Serum levels of IL-18 and sIL-2R in patients with alopecia areata receiving combined therapy with...
3
Serum levels of IL-18 and sIL-2R in patients with alopecia areata receiving combined therapy with oral cyclosporine and steroids Deborah Lee 1 , Soon-Kwon Hong 1 , Sung-Wook Park 2 , Dae-Young Hur 3 , Ji-Hong Shon 4 , Jae-Gook Shin 4 , Seon-Wook Hwang 1 and Ho-Suk Sung 1 1 Department of Dermatology, Inje University School of Medicine, Pusan, Korea; 2 Park Sung-Wook Dermatologic Clinic, Pusan, Korea; 3 Department of Anatomy and Research Center for Tumor Immunology, Inje University College of Medicine, Pusan, Korea; 4 Department of Pharmacology and PharmacoGenomics Research Center, Inje University College of Medicine, Pusan, Korea Correspondence: Deborah Lee, Inje University School of Medicine, Pusan, Korea, e-mail: [email protected] Abstract: This study was to determine which immunologic factors contribute to the prognosis of patients with alopecia areata (AA) who were receiving oral cyclosporine A and methylprednisolone. Patients with >25% hair regrowth were defined as responders, and patients exhibiting £25% regrowth were poor-responders. The serum levels of IL-18 and soluble IL-2 receptor (sIL-2R) were measured at baseline in 21 patients with AA and 22 control subjects. The mean serum level of IL-18 in the patients with extensive AA was significantly higher than that in the control subjects. The mean serum concentration of sIL-2R in the AA patients significantly decreased after 1 month of treatment. The mean basal serum level of IL-18 was highest in the responder, whereas the baseline level of sIL-2R was significantly higher in the poor-responder group than other groups. In conclusion, increased serum sIL-2R level and lower IL-18 level at baseline was associated with a poor prognosis in patients with AA. Key words: alopecia areata – IL-18 – prognostic marker – soluble IL-2 receptor Accepted for publication 5 June 2009. Please cite this paper as: Serum levels of IL-18 and sIL-2R in patients with alopecia areata receiving combined therapy with oral cyclosporine and steroids. Experimental Dermatology 2010; 19: 145–147. Background Although the aetiopathogenesis of alopecia areata (AA) is not clearly understood, evidence suggests that T cells and Th1 cytokines play important roles (1). Several studies have attempted to identify correlations among the levels of Th1 cytokines, associated extended cytokines, disease severity, and prognosis of AA (1–6). Cyclosporin A (CsA) and corticosteroids have been used for the treatment of AA with varying success (7–10). Whereas CsA specifically acts by inhibiting IL-2 gene tran- scription, corticosteroids act as non-selective immuno- suppressive agents. Thus, combined therapy with CsA and corticosteroids may have a synergistic therapeutic effect (11). Questions addressed Interleukin-2 (IL-2) plays a central role in the initiation and development of immune responses through binding of the cytokine to IL-2 receptor (IL-2R) and serum soluble IL-2 receptor (sIL-2R) measurements have been applied to a broad spectrum of human disorders involving aberrant immune activation (12). In addition, the importance of IL-18 as an immunoregulatory factor is revealed by its effect on the induction of IFN-c (13,14). So we attempted to find the meaning of serum level of IL-18 and sIL-2R as immuno- logical factor in patients with AA who were receiving combined therapy with oral CsA and methylprednisolones. Experimental design Extensive AA was defined as AA involving >50% of the scalp hair; localized AA was defined as AA involving no more than four alopecic patches (i.e. £50% of the scalp hair). The healthy volunteers were over the age of 18 and had no family or personal history of AA, other auto- immune disease and active inflammatory skin disease. CsA (Cipol-N Ò ) was started at a dose of 2.5–5 mg ⁄ kg ⁄ day and was maintained at 2.5–3 mg ⁄ kg ⁄ day. Methyl- prednisolone (Someron Ò ) was started at a dose of 16–24 mg ⁄ day, tapered down for 5–6 weeks, and then maintained at a dose of 2–4 mg ⁄ day. The treatment response was assessed from photographs and clinical records. Responders were defined as those patients with >25% hair regrowth, and poor-responders were those exhibiting £25% regrowth. DOI:10.1111/j.1600-0625.2009.00937.x www.blackwellpublishing.com/EXD Letter to the Editor ª 2009 John Wiley & Sons A/S, Experimental Dermatology, 19, 145–147 145
-
Upload
deborah-lee -
Category
Documents
-
view
212 -
download
0
Transcript of Serum levels of IL-18 and sIL-2R in patients with alopecia areata receiving combined therapy with...

