SEVERE CAP - thececonsultants.comthececonsultants.com/images/1Holtom_InfectiousDiseases.pdf ·...
11
DILEMMAS IN INFECTIOUS DISEASE Paul D. Holtom, MD Associate Professor of Medicine and Orthopaedics USC Keck School of Medicine SEVERE CAP What is the best antibiotic treatment for severe CAP? COMMON PATHOGENS IN CAP
Transcript of SEVERE CAP - thececonsultants.comthececonsultants.com/images/1Holtom_InfectiousDiseases.pdf ·...

DILEMMAS IN INFECTIOUS
DISEASE Paul D. Holtom, MD
Associate Professor of Medicine and Orthopaedics USC Keck School of Medicine
SEVERE CAP
What is the best antibiotic treatment
for severe CAP?
COMMON PATHOGENS IN CAP

CAP: Coinfection S.pneumoniae + “Atypicals”
• Jokinen (CID 2001): 21% of Sp patients had coinfection: • Mycoplasma, Chlamydia
• Lieberman (Thorax, 1996): 148 S. pneumoniae patients
– Mycoplasma: 43 29% – Chlamydia: 34 23% – Legionella: 23 15% – TOTAL 67%
CAP: INPATIENT TREATMENT
• Respiratory fluoroquinolone • β-lactam PLUS a macrolide
Mandel et. al. CID 2007;44:S27-72
30-day CAP Mortality in Hospitalized Elderly Patients
0.00 0
Days from hospital admission
Adj
uste
d m
orta
lity
0.20
0.18
0.16
0.14
0.12
0.10
0.08
0.06
0.04
0.02
5 10 15 20 25 30
2nd gen. ceph + macrolide ↓29%*
Fluoroquinolone ↓36%*
*p < 0.05
n=12,945 inpatients β-Lactam/inhibitor + macrolide ↑77%*

CAP: INPATIENT TREATMENT (ICU)
• β-lactam PLUS – Azithromycin OR – Fluoroquinolone
• For CA-MRSA – add vancomycin or linezolid
Mandel et. al. CID 2007;44:S27-72
C. Difficile DIARRHEA
What antibiotic is best
and how long should I treat?
Epidemiology of CDAD
Scanning electron micrograph
DIAGNOSTIC CHALLENGES
• EIA – Results in 2 hours – Sensitivity 60-95%; Specificity 75-100% – Repeat testing not warranted
• Changes diagnosis in <1% of cases • Increases rate of false positive test
Mohan SS et al. Am J Med 2006;119:356
STANDARD THERAPY • Withdrawal of inducing agent • Avoid drugs with antiperistaltic activity • Oral metronidazole
– 250 mg qid or 500 mg tid x 10 d – First line therapy since 1980’s – CDC preferred therapy – New reports of failure rates of 16-38%
Bartlett, Ann Int Med 2006;145:758-764
STANDARD THERAPY • Withdrawal of inducing agent • Avoid drugs with antiperistaltic activity • Oral metronidazole • Oral vancomycin
– 125 mg-250 mg po qid x 10 d – Probably more effective, esp. in seriously
ill patients
Bartlett, Ann Int Med 2006;145:758-764
ESBL-PRODUCING GRAM NEGATIVES
What antibiotic would be effective?
