
Sentinel lymph node dissection in prostate cancer using ... · SUSI®; B. Braun Melsungen AG,...
7
Vol.:(0123456789) 1 3 International Urology and Nephrology (2018) 50:1427–1433 https://doi.org/10.1007/s11255-018-1903-0 UROLOGY - ORIGINAL PAPER Sentinel lymph node dissection in prostate cancer using superparamagnetic particles of iron oxide: early clinical experience M. Staník 1 · D. Macík 1 · I. Čapák 1 · N. Marečková 1 · E. Lžíčařová 2 · J. Doležel 1 Received: 22 March 2018 / Accepted: 30 May 2018 / Published online: 15 June 2018 © Springer Nature B.V. 2018 Abstract Purpose Superparamagnetic nanoparticles of iron oxide (SPION) were shown to be non-inferior to standard radioisotope tracer in breast cancer and may be used as an alternative to identify sentinel lymph nodes (SLN). The aim of this study was to assess the feasibility of sentinel lymph node dissection (SLND) using SPION in prostate cancer and to evaluate its diagnostic accuracy. Methods Twenty patients with intermediate- and high-risk prostate cancer were prospectively enrolled in 2016. After intraprostatic injection of SPION, SLND using magnetometer was performed the following day. Extended pelvic lymph node dissection (ePLND) was added as a reference standard test. The diagnostic performance of the test were evaluated, as well as the rate of in vivo detected SLN. Surgical times of SLND and ePLND were compared using paired two-sample t test. Results In total, 97 SLN were detected with median 5 (IQR 3–7) per patient. Non-diagnostic rate of the procedure was 5%. In total, 19 nodal metastases were found in 5 patients, of which 12 were located in SLN. The sensitivity per patient for the whole cohort was 80% and per node 56%. If only patients with at least one detected SLN were considered, the sensitivity per patient and per node reached 100 and 82%, respectively. A median of 20 LNs (IQR 18–22) were removed by subsequent ePLND. Surgical times of SLND and ePLND differed significantly, with medians of 17 and 39 min, respectively (p < 0.001). Conclusions SLND with SPION is feasible and safe in prostate cancer and the diagnostic accuracy is comparable to the published results of radioguided procedures. In open surgery, SPION may be used as an alternative tracer with its main advantage being the lack of radiation hazard. Keywords Prostatic neoplasms · Lymph node excision · Sentinel lymph node biopsy · Nanoparticles Introduction Pelvic lymph node dissection (PLND) remains the best stag- ing tool to detect lymph node metastases in prostate cancer [1]. In comparison to PLND, even novel imaging modali- ties like 18F-choline- and 68Ga-prostate-specific membrane antigen (PSMA) positron emission tomography (PET)/CT have rather low sensitivity to detect metastatic nodes [2, 3]. PLND is commonly performed also with curative intention as it may be of benefit in patients with minimal nodal burden [4]. On the other hand, the complication rate of PLND is not negligible and is related to the extent of the surgical tem- plate, with approximately 10% of patients presenting with symptomatic lymphocoele [4, 5]. The concept of sentinel lymph node dissection (SLND) was introduced to surgical oncology 25 years ago [6]. It pre- sumes that lymphatic spread of tumor follows an orderly path with specific lymph nodes (sentinel nodes) draining the tumor, which have the highest risk of harboring metasta- ses. This concept thereby aims to reduce morbidity, improve staging accuracy, and individualize the extent of nodal dis- section by selective removal of SLN. Although a well-established method in breast cancer and melanoma, SLND is still considered experimental in pros- tate cancer, despite many reports of its high staging accu- racy with a sensitivity of 90–95% per patient [7]. SLND has similar staging efficacy in comparison to PLND and even * M. Staník [email protected] 1 Department of Urologic Oncology, Clinic of Surgical Oncology, Masaryk Memorial Cancer Institute, Žlutý Kopec 7, 65653 Brno, Czech Republic 2 Department of Oncological and Experimental Pathology, Masaryk Memorial Cancer Institute, Žlutý Kopec 7, 65653 Brno, Czech Republic
Transcript of Sentinel lymph node dissection in prostate cancer using ... · SUSI®; B. Braun Melsungen AG,...
