
Service Line Optimization Medicine Patients -...
14
12/3/2017 1 Service Line Optimization Medicine Patients Q11 This presenter has nothing to disclose Katharine Luther, RN, MPM Director of Quality , McGovern Medical School University of Texas, Texas Medical Center, Houston IHI’s National Forum December 11, 2017 Orlando, Florida Memorial Hermann-Texas Medical Center University of Texas- McGovern School of Medicine 1100 Beds Busiest Level 1 Trauma Center 7 th Largest Training Program Medicine Service Line Approximately 3000 patients/year • 10% uninsured • 70% admitted from ED • 117 Total beds • 16 ICU beds • 14 IMU beds • 87 floor beds (3 geographic locations)
Transcript of Service Line Optimization Medicine Patients -...

12/3/2017
1
Service Line Optimization Medicine Patients
Q11This presenter has nothing to
disclose
Katharine Luther, RN, MPMDirector of Quality , McGovern Medical SchoolUniversity of Texas, Texas Medical Center, Houston
IHI’s National ForumDecember 11, 2017
Orlando, Florida
Memorial Hermann-Texas Medical Center
University of Texas- McGovern School of Medicine
1100 Beds
Busiest Level 1 Trauma Center
7th Largest Training Program
Medicine Service Line
Approximately 3000 patients/year
• 10% uninsured
• 70% admitted from ED
• 117 Total beds • 16 ICU beds
• 14 IMU beds
• 87 floor beds (3 geographic locations)

12/3/2017
2
3
Shape or Reduce Demand
Match Capacity and Demand
Redesign the System
Staff Engagement Results
Assure key processes
EC• Form partnerships• Reduce admission delays
Downstream beds• ICU to IMU, floor
bed ratios• Discharge criteria• RRT
ICU
Stabilization - Weaning-- Mobility –Complications--End of Life

12/3/2017
3
ICU - Foundational Elements
Stabilization
• Sepsis protocol
• Fluid stability• Ventilator
management
Weaning
• Vent hours• Sedation
protocol/w holiday
• Weaning criteria – “no MD”
• 24-hour weaning, extubation
Mobility
• Protocol online
• Standard workflow
• Delirium assessment (CAM-ICU)
• Metrics
Prevent Complications
• VAP, CLABSI protocol
• FMEA –low volume
• Renal injury• DVT
End of Life
• Secure and respect wishes
• Family meeting in 24 hours
• Clear follow-up plan
Redesign the System
Match
Capacity and Demand
May-11Oct-10Mar-10Aug-09Jan-09Jul-08Nov-07Apr-07Sep-06Feb-06Jul-05
12
10
8
6
4
2
0
Observation
Ind
ivid
ua
l V
alu
e
_X=0.07
Baseline Implementation
1
MICU VAPs to Zero for 49 Consecutive Months!(Data collection period: July 2005-July 2011)
Ventilator management--weaning
FMEA on VAP after bundle at 94% compliance
Aspiration during transport
Cuff leaks
Unplanned extubations requiring reintubation
*Cocanour C., Ostrosky-Zercher, L., Peninger M., Garbade D., Tidemann T., Domonoske, B., Li T., Allen S., Luther, K., Cost of a Ventilator Associated Pneumonia in a Shock Trauma Intensive Care Unit, Surg Infect (Larchmt). 2005 Spring;6(1):65-72.
Savings per VAP*$ 57,000
15.2 ICU days11.9 vent days
Redesign the System
Match
Capacity and Demand
• Compliance increased 66% to 93%• Ventilator days decreased 5.5 days to 4.4 days • MICU -LOS for vented patients 5.0 days to 4.0 days

12/3/2017
4
Get to Green Visual Display in MICU
Mobility- Delirium Prevention8
5am:
1 patient up to neuro or regular
chair & place
on white board
8 am:
Charge get with nurses to establish assigned
mobility time and place on white board
9:00 am:
Call LIFT team to schedule
appointments for mobility
1pm:
Mobility Huddle
5 pm:
Mobility Huddle
Charge nurse update assessment and handoff report &
update white board with
Reductions: MV duration 112 to 91/hours 21 hours savedICU days 7.5 to 5.25 days 2.25 days
Redesign the System
Match
Capacity and Demand

12/3/2017
5
End of Life Care- Decision-making9
Reduced ICU LOS 10.1 days to 7.7 days
• Earlier decision-making and plan
• Decreased unnecessary interventions
Match
Capacity and Demand
Redesign the System
ED to MICU Transfers
Results Before After
Transfer < 4 hours 53% 74%
Hospital LOS 9.1 days 7.8 days
Streamline Communication
AfterBefore
Redesign the System
Match
Capacity and Demand

12/3/2017
6
Medicine Floors
Family Practice
Geriatrics Unit
Internal Medicine
Non Teaching
Internal Medicine Teaching
Team A
Team B
TeamC
Team D
Increased CMI of floor level patients from 1.36 to 1.44
Resident “Waste Tool” – ProjectMatch
Capacity and DemandStaff Engagement

12/3/2017
7
Cost reduction- Clinical Projects
Financial Implications in the Current System
Impact on Quality
Substantial Cost Savings Moderate Cost Savings
Negative Impact-no savings or loss
High •Sickle Cell management ($450K/ year)•Chest Pain management ($ 400K/year)
•To be evaluated: ICU days awaiting consultation, procedures, end of life discussions
•EC – MICU admits (duplicate tests on MICU admit)
Moderate ABG testing $15 K •Confirmatory tests•Repeat tests
•Supplies
Shape or Reduce
DemandStaff Engagement
• $1200 cost per case reduction in direct costs
Sepsis -- LOS, CostMatch
Capacity and Demand