Serum levels of IL-18 and sIL-2R in patients withalopecia areata receiving combined therapy with oralcyclosporine and steroids
Deborah Lee1, Soon-Kwon Hong1, Sung-Wook Park2, Dae-Young Hur3, Ji-Hong Shon4, Jae-Gook Shin4,
Seon-Wook Hwang1 and Ho-Suk Sung1
1Department of Dermatology, Inje University School of Medicine, Pusan, Korea;2Park Sung-Wook Dermatologic Clinic, Pusan, Korea;3Department of Anatomy and Research Center for Tumor Immunology, Inje University College of Medicine, Pusan, Korea;4Department of Pharmacology and PharmacoGenomics Research Center, Inje University College of Medicine, Pusan, Korea
Correspondence: Deborah Lee, Inje University School of Medicine, Pusan, Korea, e-mail: [email protected]
Abstract: This study was to determine which immunologic factors
contribute to the prognosis of patients with alopecia areata (AA)
who were receiving oral cyclosporine A and methylprednisolone.
Patients with >25% hair regrowth were defined as responders, and
patients exhibiting £25% regrowth were poor-responders. The
serum levels of IL-18 and soluble IL-2 receptor (sIL-2R) were
measured at baseline in 21 patients with AA and 22 control
subjects. The mean serum level of IL-18 in the patients with
extensive AA was significantly higher than that in the control
subjects. The mean serum concentration of sIL-2R in the AA
patients significantly decreased after 1 month of treatment. The
mean basal serum level of IL-18 was highest in the responder,
whereas the baseline level of sIL-2R was significantly higher in the
poor-responder group than other groups. In conclusion, increased
serum sIL-2R level and lower IL-18 level at baseline was associated
with a poor prognosis in patients with AA.
Key words: alopecia areata – IL-18 – prognostic marker – soluble
IL-2 receptor
Accepted for publication 5 June 2009. Please cite this paper as: Serum levels of IL-18 and sIL-2R in patients with alopecia areata receiving combined therapy
with oral cyclosporine and steroids. Experimental Dermatology 2010; 19: 145–147.
Background
Although the aetiopathogenesis of alopecia areata (AA) is
not clearly understood, evidence suggests that T cells and
Th1 cytokines play important roles (1). Several studies have
attempted to identify correlations among the levels of Th1
cytokines, associated extended cytokines, disease severity,
and prognosis of AA (1–6).
Cyclosporin A (CsA) and corticosteroids have been used
for the treatment of AA with varying success (7–10).
Whereas CsA specifically acts by inhibiting IL-2 gene tran-
scription, corticosteroids act as non-selective immuno-
suppressive agents. Thus, combined therapy with CsA and
corticosteroids may have a synergistic therapeutic effect (11).
Questions addressed
Interleukin-2 (IL-2) plays a central role in the initiation and
development of immune responses through binding of the
cytokine to IL-2 receptor (IL-2R) and serum soluble IL-2
receptor (sIL-2R) measurements have been applied to a
broad spectrum of human disorders involving aberrant
immune activation (12). In addition, the importance of
IL-18 as an immunoregulatory factor is revealed by its effect
on the induction of IFN-c (13,14). So we attempted to find
the meaning of serum level of IL-18 and sIL-2R as immuno-
logical factor in patients with AA who were receiving
combined therapy with oral CsA and methylprednisolones.
Experimental design
Extensive AA was defined as AA involving >50% of the
scalp hair; localized AA was defined as AA involving no
more than four alopecic patches (i.e. £50% of the scalp
hair). The healthy volunteers were over the age of 18 and
had no family or personal history of AA, other auto-
immune disease and active inflammatory skin disease.
CsA (Cipol-N�) was started at a dose of 2.5–5 mg ⁄kg ⁄ day and was maintained at 2.5–3 mg ⁄ kg ⁄ day. Methyl-
prednisolone (Someron�) was started at a dose of
16–24 mg ⁄ day, tapered down for 5–6 weeks, and then
maintained at a dose of 2–4 mg ⁄ day.
The treatment response was assessed from photographs
and clinical records. Responders were defined as those
patients with >25% hair regrowth, and poor-responders
were those exhibiting £25% regrowth.
DOI:10.1111/j.1600-0625.2009.00937.x
www.blackwellpublishing.com/EXDLetter to the Editor
ª 2009 John Wiley & Sons A/S, Experimental Dermatology, 19, 145–147 145

The serum levels of IL-18 and sIL-2R were measured
using commercially available ELISA kits (R&D Systems,
Minneapolis, MN, USA) at baseline and after 1 month of
treatment.
All analyses were performed using SPSS, version 14.0.
