Septic Shock: Unbundling bundled care
69
Septic Shock: Unbundling bundled care Daniel Henning, MD, MPH Acting Instructor Division of Emergency Medicine Harborview Medical Center
Transcript of Septic Shock: Unbundling bundled care
Septic Shock: Unbundling bundled care
Daniel Henning, MD, MPH Acting Instructor
Division of Emergency Medicine Harborview Medical Center

Disclosures

Goals
• Discuss current state of bundled care for septic shock
• Discuss the evidence supporting our typical early resuscitation of septic shock
• Understand the limitations of our approach to guiding care


Early Goal Directed Therapy (EGDT)
Rivers E, Nguyen B, Havstad S, Ressler J, Muzzin A, Knoblich B, et al. Early goal-directed therapy in the treatment of severe sepsis and septic shock. New England Journal of Medicine. 2001;345(19):1368-77.


ProCESS
PROCESS Investigators, Yealy DM, Kellum JA, Huang DT, Barnato AE, Weissfeld LA, et al. A randomized trial of protocol-based care for early septic shock. New England Journal of Medicine. 2014;370(18):1683-93.
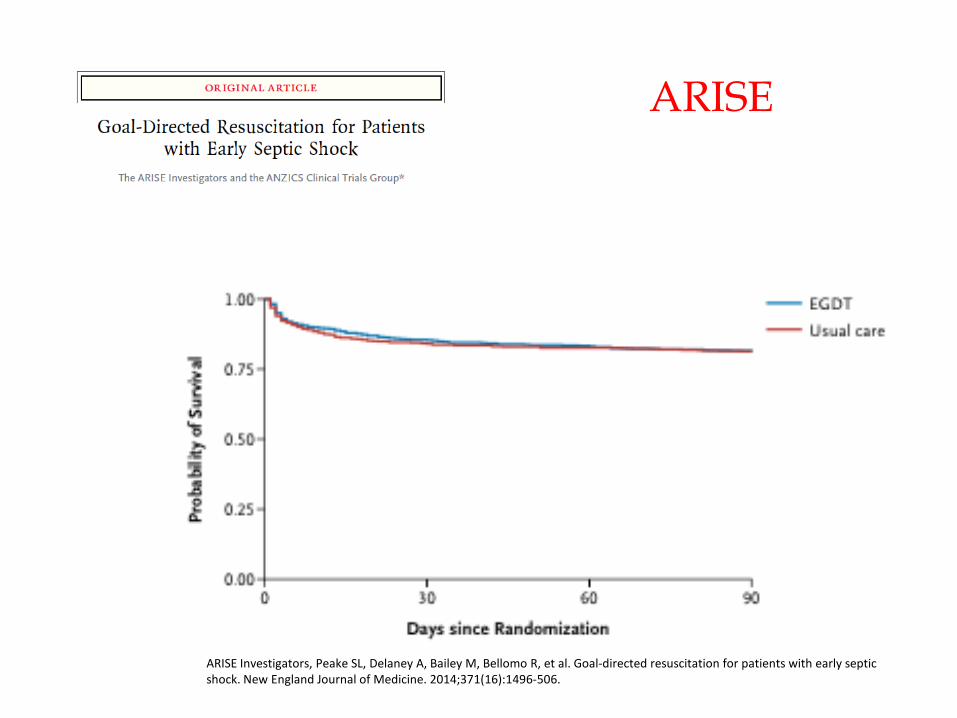
ARISE
ARISE Investigators, Peake SL, Delaney A, Bailey M, Bellomo R, et al. Goal-directed resuscitation for patients with early septic shock. New England Journal of Medicine. 2014;371(16):1496-506.
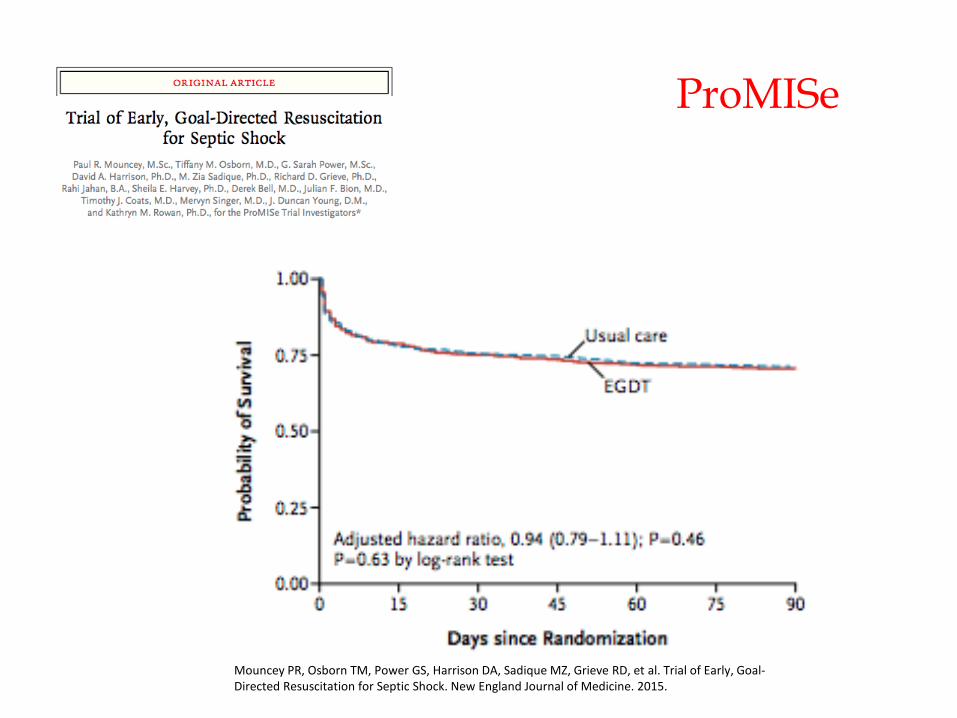
Mouncey PR, Osborn TM, Power GS, Harrison DA, Sadique MZ, Grieve RD, et al. Trial of Early, Goal-Directed Resuscitation for Septic Shock. New England Journal of Medicine. 2015.
ProMISe

