at: www.
dh.gov.uk/assetRoot/04/07/54/80/04075480.pdf
Disability Discrimination Legal Service. (2003). Beyond
Belief, Beyond Justice: The difficulties for victim/
survivors with disabilities when reporting sexual
assault and seeking justice. Melbourne.
Evans I 2007, Battle-scars: Long-term effects of prior
domestic violence, Melbourne: Centre for Women’s
Studies and Gender Research, Monash University.
Ford, E., Rosenberg, M., Holsten, M., & Boudreaux, T.
(2003). Managing Sexual Behavior on Adult Acute
Care Inpatient Psychiatric Units. PSYCHIATRIC
SERVICES, 54 (3), 346-350.
Golding, J.M. (1999) ‘Intimate partner violence as a risk
factor for mental disorders: a meta-analysis’, Journal
of Family Violence, vol. 14, no. 2: 99–132.
Goodfellow, J., & Camilleri, M. (2003). Beyond Belief,
Beyond Justice: The difficulties for victim/survivors
with disabilities when reporting sexual assault and
seeking justice. Final report of stage one of the
Sexual Offences Project. Melbourne: Disability
Discrimination Legal Service.
Goodman, L.A.; Rosenberg, S.D.; Mueser, K.T.; and
Drake, R.E. Physical and sexual assault history in
women with serious mental illness: Prevalence,
correlates, treatment, and future research directions.
Schizophrenia Bulletin, 23(4):685-696, 1997.
Goodman, L.A.; Salyers, M.P.; Mueser, K.T.; Rosenberg,
S.D.; Swartz, M.; Essock, S.M.; Osher, F.C.; and
Butterfield, M.I. Recent victimization in women and
men with severe mental illness: Prevalence and
correlates. Journal of Traumatic Stress, 14:615-632,
2001.

PaGe 78 NSW HealtH Sexual Safety of Mental Health Consumers Guidelines
Goodman, L.A.; Thompson, K.M.; Weinfurt, K.; Corl, S.;
Acker, P.; Mueser, K.T.; and Rosenberg, S.D.
Reliability of reports of violent victimization and
PTSD among men and women with SMI. Journal of
Traumatic Stress, 12:587-599, 1999.
Havig, K. (2008, January). The Health Care Experience of
Adult Survivors of Child Sexual Abuse – a
systematic review of evidence on sensitive practice.
Trauma, Violence & Abuse, pp. 19-33.
Jennings, A. (2004). The Damaging Consequences of
Violence And Trauma: Facts, Discussion Points, and
Recommendations for the Behavioural Health
System. Alexandria, VA: National Association of
State Mental Health Program Directors, National
Technical Assistance Center for State Mental Health
Planning.
Kessler, R.C.; Crum, R.M.; Warner, L.A.; Nelson, C.B.;
Schulenberg, J.; and Anthony, J.C. Lifetime
co-occurrence of DSM-III-R alcohol abuse and
dependence with other psychiatric disorders in the
national comorbidity survey. Archives of General
Psychiatry, 54:313-321, 1997.
Kessler, R.C.; Sonnega, A.; Bromet, E.; Hughes, M.; and
Nelson, C.B. Posttraumatic stress disorder in the
national comorbidity survey. Archives of General
Psychiatry, 52:1048-1060, 1995 Inappropriate
Sexual Behavior in Long-Term Care.
Making choices Keeping safe Policy and Practice
Guidelines on relationships and sexual wellbeing
when working with people with learning disabilities.
(2004) UK. Lothian National Health Service.
Mental Health ACT. (2009, January). Promotion of Sexual
Safety/Prevention and Management of Sexual
Assault in Bed Based Services Policy. ACT, Australia.
McGee H, Garavan R, deBarra M, Byrne J, Conroy R
(2002). The SAVI Report. Sexual Abuse and
Violence in Ireland. A national study of Irish
experiences, beliefs and attitudes concerning sexual
violence. Dublin: Liffey Press, 2002.
Mueser, K.T.; Goodman, L.B.; Trumbetta, S.L.; Rosenberg,
S.D.; Osher, F.C.; Vidaver, R.; Auciello, P.; and Foy,
D.W. ‘Trauma and posttraumatic stress disorder in
severe mental illness’. Journal of Consulting and
Clinical Psychology, 66:493-499, 1998.
National Disability Services WA. (2008). Guidelines for the
prevention and management of sexual abuse for
disability service providers in Western Australia –
An Information and Policy Resource.
‘National Executive Training Institute (NETI). (2005).
Training Curriculum for Reduction of Seclusion and
Restraint. Draft curriculum manual. Alexandria, VA:
National Association of State Mental Health
Program Directors (NASMHPD), National Technical
Assistance Center for State Mental Health Planning
(NTAC).
National Sexual Violence Resource Center. (2011).
Assessing Patients for Sexual Violence – A Guide for
Health Care Providers.
Paul Kettl, M. (2008). Inappropriate Sexual Behaviour in
Long-Term Care. Annals of Long-Term Care.
Petrak, J. (2002). The psychological impact of sexual
assault. In J. Petrak & B. Hedge (Eds.), The Trauma
of Sexual Assault: Treatment, Prevention and
Practice. West Sussex: John Wiley & Sons.
Powell, A. (2007). Sexual pressure and young people’s
negotiation of consent. ACSSA Aware Newsletter,
14, 8–16. Retrieved 31 July 2008.
From http://www.aifs.gov.au/acssa/pubs/newsletter/
n14.html
Powell, S. M. (2008). Sexual assault and adults with a
disability – enabling recognition, disclosure and a
just response. ACSSA Issues, No. 9.
Registered Nurses’ Association of Ontario – Nursing Best
Practice Guidelines Program. (2005). Woman
Abuse: Screening, Identification and Initial
Response. Toronto: Registered Nurses’ Association
of Ontario.

