ANIMAL (2) - MWIT€¦ · SimpleAnimals.htm Cnidae = Nettle Radial symmestry Two layer Nematocyst

38 MJA Vol 178 6 January 2003
BITES AND STINGS
Severity of Irukandji syndrome and nematocyst identification from skin scrapings
Truc T Huynh, Jamie Seymour, Peter Pereira, Richard Mulcahy, Paul Cullen, Teresa Carrette and Mark Little
Emergency Department, Cairns Base Hospital, Cairns, QLD.Truc T Huynh, MB BS, Emergency Registrar; Peter Pereira, FACEM, Director of Emergency; Richard Mulcahy, FACEM, Emergency Consultant; Paul Cullen, FACEM, Emergency Consultant. School of Tropical Biology, James Cook University, Smithfield, QLD.Jamie Seymour, PhD, Senior Lecturer; Teresa Carrette, BSc, Marine scientist. Emergency Department, Sir Charles Gairdner Hospital, Perth, WA.Mark Little, FACEM, Emergency Consultant. Reprints will not be available from the authors. Correspondence: Dr Peter Pereira, Emergency Department, Cairns Base Hospital, PO Box 902, Cairns, QLD 4870. [email protected]
The Medical Journal of Australia ISSN:0025-729X 6 January 2003 178 1 38-41©The Medical Journal of Australia 2002www.mja.com.auBites and Stings
ABSTRACT
Objectives: (1) To identify the causative jellyfish species by examining skin scrapings in patients presenting to Cairns Base Hospital with marine stings, and (2) to describe clinical outcomes of those with Irukandji syndrome and those in whom nematocysts were identified from skin scrapings.
Design and setting: (1) A retrospective case series of 128 patients, identified from Cairns Base Hospital emergency department records with discharge diagnoses of marine stings between 1 July 2001 and 30 June 2002. (2) A prospective study of skin scrapings from 50 patients presenting with marine stings from the same period.
Main outcome measures: Number of patients with Irukandji syndrome, their opioid requirements and cardiac findings (where available); identification of causative species from nematocysts isolated from skin scrapings.
Results: 116 patients retrospectively identified with marine stings had Irukandji syndrome. Of 50 patients who had skin scrapings, 39 had nematocysts consistent with Carukia barnesi. Symptoms experienced ranged from local pain alone to severe Irukandji syndrome with elevated troponin I levels, changes on electrocardiogram, cardiac dysfunction on echocardiography, and high opioid dose requirements. One patient had an unidentified cnidome on his skin scraping. He developed severe Irukandji syndrome and subsequently died from its complications.
Conclusion: This is the first published report of Carukia barnesi being successfully identified from skin scrapings. Most patients with identifiable cnidomes experiencing Irukandji syndrome were stung by Carukia barnesi, which we show causes a wide range of illness, including cardiac dysfunction. Our finding of a cnidome not consistent with Carukia barnesi in the setting of Irukandji syndrome makes it possible that other
MJA 2003; 178: 38–41
species of jellyfish may also cause this syndrome.
JELLYFISH STINGS in northern Aus-tralia cause significant morbidity andmortality. Since early descriptions ofIrukandji syndrome,1,2 relatively littlefurther knowledge has been gainedabout it. Although Carukia barnesi hasbeen shown to cause the syndrome,3
other species of jellyfish are also sus-pected to be responsible.3-7
We hypothesise, firstly, that many dif-ferent cubozoans may produce Iru-kandji syndrome in Cairns, andsecondly, that these different species ofjellyfish may be responsible for differentseverities of this syndrome.
METHODS
Retrospective case series
All patients with a discharge diagnosisof “marine stings” (ICD-10 codeT63.6)8 after presenting to Cairns BaseHospital, Queensland, between 1 July2001 and 30 June 2002 were retrospec-tively identified from the emergencydepartment computer database, andepidemiological and clinical data wereextracted and entered on a standardisedform. Details collected included geo-graphic location of sting, physiologicalparameters, analgesia required, bio-chemical abnormalities, electrocardio-graphic and echocardiographic findings.