Vol.:(0123456789)1 3
International Urology and Nephrology (2018) 50:1427–1433 https://doi.org/10.1007/s11255-018-1903-0
UROLOGY - ORIGINAL PAPER
Sentinel lymph node dissection in prostate cancer using superparamagnetic particles of iron oxide: early clinical experience
M. Staník1 · D. Macík1 · I. Čapák1 · N. Marečková1 · E. Lžíčařová2 · J. Doležel1
Received: 22 March 2018 / Accepted: 30 May 2018 / Published online: 15 June 2018 © Springer Nature B.V. 2018
AbstractPurpose Superparamagnetic nanoparticles of iron oxide (SPION) were shown to be non-inferior to standard radioisotope tracer in breast cancer and may be used as an alternative to identify sentinel lymph nodes (SLN). The aim of this study was to assess the feasibility of sentinel lymph node dissection (SLND) using SPION in prostate cancer and to evaluate its diagnostic accuracy.Methods Twenty patients with intermediate- and high-risk prostate cancer were prospectively enrolled in 2016. After intraprostatic injection of SPION, SLND using magnetometer was performed the following day. Extended pelvic lymph node dissection (ePLND) was added as a reference standard test. The diagnostic performance of the test were evaluated, as well as the rate of in vivo detected SLN. Surgical times of SLND and ePLND were compared using paired two-sample t test.Results In total, 97 SLN were detected with median 5 (IQR 3–7) per patient. Non-diagnostic rate of the procedure was 5%. In total, 19 nodal metastases were found in 5 patients, of which 12 were located in SLN. The sensitivity per patient for the whole cohort was 80% and per node 56%. If only patients with at least one detected SLN were considered, the sensitivity per patient and per node reached 100 and 82%, respectively. A median of 20 LNs (IQR 18–22) were removed by subsequent ePLND. Surgical times of SLND and ePLND differed significantly, with medians of 17 and 39 min, respectively (p < 0.001).Conclusions SLND with SPION is feasible and safe in prostate cancer and the diagnostic accuracy is comparable to the published results of radioguided procedures. In open surgery, SPION may be used as an alternative tracer with its main advantage being the lack of radiation hazard.
Keywords Prostatic neoplasms · Lymph node excision · Sentinel lymph node biopsy · Nanoparticles
Introduction
Pelvic lymph node dissection (PLND) remains the best stag-ing tool to detect lymph node metastases in prostate cancer [1]. In comparison to PLND, even novel imaging modali-ties like 18F-choline- and 68Ga-prostate-specific membrane antigen (PSMA) positron emission tomography (PET)/CT have rather low sensitivity to detect metastatic nodes [2, 3]. PLND is commonly performed also with curative intention
as it may be of benefit in patients with minimal nodal burden [4]. On the other hand, the complication rate of PLND is not negligible and is related to the extent of the surgical tem-plate, with approximately 10% of patients presenting with symptomatic lymphocoele [4, 5].
The concept of sentinel lymph node dissection (SLND) was introduced to surgical oncology 25 years ago [6]. It pre-sumes that lymphatic spread of tumor follows an orderly path with specific lymph nodes (sentinel nodes) draining the tumor, which have the highest risk of harboring metasta-ses. This concept thereby aims to reduce morbidity, improve staging accuracy, and individualize the extent of nodal dis-section by selective removal of SLN.
Although a well-established method in breast cancer and melanoma, SLND is still considered experimental in pros-tate cancer, despite many reports of its high staging accu-racy with a sensitivity of 90–95% per patient [7]. SLND has similar staging efficacy in comparison to PLND and even
* M. Staník [email protected]
1 Department of Urologic Oncology, Clinic of Surgical Oncology, Masaryk Memorial Cancer Institute, Žlutý Kopec 7, 65653 Brno, Czech Republic
2 Department of Oncological and Experimental Pathology, Masaryk Memorial Cancer Institute, Žlutý Kopec 7, 65653 Brno, Czech Republic

1428 International Urology and Nephrology (2018) 50:1427–1433
1 3
potentially increases nodal yield by dissecting SLNs beyond the borders of extended PLND. Furthermore, it is possibly associated with lower morbidity when compared to regional nodal dissection, similar to breast cancer [4, 8, 9].
The most frequently used tracer in SLND is 99m-techne-cium (99m-Tc) which has several drawbacks, including radi-ation exposure to patients and medical staff, and problems with radiocolloid logistics [7]. To circumvent these draw-backs, the technique of SLND using superparamagnetic iron oxide nanoparticles (SPION) with intraoperative detection by a handheld magnetometer was proposed as an alternative in open surgery [10, 11]. SPION was originally introduced as an MRI contrast agent, but nowadays presents wide diag-nostic and even theranostic opportunities [12]. The diam-eter of magnetic tracer Sienna+® particles used in SLND is 60 nm, which is comparable to 99m-Tc-nanocolloid and the functional properties are also similar, as SPION are accumu-lated in the sinuses and subcapsular spaces of sentinel nodes [13]. A metaanalysis of five clinical trials in breast cancer showed non-inferiority of SPION when compared with the standard technique using 99m-Tc nanocolloid [10]. Also in prostate cancer, the first study evaluating SPION in SLND confirmed it is feasible and reliably identifies SLN [11]. In our study, we evaluated our early experience with SLND guided by SPION, its feasibility, and diagnostic accuracy.
Methods
Patients
A total of 20 patients with clinically localized or locally advanced prostate cancer whose risk of lymph node metas-tasis was higher than 5% according to Briganti nomogram were included in the study from April 2016 to April 2017 [14]. The study has been approved by the Ethical committee of Masaryk Memorial Cancer Institute and informed consent was obtained from all patients.