12/3/2017
8
Patient Demographics
Time Intervals
Lactates
MAP
Apical HR
Vasopressors
Intropes
Fluids
Sepsis Flag
Sepsis
Dashboard
Staff Engagement
Sepsis Patients – Time to AntibioticsED to MICU Patients Monthly Summary – October 2015
16
13/14 (93%) of patients received 1st
antibiotics within 3 hours of ED Arrival
Staff Engagement

12/3/2017
9
WAQI Committee -- Physician Leaders
Physicians
Nursing
RT
Physical Therapy
Nutrition
Case Management
Finance
Pharmacist
Environmental Services
Others as needed
Staff Engagement
100: MICU Projects Completed
Supply room relocation and organization
Calmoseptine pre-stocked in pyxis
Infection Control Compliance (Supply Caddies Installed)
Care Team Identification
Ventilator weaning protocol
Turning schedule and compliance
New MICU orientation for physician residents
Maintaining Plateau Pressures
HUC workflow sheet
Employee Lockers
Biohazard trash cans available on unit
Visitor Badge System
Visitor Packet- Spanish Translation
Supply system/Stocking Patient Rooms
Locked Medication Cabinets
Body Mechanics for Opening Doors (Door handles)
Line Documentation Sheet
Mediscus Pad use on all patients
RRT Communication Tool
Charge Nurse Book
Nurse Driven Foley Removal Protocol
Bedside Shift Report
ER Float Guide
Staff Engagement

12/3/2017
10
Kamishibai Board19
Question No. Topic 1 2 3 4 5 6 7 8 9 10
CENTRAL LINE - A
A1 Is the central line dressing/cap clean, dry, and intact? Fail Fail Fail Fail Pass Fail Fail Pass Fail Pass
A2 Is the central line dressing dated? Pass Fail Pass Pass Pass Fail Pass Pass Pass Pass
A3 Is all tubing labeled with a date? Pass Fail Pass Fail Pass Pass Pass Fail Pass Fail
A4 Is the central line dressing a CHG dressing? Pass Fail Pass Fail Pass Pass Pass Pass Pass Pass
Staff Engagement
Situational awareness boards 20Match
Capacity and DemandStaff Engagement

12/3/2017
11
Heat maps by unit/service by month21
Current Results
Ranked Number 15 in Vizient (UHC) Overall
Ranked Number 6 in Vizient (UHC) in Safety
Medicine Mortality O/E 0.70
22

12/3/2017
12
↓ 15 floor beds
Occupancy Rate went from 78% to >90%
Turn Around Time“Bed request to Available Bed”
FY16
Pre-loss Post loss % increase
ICU 2.0 hours 3.6 hours 80%
IMU 2.5 hours 5.9 hours 136%
Floor 1.25 hours 5.2 hours 316%
12/3/2017
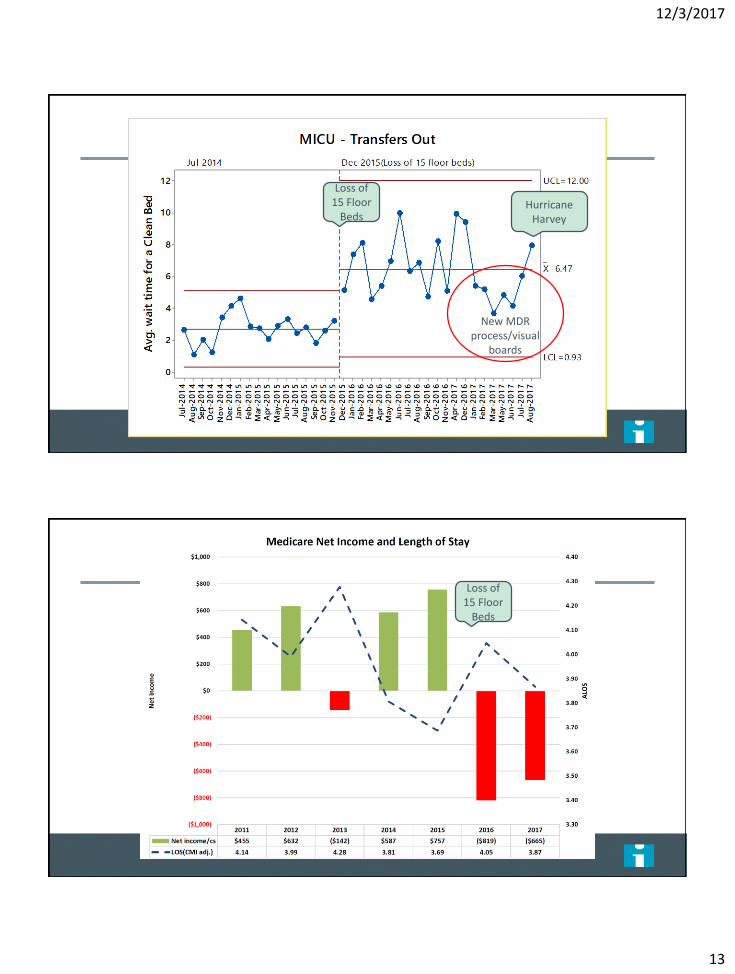
13
Loss of 15 Floor
Beds
New MDR process/visual
boards
Hurricane Harvey
Loss of 15 Floor
Beds

12/3/2017
14
Success factors
A new way of thinking vs “Projects”
Reveal the next problem
Speak the same language
Break established rhythms
Visual representations of data
Real-time feedback


