EGDT Validation
Chen C, Kollef MH. Conservative fluid therapy in septic shock: an example of targeted therapeutic minimization. Critical care (London, England). 2014;18(4):481.

Study Design
Chen C, Kollef MH. Conservative fluid therapy in septic shock: an example of targeted therapeutic minimization. Critical care (London, England). 2014;18(4):481.

Study Design
Chen C, Kollef MH. Conservative fluid therapy in septic shock: an example of targeted therapeutic minimization. Critical care (London, England). 2014;18(4):481.

Data Analysis
Miller RR, Dong L, Nelson NC, Brown SM, Kuttler KG, Probst DR, et al. Multicenter implementation of a severe sepsis and septic shock treatment bundle. American Journal of Respiratory and Critical Care Medicine. 2013;188(1):77-82.

Study Design
Ferrer R, Artigas A, Suarez D, Palencia E, Levy MM, Arenzana A, et al. Effectiveness of treatments for severe sepsis: a prospective, multicenter, observational study. American Journal of Respiratory and Critical Care Medicine. 2009;180(9):861-6.

Mortality Trends
Stevenson EK, Rubenstein AR, Radin GT, Wiener RS, Walkey AJ. Two Decades of Mortality Trends Among Patients With Severe Sepsis. Critical Care Medicine. 2014;42(3):625-31.

Mortality Trends
Kaukonen K-M, Bailey M, Suzuki S, Pilcher D, Bellomo R. Mortality Related to Severe Sepsis and Septic Shock Among Critically Ill Patients in Australia and New Zealand, 2000-2012. JAMA : the journal of the American Medical Association. 2014;311(13):1308-16.

Mortality Trends
Kaukonen K-M, Bailey M, Suzuki S, Pilcher D, Bellomo R. Mortality Related to Severe Sepsis and Septic Shock Among Critically Ill Patients in Australia and New Zealand, 2000-2012. JAMA : the journal of the American Medical Association. 2014;311(13):1308-16.
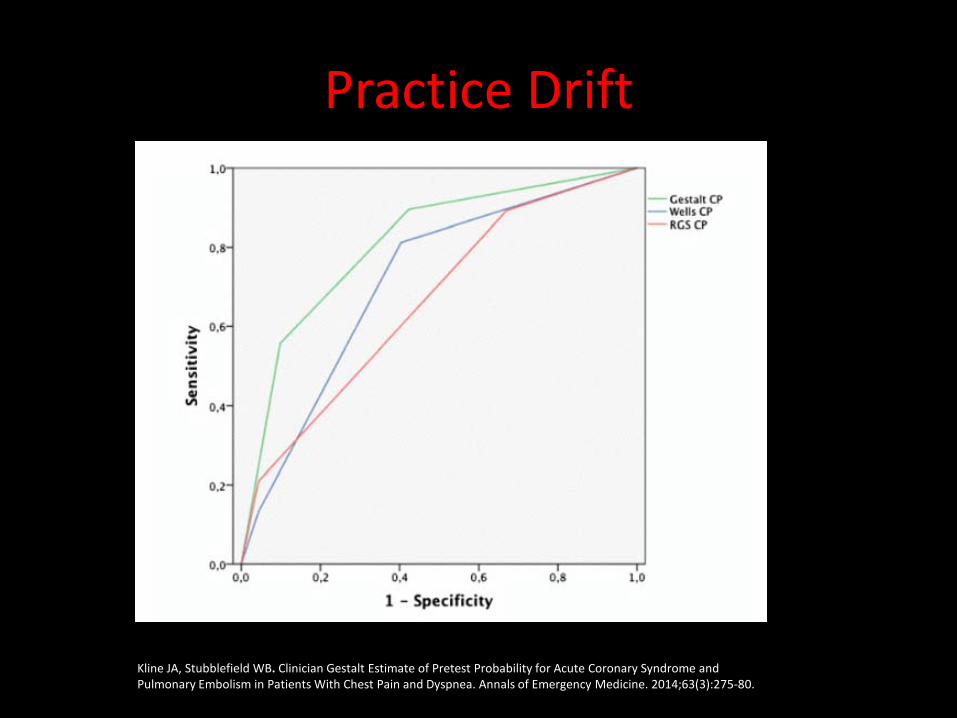
Practice Drift
Kline JA, Stubblefield WB. Clinician Gestalt Estimate of Pretest Probability for Acute Coronary Syndrome and Pulmonary Embolism in Patients With Chest Pain and Dyspnea. Annals of Emergency Medicine. 2014;63(3):275-80.
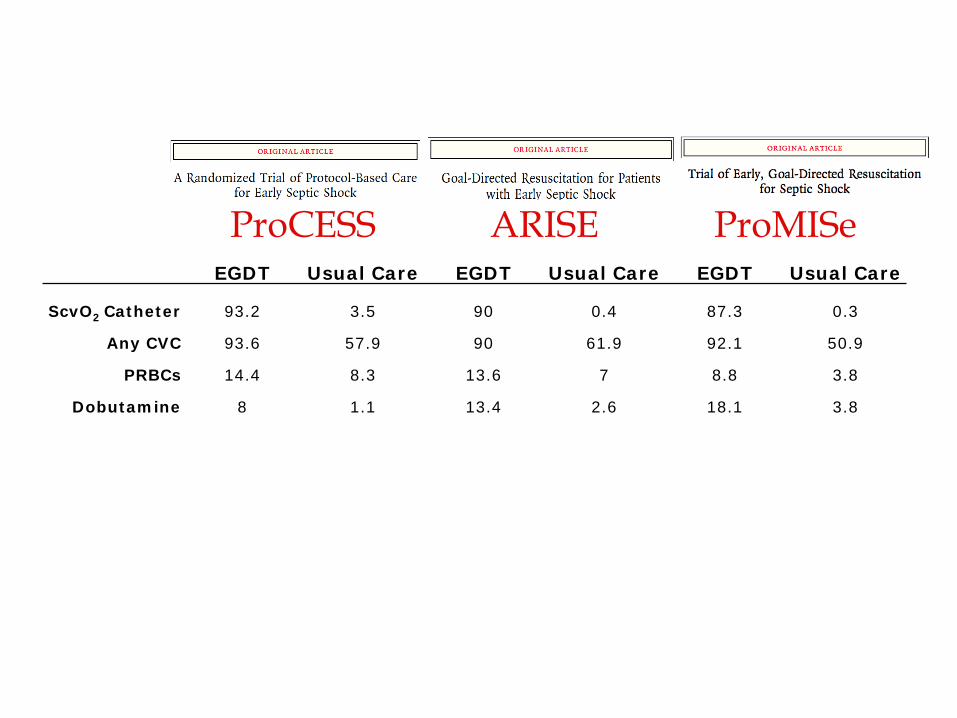
ProCESS ARISE ProMISe EGDT Usual Care EGDT Usual Care EGDT Usual Care
ScvO2 Catheter 93.2 3.5 90 0.4 87.3 0.3
Any CVC 93.6 57.9 90 61.9 92.1 50.9
PRBCs 14.4 8.3 13.6 7 8.8 3.8
Dobutamine 8 1.1 13.4 2.6 18.1 3.8