We assessed the clinical severity ofeach patient’s condition at presentationaccording to peak systolic blood pres-sure, total opioid dose administered,peak troponin I level, and length ofhospital stay. As individual patientsreceived either morphine, pethidine or
fentanyl according to clinician prefer-ence, we arbitrarily converted their opi-oid dose to “morphine equivalents”(where 1 mg morphine = 10 mgpethidine = 10 �g fentanyl) to give arough comparison of analgesic require-ments between patients.
Prospective case series
Patients presenting with marine stingsduring this period were treated accord-
ing to emergency department protocols,and additionally had skin scrapings oftheir sting site performed. Exceptionswere distressed children, patients withstings to the face, women with stings tothe breast region, and patients in whoman obvious sting site could not be iden-tified; these patients did not have skinscrapings performed.
The sampling procedure wasexplained to patients and verbal consentwas obtained. The sting site wasscraped firmly with a sterile scalpelblade, which was then placed in a sterilespecimen container containing 10%buffered formalin. The scalpel wasshaken vigorously in the specimen con-tainer to cause adherent scrapings to falloff. The specimen was then centrifugedat 5000 revolutions per minute for 10minutes, stained with eosin and distrib-

MJA Vol 178 6 January 2003 39
BITES AND STINGS
uted onto a Kova slide for microscopicexamination.
Specimens were prepared and exam-ined by one of the authors (J S), whowas blinded to the source. Identificationof jellyfish species was based on a cnid-ome database (a cnidome is a collectionof nematocysts used to distinguishbetween species of jellyfish) being for-mulated by the examiner and due forpublication in 2003.
The results of the species identifica-tion was then matched to the clinicaldata.
RESULTS
From 1 July 2001 to 30 June 2002, 128patients at the Cairns Base Hospitalemergency department had a dischargediagnosis of marine stings. Of these,116 had symptoms consistent with Iru-kandji syndrome. Sixty-seven of the 116patients (58%) were male and theiraverage age was 26.5 years (range, 3–63years).
Of the 116 patients with Irukandjisyndrome, 89 (7%) were stung alongthe shore, 26 (22%) were stung offshore(Great Barrier Reef and islands; see Box1), and one patient did not have thelocation recorded.
General clinical findings
Peak systolic blood pressure in the 94adults with Irukandji syndrome rangedfrom 100 mmHg to 230 mmHg, with amean of 145 mmHg. Nineteen of the 22children had their blood pressuresrecorded. Seven had a systolic bloodpressure 140 mmHg or above; the high-est of these was 165/95 mmHg in a 12-year-old child.
Total analgesic requirements foradults during their hospital stay rangedfrom 0 to 255 mg of morphine equiva-lents (mean, 31 mg). Of the 10 childrenwho had their weight recorded, analge-sic dose ranged from 0 to 1.4 mg per kgmorphine equivalents (mean, 0.29 mgper kg).
Cardiac findings
Troponin levels (cTnI) were measuredin 103 patients whose pain did not settlewith a single dose of parenteral opioidanalgesia. Twenty five (22%) had ele-vated cTnI levels, ranging from 1.0 to34.0 �g/L (reference range, < 0.7 �g/L). None of these patients had clinicalor chest x-ray findings of pulmonaryoedema. Eleven patients had non-spe-cific electrocardiogram (ECG) abnor-malit ies, most involving T-waveinversion and ST-segment depression.Echocardiograms were performed in 18of the 25 patients with elevated cTnIlevels, and abnormalities were found insix. Echocardiographic abnormalitiesranged from mild impairment of systolicfunction to moderate dysfunction withsegmental hypokinesis. One patient hadglobal myocardial dysfunction. Twopatients had serial echocardiographicstudies showing normalisation of theirsystolic function over time (one withinthree months and the other over sixmonths).
Among the 91 remaining patientsonly one had an abnormal ECG. Hewas a previously well 33-year-old manwho developed paroxysmal atrial fibril-lation (which resolved spontaneouslyover several hours); his echocardiogramwas normal.
Hospital admissions
Average length of admission was 1.6days and the longest was five days.
