Severe Sepsis And Septic Shock
59
-
Upload
society-of-thai-emergency-physicians -
Category
Health & Medicine
-
view
11.826 -
download
7
Transcript of Severe Sepsis And Septic Shock


Incidence of sepsis has risen dramatically increase in the number of invasive procedures
immunosuppressive therapy
advancing age of population
In United States approximately 750,000 cases/year and the frequency is increasing
At least 225,000 are fatal.
N Engl J Med 2003;348:1546-54.
Septic shock and multiorgan dysfunction are the most common causes of death in patients with sepsis.
The mortality rate severe sepsis 25 - 30%1
septic shock 40 - 70%2
The number of sepsis cases is projected to grow at a rate of 1.5% per year, making a total of nearly 18 million new cases to occur worldwide each year.
1.N Engl J Med 2001;344:699-709.2.Am J Respir Crit Care Med 2003;168:165-72.

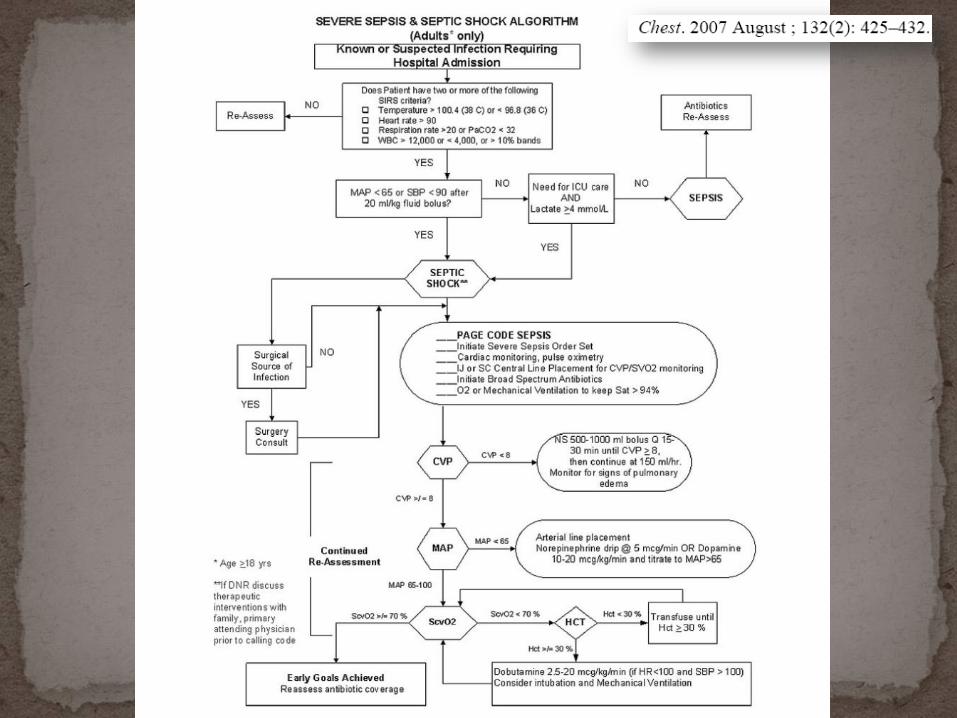
1. Systemic Inflammatory Response Syndrome (SIRS)
Two or more of the following
- BT > 38 c or < 36 c
- Heart rate > 90 beats/min
- Respiratory Rate > 20 breaths per min or PaCO2 < 32 mmHg
- White Cell Count > 12,ooo cells/mm3 , < 4,000 cells/mm3 or > 10% immature forms
2. Sepsis
SIRS resulting from documented infection.
Crit care Med 1992;20:864-874

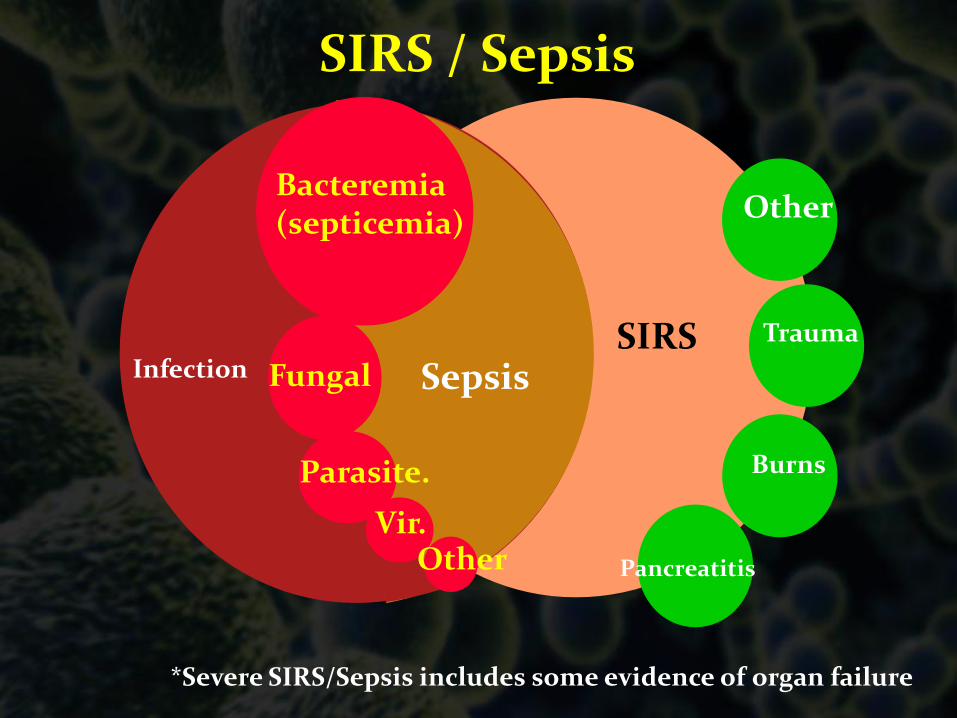
*Severe SIRS/Sepsis includes some evidence of organ failure
SIRS / Sepsis
SIRSInfection
Other
Trauma
Burns
Pancreatitis
Bacteremia(septicemia)
Fungal
Parasite.
OtherVir.
Sepsis