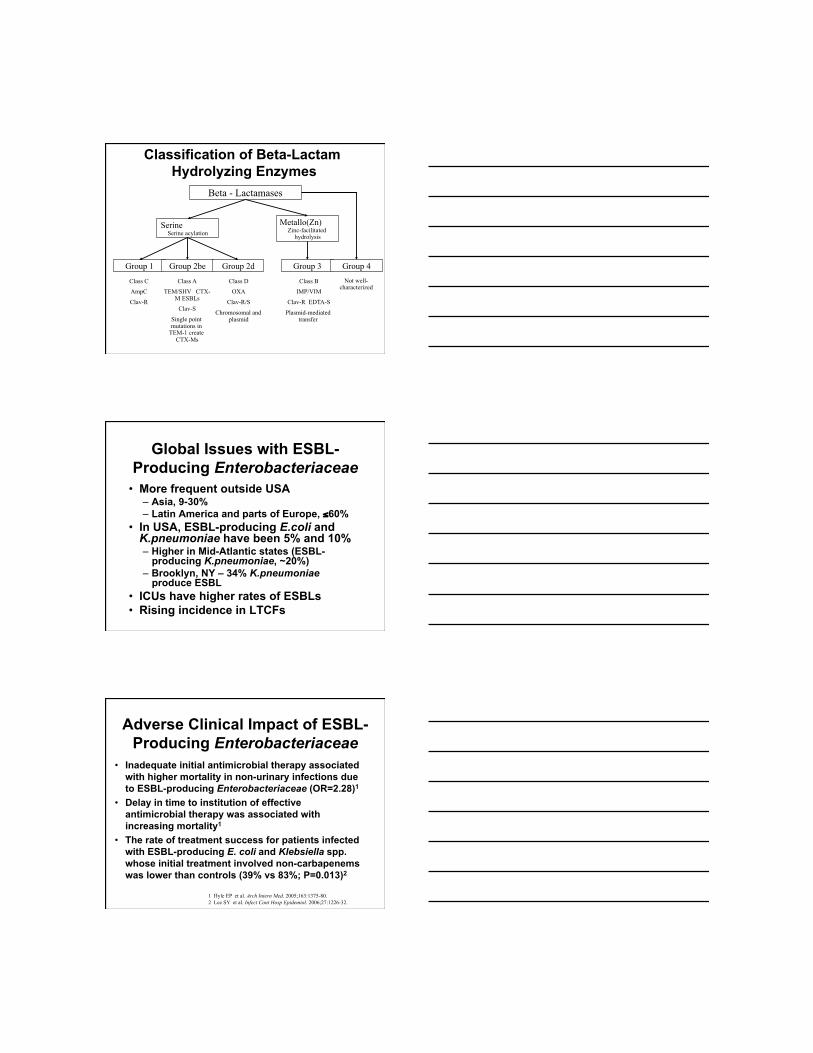
Classification of Beta-Lactam Hydrolyzing Enzymes
Group 1 Group 2be Group 2d Group 3 Group 4
Class C
AmpC
Clav-R
Class A
TEM/SHV CTX-M ESBLs
Clav-S
Single point mutations in
TEM-1 create CTX-Ms
Class D
OXA
Clav-R/S
Chromosomal and plasmid
Class B
IMP/VIM
Clav-R EDTA-S
Plasmid-mediated transfer
Not well-characterized
Serine Serine acylation
Metallo(Zn) Zinc-facilitated
hydrolysis
Beta - Lactamases
Global Issues with ESBL-Producing Enterobacteriaceae
• More frequent outside USA – Asia, 9-30% – Latin America and parts of Europe, ≤60%
• In USA, ESBL-producing E.coli and K.pneumoniae have been 5% and 10% – Higher in Mid-Atlantic states (ESBL-
producing K.pneumoniae, ~20%) – Brooklyn, NY – 34% K.pneumoniae
produce ESBL • ICUs have higher rates of ESBLs • Rising incidence in LTCFs
Adverse Clinical Impact of ESBL-Producing Enterobacteriaceae
• Inadequate initial antimicrobial therapy associated with higher mortality in non-urinary infections due to ESBL-producing Enterobacteriaceae (OR=2.28)1
• Delay in time to institution of effective antimicrobial therapy was associated with increasing mortality1
• The rate of treatment success for patients infected with ESBL-producing E. coli and Klebsiella spp. whose initial treatment involved non-carbapenems was lower than controls (39% vs 83%; P=0.013)2
