
Severe patellofemoral arthritis
23
1 Severe patellofemoral arthritis secondary to patellofemoral malalignment treated by Fulkerson osteotomy plus tricortical bone graft. A retrospective cohort of 45 knees. Autors: Dr. Edgar William Afanador Acuña * E-mail: [email protected] Dr. Francisco Javier Sánchez Villa ** E-mail: [email protected] * Ortopedista y Traumatólogo, Cirugía de Rodilla, Hospital Militar Central - Clínica Universitaria Colombia ** Residente de IV nivel de Ortopedia y Traumatología, Hospital Militar Central, Universidad Militar Nueva Granada.
-
Upload
felipe-afanador-cortes -
Category
Health & Medicine
-
view
744 -
download
0
Transcript of Severe patellofemoral arthritis

1
Severe patellofemoral arthritis secondary to patellofemoral malalignment treated by Fulkerson osteotomy plus tricortical
bone graft. A retrospective cohort of 45 knees.
Autors: Dr. Edgar William Afanador Acuña *
E-mail: [email protected]
Dr. Francisco Javier Sánchez Villa ** E-mail: [email protected]
* Ortopedista y Traumatólogo, Cirugía de Rodilla, Hospital Militar Central - Clínica Universitaria Colombia
** Residente de IV nivel de Ortopedia y Traumatología, Hospital Militar Central, Universidad Militar Nueva Granada.
2
ABSTRACT
Background: The surgical treatment options in severe patellofemoral arthritis secondary to patellofemoral malalignment are limited. The majority of the surgical procedures include distal patellar realignment through different types of tibial tuberosity osteotomies, current evidence reports different results. Aim: evaluate the functionality and the level of pain in a cohort of patients with patellofemoral arthritis secondary to patellofemoral malalignment treated by Fulkerson osteotomy plus tricortical bone graft between 2001 y 2011. Methods: We conducted a retrospective cohort study of patients with severe patellofemoral arthritis secondary to patellofemoral malalignment treated by Fulkerson osteotomy plus tricortical bone graft between 2001 and 2011. The results were evaluated using the Lysholm scale modified by Fulkerson and the VAS score. A mean follow-up of44.0± 26.8 months, range 2-11.9 years. Results:A total of 38patients (45 knees, 7 bilateral) were treated using the technique described, 35 women (92.1%). An average age of 44.7±10.9 years (range between 23 and 62 years). All of the patients showed an improvement in the VAS score. The results of the functional scales were 93.3% excellent and good results. During follow up we do not report deterioration. We do not report major complications. Conclusions: Fulkerson osteotomy plus tricortical bone graft is an adequate treatment in functionality and decreased pain severity in the short term in patients with patellofemoral arthritis secondary to patellofemoral malalignment.
Key words: patellofemoral arthritis, patellofemoral malaligment, Fulkerson osteotomy, bone graft,
Level of evidence: IV
3
INTRODUCTION
Severe patellofemoral arthritis secondary to patellofemoral malaligment results in great
and progresive impairment in the quality of life and productivity of the patients affected
by this condition. (1, 2). The non surgical options available are ineffective. The surgical
options are limited, require prolonged periods of rest and the results are variable. (3–7).
The most frequently used surgical procedures have in common a distal patellar
realigment through the different type of osteotomies of the tibial tubercle with either
medialization or anteriorization. (3,4,8) (Figures 1 and 2). The elevation of the tibial
tubercle proposed by Bandi and Maquet increases the efficacy of the Quadriceps
augmenting the lever arm while decreasing the reaction force of the patellofemoral joint
(3). Maquet concludes that there is a 50% reduction in the compresive forces at the
patellofemoral joint after a 2 cm anteriorization of the tibial tubercle. This hypothesis
has been confirmed by Ferguson and Brown (9), they proved that anteriorizations of 1,2
cms, 2,5 cms and 3,7 cms resulted in great relieve of the tension. They reported a 57%
relieve with 1,2 cms. Anteriorizations of 2,5 cms and 3,7 cms resulted in relieves of
30% and 9% respectively. These authors concluded that the main benefit is obtained
with the first 1,2cms of anteriorization and that from this point forward the
complications increased while no benefit was obtained. One of the causes of
complications, mainly in the skin, is the use of bone grafts of great size. (10).

4
Figura 1: Transverse osteotomy of the tibial tubercle (Elmslie-Trillat) where there is only medialization, anteriorization is obtained with the adition of a bone graft. ( Maquet effect).
In the Fulkerson osteotomy, the degree of inclination of the osteotomy determines the
final medialization and anteriorization. (Figura 2). The greater the degree of inclination
the greater the anteriorization is attained but also the lesser medialization results.