Resuscitating Septic Shock
1. Early identification and antibiotics
2. Volume expansion 3. Vasopressor support 4. Continued monitoring

Early Identification and Antibiotics
Finfer SR, Vincent J-L, De Backer D. Circulatory Shock. New England Journal of Medicine. 2013;369(18):1726-34.
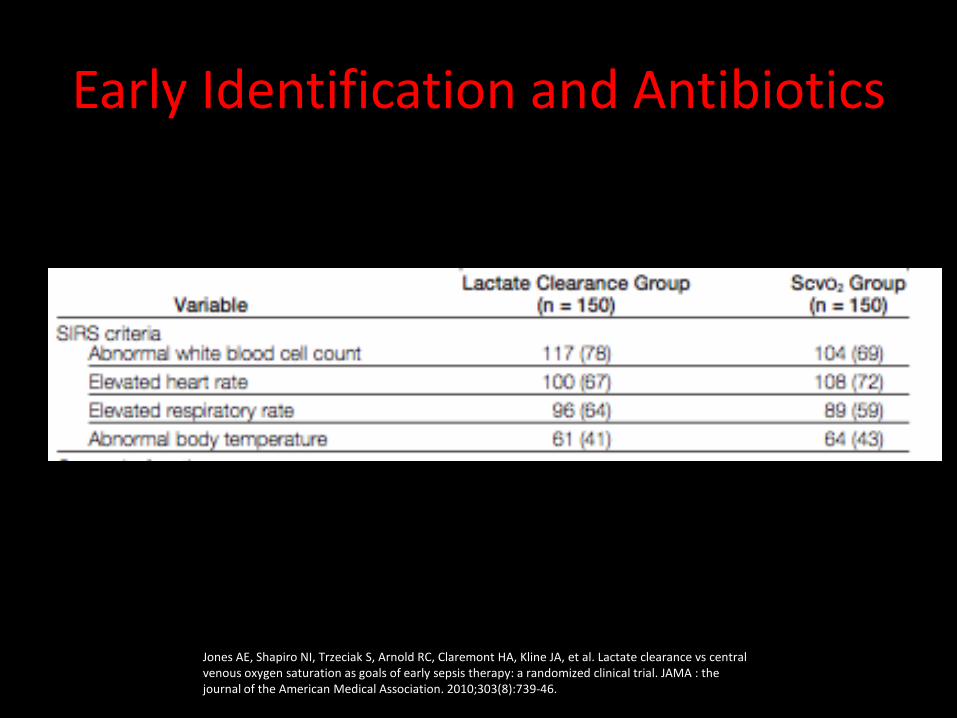
Early Identification and Antibiotics
Jones AE, Shapiro NI, Trzeciak S, Arnold RC, Claremont HA, Kline JA, et al. Lactate clearance vs central venous oxygen saturation as goals of early sepsis therapy: a randomized clinical trial. JAMA : the journal of the American Medical Association. 2010;303(8):739-46.