Forty-two patients (36%) were dis-charged home directly from the emer-gency department within eight hours ofpresentation. Fifty-four patients (47%)were discharged from the emergencydepartment observation ward the nextday, eight were transferred to the coro-nary care unit (CCU), and 11 weretransferred to the general medical orpaediatric ward for ongoing analgesia.Additionally, one patient was trans-ferred to the intensive care unit inTownsville General Hospital for neuro-surgical care for an intracerebral haem-orrhage.
Skin scrapings
Skin scrapings were taken from 50patients. Of these, four patients hadlocal symptoms only, and the remainderhad symptoms consistent with Irukandjisyndrome. Forty patients (80%) hadpositive scrapings, while, in the remain-der, either no nematocysts were foundor the nematocysts were too damaged tobe confidently identified (positive pre-dictive value of 80%). Thirty-ninepatients had a nematocyst cnidomeidentifiable as Carukia barnesi; two ofthese experienced only a mild sting atthe site, and 37 had Irukandji syn-drome. Of these 39 patients, 13 had araised cTnI level; five of these hadabnormal echocardiograms and sevenhad abnormal ECGs. Thirty-onepatients with Carukia barnesi identifiedon skin scrapings (79%) were stung atlocal mainland beaches. The rest werestung at Fitzroy Island (4), Green Island(1), and Normanby Island (1) (see Box1).
The patient with the most severesymptoms who had Carukia barnesiidentified from skin scrapings was a 44-year-old man with a peak blood pres-sure of 160/100 mmHg and peak cTnIlevel of 30.8 �g/L, who required a totalmorphine equivalent dose of 255 mgover five days. He had widespread T-wave inversion and ST-segment depres-sion on his ECG. His echocardiogramshowed severe left ventricular dysfunc-tion and anteroseptal hypokinesis, withan ejection fraction of 30%–35%. Sixmonths later his echocardiogram wascompletely normal.
One 44-year-old man had an uniden-tified cnidome on skin scraping, which
1: Map showing the coastline, islands and reef where patients were stung
Cape Tribulation
Opal Reef
Port Douglas
Fitzroy Island
Green island
Normanby Island
Palm Cove
Cairns
16
17
147
Queensland
Great
Barrier
Reef
N

40 MJA Vol 178 6 January 2003
BITES AND STINGS
is of concern, as he was one of twopatients reported to have died fromIrukandji syndrome (the other havingoccurred in the Whitsundays).9
Although some of the nematocysts iden-tified were similar to those from Carukiabarnesi, a morphologically differentadditional nematocyst was also present(Box 2). It is possible that this nemato-cyst was a “rogue” mastigmophore, andhence may be an incidental finding fromanother source. Alternatively, the cnid-ome may represent an unidentified jelly-fish. The patient was stung at Opal Reef(see Box 1), had a peak blood pressureof 230/90 mmHg, peak cTnI level of34 �g/L, and required 30mg of mor-phine equivalents before being intu-bated for a depressed level of con-sciousness from an intracerebral haem-orrhage.
DISCUSSION
In recent years a number of seriousenvenomations causing Irukandji syn-drome have been described,6,10-13 all
associated with cardiac failure and pul-monary oedema. However, it has beenobserved that most stings in the Cairnsregion are, in fact, mild, without seriouscomplications, and do not requireadmission to hospital.4 Our study con-firms this, as most patients were dis-charged within 24 hours of presentation.
Surprisingly, myocardial damage, asmeasured by an elevated cTnI level, wasseen in 25 patients (22%) experiencingIrukandji syndrome. Six of thesepatients had echocardiographic evi-dence of myocardial dysfunction. It isevident that those with continuing painand analgesic requirements are at risk ofcardiac complications. Cliniciansshould therefore consider closely moni-toring these patients with serial cTnIlevel measurements, and, if these areabnormal, consider echocardiographicevaluation.
Skin-scraping methods have beendescribed for a number of jellyfish spe-cies,14-17 but, to date, there are no pub-lished data on successful identificationof Carukia barnesi nematocysts inpatients with Irukandji syndrome.