Patients with previous pelvic surgery or radiotherapy were excluded. All patients were in intermediate- or high-risk groups and there was no defined upper level of PSA as exclusion criterium. Clinical lymphadenopathy was ruled out by preoperative magnetic resonance (MR) and if not available, computer tomography (CT) was performed (trans-verse nodal diameter < 10 mm).
Procedure
The day before scheduled surgery, 2 ml of SPION magnetic tracer Sienna+® (Endomagnetics Ltd., Cambridge, UK) was injected into prostate with a 21G Chiba needle under transrectal ultrasound guidance. We aimed for homogenous tracer distribution by injecting the tracer in four aliquots,
two fractions per each side, in the peripheral zone of the upper and lower quadrants of the prostate. Sienna+® is a dark brown suspension of organically coated SPION with a size of around 60 nm. Before contrast injection, prophylac-tic intravenous antibiotics Amoxicillin and Metronidazole were administered. After approximately 16–18 h, patients underwent surgery. All regional lymphatic basins were extraperitoneally explored with handheld magnetometer, the Sentimag system (Endomagnetics Ltd., Cambridge, UK), to detect sentinel lymph nodes with accumulated magnetic tracer in vivo (Fig. 1). During this part of the procedure, only plastic retractors and instruments were used (Aesculap® SUSI®; B. Braun Melsungen AG, Melsungen, Germany; 3B instruments, Nové Město na Moravě, Czech republic) to avoid interference with the magnetometer. The magnetom-eter was calibrated against the lateral pelvic wall and all magnetically active nodes were considered SLN.
Subsequently, patients underwent radical prostatectomy and backup extended PLND (ePLND) comprising external iliac, obturator, and internal iliac lymph nodes. The borders of dissection were genitofemoral nerve laterally, Cooper ligament distally, and bifurcation of common iliac artery proximally. Surgery included removal of lymphatic tissue along the internal iliac vessels. All removed fibro-fatty tissue was examined ex vivo to exclude previously missed SLNs. We assessed the time needed to detect and excise SLNs per pelvic side and patient. Also, the time needed for subsequent extended PLND was evaluated.
Histologic examination
The specimens from individual pelvic regions were sent separately. The lymph nodes were palpated and fixed with
Fig. 1 Intraoperative detection of sentinel lymph node on the right pelvic side (external iliac vein marked with an arrow) by handheld magnetometer (asterisk) and corresponding magnetic activity reading on Sentimag system. Plastic retractor was used during the detection of sentinel node
1429International Urology and Nephrology (2018) 50:1427–1433
1 3
formalin. Smaller nodes were halved longitudinally and nodes thicker than 4 mm were sectioned to 2 mm slices and embedded in paraffin. Standard examination consisted of three 4 µm sections stained with hematoxylin and eosin (H&E). In addition, we conducted a special histologic evalu-ation of SLNs comprising further serial sectioning every 150 µm with H&E staining and immunohistochemical staining using widespectrum anti-cytokeratin antibody (CK AE1/AE3, Biogenex) every 300 µm. In all patients, Gleason score and 2014 International Society of Urological Pathol-ogy (ISUP) was reported for both biopsy and prostatectomy results.
Statistics
Accuracy of the SLN procedure was assessed according to consensus recommendations [7]. False positives were defined as “patients with positive SLN outside the extended PLND template with a negative extended PLND” which provides a measure of the additional diagnostic value of SLND over and above PLND. False negatives were defined as “patients with nodal metastases in extended PLND but negative SLN”. A 2 × 2 table with SLND as the index test and ePLND as the reference standard was used to calcu-late sensitivity, specificity, negative predictive value, and
positive predictive value. Discrete variables were presented as rates or percentages and continuous variables were char-acterized with median, range, or interquartile range (IQR). Surgical times of SLND and ePLND were compared using paired two-sample t test. Results were considered significant if p value < 0.05 was achieved. Statistical analyses and tests were performed using SPSS software (version 22).
