Septic Arthritis in Children Hayan Hamameh Orthopaedic surgery resident Departmet of Orthopaedic...
52
Septic Arthritis in Children Hayan Hamameh Orthopaedic surgery resident Departmet of Orthopaedic Surgery Teshreen Military Hospital Suppervised by : Hussam Aldin Sulaiman Chief of Spine and Orthopaedic surgery department
-
Upload
kathleen-kelly -
Category
Documents
-
view
222 -
download
2
Transcript of Septic Arthritis in Children Hayan Hamameh Orthopaedic surgery resident Departmet of Orthopaedic...
Septic Arthritis in Children
Hayan HamamehOrthopaedic surgery resident
Departmet of Orthopaedic Surgery
Teshreen Military Hospital
Suppervised by :
Hussam Aldin SulaimanChief of Spine and Orthopaedic surgery department
Overview
1-Backgraound
pyogenic A.suppurative A.purulent A.pyarthrosis
Joint infection
viruses
fungi
Bacteria+++

Overview
1-Backgraound
challenging clinical problem because:
(1) signs and symptoms may be subtle and overlap with those found in other conditions.
(2) diagnosis methods are relatively insensitive.
(3) optimal management, including duration of antibiotics and surgical approach, is not evidence based.
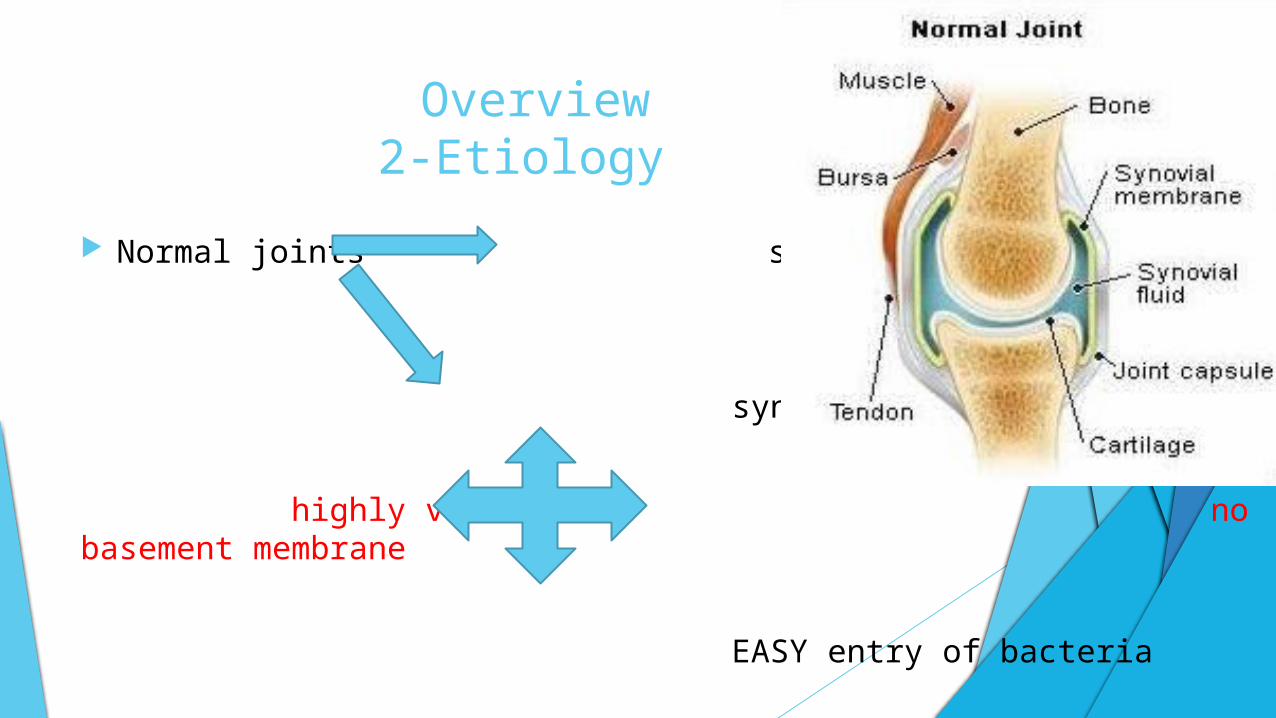
Overview2-Etiology
Normal joints synovial fluid
synovial membrane
highly vascular no basement membrane
EASY entry of bacteria