Early Identification and Antibiotics
SIRS in Severe Sepsis
Kaukonen K, Bailey M, Pilcher D, et al. Systemic Inflammatory Response Syndrome in Defining Severe Sepsis. NEJM. March 2015. 10.1056/NEJMoa1415236
1/8 patients with severe sepsis do not have 2+ SIRS

Early Identification and Antibiotics
11,389/29,083 (39.1%)
Young PJ, Saxena M, Beasley R, Bellomo R, Bailey M, Pilcher D, et al. Early peak temperature and mortality in critically ill patients with or without infection. Intensive Care Medicine. 2012;38(3):437-44.
Peak Temperature in first 24 hours


Early Identification and Antibiotics
Ferrer, R., Martin-Loeches, I., Phillips, G., Osborn, T. M., Townsend, S., Dellinger, R. P., et al. (2014). Empiric Antibiotic Treatment Reduces Mortality in Severe Sepsis and Septic Shock From the First Hour. Critical Care Medicine, 42(8), 1749–1755

Early Identification and Antibiotics
Chen C, Kollef MH. Conservative fluid therapy in septic shock: an example of targeted therapeutic minimization. Critical care (London, England). 2014;18(4):481.

Resuscitation
2. Volume Expansion 3. Vasopressor support
4. Continued Monitoring
Resuscitation

Resuscitation
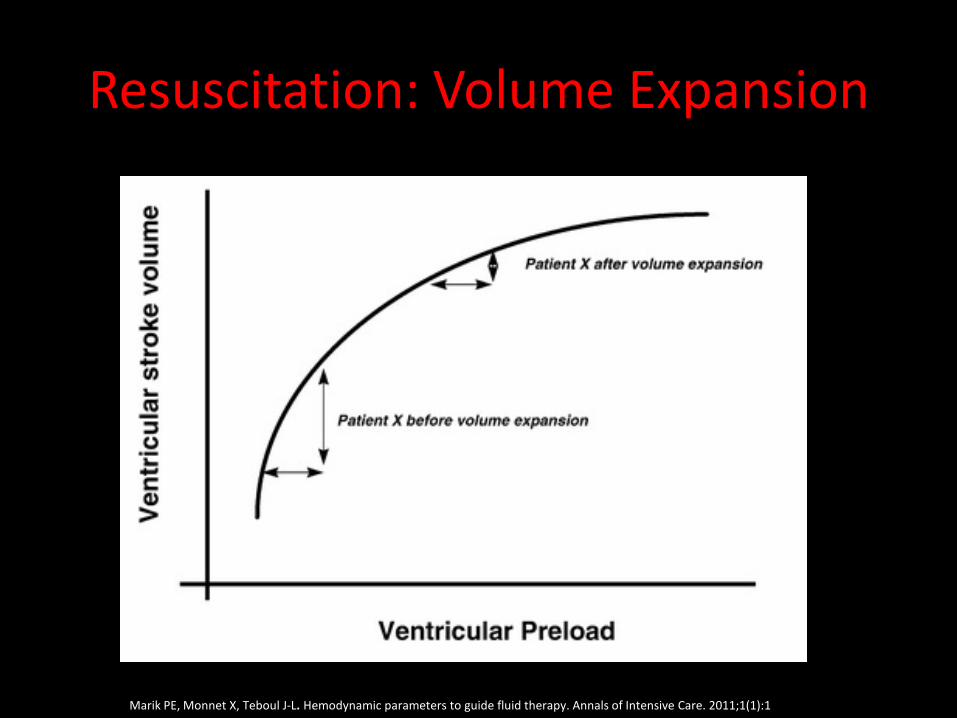
Resuscitation: Volume Expansion
Marik PE, Monnet X, Teboul J-L. Hemodynamic parameters to guide fluid therapy. Annals of Intensive Care. 2011;1(1):1

Resuscitation: Volume Expansion
How much fluid?
30 cc/kg

Resuscitation: Volume Expansion
How much fluid?
30 cc/kg…… “But not a drop more!”

ProCESS ARISE ProMISe EGDT Usual Care EGDT Usual Care EGDT Usual Care
Pre-hospital to presentation * * * * 607 599
Presentation to randomization 2254 2083 * * 1600 1790
Randomization to 6 hours 2805 2279 * * 2000 1784
Total 5059 4362 2515 2591 4207 4173