The Mann–Whitney U-test was used to compare the serum
concentrations of the immunological markers among the
patients and controls. Differences between the groups with
a P value <0.05 were considered to be significant.
Results
The serum levels of IL-18 and sIL-2R were measured in 21
patients (14 with extensive AA and seven with localized
AA) before starting drug therapy and in 22 control sub-
jects. The mean serum concentrations of sIL-2R were
613.59, 664.71, and 571.18 pg ⁄ ml in the patients with
extensive AA, the patients with localized AA and the
controls, respectively (see Table S1). The sIL-2R serum
concentration was not significantly different among the
three groups. The mean serum IL-18 concentrations were
139.49, 119.27, and 107.36 pg ⁄ ml in the patients with
extensive AA, the patients with localized AA and the
controls, respectively (see Table S1). The mean serum level
of IL-18 was significantly higher in the patients with exten-
sive AA than in the control subjects (P < 0.05, see Fig. S1).
However, no significant differences were detected between
the patients with extensive and localized AA.
The mean serum level of IL-18 decreased from 141.34 to
114.21 pg ⁄ ml after 1 month of treatment, and the mean
level of sIL-2R decreased from 624.81 to 420.81 pg ⁄ ml over
the same period. The decrease of the serum sIL-2R concen-
tration, not IL-18, after 1 month of treatment was statisti-
cally significant (P < 0.05, see Fig. S2).
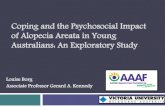
After classifying the AA patients as responder and poor-
responder groups following therapy (Fig. 1), we compared
the basal serum levels of IL-18 and sIL-2R among the two
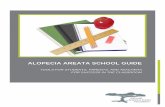
response groups and the controls. The mean serum IL-18
level in the responders was significantly higher than that in
the controls (Fig. 2a, P = 0.025, see Table S2). The mean
serum sIL-2R level in the poor-responders was significantly
higher than that in the responders (P = 0.036, see Table
S2) and that in the controls (Fig. 2b, P = 0.019).
Conclusions
In the present study, no significant difference in the mean
serum sIL-2R level was detected among the patients with
extensive AA, patients with localized AA, and control sub-
jects. On the other hand, the mean serum concentration of
sIL-2R in the patients with AA significantly decreased after
4 weeks of therapy with CsA and steroids. This is not sur-
prising because CsA inhibits T-cell activation by preventing
the transcription of IL-2 (15). Additionally, the baseline
level of sIL-2R in the poor-responders was significantly
higher than those in the responders and controls (Fig. 2b).
It is consistent with several reports suggesting positive cor-
relation between the serum sIL-2R level and disease severity
in patients with psoriasis, which shares a common immu-
nopathology with AA (16–22). Valsecchi et al. showed
serum sIL-2R level in patients with AA was significantly
higher during the active phase than the stable phase (23).
In the present study, patients with AA were all chronic, sta-
ble and refractory state. Poor-responders were thought to
be in more severe states than responders, as such the serum
level of sIL-2R was higher. The results indicate that a high
basal serum sIL-2R might be a poor prognostic marker in
patients with AA.
In the present study, the mean serum level of IL-18 in
patients with extensive AA was significantly higher than
that in the control subjects (P < 0.05). Our findings imply
that the serum level of IL-18 roughly reflects the severity of
disease in AA because extent of hair loss is a major indica-
tor of disease severity in AA. In contrast, the mean basal
serum level of IL-18 was significantly higher in the respon-
der group than in the controls (Fig. 2a). This result was
unexpected because we proposed the disease severity of
responder was less severe and would show lower IL-18 level
as in psoriasis (14). But, there are possible explanations for
these observations. First, the biologic actions of IL-18 in
AA may be different from those in psoriasis, as IL-18 does
not reflect only T cells and its precursor is expressed by
(a)
(b)
Baseline After 3 months After 7 months
Baseline After 3 months After 7 months
Figure 1. (a) Poor-responder; a 25-year-old man with alopecia
universalis, before and after combined therapy with cyclosporine and
methylprednisolone. (b) Responder; an 18-year-old man with alopecia
universalis, before and after combined therapy with cyclosporine and
methylprednisolone.
Letter to the Editor
146 ª 2009 John Wiley & Sons A/S, Experimental Dermatology, 19, 145–147

epithelial cells throughout the body (13). Second, there
may be a lag phase between disease severity and the circu-
lating IL-18 level as IL-18 increase IFN-c production, such
that the serum level may not reflect the current disease
state. There have been no studies on association between
IL-18 and AA; thus, additional studies are required to
determine its meaning.
In the present study, we demonstrated that higher levels
of sIL-2R and lower levels of IL-18 at baseline were associ-
ated with a poor prognosis in patients with AA. Additional
serial follow-up measurements of the serum concentrations
of sIL-2R and IL-18 could lead to the development of
rapid, reliable, and non-invasive prognostic markers.