Results
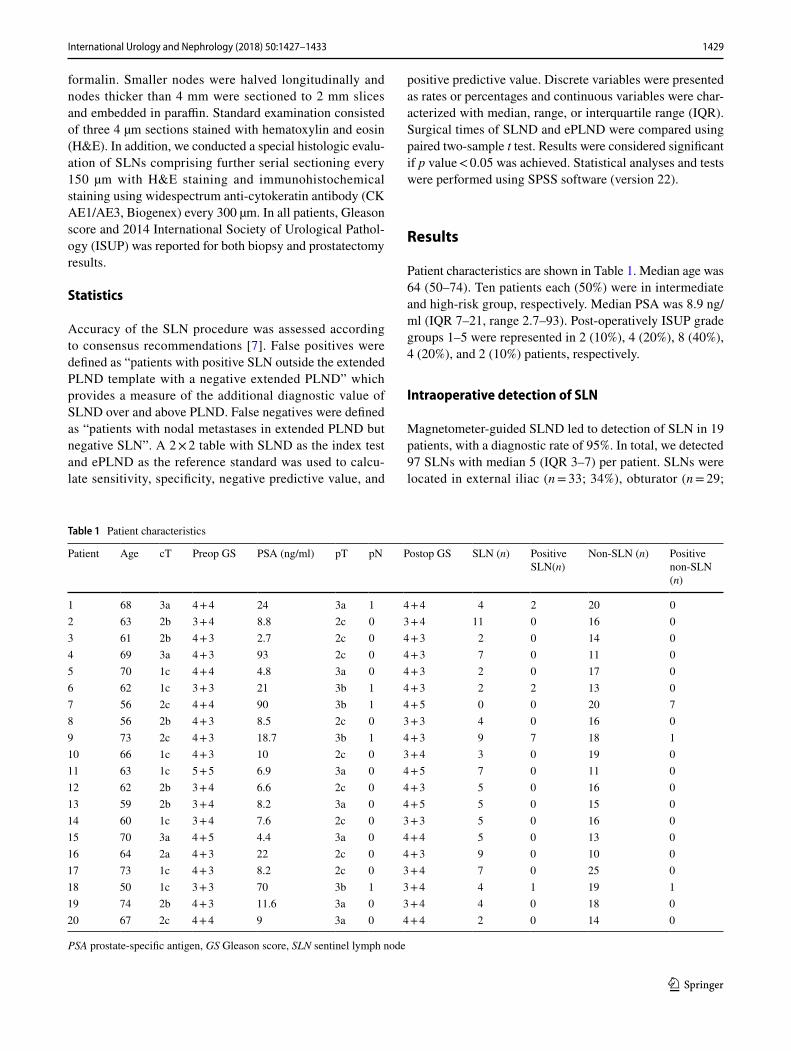
Patient characteristics are shown in Table 1. Median age was 64 (50–74). Ten patients each (50%) were in intermediate and high-risk group, respectively. Median PSA was 8.9 ng/ml (IQR 7–21, range 2.7–93). Post-operatively ISUP grade groups 1–5 were represented in 2 (10%), 4 (20%), 8 (40%), 4 (20%), and 2 (10%) patients, respectively.
Intraoperative detection of SLN
Magnetometer-guided SLND led to detection of SLN in 19 patients, with a diagnostic rate of 95%. In total, we detected 97 SLNs with median 5 (IQR 3–7) per patient. SLNs were located in external iliac (n = 33; 34%), obturator (n = 29;
Table 1 Patient characteristics
PSA prostate-specific antigen, GS Gleason score, SLN sentinel lymph node
Patient Age cT Preop GS PSA (ng/ml) pT pN Postop GS SLN (n) Positive SLN(n)
Non-SLN (n) Positive non-SLN (n)
1 68 3a 4 + 4 24 3a 1 4 + 4 4 2 20 02 63 2b 3 + 4 8.8 2c 0 3 + 4 11 0 16 03 61 2b 4 + 3 2.7 2c 0 4 + 3 2 0 14 04 69 3a 4 + 3 93 2c 0 4 + 3 7 0 11 05 70 1c 4 + 4 4.8 3a 0 4 + 3 2 0 17 06 62 1c 3 + 3 21 3b 1 4 + 3 2 2 13 07 56 2c 4 + 4 90 3b 1 4 + 5 0 0 20 78 56 2b 4 + 3 8.5 2c 0 3 + 3 4 0 16 09 73 2c 4 + 3 18.7 3b 1 4 + 3 9 7 18 110 66 1c 4 + 3 10 2c 0 3 + 4 3 0 19 011 63 1c 5 + 5 6.9 3a 0 4 + 5 7 0 11 012 62 2b 3 + 4 6.6 2c 0 4 + 3 5 0 16 013 59 2b 3 + 4 8.2 3a 0 4 + 5 5 0 15 014 60 1c 3 + 4 7.6 2c 0 3 + 3 5 0 16 015 70 3a 4 + 5 4.4 3a 0 4 + 4 5 0 13 016 64 2a 4 + 3 22 2c 0 4 + 3 9 0 10 017 73 1c 4 + 3 8.2 2c 0 3 + 4 7 0 25 018 50 1c 3 + 3 70 3b 1 3 + 4 4 1 19 119 74 2b 4 + 3 11.6 3a 0 3 + 4 4 0 18 020 67 2c 4 + 4 9 3a 0 4 + 4 2 0 14 0
1430 International Urology and Nephrology (2018) 50:1427–1433
1 3
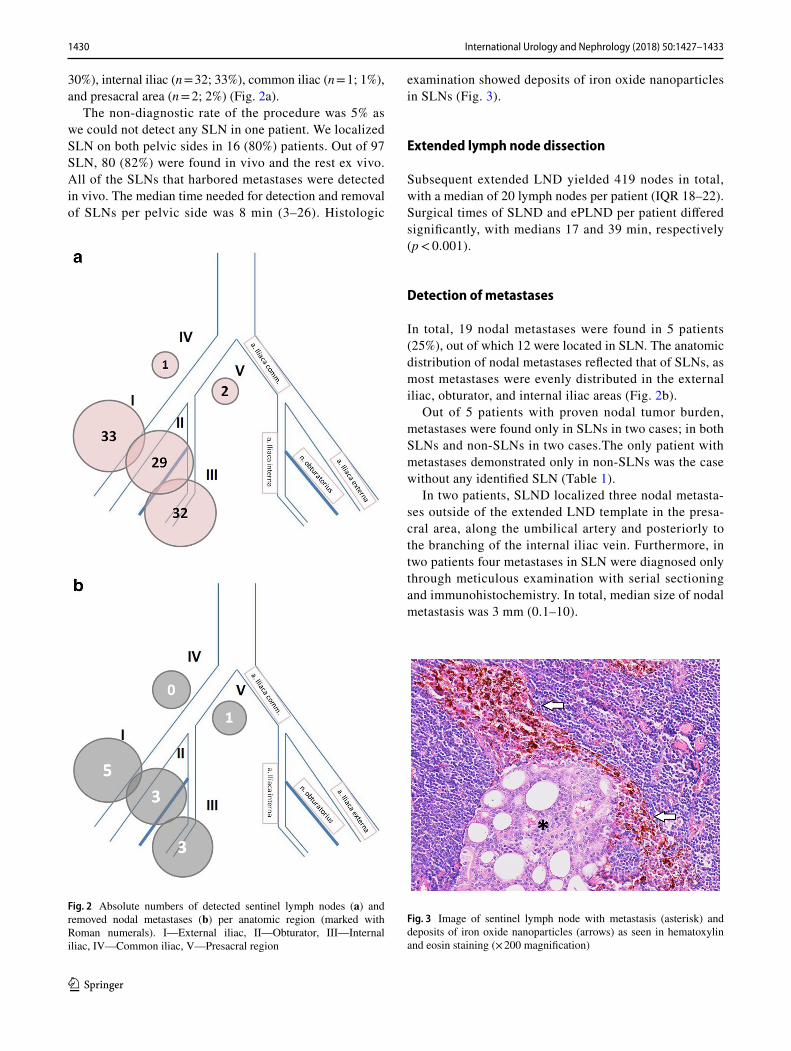
30%), internal iliac (n = 32; 33%), common iliac (n = 1; 1%), and presacral area (n = 2; 2%) (Fig. 2a).
The non-diagnostic rate of the procedure was 5% as we could not detect any SLN in one patient. We localized SLN on both pelvic sides in 16 (80%) patients. Out of 97 SLN, 80 (82%) were found in vivo and the rest ex vivo. All of the SLNs that harbored metastases were detected in vivo. The median time needed for detection and removal of SLNs per pelvic side was 8 min (3–26). Histologic
examination showed deposits of iron oxide nanoparticles in SLNs (Fig. 3).
Extended lymph node dissection