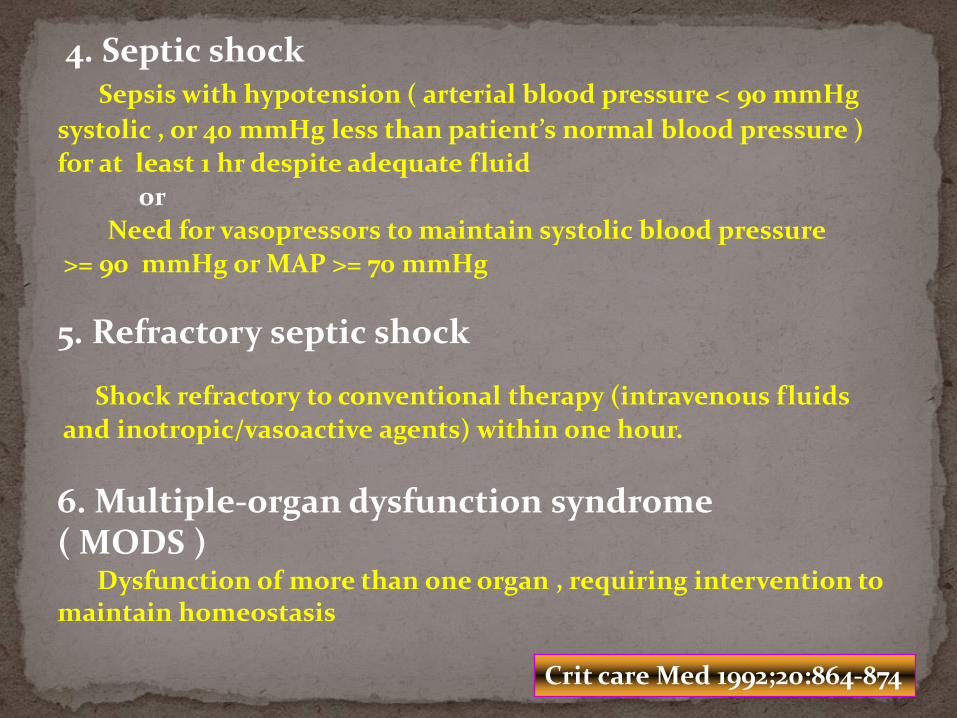
4. Septic shockSepsis with hypotension ( arterial blood pressure < 90 mmHg
systolic , or 40 mmHg less than patient’s normal blood pressure )
for at least 1 hr despite adequate fluid
or
Need for vasopressors to maintain systolic blood pressure
>= 90 mmHg or MAP >= 70 mmHg
5. Refractory septic shock
Shock refractory to conventional therapy (intravenous fluids
and inotropic/vasoactive agents) within one hour.
6. Multiple-organ dysfunction syndrome ( MODS )
Dysfunction of more than one organ , requiring intervention to maintain homeostasis
Crit care Med 1992;20:864-874