(5,8,11).
A B
Figura 2: (A) Fulkerson osteotomy at 30 degrees of inclination, results in greater medialization. (B) Fulkerson osteotomy at 45 degrees of inclination, results in greater anteriorization. From David A Buuck. 2000(5)DAVID A. BUUCK

5
For the younger patients with severe patellofemoral arthrosis in which whom
arthroplasty is not convenient, is necessary to find surgical options that are capable of
retain a functional knee.
Fulkerson described a modification to his technique, an oblique osteotomy with the
addition of a bone graft to optimize the anteriorization effect. (12,13). (Figure3).
Figura 3. Fulkerson osteotomy at 45 degrees plus bone graft at the site of osteotomy. A. Original position of the osteotomy. B. Position after the osteotomy. C. Position with the addition of a bone graft. From Fulkerson. 1994(12).
Taking these biomechanical principles into account, since 2001, at the Hospital Militar
Central and in the Clinica Universitaria Colombia, one of the authors (E. Afanador) has
implemented a Fulkerson osteotomy plus tricortical bone graft to patients with
patellofemoral malaligment and severe ( Outerbridge grade IV) patellofemoral
arthrosis. (14), choosing and oblique osteotomy of the tibial tubercle at 30 degrees,
trying to maintain a balance between the medialization effect for a good patellar
alligment and the anteriorization effect with the use of a tricortical bone graft. (Figure
4). The degree of medialization is determined in the OR through arthroscopy, once the
patellar position desired is evident.

6
Figura 4: Fulkerson Osteotomy at 30 degrees plus tricortical bone graft. The medialization effect is maintained and the anteriorization is obtained with a low volume graft. The vertical doted lines represent the degree of medialization, which is determined in the OR.
The objective of this study was to evaluate the outcomes and the level of pain in a
cohort of patients with severe patellofemoral arthrosis secondary to patellofemoral
malaligment, treated with the Fulkerson Osteotomy plus a tricortical bone graft between
2001 and 2011.
7
METHODS AND MATERIALS
A retrospective cohort was conducted in patients with severe patellofemoral arthrosis
secondary to patellofemoral malaligment treated by one of the authors (E. Afanador)
between 2001 and 2011 with the tecnique described by Fulkerson, with the addition of a
tricortical bone graft, evaluating functionality and pain.
The including criteria for the patients were: patients with severe patellofemoral
arthrosis demonstrated arthroscopically and patellofemoral malaligment treated with the
tecnique described. Patients with a follow up less than two years were excluded. The
surgical procedure was indicated in patients with anterior knee pain that did not
improved with medical treatment during six months, pain that interfered with daily life
activities, severe patellofemoral arthrosis and patellofemoral malaligment demonstrated
by X rays, Axial CT of the patella at 0º-20º-40º and confirmed by arthroscopy. (14).
The procedure was not indicated in patients with inflamatory diseases, posttraumatic
patellofemoral arthrosis and tricompartmental artrosis.
The main outcomes evaluated were functionality and pain. These were evaluated with
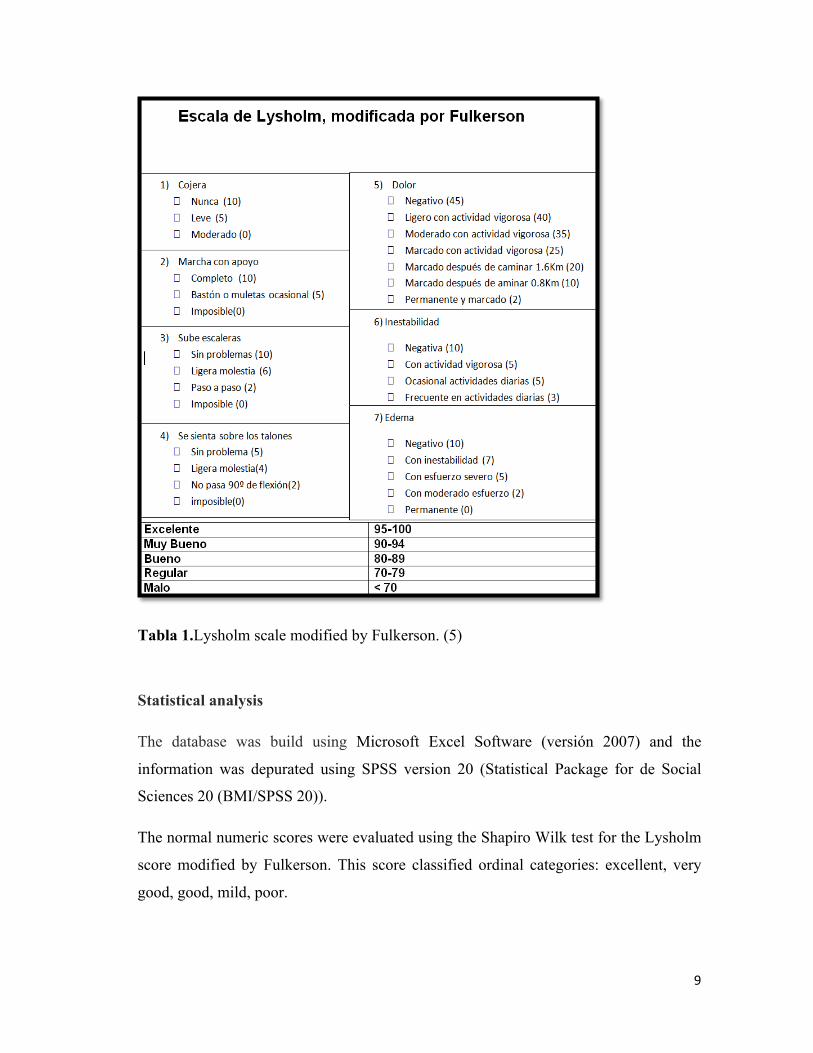
the application of the Lysholm score modified by Fulkerson (5,15) which evaluates 7
points: 1. Limp 2. Support 3. Stair climbing 4. Squatting, 5. Pain 6. Instability 7.
Swelling. This is a 100 points based score, where excellent results are obtained with a
95-100 score, very good results with a 90-94 score, good results wiht a 80-89 score,