While acknowledging some limitations,it is reasonable in this setting to equatethe species identified through cnidomeassessment with causation. Therefore,we can, with reasonable confidence,assert that Carukia barnesi was causativein 39 patients. We can also deduce thatenvenomation by this species producesa wide range in severity of illness, andthat it was the only identifiable causativecuboidal jellyfish in patients stung onthe Cairns beaches. We can less confi-dently claim that a single victim mayhave been stung by an unknown speciesof box jellyfish, ultimately leading to hisdeath. The cnidome in this case wassimilar to, but with distinct differencesfrom that of, Carukia barnesi (Box 2).We acknowledge that Carukia barnesimay have been causative in thisinstance, as the mastigophore isolatedfrom this patient may have been anincidental finding. A further possibilityis that the Carukia barnesi cnidome maychange to include mastigophores as theanimal ages or grows (as is seen withChironex fleckeri). We are ignorant of thelife cycle of Carukia barnesi, and there-fore can only speculate.
There are obvious serious implica-tions if the cnidome is that of an uni-dentified cuboidal jellyfish. It has longbeen suspected that jellyfish speciesother than Carukia barnesi can causeIrukandji syndrome.3-7 Case reportsinclude a patient with severe Irukandjisyndrome in whom a 2 mm length oftentacle not from Carukia barnesi wasfound in a skin scraping of the stingsite,6 and where tentacles isolatedresembled, but were distinctly differentfrom, those of Carukia barnesi.7 Ourresults provide further supportive evi-dence that species other than Carukiabarnesi may be linked to Irukandji syn-drome.
Interestingly, two patients with cnid-omes consistent with Carukia barnesidid not develop Irukandji syndrome.These patients had mild local symptomsonly. Thus, a sting by Carukia barnesidoes not necessarily result in Irukandjisyndrome. Factors affecting venomload, such as thickness of the kera-tinised skin, presence of hair, length oftentacle involved, duration and pressureof the contact between tentacle and skinhave been p roposed by o the rauthors.3,17
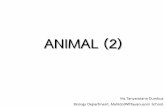
2: Nematocysts from Carukia barnesi compared with unidentified nematocysts from a fatal envenomation
A: Discharged nematocyst from the tentacle of Carukia barnesi.
B: Discharged nematocyst from the bell of Carukia barnesi.
C: Discharged nematocyst from unidentified species of jellyfish (similar morphology to [A]).
D: Cigar-shaped nematocyst from unidentified species of jellyfish.

MJA Vol 178 6 January 2003 41
BITES AND STINGS
As only a single cnidome suggestive ofa different jellyfish species was found,we can make no statistical inferencesabout the severity of Irukandji syn-drome and the jellyfish species identi-fied from skin scrapings. Additionally,patients were not randomly selected interms of whether or not they would haveskin scrapings performed. Thus, it ispossible that more seriously affectedpatients would have attracted moreinterest and were more likely to haveskin scrapings performed.
Our interpretation of these findings isbased on a number of assumptions. Ourconversion of “equivalent doses” of nar-cotics has not taken into account thedifferences in their duration of action.Finally, we have assumed that jellyfish(indicated by their cnidome) caused thepatients’ symptoms.
In conclusion, we can infer that, inpatients with Irukandji syndrome, thecausative jellyfish can usually be suc-cessfully identified from skin scrapingson the basis of known cnidomes. Mostpatients with Irukandji syndrome in theCairns region were stung by Carukiabarnesi, which has now been shown to
cause illness ranging from local symp-toms to severe Irukandji syndrome withcardiac dysfunction. Our finding of acnidome that was not that of Carukiabarnesi suggests that other species ofjellyfish may cause Irukandji syndrome.
COMPETING INTERESTS
None identified
REFERENCES
1. Southcott RV. Fatal stings in North Queenslandbathers. Med J Aust 1952; 1: 272-273.
2. Flecker H. Irukandji sting to North Queensland bath-ers without production of wheals but severe generalsymptoms. Med J Aust 1952; 2: 89-91.
3. Barnes JH. Cause and effect in Irukandji stingings.Med J Aust 1964; 1: 897-904.
4. Little M, Mulcahy RF. A year's experience of Irukandjienvenomation in far north Queensland. Med J Aust1998; 169: 638-641.
5. Fenner P, Carney I. The Irukandji syndrome. Adevastating syndrome caused by a north Australianjellyfish. Aust Fam Physician 1999; 28: 1131-1137.