Overview2-Etiology
Bacteria deposition in S. membrane acute inflammatory cell response.
no basement plate bacteria may access to the S. fluid.
bacterial endotoxin host cells cytokines stimulate the release of proteolytic enzymes and increase leukocyte migration
Overview2-Etiology
Proteolytic enzymes damage joint cartilage + collagen matrix
inflammatory mediators, bacteria, and pus increase pressure within the joint Pressure necrosis destroy synovium or cartilage
Distension of the joint capsule may cause laxity, with possible subluxation or dislocation as a sequela
Overview2-Etiology
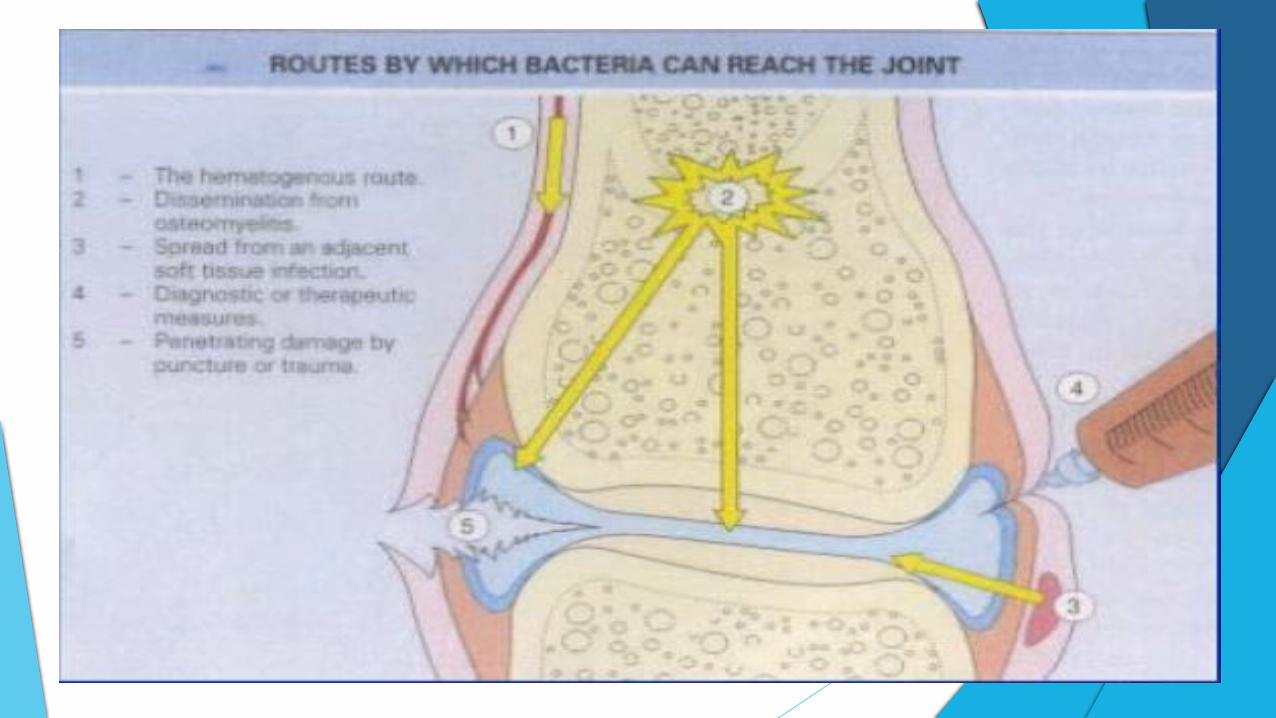
hematogenous spread
direct inoculation
extension of a contiguous focus of infection (e.g., osteomyelitis).

Overview2-Etiology
neonates and young children often have coexisting septic arthritis and osteomyelitis.
capsule insertion allowing bone infection to invade the joint space.
Nutrient capillaries & physeal plate relationship
osteomyelitis SA in 35%
SA secondary osteomyelitis RARE


Overview2-Etiology-microbiology
Gram positive
s.aureus
streptococciG
ram
n
eg
ati
ve
H. influenzae
N.meningitidis
N.gonorrheae
K.Kingae
Salmonella

Overview2-Epidemiology
Children > adults < 3 years Boys to girls 1.2-2 to 1 Lower extremity 80% Hip & knee +++ upper extremity Elbow Neonates polyarticular SA.