*Severe SIRS/Sepsis includes some evidence of organ failure
SIRS / Sepsis
SIRSInfection
Other
Trauma
Burns
Pancreatitis
Bacteremia(septicemia)
Fungal
Parasite.
OtherVir.
SepsisSevere
sepsis/MODS
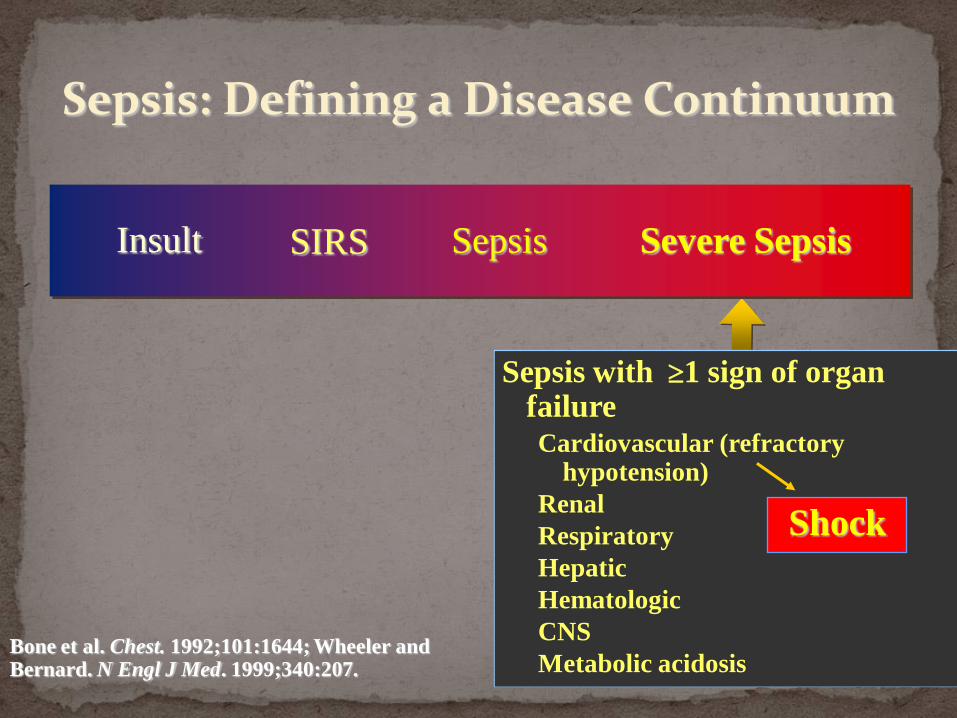
Sepsis: Defining a Disease Continuum
Bone et al. Chest. 1992;101:1644; Wheeler and Bernard. N Engl J Med. 1999;340:207.
SepsisSIRSInsult Severe Sepsis
Sepsis with 1 sign of organ failureCardiovascular (refractory
hypotension)
Renal
Respiratory
Hepatic
Hematologic
CNS
Metabolic acidosis
Shock

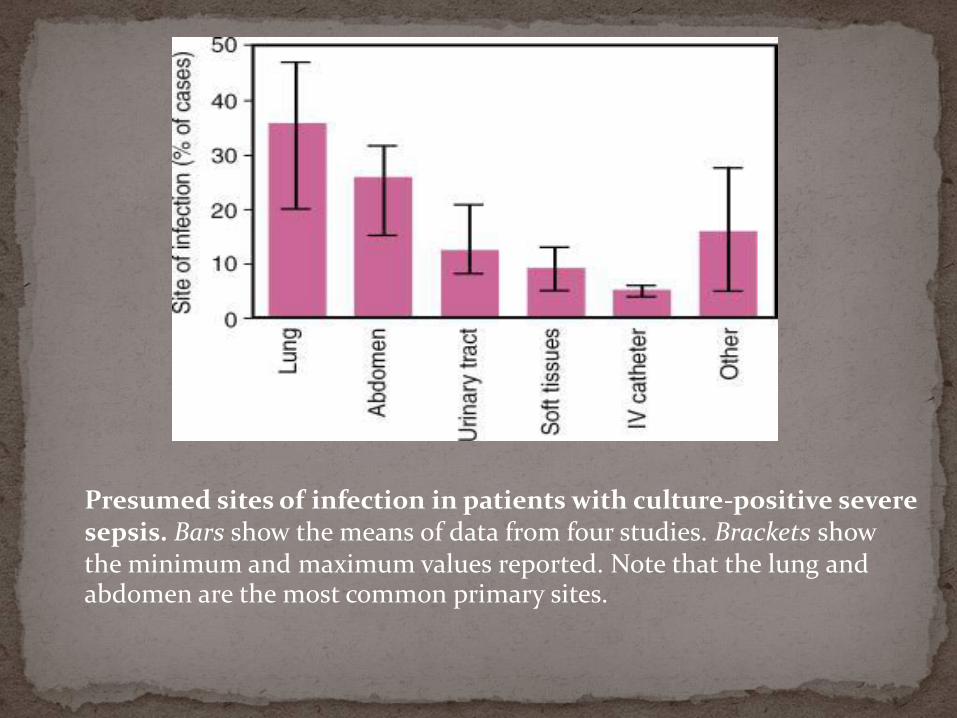
Presumed sites of infection in patients with culture-positive severe sepsis. Bars show the means of data from four studies. Brackets show the minimum and maximum values reported. Note that the lung and abdomen are the most common primary sites.



TLR = toll-like receptors; NF-κB = cytosolic nuclear factor κB; TNF-α = tumornecrosis factor α; iNOS = inducible nitric oxide synthase.