Sexual Safety of Mental Health Consumers Guidelines NSW HealtH PaGe 79
Royal Australian College of General Practitioners – Quality
Care and Research Unit. (2008). Abuse and
violence: Working with our patients in general
prctice (3rd edition).
Simpson GK. & Orchison R (2006). Sexuality after
traumatic brain injury: issues and strategies.
In: Introduction to traumatic brain injury: a training
kit. http://www.tbistafftraining.info
Stepakoff, S. (1998). Effects of sexual victimization on
suicidal ideation and behaviour in U.S. college
women. Suicide and Life-Threatening Behavior,
28(1), 107–126.
Taft, A. (2003), ‘Promoting women’s mental health:
The challenges of intimate/domestic violence
againstwomen’, Issues Paper 8, Australian Family
and Domestic Violence Clearinghouse, Sydney.
Available: www.adfvc.unsw.edu.au/PDF%20files/
Issues_Paper_8.pdf
Teasdale,B. (2009) ‘Mental Disorder and Violent
Victimization’, Criminal Justice and Behaviour,
Issue 36: 513-535.
Urbis Keys Young for the Office of the Status of Women,
Department of the Prime Minister and Cabinet.
(2004). National Framework for Sexual Assault
Prevention. ACT: Commonwealth of Australia.
Victorian Women and Mental Health Network. (2009).
Increasing Safety and Gender Sensitivity in mixed
sex psychiatric units.
Wahl, J. (2008). Sexuality in Long Term Care Homes –
the Legal Issues. Toronto, Ontario, Canada.
Warner, J., Pitts, N., Crawford, M. J., Serfaty, M.,
Prabhakaran, P., & Amin, R. (2004). Sexual activity
among patients in psychiatric hospital wards. Journal
of the Royal Society of Medicine, 97, 477-479.
Woman Abuse: Screening, Identification and Initial
Response – Nursing Best Practice Guideline. (2005).
Registered Nursing Association of Ontario, CAN.
The Women’s Health Council. (2007). A Guide to
Creating Gender-Sensitive Health Services.
The Women’s Health Council. Women’s Mental Health:
Promoting a Gendered Approach to Policy and
Service Provision. Dublin.
Women’s Centre for Health Matters Inc. (2009). WCHM
Position Paper on Gender Sensitive Mental Health
Service Delivery. Canberra.
World Health Organization, International Consortium of
Psychiatric Epidemiology. 2000. Crossnational
comparisons of mental disorders. Bulletin of the
World Health Organization, 78: 413-426.
World Health Organization (2006). Gender disparities in
mental health. Available at:
www.who.int/mental_health/media/en/242.pdf.
Accessed 9 July 2012.

Disclaimer
While every effort has been made to ensure the accuracy and reliability of the information in this document at the time of publication, it is the
responsibility of users to check the currency of key documents, policies and procedures.
Acknowledgements
NSW Health would like to thank all members of the Working Group and the Reference Group, and a range of key stakeholders, who provided
support, guidance, advice and feedback during the development of the Sexual Safety of Mental Health Consumers Guidelines.
The NSW Ministry of Health extends special thanks to:
AIDS Council of NSW Inc (ACON)
Association of Relatives and Friends of the Mentally Ill (ARAFMI) NSW
Assoc. Prof Julian Trollor
Chair, Intellectual Disability Mental Health, School of Psychiatry
Head, Department of Developmental Disability Neuropsychiatry
University of New South Wales
Education Centre Against Violence (ECAV)
Ministry of Health, Centre for Aboriginal Health
Ministry of Health, Mental Health Program Council Consumer Sub-committee
Ministry of Health, Mental Health Clinical Advisory Council
Ministry of Health, MH-Kids, Mental Health and Drug and Alcohol Office (MHDAO)
Ministry of Health, Primary Health and Community Partnerships Branch
Ministry of Health, MHDAO, Older Persons Mental Health
NSW Consumer Advisory Group – Mental Health (Inc) (NSW CAG)
NSW Health Local Health District (LHD) mental health clinicians and staff
NSW Health Sexual Assault Services
NSW Police Force
Transcultural Mental Health Centre

SHPN (MHDAO) 120421


