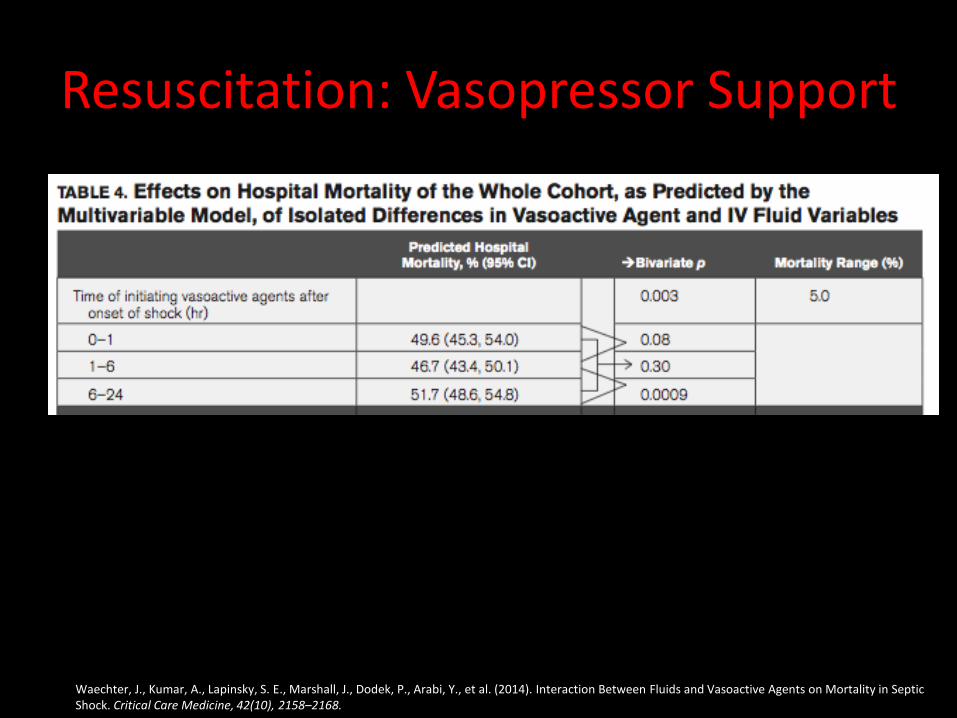
Resuscitation: Volume Expansion
Waechter, J., Kumar, A., Lapinsky, S. E., Marshall, J., Dodek, P., Arabi, Y., et al. (2014). Interaction Between Fluids and Vasoactive Agents on Mortality in Septic Shock. Critical Care Medicine, 42(10), 2158–2168. doi:10.1097/CCM.0000000000000520

Resuscitation: Volume Expansion
Central Venous Pressure (CVP) IVC Ultrasound Passive Leg Raise (PLR) Lactate
How much fluid?

Resuscitation: Volume Expansion
“This approach to fluid resuscitation is without a scientific basis and should be abandoned.”

Resuscitation: Volume Expansion
Marik PE, Monnet X, Teboul J-L. Hemodynamic parameters to guide fluid therapy. Annals of Intensive Care. 2011;1(1):1

Resuscitation: Volume Expansion
Boyd JH, Forbes J, Nakada T-a, Walley KR, Russell JA. Fluid resuscitation in septic shock: A positive fluid balance and elevated central venous pressure are associated with increased mortality*. Critical Care Medicine. 2011;39(2):259-65.
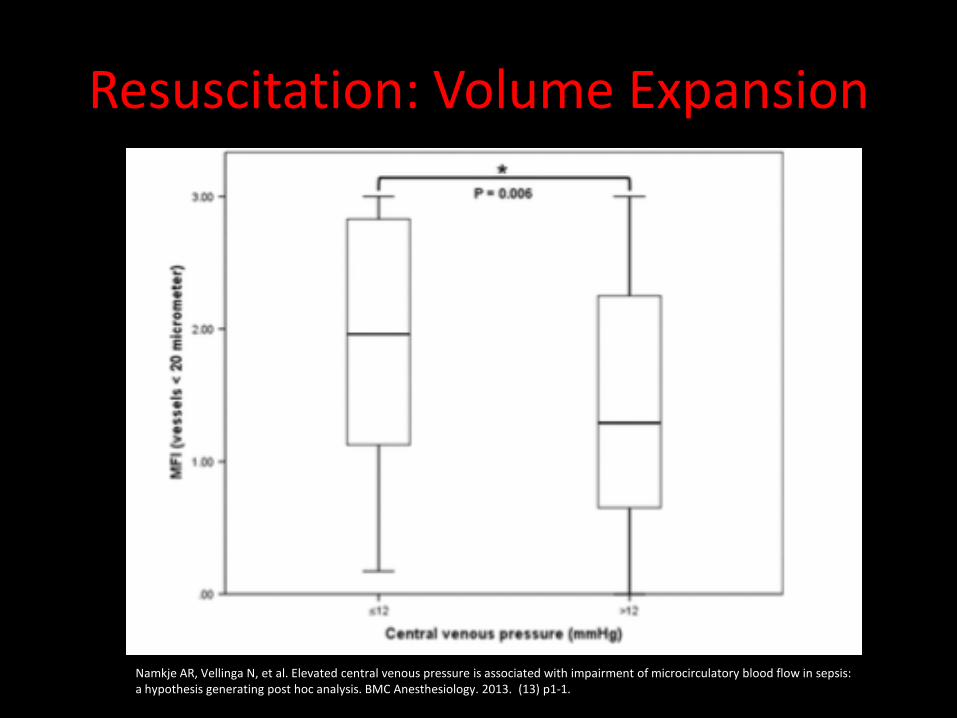
Resuscitation: Volume Expansion
Namkje AR, Vellinga N, et al. Elevated central venous pressure is associated with impairment of microcirculatory blood flow in sepsis: a hypothesis generating post hoc analysis. BMC Anesthesiology. 2013. (13) p1-1.