Subsequent extended LND yielded 419 nodes in total, with a median of 20 lymph nodes per patient (IQR 18–22). Surgical times of SLND and ePLND per patient differed significantly, with medians 17 and 39 min, respectively (p < 0.001).
Detection of metastases
In total, 19 nodal metastases were found in 5 patients (25%), out of which 12 were located in SLN. The anatomic distribution of nodal metastases reflected that of SLNs, as most metastases were evenly distributed in the external iliac, obturator, and internal iliac areas (Fig. 2b).
Out of 5 patients with proven nodal tumor burden, metastases were found only in SLNs in two cases; in both SLNs and non-SLNs in two cases.The only patient with metastases demonstrated only in non-SLNs was the case without any identified SLN (Table 1).
In two patients, SLND localized three nodal metasta-ses outside of the extended LND template in the presa-cral area, along the umbilical artery and posteriorly to the branching of the internal iliac vein. Furthermore, in two patients four metastases in SLN were diagnosed only through meticulous examination with serial sectioning and immunohistochemistry. In total, median size of nodal metastasis was 3 mm (0.1–10).
Fig. 2 Absolute numbers of detected sentinel lymph nodes (a) and removed nodal metastases (b) per anatomic region (marked with Roman numerals). I—External iliac, II—Obturator, III—Internal iliac, IV—Common iliac, V—Presacral region
Fig. 3 Image of sentinel lymph node with metastasis (asterisk) and deposits of iron oxide nanoparticles (arrows) as seen in hematoxylin and eosin staining (× 200 magnification)

1431International Urology and Nephrology (2018) 50:1427–1433
1 3
Accuracy of the SLND procedure
With ePLND as the reference test, the sensitivity of SLND per patient for the whole cohort was 80% (95% CI 38–96) and per node 56% (95% CI 30–80) (Table 2). False negativ-ity and false positivity rates per patient were 20 and 0%, respectively. Per node, the rates were 44 and 4%, respec-tively. Furthermore, per patient, SLND demonstrated spec-ificity of 100%, positive and negative predictive value of 100% (95% CI 51–100) and 94% (95% CI 72–99), respec-tively. If only patients with at least one detected SLN were considered, the sensitivity per patient and per node would be 100% (95% CI 51–100) and 82% (95% CI 52–95), respec-tively, and negative predictive value per patient 100% (95% CI 80–100).