Risk factors for SA in neonate (younger than one month)
#Umbilical vessel catheterization
#Presence of central venous catheters
#Femoral vessel blood sampling
#Osteomyelitis

Risk factors for SA in older infants and children Immunodeficiency
joint surgery
Hemoglobinopathies
underlying arthritis == JIA
Diabetes
Overview3-Prognosispoor outcome associated with : Time to diagnosis is the most important prognostic factor (>4-7 days)
Involvement of the hip
Involvement of the hip or shoulder with concomitant osteomyelitis
Young age (i.e., less than one year)
The causative organism (Enterobacteriaceae and S. aureus)
Presentation1-History
The presentation age , site , organism.
Neonates and infants : = septicemia ( irritability, apprehension, poor feeding) or fever without a focus of infection .
lack of use of the involved extremity ("pseudoparalysis")
discomfort when handled or having the diaper changed.
extremity swelling.

Presentation1-History Older children and adolescents :
fever and constitutional symptoms (malaise, poor appetite, irritability, tachycardia)
Joint findings (e.g. swelling, tenderness) are generally present but may be subtle.
Pain with active or passive movement is a cardinal feature.
limp or refusal to walk or bear weight.
Referred pain :
SA of hip knee pain
SA of sacroiliac joint symptoms may mimic appendicitis, pelvic neoplasm, or urinary tract infection

Presentation2-Physical Examination
Decreased or absent ROM, joint tenderness, swelling, warmth, and erythema.
Joint position :
hip is flexed, abducted, and externally rotated.
The knee, ankle, and elbow are partially flexed.
shoulder is adducted and internally rotated.
Fever: mostly low-grade


DDX Transient Synovitis:
Kocher’s Criteria :
1) Fever +++
2) difficulty of bearing weight on a limb
3) ESR > 40 mm/hr
4) peripheral (WBC) > 12,000 cells/μL
were independent variables that best distinguished SA from transient synovitis.
Slipped capital femoral epiphysis
Perth's disease
Clinical features, imaging studies, and/or synovial fluid analysis usually differentiate these conditions from acute SA.

Workup
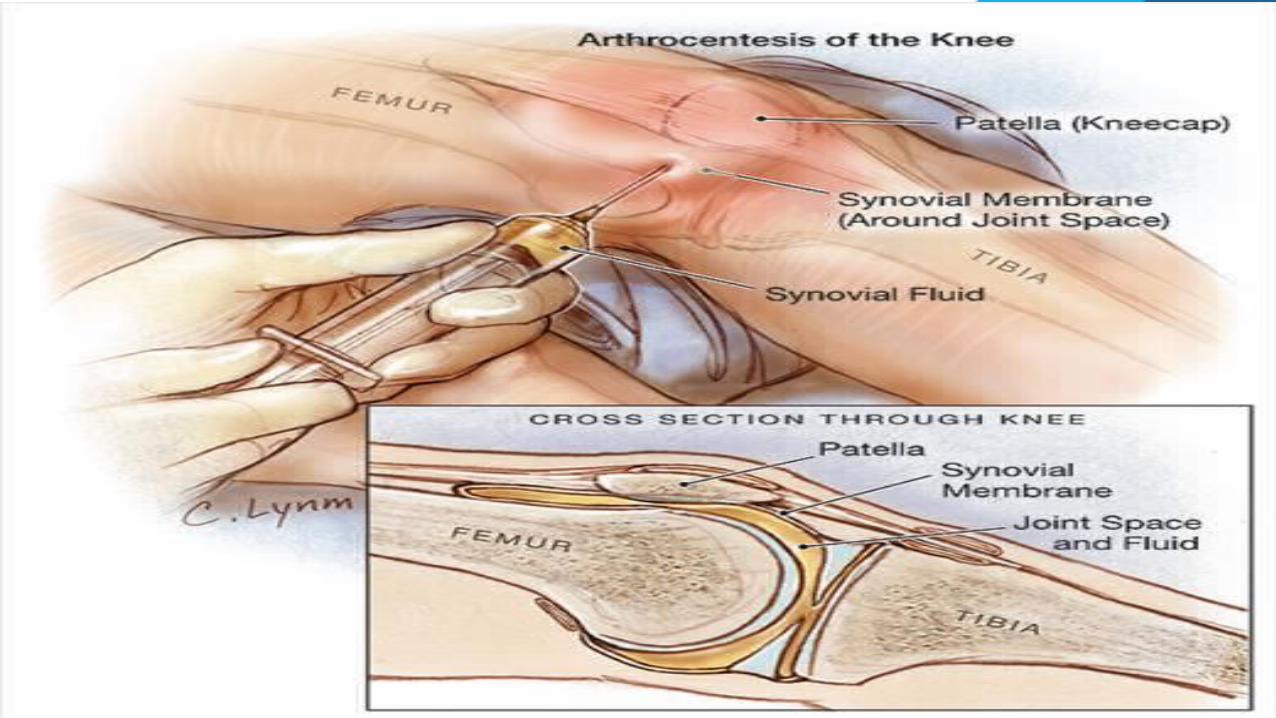
Diagnosis = clinical findings + synovial fluid analysis
low threshold for performing arthrocentesis