TNF-α and interleukin-1β are proinflammatory cytokines that activate the adaptive immune response but also cause both direct and indirect host injury.
Interleukin-10 is an antiinflammatory cytokine that inactivates macrophages and has other antiinflammatoryeffects.
Proteases, oxidants, prostaglandins, and leukotrienesinjure endothelial cells, leading to increased permeability, further vasodilation, and alteration of the procoagulant–anticoagulant balance.
Cytokines also activate the coagulation cascade.
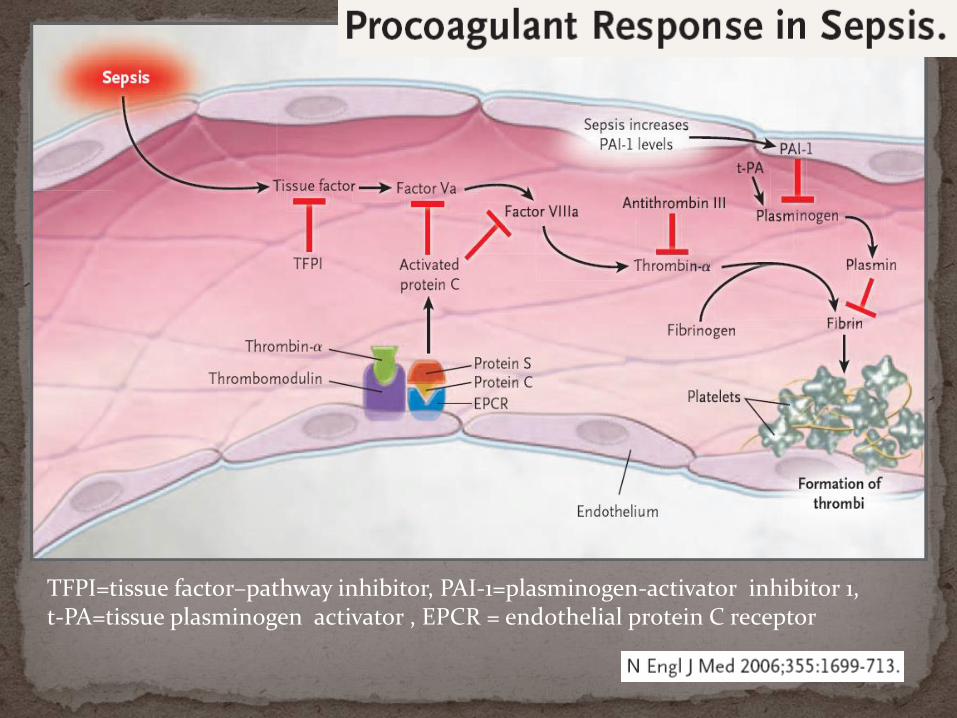
TFPI=tissue factor–pathway inhibitor, PAI-1=plasminogen-activator inhibitor 1, t-PA=tissue plasminogen activator , EPCR = endothelial protein C receptor

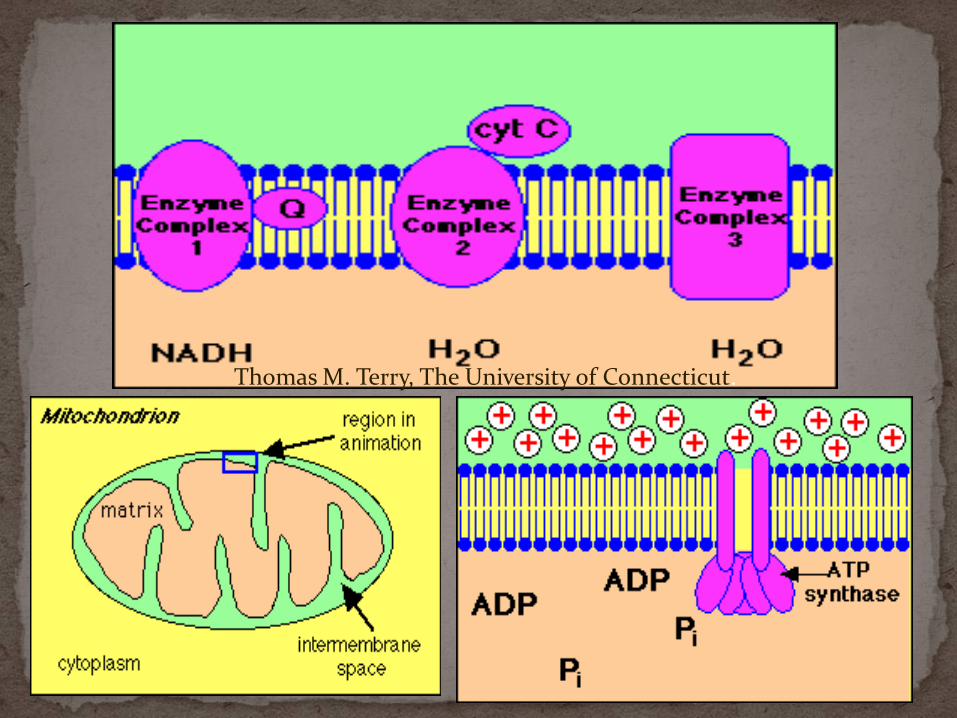
Thomas M. Terry, The University of Connecticut.