mild results with a 70-79 score and poor results with a 70 or less score (Table 1).
The pain was evaluated with the VAS score, (VAS)(16) patients were asked for their
pain before the procedure and at the moment of the evaluation for this study. The
degree of subjective satisfaction after the surgical intervention was evaluated too, if the
patient was better, the same or worst after the procedure (17) and if the patient would
recommend this procedure to other patients. Other variables evaluated were age,
gender, laterality and associated complications.

8
The information was obtained post surgery, the scores were used obtaining variable
times among the patienst according to the time of the surgery and the moment when
they were evaluated. All the patients gave their verbal authorization for the realization
of the study, the use of the scales and questionnaires. No patient refused to be in the
study. The patients were taken from the Hospital Militar Central and the Clinica
Universitaria Colombia databases. All the information was condensed in a new
database made with Microsoft Excel software 2007 version. The deparments of
epidemiology and stadistics of the Hospital Militar Central and the Clinica Universitaria
Colombia evaluated also the study to determine its quality. The clinical charts of the
patients were evaluated to confirm the diagnosis and the surgical procedure conducted,
the age, gender, diagnosis, laterality of the affected limb, time of surgery and
complications.
9
Tabla 1.Lysholm scale modified by Fulkerson. (5)
Statistical analysis
The database was build using Microsoft Excel Software (versión 2007) and the
information was depurated using SPSS version 20 (Statistical Package for de Social
Sciences 20 (BMI/SPSS 20)).
The normal numeric scores were evaluated using the Shapiro Wilk test for the Lysholm
score modified by Fulkerson. This score classified ordinal categories: excellent, very
good, good, mild, poor.

10
The VAS score changes were evaluated before the surgery and in the post surgical
period with the non parametric test of Wilcoxon. For determining if it was significant
difference in the functionality Fulkerson score we used the non parametric ANOVA
from Kruskall-Wallis.
The results were statistically significant with a level of 5% (p<0,05).
Surgical Tecnique
The arthroscopy was conducted without the use of a tourniquet. It was verified the
subluxation and the severe patellofemoral arthrosis through the conventional portals for
the knee. Associated lesions were also evaluated. The tricortical bone autograft was
harvested from the ipsilateral iliac crest, shaping it in a trapezoidal way of 10mm. Later
the external liberation was conducted. Anterolateral longitudinal approach of 5-6cm
below the external articular line through caudal parallel to the tibial tubercle.
Subperiostical elevation of the muscular structures of the anterolateral fossa, avoiding
the use of separators in the posterior aspect of the tibia to diminish the risk of
neurological damage.
The external liberation of the lateral retinaculum, capsule and sinovia is completed
from caudal (site of the osteotomy) to cephalic (proximal pole of the patella). Excision
of the infrapatellar fat pad. Delineate of the osteotomy on the lateral cortical of the tibial
tubercle, 7 cms of longitude by 1 cms of thickness in relation with the anterior border of
the tibia, perforation of the lateral cortical through the medial cortical with a 3.2 drill,
with a 30 degrees inclination from posterior to anterior and from lateral to medial.