Resuscitation: Volume Expansion

Resuscitation: Volume Expansion
Muller L, Bobbia X, Toumi M, Louart G, Molinari N, Ragonnet B, et al. Respiratory variations of inferior vena cava diameter to predict fluid responsiveness in spontaneously breathing patients with acute circulatory failure: need for a cautious use. Critical care (London, England). 2012;16(5):R188.
IVC Ultrasound

Resuscitation: Volume Expansion
Marik PE, Monnet X, Teboul J-L. Hemodynamic parameters to guide fluid therapy. Annals of Intensive Care. 2011;1(1):1
Passive Leg Raise

Howell, M. D., Donnino, M., Clardy, P., Talmor, D., & Shapiro, N. I. (2007). Occult hypoperfusion and mortality in patients with suspected infection. Intensive Care Medicine, 33(11), 1892–1899. doi:10.1007/s00134-007-0680-5
Resuscitation: Volume Expansion
lactate
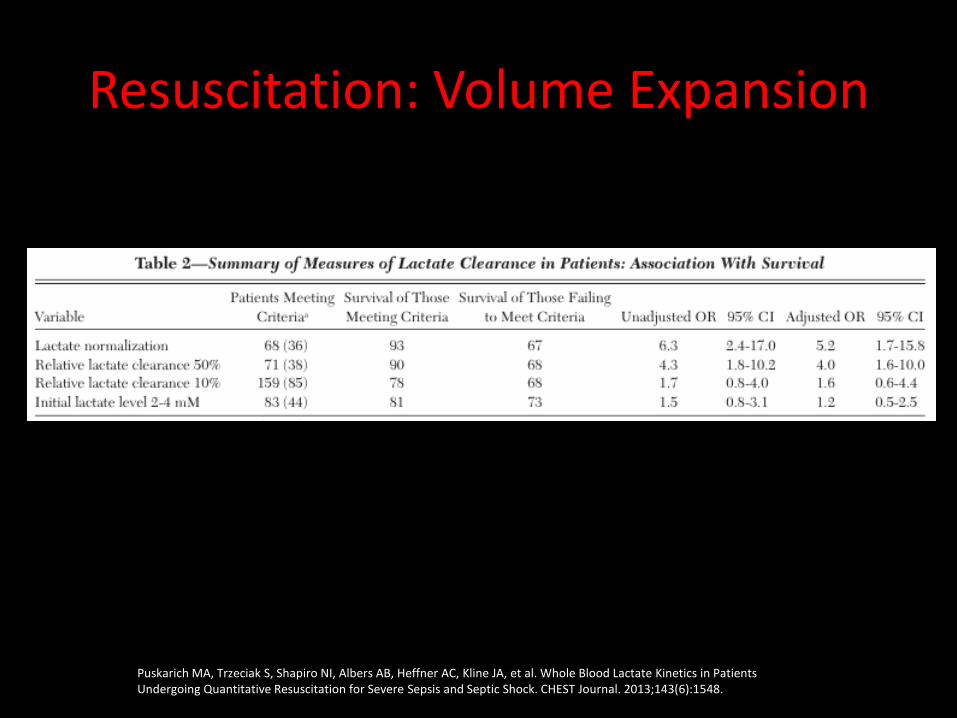
Resuscitation: Volume Expansion
Puskarich MA, Trzeciak S, Shapiro NI, Albers AB, Heffner AC, Kline JA, et al. Whole Blood Lactate Kinetics in Patients Undergoing Quantitative Resuscitation for Severe Sepsis and Septic Shock. CHEST Journal. 2013;143(6):1548.

Resuscitation: Volume Expansion
2L IV fluids, then start vasopressors Continuing IVF administration if ultrasound suggests fluid responsiveness
How much fluid?

Resuscitation: Vasopressor Support
De Backer, D., Biston, P., Devriendt, J., Madl, C., Chochrad, D., Aldecoa, C., et al. (2010). Comparison of dopamine and norepinephrine in the treatment of shock. New England Journal of Medicine, 362(9), 779–789. doi:10.1056/NEJMoa0907118

• Norepinephrine is the 1st line agent
• Add Vasopressin as second line agent (VASST)
• Dopamine if bradycardic or low likelihood of tachyarrhythmia.
Resuscitation: Vasopressor Support