Sepsis Resuscitation BundleSepsis Management Bundle

Sepsis Resuscitation Bundle:
1. Serum lactate measured
2. Blood cultures obtained prior to antibiotic administration
3. From the time of presentation, broad-spectrum antibiotics administered within 3 hours for ED admissions and 1 hour for non-ED ICU admissions
4. In the event of hypotension and/or lactate > 4 mmol/L (36 mg/dl): Deliver an initial minimum of 20 ml/kg of crystalloid (or colloid equivalent)
Apply vasopressors for hypotension not responding to initial fluid resuscitation to maintain mean arterial pressure (MAP) > 65 mm Hg
5. In the event of persistent hypotension despite fluid resuscitation (septic shock) and/or lactate > 4 mmol/L (36 mg/dl):
Achieve central venous pressure (CVP) of > 8 mm Hg
Achieve central venous oxygen saturation (ScvO2) of > 70%
www.ihi.org/IHI/Topics/CriticalCare/Sepsis
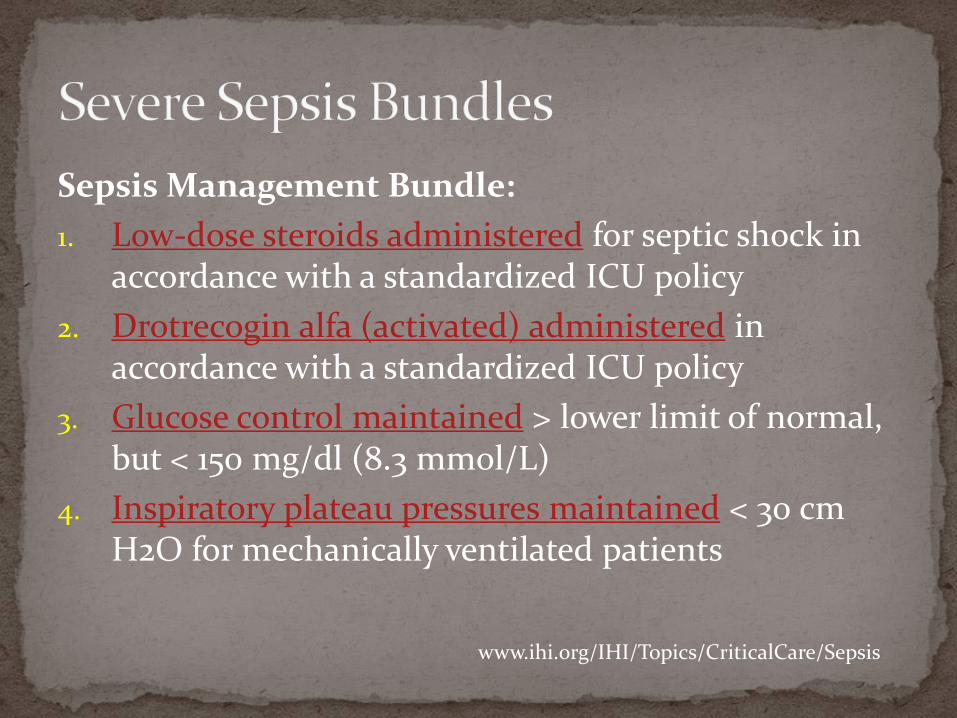
Sepsis Management Bundle:
1. Low-dose steroids administered for septic shock in accordance with a standardized ICU policy
2. Drotrecogin alfa (activated) administered in accordance with a standardized ICU policy
3. Glucose control maintained > lower limit of normal, but < 150 mg/dl (8.3 mmol/L)
4. Inspiratory plateau pressures maintained < 30 cm H2O for mechanically ventilated patients
www.ihi.org/IHI/Topics/CriticalCare/Sepsis

Secondary to anaerobic metabolism due to hypoperfusion.
Limitations:
Elevated lactate levels can also result from decreased clearance by the liver.
www.ihi.org/IHI/Topics/CriticalCare/Sepsis/Changes/IndividualChanges/SerumLactateMeasured.htm

Implications:
Given the high risk for septic shock, all patients with lactate > 4 mmol/L (36 mg/dl) will enter the early goal-directed therapy portion of the Severe Sepsis Resuscitation Bundle, regardless of blood pressure.
www.survivingsepsis.org/Bundles/Individual_Changes/Pages/serum_lactate.aspx

Turnaround Time
Serum lactate must be available in your institution with rapid turnaround time (within minutes) to effectively treat severely septic patients.
An arterial blood gas analyzer located in the clinical laboratories usually accomplishes this.
www.survivingsepsis.org/Bundles/Individual_Changes/Pages/serum_lactate.aspx
Tips If not rapidly available in your institution, invest in
equipment to make rapid assessment possible.
This should be presented to hospital and laboratory administration as a present standard of care.
Create a standardized protocol to manage severe sepsis that includes measurement of serum lactate.
Attach a lactate blood tube to blood culture tubes to increase the number of patients that are screened.
www.survivingsepsis.org/Bundles/Individual_Changes/Pages/serum_lactate.aspx

: Indicates a strong recommendation or “we recommend” : Indicates a weak recommendation or “we suggest”