(Figure 5). The ostetomy is completed with an oscillanting saw.

11
Figura 5. Intra-procedure picture of the osteotomy at 30 degrees of inclination.
Subperiostal elevation of the medial flap to preserve periostium and to conserve the
pedicle of the fragment of the tibial tubercle. Percutaneous bone perforations at the
external facet of the patella and at the femoral groove with a K-wire of 2.0 mm with a
median distance of 5 mm between each orifice. (Figure 6).

12
Figura 6. Extensive Osteochondral lesión Outerbridge Grade IV of the lateral facet of the patella after spongialization.
Through the tibial incisión any osteophyte is removed from the lateral margin of the
patella and from the lateral femoral condyle. The anteriorization of the tibial tubercle is
obtained with the oblique osteotomy and the addition of the tricortical bone graft of 10
mm of spesor. The degree of medialization of the tibial tubercle is determined once the
patella is in an adequate position. A temporal fixation of the tibial tubercle is obtained
with a K wire of 2.0mm without perforating the bone graft. The right patellofemoral
position is verified arthoscopically and definitive fixation is obtained using two cortical
screws of 4.5 mm with a washer, using a lag screw tecnique, avoiding the perforation
of the bone graft to diminish the risk of fracture. (Figure 7).
13
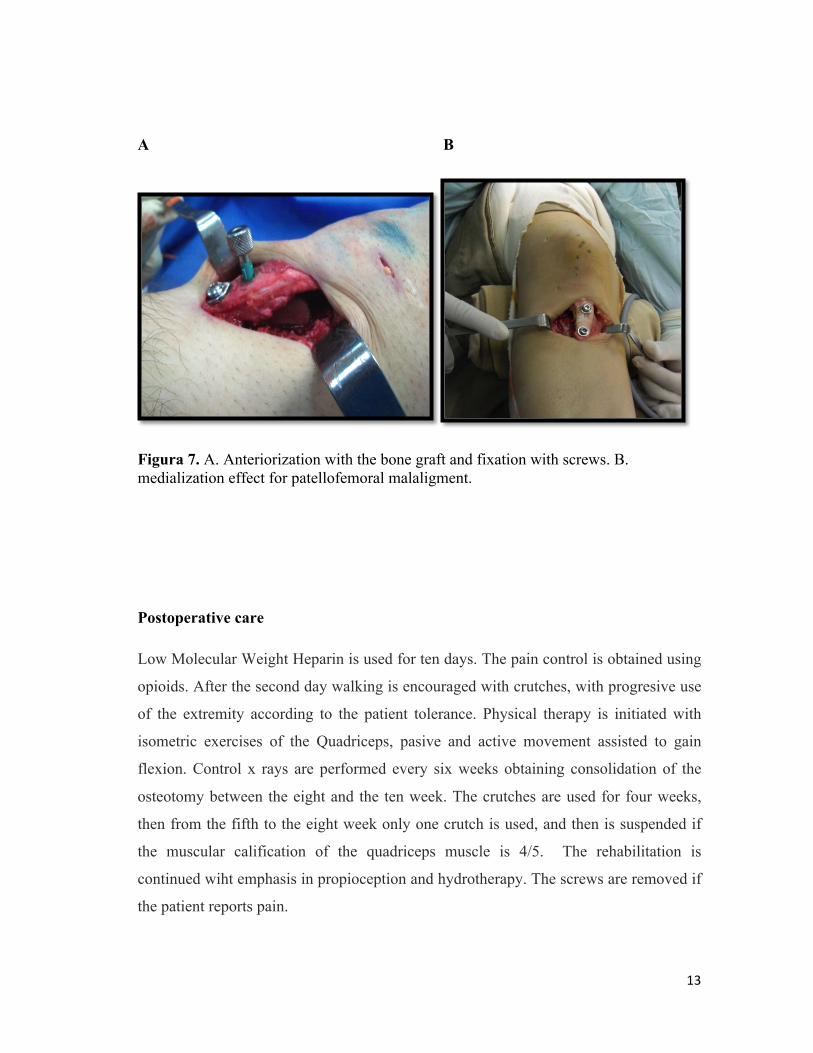
A B
Figura 7. A. Anteriorization with the bone graft and fixation with screws. B. medialization effect for patellofemoral malaligment.
Postoperative care
Low Molecular Weight Heparin is used for ten days. The pain control is obtained using
opioids. After the second day walking is encouraged with crutches, with progresive use
of the extremity according to the patient tolerance. Physical therapy is initiated with
isometric exercises of the Quadriceps, pasive and active movement assisted to gain
flexion. Control x rays are performed every six weeks obtaining consolidation of the
osteotomy between the eight and the ten week. The crutches are used for four weeks,
then from the fifth to the eight week only one crutch is used, and then is suspended if
the muscular calification of the quadriceps muscle is 4/5. The rehabilitation is
continued wiht emphasis in propioception and hydrotherapy. The screws are removed if
the patient reports pain.