Resuscitation: Vasopressor Support
Bai X, Yu W, Ji W, Lin Z, Tan S, Duan K, et al. Early versus delayed administration of norepinephrine in patients with septic shock. Critical care (London, England). 2014;18(5):532.
Waechter, J., Kumar, A., Lapinsky, S. E., Marshall, J., Dodek, P., Arabi, Y., et al. (2014). Interaction Between Fluids and Vasoactive Agents on Mortality in Septic Shock. Critical Care Medicine, 42(10), 2158–2168.
Resuscitation: Vasopressor Support
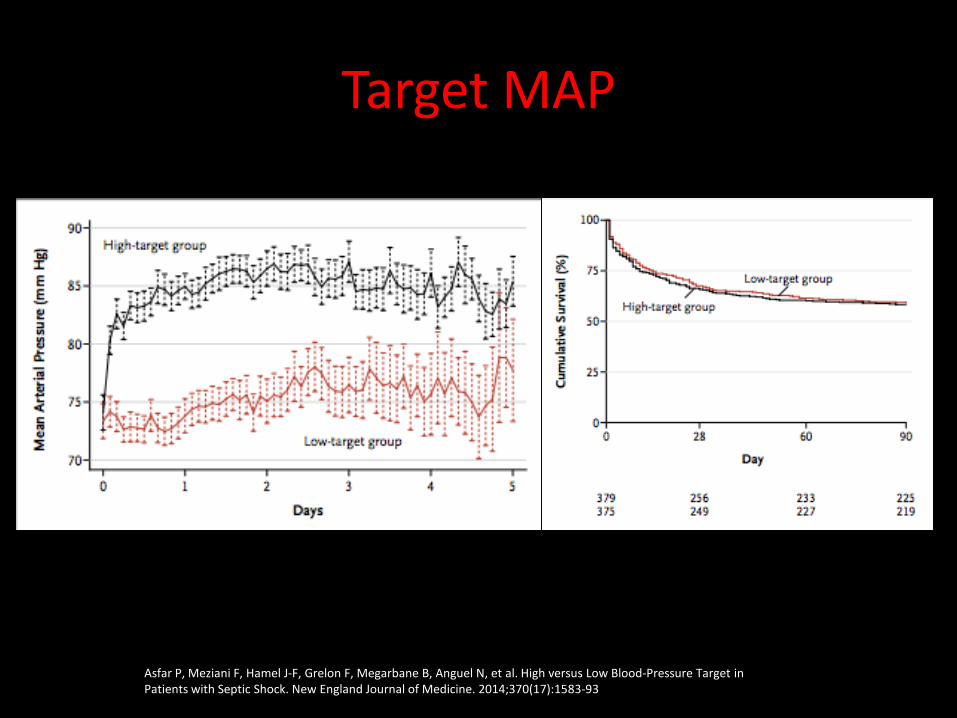
Target MAP
Asfar P, Meziani F, Hamel J-F, Grelon F, Megarbane B, Anguel N, et al. High versus Low Blood-Pressure Target in Patients with Septic Shock. New England Journal of Medicine. 2014;370(17):1583-93

Target MAP
Filbin MR, Hou PC, Massey M, Barche A, Kao E, Bracey A, et al. The Microcirculation Is Preserved in Emergency Department Low-acuity Sepsis Patients Without Hypotension. Academic Emergency Medicine. 2014;21(2):154-62.

SCVO2 vs Lactate
Resuscitation: Continued Monitoring

• Meant to assess whether the metabolic demand of cells was being met by the current delivery of oxygen.
• The major intervention in the Rivers Trial
• Intervention is PRBCs for HCT< 30 or dobutamine
Resuscitation: Continued Monitoring

Resuscitation: Continued Monitoring
Rivers E, Nguyen B, Havstad S, Ressler J, Muzzin A, Knoblich B, et al. Early goal-directed therapy in the treatment of severe sepsis and septic shock. New England Journal of Medicine. 2001;345(19):1368-77.

Resuscitation: Continued Monitoring
Jones AE, Shapiro NI, Trzeciak S, Arnold RC, Claremont HA, Kline JA, et al. Lactate clearance vs central venous oxygen saturation as goals of early sepsis therapy: a randomized clinical trial. JAMA : the journal of the American Medical Association. 2010;303(8):739-46.

ProCESS ARISE ProMISe EGDT Usual Care EGDT Usual Care EGDT Usual Care
ScvO2 Catheter 93.2 3.5 90 0.4 87.3 0.3
Any CVC 93.6 57.9 90 61.9 92.1 50.9
PRBCs 14.4 8.3 13.6 7 8.8 3.8
Dobutamine 8 1.1 13.4 2.6 18.1 3.8
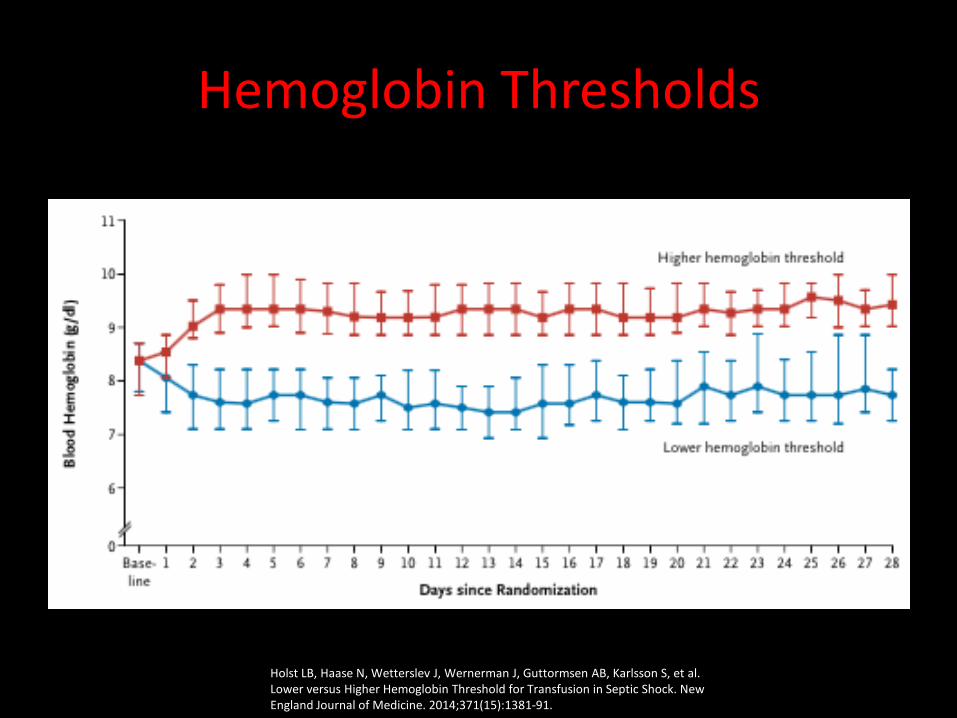
Hemoglobin Thresholds
Holst LB, Haase N, Wetterslev J, Wernerman J, Guttormsen AB, Karlsson S, et al. Lower versus Higher Hemoglobin Threshold for Transfusion in Septic Shock. New England Journal of Medicine. 2014;371(15):1381-91.