Workup1-laboratory studies
Blood tests (CBC ,ESR ,C-RP , culture)
Synovial fluid WBC , Gram stain , culture , and susceptibility test.
Additional lab. Studies when particular organisms are suspected

Workup1-laboratory studies - Blood tests
Peripheral WBC +ESR+C-RP usually elevated…some cases mildly elevated
ESR and/or C-RP are better – than + predictors of SA.
ESR > 20 mm/hr in most children with SA …mean= 55mm/hr
rise for 35 days after institution of appropriate therapy …my still raised for 30 days.
C-RP mean=8.5 mg/dl…rise within 3650 hrs. of onset of infection and usually falls to normal within a week of successful treatment
Better than ESR to monitor response to treatment

Workup1-laboratory studies - Blood tests
aerobic blood cultures in all patients in whom SA is a consideration
anaerobic cultures should be obtained if anaerobic infection is a concern (eg, direct inoculation).
Blood cultures are positive in approximately 40% of cases and sometimes yield the pathogen when joint fluid cultures are negative .

Workup1-laboratory studies – synovial fluid
Aspiration ASAP = identification of organisms + joint decompression
Hip aspiration + imaging guidance to confirm joint entry
heparinized syringe so that clot formation does not preclude enumeration of leukocytes

Workup1-laboratory studies – synovial fluid
synovial fluid should be obtained for (CBC), glucose, Gram stain, and culture.
Synovial culture has poor sensitivity (60-70%)
S. fluid WBC > 50,000/µL suggests SA, especially if> 100,000/mL or if a predominance of polymorphonuclear cells
The S. fluid glucose 30% of that in the serum,unique to SA.
The S. fluid WBC <50,000 cells/microL in patients with unusual causes of bacterial arthritis (eg, Brucella) and may >50,000 cells/microL in children with JIA, serum sickness, or reactive arthritis.

Workup1-laboratory studies – synovial fluid
Gram stain — bacteriostatic effects. Approximately 40- 50% of joint aspirates are sterile…
Culture — The identification of organisms in joint fluid is the primary criterion for the diagnosis of SA.
Synovial fluid cultures are positive in approximately 50-60% of patients with other clinical and laboratory findings of bacterial arthritis.
False negative synovial fluid cultures may occur with fastidious organisms, inadequate laboratory techniques, or prior treatment with antibiotics.