References
1 Arca E, Musabak U, Akar A, Erbil A H, Tastan H B. Eur J Dermatol 2004: 14:33–36.
2 Hoffmann R. J Invest Dermatol Symp Proc 1999: 4: 235–238.3 Freyschmidt-Paul P, McElwee K J, Hoffmann R et al. Br J Dermatol 2006: 155:
515–521.4 Cho W I, Seo S J, Kim M N, Hong C K, Ro B I. Kor J Dermatol 2006: 44: 399–
404.5 Teraki Y, Imanishi K, Shiohara T. Acta Derm Venereol 1996: 76: 421–423.6 Shohat M, Mimouni D, Ben-Amitai D et al. Clin Exp Dermatol 2005: 30:
432–434.7 Kim B J, Min S U, Park K Y et al. J Dermatol Treat 2008: 19: 216–220.8 Park H H, Sim W Y. J Kor Dermatol 2002: 40: 1311–1315.9 Teshima H, Urabe A, Irie M, Nakagawa T, Nakayama J, Hori Y. Int J Dermatol
1992: 31: 513–516.10 Sun J, Silva K A, McElwee K J, King L E Jr, Sundberg J P. Exp Dermatol 2008:
17: 793–805.11 Ferron G M, Pyszczynski N A, Jusko W L. Transplantation 1998: 65: 1203–
1209.12 Rubin L A, Nelson D L. Ann Intern Med 1990: 113: 619–627.13 Dinarello C A. Semin Nephrol 2007: 27: 98–114.14 Flisiak I, Klepacki A, Chodynicka B. Biomarkers 2006: 11: 194–200.15 Cooper K D, Baadsgaard O, Ellis C N, Duell E, Voorhees J J. J Invest Dermatol
1990: 94: 649–656.16 Economidou J, Barkis J, Demetriou Z et al. Dermatology 1999: 199: 144–148.17 Kapp A, Piskorski A, Schopf E. Br J Dermatol 1988: 119: 707–710.18 Cauducci M, Mussi A, Bonifati C, Fazio M, Ameglio F. Arch Dermatol Res
1994: 286: 420–421.19 de Rie M A, Hamerlinck F, Hintzen R Q, Bos J D, van Lier R A W. Arch Derma-
tol Res 1991: 283: 533–534.20 Duncan J I, Horrocks C, Ormerod A D et al. Clin Exp Immunol 1991: 85: 293–
296.21 De Rie M A, Zonneveld I M, Witkamp L, Van Lier R A, Out T A, Bos J D. Acta
Derm Venereol 1996: 76: 357–360.22 Yamamoto T, Kimura K, Katayama I et al. Arch Dermatol Res 1996: 289:
57–59.23 Valsecchi R, Imberti G, Martino D, Cainelli T. Dermatology 1992: 184:
126–128.
Supporting information
Additional Supporting Information may be found in the
online version of this article:
Table S1. Comparison of the serum cytokine levels in
patients with extensive alopecia areata, patients with loca-
lized alopecia areata, and control subjects.
Table S2. Comparison of the baseline serum levels of IL-
18 and soluble IL-2 receptor in the patients and controls.
Figure S1. Serum levels of IL-18 in the controls and the
patients with extensive alopecia areata.
Figure S2. Changes in the serum level of soluble IL-2
receptor after combined therapy with cyclosporine and
steroids Methods.
Please note: Wiley-Blackwell are not responsible for the
content or functionality of any supporting materials sup-
plied by the authors. Any queries (other than missing
material) should be directed to the corresponding author
for the article.
Ser
um
co
nce
ntr
atio
n o
f IL
-18
(pg
/ml)
0
50
100
150
200
250
300S
eru
m c
on
cen
trat
ion
of
sIL
-2R
(p
g/m
l)
0
200
400
600
800
1000
Control Responder Poor-responder
Control Responder Poor-responder
* P < 0.05
‡ P < 0.05
†P < 0.05
(a)
(b)
Figure 2. (a) Comparison of the baseline serum levels of IL-18 among
the patient groups with alopecia areata and the controls. (b)
Comparison of the baseline levels of soluble IL-2 receptor among the
patient groups with alopecia areata and the controls (mean ± SD
values). *Responders versus controls, P = 0.025. �Poor responders versus
Responders, P = 0.036. �Poor responders versus Controls, P = 0.019.
Statistical analysis was performed with the Mann–Whitney U-test,
P < 0.05.
Letter to the Editor
ª 2009 John Wiley & Sons A/S, Experimental Dermatology, 19, 145–147 147