6. Little M, Mulcahy RF, Wenck DJ. Life-threateningcardiac failure in a healthy young female with Iru-kandji syndrome. Anaesth Intensive Care 2001; 29:178-180.
7. Taylor D, Pereira P, Seymour J, Winkel K. A stingfrom an unknown jellyfish species associated withpersistent symptoms and raised troponin I levels.Emerg. Med 2002; 14: 175-180.
8. National Centre for Classification in Health – ICD-10–Australian Modification. Sydney, NCCH Publishers,Shannon Books, 2002.
9. Fenner PJ, Hadok JC. Fatal envenomation by jelly-fish causing Irukandji syndrome. Med J Aust 2002;177: 362-363.
10. Fenner PJ, Burnett JW, Colquhoun DM, et al. The“Irukandji Syndrome” and acute pulmonary oedema.Med J Aust 1988; 149: 150-156.
11. Herceg I. Pulmonary oedema following an Irukandjisting. SPUMS J (South Pacific Underwater MedicineSociety Journal) 1987; 17: 95-97.
12. Martin JC, Audley I. Cardiac failure following Iru-kandji envenomation. Med J Aust 1990; 153: 164-166.
13. Fenner PJ, Williamson J, Callanan VI, Audley I.Further understandings of and a new treatment for“Irukandji” (Carukia barnesi) stings. Med J Aust1986; 145: 569-574.
14. Barnes JH. Observations on jellyfish stingings inNorth Queensland. Med J Aust 1960; 2: 993-999.
15. Currie BJ, Wood YK. Identification of Chironex fleck-eri envenomation by nematocyst recovery from skin.Med J Aust 1995; 162: 478-480.
16. Fenner PJ, Fitzpatrick PF, Hartwick RJ, Skinner R.“Morbakka”, another cubomedusan. Med J Aust1985; 143: 550-555.
17. Lumley J, Williamson A, Fenner PJ, et al. Fatalenvenomation by Chironex fleckeri, the north Aus-tralian jellyfish: the continuing search for lethalmechanisms. Med J Aust 1988; 148: 527-534.
(Received 23 Sep 2002, accepted 1 Nov 2002) ❏
Stoking the fires of drug controversyModernising Australia’s drug policy. Alex D Wodak and Timothy Moore. Sydney: UNSW Press, 2002 (103pp, $19.95). ISBN 0 86840 482 9.
THE DISCUSSION OF ILLICIT drugs policyis littered with controversy, stoked by strongfeelings on both sides and full of assertionsthat fundamental morality is at stake. Thosewho support prohibition and have a clear
view of law enforcement as the answer neednot read this book, as they will find little to relate to.
The authors have a long record of challenging thecurrent international philosophy of prohibition, stemmingas it does from the muscular nationalism of Teddy Roo-sevelt, who convened the Shanghai Conference in 1909.That policy has been honed and developed with USleadership in successive international treaties of 1912,1926, 1961, 1971 and 1988. Richard Nixon’s invention ofthe politically potent “War on Drugs” in 1972 is givenattention in its Australian incarnation “Tough on Drugs”.The book is readable, rather than scholarly, and tells of thefolly of this ideological commitment in terms of failed
outcomes. Its assertions are not referenced, but theauthors speak from a position of authority after years ofcontributing to the debate. It is an easy read.
The book urges the separation of cannabis markets fromheroin and cocaine, but is critical of half-hearted decrimi-nalisation when legalisation, with regulation, taxation andhealth advice about cannabis, would be far more appropri-ate. The rationale is compelling. It argues clearly that themajor problems for society from illicit drugs — crime,corruption, disease and overdose deaths — are primarilythe consequences of prohibition rather than the drugs.
Misleading advocacy and misuse of naltrexone are welldiscussed. There is little coverage of cocaine and ampheta-mines. Although occasionally repetitive, it is worthwhilereading for all concerned citizens, including politicians,medical practitioners and parents. It is good value as apaperback entry to a difficult area of public policy.
David G PeningtonEmeritus Professor, and Past Chairman
Victorian Premier's Drug Advisory CouncilMelbourne, VIC
book review