14
Ethical Aspects
This study is classified as an investigation with minimal risks according to the artículo
5, Res. Nº 008430 from the national ethics code.

15
RESULTS
The cohort was conformed by 38 patients and a total of 45 knees. ( 26 right knees and 19
left knees) whom were intervened with a fulkerson osteotomy plus a tricortical bone graft
and spongialization between 2001 and 2011. The most frequent gender was femenine with
a 92,1% (n=35) and the average age was 44,7±10,9 años, with variation between 23 and
62 years. The mean follow up from the date of the surgical procedure to the application of
the questionnaries was 44,0±26,8 months (mean=34,3 months) with a range between 2and
11,9 years. All of the patients showed and improved pain according to the VAS score, with
an average VAS score of 9 in the pre surgical period and an average VAS score of 2 in the
postoperative period, with a seven point improvement in the VAS score. (p <0,001, non
parametric test of Wilcoxon) (Figure 8).
Figura 8. Comparison of the pain score befor surgery and afeter the surgical intervention.
The numerical values from 2 to 100 of the lysholm score modified by fulkerson showed a
different to normal (p=0,002, Shapiro Wilk test), with left asimmetry (CA=-0,787). The
16
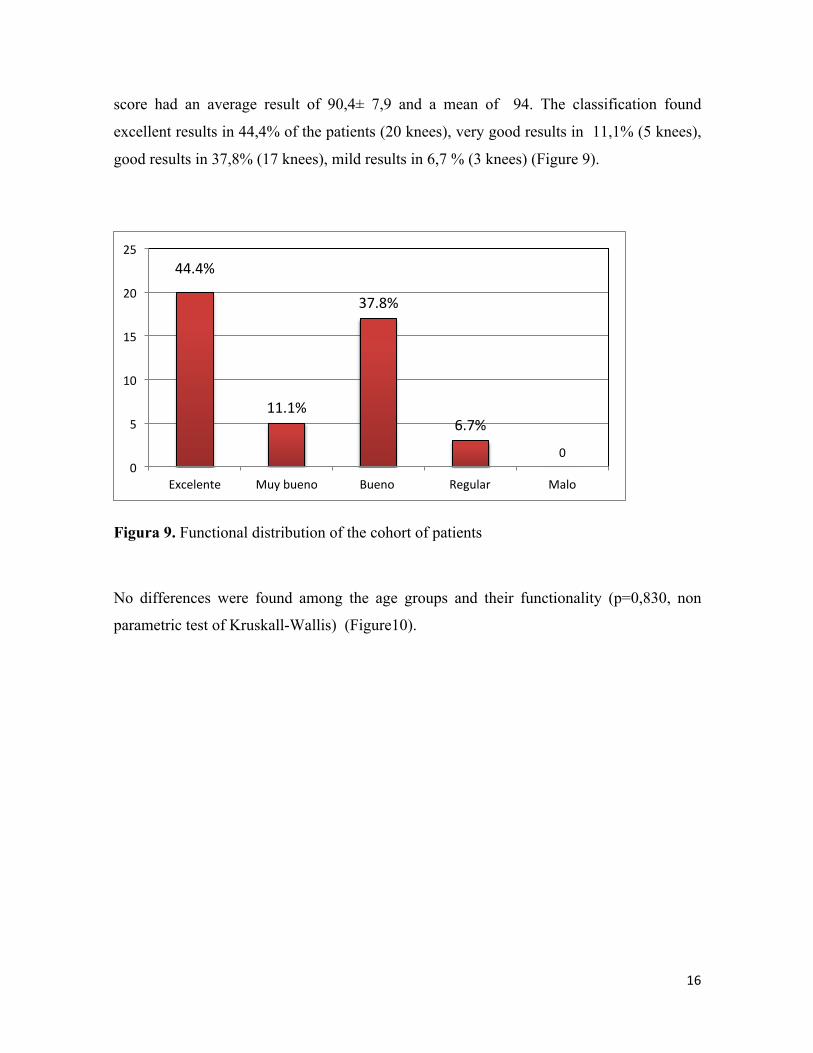
score had an average result of 90,4± 7,9 and a mean of 94. The classification found
excellent results in 44,4% of the patients (20 knees), very good results in 11,1% (5 knees),
good results in 37,8% (17 knees), mild results in 6,7 % (3 knees) (Figure 9).