Complications of the procedure
There were no infectious or bleeding complications related to intraprostatic biopsy of the tracer. Intraoperatively, no complication occurred in relation to SLND or ePLND. In two patients (10%), symptomatic lymphocoele was detected postoperatively requiring percutaneous drainage (Clavien 3a). There was no thromboembolic complication.
Discussion
In nodal staging, SLND represents a step towards pre-cision, limiting the extent of dissection of ePLND and concentrating on the risk nodes only. It suggests that the metastatic process via lymphatics follows a hierarchical path through a nodal chain and in the last 25 years; SLND has become a standard technique of nodal staging in breast cancer and melanoma. According to a recent systematic review, SLND has the same staging accuracy as PLND in prostate cancer patients [7]. Notably, SLND leads to higher detection of metastases through the removal of
nodes outside the template and meticulous histopathologic examination of SLNs [15]. The most frequently used tracer in SLND is radiocolloid, however, recently a magnetic tracer using SPION has been shown to be non-inferior to radiocolloid in studies with breast cancer [10].
In our study, we demonstrated that SLND with SPION has a high detection rate of 95%, high specificity of 100% but slightly lower sensitivity of 80% due to a false nega-tive case. In one high-risk patient, we could not detect any SLN and definitive analysis showed nodal metastases in 5 non-SLNs, which influenced mainly the per node sensitiv-ity of our study. It is well known that one of the limita-tions of SLND in advanced disease may be obliteration of lymphatics with tumor, leading to either a non-diagnostic case without any visualized SLN or to a false negative case [16]. According to recent consensus, it is agreed that in those cases where no SLN was visualized, PLND should be performed [17]. Interestingly, in patients with at least one SLN detected, the sensitivity per patient was 100% in our cohort. In comparison, a recent systematic review reported a diagnostic rate of 95.9% and a median cumula-tive sensitivity of 95.2% for SLND with radiotracer [7].
The pattern of anatomic distribution of SLNs and metastases in our study was similar to previous mapping studies [15, 18], confirming that most of metastases are located in the template of extended PLND (external iliac, obturator and internal iliac). Interestingly, we detected one out of 12 (8%) metastatic SLNs in presacral region. This is in agreement with landmark mapping study by Joniau et al., which included presacral and common iliac nodes in the template of PLND; they showed that presacral metas-tases were quite frequent (8%) in 4 out of 74 examined patients [18]. As a result, the authors proposed superex-tended template of PLND, comprising the presacral nodes, however, any expansion of PLND template must be out-weighed by clear clinical benefit, which in this case has not yet been demonstrated.
The largest experience with SPION comes from studies in breast cancer. A recent metaanalysis of seven studies with 1118 patients demonstrated similar detection rates (94–98%) and concordance rates per patient between SPION and the conventional technique with radiotracer, with a slightly higher detection rate per node in the SPION group [10]. In prostate cancer, Winter et al. reported their initial experience with SPION in 20 patients. They showed a high diagnostic rate of 90% and sensitivity of 100%, as all nodal metastases were found only in SLNs [11]. The same group later pub-lished an expanded cohort of 104 high-risk patients with an exceptionally high diagnostic rate of 100%. They also demonstrated very high sensitivity of 96.6% and specificity of 95.6%, with low false negative rate of 3.4% [19]. In their study, the median of 8 detected SLN was higher than the 5 SLN in our cohort. In comparison, the median number of
Table 2 Diagnostic performance of sentinel lymph node dissection
SLN sentinel lymph node
Per patientN (%)
Per node (SLN)N (%)
Diagnostic rate 19/20 (95%) 80/97 (82%) in vivoSensitivity 4/5 (80%) 9/16 (56%)Specificity 15/15 (100%) 74/77 (96%)Negative predictive value 15/16 (94%) 74/81 (91%)Positive predictive value 4/4 (100%) 9/12 (75%)False negativity 1/5 (20%) 7/16 (44%)False positivity 0% 3/77 (4%)Metastases in SLNs only 2/5 (40%) 12/19 (63%)

1432 International Urology and Nephrology (2018) 50:1427–1433
1 3
detected SLNs in the previously published studies of SLND as assessed by Wit et al. was four.