Workup1-laboratory studies – synovial fluid
Other studies
Polymerase chain reaction (PCR) testing for Kingella kingae and other fastidious pathogens.
Serology for Borrelia antigens should be sent when Lyme-disease-related articular disease is suspected.
Workup2-imaging studies
plain radiography
is insensitive… may be most helpful in screening for etiologies other than SA as a cause of joint pain. E.g. bony changes suggestive of osteomyelitis, bony tumors or fractures as the source of swelling, and Legg-Perthes disease or a slipped capital femoral epiphysis.
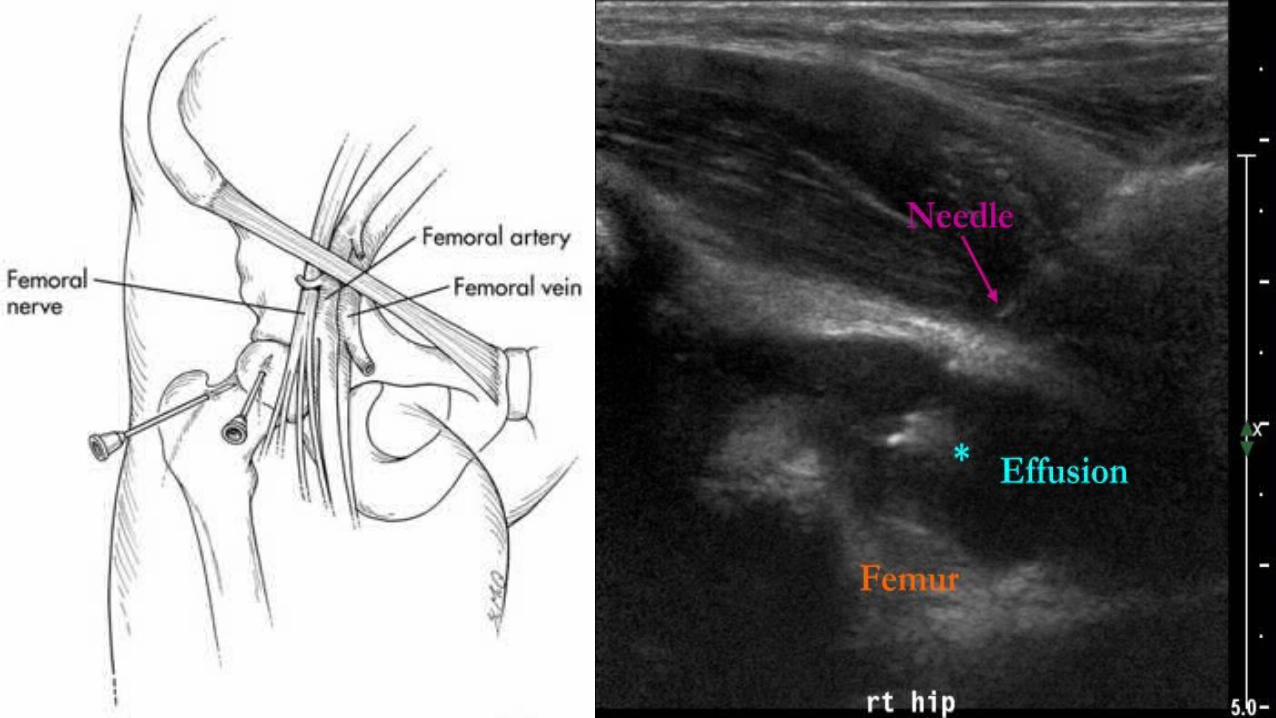
Ultrasonography
Hip effusion & to guide the aspiration needle if an effusion is detected.
Scintigraphy
limited role , may be helpful if multifocal disease is suspected in neonates
assists with the detection of an associated osteomyelitis.



Treatment
The Goals:
sterilization and decompression of the joint space
removal of inflammatory debris to relieve pain and prevent deformity or functional sequelae .
Clinical decision making in the management of the child with bacterial arthritis includes the following questions :
How should the joint be drained and irrigated?
Which antibiotics should be administered?
What is the optimal duration of antimicrobial therapy?
When is it safe to switch from parenteral to oral therapy?

Treatment
Hospitalize
Obtain cultures initiate empiric antibiotics before culture results.
immobilization 2-3 days then Encourage early passive ROM to stretch tendons and prevent contractures.
Medication- Drainage (arthrotomy , arthroscopy, needle aspiration)

Medications
ASAP after cultures
All antibiotics that have been studied readily enter the joint fluid after systemic administration; intraarticular injection of antibiotics is unnecessary.
Most children can be treated with sequential antibiotic therapy (parenteral oral) to minimize the length of hospital stay and complications from prolonged vascular access.
Adjunctive therapies:
Analgesia :Opioid (codeine or morphine)acetaminophen or ibuprofen
NSAIDs : reactive synovitis associated with bacterial arthritis
Dexamethasone ??!! :for the first four days of therapy//remains investigational
Medications
Empiric therapy:
- based on age ,clinical features , Gram stain, and local bacterial susceptibility patterns.
- includes coverage for S. aureus in all ages.
-Commonly used drugs are listed in the table
MedicationEmpiric therapy
Birth to 3 months: S.aureus , GAS S. , G- bacilli
An antistaphylococcal agent (nafcillin, oxacillin, or vancomycin)
Gentamycin or cefotaxime
vancomycin should be included in the regimen for neonates who have been in the ICU for more than one week because of the risk of nosocomial infection with (MRSA) or coagulase-negative staphylococci.