1 Hyle EP et al. Arch Intern Med. 2005;163:1375-80. 2 Lee SY et al. Infect Cont Hosp Epidemiol. 2006;27:1226-32.
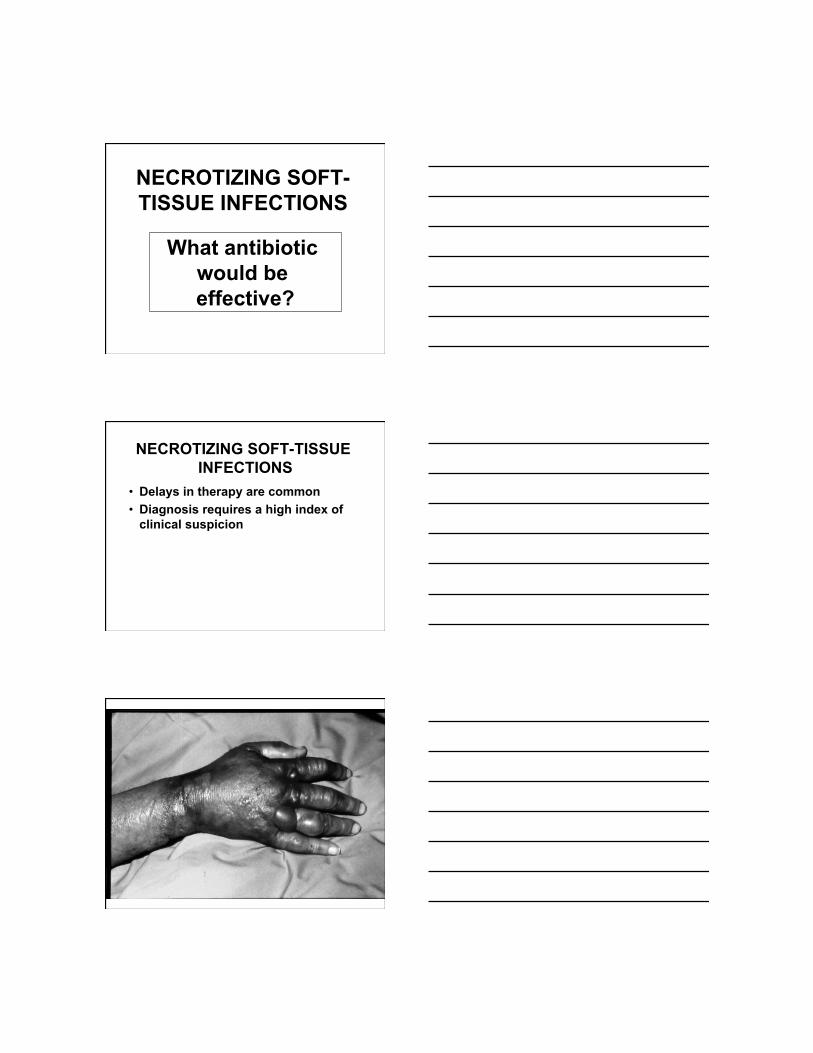
NECROTIZING SOFT-TISSUE INFECTIONS
What antibiotic would be effective?
NECROTIZING SOFT-TISSUE INFECTIONS
• Delays in therapy are common • Diagnosis requires a high index of
clinical suspicion
CLASSICAL TRIAD OF NECROTIZING
SOFT-TISSUE INFECTIONS
• Fever • Crepitance • Hypotension
SIGNS OF NECROTIZING SOFT-TISSUE INFECTIONS
• Edema > erythema • Skin vesicles or bullae • Subcutaneous gas • No lymphangitis or
lymphadenitis
DIAGNOSIS OF NECROTIZING STI
• Clinical findings • Laboratory testing
– Of little use – Lacks sensitivity and specificity
• Ultrasound • MRI scan • SURGERY
CLASSIFICATION OF NECROTIZING FASCIITIS
• Type I – Polymicrobial – Most common in diabetics,
immunocompromized
CLASSIFICATION OF NECROTIZING FASCIITIS
• Type I • Type II
– Group A Strep (Strep. pyogenes) – Most common type – 20% are nosocomial – 50% have no obvious portal of entry
CLASSIFICATION OF NECROTIZING FASCIITIS
• Type I • Type II • Type III
– Marine vibrio – Acquired by puncture from fish or
ingestion of shellfish
NECROTIZING STI: THERAPY
• Prompt recognition • Urgent debridement • Broad-spectrum antibiotics
McHenry et al, Ann Surg 1995;221:558
NECROTIZING STI: ANTIMICROBIAL THERAPY
• Beta-lactam antibiotic • Streptococcal coverage
– + Clindamycin • Gram negative coverage • Anaerobic coverage
CID 2005;41:1373-406
NECROTIZING STI: OTHER THERAPY
• ? IVIG – Streptococcal necrotizing infections
• Study: 21 pts vs 32 historical controls • Improved 30 mortality rate
Kaul et al. CID 1999;28:800-7
NECROTIZING STI: OTHER THERAPY
• ? IVIG • ? Hyperbaric oxygen
– Post debridement – Several studies (observational, non-
randomized, suggest lower mortality)
THANK YOU