Hemoglobin Thresholds
Holst LB, Haase N, Wetterslev J, Wernerman J, Guttormsen AB, Karlsson S, et al. Lower versus Higher Hemoglobin Threshold for Transfusion in Septic Shock. New England Journal of Medicine. 2014;371(15):1381-91.

Puskarich MA, Trzeciak S, Shapiro NI, Albers AB, Heffner AC, Kline JA, et al. Whole Blood Lactate Kinetics in Patients Undergoing Quantitative Resuscitation for Severe Sepsis and Septic Shock. CHEST Journal. 2013;143(6):1548.
Resuscitation: Continued Monitoring
Lactate Clearance

Resuscitation: Continued Monitoring
Summary
The three RCTs comparing EGDT to usual care should inform our current care for patients with septic shock

Surviving Sepsis Campaign Updates
Required monitoring of central venous pressure (CVP) and central venous oxygen saturation (ScvO2) via a central venous catheter as part of an early resuscitation strategy does not confer survival benefit in all patients with septic shock who have received timely antibiotics and fluid resuscitation compared with controls.

Surviving Sepsis Campaign Updates
Requiring measurement of CVP and ScvO2 in all patients who have lactate results >4 mmol/L and/or persistent hypotension after initial fluid challenge and who have received timely antibiotics is not supported by the available scientific evidence.

Summary
• Early recognition and broad antibiotics is key
• Fluid resuscitate first, preferably guided by a dynamic test of fluid responsiveness
• Early addition of vasopressors if hypotension is not fluid responsive
• Addition of dobutamine or PRBCs on a limited basis

Questions?

Fluid Balance
Micek ST, McEvoy C, McKenzie M, Hampton N, Doherty JA, Kollef MH. Fluid balance and cardiac function in septic shock as predictors of hospital mortality. Critical Care. 2013;17(5):1-
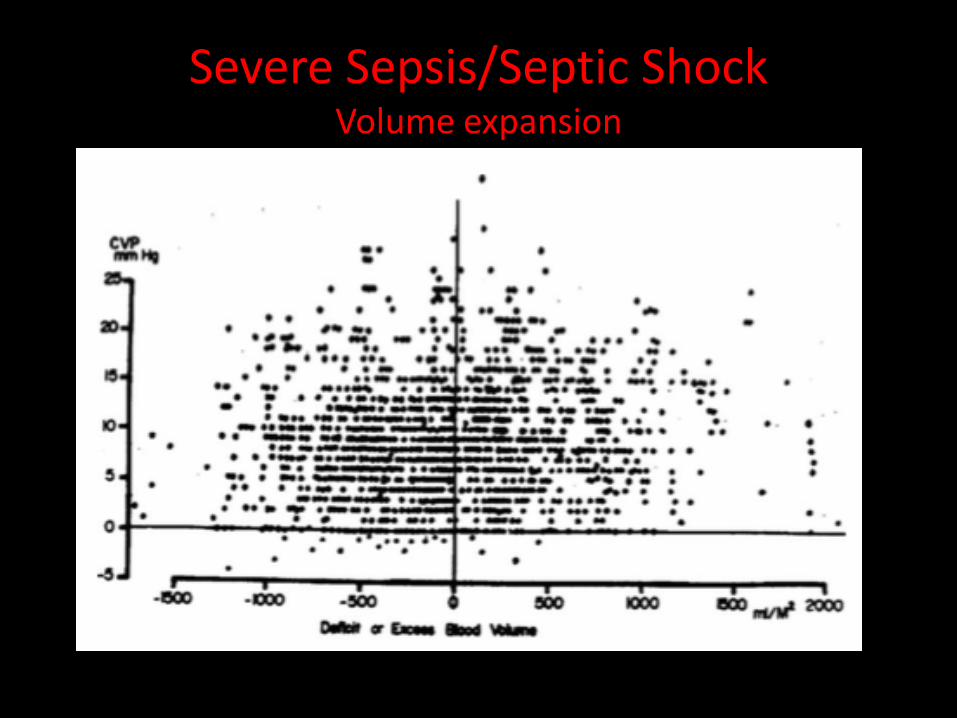
Severe Sepsis/Septic Shock Volume expansion
CVP

Resuscitation: Continued Monitoring
Pope JV, Jones AE, Gaieski DF, Arnold RC, Trzeciak S, Shapiro NI, et al. Multicenter study of central venous oxygen saturation (ScvO(2)) as a predictor of mortality in patients with sepsis. Annals of Emergency Medicine. 2010;55(1):40-6.e1.
< 70 70 < x < 90 > 90