MedicationEmpiric therapy Older than three months : S. aureus , G+ organisms (GAS S. ,
pneumococci). Additional coverage for other pathogens (K. kingae, [Hib], Neisseria gonorrhoeae) may be necessary in select populations.
antistaphylococcal and antistreptococcal agents :
nafcillin , clindamycin , vancomycin , Cefazolin
MedicationSpecific therapy
Specific therapy
S.aureus 3weeks
Pneumococci/N. meningitidis 2weeks
discontinue if ESR and/or CRP have returned to normal by these time points and there is no radiographic evidence of unsuspected osteomyelitis.
Longer courses may be necessary for SA of the hip, and for arthritis caused by Enterobacteriaceae or other unusual organisms.
1970s
MedicationSpecific therapy- Route
Start parenterally
In neonates (<1 month), the entire course should be administered parenterally .the gastrointestinal absorption is unpredictable
>1 month, continue parenterally at least until clinical and laboratory improvement have been demonstrated orally
Clear improvement usually is established 5 to 10 days after initiation of antibiotic therapy. It is indicated by achievement of each of the following conditions:
*The patient has been afebrile for 48 to 72 hours
* Local signs and symptoms of infection are reduced considerably
*WBC has normalized
*CRP and/or ESR has decreased
Oral Antibiotics Complete the course in ages >1 month providing unequivocal
improvement
In randomized and observational studies, treatment of SA with IV antibiotics for short periods (approximately seven days) followed by oral therapy, was as successful as longer courses of parenteral therapy.
Subsequent oral therapy may be substituted for parenteral treatment provided that certain criteria are met:
1) Clear demonstration of clinical and laboratory improvement (ie, swelling, tenderness, and erythema, reduction of C-reactive protein)
2) Decreasing or absent fever
3) oral agent with appropriate coverage is available in a formulation that the child can swallow
4) Adherence to the antibiotic and monitoring regimen are assured
Oral Antibiotics
Cultures isolated organism susceptibility test
not isolated age, clinical features, Gram stain, and local bacterial susceptibility patterns.
Similar spectrum:
Cefazolin cephalexin
Clindamycin oral clindamycin
higher doses than antibitics used for treatment of other infections and recommended in package inserts
The initial doses of oral therapy should be administered while the child is in the hospital to ensure that the drug is tolerated.

DRAINAGE
Drainage V.S. no drainage ?? Human/animals

Arthroscopy alternative for drainage , particularly for SA of the knee.
successful arthroscopic drainage of the hip also has been reported, but the number of cases successfully managed is small and largely involves older children.
Successful management of SA of the shoulder joint of infants has also been described.
When arthroscopic drainage is performed, the surgeon must obtain a full view of the interior of the joint to ensure that no loculated pockets of purulent material remain after the procedure

Needle aspiration
discomfortable. minimal morbidity , in the older child, may not
require general anesthesia for uncomplicated SA involving joints other than the
hip or shoulder, serial needle aspirations are performed.
These may be discontinued once fluid no longer reaccumulates.

RESPONSE TO THERAPY
Clinical and laboratory improvement is indicated by:
Resolution of fever Decreased joint pain, swelling, and erythema Increased joint mobility Decrease in peripheral WBC count and synovial fluid
WBC Decrease in ESR and/or CRP

Complications Joint laxity, subluxation, or dislocation
Joint restriction
Limb-length discrepancy (if the growth plate is involved)
Avascular necrosis
Enlargement of the femoral head (coxa magna) in bacterial arthritis of the hip
Pathologic fractures
The reported complication rates vary depending upon the patient population, the involved joint, and the duration of follow-up:
residual dysfunction is 10 to 25 percent.
Even with appropriate management, approximately 40% of patients with hip involvement and 10% of patients with knee involvement develop significant complications