Regarding the staging and curative potential of SLND, it is very important to distinguish between sensitivity per patient and per node, as the former is usually very high, around 90–95%, and reflects good performance as a staging procedure. However, the latter is usually much lower, around 50–70%, which is due to the presence of metastases also in non-sentinel lymph nodes. Therefore, especially in high risk patients with more advanced disease and more positive higher tier nodes, SLND may leave metastases behind if performed without extended PLND, therefore, it is presently recommended to combine these two techniques in high-risk patients [7, 17]. The frozen section of SLN may not be help-ful to decide in which patients ePLND should be added, as intraoperatively the pathologist is not able to examine the median of 4–7 SLNs thoroughly and without extensive SLN sectioning the sensitivity of frozen section is only 40% for the detection of micrometastases [20].
In agreement with the aforementioned, the sensitivity per node in our study was 56%. Similarly, in the study by Winter et al. only 56% of patients with positive nodes had metas-tases detected in SLNs only; in our study the rate was 63%. This is a problem also with other tracers. Based on a recent systematic review of SLND with radiotracer, metastases were found in SLN only with median of 69% [7].
Despite lower per node sensivity, the concept of SLND should not be dismissed in prostate cancer as there are sev-eral arguments for it. First, SLND offers more accurate stag-ing than ePLND, with fewer nodes subjected to meticulous histological examination that leads to higher detection of micrometastases [15]. Second, SLND may detect up to 8% of nodal metastases outside the ePLND template (false posi-tive rate) [7]. Third, SLND as an optimal staging procedure may serve as a stratification tool for adjuvant treatment [4, 7]. Fourth, the curative potential of ePLND has not been convincingly proven and we have to wait for results of rand-omized studies [4]. ePLND without adjuvant treatment leads to biochemical recurrence free survival in a maximum of 30% of those patients with positive nodes and the best out-comes of PLND are expected if only 1–2 positive nodes are present. These cases with limited nodal involvement rep-resent the scenario in which SLND may even be curative, because metastases will probably be limited to SLN [21]. Fifth and finally, the concept of SLND means less trauma and less morbidity associated with nodal dissection, as shown for breast cancer, although this remains to be proven in randomized trials for prostate cancer.
One of the limitations of using SPION as a guiding tracer for SLND is a lack of preoperative imaging and anatomic delineation of SLNs. In radioguided surgery for prostate cancer, single-photon emission computed tomog-raphy (SPECT) is available for preoperative planning of the
dissection. Recently, a feasibility study showed that preop-erative MRI can be used to localize SLNs before surgery in breast and prostate cancer as nodes with uptake of tracer have decreased signal intensity in T2-weighted images [22]. In 30 patients with prostate cancer, a preoperative MRI was performed the day after SPION injection and the authors reported a high detection rate of 100% with an extremely high median of 14 SLNs detected, probably depicting higher tier nodes, therefore, more studies are needed to refine the technique and examination protocol [23].
The near future may bring even more precision regarding nodal staging, with the focus shifting from sentinel nodes to metastatic nodes only. Better functional imaging, with PSMA-based PET/CT as an example, has the potential to improve preoperative staging and also to intraoperatively guide the detection of lymph node metastases, with tracer selectively accumulated in metastatic nodes due to its link-age to tumor cells [24].
Conclusion
SLND with SPION is feasible in prostate cancer and the diagnostic accuracy is comparable to the published results of radioguided procedure. Although SLND is a promising pro-cedure, potentially reducing morbidity of lymphadenectomy, further studies are needed to define its role and added value. Magnetic tracer is an attractive alternative to radiocolloid as it poses no radiation hazards and the procedure is completely in the hands of the urologist. An absence of preoperative imaging of SLN is a potential drawback; therefore, the role of MRI in this setting has to be explored.
Acknowledgements Supported by the Ministry of Health of the Czech Republic MH CZ—DRO (MMCI, 00209805).
Compliance with ethical standards
Conflict of interest The authors declare that they have no conflict of interest.
Ethical approval All procedures performed in studies involving human participants were in accordance with the ethical standards of the insti-tutional and/or national research committee and with the 1964 Helsinki declaration and its later amendments or comparable ethical standards.