Figura 9. Functional distribution of the cohort of patients
No differences were found among the age groups and their functionality (p=0,830, non
parametric test of Kruskall-Wallis) (Figure10).
44.4%
11.1%
37.8%
6.7%
0 0
5
10
15
20
25
Excelente Muy bueno Bueno Regular Malo

17
Figura 10. Functionality results among age groups.
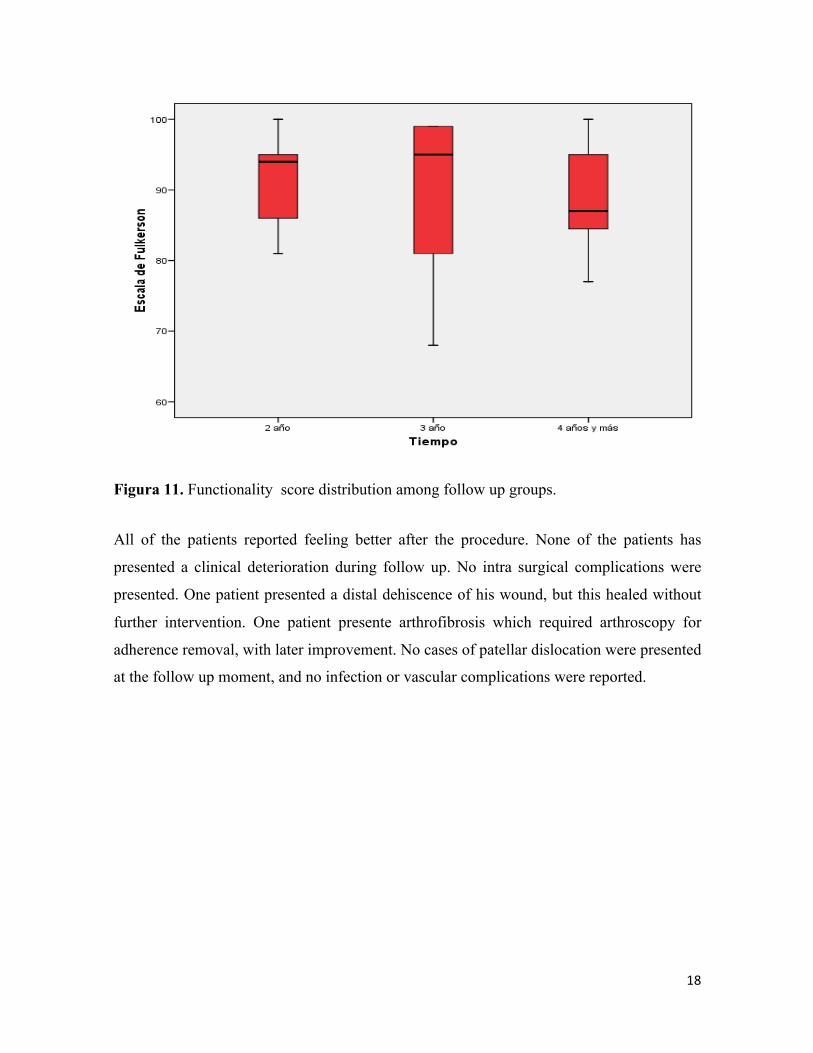
Among the follow up groups and the functionality scores we found no differences
(p=0,722, non parametric test of Kruskall-Wallis). The mean functionality scores during the
second year were 94,0; during the third year were 95,0, and of 87,0 at the fourth year or
more (Figure 11).
18
Figura 11. Functionality score distribution among follow up groups.
All of the patients reported feeling better after the procedure. None of the patients has
presented a clinical deterioration during follow up. No intra surgical complications were
presented. One patient presented a distal dehiscence of his wound, but this healed without
further intervention. One patient presente arthrofibrosis which required arthroscopy for
adherence removal, with later improvement. No cases of patellar dislocation were presented
at the follow up moment, and no infection or vascular complications were reported.