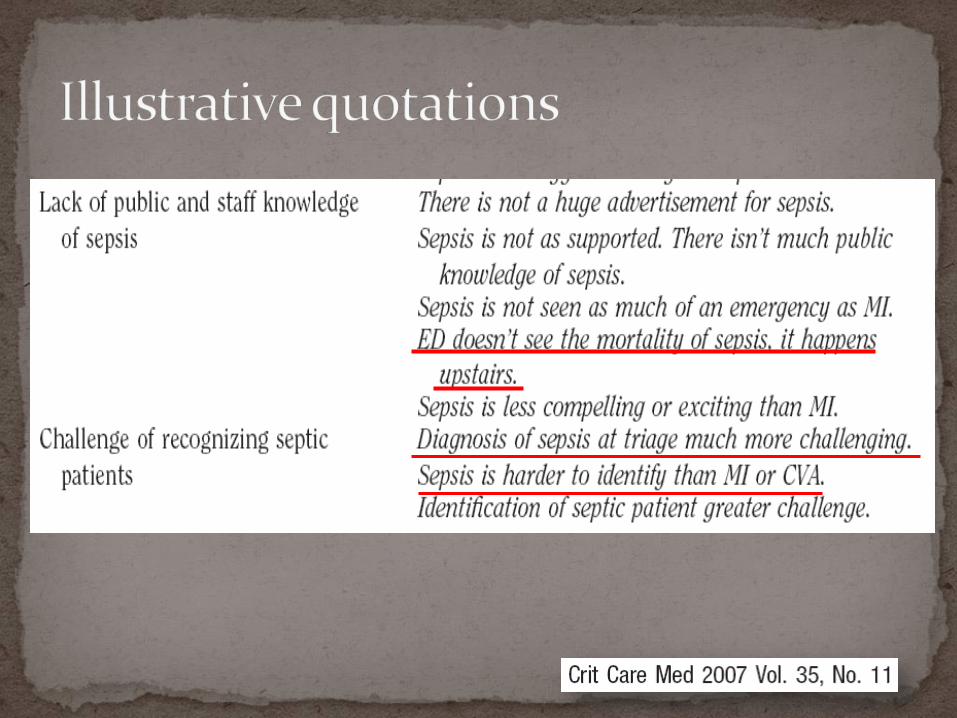
The Problem Inconsistency in the early diagnosis of severe sepsis and
septic shock Frequent inadequate volume resuscitation without defined
endpoints Late or inadequate use of antibiotics Frequent failure to support the cardiac output when
depressed Frequent failure to control hyperglycemia adequately Frequent failure to use low tidal volumes and pressures in
acute lung injury Frequent failure to treat adrenal inadequacy in refractory
shock
Begin resuscitation immediately in patients with hypotension or elevated serum lactate ≥ 4mmol/L; do not delay pending ICU admission. (1C)
Resuscitation goals: (1C)
• Central venous pressure (CVP) 8–12 mm Hg*• Mean arterial pressure ≥ 65 mm Hg• Urine output ≥ 0.5 mL.kg-1.hr-1• Central venous (superior vena cava) oxygen saturation(ScVO2) ≥
70%,or mixed venous (SvO2)≥ 65%
If venous O2 saturation target not achieved: (2C)
• Consider further fluid• Transfuse packed red blood cells if required to hematocrit of ≥ 30%and/or• Dobutamine infusion max 20 μg.kg-1.min-1
* A higher target CVP of 12-15 mmHg is recommended in the presence of mechanical ventilation or pre-existing decreased ventricular compliance.
Obtain appropriate cultures before starting antibiotics provided this does not significantly delay antimicrobial administration.(1C)
• Obtain two or more blood cultures (BCs)
• One or more BCs should be percutaneous
• One BC from each vascular access device in place >48 hours
• Culture other sites as clinically indicated
Perform imaging studies promptly in order to confirm and sample any source of infection (1C)

If the same organism is recovered from both cultures, the likelihood that the organism is causing the severe sepsis is enhanced.
If the culture drawn through the vascular access device is positive > 2 hours earlier than the peripheral blood culture, it may offer support that the vascular access device is the source of the infection.

Indications:
Fever
Chills
Hypothermia
Leukocytosis
Left shift of neutrophils
Neutropenia
Unexplained organ dysfunction, e.g., renal failure or signs of hemodynamic compromise.
Blood cultures should be taken as soon as possible after the onset of fever or chills.