References
1. Mottet N, Bellmunt J, Bolla M et al (2017) EAU-ESTRO-SIOG guidelines on prostate cancer. Part 1: screening, diagnosis, and local treatment with curative intent. Eur Urol 71:618–629
2. Budiharto T, Joniau S, Lerut E et al (2011) Prospective evaluation of 11C-choline positron emission tomography/computed tomog-raphy and diffusion-weighted magnetic resonance imaging for the

1433International Urology and Nephrology (2018) 50:1427–1433
1 3
nodal staging of prostate cancer with a high risk of lymph node metastases. Eur Urol 60:125–130
3. Maurer T, Gschwend JE, Rauscher I et al (2016) Diagnostic effi-cacy of 68gallium-PSMA positron emission tomography com-pared to con-ventional imaging for lymph node staging of 130 consecutive patients with intermediate to high risk prostate cancer. J Urol 195:1436–1443
4. Fossatti N, Willemse PM, Van den Broeck T et al (2017) The benefits and harms of different extents of lymph node dissection during radical prostatectomy for prostate cancer: a systematic review. Eur Urol 72:84–109
5. Briganti A, Blute ML, Eastham JH et al (2009) Pelvic lymph node dissection in prostate cancer. Eur Urol 55:1251–1265
6. Alex JC, Krag DN (1993) Gamma-probe guided localization of lymph nodes. Surg Oncol 2:137–143
7. Wit EMK, Acar C, Grivas N et al (2017) Sentinel node procedure in prostate cancer: a systematic review to assess diagnostic accu-racy. Eur Urol 71:596–605
8. Bafford A, Gadd M, Gu X, Lipsitz S, Golshan M (2010) Diminish-ing morbidity with the increased use of sentinel node biopsy in breast carcinoma. Am J Surg 200:374–377
9. Winter A, Vogt C, Weckermann D, Wawroschek F (2011) Compli-cations of pelvic lymphadenectomy in clinically localised prostate cancer: different techniques in comparison and dependency on the number of removed lymph nodes. Aktuelle Urol 42:179–183
10. Teshome M, Wei C, Hunt KK, Thompson A, Rodriguez K, Mit-tendorf EA (2016) Use of a magnetic tracer for sentinel lymph node detection in early-stage breast cancer patients: a meta-anal-ysis. Ann Surg Oncol 23:1508–1514
11. Winter A, Woenkhaus J, Wawroschek F (2014) A novel method for intraoperative sentinel lymph node detection in prostate cancer patients using superparamagnetic iron oxide nanoparticles and a handheld magnetometer: the initial clinical experience. Ann Surg Oncol 21:4390–4396
12. Thomas R, Park IK, Jeong YY (2013) Magnetic iron oxide nano-particles for multimodal imaging and therapy of cancer. Int J Mol Sci 14:15910–15930
13. Winter A, Engels S, Wawroschek F (2018) Sentinel lymph node surgery in prostate cancer using magnetic particles. Curr Opin Urol 28:184–190
14. Briganti A, Larcher A, Abdollah F, Capitanio U (2012) Updated nomogram predicting lymph node invasion in patients with
prostate cancer undergoing extended pelvic lymph node dissec-tion: the essential importance of percentage of positive cores. Eur Urol 61:480–487
15. Staník M, Čapák I, Macík D et al (2014) Sentinel lymph node dis-section combined with meticulous histology increases the detec-tion rate of nodal metastases in prostate cancer. Int Urol Nephrol 46:1543–1549
16. Nguyen DP, Huber PM, Metzger TA, Genitsch V, Schudel HH, Thalmann GN (2016) A specific mapping study using fluores-cence sentinel lymph node detection in patients with intermediate- and high-risk prostate cancer undergoing extended pelvic lymph node dissection. Eur Urol 70:734–737
17. van der Poel HG, Wit EM, Acar C, van den Berg NS et al (2017) Sentinel node biopsy for prostate cancer: report from a consensus panel meeting. BJU Int 120:204–211
18. Joniau S, Van den Bergh L, Lerut E et al (2013) Mapping of pelvic lymph node metastases in prostate cancer. Eur Urol 63:450–458
19. Winter A, Engels S, Reinhardt L, Wasylow C, Gerullis H, Wawro-schek F (2017) Magnetic marking and intraoperative detection of primary draining lymph nodes in high-risk prostate cancer using superparamagnetic iron oxide nanoparticles: additional diagnostic value. Molecules. https ://doi.org/10.3390/molec ules2 21221 92
20. Liu LC, Lang JE, Lu y et al (2011) Intraoperative frozen section analysis of sentinel lymph nodes in breast cancer patients: a meta-analysis and single-institution experience. Cancer 117:250–258
21. Touijer KA, Mazzola CR, Sjoberg DD, Scardino PT, Eastham JA (2014) Long-term outcomes of patients with lymph node metasta-sis treated with radical prostatectomy without adjuvant androgen-deprivation therapy. Eur Urol 65:20–25
22. Pouw JJ, Grootendorst MR, Bezooijen R et al (2015) Pre-operative sentinel lymph node localization in breast cancer with superpara-magnetic iron oxide MRI: the SentiMAG multicentre trial imaging subprotocol. Br J Radiol 88:20150634
23. Winter A, Kowald T, Paulo T et al (2016) Magnetic resonance sentinel lymph node imaging in prostate cancer using intrapros-tatic injection of superparamagnetic iron oxide nanoparticles: the first in-human results. Eur Urol Suppl 15(Suppl 3):1060
24. Maurer T, Gschwend JE, Eiber M (2018) Prostate-specific mem-brane antigen-guided salvage lymph node dissection in recurrent prostate cancer: a novel technology to detect lymph node metas-tases. Curr Opin Urol 28:191–196


