19
DISCUSSION
All of the patients reported an improvement in the VAS score, with a mean
improvement of 7 points. All of the patient manifested their satisfaction with the
functional result obtained with the procedure. The results obtained with the lysholm
score modified by 93,3% of the patients had excellent to good results. Comparing this
cohort with the current reports of the literature in which only a transverse osteotomy is
performed (Elmslie-Trillat-Maquet)(3,4) or only the oblique Fulkerson osteotomy is
performed without the use of bone graft (5,6) we observe an improvement in the
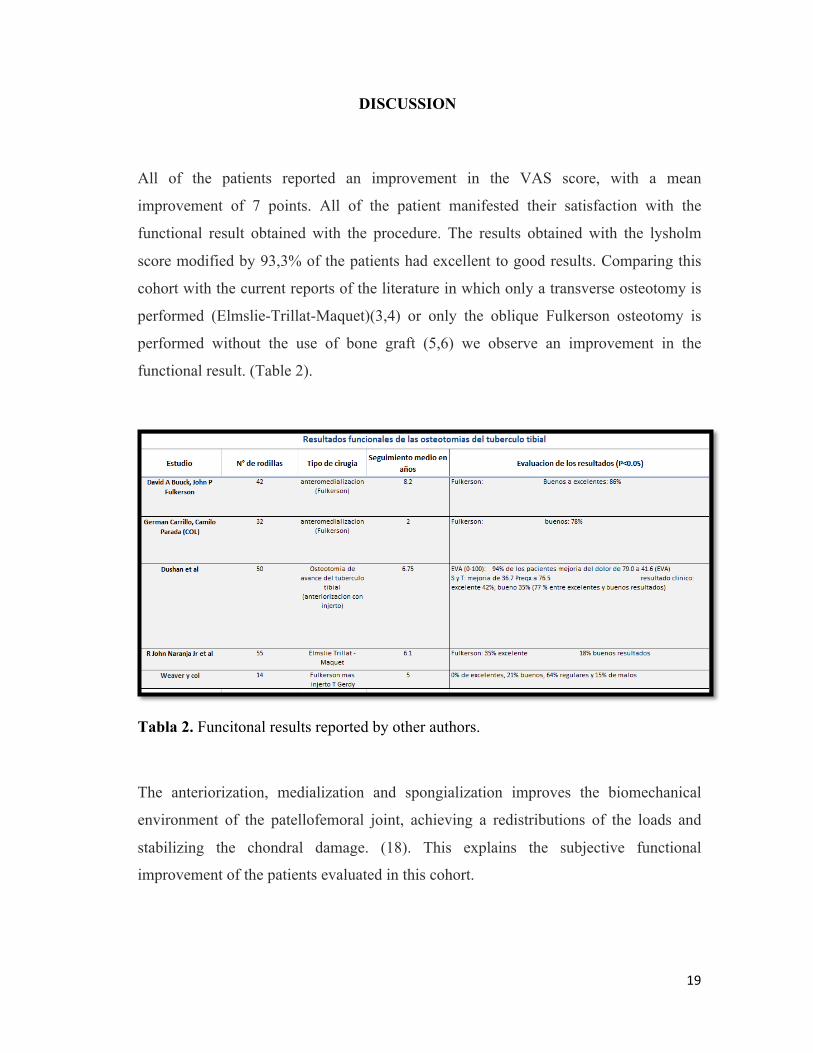
functional result. (Table 2).
Tabla 2. Funcitonal results reported by other authors.
The anteriorization, medialization and spongialization improves the biomechanical
environment of the patellofemoral joint, achieving a redistributions of the loads and
stabilizing the chondral damage. (18). This explains the subjective functional
improvement of the patients evaluated in this cohort.
20
David A. Buuck and J Fulkerson(5) in their series of 42 knees with a mean follow up of
8,2 years reported 86% (36 knees) of excellent to good results with an oblique
osteotomy without the use of a bone graft. Carrillo and Parada(6) in their series of 32
knees with a mean follow up of 2 to 7 years performing a fulkerson osteotomy for
severe patellofemoral arthrosis and patellofemoral malalignment showed a 78% of good
results, 9% of mild results and 13% of poor results after applying the lysholm score
modified by fulkerson. Our study showed a 93,3% of excellent to good results
compared to their study.
We consider that the fulkerson osteotomy at 30 degrees plus the use of a tricortical
bone graft (maquet effect) and spongialization is a good alternative for the treatment of
severe patellofemoral arthrosis secondary to patellofemoral malalignment, it is a secure
option with a low rate of complications which gives the patients, mainly the younger
patients a great improvement in their pain and functionality. Nevertheless, it is
important to conduct prospective studies among the different surgical tecniques to
support these findings. Another future alternative is to combine these tecniques with
the use of implantation of autologus chondrocites for the regeneration of the native
cartilage.
An important aspect is the degree of inclincation of the osteotomy, which determines
the rate of medialization. If a 45 degrees osteotomy is performed and then the bone
graft is used, the medialization effect would be lost, for this reason, with the use of an
osteotomy at 30 degrees of inclination we could obtain the medialization effect while
optimizing the anteriorization effect with the use of a small bone graft.
The surgeon and the patient must know that this procedure is mainly indicated to give
more time for a severe damaged knee in which arthroplasty is not yet an option. The
patients and their families must comprehend the objectives of the procedure.
21
One of the limitations of this study was that the lysholm score modified by fulkerson
was not evaluated in a periodic way, was applied in a variable time in the postoperative
period and was not used in the preoperative period.