Begin intravenous antibiotics as early as possible, and always within the first hour of recognizing severe sepsis (1D) and septic shock. (1B)
Broad-spectrum: one or more agents active against likely bacterial/fungal pathogens and with good penetration into presumed source. (1B)
Consider combination therapy in Pseudomonas infections. (2D)
Consider combination empiric therapy in neutropenic patients. (2D)

Harbarth S. Am J Med 2003;115(7):529–35 Inappropriate initial antibiotic therapy was associated
with excess mortality (OR 1.8)
Leibovici L. J Intern Med 1998;244:379–86.
Appropriate empiric antibiotic treatment resulted in a decrease in mortality from 34% 20%.
Fatality with inappropriate antibiotics and septic shock OR 1.6

Reassess antimicrobial regimen daily to optimize efficacy, prevent resistance, avoid toxicity, & minimize costs. (1C)
Combination therapy no more than 3-5 days and de-escalation following susceptibilities. (2D)
Duration of therapy typically limited to 7–10 days; longer if response slow, undrainable foci of infection, or immunologic deficiencies. (1D)
Stop antimicrobial therapy if cause is found to be non-infectious. (1D)
A specific anatomic site of infection should be established as rapidly as possible (1C) and within the first 6 hours of presentation. (1D)
Implement source control measures as soon as possible following successful initial resuscitation. (1C)
Exception: infected pancreatic necrosis, where surgical intervention best delayed. (2B)
Choose source control measure with maximum efficacy and minimal physiologic upset. (1D)
Remove intravascular access devices if potentially infected. (1C)
Fluid-resuscitate using crystalloids or colloids. (1B)
Target a CVP of ≥ 8mmHg (≥12mmHg if mechanically ventilated). (1C)
Use a fluid challenge technique while associated with a hemodynamic improvement. (1D)
Give fluid challenges of 1000 mL of crystalloids or 300–500 mL of colloids over 30 minutes. More rapid and larger volumes may be required in sepsis-induced tissue hypoperfusion. (1D)
Rate of fluid administration should be reduced if cardiac filling pressures increase without concurrent hemodynamic improvement. (1D)
Administration of 20 ml/kg of crystalloid as a fluid challenge in cases of suspected hypovolemia or serum lactate greater > 4 mmol/L (36 g/dl).
A colloid equivalent is an acceptable alternative to crystalloid, and an equivalent dose generally ranges from 0.2 g/kg to 0.3 g/kg depending upon the colloid.
The Saline vs. Albumin Fluid Evaluation (SAFE) study has been completed, having enrolled 7,000 patients.
The results of this study showed identical mortality rate in patients receiving albumin or 0.9% sodium chloride.
NEJM. 2004;350:2247–56.

Maintain MAP ≥ 65mmHg. (1C)Norepinephrine or dopamine centrally administered
are the initial vasopressors of choice. (1C) Epinephrine, phenylephrine, or vasopressin should
not be administered as the initial vasopressor in septic shock. (2C)
Use epinephrine as the first alternative agent in septic shock when blood pressure is poorly responsive to norepinephrine or dopamine. (2B)
Do not use low-dose dopamine for renal protection. (1A)
In patients requiring vasopressors, insert an arterial catheter as soon as practical. (1D)
Physiologic goal-directed resuscitation in sepsis Discussed and debated extensively in critical care
Only a randomized clinical trial has been able to show a survival benefit from a specific protocol.
Outcome before and after systematic initiation of this protocol have supported this observation.