AGRADECIMIENTOS
Agradecemos al Servicio de Ortopedia y Traumatología del Hospital Militar Central y a La
Clínica Universitaria Colombia Sanitas por su colaboración y a los pacientes de las
respectivas instituciones que autorizaron participar en la elaboración del presente estudio.
A los departamentos de Educación Médica e Investigación del Hospital Militar Central y de
La Clínica Universitaria Colombia Sanitas.
A la Doctora Michelle Cortés, asesora epidemiológica de la SCCOT, por sus valiosas
orientaciones y sugerencias.
Al Doctor Milcíades Ibáñez Pinilla, Experto en Bioestadística y Epidemiología, Centro de
Investigación, Ciencias de la Salud, Fundación Universitaria Sanitas.
Al Doctor Andrés Prada, Médico General, Universidad Militar Nueva Granada, por su
valiosa colaboración en la recolección de la información y desarrollo metodológico.
22
BIBLIOGRAFÍA
1. Grelsamer RP. Patellar malalignment. The Journal of bone and joint surgery. American volume. 2000 Nov;82-A(11):1639–50.
2. Fulkerson JP. Current Disorders Concepts Review Alignment of Patellofemoral. J Bone and Joint Surgery. 1990;72A(9):1424–9.
3. Maquet P. Advancement of the tibial tuberosity. CLin Orthop. 1976;115:225–30.
4. Naranja RJ, Reilly PJ, Kuhlman JR, Haut E, Torg JS. Long-term evaluation of the Elmslie-Trillat-Maquet procedure for patellofemoral dysfunction. The American journal of sports medicine. 24(6):779–84.
5. Buuck D a., Fulkerson JP. Anteromedialization of the tibialtubercle: A 4- to 12-year follow-up. Operative Techniques in Sports Medicine. 2000 Apr;8(2):131–7.
6. Carrillo, G. Parada C. Osteotomía de desplazamiento anterior e interno de la tuberosidad anterior de la tibia (Fulkerson) en pacientes con artrosis y mal alineamiento patelofemoral. Revista colombiana de Ortopedia y Traumatologia. 2004;18(1):42–50.
7. Atkinson HD, Bailey C a, Anand S, Johal P, Oakeshott RD. Tibial tubercle advancement osteotomy with bone allograft for patellofemoral arthritis: a retrospective cohort study of 50 knees. Archives of orthopaedic and trauma surgery. 2012 Apr;132(4):437–45.
8. Fulkerson J. Anteromedialization of the tibial tuberosity for petellofemoral malalignment. CLin Orthop. 1983;177:176–81.

23
9. Ferguson A. Relief of patellofemoral contact stress by anterior displacement of the tibial tubercle. J Bone and Joint Surgery. 1982;61:766.
10. Kadambande S. A review of wound healing following Maquet osteotomy. The Knee. 2003 Dec 3;11:463–7.
11. Steimer O, Kohn D. Anteromedialization of the Tibial Tubercle. Operative Techniques in Orthopaedics. 2007 Jan;17(1):66–71.
12. Fulkerson JP. Patellofemoral Pain Disorders : Evaluation and Management. J Am Acad Orthop Surg. 1994;2:124–32.
13. Fulkerson JP. Anteromedial tibial tuberosity transfer. The Knee. 1996;3:88–90.
14. Outerbridge RE. The etiology of chondromalacia patellae. 1961. J Bone and Joint Surgery. 1961 Aug;(43-B):752–7.
15. Lysholm J, Gillquist J. Evaluation of knee ligament surgery results with special emphasis on use of a scoring scale. The American journal of sports medicine. 10(3):150–4.
16. Crossley KM, Bennell KL, Cowan SM, Green S. Analysis of outcome measures for persons with patellofemoral pain: which are reliable and valid? Archives of Physical Medicine and Rehabilitation. 2004 May;85(5):815–22.
17. Harwin SF. Arthroscopic debridement for osteoarthritis of the knee: predictors of patient satisfaction. Arthroscopy : the journal of arthroscopic & related surgery : official publication of the Arthroscopy Association of North America and the International Arthroscopy Association. 1999 Mar;15(2):142–6.
18. Scott F. Dye. Reflections on Patellofemoral Disorders. In: Biedert RM, editor. Patellofemoral Disorders: Diagnosis and Treatment. Chichester, UK: John Wiley & Sons, Ltd; 2004. p. 31–46.
19. Weaver, JK. Wieder, D. Derkash R. Patellofemoral arthritis resulting from malalignment: a long-term evaluation of treatment options. Orthop Rev. 1991;20:1075–81.


