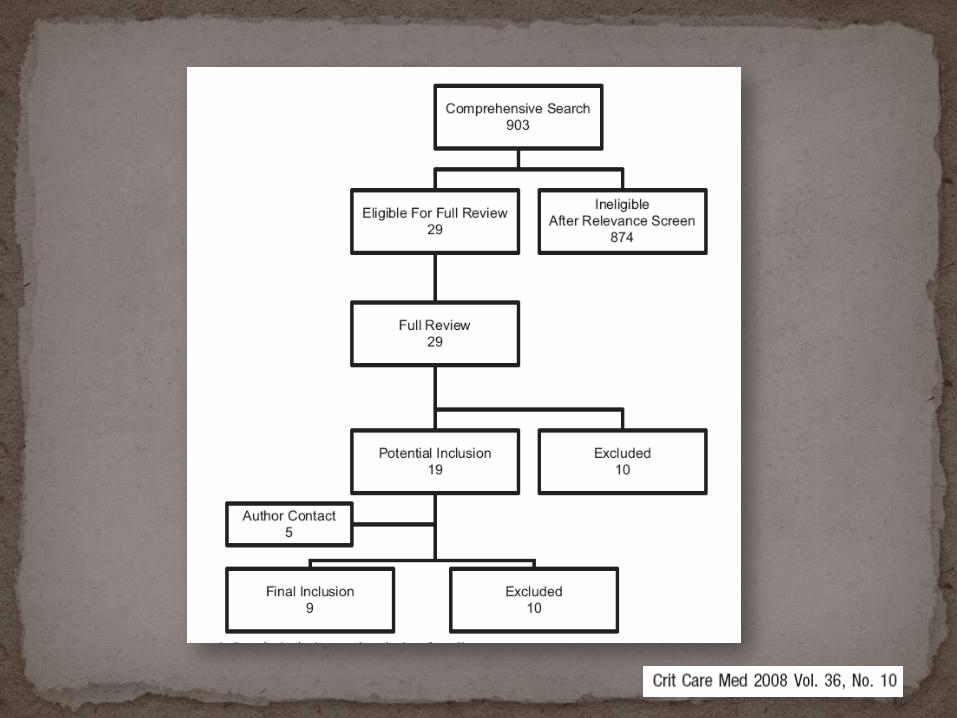
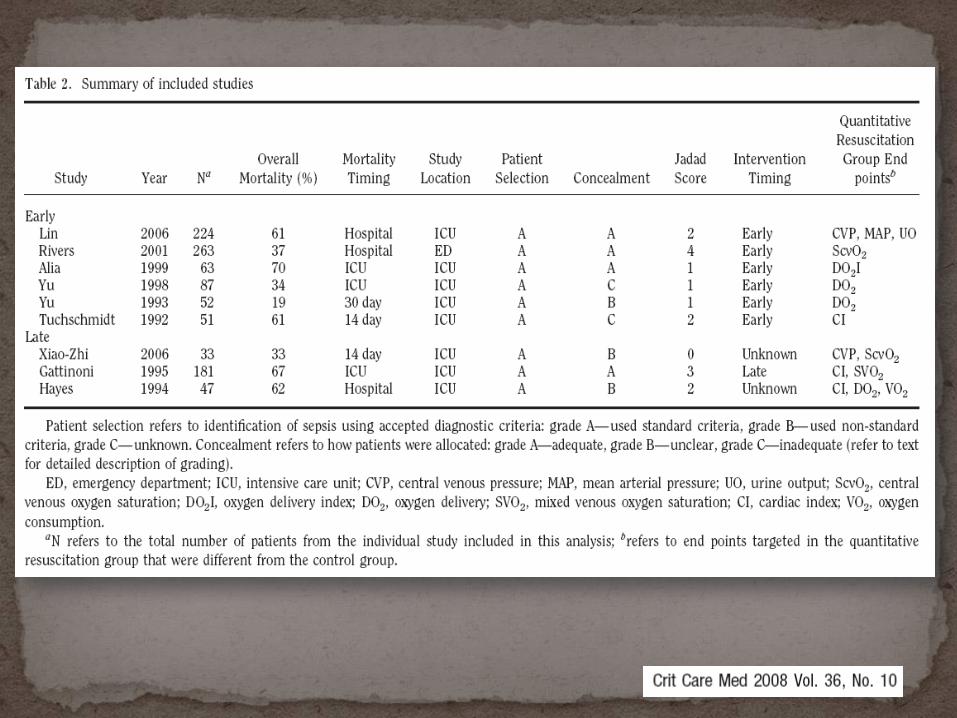
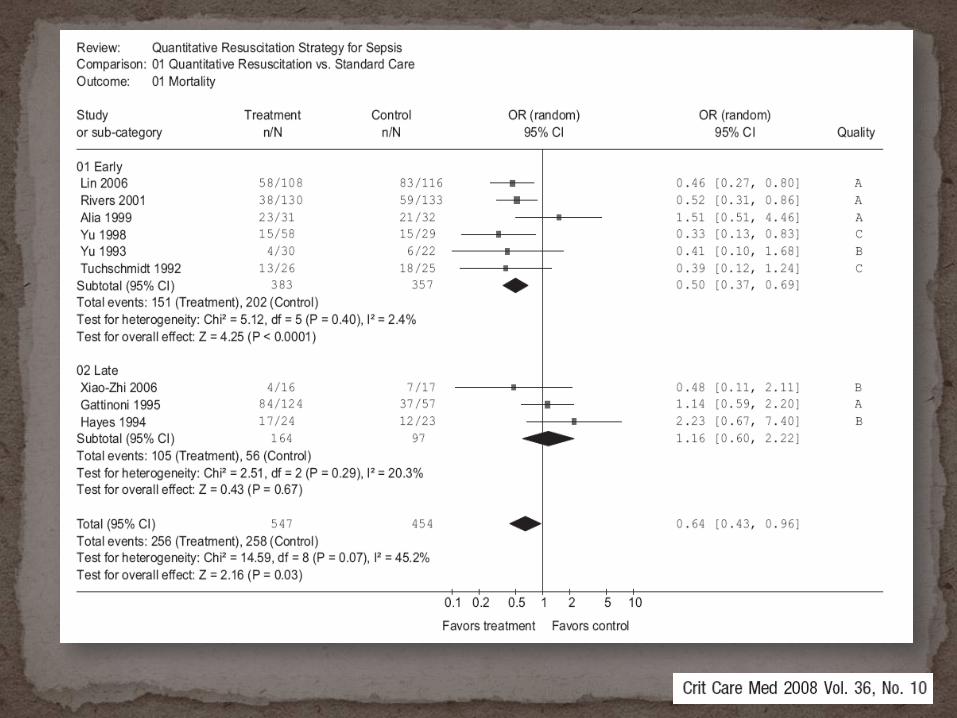
Data synthesized from nine randomized controlled trials demonstrate a clear survival benefit afforded by quantitative resuscitation to treat sepsis at or near the time of recognition.
Our results provide the strongest support to date for the Surviving Sepsis Campaign recommendation of providing quantitative resuscitation at the time of severe sepsis recognition